
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Cardiovasc. Med. , 15 July 2022
Sec. General Cardiovascular Medicine
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.823885
This article is part of the Research Topic Cardiorenal Syndromes: From pathogenesis to clinical research View all 10 articles
 Dong-Hong Zhang1Chen Yuan2Bei-Bei Wang3
Dong-Hong Zhang1Chen Yuan2Bei-Bei Wang3 Xin-Jiang Dong4Shu-Ping Lv5Fei-Hong Li6Zhen-Xiu Hou3Xiao-Li Liu7Kang Chen2*
Xin-Jiang Dong4Shu-Ping Lv5Fei-Hong Li6Zhen-Xiu Hou3Xiao-Li Liu7Kang Chen2*Purpose: Cardiac syndrome X (CSX) is a condition with normal coronary angiography but angina pectoris. Chronic inflammation caused by Helicobacter pylori (H. pylori) infection may play a pathogenic role in CSX. Therefore, we conducted a meta-analysis to explore the relationship between H. pylori infection and risk of CSX.
Methods: A systematic search in the Web of Science, Medline, Embase and Chinese databases (CNKI and Wanfang) was conducted up to October 2021. Articles on the association between H. pylori infection and the risk of CSX were included and were analyzed by R software (version 4.1.0).
Results: Ten case-control studies involving 703 CSX patients and 731 healthy controls were included. H. pylori infection was associated with an increased risk of CSX (OR: 8.29, 95% CI: 4.64–14.82). We also found a significant association in those 25–40 years of age (OR: 1.34, 95% CI: 1.04–1.72), those 40–50 years of age (OR: 11.27, 95% CI: 4.29–29.61), those over 50 years of age (OR: 7.18, 95% CI: 3.59–14.36), those in developing countries [Iran (OR: 12.99, 95% CI: 8.61–19.60) and China (OR: 5.14, 95% CI: 3.09–8.56)]. However, this association was not apparent in a developed country [Italy (OR: 0.93, 95% CI: 0.37–2.33)].
Conclusions: Our study suggested a possible association between H. pylori infection and the risk of CSX. Its pathogenicity is stronger in middle-aged individuals and some developing countries. However, more studies are needed to further investigate whether early eradication of H. pylori can reduce the incidence rate of CSX, especially in middle-aged individuals and some developing countries.
Helicobacter pylori (H. pylori) is a gram-negative bacterium that causes a variety of gastrointestinal disorders, including chronic gastritis, duodenal ulcer and gastric cancer (1, 2). It may also cause some extra-intestinal diseases, some of which are manifested as respiratory diseases and functional ischemic heart disease (1, 2), recently found to be related to Cardiac Syndrome X (CSX) (3–5). Virulent strains H. pylori can be divided into two subgroups based upon the expression of (6) an immunodominant, 120–145 kDa protein, cytotoxin-associated gene A (CagA). Infection with CagA may be a strong risk factor for the development of CSX by inducing endothelial dysfunction (7).
CSX is characterized by typical exertional angina pectoris, positive electrocardiograph (ECG) or exercise treadmill test, normal coronary angiography with the exclusion of coronary artery spasm. In angina patients undergoing angiography, up to 20% of patients have this symptom (3). Despite extensive studies, the mechanism of this syndrome is still unclear. Nevertheless, it has been proposed that coronary artery endothelial dysfunction is the main pathogenic mechanism underlying CSX (5).
While many studies have attempted to reveal the role of H. pylori infection in CSX, their results are contradictory. Thus, we conducted a meta-analysis of relevant articles in an attempt to reveal the association between H. pylori infection and the risk of CSX.
Our meta-analysis strictly adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (8).
The meta-analysis was performed with a structured articles search, using the Web of Science, Medline, Embase and Chinese databases (CNKI and Wanfang). The keywords “H. pylori” or “Helicobacter pylori,” combined with “Cardiac syndrome X,” “microvascular angina,” “CSX,” and “MVA” were used as search terms. There were no language restrictions in the search. The references in the identified articles were checked and if suitable, were also included in the search. The deadline for searching was October 2021.
