
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Cardiovasc. Med. , 02 March 2022
Sec. Cardiac Rhythmology
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.832446
This article is part of the Research Topic Cardiac Arrhythmias and Stereotactic Radioblation: Pros and cons View all 14 articles
 Antonio Di Monaco1,2†
Antonio Di Monaco1,2† Fabiana Gregucci3†
Fabiana Gregucci3† Ilaria Bonaparte3
Ilaria Bonaparte3 Federica Troisi1
Federica Troisi1 Alessia Surgo3Domenico Di Molfetta4Nicola Vitulano1Federico Quadrini1Roberta Carbonara3Gaetano Martinelli4Pietro Guida1
Alessia Surgo3Domenico Di Molfetta4Nicola Vitulano1Federico Quadrini1Roberta Carbonara3Gaetano Martinelli4Pietro Guida1 Maria Paola Ciliberti3
Maria Paola Ciliberti3 Alba Fiorentino3*
Alba Fiorentino3* Massimo Grimaldi1
Massimo Grimaldi1Treatment approach for elderly patients with atrial fibrillation (AF) is difficult. The present prospective phase-II trial evaluated LINAC-based stereotactic arrhythmia radioablation safety in this population. The reported data of the first 5 patients worldwide, showed no side effects, absence of AF episodes and without antiarrhythmic drugs.
Trial Registration: ClinicalTrials.gov, identifier: NCT04575662.
Atrial fibrillation (AF) is the most common cardiac arrhythmia affecting more than 40 million individuals in the world, and elderly age is a prominent risk factor (1).
AF increased the risk of stroke and heart failure with a reduction in functional capacity (1). Current guidelines recommend Pulmonary Veins (PVs) isolation with catheter ablation (CA) in symptomatic patients refractory to antiarrhythmic therapy (AAT) (1).
In elderly, paroxysmal AF is difficult to treat with drugs, since they alternate sinus bradycardia and fast rate AF in the so-called tachy-bradi syndrome, and by CA due to the higher complication rate (1, 2). Thus, a non-invasive approach should be favorite.
Other ablation approaches have been implemented in cardiac arrhythmia, including stereotactic arrhythmia radioablation (STAR) or radiosurgery which is a safe and effective arm in the oncological and non-oncological scenario. STAR, using high-dose radiation, produced great biological cell kill death by multifactorial results (DNA double-strand breaks, apoptosis, vascular damage, ischemic cell-death) (3–5).
As we reported in a previous review, in field of preclinical research applied to STAR, several studies were conducted in animal models, showed also in porcine model the PVs isolation to treat AF could be achieved by radiosurgery with a conventional LINear ACcelerators (LINACs) (3).
Several STAR data were published for ventricular tachycardia, using different technologies, including LINACs or Cyberknife, but, as reported recently by Lydiard et al., “LINACs have not yet been used for AF treatments” (6).
Based on the latter background, a prospective phase-II trial was designed to evaluate safety of LINAC-based STAR (ClinicalTrials.gov: NCT04575662). We selected the elderly population with refractory AF due to the risk of recurrence of FA after the standard CA procedure and due to the risk of complication for these patients.
Here, the data of the first 5 elderly patients worldwide were preliminary reported.
Inclusion criteria were: age more than 70 years; symptomatic paroxysmal AF; intolerance or non-response to AAT. All patients performed 1-week ECG-Holter monitoring (ECG-HM) (during AAT and AAT wash-out), a complete transthoracic echocardiogram, including the left atrial (LA) strain evaluation before STAR.
The study was approved by the local Ethics Committee and all patients signed informed consent.
The Transthoracic echocardiogram and atrial strain evaluation were performed. For 2D-STE analysis, a volumetric image of LA from the apical view was obtained and stored. An echocardiography core laboratory measured parameters related to LA Strain with a dedicated software (Philips, Epiq 7-Auto Strain Tomtec Application). To assess LA Strain we evaluated LA Reservoir-Strain (LASr) based on ED (End-Diastole) and Pre-A (pre-Atrial contraction), LA Conduit-Strain (LAScd) based on ED and Pre-A, LA Contraction-Strain (LASct) based on ED and Pre-A. LA area strain analysis was performed according to the methods previously described and according to the Task Force to standardize deformation imaging (7).
