 Jialu Wang
Jialu Wang Shidong Liu2†
Shidong Liu2† Yang Chen
Yang Chen
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Cardiovasc. Med. , 08 April 2022
Sec. Heart Valve Disease
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.842929
Background: Left bundle branch block (LBBB) is a common complication of the transcatheter aortic valve replacement (TAVR), and its impact on prognosis is controversial.
Methods: A comprehensive electronic search was conducted in databases (PubMed, Embase, Cochrane Library, and The Web of Science), from the date of database establishment till March 2021, to screen for studies on new-onset LBBB after TAVR. We next performed a meta-analysis to evaluate the effect of new-onset LBBB after TAVR on patient prognosis, based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.
Results: A total of 17 studies, including 9205 patients, were eligible for our analysis. Patients with new-onset LBBB had elevated all-cause mortality risk verses patients without new-onset LBBB, during all follow ups. The relevant data are as follows: 30-day (RR:1.71; 95%CI:1.27–2.29; P < 0.001), 1-year (RR:1.31; 95%CI:1.12–1.52; P < 0.001), and 2-year (RR:1.31; 95%CI:1.09–1.56; P = 0.003) follow ups. Likewise, new-onset LBBB patients also experienced increased cardiovascular mortality, compared to non-new-onset LBBB patients, but only in the 1-year follow up (RR:1.49; 95%CI:1.23–1.82; P < 0.001). Hospitalization for heart failure was dramatically elevated in patients with new-onset LBBB verses non-new-onset LBBB, in all follow ups. The relevant data are as follows: 30-day (RR:1.56; 95%CI:1.13–2.12; P = 0.007), 1-year (RR:1.35; 95%CI:1.08–1.68; P = 0.007), and 2-year (RR:1.49; 95%CI:1.21–1.84; P < 0.001). Similarly, new-onset LBBB patients had higher PPI risk than non-new-onset LBBB patients, in all follow ups. The relevant data are as follows: 30-day (RR:3.05; 95%CI:1.49–6.22; P = 0.002), 1-year (RR:2.15; 95%CI:1.52–3.03; P < 0.001), and 2-year (RR:2.52; 95%CI:1.68–3.78; P < 0.001).
Conclusion: Patients with new-onset LBBB have worse prognosis after TAVR than those without new-onset LBBB. Recognition of the adverse effects of post-TAVR new-onset LBBB can lead to the development of new strategies that enhance clinical outcomes.
Systematic Trial Registration: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=197224, identifier: 19722.
With increase in life expectancy and a growing aged population, aortic stenosis (AS) has become one of the most common valvular heart diseases as of today (1). In fact, the current prevalence of severe AS, among people >75 years of age, is 3.4% (2). When symptomatic, the 2-year mortality rate is observed in approximately 50% of severe AS cases (3). Because AS involves a mechanical obstruction, drug treatments are often ineffective, and valve replacement remains the only solution that can improve clinical symptoms and prolong life (4). Since its introduction in 2002, transcatheter aortic valve replacement (TAVR) has gradually emerged as an alternative to in the higher-risk population surgical aortic valve replacement (SAVR) procedure for patients with severe AS (5–7).
Fortunately, the development of valve implantation technology, the wide application of surgery, the accumulation of experience of the operators, and the emergence of new valve prosthesis have greatly reduced the incidence of serious complications (8). However, conduction disturbance after TAVR remains a highly common complication, mainly involving the new-onset left bundle branch block (LBBB) and the high-grade atrioventricular block (AVB), thereby requiring permanent pacemaker implantation (PPI), with a 4–30% incidence of the balloon-expandable valve and an 18–65% incidence of self-expanding valve (9). LBBB can lead to electromechanical asynchrony of the left ventricular activation, leading to ventricular pathological remodeling and left ventricular dysfunction. These pathological alterations can contribute to an elevated heart failure risk and poor prognosis (10, 11).
Till date, the prognostic effect of the new-onset LBBB after TAVR remains controversial. Conclusions from prior meta-analysis results were contradictory, and the studies were only conducted over 1 year of follow-up (12, 13). This may obscure the true long-term effect of new-onset LBBB. High quality meta-analysis is increasingly regarded as one of the key tools of obtaining evidence for clinical efficacy (14). Our aim, therefore, was to undertake a comprehensive and systematic overview of the clinical outcomes of patients, with and without new-onset LBBB following TAVR, during the 30-day, 1, and 2-year follow ups.
This study was conducted, according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. The complete study protocol is registered in the PROSPERO international database (CRD42020197224) (15, 16). Additionally, the methodological quality was assessed with A Measurement Tool to Assess Systematic Reviews (17, 18).
The PubMed, Cochrane Library, Web of Science, and EMBASE databases were systematically searched from the establishment of the databases till the end of March 2021, using keywords “transcatheter aortic valve implantation,” “transcatheter aortic valve replacement,” “TAVI,” “TAVR,” “bundle-branch block,” “heart bundle branch block,” and “LBBB.” To ensure no relevant publications were overlooked, we also manually searched for qualifying publications in the reference lists of eligible articles.
The authors screened the titles and study abstracts, based on the inclusion/exclusion criteria. Publications encompassing the following criteria were included in this meta-analysis: (1) AS patients who received TAVR; (2) contained new-onset LBBB incidence report; (3) examined the clinical outcomes of interest in a ≥ 1-year follow up study; and (4) consisted of non-new-onset LBBB controls. Among the publications excluded from the meta-analysis were conference reports, reviews, case reports, summaries, editorials, and studies published in a language other than English.
Based on the PRISMA statement, two authors extracted patient data, including first author, region, year, study type, number of patients, inclusion and exclusion criteria, gender, age, past history, echocardiography data, NYHA grade, logistic EuroSCORE, STS-PROM, valve type, access site, follow-up time, all-cause mortality, cardiovascular mortality, hospitalization for heart failure and PPI, and studied the data using standardized data extraction tables. To ensure accuracy, the data was further verified by a third author.
The Newcastle Ottawa scale was employed for the assessment of eligible publication, and it primarily focused on the selection of study group, comparability between groups, and determination of exposure. We assigned a score of 0–9 for each study, following the evaluation. Higher scores represented higher study quality.
The primary outcome of this study was all-cause mortality during the 30-day, 1, and 2-year follow ups after TAVR. Secondary outcomes examined were cardiovascular mortality, hospitalization rate for heart failure, and PPI during the 30-day, 1, and 2-year follow ups post TAVR.