We repeated all selections. The final inclusion of articles was decided upon by consensus, and when this decision failed, the third author (LXL) made a ruling.
Observational studies (cohort, case–control and cross-sectional) were included if the following criteria were met:
1. Studies were conducted in humans.
2. H. pylori infection was determined by serological tests, including antigen-specific enzyme-linked immunosorbent assay (ELISA) and Western blotting, or non-serological tests including rapid urease test, and 13C-urea breath test (UBT) according to the manufacturer's instructions.
3. The diagnosis of CSX included the following criteria: typical history of angina and normal coronary angiography; atypical chest pain with an abnormal myocardial perfusion Image; or exercise electrocardiogram and completely normal results on coronary angiography, with no inducible spasm on ergonovine-provocation test.
4. A control group was included. Studies with matched and sufficient information on the association between H. pylori infection and the risk of CSX were selected.
5. For articles with data published more than once, only the article with an adequate study strategies and large number of cases was selected.
6. Patients with evidence of left or right ventricular dysfunction, cardiomyopathy, valvular heart disease, myocardial infarction, concomitant acute and chronic disease were excluded.
Two well-trained researchers (LSP and LFH) independently extracted the following data based on the pre-specified scheme: first author or second author; average age of case group; year of publication; country; study size; case type; control type; and matching variables. All data were double input.
Our meta-analysis was conducted according to the recommendations of Cochrane Collaboration and meta-analysis report quality guidelines (9, 10) and was performed using R software (version 4.1.0). The I2 statistics were used to assess statistical heterogeneity. A value >50% was considered to have significant heterogeneity and random effect models were used to pool data. Otherwise, the fixed effects model was used. The estimated effect measure was the odds ratio (OR) with 95% confidence intervals (95% CIs) for the dichotomous data. If the 95% CI did not contain the value one, the OR was considered to be statistically significant.
The Egger's and Begg's tests were used to assess potential publication bias. Each article in this analysis was sequentially deleted to determine how much it contributed to the overall effect size. The Newcastle-Ottawa Scale (NOS) was adopted to score all articles. Articles that scored ≥7 points were considered “high-quality articles.” Several subgroup meta-analyses were performed based on country, mean age, case type, H. pylori detection method, socioeconomic status and year of publication.
Using our keywords and the references from identified articles, a total of 478 potentially relevant articles were identified. After excluding duplicates, 193 articles remained, of which 152 articles were excluded after checking the title and abstract. After carefully assessing the full text of the remaining 41 articles, 31 articles were determined to not meet inclusion criteria. This was because: (1) They were comments/reviews/case reports without raw data; or (2) They were other special studies, such as in vitro studies, animal studies, or epidemic pathological studies focusing on the relationship between H. pylori infection and coronary artery disease, rather than CSX. After this exclusion, 10 articles remained in our study (3, 11–19). The selection process for this meta-analysis is shown in Figure 1. The detailed information of all identified articles is shown in Table 1.
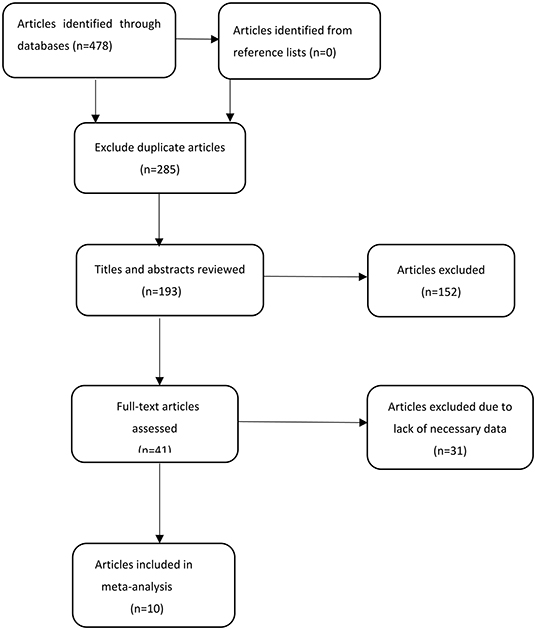
Figure 1. Selection process for articles included in the meta-analysis.
