 Georges Jourdi
Georges Jourdi Anne Godier3,4
Anne Godier3,4 Marie Lordkipanidzé
Marie Lordkipanidzé Guillaume Marquis-Gravel
Guillaume Marquis-Gravel Pascale Gaussem
Pascale Gaussem- 1Research Center, Montreal Heart Institute, Montreal, QC, Canada
- 2Faculty of Pharmacy, Université de Montréal, Montreal, QC, Canada
- 3Université de Paris, Innovative Therapies in Haemostasis, INSERM UMR_S1140, Paris, France
- 4Department of Anesthesiology and Critical Care, AP-HP, Université de Paris, Hôpital Européen Georges Pompidou, Paris, France
- 5Faculty of Medicine, Université de Montréal, Montreal, QC, Canada
- 6Service d'Hématologie Biologique, AP-HP, Université de Paris, Hôpital Européen Georges Pompidou, Paris, France
Antiplatelet agents, with aspirin and P2Y12 receptor antagonists as major key molecules, are currently the cornerstone of pharmacological treatment of atherothrombotic events including a variety of cardio- and cerebro-vascular as well as peripheral artery diseases. Over the last decades, significant changes have been made to antiplatelet therapeutic and prophylactic strategies. The shift from a population-based approach to patient-centered precision medicine requires greater awareness of individual risks and benefits associated with the different antiplatelet strategies, so that the right patient gets the right therapy at the right time. In this review, we present the currently available antiplatelet agents, outline different management strategies, particularly in case of bleeding or in perioperative setting, and develop the concept of high on-treatment platelet reactivity and the steps toward person-centered precision medicine aiming to optimize patient care.
Introduction
Antiplatelet therapy, mainly including aspirin (acetylsalicylic acid, ASA) and P2Y12 receptor antagonists, is one of the most prescribed therapies in medicine due to the worldwide high prevalence of cardiovascular diseases (CVD) (1). Antiplatelet agents have significantly improved patient clinical outcomes during the last century, thus preventing a substantial number of atherothrombotic events and decreasing cardiovascular mortality rates. However, secondary bleeding complications remain relatively frequent (2–5). Substantial efforts have been made to develop tools to predict individual ischemic and bleeding risks, to minimize antiplatelet exposure among patients with high bleeding risk and/or low ischemic risk, and to improve percutaneous stent technologies reducing late thrombotic risks. This manuscript provides an overview of the antiplatelet agents currently available, details their management in clinical scenarios such as surgeries and bleeding complications, discusses the consequences of residual high on-treatment platelet reactivity (HTPR), and summarizes the current trends toward patient-centered precision medicine.
Current Arsenal of Antiplatelet Agents
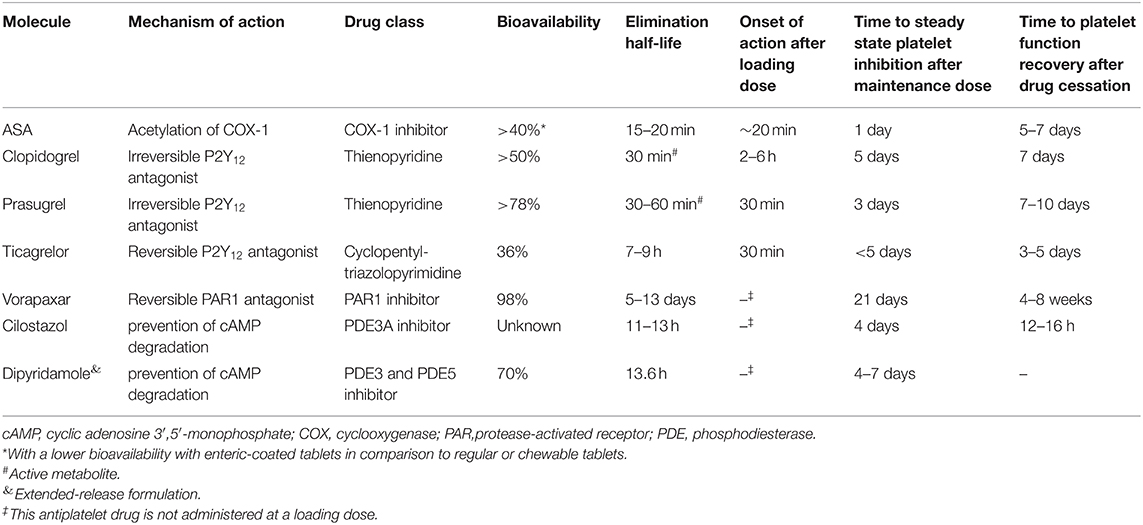
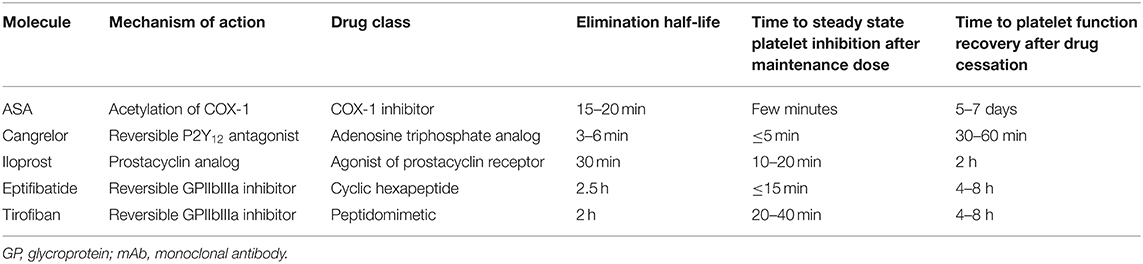
Antiplatelet drugs represent key components of antithrombotic agents, mainly prescribed for the treatment and prevention of atherothrombotic diseases including acute coronary syndromes (ACS), stable coronary artery disease (CAD), peripheral artery disease (PAD), ischemic stroke, and transient ischemic attack (TIA). Antiplatelet agents act either by preventing the formation of second messengers, by interacting with intracellular signaling pathways, by blocking membrane receptors, or by inhibiting platelet aggregation per se (Figure 1). Their main pharmacokinetic/pharmacodynamic characteristics are summarized in Tables 1, 2.
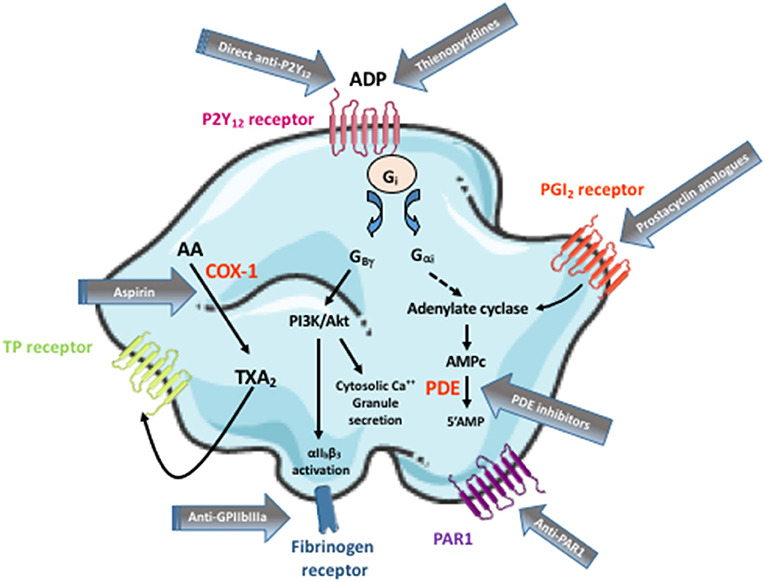
Figure 1. Targets of the commercialized antiplatelet agents. Arachidonic acid (AA) is produced by membrane phospholipids upon the action of phospholipase A2. It is metabolized in cyclic endoperoxydes by the cycloxygenase-1 (COX-1) enzyme, then in thromboxane A2 (TXA2) by the thromboxane synthase. TXA2 activates the Thromboxane Prostanoid (TP) receptor in return. ADP, by activating P2Y12 receptor, induces an inhibition of adenylate cyclase which downregulates cAMP (a powerful platelet inhibitor) synthesis. It also stimulates the phosphoinositide 3-kinase (PI3K) via Gβγ protein complex resulting in Akt stimulation, which activates a number of downstream substrate proteins thereby increasing the cytosolic Ca2+ levels and inducing granule secretion. Inversely, prostacyclin (PGI2) binds to its receptor on platelet surface and increases cAMP intraplatelet level. cAMP is metabolized by phosphodiesterases (PDE) in 5'AMP. Blocking ADP binding site with a P2Y12 receptor antagonist (including thienopyridines and direct anti-P2Y12), stimulating PGI2 receptor or inhibiting PDE maintains cAMP intraplatelet concentration at a high level thus keeping platelets in a resting state. Following coagulation activation, thrombin is generated and cleaves its receptor on platelet surface, i.e., the protease-activated receptor 1 (PAR1), resulting in its activation. TP, P2Y12, or PAR1 activation leads to a conformational change of the glycoprotein (GP)IIbIIIa (also called the integrin αIIbβ3) on platelet surface which links fibrinogen resulting in platelet aggregation. This figure does not aim to represent platelet physiology with the different signaling pathways. It rather illustrates in a very simple manner the targets of the currently available antiplatelet drugs.
Aspirin
ASA reduces the formation of thrombi via irreversible cyclooxygenase (COX)-1 inhibition, thereby suppressing platelet thromboxane A2 (TXA2) synthesis (6). It can be administered intravenously (in Europe) or as an oral loading dose (usually with chewable tablets in North America), in the first phase of ACS treatment, followed by daily maintenance dose, usually with enteric-coated tablets that may be absorbed more slowly and less efficiently in some patients (24). Lysine acetylsalicylate is the only formulation available in some countries that can be administered intravenously. Intravenous lysine acetylsalicylate provided more rapid and consistent platelet inhibition (evaluated by arachidonic acid-induced platelet aggregation measured using light transmission aggregometry) than oral ASA within the first hour after dosing in healthy volunteers (25). In the ECCLIPSE trial, a loading dose of intravenous lysine acetylsalicylate achieved an earlier platelet inhibition with less inter-individual variability than the oral loading dose of ASA (26). However, it has been suggested by some investigators that IV administration of lysine acetylsalicylate may have an acutely negative effect on endothelial vasodilatory prostaglandin production; the clinical impact of this potential endothelial inhibition has not been directly studied in clinical studies. Lysine acetylsalicylate can also be given orally, and was shown to induce fewer gastrointestinal adverse effects than ASA (27) with similar or higher inhibitory effect on light transmission platelet aggregometry in healthy volunteers and CAD patients (28, 29). Considering the limited evidence comparing the effects of intravenous lysine acetylsalicylate and oral ASA on platelet inhibition and endothelial prostacyclin biosynthesis in humans, this remains to be more extensively explored in future clinical studies.
In ACS setting, ASA is indicated in association with a P2Y12 receptor antagonist for 6–12 months depending on the balance between bleeding and ischemic risks (30–32). Dual antiplatelet therapy (DAPT) duration can be extended for up to 3 years in patients at high risk of ischemic events. Afterwards, ASA is recommended indefinitely as a single antiplatelet therapy (SAPT). ASA is also commonly prescribed in patients with stable CAD. It can be associated with clopidogrel for up to 12 months in patients undergoing elective coronary percutaneous intervention (PCI) (31–33). In patients with chronic symptomatic PAD, ASA is commonly prescribed as a long-term SAPT (34, 35). Its efficacy is counterbalanced by concerns of safety thus it is not recommended routinely in primary prevention, but can be considered for higher-risk patients on a case-by-case basis (36–40). ASA can also be prescribed in combination to clopidogrel for up to 90 days in patients with recent (within 30 days) TIA or stroke (41). It can also be prescribed for the secondary long-term prevention of stroke and TIA as a single therapy or in combination with dipyridamole (42, 43).