Continuous variables are represented by standardized mean and standard deviation, and categorical variables are expressed by percentages. We employed the random-effects model to compute risk ratio (RR) and 95% confidence interval (CI). We also used Cochran's Q statistic and I2 to test the heterogeneity across studies. When P < 0.10 or I2 ≥ 50%, the heterogeneity of the study was considered significant. The publication bias was visually evaluated using a funnel plot, and Egger's test was used to quantify publication bias. The robustness of the results and the effect of potential effect modifiers were examined with sensitivity analysis. All P-values were two-sided and P < 0.05 was considered statistically significant. Stata15.0 statistical analysis software was used for data analysis.
As illustrated in Figure 1, a total of 1,888 articles were selected in the preliminary search. In addition, 8 suitable articles were obtained from the reference lists of the above-mentioned publications. Upon elimination of duplicate studies, 1,195 publications were screened by title and abstract. Among them, 54 were read in full to evaluate inclusion in the meta-analysis, 38 were eliminated, due to the following reasons: 15 publications were without a control group, 21 did not have an outcome of interest, and 2 were non-English. Finally, 9,205 patients, in 17 publications (19–35), met the inclusion criteria for the final meta-analysis. Details of the updated eligible publications are reported in Table 1.
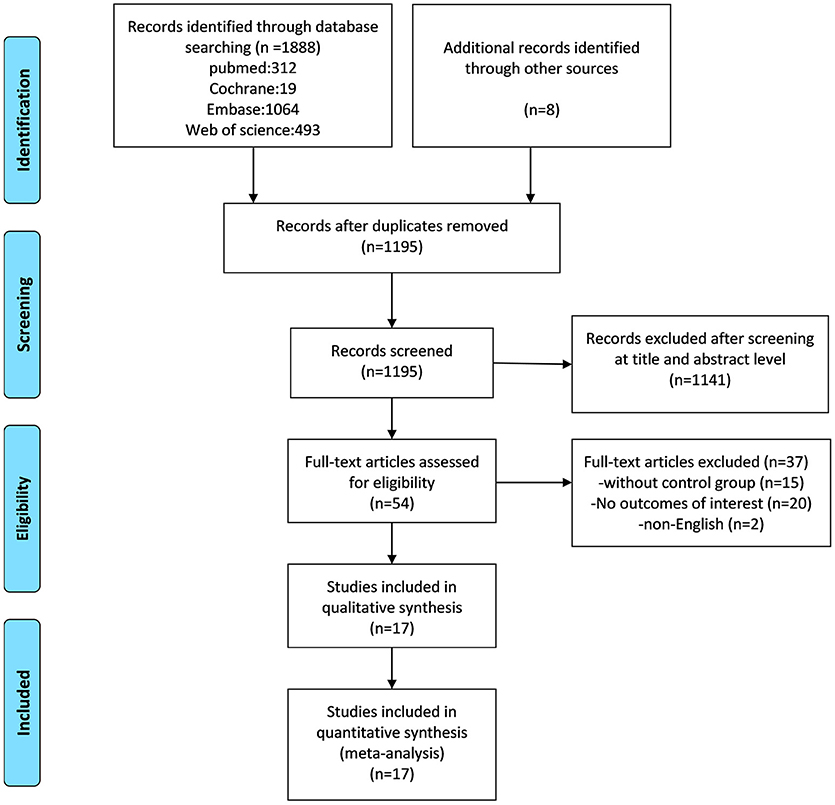
Figure 1. A flow diagram of the study selection process, based on the PRISMA statement.
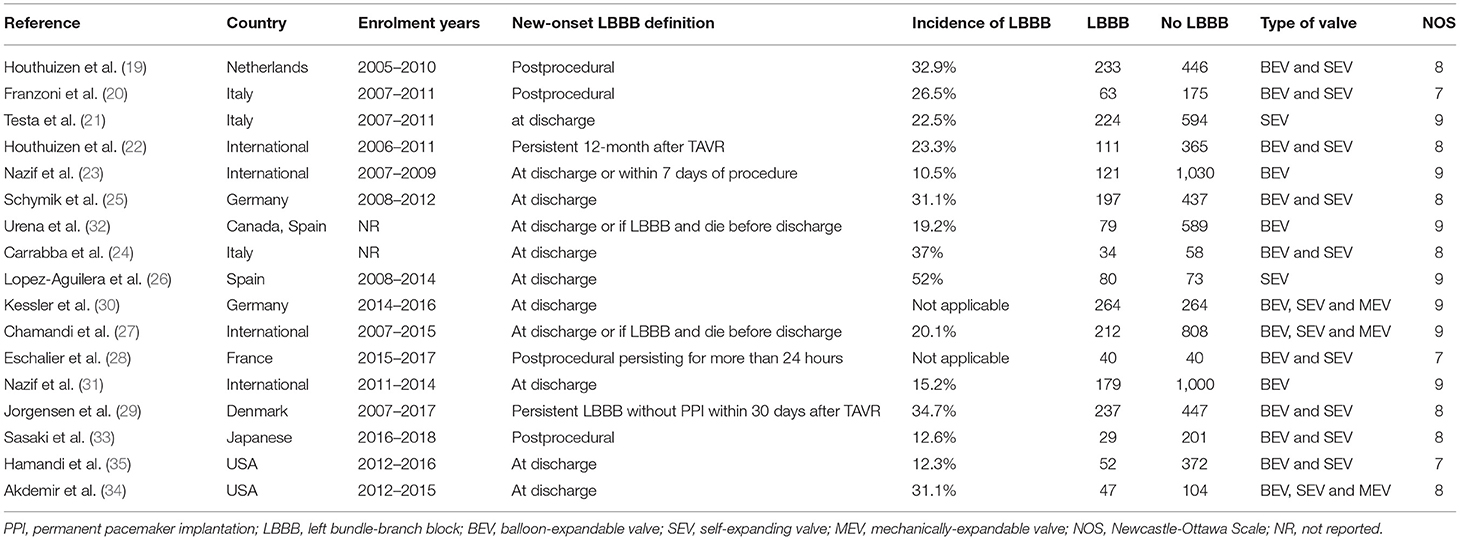
Table 1. Characteristics of included studies.
Table 2 summarizes the baseline and procedural characteristics of patients included in the selected publications. There were no significant differences in the STS score and logistic EuroSCORE between the two groups (Figure 2). Generally, the most commonly used vascular access is the TF-TAVR approach. Among all studies, three employed balloon-expandable valves, three others employed self-expanding valves, and the remaining employed multiple categories of valves.