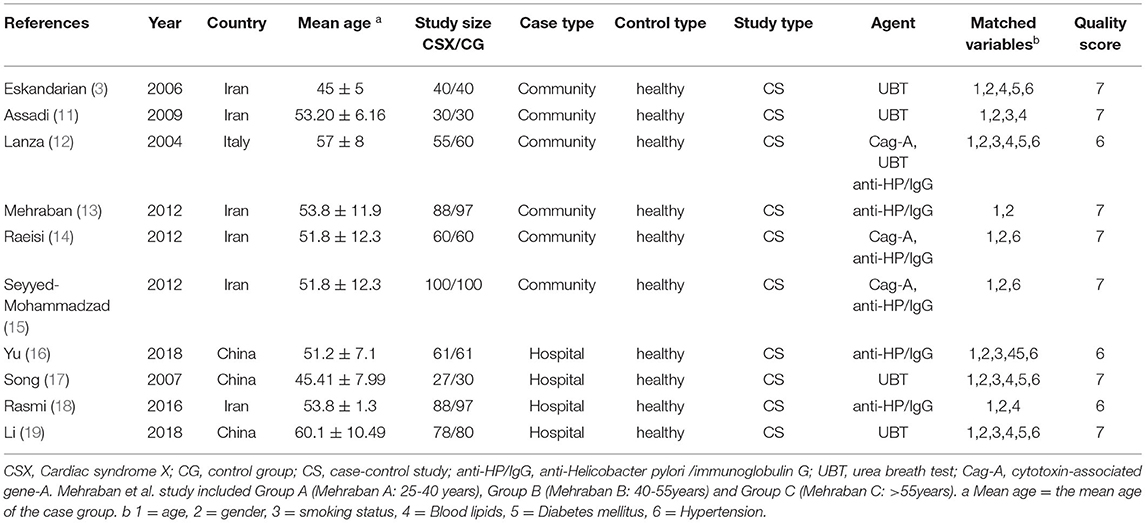
Table 1. Characteristics of studies in the meta-analysis.
We found 10 articles that reported an association of H. pylori infection with the risk of CSX. The combined random effect odds ratio (OR) was 8.29 (95% CI: 4.64–14.82) (Figure 2). After excluding three articles with low scores (six points), seven articles remained. Another meta-analysis showed that the combined fixed effect OR was 9.22 (95% CI: 6.49–13.10) (Figure 3). We also selected seven articles with ≥ four matched variables and performed meta-analysis. The combined random effect OR was 6.06 (95% CI: 2.23–16.43) (Figure 4).
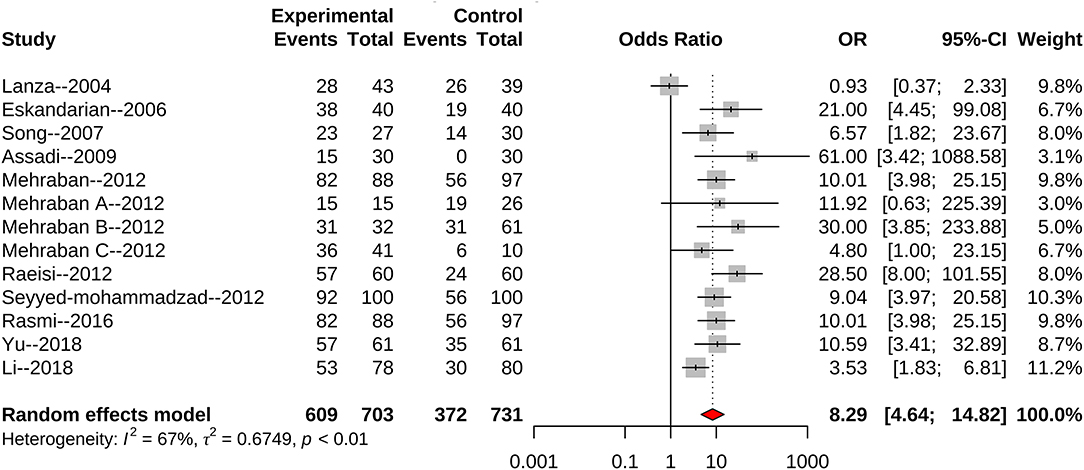
Figure 2. All identified articles evaluating H. pylori infection and the risk of CSX.
