 Helia Robert-Ebadi
Helia Robert-Ebadi Grégoire Le Gal2,3
Grégoire Le Gal2,3 Marc Righini
Marc Righini- 1Division of Angiology and Hemostasis, Geneva University Hospitals and Faculty of Medicine, Geneva, Switzerland
- 2Department of Medicine, Ottawa Hospital Research Institute, University of Ottawa, Ottawa, ON, Canada
- 3EA3878 University of Brest, Brest, France
Pulmonary embolism (PE) is one of the most common causes of severe morbidity and mortality during pregnancy. PE diagnosis during pregnancy remains a true challenge for all physicians, as many of the symptoms and signs associated with PE are often reported during physiological pregnancy. The fear of missing a PE during pregnancy leads a low threshold of suspicion, hence to a low prevalence of confirmed PE among pregnant women with suspected PE. This means that most pregnant women with suspected PE do not have the disease. Until recently, international guidelines suggested thoracic imaging in all pregnant women with suspected PE. Two recent prospective management outcome studies based on clinical probability assessment, D-dimer measurement, venous compression ultrasonography of the lower limbs (CUS) and computed tomography pulmonary angiography (CTPA) proved the safety of such strategies, with a very low failure rate. For the first time, these studies also demonstrated that the association of a clinical prediction rule and D-dimer measurement allowed a safe exclusion of PE in a significant proportion of pregnant women, without the need for radiating imaging tests. These two prospective studies pave the way to further improvements in the diagnostic strategies. Indeed, both specific clinical prediction rules and possibly D-dimer cutoffs adapted to pregnant women could help to further reduce the proportion of patients needing thoracic imaging. As an imaging test will still ultimately be necessary in a significant proportion of women, further technical advances in CT scans protocols could reduce the radiation dose to both the fetus and the mother, an important step to reassure clinicians. Finally, educational efforts should be encouraged in the future to pass the challenge of implementing these validated diagnostic strategies in everyday clinical practice.
Introduction
Pregnancy represents a period at risk of venous thromboembolism (VTE) in women of child bearing age who are otherwise at low risk of developing VTE. The overall incidence of VTE is estimated at 1/1'000 pregnancies, and in western countries, pulmonary embolism (PE) remains a leading cause of maternal mortality (1, 2). The risk is highest during the third trimester and the 6 to 12 weeks following delivery (3).
Clinical Suspicion of PE During Pregnancy
PE diagnosis during pregnancy remains a true challenge for physicians, as many of the symptoms and signs frequently reported during physiological pregnancy–such as shortness of breath or tachypnea–may also suggest the diagnosis of PE (4). This is also true for symptoms and signs suggestive of the presence of a deep vein thrombosis (DVT). Indeed, lower limb pain and/or edema is often reported by pregnant women, especially during the second half of pregnancy (5). It is therefore particularly difficult to set a threshold between what can be considered physiological and what should raise the suspicion of VTE and lead to further investigations.
Prevalence of Confirmed PE Among Pregnant Women With Suspected PE
Although VTE risk is increased 7 to 10-fold during pregnancy compared to age-matched controls, the absolute incidence remains low (around 1/1'000) (6). Nevertheless, the fear of missing a PE during pregnancy leads to a low threshold to suspect the disease. This results in a very low prevalence of confirmed events among suspected patients even in the setting of clinical trials. Compared to the PE prevalence observed in diagnostic trials outside pregnancy (10–20% depending on geographic location) (7, 8), the reported PE prevalence in pregnant women is much lower at around 2–7% (4, 9, 10). In other words, the vast majority of pregnant women in whom PE is suspected do not have PE. Therefore, the main focus of diagnostic strategies is–even more than outside pregnancy–to rule out the diagnosis. This is an important information to bear in mind when considering the use of radiating imaging tests, and highlights the necessity of finding alternative strategies to minimize the proportion of pregnant women who need chest imaging.
Diagnostic Approach to Pregnant Women With Suspected Pulmonary Embolism
Historically, all pregnant women with suspected PE underwent a thoracic imaging test. In the 1990's, ventilation-perfusion scintigraphy (V/Q scan) was assessed in the PIOPED trial in the general population of patients with suspected PE (11), and perfusion only scans were rapidly adopted in clinical practice in pregnant women, albeit without previous scientific validation. Interestingly, in a study assessing the appropriateness of diagnostic management of patients with suspected PE, pregnancy was by far the strongest predictor of inappropriate management: 69% of pregnant women with suspected PE were indeed not appropriately managed (12). The lack of solid prospective data specific to this patient population is highly likely to have contributed to this observation published in 2006 (12).