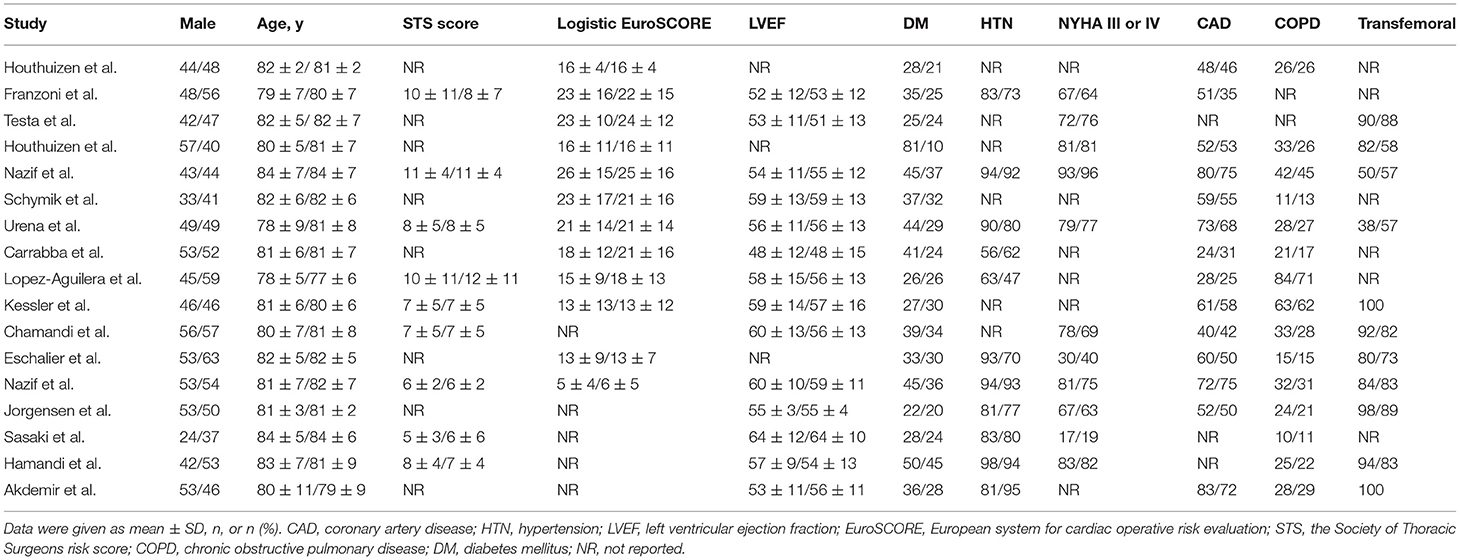
Table 2. Patient and procedural characteristics of included studies.

Figure 2. Forest plots illustrating the surgical risk score. (A) STS score; (B) Logistic EuroSCORE.
Based on the Newcastle Ottawa scale (Table 1), the quality of the selected publications was generally high. No evidence of publication bias was found, as evidenced by the funnel plot and Egger's test.
All-cause mortality was the primary outcome of our meta-analysis. At the 30-day follow up, 11 publications reported an association between new-onset LBBB and all-cause mortality. In particular, patients with new-onset LBBB after TAVR had a higher risk of all-cause mortality than those without new-onset LBBB (RR:1.71; 95%CI:1.27–2.29; P < 0.001; I2 = 21.3%). At the 1-year follow up, 17 publications reported all-cause mortality, and the patients with new-onset LBBB had a higher all-cause mortality (RR:1.31; 95%CI:1.12–1.52; P < 0.001; I2 = 33.7%) relative to those without. Finally, at the 2-year follow up, 6 publications reported all-cause mortality, with an increased risk of all-cause mortality among the new-onset LBBB patients vs. non-new-onset LBBB patients after TAVR (RR:1.31; 95%CI:1.09–1.56; P < 0.001; I2 = 28.7%) (Figure 3). No significant heterogeneity was observed among the publications. Additionally, sensitivity analysis, performed by one by one exclusion study, failed to alter the conclusion of our analysis.
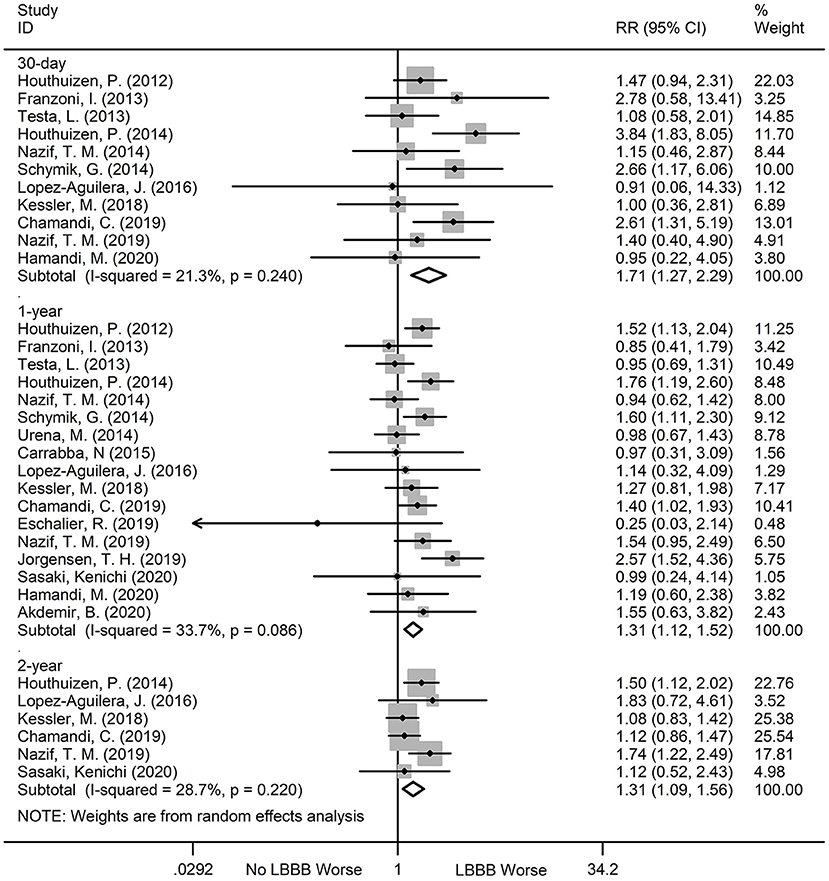
Figure 3. Forest plot comparing all-cause mortality risk between patients with and without new-onset LBBB after TAVR.
There was no statistically significant difference in the 30-day (RR:1.28; 95%CI:0.68–2.39; P = 0.445; I2 = 0%) and 2-year (RR:1.40; 95%CI:0.63–3.10; P = 0.404; I2 = 74.8%) cardiovascular mortality between patients with new-onset LBBB and those without. However, the new-onset LBBB was associated with significantly higher 1-year cardiovascular mortality (RR:1.49; 95%CI:1.23–1.82; P < 0.001; I2 = 0%), compared to the non-new-onset LBBB patients (Figure 4). We observed significant heterogeneity (I2 = 74.8%) at the 2-year follow-up. However, after excluding the studies one by one, the results of sensitivity analysis remained the same.