STAR procedures were shown in Figure 1. They were immobilized using a vac-lock bag and 3 Computed Tomography (CT, 1 mm slice-thickness), in the supine position were performed: basic free-breathing CT for dose calculation; 4-Dimension CT for moving evaluation; CT with contrast for anatomical accuracy (3–5).
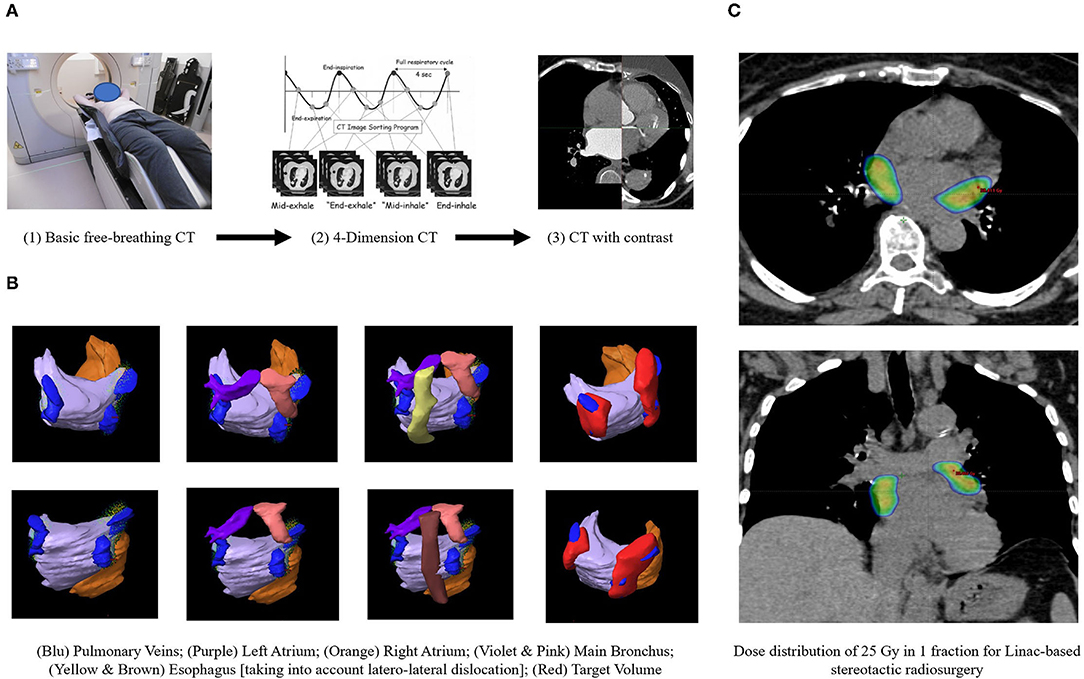
Figure 1. The workflow of LINAC-based STAR. (A) Simulation procedures. (B) Organs at risks and target volume identification. (C) Treatment planning.
Several Organs at Risks (OaRs) were contoured, making more attention to esophagus and main bronchus, for which a planning risk volume (PRV) was built. The clinical target volume (CTV) was identified by radiation oncologists and cardiologist and was defined as the area around PVs. From CTV, an internal target volume (ITV) was created to compensate heart and respiratory movement. Finally, the planning target volume (PTV) was defined adding 0–3 mm to the ITV, excluding the overlap area with OaRs/PRV, where PTV was cropped.