P2Y12 Receptor Antagonists
The P2Y12 receptor antagonists include two drug classes: the pro-drugs thienopyridines and the direct acting nucleoside–nucleotide derivatives. Clopidogrel is a pro-drug that requires two sequential oxidative reactions involving several CYP enzymes, mainly CYP2C19, to generate the active metabolite (Figure 2). Prasugrel is also a pro-drug. Its active metabolite irreversibly and competitively inhibits adenosine diphosphate (ADP)-induced platelet aggregation faster, more consistently and to a higher degree than clopidogrel (44, 45). Ticagrelor and cangrelor belong to the class of reversible P2Y12 receptor antagonists. While cangrelor is administered intravenously with a binding site at the P2Y12 receptor level not precisely defined (46), ticagrelor is an oral adenosine triphosphate (ATP) analog that binds the P2Y12 receptor at a distinct site from that of ADP. It does not require metabolic activation and achieves a faster, more potent and more predictable antiplatelet effect than clopidogrel (7). Very few studies compared prasugrel to ticagrelor antiplatelet effects. In diabetes mellitus (DM) patients with ACS, ticagrelor achieved a significantly higher platelet inhibition than prasugrel in Alexopoulos et al. (47) study while no difference was observed in Ndrepepa et al. (48) study. In ST elevation myocardial infarction (STEMI) patients undergoing primary PCI, ticagrelor did not show superiority compared to prasugrel in reducing platelet reactivity during the first 24 h (49). A recent meta-analysis compared the effects of prasugrel and ticagrelor on HTPR and low on-treatment platelet reactivity (LTPR) ACS patients. Prasugrel seemed less efficient in lessening the number of HTPR patients (50). However, this should be interpreted with caution since it was only obtained in a limited number of observational studies and case reports. In the light of these few studies (non-exhaustive list), no clear difference on platelet reactivity is reported between prasugrel and ticagrelor.
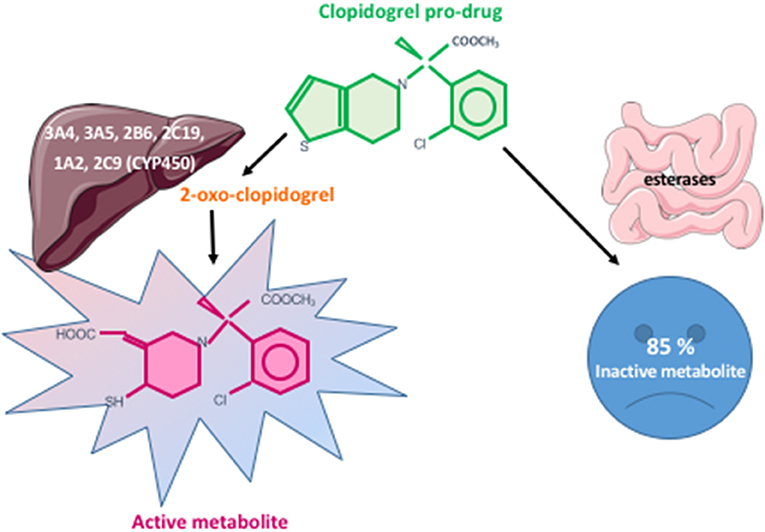
Figure 2. Clopidogrel metabolism pathways. Clopidogrel is a pro-drug. Eighty-five percent of the administered dose is metabolized into an inactive metabolite by intestinal esterases. The remaining 15% undergoes two sequential oxidative reactions involving several CYP enzymes leading, respectively, to 2-oxo-clopidogrel then to the active metabolite.
Ticagrelor is metabolized mainly by CYP3A4 to an active metabolite that represents 30–40% of circulating active drug. Additionally, ticagrelor inhibits adenosine reuptake via a membrane-bound channel called the type 1 equilibrative nucleoside transporter (ENT1) in erythrocytes and platelets, which might potentiate its antiplatelet effect (51). Ticagrelor is indicated in association with ASA in medically-managed ACS patients. Both prasugrel and ticagrelor are preferred over clopidogrel in ACS patients undergoing PCI, but prasugrel is contra-indicated in patients with a prior stroke or TIA. Prasugrel is associated with a significantly lower risk of CV events compared with ticagrelor in ACS patients planned for invasive therapy (52). It could be preferred over ticagrelor post-PCI in non-ST elevation (NSTE) ACS patients (53). Clopidogrel may be a favorable alternative to ticagrelor or prasugrel in NSTE-ACS patients aged 70 years or older because of the higher bleeding risk (54). A recent meta-analysis of six trials (DACAB, GLASSY, SMART-CHOICE, STOP-DAPT 2, TICO, and TWILIGHT) revealed that P2Y12 receptor antagonist monotherapy was associated with a similar risk of fatal and ischemic events and lower rates of major bleeding compared with DAPT in patients undergoing coronary revascularization particularly among females. ASA could thus be stopped 1–3 months after coronary revascularization and P2Y12 receptor antagonist monotherapy continued instead of DAPT, especially in women (55). However, no formal proposal has yet been published. In ACS patients undergoing urgent PCI and not pre-treated with an oral P2Y12 receptor antagonist, cangrelor might be an interesting therapeutic option (56). It can also be used in those who require DAPT bridging before surgery (57). Clopidogrel can also be prescribed as part of triple antithrombotic therapy [in association with ASA and an oral anticoagulant (OAC)] (31, 58, 59) in patients with atrial fibrillation suffering from ACS. Triple therapy is used during index hospitalization or up to 1 or 6 months (depending on patient ischemic and bleeding risks). It is followed by dual antithrombotic therapy (P2Y12 receptor antagonist plus OAC) for 1 year after coronary stenting then by an OAC indefinitely. While clopidogrel is commonly prescribed as part of the dual antithrombotic therapy, prasugrel is allowed in the Japanese guidelines (60) and ticagrelor might be an alternative to clopidogrel in patients with high ischemic and low bleeding risks according to the American and European guidelines (61, 62). In patients with mechanical heart valves undergoing PCI, a daily dose of clopidogrel in addition to vitamin K antagonist is indicated following an initial period of triple therapy (up to 6 months) (63). Prasugrel and ticagrelor are preferred over clopidogrel in DM patients with CVD necessitating DAPT, due to increased platelet reactivity seen at baseline and on-treatment in diabetic patients (4, 64–67).
Clopidogrel is the only P2Y12 receptor antagonist approved in association with ASA for 3–6 months in CAD patients undergoing elective PCI (31–33). It is also a good alternative for stroke and TIA prevention in patients with frequent headaches secondary to ASA/dipyridamole combination (43, 68).
GPIIbIIIa Inhibitors
GPIIbIIIa inhibitors are intravenous antiplatelet agents that block the association of fibrinogen and von Willebrand factor (VWF) to the glycoproteins (GP) on the platelet surface. Abciximab was the first agent of this class, but it was withdrawn from the pharmaceutical market in 2019 following the interruption of its production by Janssen laboratories. Tirofiban is a non-peptide derivative of tyrosine mimicking the fibrinogen binding sequence within GPIIbIIIa while eptifibatide is a cyclic heptapeptide. Both are small molecules that inhibit GPIIbIIIa in a competitive manner with a stoichiometric ratio > 100:1 (69, 70). They are currently mainly considered as a bailout therapy in the event of angiographic evidence of a large thrombus, slow- or no-reflow, and other thrombotic complications in STEMI patients undergoing PCI or in NSTE-ACS patients undergoing high-risk PCI without pre-treatment with oral P2Y12 receptor antagonists (33).
PAR1 Antagonist
Vorapaxar is an oral reversible PAR1 antagonist (71) that was approved by the Food and Drug Administration (FDA) in 2014. It has not yet gained the European Medicines Agency (EMA) approval (8). It is very rarely prescribed on top of standard antiplatelet therapy for secondary prevention in patients with a history of myocardial infarction or symptomatic PAD without any history of stroke, TIA or intracranial hemorrhage (72–74).
Other Agents: Phosphodiesterase Inhibitors and Analog of Prostacyclin
Iloprost is a stable analog of prostacyclin (PGI2) that activates adelylate cyclase to increase intraplatelet cAMP level. It is also an arterial vasodilator which increases its therapeutic value for systemic administration in patients with severe PAD but increases the risk of hypotension (75). Dipyridamole is another antiplatelet agent that increases cAMP level within platelets by inhibiting its degradation by phosphodiesterase (PDE)3 and PDE5 (9, 76). It also induces endothelial synthesis and release of PGI2 (77, 78) and raises the extracellular levels of adenosine by inhibiting its reuptake by red blood cells and scavenges peroxy radicals, thus preventing vascular and tissue damage (76). It is worth mentioning that anticipated pharmacodynamics of both iloprost and dipyridamole should strictly match their pharmacokinetics. Dipyridamole is usually used in association with ASA for the secondary long-term prevention of stroke and TIA as previously mentioned.
Cilostazol is a selective inhibitor of PDE3A (the main subtype of PDE3 expressed in platelets) preventing the degradation of cyclic adenosine 3′,5′-monophosphate (cAMP) and to a lesser degree of cyclic guanosine 3′,5′-monophosphate (cGMP) thus resulting in an increase in the active forms of protein kinase A (PKA) and PKG. It also inhibits adenosine uptake and has a vasodilatory effect by relaxing the vascular smooth muscle cells (10). Cilostazol is recommended for the treatment of patients with intermittent claudication in the absence of tissue necrosis or rest pain (10). In the light of CSPS, CSPS2 and CASISP trials (79–81), it may also be used for secondary stroke prevention, particularly in Asian patients (82). Randomized trials are still needed to determine its usefulness for the secondary stroke prevention in non-Asian populations.
Switching Between Antiplatelet Agents
Switching strategies between oral P2Y12 depends on the clinical setting (Figure 3). In the acute setting, switching to prasugrel or ticagrelor can occur irrespective of prior clopidogrel dosing and timing, whereas deescalation to clopidogrel should occur at 24 h from the last prasugrel or ticagrelor dose. Transitions between prasugrel and ticagrelor should also occur at 24 h from the last dose (46, 83) except in the Canadian guidelines, which advise a transition from ticagrelor to prasugrel 12 h after the last dose of the former in ACS setting (58). In the chronic setting, a loading dose is recommended at 24 h from the last dose when transitioning from ticagrelor to prasugrel or clopidogrel to avoid drug-to-drug interactions limiting the antiplatelet effect (46, 83).
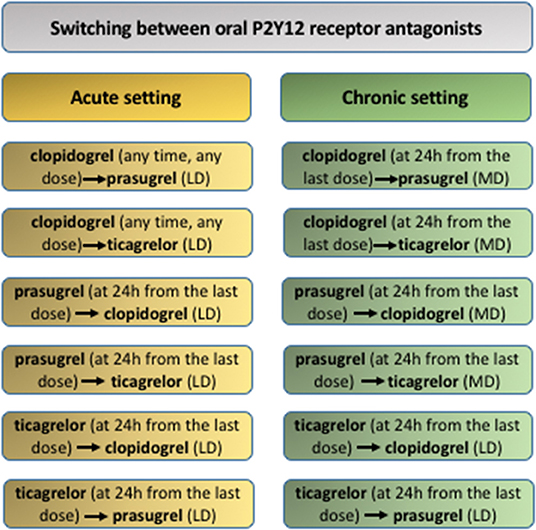
Figure 3. Switching strategy between oral P2Y12 receptor antagonists. LD, loading dose; clopidogrel LD = 600 mg; prasugrel LD = 60 mg; ticagrelor LD = 180 mg. MD, maintenance dose; clopidogrel MD = 75 mg q.d.; prasugrel MD = 10 mg q.d.; ticagrelor MD = 90 mg b.i.d.