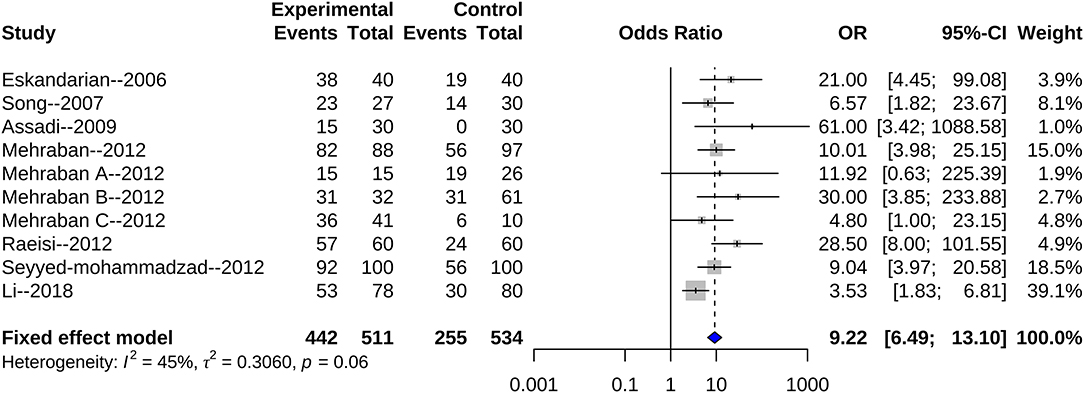
Figure 3. High quality articles evaluating H. pylori infection and the risk of CSX.
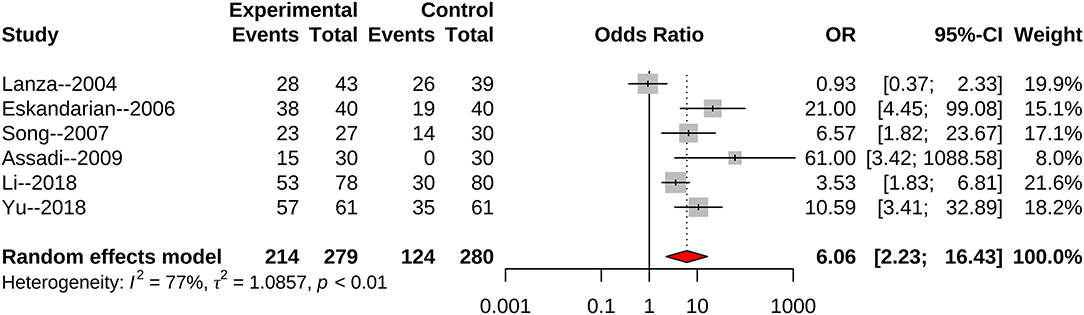
Figure 4. Articles with ≥4 matched variables to evaluate H. pylori infection and the risk of CSX.
The data were separately stratified by country, mean age, case type, H. pylori diagnostic methods, socioeconomic status and publication year. Two parallel meta-analyses were performed in each subgroup. Those results are presented in Table 2. Results suggested that the association of H. pylori infection with the risk of CSX may be much stronger in middle-aged individuals. Similarly, we found that this association is also more common in developing countries (China and Iran), but was not apparent in developed countries (Italy). When we excluded articles with six points, the meta-analysis was performed again. Differences in age and developing countries were still related to bacterial pathogenicity. Whether the articles with six points only or all included articles were analyzed, factors such as age or developing country were consistently observed to influence bacterial pathogenicity.