Since then, two prospective management outcome studies have assessed two different strategies, and were published in 2018 (9) and 2019 (10). These two studies represent the first prospective scientific validation of PE diagnostic strategies during pregnancy and will be described in detail below.
Is There Any Clinical Pre-test Probability Assessment Tool I Could Use During Pregnancy?
In patients with suspected PE, the assessment of clinical pre-test probability (PTP) is the first step of all current diagnostic management strategies and is strongly encouraged in international guidelines (13, 14). It allows identifying a subgroup of patients with a low prevalence of the disease in whom a negative D-dimer safely rules out PE without imaging. It is also sometimes used for the final diagnostic interpretation of V/Q scan results.
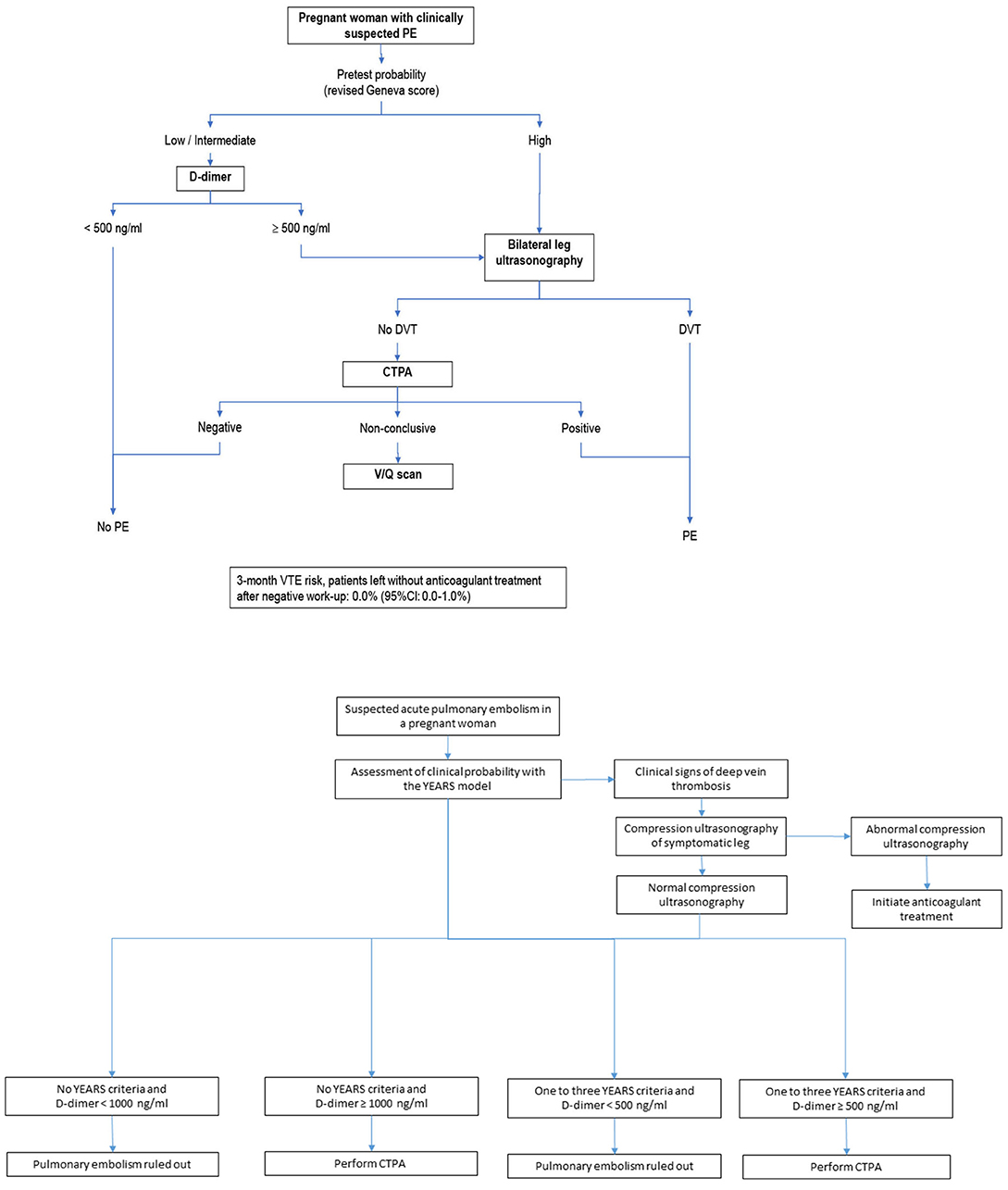
Available clinical decision rules (CDRs) have not been derived or validated in pregnant women (15). This has been one of the reasons brought by some physicians for not using D-dimer in this setting. The CT-PE pregnancy and ARTEMIS studies assessed diagnostic strategies in the specific setting of pregnant women with suspected PE (9, 10). These studies used two different PTP assessment tools–the Geneva score and a pregnancy-adapted YEARS model- that had not been previously derived nor validated in a pregnant population. Nevertheless, these two CDRs both proved efficient and accurate in integrated diagnostic algorithms (see Figure 1) (9, 10).