STAR was performed in free-breathing with a PTV prescription total dose (Dp) of 25 Gy/1 fraction. A “simultaneous integrated protection” dose was realized to the interface between PTV-PRV to ensure the tolerability of critical structures (8). Flattening Filter Free (FFF), Volumetric Modulated Arc Therapy (VMAT) plan was generated, normalizing 100% Dp to 95% of the volume, while large intra-target dose heterogeneity D2% (PTV) <150%Dp was accepted. The treatment was generated, optimized and delivered by TrueBeamTM (Varian Medical System). Image-guided radiotherapy (IGRT) with Cone Beam CT and Surface-Guided RadioTherapy (SGRT) with Align-RT (Vision RT) were used to reduce set-up error and to monitor patients during fraction.
Follow-up consisted of clinical evaluation during and for 48 h after STAR. One-week ECG-Holter monitoring, transthoracic echocardiogram and clinical evaluation are performed 1, 3, 6, and 12 months after STAR.
The primary endpoint is the 1-month post-STAR safety, as complete STAR delivery and no acute treatment-related adverse events more than G3, assessed according to the Common Terminology Criteria for Adverse Events (version 5.0). Secondary endpoints were: reductions in AF episodes and in AAT, overall survival. The sample size planning is 20 cases based on 95% success for the primary endpoint, with a significant level of 5% and a power of 90%.
From May 2021 to January 2022, 11 elderly patients were enrolled, of which 6 were treated. AAT was stopped after enrollment.