Table 2. Subgroup analyses about relationship between the risk of CSX and H. pylori infection.
We also found three studies focusing on the association of CagA strain infection with the risk of CSX. The combined random effect OR was 3.29 (95%CI: 0.58–18.55 (Figure 5). Two studies scored seven points, with an OR 7.70 (95%CI: 0.65–91.37). Because of the lack of data, a subgroup meta-analysis of CagA strains could not be performed.
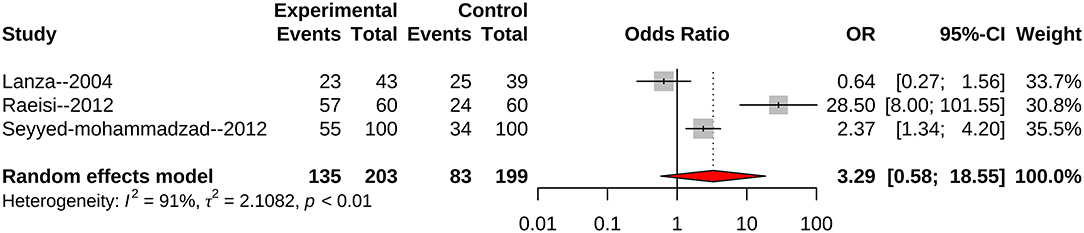
Figure 5. All identified articles evaluating CagA strain infection and the risk of CSX.
As far as we know, the relationship between H. pylori infection and the risk of CSX is still controversial, and our study is the first systematic review and meta-analysis on this topic. Based on the results of our meta-analysis, we estimate that the risk of CSX caused by the bacterial infection increases by ~87%.
The meta-analysis included 10 articles, nine of which found that H. pylori infection increased the risk of CSX. However, one article held the opposite view. Each article in the meta-analysis had a weight range of 3.0–11.2%. Sensitivity analysis was further conducted and concluded that the deletion of any single article would not have a significant impact on the overall effect size (Figure 6). There was significant heterogeneity among included articles, which may be attributable to different study designs and different study populations.
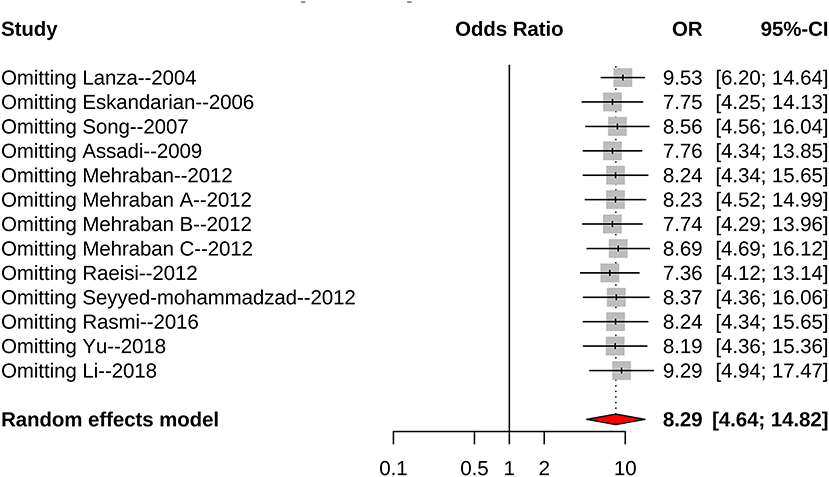
Figure 6. Forest plot for sensitivity analysis.
In the meta-analysis, all articles achieved satisfactory scores (≥ six points) for quality assessment. Included articles with seven points yielded more reliable results, and there was no difference between studies with low scores (six points) and studies with high scores (seven points). We performed Egger's test (P > 0.05) and Begg's test (P > 0.05) and the results suggested no potential publication bias in our meta-analysis, assuring confidence in our results.