Transition from cangrelor to oral P2Y12 receptor antagonists requires loading doses of clopidogrel and prasugrel to be administered immediately after the end of the cangrelor infusion to avoid drug interactions (46). Indeed, cangrelor blocks the binding of thienopyridine active metabolites on P2Y12 receptor, impairing their antiplatelet effect (83). On the contrary, ticagrelor can be administered before, during or after the cangrelor infusion (ideally within the last hour of the cangrelor infusion) without significant drug interactions (84).
Peri-Operative Management of Antiplatelet Agents
Each year, 4–8% of patients receiving long-term antiplatelet therapy require major surgery (85). Peri-operative management of antiplatelet drugs is challenging since their continuation increases the risk of peri-procedural bleeding while their discontinuation increases the risk of thrombotic events. Moreover, delaying surgery can be detrimental in many cases including malignant and vascular diseases. Several factors should therefore be considered depending on whether the surgery is elective, urgent, associated with a high or low bleeding risk, or necessitates neuraxial anesthesia.
Elective Surgery
The management of antiplatelet drugs is based on their indication and the procedure, particularly whether it is an elective cardiac or non-cardiac surgery. The risk of bleeding related to non-cardiac procedure can be divided into high, moderate, and low categories depending on the possibility of performing the procedure in patients receiving antiplatelet agents (none, SAPT or DAPT). Evaluation of the procedure-related bleeding risk also includes the type of anesthetic technique selected. POISE-2 study has suggested that administration of ASA before surgery and throughout the early postsurgical period had no significant effect on the rate of death or non-fatal myocardial infarction but increased the risk of major bleeding (86). However, continuation of ASA therapy is in general advocated in patients having stent. It could also be continued around the time of most elective non-cardiac surgeries since there are not many high bleeding risk procedures except complex hepato-biliary surgeries, open thoracic and thoraco-abdominal vascular surgeries, spinal, and intracranial surgeries (85, 87). Otherwise, a joint-decision making with the patient is suggested depending on baseline ischemic and bleeding risk. If the procedure requires discontinuation of antiplatelet therapy, the last intake of ASA, clopidogrel, ticagrelor, and prasugrel 3, 5, 5, and 7 days before surgery, respectively, is proposed (Table 3) (88). In case of intracranial surgery, 2 additional days free of antiplatelet therapy should be considered.
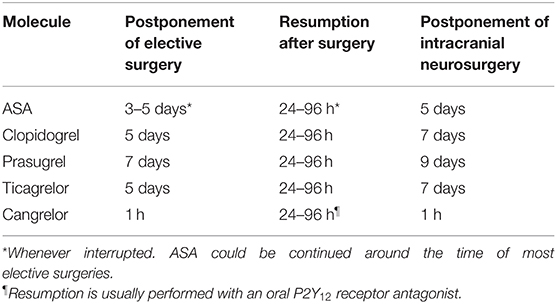
Table 3. Perioperative management of antiplatelet drugs in case of elective non-cardiac surgery.
The thrombotic risk associated with discontinuation should be assessed according to each specific indication of antiplatelet therapy: the risk is lower for patients receiving SAPT for CV prevention, for secondary stroke prevention or for lower extremity arterial disease than for those receiving DAPT following PCI (89). The risk is even higher for patients with a recent history of myocardial infarction or stent implantation as non-cardiac surgery exposes to an increased risk of stent thrombosis during the first few weeks, especially if both oral antiplatelet agents have to be discontinued due to a high procedure bleeding risk (31, 90). Thus, for patients with stent, procedures should be postponed until completion of DAPT if possible, and at least 1 month after implantation of drug-eluting stent (DES) when surgery should be rapidly performed (31, 58, 90, 91). If surgery is performed within the first month after DES implantation anyway, preoperative bridging therapy could be considered, using cangrelor or GPIIbIIIa inhibitors. GPIIbIIIa inhibitors should be started 2 days after stopping DAPT and stopped 6 h before surgery (12 h if creatinine clearance is <60 mL/min) (92), whereas cangrelor should be introduced 24 h after the last intake and stopped 1 h before the procedure. Resumption of P2Y12 receptor antagonists is recommended 24–96 h post-operatively and ideally within 48 h in patients with recent (<6 weeks) PCI or who presented with ACS (Table 3) (31).
ASA should be continued throughout the perioperative period in all patients requiring elective cardiac surgery. To minimize the risk of bleeding in patients under DAPT, a minimum interruption of ticagrelor and clopidogrel for 48–72 h (ideally for 5 days) and of prasugrel for 5 days (ideally for 7 days) is suggested in the Canadian guidelines (58). The European Society of Cardiology (ESC) and the Japanese Circulation Society (JCS) recommend a minimum interruption for 3, 5, and 7 days, respectively (33, 91). P2Y12 receptor antagonists should be resumed post-operatively as soon as it is deemed safe (32, 33, 58).
Non-elective Invasive Surgery
In case of non-elective invasive procedure, management of oral antiplatelet drugs is based on their pharmacokinetic/pharmacodynamics parameters, the degree of urgency of the procedure and the associated bleeding risk. Platelet function testing may be considered to guide this management, but no evidence-based method has been approved for this indication (93, 94). When the bleeding risk induced by antiplatelet drugs may worsen the prognosis, measures should be taken to neutralize these drugs (95). ASA and thienopyridines, namely clopidogrel and prasugrel as well as their active metabolites, have short half-lives and bind irreversibly to their targets, thus exhibit inhibitory effects that last for the platelets' lifetime. Consequently, transfusion of a sufficient number of normal platelets should enable hemostasis by replacing the inhibited platelets (88). Administration of 0.7 × 1011 platelets/10 kg of body weight produces a rise in platelet count of ~40 × 109/L (96). It is worth mentioning that the average size of a pool of platelets varies between countries and institutions. The above-mentioned dose is recommended in situations requiring neutralization of ASA while a higher dose is proposed for patients receiving clopidogrel or prasugrel (double for the former and even higher for the latter) (95). Neutralization of ticagrelor is more challenging due to its longer half-life along with that of its active metabolite compared to ASA, clopidogrel, and prasugrel. Consequently, circulating active compounds inhibit transfused platelets for at least 24 h after the last ticagrelor intake (97, 98). Beyond 24 h, platelet transfusion might be beneficial (88, 99). When the procedure must be performed within 24 h after the last intake, no therapeutic option could be recommended. When possible, postponing non-elective invasive procedures at least for a few hours or even a few days should be considered. Recombinant factor VIIa has been proposed to neutralize ticagrelor but its clinical efficacy has not been evaluated and it exposes to a thrombotic risk (100). Tranexamic acid is an option as it may reduce bleeding whether the patient has received antiplatelet drugs or not (101, 102). In April 2019, bentracimab (PB2452) received a breakthrough therapy designation from the FDA as a potential specific antidote for ticagrelor. It is a monoclonal antibody fragment that binds ticagrelor and its active metabolite with an affinity 100-fold higher than their affinities to P2Y12 receptor (103). It has completed a phase 1 clinical trial and further studies are awaited (104).
Regional Anesthesia
Spinal epidural hematoma is a devastating complication of central neuraxial anesthesia, which includes spinal anesthesia and epidural with or without catheters. The risk of spinal hematoma related to ASA appears very low (105, 106), thus ASA is not a contraindication to neuraxial anesthesia if the benefit-risk ratio is favorable. The P2Y12 receptor antagonists carry a greater risk of bleeding than ASA, therefore neuraxial anesthesia is contraindicated in patients on clopidogrel, prasugrel or ticagrelor, unless those antiplatelet agents were discontinued 5, 7, and 5 days before the procedure, respectively, according to the French recommendations (88). In parallel, the American Society of Anesthesia and Regional Pain Medicine recommends a 5-days discontinuation period for all oral P2Y12 receptor antagonists (107). The insertion of an epidural catheter makes the management of antiplatelet agents more complex. Catheter manipulation and removal carry similar risks to insertion and the same rules should apply. The use of an epidural catheter should not compromise the postoperative resumption of antiplatelet agents, especially of P2Y12 receptor antagonists and DAPT. The benefit of the catheter should thus be carefully balanced with the thrombotic risk of delaying resumption (107).
Peripheral nerve blocks can be divided into two groups according to the degree of bleeding risk. Peripheral nerve blocks associated with a high bleeding risk follow the same rules as neuraxial anesthesia. They include deep blocks such as the para-sacral sciatic block, posterior lumbar plexus block, infraclavicular block, etc. On the contrary, peripheral nerve blocks associated with low bleeding risk could be performed in patients on SAPT or DAPT. Those blocks include superficial blocks such as the axillary block, popliteal sciatic block, femoral block, etc.
Management of Bleeding Associated With Antiplatelet Therapy
Bleeding associated with antiplatelet drugs is heterogeneous thus no one course can be universally recommended. Several characteristics should be considered: type of bleeding (spontaneous vs. associated with trauma or injury), location and intensity of bleeding, type of antiplatelet therapy, time-interval since the last intake, etc. Combination of antiplatelet drugs or the use of the more-potent P2Y12 receptor antagonists (ticagrelor or prasugrel) are associated with an increased risk of hemorrhagic complications in comparison to ASA or clopidogrel monotherapy (5). In all cases, etiological and symptomatic treatment of bleeding is essential. Conventional hemostatic means include mechanical (embolization, endoscopy, compression, surgery, etc.) and resuscitation measures (fluids, red blood cells, plasma and/or factor concentrates administration, prevention of hypothermia, etc.). If hemostatic measures are not sufficient to stop the bleeding, neutralization of antiplatelet therapy could be considered taking into account the type of antiplatelet drug, the time-interval since the last intake, the ischemic risk of the patient and the characteristics of the bleeding event (site, severity). Practical guidelines for the bleeding management in patients on antiplatelet therapy are mainly based on expert opinion since no solid clinical evidence are available. They could be summarized as followed.
Gastrointestinal Hemorrhage
Gastrointestinal hemorrhage is the most frequent bleeding complication associated with antiplatelet agents. Gastrointestinal bleeding secondary to ASA therapy is dose-related (42) most probably linked to the inhibition of COX-2 (and COX-1) in the endothelial cells lining the stomach, which suppresses cytoprotective PGE2 production. A meta-analysis of adverse events of low-dose ASA in 14 randomized controlled trials reported a modest annual absolute rate of 0.12%/year, slightly higher than that induced by clopidogrel (2, 108). Prasugrel and ticagrelor are associated with a higher rate compared to clopidogrel (3, 4). This rate is estimated at 1.3–4.6%/year with the DAPT combining ASA and clopidogrel (109). Endoscopic control of bleeding is recommended for patients suspected to have upper gastrointestinal hemorrhage (110). Proton pump inhibitors are recommended in all patients as they improve outcomes in acute bleeding and prevent upper gastro-intestinal re-bleeds in patients continuing SAPT or DAPT (111–113). Moreover, proton pump inhibitors are also recommended in patients with a history or an increased risk of gastrointestinal bleeding, including the elderly and patients with concomitant use of vitamin K antagonists, steroids, and nonsteroidal anti-inflammatory drugs. Nevertheless, their routine use for patients at low risk of gastrointestinal bleeding is not recommended (31, 32). The choice of the proton pump inhibitor should take into account the degree of inhibition of CYP2C19, particularly in patients receiving clopidogrel. Omeprazole has been shown to reduce platelet inhibition ex vivo in the OCLA study (114), however, no significant increase in CV events was noted in patients treated with clopidogrel and omeprazole in the COGENT trial (115). Pantoprazole and esomeprazole appear to be safe alternatives (116), while lansoprazole might impair platelet inhibition in patients receiving clopidogrel (117). In case of severe bleeding, the benefit of platelet transfusion has been poorly assessed (111, 118). It should thus be reserved to specific severe cases after failure of etiological and symptomatic treatments (95, 119).