For primary endpoint (side effects at 1 month after STAR), 5 patients completed treatment without acute treatment-related adverse events (>G1) and 1 patient has only 7 days of follow-up. The main STAR data are summarized in Table 1. The treatment plan was delivered with 3 no-coplanar arcs, in all cases. The mean Overall Treatment Time (OTT) was 3 min. Only patient-1 needed adaptive real-live radiotherapy due to the esophagus position, in fact at IGRT before STAR the esophagus position was completely different from CT simulation.
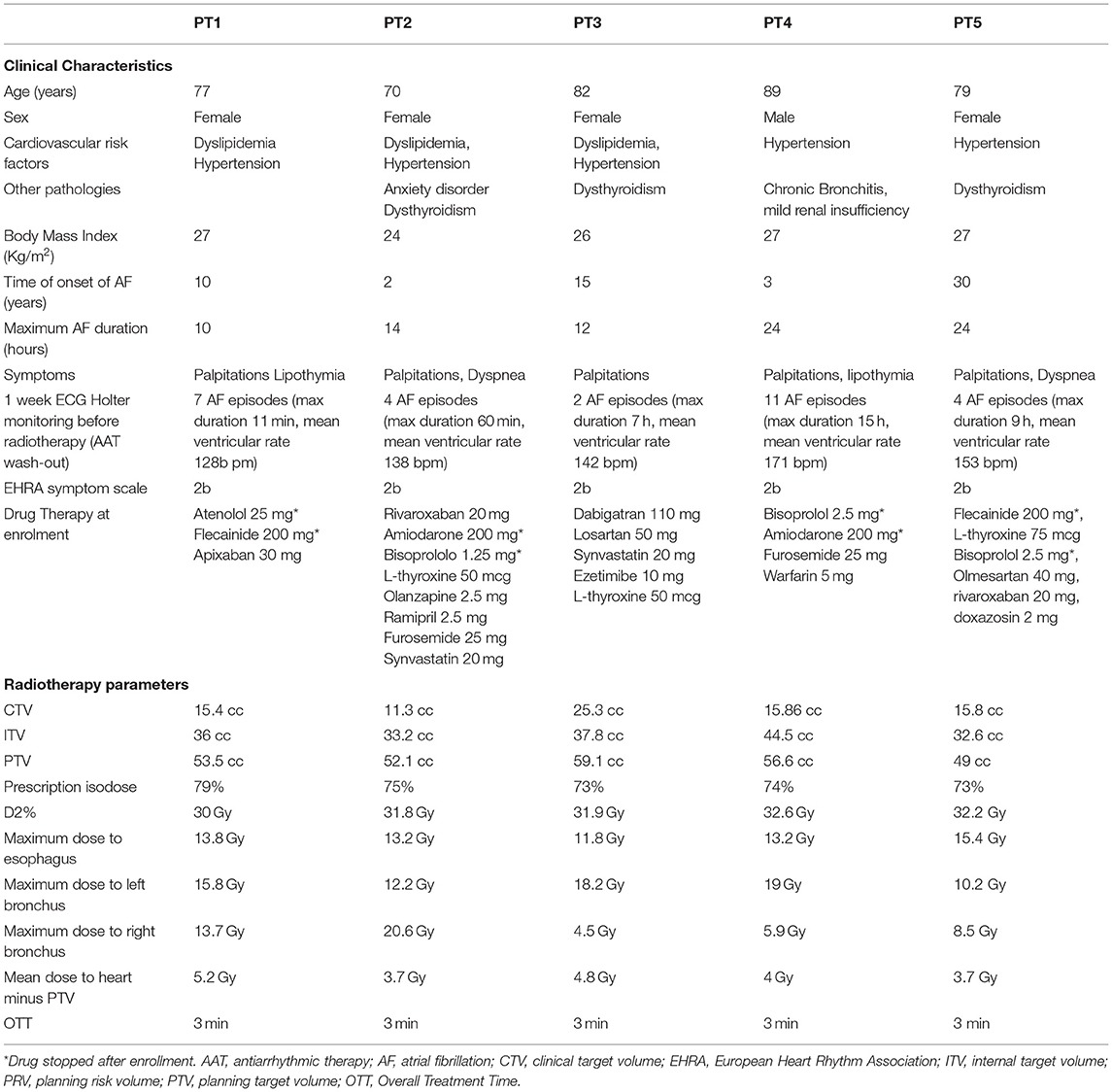
Table 1. Patient characteristics and main treatment planning and dosimetric data.
Four patients completed a 3 months FUP with transthoracic echocardiogram data. At baseline, LAV and LAA in PT-1 were significantly increased, in PT-2 moderately and in PT-3 slightly compared to the reference values. Strain parameters at baseline were also mild to moderate compromised or severely compromised compared to the reference values (Table 2).
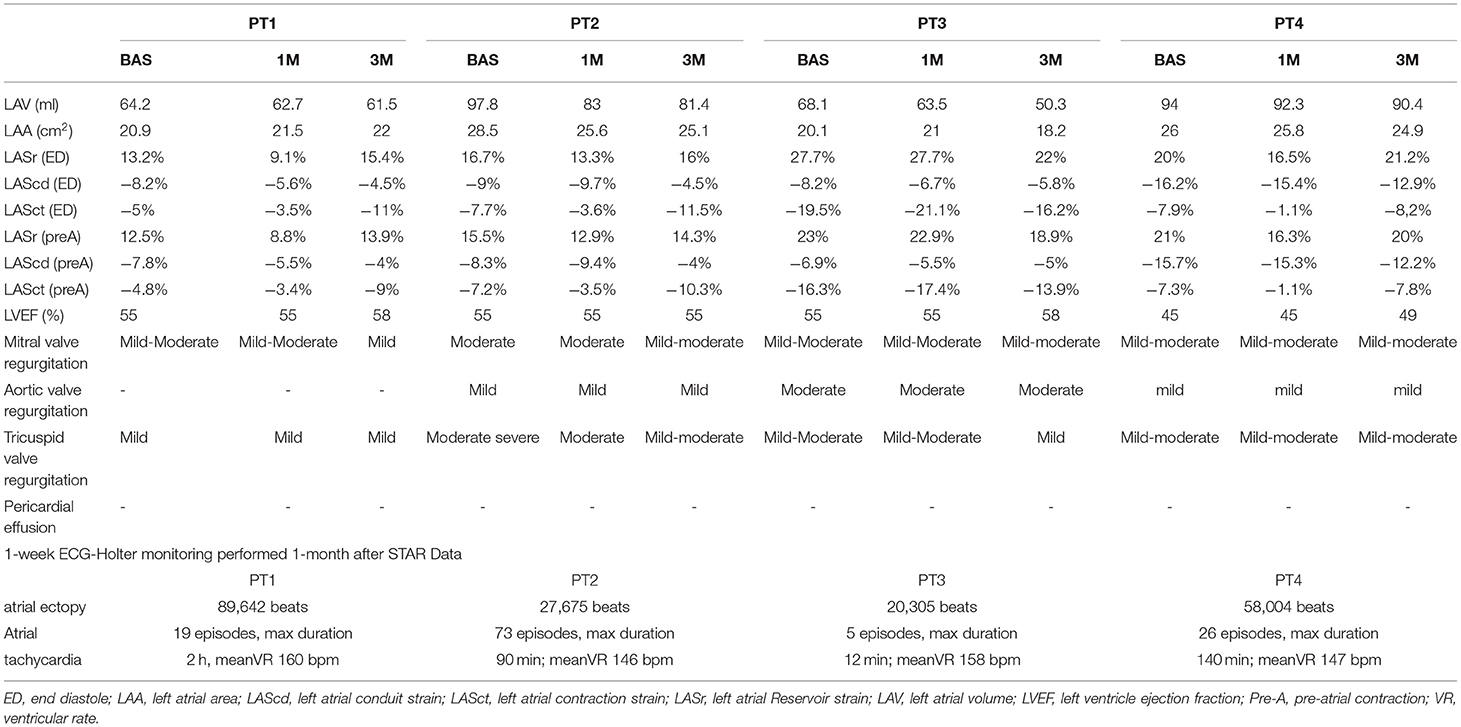
Table 2. Main echocardiographic and ECG-HOLTER parameters.
The 1-week ECG-HM performed 1-month after procedure documented frequent atrial ectopy and atrial tachycardia without AF recurrences. A rare atrial ectopy without AF recurrences was documented at 3 months after procedure. No patients started AAT after radiotherapy. Regarding echocardiographic data, at 1-month follow-up in PT1-2-4 LASr (ED) and LASr (pre-A) were reduced with a prevalent reduction of the LASct component. In the PT-3, no significant reduction in the strain parameters was reported. At 3-month, a recovery trend of the global strain parameter was shown in PT1-2-4. At 1 and 3-months LAV and LAA were slightly reduced in all patients.
Patients 1–3 had a FUP of 6–7 months, Patient 4 a FUP of 3 months, Patient 5 a FUP of 1 month. For all treated patients with a mean follow-up of 4 months, no acute and late side effects were reported. Only one patient experienced G1 esophagitis (7 days from STAR), improved by 5 days of medical therapy.