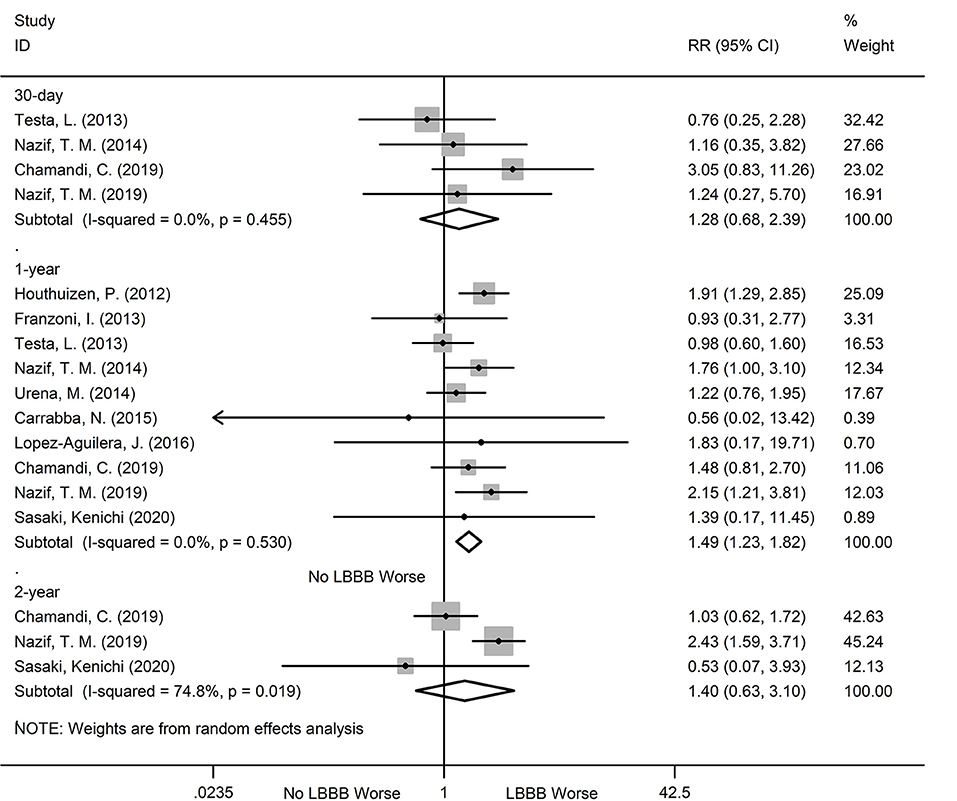
Figure 4. Forest plot comparing cardiovascular mortality risk between patients with and without new-onset LBBB after TAVR.
During the 30-day, 1, and 2-year follow ups, the new-onset LBBB patients after TAVR showed a dramatic increase in hospitalization risk for heart failure, relative to non- new-onset LBBB patients. The relevant data are as follows: 30-day (RR:1.56; 95%CI:1.13–2.15; P = 0.007; I2 = 0%), 1-year (RR:1.35; 95%CI:1.08–1.68; P = 0.007, I2 = 31.5%), 2-year (RR:1.49; 95%CI:1.21–1.84; P < 0.001; I2 = 0%) (Figure 5). Additionally, no obvious heterogeneity was observed, and there was no obvious change in sensitivity analysis.

Figure 5. Forest plot comparing hospitalization for heart failure risk between patients with andwithout new-onset LBBB after TAVR.
The new-onset LBBB patients after TAVR were also more likely to undergo PPI, during all follow ups, compared to the non-new-onset LBBB patients. The relevant data are as follows: 30-day (RR:3.05; 95%CI:1.49–6.22; P = 0.002; I2 = 81.7%), 1-year (RR:2.15;95%CI:1.52–3.03; P < 0.001; I2 = 70.2%), 2-year (RR:2.52; 95%CI:1.68–3.78; P < 0.001; I2 = 19.3%) (Figure 6). Significant heterogeneity was observed among the two groups (I2 = 81.7% and I2 = 70.2%), but the sensitivity analysis did not markedly alter the results.
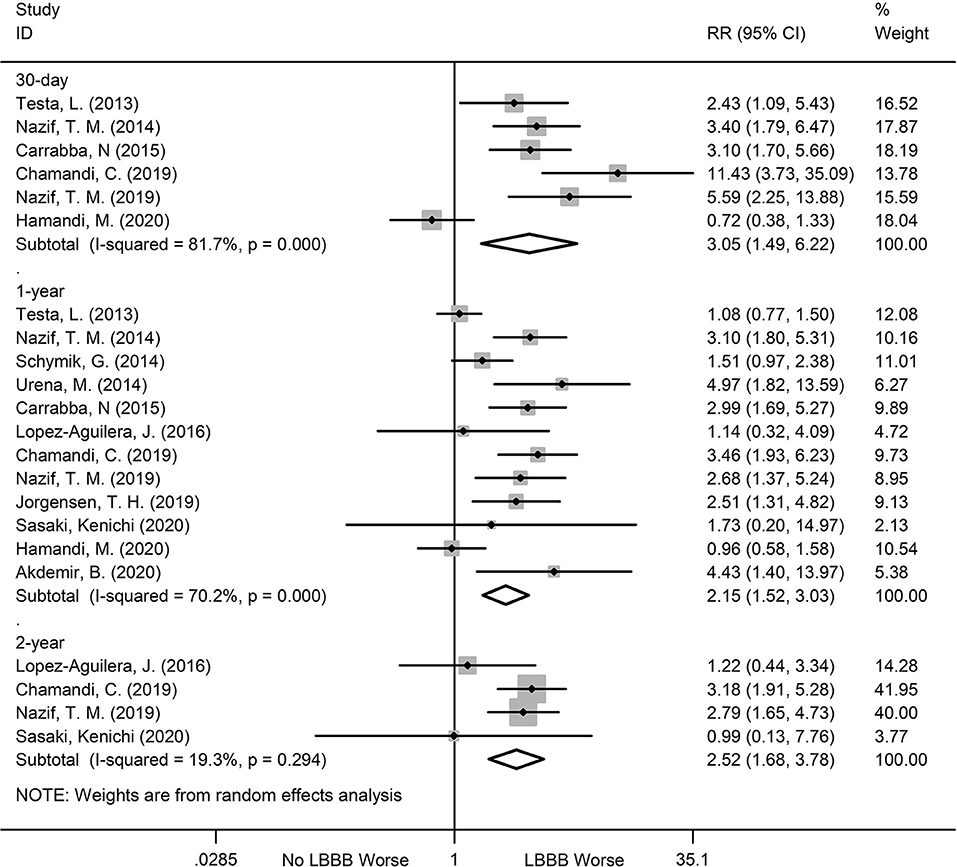
Figure 6. Forest plot comparing PPI risk between patients with and without new-onset LBBB after TAVR.