The dilemma of if and when antiplatelet agents should be reintroduced following gastrointestinal bleeding persists since randomized trials are lacking. Consequently, practice is variable and not necessarily evidenced-based. As such, in patients under secondary prophylaxis, there is a clear benefit in restarting antiplatelet therapy. When the risk of re-bleeding is low, single agent ASA can be continued without interruption, especially when endoscopic control has been achieved. When bleeding risk is high, ASA should be withheld but reintroduced early (within 3–7 days) as outlined in the recent review by Scott et al. (120). For patients receiving DAPT, particularly following recent cardiac stent insertion, ASA should be continued and the reintroduction of the second antiplatelet agent should be discussed with the cardiologist (99).
Intracranial Hemorrhage
Conflicting results were reported on the association between ASA use and the risk of intracranial hemorrhage or cerebral microbleeds (121–124). More information may be generated from the ongoing ASPREE-NEURO study (125). Prasugrel and ticagrelor were associated with more intracranial hemorrhage compared to clopidogrel in the TRITON-TIMI 38 and PLATO trials, respectively. Prior stroke or TIA and previous intracranial hemorrhage are contraindications to prasugrel. Ticagrelor should be used with precautions in this context (4, 7). Alike, vorapaxar is contraindicated in patients at high risk of intracranial hemorrhage (8). That said, once intracranial hemorrhage occurs, antiplatelet therapy worsens the prognosis.
Efficacy of platelet transfusion in this case depends on many factors including the type of the drug, the time from the last drug intake and from the hemorrhage, the site of bleeding and the mechanism (spontaneous vs. traumatic). The required dose and the optimal timing of delivery relative to the last dose of antiplatelet agent remain uncertain. Platelet transfusion is recommended in treated patients suffering from intracranial hemorrhage and requiring urgent neurosurgery (121). Guidelines also propose platelet function testing prior to transfusion when possible (95). In non-surgical settings, platelet transfusion efficacy is not recommended to neutralize ASA (121) since the PATCH study reported worsened outcomes post-transfusion in patients on ASA as monotherapy and presenting supratentorial intracerebral hemorrhage with Glasgow Coma Scores ≥ 8 on admission (126). No study has assessed yet the effect of platelet transfusion in patients presenting intracranial hemorrhage with altered consciousness or in cases of treatment by P2Y12 receptor antagonists, thus no formal recommendation could be proposed.
Hemorrhagic Shock
Platelet function recovery is essential and critical in case of hemorrhagic shock in patients under antiplatelet therapy. Neutralization of antiplatelet drugs is therefore usually proposed (88, 127, 128).
Non-severe Bleeding
Non-severe bleeding complications only require symptomatic treatment without neutralizing or discontinuing antiplatelet therapy, along with the re-evaluation of the indication for antithrombotic treatment.
High On-Treatment Platelet Reactivity and Precision Medicine
Numerous studies have demonstrated substantial interpatient variability in the responsiveness to antiplatelet therapy, based on clinical outcomes and/or laboratory methods used to assess platelet reactivity. It is critically important to note that true pharmacological resistance, i.e., non-response, to antiplatelet therapy is extremely rare. In most cases, HTPR cannot be directly pinpointed to a pharmacological mechanism (such as a mutation of the drug targets or alteration of the prodrug bioactivation, etc., cf infra). Notwithstanding, high residual on-treatment platelet reactivity either on ASA or on DAPT is a negative prognostic factor for the occurrence of future CV events, once drug interactions and non-compliance have been ruled out. Similarly, LTPR is associated with increased risk of bleeding, making the selection of the intensity and duration of antiplatelet therapy for individual patients a clinical challenge. A tailored personalized therapeutic approach, particularly on the basis of a better stratification of the individual risk profile and the evolution in stent technology, in pharmacogenomics and in laboratory assays used to evaluate platelet reactivity, would be beneficial.
Scores Predicting Individual Ischemic and Bleeding Risk
Many scores and risk stratifying models have been developed to help tailor antiplatelet therapy with the aim to maximize ischemic protection and minimize bleeding risk, although an increasing body of evidence suggests that ischemic and bleeding risks are dynamic, fluctuating in time, and depending on patient characteristics, including ethnicity. For instance, East Asian patients have a lower rate of ischemic events after PCI compared to Caucasian patients while their bleeding risk is higher (129). A standardized definition of high bleeding risk has been recently proposed by consensus by the Academic Research Consortium for high bleeding risk (ARC-HBR) and validated in ACS or CAD patients undergoing PCI. It includes advanced age, anemia, thrombocytopenia, liver cirrhosis, use of oral anticoagulation, steroids or non-steroidal anti-inflammatory drugs, chronic kidney disease, history of spontaneous bleeding, stroke or active malignancy, chronic bleeding diathesis, planned surgery and trauma or surgery within 30 days before PCI (130). The PRECISE-DAPT score helps predicting bleeding events at 1 year in patients having completed successful PCI and requiring DAPT. This score evaluates five items namely age, creatinine clearance, hemoglobin, white blood cell count, and history of bleeding (131). Very recently, Pelliccia et al. (132) showed that the risk of bleeding changes over time in a substantial proportion of patients on DAPT after PCI. Frequent evaluation and recalculation of the PRECISE-DAPT score might therefore offset the excess bleeding associated with long DAPT in patients with comorbidities. Four other scores, namely DAPT, PARIS, CALIBER, and CREDO Kyoto scores, stratify both ischemic and bleeding risks (133–136). Patients with acute activation of the atherosclerotic process (ACS, ischemic stroke or TIA, and acute limb ischemia), extended diffuse atherosclerotic disease (PAD, diffuse coronary atherosclerosis, aortic, and carotid plaques), high burden of risk factors (current smoking habit, DM, and systemic arterial hypertension) and/or comorbidities (low ejection fraction, i.e., <30%, heart congestive disease, previous myocardial infarction and previous PCI) are particularly at higher risk of ischemic complications (133). Several other risk assessment models have also been proposed in the TRA 2P-TIMI 50, ADAPT-DES, HORIZON AMI, TRILOGY ACS, and CRUSADE trials (137–142). Of note, these scores and risk-predicting models still need to be tested in prospective randomized controlled trials to verify their real predictive values in guiding antiplatelet therapy especially that their discrimination ability in retrospective validation studies is at best moderate-to-good (143, 144).
Choice of Stent Type
Individualization of antiplatelet therapy should also consider the stent type. Thrombotic risk of any stent type is highest initially and decreases over time but is never null. Bare metal stents (BMS) were associated with high rate of repeat revascularization because of restenosis (145). First generation DES (eluting paclitaxel or sirolimus) were subsequently developed to reduce this risk. However, they are associated with a higher risk of late and very late in-stent thrombosis compared to BMS. Thus, long-term DAPT was recommended (146). Unlike bioresorbable scaffolds, second-generation DES (zotarolimus, ridaforlimus, and everolimus) confer a lesser in-stent thrombotic risk, concentrated during the first 30 days (31, 147) enabling reduction of the DAPT duration. Compared to the first-generation DES, they have less bulky struts, use less thrombogenic polymers and provide better kinetics of drug release which explains the widespread preference for second-generation DES over the others. Moreover, guiding stent implantation using meticulous intravascular images decreases the thrombotic risk (148). Continuous development in stent technology will undoubtedly provide new perspectives in the contemporary use of antiplatelet therapy. Further well-designed studies are necessary to explore safe antiplatelet scenarios with newer generation stents.
Pharmacogenomics of Antiplatelet Therapy
Although the cause of the variability in antiplatelet therapy efficacy is likely to be multifactorial, a substantial part is attributed to genetic etiology. The study of pharmacogenomics presents the possibility of individualized optimization of antiplatelet therapy tailored to each patient's unique genetic traits. ASA and clopidogrel are the most studied antiplatelet agents regarding genetic polymorphisms. Some genetic variants in COX-1 and 2 proteins (PTSG1 and PTSG2 genes), in P2RY1 receptor gene, or in some platelet GP such as the integrin α2/β1 (GPIaIIa), a platelet collagen receptor encoded by ITGA2 gene, or the IIIa subunit of GPIIbIIIa receptor (ITGB3 gene) (149, 150) have been reported to be associated with HTPR. However, the clinical outcomes in patients carrying these variants have not robustly demonstrated lesser clinical benefit from ASA therapy.
The strongest genetic associations for platelet responses to clopidogrel are with the CYP responsible for its bioactivation, most notably CYP2C19. The pharmacological importance of CYP2C19 genotypes in clopidogrel therapy has been first described in healthy volunteers (151) then extensively studied in various patient groups. This enzyme is highly variable in the general population with at least eight alleles of various levels of activity that could be classified into 4 categories (152, 153): (i) extensive metabolizer having wild type fully functional allele (*1) with a prevalence of 69.5% in the general population; (ii) poor metabolizer carrying two loss-of-function alleles (*2–*9) with *2 (rs4244285, c.681G>A) having a minor allele frequency (MAF) of ~12–15, 15–18, and 25–30% in European, African, and Asian populations, respectively; (iii) intermediate metabolizer carrying one loss-of-function allele plus one functional or increased-activity allele; and (iv) ultra-rapid metabolizer having at least one increased-activity allele [*17 (rs12248560, −608C>T) having a MAF of ~20% in European and Black populations and 5% in Asian populations] (152, 154, 155). These genetic variants might significantly affect clopidogrel metabolism thus its active metabolite plasma concentrations modifying therefore the risk of ischemic and bleeding complications (153, 156, 157). Indeed, poor active metabolite production and ensuing HTPR on clopidogrel can be overcome by increasing the dose of clopidogrel in heterozygous carriers of the loss-of-function allele (namely the CYP2C19*2) but not in homozygous carriers as was previously shown in the CLOVIS and CLOVIS-2 studies (158, 159).
Prasugrel and ticagrelor are sensible alternatives among patients with loss-of-function genetic variants since their pharmacokinetics, antiplatelet effects and clinical effectiveness are less, if at all, impacted by CYP2C19 genotype (156, 160). Of note, genetic variants associated with reduced clinical effectiveness of prasugrel and ticagrelor have not been identified to date. Similarly, while patients with increased CYP2C19 activity, such as *17 homozygotes, have been shown to exhibit increased response to clopidogrel (161) a recent study failed to show any clinical impact of the *17 variant in patients treated by clopidogrel (162).
Besides, genetic variants in ABCB1 and CYP enzymes (CYP3A4*1G, CYP3A5*1, and CYP3A5*3) genes have been investigated for their impacts on clopidogrel pharmacokinetic profile, however, heterogeneous outcomes are reported and more studies are required to draw clear conclusions of their importance (163, 164).