Several potential confounding factors, such as age, gender, and socioeconomic status, cannot be ignored because they are associated with H pylori infection and the risk of CSX. Age and gender were matched in all articles. A meta-analysis of articles with ≥ four matched variables was performed and the pooled result did not change. Thus, we believe that these confounding factors are evenly distributed in the control group and the case group. Potential confounding factors had no effect on the reliability of the results.
The meta-analysis showed that CagA-positive bacterial infections may not significantly increase the risk of CSX. However, we believe that this conclusion is controversial for two main reasons: first, CagA-positive strains showed high pathogenicity in a number of diseases including atherosclerotic diseases and peptic ulceration (20, 21). Second, the lack of data may be one reason for conflicting results as only three articles were included. As a result, more well-designed studies should be performed.
According to subgroup results, we found that the association between H. pylori infection and the risk of CSX was age-dependent, and the incidence rate of CSX was likely greater in middle-aged group than in other groups. This finding is similar to those of previous studies, which have shown that the association between the risk of CSX and H. pylori tends to be stronger in middle-aged people (16). We also found some preliminary evidence that the bacteria in developing countries are more pathogenic than in developed countries. Compared with developed countries, the annual recurrence rate of H. pylori in developing countries is higher, which may cause CXS to be more pathogenic (22). Additionally, although the H. pylori-immunoglobulin G (IgG) antibody test cannot indicate current infection and may overestimate the relationship between the bacteria and the risk of CSX, it is consistent with the results obtained by the urea breath test (UBT) test detects current infection.
After excluding low-scoring articles, several meta-analyses were performed, and differences in these subgroups still existed, supporting the reliability of our results. Previous studies have shown that the incidence rate of H. pylori infection was significantly increased with concurrent diseases, such as diabetes and malignant tumors (23, 24). The control group used in our study were all healthy individuals. Therefore, the selection of the control group fully takes into account the differences in H. pylori between the groups.
H. pylori infection is able to cause CSX through a variety of mechanisms. Chronic inflammation caused by infection enhances the risk of vascular disease by increasing some acute reactants and inflammatory mediators, leading to endothelial cell damage and blood coagulation (25, 26). Chronic infection caused by H. pylori infection, especially CagA-positive strains, can lead to continuously elevated inflammatory metabolites, such as the cytokines Interleukin-1 (IL-1), Interleukin-1 (IL-6), and tumor-necrotic factor (TNF-1), which can affect vascular activity and lead to endothelial dysfunction (5, 27). Also, Chronic H. pylori infection can cause a decrease in vitamin B12 and folate absorption, resulting in hyperhomocysteinemia, which promotes the production of intracellular oxygen free radicals and the degradation of nitric oxide, leading to endothelial cell dysfunction (16).
The strength of our study is that it is the first attempt using meta-analysis to identify the association of H. pylori infection with the risk of CSX. However, our study also has some limitations. First, due to lack of data, we mainly obtained the age and country information related to CSX individuals. Other factors we could not account for, such as gender and the instrument for measuring H. pylori, may also affect the accuracy of our results. Second, our study primarily focuses on three countries, which were divided into developed (Italy) and developing (China, Iran). An expansion of this analysis to other countries is needed to further verify our conclusions. Finally, the sample size of this meta-analysis is relatively small, which may affect the accuracy of our results. Therefore, additional, larger, well-designed studies should be encouraged to validate our results.
In conclusion, our meta-analysis suggested a possible association between H. pylori infection and the risk of CSX. Its pathogenicity is stronger in middle-aged individuals and some developing countries. However, more studies are needed to further investigate whether early eradication of H. pylori can reduce the incidence rate of CSX, especially in middle-aged individuals and some developing countries.
The original contributions presented in the study are included in the article/supplementary materials, further inquiries can be directed to the corresponding author/s.