Further steps were taken in the validation process of pregnancy-adapted CDRs with the external validation of the YEARS model in the CT-PE pregnancy population, confirming the safety of this model in a second cohort of patients (16). Moreover, a novel PTP assessment tool-the Pregnancy-Adapted Geneva Score (PAG score)–was recently developed. The PAG score contains only objective items that are all relevant to pregnant women (see Table 1) (17). It allows classifying pregnant women with suspected PE in three categories of PTP that correspond to increasing prevalence of the disease (see Table 1). However, before advocating its large scale use in clinical practice, the PAG score needs to be prospectively validated.
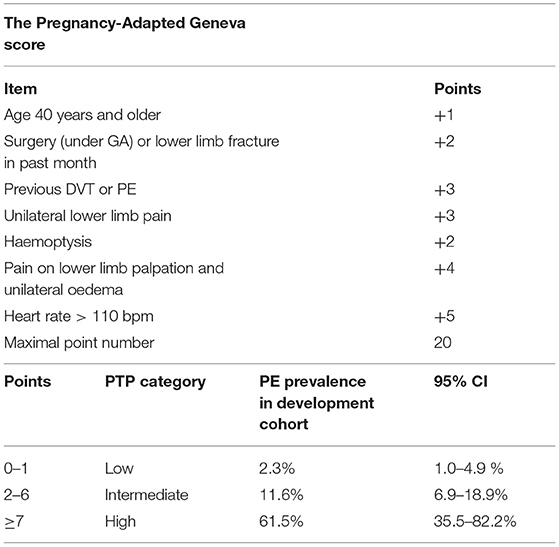
Table 1. The Pregnancy-Adapted Geneva score for assessment of pre-test clinical probability of PE in pregnant women (17).
Should I Use D-Dimer to Exclude PE During Pregnancy?
In clinical practice, D-dimer testing tends to be more often skipped in pregnant women than in the general population because of the knowledge of gradually increasing D-dimer levels during pregnancy. Physicians therefore tend to consider D-dimer as “useless” in this setting. Another reason which likely contributes to a reluctance to use D-dimer during pregnancy is, as said above, the lack of clinical PTP assessment scores specifically developed and validated in pregnant women. Finally, the safety of excluding PE by a negative D-dimer during pregnancy has been challenged by some authors (18).
Nevertheless, the safety of a negative D-dimer associated with a non-high/unlikely PTP to exclude PE without imaging is widely accepted outside pregnancy (7, 8, 19). There is no biological rationale which could support the hypothesis of a lower sensitivity of D-dimer during pregnancy. The CT-PE pregnancy and ARTEMIS studies have both confirmed the safety of excluding PE during pregnancy by a negative D-dimer test in stepwise diagnostic algorithms (see Figure 1). The number of patients remains limited in these studies and needs to be extended and enriched by data from future prospective trials. Nonetheless, a recent meta-analysis reported a high negative predictive value of D-dimer to exclude PE during pregnancy. The pooled estimate values were indeed 99.5% for sensitivity (95% CI 95.0–100.0%) and 100% for negative predictive value (95% CI 99.19–100.0%) (20).