Most genetic intervention studies have thus targeted the CYP2C19 polymorphism for personalized antiplatelet approaches, and some have shown promise, including PHARMCLO, POPular Genetics and TAILOR-PCI trials (157, 165, 166). While the recent ESC guidelines do not make recommendations regarding CYP2C19 genotyping (167), the American College of Cardiology/American Heart Association (ACC/AHA), and the Society for Cardiovascular Angiography and Interventions (ACCF/AHA/SCAI) PCI guidelines state that CYP2C19 genetic testing may be considered in patients undergoing PCI who are at high risk of poor outcome due to inadequate platelet inhibition (168). In the setting of acute ischemic stroke, TIA and cerebrovascular intervention, prospective data characterizing the impact of a CYP2C19 genotype-guided anti-P2Y12 therapy selection strategy on adverse neurological, vascular and bleeding outcomes are still needed. No recommendations regarding the use of CYP2C19 testing were issued either by the American Stroke Association (169) or the European Stroke Organization (170).
Laboratory Assessment of Antiplatelet Therapy
While some trials suggested positive impact of personalized antiplatelet therapy based exclusively (i.e., without relying on pharmacogenomics data) on platelet function testing (MADONNA, ISAR-HPR, TROPICAL-ACS, CREATIVE, and Aradi et al.) (171–175), others have failed to show benefit (ARCTIC, ANTARCTIC, TRIGGER-PCI, and GRAVITAS) (176–179) (Table 4). Discrepancies could be explained, at least partly by study design, selected patient populations, timing of platelet function, antiplatelet therapy strategies, and evaluated assays. That said, platelet function testing in treated patients is currently not recommended in routine clinical practice by either ACC/AHA or ESC. However, it may be considered in selected patients at high ischemic risk leading to poor clinical outcomes or with variable therapeutic observance. According to the 2018 ESC guidelines for myocardial revascularization, de-escalation of P2Y12 receptor antagonists based therapy (e.g., from prasugrel to clopidogrel in patients with normal clopidogrel platelet inhibition response) guided by platelet function testing may be considered, particularly in ACS patients unsuitable for 12-month DAPT (33).
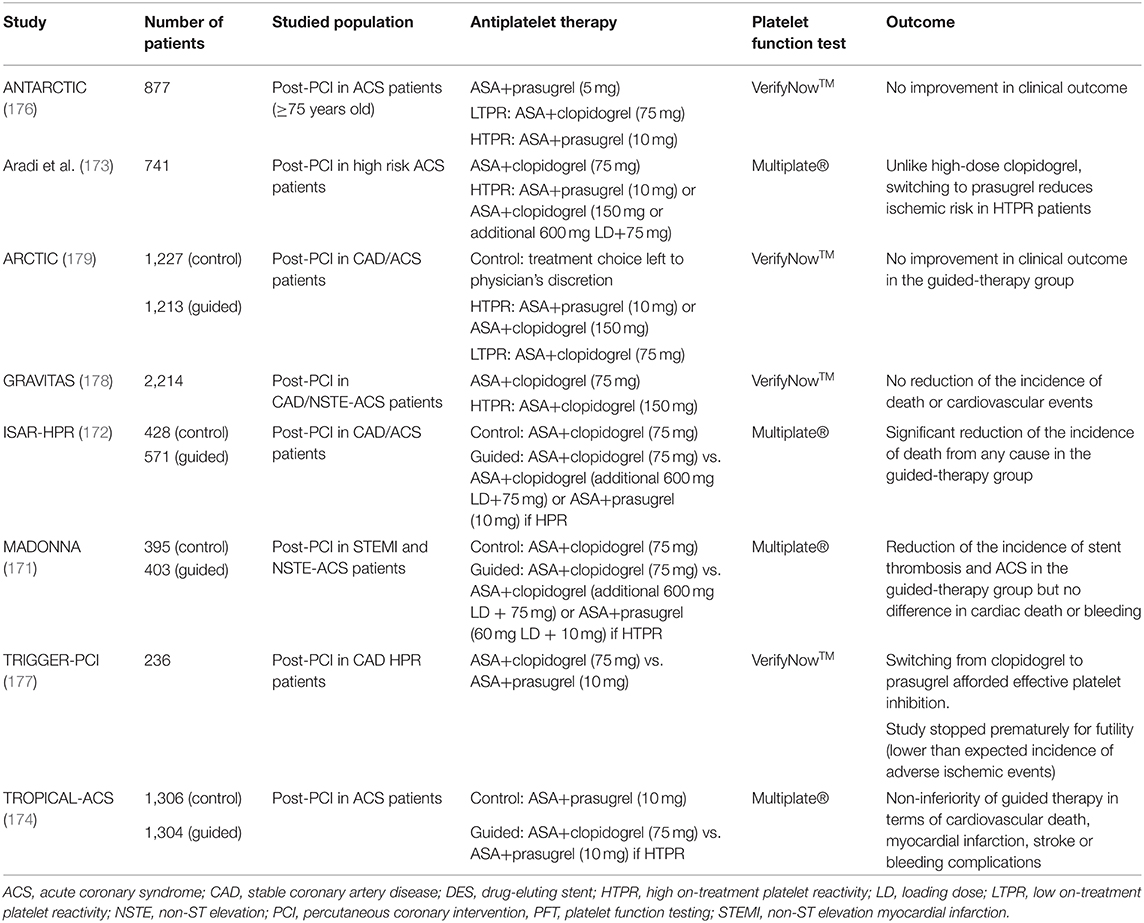
Table 4. Clinical trials evaluating personalized antiplatelet therapy based exclusively on platelet function testing.
The gold standard method for platelet function analysis is the light transmission aggregometry, a functional assay performed in citrate-anticoagulated platelet rich plasma, ideally within 4 h following blood sampling without any adjustment of the platelet count (unless it exceeds 600 × 109 L−1) (180). Platelet aggregation induced by arachidonic acid and ADP might be used to assess ASA- and P2Y12 receptor antagonists-related inhibition with a maximal platelet aggregation ≤ 20% (181) and ≤ 50% (182) in good responders' patients, respectively. However, this assay is time-consuming, requires sample preparation and dedicated laboratory resources, is poorly standardized and lacks specificity. Indeed, ASA was shown to influence ADP-induced platelet aggregation and, inversely, clopidogrel significantly inhibited arachidonic acid-induced platelet aggregation in patients on DAPT (183). ASA antiplatelet efficacy can also be evaluated by measuring TXA2 stable metabolite concentration in serum, namely TXB2, or 11-deoxy-TXB2 in the urine (Figure 4). However, these tests are not adapted to emergency context and are not entirely specific to ASA antiplatelet effect since TXA2 might be synthetized and secreted by other cells than platelets on one hand, and anti-P2Y12 receptor antagonists as well as non-steroidal anti-inflammatory drugs and anticoagulants (by inhibiting thrombin generation thus subsequent platelet activation) can also inhibit the amplification of platelet activation thus the TXA2 biosynthesis on the other hand (183). The pharmacological inhibition of the P2Y12 receptor can be evaluated by measuring the phosphorylation rate of the vasodilator-stimulated phosphoprotein (VASP) using flow cytometry or ELISA assays, which is insensitive to concomitant ASA therapy (183) and can be performed on blood samples drawn with a time-frame of 48 h (Figure 5). This test has shown good correlations with plasma concentrations of the drugs and their active metabolites, particularly for clopidogrel (184) and ticagrelor (185). Therefore, while both being centered on and close to the molecular effect of the antiplatelet drugs, VASP assay is insensitive to ASA while the levels of TXB2 in serum might be affected by P2Y12 receptor antagonists in patients on DAPT.
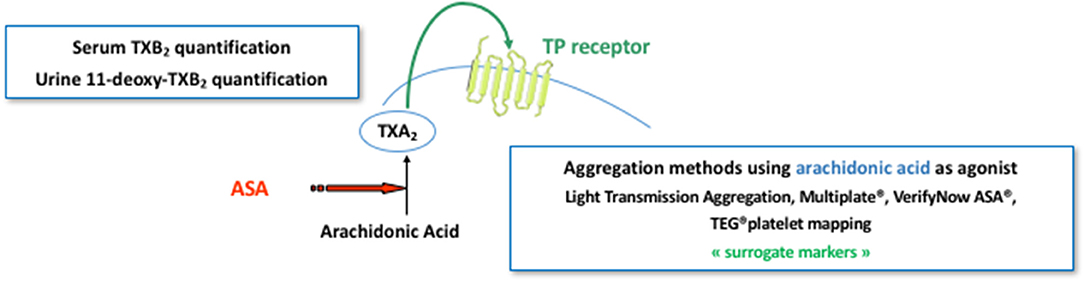
Figure 4. Pharmacodynamics of ASA. ASA pharmacodynamics can be evaluated using either an aggregation-based method evaluating the in vitro platelet capacity to be activated with arachidonic acid or by assessing the in vivo biosynthesis of thromboxane A2 via the quantification of its stable metabolite, namely thromboxane B2 (TXB2) in serum or 11-deoxy-TXB2 in urine. Aggregation-based method could be performed using the gold standard method for platelet function analysis, i.e., light transmission aggregometry, or one of the commercialized point-of-care tests, mainly Multiplate®, VerifyNow ASA®, and TEG® platelet mapping.
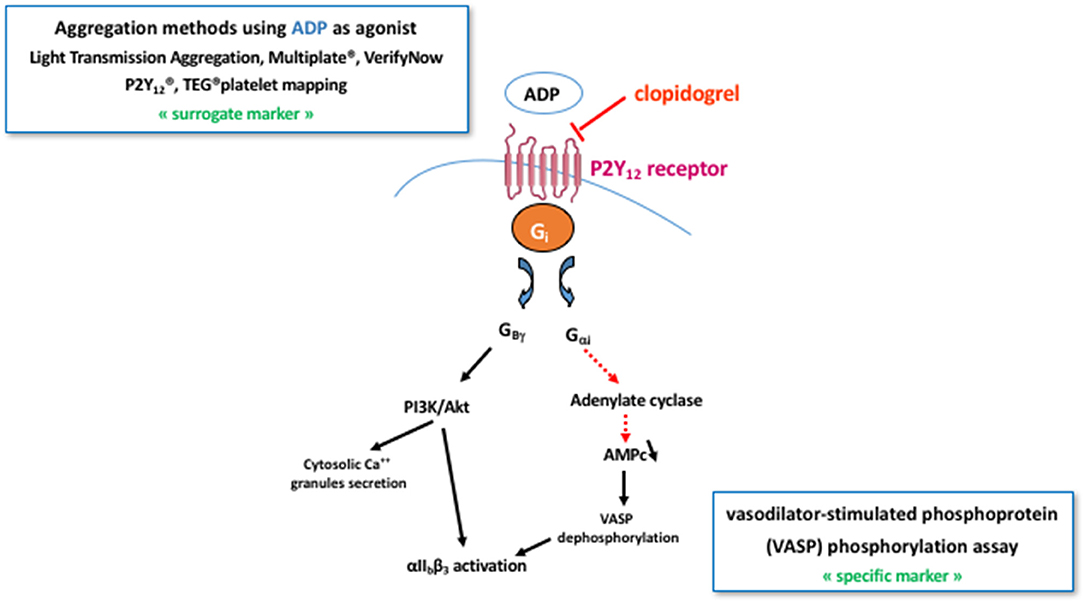
Figure 5. Pharmacodynamics of clopidogrel. Clopidogrel pharmacodynamics can be evaluated using either an aggregation-based method with ADP as platelet agonist or, more specifically by measuring the phosphorylation rate of the vasodilator-stimulated phosphoprotein (VASP) using flow cytometry or ELISA assays. The former can use the gold standard method for platelet function analysis, i.e. light transmission aggregometry, or one of the commercialized point-of-care tests, mainly Multiplate®, VerifyNow P2Y12, and TEG® platelet mapping. PI3K, phosphoinositide 3-kinase.