D-HZ, KC, CY, and X-JD designed and analyzed the study. D-HZ, KC, CY, X-JD, and B-BW wrote and revised the manuscript. S-PL, F-HL, Z-XH, and X-LL collected the data. All authors have read and approved the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Kanbay M, Kanbay A, Boyacioglu S. Helicobacter pylori infection as a possible risk factor for respiratory system disease: a review of the literature. Respir Med. (2007) 101:203–9. doi: 10.1016/j.rmed.2006.04.022
2. Oshima T, Ozono R, Yano Y, Oishi Y, Teragawa H, Higashi Y, et al. Association of Helicobacter pylori infection with systemic inflammation and endothelial dysfunction in healthy male subjects. J Am Coll Cardiol. (2005) 45:1219–22. doi: 10.1016/j.jacc.2005.01.019
3. Eskandarian R, Malek M, Mousavi SH, Babaei M. Association of Helicobacter pylori infection with cardiac syndrome X. Singapore Med J. (2006) 47:704–6.
4. Alroy S, Preis M, Barzilai M, Cassel A, Lavie L, Halon DA, et al. Endothelial cell dysfunction in women with cardiac syndrome X and MTHFR C677T mutation. Isr Med Assoc J. (2007) 9:321–5. doi: 10.1007/s00108-007-1833-x
5. Nocente R, Gentiloni N, Cremonini F, Giorgi A, Serricchio M, Santoliquido A, et al. Resolution of syndrome X after eradication of virulent CagA-positive Helicobacter pylori. South Med J. (2000) 93:1022–3. doi: 10.1097/00007611-200010000-00016
6. Jafarzadeh A, Rezayati M T, Nemati M. Specific serum immunoglobulin G to H. pylori and CagA in healthy children and adults (south-east of Iran). World J Gastroenterol. (2007) 13:3117–21. doi: 10.3748/wjg.v13.i22.3117
7. Kato S, Sugiyama T, Kudo M, Ohnuma K, Blaser MJ, Iinuma K et al. CagA antibodies in Japanese children with nodular gastritis or peptic ulcer disease. J Clin Microbiol. (2000) 38:68–70.
8. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. (2009) 62:e1–34. doi: 10.1016/j.jclinepi.2009.06.006
9. Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D et al. Meta-analysis of observational studies in epidemiology (MOOSE): a proposal for reporting. JAMA. (2000) 283:2008–12.doi: 10.1001/jama.283.15.2008
10. Clarke M, Horton R. Bringing it all together: Lancet-Cochrane collaborate on systematic reviews. Lancet. (2001)357:1728. doi: 10.1016/S0140-6736(00)04934-5
11. Assadi M, Saghari M, Ebrahimi A, Pourbehi MR, Eftekhari M, Nabipour I, et al. The relation between Helicobacter pylori infection and cardiac syndrome X: A preliminary study. Int J Cardiol. (2009) 134:e124–5. doi: 10.1016/j.ijcard.2008.01.029
12. Lanza GA, Sestito A, Cammarota G, Grillo RL, Vecile E, Cianci R, et al. Assessment of systemic inflammation and infective pathogen burden in patients with cardiac syndrome X. Am J Cardiol. (2004) 94:40-4. doi: 10.1016/j.amjcard.2004.03.027
13. Rasmi Y, Mehraban K, Sadreddini M, Zeynalzadeh J, Babazadeh H. Lack of significant association between Helicobacter pylori infection and homocysteine levels in patients with cardiac syndrome X. Cardiol J. (2012) 19:466. doi: 10.5603/CJ.2012.0086
14. Rasmi Y, Raeisi S, Mohammadzad M. Association of inflammation and cytotoxin-associated gene A positive strains of Helicobacter Pylori in cardiac syndrome X. Helicobacter. (2012) 17: 116–20. doi: 10.1111/j.1523-5378.2011.00923.x
15. Rasmi Y, Seyyed-Mohammadzad MH. Frequency of Helicobacter pylori and cytotoxine associated gene A antibodies in patients with cardiac syndrome X. J Cardiovasc Dis Res. (2012) 3:19. doi: 10.4103/0975-3583.91597
16. Yu ZY, Lu K, Cheng ZF. Analysis of the correlation between HP infection and blood homocysteine levels and CSX. Zhejiang Clin Med J. (2018) 20:1012–3.