Till date, our meta-analysis and systematic review offers the greatest relationship between new-onset LBBB and patient prognosis, and is the first to conduct pooled analyses of long-term prognosis of new-onset LBBB after TAVR. Our analysis demonstrated 2 main findings: (1) patients with new-onset LBBB, but not without new-onset LBBB, experience an increased risk of all-cause mortality, hospitalization for heart failure, and PPI at the 30-day, 1 and 2-year follow ups post TAVR; and (2) patients with new-onset LBBB also have an increased risk of cardiovascular mortality 1 year after TAVR, as opposed to those without new-onset LBBB.
LBBB is generally considered to be a marker of poor prognosis (10, 36). Our analysis revealed that patients with new-onset LBBB had a higher risk of all-cause mortality than those without new-onset LBBB. The reason may be multifactorial. On one hand, the adverse prognosis may be related to the ventricular asynchrony, diastolic shortening, and ventricular septal motion abnormality, caused by LBBB itself. With the progression of time, this can lead to a reduction in LVEF, resulting in asymmetric dilation, hypertrophy of the heart, and ultimately heart failure (10). Additionally, LBBB may also increase the risk of life-threatening ventricular arrhythmias, severe bradyarrhythmias, and sudden death (33). Previous studies investigating the effects of new-onset LBBB after TAVR on patient prognosis provided inconsistent results. For example, the meta-analysis by Regueiro et al. (12). did not show an association between new-onset LBBB and all-cause mortality (RR:1.21; 95%CI:0.98–1.50). However, a strong positive association between new-onset LBBB and all-cause mortality risk was reported (RR:1.32; 95%CI:1.17–1.49) in another study (13). Similarly, several retrospective investigations reported that new-onset LBBB after TAVR has no effect on long-term mortality (26, 27, 30), while other studies suggested that LBBB is a marker of enhanced long-term mortality after TAVR (22, 31). This obvious discrepancy in conclusions may be due to the difference in LBBB patient populations and insufficient follow-up time. To circumvent these limitations, our meta-analysis was the first to include a 2-year follow-up and demonstrated that LBBB after TAVR was, in fact, associated with significant increases in all-cause mortality, hospitalization for heart failure and PPI during all follow ups, and cardiovascular mortality, only at the 1-year follow up.
The effect of new-onset LBBB after TAVR on heart failure-driven hospitalization is also controversial. Some studies reported no association between new-onset LBBB and increased risk of hospitalization for heart failure after TAVR (21, 32). Conversely, in a meta-analysis involving pooled data from six studies, Faroux et al. (13). revealed that new-onset LBBB significantly increased the incidence of 1-year hospitalization for heart failure (RR1.35, 95%CI 1.05–1.72). Using extensive overview of published reports, we compiled available evidence on this issue, that revealed that the new-onset LBBB after TAVR does, in fact, increase the rate of hospitalization for heart failure. This may be related to the ventricular remodeling and left ventricular functional deterioration, caused by LBBB. During the 6–12 months follow-ups, Nazif et al. (23) showed that LVEF failed to improve after TAVR in the newly-onset LBBB patients and the values remained lower than that in patients without LBBB (53 vs. 58%, p < 0.001). Moreover, Carabba et al. (24). demonstrated that in patients without conduction disorders, LVEF was significantly improved in the early stage after TAVR and gradually stabilized over time. However, the recovery of cardiac function was slow in patients with new-onset LBBB after TAVR, as opposed to patients without new-onset LBBB, and LVEF showed a downward trend at the 1-year follow-up.
Our study also demonstrated an increased risk of PPI in the new-onset LBBB patients after TAVR, relative to non-new-onset LBBB patients. This is consistent with other studies confirming the effects of LBBB on PPI after TAVR. Data from two previous meta-analyses confirmed a two-fold increase in the risk of 1-year PPI in new-onset LBBB patients after TAVR, relative to non-new-onset LBBB patients (12, 13). From an electrophysiological point of view, the risk of LBBB progression to complete AVB after TAVR is relatively high, due to the near complete disruption of the left bundle branch conduction in these patients, even though the right bundle branch remains sufficiently activated (33). Furthermore, TAVR is mostly implanted in elderly patients, who have a high prevalence of conduction system dysfunctions, along with an increased tendency to develop high AVB from LBBB (37). Interestingly, in our meta-analysis, we discovered that patients with new-onset LBBB had the highest risk of early PPI, as opposed to non-new-onset LBBB patients. This is likely due to the fact that doctors have a lower diagnostic threshold, brought on by fear of progressing to high AVB (23). Moreover, postoperative septal inflammation, compression, and edema can increase the risk of early progression to high AVB, while over time, compression and inflammation resolution can reduce the risk of high AVB and therefore, reduce the demand for PPI (34).
Interestingly, the LBBB incidence in first-generation valvular devices after TAVR is much higher (4–65%) than with SAVR (2.3–8.6%) (38, 39). Possible reasons could include usage of different surgical equipment, records of only transient or persistent LBBB, differences in the risk of conduction disturbances, and different time points of ECG collection (40). New-onset LBBB with the SAPIEN 3 valve ranges from 6 to 29% and appears to be similar to the prior generation valve, while New-onset LBBB rate with the CoreValve Evolut R system seems to be lower than that reported with the prior CoreValve system (9). The use of mechanically expandable lotus valves confers the largest LBBB incidence after TAVR (55–77%) (41–43). Most of the conduction disturbances (90%) occur during the first week post valve implantation (44). New-onset LBBB, on the other hand, can be transient, for instance, in 19–34% of patients, it can disappear within the first few days, but in most patients (62%), it can still be detected on the 30-day follow up (21). However, it can also become a long-lasting condition, as is seen in about 66% of patients who suffer from new-onset LBBB for a year or the 0.8% of patients who experience new-onset LBBB >1-year after TAVR (37). Compared to the Edwards system, LBBB spontaneous recovery was much less frequent than with the CoreValve system (39 vs. 9.5%) (22). LBBB is an anatomic condition that occurs due to the proximity of the aortic annulus to the atrioventricular nodal-Hisian conduction system, which allows the conduction tissue in the ventricle to be vulnerable to damage, during TAVR (45). Additionally, continuous radial force, transient tissue inflammation, edema, and ischemia are thought to contribute to the possible mechanisms of abnormal conduction after TAVR (46). Multiple studies have established that predictors like valve implantation depth (47), mean aortic gradient (34), degree of annular calcification (48), prosthesis type (25), and pre-existing right bundle branch block (49), can play an important role in post-TAVR conduction abnormalities.