Assessment of platelet function might be particularly helpful in some urgent situations such as in the perioperative context or in bleeding patients with missing information of their antiplatelet therapy such as in unconscious, mentally incapacitated or amnesic patients. Indeed, point-of-care (POC) tests can aid determination of safe timing of invasive procedures in treated patients and management of hemorrhagic complications although these tests still need refinement and standardization and special expertise is needed to reliably interpret the results (186, 187). Moreover, the majority of the interventional studies (if not all) that evaluated the impact of the personalized antiplatelet therapy based exclusively on platelet function testing (Table 4) included POC tests rather than the light transmission aggregometry with usually missing pre-analytical and analytical assay details. Commercialized POC platelet analyzers include PFA-100®, VerifyNowTM, Multiplate®, Quantra, and TEG®-PM (platelet mapping). Briefly, PFA-100® is a quick test in which citrate-anticoagulated whole blood is aspirated in the presence of high shear rate through an aperture in a membrane coated with collagen and ADP or epinephrine until the aperture is completely occluded by a platelet plug. This POC is highly affected by VWF antigen level and activity and lacks sensitivity and reliability thus should not be used to assess antiplatelet therapy (188–190). VerifyNowTM is a quick but relatively expensive assay which consists on activating thrombin receptors on platelets surface resulting in their agglutination with the fibrinogen-coated beads thus increasing the light transmission through the sample. Yet, the analytical details explaining how light can be transmitted though whole blood remains undisclosed. It can be effective to assess ASA, P2Y12 receptor antagonists and GPIIbIIIa inhibitors using three specific cartridges. It has been assessed in many clinical trials (176–179) and was shown to accurately reflect the plasma concentration of some active antiplatelet compounds (184, 185). Nevertheless, several factors influence its performance, including fibrinogen levels, hematocrit, platelet count, triglyceride levels, and time from blood sampling to testing (191). The Multiplate® measures the increase of impedance between two electrodes caused by platelet aggregation in whole blood and is relatively sensitive to antiplatelet agents. Many studies demonstrated the benefit of tailoring antiplatelet therapy according to platelet function analysis using Multiplate® (171–174, 192). However, this test requires more laboratory expertise and is more time-consuming than other bedside assays. Finally, TEG®-PM and Quantra are POCs used in surgery and anesthesiology that measure platelet inhibition relative to baseline global viscoelastic profile. Few studies have evaluated their performance for assessing antiplatelet therapy. They reported conflicting results with a substantial intra- and inter-individual variability (186, 193–195). Each of these POC tests has strengths and weaknesses and no gold standard method for clinical application is yet identified, standardized and validated (196–198).
Conclusion
The worldwide increasing trend in clinical practice toward patient-centered precision medicine applies to antiplatelet therapy. It aims to select the appropriate antiplatelet agent with the optimal dose and therapy duration and requires careful balancing of benefits and risks in light of each patient's clinical characteristic and circumstances. Despite major advances in antiplatelet therapy, many areas of development deserve further investigation in order to appropriately manage the currently available agents and provide better guidance in clinical scenarios such as bleeding and surgery. Development of effective and safe reversal compounds for antiplatelet agents is also an area of unmet need. Moreover, novel antiplatelet drugs are in the pipeline (among which RUC-4, selatogrel, revacept, glenzocimab; non-exhaustive list) (199–203). How these potential new therapeutics will fit within the current paradigm of antiplatelet therapy and whether they will lead to safer combinations in the clinical practice remain to be determined. Therefore, while substantial research has allowed breakthroughs optimization of antiplatelet therapy, there is still much further to go.
Author Contributions
GJ and PG designed and drafted the work. AG, ML, and GM-G substantially revised the work. All authors have read and approved the submitted version.
Conflict of Interest
AG reports honoraria and travel fees from Bayer-Healthcare, Boehringer-Ingelheim, Bristol-Myers-Squibb/Pfizer, LFB, Octapharma, and Sanofi. ML has received speaker fees from Bayer; has participated in industry-funded trials from Idorsia; has served on advisory boards for Servier and JAMP/Orimed Pharma; and has received in-kind and financial support for investigator-initiated grants from Leo Pharma, Roche Diagnostics, Aggredyne, and Fujimori Kogyo. GM-G reports speaker fees and advisory board fees from JAMP Pharma, and research funding from Bayer.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Virani SS, Alonso A, Aparicio HJ, Benjamin EJ, Bittencourt MS, Callaway CW, et al. Heart disease and stroke statistics-2021 update: a report from the American Heart Association. Circulation. (2021) 143:e254–e743. doi: 10.1161/CIR.0000000000000950
2. McQuaid KR, Laine L. Systematic review and meta-analysis of adverse events of low-dose aspirin and clopidogrel in randomized controlled trials. Am J Med. (2006) 119:624–38. doi: 10.1016/j.amjmed.2005.10.039
3. Wallentin L, Becker RC, Budaj A, Cannon CP, Emanuelsson H, Held C, et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. (2009) 361:1045–57. doi: 10.1056/NEJMoa0904327
4. Wiviott SD, Braunwald E, McCabe CH, Montalescot G, Ruzyllo W, Gottlieb S, et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. (2007) 357:2001–15. doi: 10.1056/NEJMoa0706482
5. Serebruany VL, Malinin AI, Eisert RM, Sane DC. Risk of bleeding complications with antiplatelet agents: meta-analysis of 338,191 patients enrolled in 50 randomized controlled trials. Am J Hematol. (2004) 75:40–7. doi: 10.1002/ajh.10451
7. Wallentin L. P2Y(12) inhibitors: differences in properties and mechanisms of action and potential consequences for clinical use. Eur Heart J. (2009) 30:1964–77. doi: 10.1093/eurheartj/ehp296
8. Gremmel T, Panzer S. Oral antiplatelet therapy: impact for transfusion medicine. Vox Sang. (2017) 112:511–7. doi: 10.1111/vox.12537
9. Lenz T, Wilson A. Clinical pharmacokinetics of antiplatelet agents used in the secondary prevention of stroke. Clin Pharmacokinet. (2003) 42:909–20. doi: 10.2165/00003088-200342100-00003
10. Noma K, Higashi Y. Cilostazol for treatment of cerebral infarction. Expert Opin Pharmacother. (2018) 19:1719–26. doi: 10.1080/14656566.2018.1515199
11. Oprea AD, Popescu WM. ADP-receptor inhibitors in the perioperative period: the good, the bad, and the ugly. J Cardiothorac Vasc Anesth. (2013) 27:779–95. doi: 10.1053/j.jvca.2012.11.014
12. Kosoglou T, Reyderman L, Tiessen RG, van Vliet AA, Fales RR, Keller R, et al. Pharmacodynamics and pharmacokinetics of the novel PAR-1 antagonist vorapaxar (formerly SCH 530348) in healthy subjects. Eur J Clin Pharmacol. (2012) 68:249–58. doi: 10.1007/s00228-011-1120-6
13. Floyd CN, Passacquale G, Ferro A. Comparative pharmacokinetics and pharmacodynamics of platelet adenosine diphosphate receptor antagonists and their clinical implications. Clin Pharmacokinet. (2012) 51:429–42. doi: 10.2165/11630740-000000000-00000
14. Dobesh PP, Oestreich JH. Ticagrelor: pharmacokinetics, pharmacodynamics, clinical efficacy, and safety. Pharmacotherapy. (2014) 34:1077–90. doi: 10.1002/phar.1477
15. Patrono C, Coller B, FitzGerald GA, Hirsh J, Roth G. Platelet-active drugs: the relationships among dose, effectiveness, and side effects: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. (2004) 126:234S−264S. doi: 10.1378/chest.126.3_suppl.234S
16. Butler K, Teng R. Pharmacokinetics, pharmacodynamics, safety and tolerability of multiple ascending doses of ticagrelor in healthy volunteers. Br J Clin Pharmacol. (2010) 70:65–77. doi: 10.1111/j.1365-2125.2010.03669.x
17. Jakubowski JA, Matsushima N, Asai F, Naganuma H, Brandt JT, Hirota T, et al. A multiple dose study of prasugrel (CS-747), a novel thienopyridine P2Y12 inhibitor, compared with clopidogrel in healthy humans. Br J Clin Pharmacol. (2007) 63:421–30. doi: 10.1111/j.1365-2125.2006.02792.x
18. Iwamoto T, Kin K, Miyazaki K, Shin K, Takasaki M. Recovery of platelet function after withdrawal of cilostazol administered orally for a long period. J Atheroscler Thromb. (2003) 10:348–54. doi: 10.5551/jat.10.348
19. Eikelboom JW, Hirsh J, Spencer FA, Baglin TP, Weitz JI. Antiplatelet drugs: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. (2012) 141:e89S–e119S. doi: 10.1378/chest.11-2293
20. Steinhubl SR, Kottke-Marchant K, Moliterno DJ, Rosenthal ML, Godfrey NK, Coller BS, et al. Attainment and maintenance of platelet inhibition through standard dosing of abciximab in diabetic and nondiabetic patients undergoing percutaneous coronary intervention. Circulation. (1999) 100:1977–82. doi: 10.1161/01.CIR.100.19.1977
21. Kereiakes DJ, Broderick TM, Roth EM, Whang D, Shimshak T, Runyon JP, et al. Time course, magnitude, and consistency of platelet inhibition by abciximab, tirofiban, or eptifibatide in patients with unstable angina pectoris undergoing percutaneous coronary intervention. Am J Cardiol. (1999) 84:391–5. doi: 10.1016/S0002-9149(99)00321-5
22. Makris M, Van Veen JJ, Tait CR, Mumford AD, Laffan M, British Committee for Standards in Haematology. Guideline on the management of bleeding in patients on antithrombotic agents. Br J Haematol. (2013) 160:35–46. doi: 10.1111/bjh.12107
23. Darius H, Hossmann V, Schrör K. Antiplatelet effects of intravenous iloprost in patients with peripheral arterial obliterative disease. A placebo-controlled dose-response study. Klin Wochenschr. (1986) 64:545–51. doi: 10.1007/BF01735317
24. Haastrup PF, Grønlykke T, Jarbøl DE. Enteric coating can lead to reduced antiplatelet effect of low-dose acetylsalicylic acid. Basic Clin Pharmacol Toxicol. (2015) 116:212–5. doi: 10.1111/bcpt.12362
25. Nagelschmitz J, Blunck M, Kraetzschmar J, Ludwig M, Wensing G, Hohlfeld T. Pharmacokinetics and pharmacodynamics of acetylsalicylic acid after intravenous and oral administration to healthy volunteers. Clin Pharmacol Adv Appl. (2014) 6:51–9. doi: 10.2147/CPAA.S47895
26. Vivas D, Martín A, Bernardo E, Ortega-Pozzi MA, Tirado G, Fernández C, et al. Impact of intravenous lysine acetylsalicylate versus oral aspirin on prasugrel-inhibited platelets: results of a prospective, randomized, crossover study (the ECCLIPSE trial). Circ Cardiovasc Interv. (2015) 8:e002281. doi: 10.1161/CIRCINTERVENTIONS.114.002281
27. Bretagne JF, Feuillu A, Gosselin M, Gastard J. [Aspirin and gastroduodenal toxicity. A double-blind endoscopic study of the effects of placebo, aspirin and lysine acetylsalicylate in healthy subjects]. Gastroenterol Clin Biol. (1984) 8:28–32.