17. Song YH, Dai YG, Cai LA. Association of helicobacter pylori infection with cardiac syndrome X. Chin J Cardiovasc Res. (2007) 5:456–458. doi: 10.3969/j.issn.1672-5301.2007.06.022
18. Rasmi Y, Rouhrazi H, Khayati-Shal E, Shirpoor A, Saboory E. Association of helicobacter pylori infection with cardiac syndrome X. Biomed J. (2016) 39:339–45. doi: 10.1016/j.bj.2016.01.010
19. Li SJ, Zhang LP, Pan LM, Feng J, Wang J, Zou AC, et al. Research on correlation between helicobacter pylori infection? high sensitive C reactive protein and cardiac syndrome X. China Medical Herald. (2018) 15:30–33.
20. Zhang S, Guo Y, Ma Y, Teng Y. Cytotoxin-associated gene-A-seropositive virulent strains of Helicobacter pylori and atherosclerotic diseases: a systematic review. Chin Med J. (2008) 121:946–51. doi: 10.1023/A:1016079505458
21. Atherton JC, Cao P, Peek RM, Tummuru MK, Blaser MJ, Cover TL. Mosaicism in vacuolating cytotoxin alleles of Helicobacter pylori: association of specific vacA types with cytotoxin production and peptic ulceration. J Biol Chem. (1995) 270:17771–7. doi: 10.1074/jbc.270.30.17771
22. Niv Y, Hazazi R. Helicobacter pylori: recurrence in developed and developing countries: meta-analysis of 13 C-urea breath test follow-up after eradication. Helicobacter. (2008) 13:56–61. doi: 10.1111/j.1523-5378.2008.00571.x
23. Roussos A, Philippou N, Gourgoulianis KI. Helicobacter pylori infection and respiratory diseases a review. World J Gastroenterol. (2003) 9:5–8. doi: 10.3748/wjg.v9.i1.5
24. Talebi-Taher M, Mashayekhi M, Hashemi MH, Bahrani V. Helicobacter pylori in diabetic and non-diabetic patients with dyspepsia. Acta Med Iran. (2012) 50:315–8. doi: 10.1080/00365520310001950
25. Luis DA, De Lahera M, Canton R, Boixeda D, Roman AS, Aller R, et al. Association of Helicobacter pylori infection with cardiovascular and cerebrovascular disease in diabetic patients. Diabetes Care. (1998) 21:1129–32. doi: 10.2337/diacare.21.7.1129
26. Liuba P, Pesonen E, Paakkari I, Batra S, Andersen L, Forslid A, et al. Co-infection with Chlamydia pneumoniae and Helicobacter pylori results in vascular endothelial dysfunction and enhanced VCAM-1 expression in ApoE-knockout mice. J Vasc Res. (2003) 40:115–22. doi: 10.1159/000070708
Keywords: Helicobacter pylori infection, Cardiac syndrome X, cytotoxin-associated gene A, meta-analysis, systematic review
Citation: Zhang D-H, Yuan C, Wang B-B, Dong X-J, Lv S-P, Li F-H, Hou Z-X, Liu X-L and Chen K (2022) Helicobacter pylori Infection Maybe a Risk Factor for Cardiac Syndrome X. Front. Cardiovasc. Med. 9:823885. doi: 10.3389/fcvm.2022.823885
Received: 28 November 2021; Accepted: 16 June 2022;
Published: 15 July 2022.
Edited by:
Yong Liu, Guangdong Provincial People's Hospital, ChinaReviewed by:
Khitam Muhsen, Tel Aviv University, IsraelCopyright © 2022 Zhang, Yuan, Wang, Dong, Lv, Li, Hou, Liu and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kang Chen, MTQ0ODYzMjc4OUBxcS5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.