While awaiting additional data, the clinician should bear in mind that the percentage of pregnant women in whom PE diagnosis can be safely excluded by a non-high PTP and negative D-dimer without any additional tests (CUS or thoracic imaging) was of 12% in the CT-PE-pregnancy study, which corresponds to a number of patients needed to test to exclude one PE of 8.3 (9). In a setting where minimizing radiating tests is a central concern, this efficiency is not negligible. Avoiding radiation exposure by a simple blood test in 1 out of 8 pregnant women with suspected PE is already highly appealing. Of note, although the risk of developing PE is highest during the post-partum and the third trimester, the chances of obtaining a negative D-dimer test decreases with advancing pregnancy. In the CT-PE pregnancy study, the proportion of negative D-dimer results was 25% during the first trimester, 11% during the second trimester, and 4% during the third trimester.
The ARTEMIS study also showed a high efficiency of the diagnostic algorithm to avoid thoracic imaging (39%). However, the non-invasive strategy tested in this study was not solely based on PTP and D-dimer but included the pre-exclusion of DVT by lower limb CUS in patients with lower limb symptoms, and so represented a more complex selection of “low-risk” women in whom a higher D-dimer cutoff was used to exclude PE (see Figure 1) (10). When pooling all the available evidence to address this question, the recent meta-analysis mentioned above demonstrated an overall efficiency of 34% of D-dimer to safely exclude PE (95% CI 15.9–55.23%) (20). Giving the chance to a pregnant woman with suspected PE to avoid a radiating test should therefore not be neglected, and in spite of the controversies in international guidelines (21), we believe that the use of D-dimer in this setting should be strongly encouraged.
Should I Refer My Patient for Lower Limb Compression Ultrasound Before Chest Imaging?
The information required to answer this question is provided by the CT-PE pregnancy and the ARTEMIS studies. Bilateral lower limb compression ultrasound (CUS) was indeed part of the diagnostic strategies of both studies (see Figure 1). In the CT-PE pregnancy study, CUS was performed in 75% of the overall population, and proximal DVT was diagnosed in 2% of patients without leg symptoms and 9% of patients with leg symptoms (9). In the ARTEMIS study, CUS was performed in 88% of the overall population, and DVT was confirmed in 1% of patients without leg symptoms and 7% of patients with leg symptoms (10). CUS seems thus mainly useful in pregnant women with lower limb symptoms (lower limb pain and or edema). Nevertheless, focusing again on the need to maximize the number of avoidable radiating tests rather than on cost-effectiveness, the yield of 1–2% avoided radiating tests provided by screening pregnant women with CUS is considered worthwhile by some. Depending on the structure of medical care facilities, obtaining a CUS can however be more challenging that obtaining a CTPA and represents an obstacle to the implementation of a sequential testing strategy (15). Another potential limitation is the difficulty to assess iliac veins and diagnose isolated iliac DVT, which is however mainly a problem in pregnant women with suspected DVT with no concomitant PE suspicion. Interestingly, international guidelines currently recommend bilateral CUS in pregnant women with suspected PE in whom PE diagnosis could not be excluded by the combination of PTP and D-dimer, in whom further testing is needed, before pursuing to chest imaging (13).
What Chest Imaging Modality Should I Choose in Pregnant Women and Why?
In spite of all the efforts described above to minimize chest imaging, a significant proportion of pregnant women with suspected PE (around 2/3) will ultimately need thoracic imaging in their diagnostic management (20). Radiation exposure to the mother and to the fetus are both matters of concern (22). CTPA and V/Q scan are the two chest imaging modalities studied on a large scale basis outside pregnancy. Due to its high diagnostic accuracy and accessibility, CTPA has become the new “gold standard” for the diagnosis of PE and is the most widely used test in clinical practice (23). Another advantage of CTPA is the possibility to identify an alternative diagnosis such as aortic dissection, pneumonia, pneumothorax, which can be missed by V/Q scan.
This has even led to major concerns about over-testing and over-diagnosis, which are beyond the scope of the present paper. In pregnant women, radiation exposure and the rate of non-diagnostic tests remain the two central matters of concern.