Due to its long-term safety implications, TAVR is more commonly used for low-to-intermediate risk patients. At present, the management of LBBB after TAVR has not been clearly defined by an international standard, so each treatment center has developed its own management strategies. Hence, it is necessary to improve identification of the predictive biomarkers for LBBB, as prompt post-procedural identification and treatment of new-onset LBBB can significantly reduce post-procedural complications. TAVR-induced LBBB is often related to a decrease in global longitudinal and radial systolic function. Therefore, prompt cardiac resynchronization therapy may restore inter-and intra-ventricular dyssynchrony and may be effective in improving left ventricular function and reducing rehospitalization incidence for heart failure. Moreover, given the adverse effects of LBBB on ventricular remodeling, operators need to take extra precaution to reduce the risk of LBBB induced by TAVR. A recent study showed that preprocedural CT imaging can help identify risk factors for conduction disturbances, such as membranous septum length, device landing zone calcium, and annular size (50). The Minimizing Depth According to the Membranous Septum (MIDAS) approach, in which operators attempted to position the self-expandable valve at a prerelease depth in relation to the non-coronary cusp of length smaller than that of the membranous septum, significantly reduced the rate of new PPI (3.0 vs. 9.7%) and new-onset LBBB (9.0 vs. 25.8%) without valve embolization or a need of second valve (51). Periprocedural planning based on the CT findings is important to reduce the risk of conduction disturbances after TAVR. Lastly, to reduce the occurrence of LBBB and prevent the potential impact of LBBB on patient prognosis, the following steps are encouraged: strictly screen patients before surgery; mastery of indications; selection of optimal surgical approach and matching valve system.
Our meta-analysis had several potential limitations: (1) we mostly analyzed observational studies, which may have introduced bias; (2) we may have unintentionally introduced information bias, due to the limited availability of original data; moreover, we extracted some RR mortality data from the Kaplan Meier curve, which may have reduced the accuracy of our results; (3) our analysis of the mortality and PPI risk in the new-onset LBBB patients post-TAVR showed heterogeneity. However, the sensitivity analysis revealed no change; (4) some of the publications, in our analysis, had non-uniformity; (5) the publication selection process was limited to the English language, which may have introduced potential language bias.
Based on our meta-analysis, patients with new-onset LBBB after TAVR had a higher risk of all-cause mortality, hospitalization for heart failure, and PPI, compared to those without new-onset LBBB. With TAVR indications expanding to patients with low surgical risk, conduction block remains an ongoing problem, and future efforts must be undertaken to identify factors associated with the progression of conduction disturbances and strengthen management to improve patient clinical outcomes.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Data analysis, interpretation, and manuscript writing were performed by JW. Literature search, study selection, data extraction, and quality assessment were performed by XH, YC, HC, and ZW. SL and BS were responsible for the conception, design of the study, and revised the manuscript carefully. All authors contributed to the article and approved the submitted version.
This systematic review was supported by the Natural Science Foundation of Gansu Province (Grant No. 20JR10RA689).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Kanwar A, Thaden JJ, Nkomo VT. Management of patients with aortic valve stenosis. Mayo Clin Proc. (2018) 93:488–508. doi: 10.1016/j.mayocp.2018.01.020
2. Osnabrugge RL, Mylotte D, Head SJ, Van Mieghem NM, Nkomo VT, LeReun CM, et al. Aortic stenosis in the elderly: disease prevalence and number of candidates for transcatheter aortic valve replacement: a meta-analysis and modeling study. J Am Coll Cardiol. (2013) 62:1002–12. doi: 10.1016/j.jacc.2013.05.015
3. Otto CM, Prendergast B. Aortic-valve stenosis–from patients at risk to severe valve obstruction. N Engl J Med. (2014) 371:744–56. doi: 10.1056/NEJMra1313875
4. Patel A, Kirtane AJ. Aortic valve stenosis. JAMA Cardiol. (2016) 1:623. doi: 10.1001/jamacardio.2016.2060
5. Leon MB, Smith CR, Mack MJ, Makkar RR, Svensson LG, Kodali SK, et al. Transcatheter or surgical aortic-valve replacement in intermediate-risk patients. N Engl J Med. (2016) 374:1609–20. doi: 10.1056/NEJMoa1514616
6. Kolte D, Vlahakes GJ, Palacios IF, Sakhuja R, Passeri JJ, Inglessis I, et al. Transcatheter versus surgical aortic valve replacement in low-risk patients. J Am Coll Cardiol. (2019) 74:1532–40. doi: 10.1016/j.jacc.2019.06.076
7. Smith CR, Leon MB, Mack MJ, Miller DC, Moses JW, Svensson LG, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. (2011) 364:2187–98. doi: 10.1056/NEJMoa1103510
8. Auffret V, Lefevre T, Van Belle E, Eltchaninoff H, Iung B, Koning R, et al. Temporal trends in transcatheter aortic valve replacement in France: FRANCE 2 to FRANCE TAVI. J Am Coll Cardiol. (2017) 70:42–55. doi: 10.1016/j.jacc.2017.04.053
9. Auffret V, Puri R, Urena M, Chamandi C, Rodriguez-Gabella T, Philippon F, et al. Conduction disturbances after transcatheter aortic valve replacement: current status and future perspectives. Circulation. (2017) 136:1049–69. doi: 10.1161/CIRCULATIONAHA.117.028352
10. Zannad F, Huvelle E, Dickstein K, van Veldhuisen DJ, Stellbrink C, Kober L, et al. Left bundle branch block as a risk factor for progression to heart failure. Eur J Heart Fail. (2007) 9:7–14. doi: 10.1016/j.ejheart.2006.04.011