Elderly patients affected by AF are a fragile population at higher risk of all CA procedural complications (1, 2), including vascular injury, cardiac perforation, phrenic nerve injury, stroke, and most concerning, atrio-esophageal fistula, which portend a high mortality rate and a higher rate of AF recurrences. For the latter reasons, in the clinical practice it is preferred to use pharmacological treatment rather than interventional procedures to treat AF in elderly.
STAR approach have been recently implemented, but no experience of LINAC has been published for AF (6). The present phase-II preliminary worldwide LINAC-STAR data on elderly patients showed: no acute toxicities; no AF episodes; no AAT use.
Three STAR-AF cases were published with Cyberknife technology, reporting an OTT of 90 min (9, 10). To optimize target tracking during cardiorespiratory motion, an internal fiducial marker was placed transvenously in proximity to the left atrial target (9). In 2 out 3 patients, AF occurred at 6-months from Cyberknife-STAR (9, 10).
Comparing the latter data with the present analysis, 2 differences should be highlighted.
In regards to target volume, the mainstay AF ablation approach is a PVs isolation, while appropriate/effective ablation targets, including atrial wall, remain poorly defined (1, 9, 10). In the Cyberknife cases, PVs and the left atrial posterior wall were irradiated, while in the present study, target was defined as the area around PVs. Moreover, higher dose was mainly located on the left lateral ridge, the area between appendage and left PVs (higher arrhythmogenesis area) (11).