A recent meta-analysis comparing all the available data on these two imaging techniques in pregnant women could not conclude on the relative risk of radiation of CTPA vs. V/Q scan due to lack of homogeneity in the calculation methods and the scan protocols used (22). The important message conveyed by this work is however that all reported radiation measurements for both tests were clearly below the commonly accepted harmful threshold of 100 mGy, in spite of the inclusion of older studies preceding the implementation of adapted imaging protocols in pregnant women (22). Moreover, as previously stated by scientific societies and experts, the risks associated with either test is by far lower than the potential risks of inappropriate diagnostic management leading to a missed diagnosis (with the risk of death) or to an unjustified anticoagulant treatment based on a “clinical” diagnosis (with the risk of bleeding and the long term consequences on delivery and subsequent pregnancies of a unduly confirmed PE) (24, 25). Regarding the proportion of inconclusive tests, the pooled rates of non-diagnostic results were similar between CTPA (14%) and V/Q scan (12%), but the range of reported rates was very broad (0–57% for CTPA and 1–40% for V/Q scan) across the included studies (22).
The technical evolution of CTPA has considerably decreased radiation exposure, and pregnancy-adapted CTPA protocols include a reduced anatomical coverage of the scan and reduced kilovoltage. These specific protocols also include a high-concentration, high-volume and high-rate of injection of contrast media followed by saline flush as well as shallow inspiration breath-hold to avoid a Valsalva manoeuver, in order to optimize arterial opacification and avoid non-diagnostic tests (26). The technical evolution of nuclear medicine imaging modalities, including tomographic lung scintigraphy (SPECT) may also be promising, albeit not yet supported by prospective management outcome data. A prospective study comparing SPECT to CTPA and V/Q scan in non-pregnant patients is currently ongoing (NCT02983760), and SPECT may possibly be a promising technique in the future for pregnant women.
In spite of the optimization of CTPA protocols for pregnant women, the historical belief of significantly higher radiation doses to the mother's breast tissue of CTPA compared to V/Q scan still influences some physicians in their choice toward scintigraphy. Because of a very low likelihood of pulmonary comorbidity in this population, a two-step protocol is used in some centers: a perfusion scan is performed; PE is excluded in case of a normal perfusion scan. Ventilation sequences are only performed in case of an abnormal perfusion pattern to seek for a mismatch suggestive of PE. It should be noted that such a stepwise strategy has however not been validated in prospective trials. Caution is required in particular in the positive diagnosis of PE based on a perfusion scan alone, without having objectively confirmed that the perfusion abnormality is not associated with any parenchymal/ventilation abnormality.
The 2018 American Society of Hematology (ASH) guidelines for the diagnosis of VTE are highly driven by the willingness to avoid radiation even in the general population, and thus advocate for V/Q scan for patients likely to have a diagnostic scan and in centers where V/Q scans are available with expertise to interpret the results in a timely manner (14). The latest European Society of Cardiology (ESC) 2019 Guidelines provide specific recommendations for pregnant women. In terms of imaging test, their recommendation states “perfusion scintigraphy or CTPA with a low-radiation dose protocol” with a Class IIa, level C recommendation (13).
Current Diagnostic Algorithms
As said before, to date, only two prospective management outcome studies have been published in pregnant women with suspected PE, reflecting the challenges of leading clinical trials in this setting.
CT-PE Pregnancy Algorithm
The CT-PE pregnancy study published in 2018 (9) included 395 women with suspected PE and applied a diagnostic algorithm based on the sequential assessment of clinical PTP, D-dimer with the standard 500 ng/mL cutoff, lower limb venous CUS regardless of the presence of leg symptoms or signs, and CTPA as the first-line chest imaging technique (see Figure 1). PE prevalence was 7%, the failure rate of the strategy was 0.0% (95% CI 0.0–1.0%) and the percentage of patients managed without thoracic imaging 12%.
ARTEMIS Algorithm
The ARTEMIS study published in 2019 (10) included 498 women with suspected PE and applied an adapted YEARS model (see Figure 1). PE prevalence was 4%, the failure rate of the strategy was 0.21% (95% CI 0.04–1.2%) and the percentage of patients managed without thoracic imaging 39%.
The detailed description of the respective strengths and limitations of these studies have been described elsewhere and are beyond the scope of this paper (15). The important message here is that such prospective outcome studies are gradually filling the knowledge gap in the optimal diagnostic management of pregnant women with suspected PE, and will certainly contribute to increase the appropriateness of these patient's management in the future.