11. Auffret V, Martins RP, Daubert C, Leclercq C, Le Breton H, Mabo P, et al. Idiopathic/Iatrogenic left bundle branch block-induced reversible left ventricle dysfunction: JACC state-of-the-art review. J Am Coll Cardiol. (2018) 72:3177–88. doi: 10.1016/j.jacc.2018.09.069
12. Regueiro A, Abdul-Jawad Altisent O, Del Trigo M, Campelo-Parada F, Puri R, Urena M, et al. Impact of new-onset left bundle branch block and periprocedural permanent pacemaker implantation on clinical outcomes in patients undergoing transcatheter aortic valve replacement: a systematic review and meta-analysis. Circ Cardiovasc Interv. (2016) 9:e003635. doi: 10.1161/CIRCINTERVENTIONS.115.003635
13. Faroux L, Chen S, Muntane-Carol G, Regueiro A, Philippon F, Sondergaard L, et al. Clinical impact of conduction disturbances in transcatheter aortic valve replacement recipients: a systematic review and meta-analysis. Eur Heart J. (2020) 41:2771–81. doi: 10.1093/eurheartj/ehz924
14. Tian J, Zhang J, Ge L, Yang K, Song F. The methodological and reporting quality of systematic reviews from China and the USA are similar. J Clin Epidemiol. (2017) 85:50–8. doi: 10.1016/j.jclinepi.2016.12.004
15. Ge L, Tian JH, Li YN, Pan JX, Li G, Wei D, et al. Association between prospective registration and overall reporting and methodological quality of systematic reviews: a meta-epidemiological study. J Clin Epidemiol. (2018) 93:45–55. doi: 10.1016/j.jclinepi.2017.10.012
16. Wang X, Chen Y, Yao L, Zhou Q, Wu Q, Estill J, et al. Reporting of declarations and conflicts of interest in WHO guidelines can be further improved. J Clin Epidemiol. (2018) 98:1–8. doi: 10.1016/j.jclinepi.2017.12.021
17. Yan P, Yao L, Li H, Zhang M, Xun Y, Li M, et al. The methodological quality of robotic surgical meta-analyses needed to be improved: a cross-sectional study. J Clin Epidemiol. (2019) 109:20–9. doi: 10.1016/j.jclinepi.2018.12.013
18. Pieper D, Buechter RB, Li L, Prediger B, Eikermann M. Systematic review found AMSTAR, but not R(evised)-AMSTAR, to have good measurement properties. J Clin Epidemiol. (2015) 68:574–83. doi: 10.1016/j.jclinepi.2014.12.009
19. Houthuizen P, Van Garsse LA, Poels TT, de Jaegere P, van der Boon RM, Swinkels BM, et al. Left bundle-branch block induced by transcatheter aortic valve implantation increases risk of death. Circulation. (2012) 126:720–8. doi: 10.1161/CIRCULATIONAHA.112.101055
20. Franzoni I, Latib A, Maisano F, Costopoulos C, Testa L, Figini F, et al. Comparison of incidence and predictors of left bundle branch block after transcatheter aortic valve implantation using the corevalve versus the edwards valve. Am J Cardiol. (2013) 112:554–9. doi: 10.1016/j.amjcard.2013.04.026
21. Testa L, Latib A, De Marco F, De Carlo M, Agnifili M, Latini RA, et al. Clinical impact of persistent left bundle-branch block after transcatheter aortic valve implantation with corevalve revalving system. Circulation. (2013) 127:1300–7. doi: 10.1161/CIRCULATIONAHA.112.001099
22. Houthuizen P, van der Boon RM, Urena M, Van Mieghem N, Brueren GB, Poels TT, et al. Occurrence, fate and consequences of ventricular conduction abnormalities after transcatheter aortic valve implantation. EuroIntervention. (2014) 9:1142–50. doi: 10.4244/EIJV9I10A194
23. Nazif TM, Williams MR, Hahn RT, Kapadia S, Babaliaros V, Rodés-Cabau J, et al. Clinical implications of new-onset left bundle branch block after transcatheter aortic valve replacement: analysis of the PARTNER experience. Eur Heart J. (2014) 35:1599–607. doi: 10.1093/eurheartj/eht376
24. Carrabba N, Valenti R, Migliorini A, Marrani M, Cantini G, Parodi G, et al. Impact on left ventricular function and remodeling and on 1-year outcome in patients with left bundle branch block after transcatheter aortic valve implantation. Am J Cardiol. (2015) 116:125–31. doi: 10.1016/j.amjcard.2015.03.054
25. Schymik G, Tzamalis P, Bramlage P, Heimeshoff M, Wurth A, Wondraschek R, et al. Clinical impact of a new left bundle branch block following TAVI implantation: 1-year results of the TAVIK cohort. Clin Res Cardiol. (2015) 104:351–62. doi: 10.1007/s00392-014-0791-2
26. Lopez-Aguilera J, Segura Saint-Gerons JM, Mazuelos Bellido F, Suarez de Lezo Herreros de Tejada J, Pineda SO, Pan Alvarez-Ossorio M, et al. Effect of new-onset left bundle branch block after transcatheter aortic valve implantation (CoreValve) on mortality, frequency of re-hospitalization, and need for pacemaker. Am J Cardiol. (2016) 118:1380–5. doi: 10.1016/j.amjcard.2016.07.057
27. Chamandi C, Barbanti M, Munoz-Garcia A, Latib A, Nombela-Franco L, Gutierrez-Ibanez E, et al. Long-term outcomes in patients with new-onset persistent left bundle branch block following TAVR. JACC Cardiovasc Interv. (2019) 12:1175–84. doi: 10.1016/j.jcin.2019.03.025
28. Eschalier R, Massoullie G, Nahli Y, Jean F, Combaret N, Ploux S, et al. New-onset left bundle branch block after TAVI has a deleterious impact on left ventricular systolic function. Can J Cardiol. (2019) 35:1386–93. doi: 10.1016/j.cjca.2019.05.012
29. Jorgensen TH, De Backer O, Gerds TA, Bieliauskas G, Svendsen JH, Sondergaard L. Mortality and heart failure hospitalization in patients with conduction abnormalities after transcatheter aortic valve replacement. JACC Cardiovasc Interv. (2019) 12:52–61. doi: 10.1016/j.jcin.2018.10.053
30. Kessler M, Gonska B, Seeger J, Rottbauer W, Wohrle J. Long-term clinical outcome of persistent left bundle branch block after transfemoral aortic valve implantation. Catheter Cardiovasc Interv. (2019) 93:538–44. doi: 10.1002/ccd.27850
31. Nazif TM, Chen S, George I, Dizon JM, Hahn RT, Crowley A, et al. New-onset left bundle branch block after transcatheter aortic valve replacement is associated with adverse long-term clinical outcomes in intermediate-risk patients: an analysis from the PARTNER II trial. Eur Heart J. (2019) 40:2218–27. doi: 10.1093/eurheartj/ehz227