In terms of TT, Cyberknife device is mounted on a robotic arm to deliver radiation to a tumor from different trajectories, while LINAC with a rotation of its gantry deliver high dose of radiation in a shorter time (3 vs. 90 min) (12). However, the shorter time is essential for reducing intrafraction motion, so in the present trial, due to the motion study and IGRT/SGRT monitoring, the introduction of fiducial was not necessary (3–5, 12).
Cyberknife device is mounted on a robotic arm to deliver radiation to a tumor from different trajectories, while LINAC with a rotation of its gantry deliver high dose of radiation in a shorter time (3 vs. 90 min).
Due to the innovation of this treatment for AF, sufficient data regarding procedural complications are not still available. However, previous studies reported STAR related complications during ventricular tachycardia treatment. In particular, a low percentage of complications was reported mainly within 90 days from STAR (heart failure exacerbation, radiation pericarditis and pneumonitis, nausea) and at long term follow up (mitral valve regurgitation worsening, pericardial effusions and gastro-pericardial fistula) (12).
Moreover, this analysis is the first to report clinical response. The frequent atrial ectopy and the atrial strain variations after procedure are probably indirect signs of effective atrial irritation due to radiotherapy. Some recent studies have shown the correlation between LA strain and atrial fibrosis, hypothesizing its prediction of the usefulness of ablation procedure (13). In this study, LAS parameters, based on ED and Pre-A, in three patients reduced 1-month after STAR. The LASct decreasing is related to atrial contraction phase of the cardiac cycle, probably due to acute irritation of the atrium immediately after STAR. The patient-3 showed no significant reduction in LAS parameters in the 1-month follow-up probably because atrial strain values were slightly reduced compared to normal. At the 3-month, a trend in recovery of LASr was found in the three patients. Finally, a reduction trend in LA volume and area was found in all patients probably because the maintenance of sinus rhythm improved ventricular performance with a reduction in the extent of mitral and tricuspid insufficiency and LA volume overload.
The present collected data are promising, showing the safety of LINAC-based STAR for AF for the first 5 patients. This new ablation approach could represent a valid non-invasive alternative for elderly who were excluded from catheter ablation. Prospective randomized trials are guaranteed.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Comitato Etico Interregionale; Policlinico di Bari - Bari. The patients/participants provided their written informed consent to participate in this study.
AD, FG, AF, and MG write the protocol study and have the idea. IB, FG, AS, RC, MC, and AF are the responsibility of radiotherapy and radiotherapy data. AD, MG, NV, FQ, and FT are responsible of cardiological data. GM and DD are responsible of radiological data. AD, FG, and AF write the paper. PG analyzed the statistical data. All authors corrected, improved the manuscript, and interpreted the results.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. (2021) 42:373–498. doi: 10.1093/eurheartj/ehaa612
2. Kennedy R, Oral H. Catheter ablation of atrial fibrillation in the elderly: does the benefit outweigh the risk? Expert Rev Cardiovasc Ther. (2013) 11:697–704. doi: 10.1586/erc.13.2
3. Fiorentino A, Gregucci F, Bonaparte I, Vitulano N, Surgo A, Mazzola R, et al. Stereotactic Ablative radiation therapy (SABR) for cardiac arrhythmia: a new therapeutic option? Radiol Med. (2021) 126:155–62. doi: 10.1007/s11547-020-01218-7