Remaining Controversies
Despite the recently published prospective data and evidence, controversies regarding the optimal diagnostic strategy for PE in pregnant women are still alive and the topic remains highly debated. As an example, the CT-PE pregnancy and ARTEMIS models have been challenged in an analysis performed on a UK cohort of 219 patients (DiPEP study) which includes pregnant women having PE diagnosed primarily by imaging. The authors concluded that both strategies were not safe (18). However, the original DiPEP study this retrospective analysis was performed on, suffered from many limitations. In particular, the DiPEP cohort was not a purely prospective cohort, different D-dimer tests with variable cutoffs were used, and there was no standardized diagnostic algorithm (27). The reported inferences from the recent analysis performed on this partly retrospective cohort are probably not as robust as the prospective management outcome trials, and the message advocating against D-dimer use based on this data should therefore be interpreted with caution.
Regarding the imaging test of choice, the major concern surrounding the use of any diagnostic test is the risk of maternal and fetal radiation exposure. While fetal exposure seems to be in the same range with both tests, CTPA is more radiating for the mother's breasts. Although no increased risk of early-onset breast cancer was observed in a large population cohort study with a median follow-up of almost 6 years after CTPA and of 7.3 years after V/Q scan, these findings might be considered as insufficiently reassuring, due to the limited length of follow-up (28). Also, the cumulative effect of repeated chest imaging is not well known. Importantly, the previously reported 12% rate of inconclusive CTPAs was not confirmed in the CT-PE pregnancy and in the ARTEMIS studies (reported rates of 7 and 0%, respectively) (9, 15), so that repeat chest imaging during the same diagnostic workup remains exceptional.
Despite these limitations, the risks associated with radiation exposure of both CTPA and V/Q scan are lower than the risk of missing a PE or of exposing unduly a pregnant woman to an anticoagulant treatment. As emergency access to V/Q scan is becoming difficult even in University Hospitals, CTPA will likely become the most used diagnostic test for most pregnant women with suspected PE who could not have the diagnosis excluded by PTP and D-dimer. Noteworthy, the radiation dose to the maternal breast with modern CTPA techniques is steadily decreasing and will probably reassure prescribing physicians in the near future. Ongoing prospective studies on this topic include the OPTICA study (NCT 04179487) whose aim is to assess the usefulness and safety of a low-dose CTPA protocol in pregnant patients with suspected PE (29).
In conclusion, despite the important recent advances in the field, there is room for further refinements and improvements of diagnostic strategies for suspected PE in pregnant women. Educational efforts should be strongly encouraged to pass the challenge of implementing validated diagnostic strategies in everyday clinical practice.
Author Contributions
HR-E drafted the paper. GL and MR revised it critically for important intellectual content. All authors provided final approval of the version to be published.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor, BT, declared a past collaboration with one of the author GL.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Cantwell R, Clutton-Brock T, Cooper G, Dawson A, Drife J, Garrod D, et al. Saving mothers' lives: reviewing maternal deaths to make motherhood safer: 2006-2008. the eighth report of the confidential enquiries into maternal deaths in the United Kingdom. BJOG. (2011) 118:1–203. doi: 10.1111/j.1471-0528.2010.02847.x