32. Urena M, Webb JG, Cheema A, Serra V, Toggweiler S, Barbanti M, et al. Impact of new-onset persistent left bundle branch block on late clinical outcomes in patients undergoing transcatheter aortic valve implantation with a balloon-expandable valve. JACC Cardiovasc Interv. (2014) 7:128–36. doi: 10.1016/j.jcin.2013.08.015
33. Sasaki K, Izumo M, Kuwata S, Ishibashi Y, Kamijima R, Watanabe M, et al. Clinical impact of new-onset left bundle-branch block after transcatheter aortic valve implantation in the japanese population- a single high-volume center experience. Circ J. (2020) 84:1012–9. doi: 10.1253/circj.CJ-19-1071
34. Akdemir B, Roukoz H. A single-centre cohort and short-term follow-up of patients who developed persistent new onset left bundle branch block after transcatheter aortic valve replacement. Acta Cardiol. (2020) 75:360–5. doi: 10.1080/00015385.2020.1713520
35. Hamandi M, Tabachnick D, Lanfear AT, Baxter R, Shin K, Zingler B, et al. Effect of new and persistent left bundle branch block after transcatheter aortic valve replacement on long-term need for pacemaker implantation. Proc (Bayl Univ Med Cent). (2020) 33:157–62. doi: 10.1080/08998280.2020.1717906
36. Witt CM, Wu G, Yang D, Hodge DO, Roger VL, Cha YM. Outcomes with left bundle branch block and mildly to moderately reduced left ventricular function. JACC Heart Fail. (2016) 4:897–903. doi: 10.1016/j.jchf.2016.07.002
37. Massoullié G, Bordachar P, Ellenbogen KA, Souteyrand G, Jean F, Combaret N, et al. New-onset left bundle branch block induced by transcutaneous aortic valve implantation. Am J Cardiol. (2016) 117:867–73. doi: 10.1016/j.amjcard.2015.12.009
38. Poels TT, Houthuizen P, Van Garsse LA, Soliman Hamad MA, Maessen JG, Prinzen FW, et al. Frequency and prognosis of new bundle branch block induced by surgical aortic valve replacement. Eur J Cardiothorac Surg. (2015) 47:e47–53. doi: 10.1093/ejcts/ezu435
39. Van Mieghem NM, Head SJ, de Jong W, van Domburg RT, Serruys PW, de Jaegere PP, et al. Persistent annual permanent pacemaker implantation rate after surgical aortic valve replacement in patients with severe aortic stenosis. Ann Thorac Surg. (2012) 94:1143–9. doi: 10.1016/j.athoracsur.2012.04.038
40. Muntané-Carol G, Guimaraes L, Ferreira-Neto AN, Wintzer-Wehekind J, Junquera L, Del Val D, et al. How does new-onset left bundle branch block affect the outcomes of transcatheter aortic valve repair? Expert Rev Med Devices. (2019) 16:589–602. doi: 10.1080/17434440.2019.1624161
41. Zaman S, McCormick L, Gooley R, Rashid H, Ramkumar S, Jackson D, et al. Incidence and predictors of permanent pacemaker implantation following treatment with the repositionable Lotus™ transcatheter aortic valve. Catheter Cardiovasc Interv. (2017) 90:147–54. doi: 10.1002/ccd.26857
42. Rampat R, Khawaja MZ, Byrne J, MacCarthy P, Blackman DJ, Krishnamurthy A, et al. Transcatheter aortic valve replacement using the repositionable LOTUS valve: United Kingdom experience. JACC Cardiovasc Interv. (2016) 9:367–72. doi: 10.1016/j.jcin.2015.12.012
43. Keßler M, Gonska B, Seeger J, Rottbauer W, Wöhrle J. Predictors of permanent pacemaker implantation after transfemoral aortic valve implantation with the Lotus valve. Am Heart J. (2017) 192:57–63. doi: 10.1016/j.ahj.2017.07.011
44. Nazif TM, Dizon JM, Hahn RT, Xu K, Babaliaros V, Douglas PS, et al. Predictors and clinical outcomes of permanent pacemaker implantation after transcatheter aortic valve replacement: the PARTNER (Placement of AoRtic TraNscathetER Valves) trial and registry. JACC Cardiovasc Interv. (2015) 8:60–9. doi: 10.1016/j.jcin.2014.07.022
45. Piazza N, de Jaegere P, Schultz C, Becker AE, Serruys PW, Anderson RH. Anatomy of the aortic valvar complex and its implications for transcatheter implantation of the aortic valve. Circ Cardiovasc Interv. (2008) 1:74–81. doi: 10.1161/CIRCINTERVENTIONS.108.780858
46. Piazza N, Onuma Y, Jesserun E, Kint PP, Maugenest AM, Anderson RH, et al. Early and persistent intraventricular conduction abnormalities and requirements for pacemaking after percutaneous replacement of the aortic valve. JACC Cardiovasc Interv. (2008) 1:310–6. doi: 10.1016/j.jcin.2008.04.007
47. Aktug O, Dohmen G, Brehmer K, Koos R, Altiok E, Deserno V, et al. Incidence and predictors of left bundle branch block after transcatheter aortic valve implantation. Int J Cardiol. (2012) 160:26–30. doi: 10.1016/j.ijcard.2011.03.004
48. Hein-Rothweiler R, Jochheim D, Rizas K, Egger A, Theiss H, Bauer A, et al. Aortic annulus to left coronary distance as a predictor for persistent left bundle branch block after TAVI. Catheter Cardiovasc Interv. (2017) 89:E162–e8. doi: 10.1002/ccd.26503
49. Auffret V, Webb JG, Eltchaninoff H, Muñoz-García AJ, Himbert D, Tamburino C, et al. Clinical impact of baseline right bundle branch block in patients undergoing transcatheter aortic valve replacement. JACC Cardiovasc Interv. (2017) 10:1564–74. doi: 10.1016/j.jcin.2017.05.030
50. Nakashima M, Jilaihawi H. Conduction disturbances and pacing in transcatheter aortic valve replacement. Interv Cardiol Clin. (2021) 10:455–63. doi: 10.1016/j.iccl.2021.05.003
Keywords: transcatheter aortic valve replacement, left bundle branch block, mortality, hospitalization for heart failure, permanent pacemaker implantation
Citation: Wang J, Liu S, Han X, Chen Y, Chen H, Wan Z and Song B (2022) Prognostic Outcome of New-Onset Left Bundle Branch Block After Transcatheter Aortic Valve Replacement in Patients With Aortic Stenosis: A Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 9:842929. doi: 10.3389/fcvm.2022.842929
Received: 24 December 2021; Accepted: 03 March 2022;
Published: 08 April 2022.
Edited by:
Verena Veulemans, University Hospital of Düsseldorf, GermanyReviewed by:
Alexander Sedaghat, University Hospital Bonn, GermanyCopyright © 2022 Wang, Liu, Han, Chen, Chen, Wan and Song. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bing Song, c29uZ2JpbmxkeXlAMTYzLmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.