4. Bonaparte I, Gregucci F, Surgo A, Di Monaco A, Vitulano N, Ludovico E, et al. Linac-based STereotactic Arrhythmia Radioablation (STAR) for ventricular tachycardia: a treatment planning study. Jpn J Radiol. (2021) 39:1223–8 doi: 10.1007/s11604-021-01159-9
5. Fiorentino A, Di Monaco A, Surgo A, Vitulano N, Gregucci F, Ludovico E, et al. Linac-based STereotactic Arrhythmia Radioablation (STAR) of ventricular tachycardia: case report and literature review. Clin Case Rep. (2020) 9:362–6. doi: 10.1002/ccr3.3530
6. Lydiard S, Blanck O, Hugo G, O'Brien R, Keall P. A review of Cardiac Radioablation (CR) for arrhythmias: procedures, technology, and future opportunities. Int J Radiat Oncol Biol Phys. (2021) 109:783–800. doi: 10.1016/j.ijrobp.2020.10.036
7. Badano LP, Kolias TJ, Muraru D, Abraham TP, Aurigemma G, Edvardsen T, et al. Standardization of left atrial, right ventricular, and right atrial deformation imaging using two-dimensional speckle tracking echocardiography: a consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur Heart J Cardiovasc Imaging. (2018) 19:591–600. doi: 10.1093/ehjci/jey042
8. Benedict SH, Yenice KM, Followill D, Galvin JM, Hinson W, Kavanagh B, et al. Stereotactic body radiation therapy: the report of AAPM Task Group 101. Med Phys. (2010) 37:4078–101. doi: 10.1118/1.3438081
9. Monroy E, Azpiri J, De La Peña C, Cardona C, Hinojosa M, Zamarripa R, et al. Late gadolinium enhancement cardiac magnetic resonance imaging post-robotic Radiosurgical Pulmonary Vein Isolation (RRPVI): first case in the world. Cureus. (2016) 8:e738. doi: 10.7759/cureus.738
10. Qian PC, Azpiri JR, Assad J, Gonzales Aceves EN, Cardona Ibarra CE, de la Pena C, et al. Noninvasive stereotactic radioablation for the treatment of atrial fibrillation: First-in-man experience. J Arrhyth. (2020) 36:67–74. doi: 10.1002/joa3.12283
11. Di Monaco A, Quadrini F, Troisi F, Vitulano N, Cecere G, Guida P, et al. Bilateral left lateral ridge ablation increases the long-term success of patients ablated for atrial fibrillation. J Cardiovasc Med (Hagerstown). (2019) 20:186–91 doi: 10.2459/JCM.0000000000000779
12. Jumeau R, Ozsahin M, Schwitter J, Elicin O, Reichlin T, Roten L, et al. Stereotactic radiotherapy for the management of refractory ventricular tachycardia: promise and future directions. Front Cardiovasc Med. (2020) 7:108. doi: 10.3389/fcvm.2020.00108
13. Laish-Farkash A, Perelshtein Brezinov O, Valdman A, Tam D, Rahkovich M, Kogan Y, et al. Evaluation of left atrial remodeling by 2D-speckle-tracking echocardiography versus by high-density voltage mapping in patients with atrial fibrillation. J Cardiovasc Electrophysiol. (2021) 32:305–15. doi: 10.1111/jce.14837
Keywords: radioablation, stereotactic body radiotherapy, arrhythmia, atrial fibrillation (AF), elderly patients
Citation: Di Monaco A, Gregucci F, Bonaparte I, Troisi F, Surgo A, Di Molfetta D, Vitulano N, Quadrini F, Carbonara R, Martinelli G, Guida P, Ciliberti MP, Fiorentino A and Grimaldi M (2022) Paroxysmal Atrial Fibrillation in Elderly: Worldwide Preliminary Data of LINAC-Based Stereotactic Arrhythmia Radioablation Prospective Phase II Trial. Front. Cardiovasc. Med. 9:832446. doi: 10.3389/fcvm.2022.832446
Received: 09 December 2021; Accepted: 08 February 2022;
Published: 02 March 2022.
Edited by:
Maria Lucia Narducci, Catholic University of the Sacred Heart, ItalyReviewed by:
Silvia Magnani, New York University, United StatesCopyright © 2022 Di Monaco, Gregucci, Bonaparte, Troisi, Surgo, Di Molfetta, Vitulano, Quadrini, Carbonara, Martinelli, Guida, Ciliberti, Fiorentino and Grimaldi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alba Fiorentino, YS5maW9yZW50aW5vQG1pdWxsaS5pdA==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.