2. Heit JA, Kobbervig CE, James AH, Petterson TM, Bailey KR, Melton LJ. Trends in the incidence of venous thromboembolism during pregnancy or postpartum: a 30-year population-based study. Ann Intern Med. (2005) 143:697–706. doi: 10.7326/0003-4819-143-10-200511150-00006
3. Kamel H, Navi BB, Sriram N, Hovsepian DA, Devereux RB, Elkind MS. Risk of a thrombotic event after the 6-week postpartum period. N Engl J Med. (2014) 370:1307–15. doi: 10.1056/NEJMoa1311485
4. Chan WS, Ray JG, Murray S, Coady GE, Coates G, Ginsberg JS. Suspected pulmonary embolism in pregnancy: clinical presentation, results of lung scanning, and subsequent maternal and pediatric outcomes. Arch Intern Med. (2002) 162:1170–5. doi: 10.1001/archinte.162.10.1170
5. Chan WS, Lee A, Spencer FA, Crowther M, Rodger M, Ramsay T, et al. Predicting deep venous thrombosis in pregnancy: out in “LEFt” field? Ann Intern Med. (2009) 151:85–92. doi: 10.7326/0003-4819-151-2-200907210-00004
6. Bourjeily G, Paidas M, Khalil H, Rosene-Montella K, Rodger M. Pulmonary embolism in pregnancy. Lancet. (2010) 375:500–12. doi: 10.1016/S0140-6736(09)60996-X
7. Righini M, Van Es J, Den Exter PL, Roy PM, Verschuren F, Ghuysen A, et al. Age-adjusted D-dimer cutoff levels to rule out pulmonary embolism: the ADJUST-PE study. JAMA. (2014) 311:1117–24. doi: 10.1001/jama.2014.2135
8. van der Hulle T, Cheung WY, Kooij S, Beenen LFM, van Bemmel T, van Es J, et al. Simplified diagnostic management of suspected pulmonary embolism (the YEARS study): a prospective, multicentre, cohort study. Lancet. (2017) 390:289–97. doi: 10.1016/S0140-6736(17)30885-1
9. Righini M, Robert-Ebadi H, Elias A, Sanchez O, Le Moigne E, Schmidt J, et al. Diagnosis of pulmonary embolism during pregnancy: a multicenter prospective management outcome study. Ann Intern Med. (2018) 169:766–73. doi: 10.7326/M18-1670
10. van der Pol LM, Tromeur C, Bistervels IM, Ni Ainle F, van Bemmel T, Bertoletti L, et al. Pregnancy-adapted YEARS algorithm for diagnosis of suspected pulmonary embolism. N Engl J Med. (2019) 380:1139–49. doi: 10.1056/NEJMoa1813865
11. Investigators P. Value of the ventilation/perfusion scan in acute pulmonary embolism. results of the prospective investigation of pulmonary embolism diagnosis (PIOPED). JAMA. (1990) 263:2753–9. doi: 10.1001/jama.263.20.2753
12. Roy PM, Meyer G, Vielle B, Le Gall C, Verschuren F, Carpentier F, et al. Appropriateness of diagnostic management and outcomes of suspected pulmonary embolism. Ann Intern Med. (2006) 144:157–64. doi: 10.7326/0003-4819-144-3-200602070-00003
13. Konstantinides SV, Meyer G, Becattini C, Bueno H, Geersing GJ, Harjola VP, et al. 2019 ESC guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European respiratory society (ERS). Eur Heart J. (2020) 41:543–603. doi: 10.1093/eurheartj/ehz405
14. Lim W, Le Gal G, Bates SM, Righini M, Haramati LB, Lang E, et al. American society of hematology 2018 guidelines for management of venous thromboembolism: diagnosis of venous thromboembolism. Blood Adv. (2018) 2:3226–56. doi: 10.1182/bloodadvances.2018024828
15. Chan WS. Can pregnancy-adapted algorithms avoid diagnostic imaging for pulmonary embolism? Hematology Am Soc Hematol Educ Program. (2020) 2020:184–9. doi: 10.1182/hematology.2020000105
16. Langlois E, Cusson-Dufour C, Moumneh T, Elias A, Meyer G, Lacut K, et al. Could the YEARS algorithm be used to exclude pulmonary embolism during pregnancy? data from the CT-PE-pregnancy study. J Thromb Haemost. (2019) 17:1329–34. doi: 10.1111/jth.14483
17. Robert-Ebadi H, Elias A, Sanchez O, Le Moigne E, Schmidt J, Le Gall C, et al. Assessing the clinical probability of pulmonary embolism during pregnancy: The pregnancy-adapted geneva (PAG) score. J Thromb Haemost. (2021) 19:3044-3044. doi: 10.1111/jth.15521
18. Goodacre S, Horspool K, Nelson-Piercy C, Knight M, Shephard N, Lecky F, et al. The DiPEP study: an observational study of the diagnostic accuracy of clinical assessment, D-dimer and chest x-ray for suspected pulmonary embolism in pregnancy and postpartum. BJOG Int J Obstet Gynaecol. (2019) 126:383–92. doi: 10.1111/1471-0528.15286
19. Robert-Ebadi H, Robin P, Hugli O, Verschuren F, Trinh-Duc A, Roy PM, et al. Impact of the age-adjusted d-dimer cutoff to exclude pulmonary embolism: a multinational prospective real-life study (the RELAX-PE Study). Circulation. (2021) 143:1828–30. doi: 10.1161/CIRCULATIONAHA.120.052780
20. Bellesini M, Robert-Ebadi H, Combescure C, Dedionigi C, Le Gal G, Righini M. D-dimer to rule out venous thromboembolism during pregnancy: a systematic review and meta-analysis. J Thromb Haemost. (2021) 19:2454–67. doi: 10.1111/jth.15432
21. Wan T, Skeith L, Karovitch A, Rodger M, Le Gal G. Guidance for the diagnosis of pulmonary embolism during pregnancy: consensus and controversies. Thromb Res. (2017) 157:23–8. doi: 10.1016/j.thromres.2017.06.025
22. Tromeur C, van der Pol LM, Le Roux PY, Ende-Verhaar Y, Salaun PY, Leroyer C, et al. Computed tomography pulmonary angiography versus ventilation-perfusion lung scanning for diagnosing pulmonary embolism during pregnancy: a systematic review and meta-analysis. Haematologica. (2019) 104:176–88. doi: 10.3324/haematol.2018.196121
23. Robert-Ebadi H, Le Gal G, Righini M. Evolving imaging techniques in diagnostic strategies of pulmonary embolism. Expert Rev Cardiovasc Ther. (2016) 14:495–503. doi: 10.1586/14779072.2016.1134316
24. McLintock C, Brighton T, Chunilal S, Dekker G, McDonnell N, McRae S, et al. Recommendations for the diagnosis and treatment of deep venous thrombosis and pulmonary embolism in pregnancy and the postpartum period. Aust N Z J Obstet Gynaecol. (2012) 52:14–22. doi: 10.1111/j.1479-828X.2011.01361.x
25. Leung AN, Bull TM, Jaeschke R, Lockwood CJ, Boiselle PM, Hurwitz LM, et al. American thoracic society documents: an official American thoracic society/society of thoracic radiology clinical practice guideline–evaluation of suspected pulmonary embolism in pregnancy. Radiology. (2012) 262:635–46. doi: 10.1148/radiol.11114045
26. Ridge CA, Mhuircheartaigh JN, Dodd JD, Skehan SJ. Pulmonary CT angiography protocol adapted to the hemodynamic effects of pregnancy. AJR Am J Roentgenol. (2011) 197:1058–63. doi: 10.2214/AJR.10.5385
27. Hunt BJ, Parmar K, Horspool K, Shephard N, Nelson-Piercy C, Goodacre S, et al. The DiPEP (diagnosis of PE in pregnancy) biomarker study: an observational cohort study augmented with additional cases to determine the diagnostic utility of biomarkers for suspected venous thromboembolism during pregnancy and puerperium. Br J Haematol. (2018) 180:694–704. doi: 10.1111/bjh.15102
28. Burton KR, Park AL, Fralick M, Ray JG. Risk of early-onset breast cancer among women exposed to thoracic computed tomography in pregnancy or early postpartum. J Thromb Haemost. (2018) 16:876–85. doi: 10.1111/jth.13980
29. Gillespie C, Foley S, Rowan M, Ewins K, NiAinle F, MacMahon P. The OPTICA study (optimised computed tomography pulmonary angiography in pregnancy quality and safety study): rationale and design of a prospective trial assessing the quality and safety of an optimised CTPA protocol in pregnancy. Thromb Res. (2019) 177:172–9. doi: 10.1016/j.thromres.2019.03.007
Keywords: pulmonary embolism, diagnostic strategy, D-dimer, clinical probability, pregnancy, computed tomography pulmonary angiography, ventilation-perfusion lung scan
Citation: Robert-Ebadi H, Le Gal G and Righini M (2022) Diagnostic Management of Pregnant Women With Suspected Pulmonary Embolism. Front. Cardiovasc. Med. 9:851985. doi: 10.3389/fcvm.2022.851985
Received: 10 January 2022; Accepted: 10 February 2022;
Published: 16 March 2022.
Edited by:
Bernard Tardy, INSERM CIC1408, FranceReviewed by:
Eli Westerlund, Karolinska Institutet, SwedenNina Olausson, Danderyd University Hospital, Sweden
Copyright © 2022 Robert-Ebadi, Le Gal and Righini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Helia Robert-Ebadi, aGVsaWEucm9iZXJ0LWViYWRpQGhjdWdlLmNo