28. Majluf-Cruz A, Chavez-Ochoa AR de, Majluf-Cruz K, Coria-Ramirez E, Pineda Del Aguila I, Treviño-Perez S, et al. Effect of combined administration of clopidogrel and lysine acetylsalicylate versus clopidogrel and aspirin on platelet aggregation and activated GPIIb/IIIa expression in healthy volunteers. Platelets. (2006) 17:105–7. doi: 10.1080/09537100500438156
29. Gurfinkel EP, Altman R, Scazziota A, Heguilen R, Mautner B. Fast platelet suppression by lysine acetylsalicylate in chronic stable coronary patients. Potential clinical impact over regular aspirin for coronary syndromes. Clin Cardiol. (2000) 23:697–700. doi: 10.1002/clc.4960230912
30. Kimura K, Kimura T, Ishihara M, Nakagawa Y, Nakao K, Miyauchi K, et al. JCS 2018 Guideline on diagnosis and treatment of acute coronary syndrome. Circ J. (2019) 83:1085–196. doi: 10.1253/circj.CJ-19-0133
31. Valgimigli M, Bueno H, Byrne RA, Collet J-P, Costa F, Jeppsson A, et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: the Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. (2018) 39:213–60. doi: 10.1093/eurheartj/ehx638
32. Levine GN, Bates ER, Bittl JA, Brindis RG, Fihn SD, Fleisher LA, et al. 2016 ACC/AHA guideline focused update on duration of dual antiplatelet therapy in patients with coronary artery disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. (2016) 68:1082–115. doi: 10.1016/j.jacc.2016.03.513
33. Neumann F-J, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur Heart J. (2019) 40:87–165. doi: 10.1093/eurheartj/ehy855
34. Gerhard-Herman MD, Gornik HL, Barrett C, Barshes NR, Corriere MA, Drachman DE, et al. 2016 AHA/ACC guideline on the management of patients with lower extremity peripheral artery disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. (2017) 69:1465–508. doi: 10.1016/j.jacc.2016.11.008
35. Cacoub PP, Bhatt DL, Steg PG, Topol EJ, Creager MA, CHARISMA Investigators. Patients with peripheral arterial disease in the CHARISMA trial. Eur Heart J. (2009) 30:192–201. doi: 10.1093/eurheartj/ehn534
36. McNeil JJ, Wolfe R, Woods RL, Tonkin AM, Donnan GA, Nelson MR, et al. Effect of aspirin on cardiovascular events and bleeding in the healthy elderly. N Engl J Med. (2018) 379:1509–18. doi: 10.1056/NEJMoa1805819
37. ASCEND Study Collaborative Group, Bowman L, Mafham M, Wallendszus K, Stevens W, Buck G, et al. Effects of aspirin for primary prevention in persons with diabetes mellitus. N Engl J Med. (2018) 379:1529–39. doi: 10.1056/NEJMoa1804988
38. Gaziano JM, Brotons C, Coppolecchia R, Cricelli C, Darius H, Gorelick PB, et al. Use of aspirin to reduce risk of initial vascular events in patients at moderate risk of cardiovascular disease (ARRIVE): a randomised, double-blind, placebo-controlled trial. Lancet Lond Engl. (2018) 392:1036–46. doi: 10.1016/S0140-6736(18)31924-X
39. Cosentino F, Grant PJ, Aboyans V, Bailey CJ, Ceriello A, Delgado V, et al. 2019 ESC Guidelines on diabetes, pre-diabetes, cardiovascular diseases developed in collaboration with the EASD. Eur Heart J. (2020) 41:255–323. doi: 10.1093/eurheartj/ehz486
40. Yusuf S, Joseph P, Dans A, Gao P, Teo K, Xavier D, et al. Polypill with or without aspirin in persons without cardiovascular disease. N Engl J Med. (2021) 384:216–28. doi: 10.1056/NEJMoa2028220
41. Kleindorfer DO, Towfighi A, Chaturvedi S, Cockroft KM, Gutierrez J, Lombardi-Hill D, et al. 2021 guideline for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline from the American Heart Association/American Stroke Association. Stroke. (2021) 52:e364–e467. doi: 10.1161/STR.0000000000000375
42. Antithrombotic Trialists' Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ. (2002) 324:71–86. doi: 10.1136/bmj.324.7329.71
43. Rothwell PM, Algra A, Chen Z, Diener H-C, Norrving B, Mehta Z. Effects of aspirin on risk and severity of early recurrent stroke after transient ischaemic attack and ischaemic stroke: time-course analysis of randomised trials. Lancet Lond Engl. (2016) 388:365–75. doi: 10.1016/S0140-6736(16)30468-8
44. Jernberg T, Payne CD, Winters KJ, Darstein C, Brandt JT, Jakubowski JA, et al. Prasugrel achieves greater inhibition of platelet aggregation and a lower rate of non-responders compared with clopidogrel in aspirin-treated patients with stable coronary artery disease. Eur Heart J. (2006) 27:1166–73. doi: 10.1093/eurheartj/ehi877
45. Brandt JT, Payne CD, Wiviott SD, Weerakkody G, Farid NA, Small DS, et al. A comparison of prasugrel and clopidogrel loading doses on platelet function: magnitude of platelet inhibition is related to active metabolite formation. Am Heart J. (2007) 153:66.e9–e16. doi: 10.1016/j.ahj.2006.10.010
46. Rollini F, Franchi F, Angiolillo DJ. Switching P2Y12-receptor inhibitors in patients with coronary artery disease. Nat Rev Cardiol. (2016) 13:11–27. doi: 10.1038/nrcardio.2015.113
47. Alexopoulos D, Xanthopoulou I, Mavronasiou E, Stavrou K, Siapika A, Tsoni E, et al. Randomized assessment of ticagrelor versus prasugrel antiplatelet effects in patients with diabetes. Diabetes Care. (2013) 36:2211–6. doi: 10.2337/dc12-2510
48. Ndrepepa G, Kastrati A, Menichelli M, Neumann F-J, Wöhrle J, Bernlochner I, et al. Ticagrelor or prasugrel in patients with acute coronary syndromes and diabetes mellitus. JACC Cardiovasc Interv. (2020) 13:2238–47. doi: 10.1016/j.jcin.2020.07.032
49. Alexopoulos D, Xanthopoulou I, Gkizas V, Kassimis G, Theodoropoulos KC, Makris G, et al. Randomized assessment of ticagrelor versus prasugrel antiplatelet effects in patients with ST-segment-elevation myocardial infarction. Circ Cardiovasc Interv. (2012) 5:797–804. doi: 10.1161/CIRCINTERVENTIONS.112.972323
50. Wen M, Li Y, Qu X, Zhu Y, Tian L, Shen Z, et al. Comparison of platelet reactivity between prasugrel and ticagrelor in patients with acute coronary syndrome: a meta-analysis. BMC Cardiovasc Disord. (2020) 20:430. doi: 10.1186/s12872-020-01603-0
51. Nylander S, Femia EA, Scavone M, Berntsson P, Asztély A-K, Nelander K, et al. Ticagrelor inhibits human platelet aggregation via adenosine in addition to P2Y12 antagonism. J Thromb Haemost. (2013) 11:1867–76. doi: 10.1111/jth.12360
52. Mayer K, Bongiovanni D, Karschin V, Sibbing D, Angiolillo DJ, Schunkert H, et al. Ticagrelor or prasugrel for platelet inhibition in acute coronary syndrome patients: the ISAR-REACT 5 trial. J Am Coll Cardiol. (2020) 76:2569–71. doi: 10.1016/j.jacc.2020.09.586
53. Collet J-P, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, et al. 2020 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. (2021) 42:1289–367. doi: 10.1093/eurheartj/ehaa909
54. Gimbel M, Qaderdan K, Willemsen L, Hermanides R, Bergmeijer T, de Vrey E, et al. Clopidogrel versus ticagrelor or prasugrel in patients aged 70 years or older with non-ST-elevation acute coronary syndrome (POPular AGE): the randomised, open-label, non-inferiority trial. Lancet Lond Engl. (2020) 395:1374–81. doi: 10.1016/S0140-6736(20)30325-1
55. Valgimigli M, Gragnano F, Branca M, Franzone A, Baber U, Jang Y, et al. P2Y12 inhibitor monotherapy or dual antiplatelet therapy after coronary revascularisation: individual patient level meta-analysis of randomised controlled trials. BMJ. (2021) 373:n1332. doi: 10.1136/bmj.n1332
56. Bhatt DL, Stone GW, Mahaffey KW, Gibson CM, Steg PG, Hamm CW, et al. Effect of platelet inhibition with cangrelor during PCI on ischemic events. N Engl J Med. (2013) 368:1303–13. doi: 10.1056/NEJMoa1300815
57. Angiolillo DJ, Firstenberg MS, Price MJ, Tummala PE, Hutyra M, Welsby IJ, et al. Bridging antiplatelet therapy with cangrelor in patients undergoing cardiac surgery: a randomized controlled trial. JAMA. (2012) 307:265–74. doi: 10.1001/jama.2011.2002
58. Mehta SR, Bainey KR, Cantor WJ, Lordkipanidzé M, Marquis-Gravel G, Robinson SD, et al. 2018 Canadian Cardiovascular Society/Canadian Association of Interventional Cardiology focused update of the guidelines for the use of antiplatelet therapy. Can J Cardiol. (2018) 34:214–33. doi: 10.1016/j.cjca.2017.12.012
59. January CT, Wann LS, Calkins H, Chen LY, Cigarroa JE, Cleveland JC, et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in Collaboration With the Society of Thoracic Surgeons. Circulation. (2019) 140:e125–e51. doi: 10.1161/CIR.0000000000000665
60. Saito Y, Kobayashi Y. Update on antithrombotic therapy after percutaneous coronary intervention. Intern Med Tokyo Jpn. (2020) 59:311–21. doi: 10.2169/internalmedicine.3685-19
61. Angiolillo DJ, Goodman SG, Bhatt DL, Eikelboom JW, Price MJ, Moliterno DJ, et al. Antithrombotic therapy in patients with atrial fibrillation treated with oral anticoagulation undergoing percutaneous coronary intervention: a North American perspective-2018 update. Circulation. (2018) 138:527–36. doi: 10.1161/CIRCULATIONAHA.118.034722
62. Lip GYH, Collet J-P, Haude M, Byrne R, Chung EH, Fauchier L, et al. 2018 Joint European consensus document on the management of antithrombotic therapy in atrial fibrillation patients presenting with acute coronary syndrome and/or undergoing percutaneous cardiovascular interventions: a joint consensus document of the European Heart Rhythm Association (EHRA), European Society of Cardiology Working Group on Thrombosis, European Association of Percutaneous Cardiovascular Interventions (EAPCI), and European Association of Acute Cardiac Care (ACCA) endorsed by the Heart Rhythm Society (HRS), Asia-Pacific Heart Rhythm Society (APHRS), Latin America Heart Rhythm Society (LAHRS), and Cardiac Arrhythmia Society of Southern Africa (CASSA). Eurpace. (2019) 21:192–3. doi: 10.1093/europace/euy174
63. Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, et al. 2017 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J. (2017) 38:2739–91. doi: 10.1016/j.rec.2017.12.013
64. Hamilos M, Petousis S, Xanthopoulou I, Goudevenos J, Kanakakis J, Sitafidis G, et al. Antiplatelet treatment in diabetic patients with acute coronary syndrome undergoing percutaneous coronary intervention: a GReek AntiPlatElet registry substudy. Coron Artery Dis. (2018) 29:53–9. doi: 10.1097/MCA.0000000000000547
65. Angiolillo DJ, Fernandez-Ortiz A, Bernardo E, Ramírez C, Sabaté M, Jimenez-Quevedo P, et al. Platelet function profiles in patients with type 2 diabetes and coronary artery disease on combined aspirin and clopidogrel treatment. Diabetes. (2005) 54:2430–5. doi: 10.2337/diabetes.54.8.2430
66. Kaur R, Kaur M, Singh J. Endothelial dysfunction and platelet hyperactivity in type 2 diabetes mellitus: molecular insights and therapeutic strategies. Cardiovasc Diabetol. (2018) 17:121. doi: 10.1186/s12933-018-0763-3
67. Vinik AI, Erbas T, Park TS, Nolan R, Pittenger GL. Platelet dysfunction in type 2 diabetes. Diabetes Care. (2001) 24:1476–85. doi: 10.2337/diacare.24.8.1476
68. Sacco RL, Diener H-C, Yusuf S, Cotton D, Ounpuu S, Lawton WA, et al. Aspirin and extended-release dipyridamole versus clopidogrel for recurrent stroke. N Engl J Med. (2008) 359:1238–51. doi: 10.1056/NEJMoa0805002
69. De Luca G, Savonitto S, van't Hof AWJ, Suryapranata H. Platelet GP IIb-IIIa receptor antagonists in primary angioplasty: back to the future. Drugs. (2015) 75:1229–53. doi: 10.1007/s40265-015-0425-7
70. Muñiz-Lozano A, Rollini F, Franchi F, Angiolillo DJ. Update on platelet glycoprotein IIb/IIIa inhibitors: recommendations for clinical practice. Ther Adv Cardiovasc Dis. (2013) 7:197–213. doi: 10.1177/1753944713487781
71. Franchi F, Rollini F, Park Y, Angiolillo DJ. Platelet thrombin receptor antagonism with vorapaxar: pharmacology and clinical trial development. Future Cardiol. (2015) 11:547–64. doi: 10.2217/fca.15.50
72. Morrow DA, Braunwald E, Bonaca MP, Ameriso SF, Dalby AJ, Fish MP, et al. Vorapaxar in the secondary prevention of atherothrombotic events. N Engl J Med. (2012) 366:1404–13. doi: 10.1056/NEJMoa1200933
73. Tricoci P, Huang Z, Held C, Moliterno DJ, Armstrong PW, Van de Werf F, et al. Thrombin-receptor antagonist vorapaxar in acute coronary syndromes. N Engl J Med. (2012) 366:20–33. doi: 10.1056/NEJMoa1109719
74. Bonaca MP, Scirica BM, Creager MA, Olin J, Bounameaux H, Dellborg M, et al. Vorapaxar in patients with peripheral artery disease: results from TRA2{degrees}P-TIMI 50. Circulation. (2013) 127:1522–9:9e1–6. doi: 10.1161/CIRCULATIONAHA.112.000679
75. Grant SM, Goa KL. Iloprost. A review of its pharmacodynamic and pharmacokinetic properties, and therapeutic potential in peripheral vascular disease, myocardial ischaemia and extracorporeal circulation procedures. Drugs. (1992) 43:889–924. doi: 10.2165/00003495-199243060-00008
76. Gresele P, Momi S, Falcinelli E. Anti-platelet therapy: phosphodiesterase inhibitors. Br J Clin Pharmacol. (2011) 72:634–46. doi: 10.1111/j.1365-2125.2011.04034.x
77. Deckmyn H, Gresele P, Arnout J, Todisco A, Vermylen J. Prolonging prostacyclin production by nafazatrom or dipyridamole. Lancet Lond Engl. (1984) 2:410–1. doi: 10.1016/S0140-6736(84)90582-8
78. Masotti G, Poggesi L, Galanti G, Neri Serneri GG. Stimulation of prostacyclin by dipyridamole. Lancet Lond Engl. (1979) 1:1412. doi: 10.1016/S0140-6736(79)92053-1
79. Gotoh F, Tohgi H, Hirai S, Terashi A, Fukuuchi Y, Otomo E, et al. Cilostazol stroke prevention study: a placebo-controlled double-blind trial for secondary prevention of cerebral infarction. J Stroke Cerebrovasc Dis. (2000) 9:147–57. doi: 10.1053/jscd.2000.7216
80. Shinohara Y, Katayama Y, Uchiyama S, Yamaguchi T, Handa S, Matsuoka K, et al. Cilostazol for prevention of secondary stroke (CSPS 2): an aspirin-controlled, double-blind, randomised non-inferiority trial. Lancet Neurol. (2010) 9:959–68. doi: 10.1016/S1474-4422(10)70198-8
81. Huang Y, Cheng Y, Wu J, Li Y, Xu E, Hong Z, et al. Cilostazol as an alternative to aspirin after ischaemic stroke: a randomised, double-blind, pilot study. Lancet Neurol. (2008) 7:494–9. doi: 10.1016/S1474-4422(08)70094-2
82. Sahara N, Kuwashiro T, Okada Y. [Cerebral infarction and transient ischemic attack]. Nihon Rinsho Jpn J Clin Med. (2016) 74:666–70.
83. Angiolillo DJ, Rollini F, Storey RF, Bhatt DL, James S, Schneider DJ, et al. International expert consensus on switching platelet P2Y12 receptor-inhibiting therapies. Circulation. (2017) 136:1955–75. doi: 10.1161/CIRCULATIONAHA.117.031164
84. Badreldin HA, Carter D, Cook BM, Qamar A, Vaduganathan M, Bhatt DL. Safety and tolerability of transitioning from cangrelor to ticagrelor in patients who underwent percutaneous coronary intervention. Am J Cardiol. (2017) 120:359–61. doi: 10.1016/j.amjcard.2017.04.034
85. Savonitto S, Caracciolo M, Cattaneo M, DE Servi S. Management of patients with recently implanted coronary stents on dual antiplatelet therapy who need to undergo major surgery. J Thromb Haemost. (2011) 9:2133–42. doi: 10.1111/j.1538-7836.2011.04456.x
86. Devereaux PJ, Mrkobrada M, Sessler DI, Leslie K, Alonso-Coello P, Kurz A, et al. Aspirin in patients undergoing noncardiac surgery. N Engl J Med. (2014) 370:1494–503. doi: 10.1056/NEJMoa1401105
87. Rossini R, Musumeci G, Visconti LO, Bramucci E, Castiglioni B, De Servi S, et al. Perioperative management of antiplatelet therapy in patients with coronary stents undergoing cardiac and non-cardiac surgery: a consensus document from Italian cardiological, surgical and anaesthesiological societies. EuroIntervention. (2014) 10:38–46. doi: 10.4244/EIJV10I1A8
88. Godier A, Garrigue D, Lasne D, Fontana P, Bonhomme F, Collet J-P, et al. Management of antiplatelet therapy for non-elective invasive procedures or bleeding complications: proposals from the French Working Group on Perioperative Haemostasis (GIHP) and the French Study Group on Thrombosis and Haemostasis (GFHT), in collaboration with the French Society for Anaesthesia and Intensive Care (SFAR). Arch Cardiovasc Dis. (2019) 112:199–216. doi: 10.1016/j.acvd.2018.10.004
89. Roffi M, Patrono C, Collet J-P, Mueller C, Valgimigli M, Andreotti F, et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J. (2016) 37:267–315. doi: 10.1093/eurheartj/ehv320
90. Di Minno MND, Milone M, Mastronardi P, Ambrosino P, Di Minno A, Parolari A, et al. Perioperative handling of antiplatelet drugs. A critical appraisal. Curr Drug Targets. (2013) 14:880–8. doi: 10.2174/1389450111314080008
91. Nakamura M, Kimura K, Kimura T, Ishihara M, Otsuka F, Kozuma K, et al. JCS 2020 guideline focused update on antithrombotic therapy in patients with coronary artery disease. Circ J. (2020) 84:831–65. doi: 10.1253/circj.CJ-19-1109
92. Howard TM, Khot UN. Dual antiplatelet therapy after percutaneous coronary intervention: personalize the duration. Cleve Clin J Med. (2021) 88:325–32. doi: 10.3949/ccjm.88a.20113
93. Malm CJ, Hansson EC, Åkesson J, Andersson M, Hesse C, Shams Hakimi C, et al. Preoperative platelet function predicts perioperative bleeding complications in ticagrelor-treated cardiac surgery patients: a prospective observational study. Br J Anaesth. (2016) 117:309–15. doi: 10.1093/bja/aew189
94. Ranucci M, Baryshnikova E, Soro G, Ballotta A, De Benedetti D, Conti D, et al. Multiple electrode whole-blood aggregometry and bleeding in cardiac surgery patients receiving thienopyridines. Ann Thorac Surg. (2011) 91:123–9. doi: 10.1016/j.athoracsur.2010.09.022
95. Godier A, Albaladejo P On On Perioperative Haemostasis Gihp Group TFWG. Management of bleeding events associated with antiplatelet therapy: evidence, uncertainties and pitfalls. J Clin Med. (2020) 9:2318. doi: 10.3390/jcm9072318
96. Mohanty D. Current concepts in platelet transfusion. Asian J Transfus Sci. (2009) 3:18–21. doi: 10.4103/0973-6247.45257
97. Godier A, Taylor G, Gaussem P. Inefficacy of platelet transfusion to reverse ticagrelor. N Engl J Med. (2015) 372:196–7. doi: 10.1056/NEJMc1409373
98. Zafar MU, Smith DA, Baber U, Sartori S, Chen K, Lam DW, et al. Impact of timing on the functional recovery achieved with platelet supplementation after treatment with ticagrelor. Circ Cardiovasc Interv. (2017) 10:e005120. doi: 10.1161/CIRCINTERVENTIONS.117.005120
99. Swan D, Loughran N, Makris M, Thachil J. Management of bleeding and procedures in patients on antiplatelet therapy. Blood Rev. (2020) 39:100619. doi: 10.1016/j.blre.2019.100619
100. Levi M, Levy JH, Andersen HF, Truloff D. Safety of recombinant activated factor VII in randomized clinical trials. N Engl J Med. (2010) 363:1791–800. doi: 10.1056/NEJMoa1006221
101. Weber CF, Görlinger K, Byhahn C, Moritz A, Hanke AA, Zacharowski K, et al. Tranexamic acid partially improves platelet function in patients treated with dual antiplatelet therapy. Eur J Anaesthesiol. (2011) 28:57–62. doi: 10.1097/EJA.0b013e32834050ab
102. Estcourt LJ, Birchall J, Allard S, Bassey SJ, Hersey P, Kerr JP, et al. Guidelines for the use of platelet transfusions. Br J Haematol. (2017) 176:365–94. doi: 10.1111/bjh.14423
103. Buchanan A, Newton P, Pehrsson S, Inghardt T, Antonsson T, Svensson P, et al. Structural and functional characterization of a specific antidote for ticagrelor. Blood. (2015) 125:3484–90. doi: 10.1182/blood-2015-01-622928
104. Bhatt DL, Pollack CV, Weitz JI, Jennings LK, Xu S, Arnold SE, et al. Antibody-based ticagrelor reversal agent in healthy volunteers. N Engl J Med. (2019) 380:1825–33. doi: 10.1056/NEJMoa1901778
105. Horlocker TT, Wedel DJ, Schroeder DR, Rose SH, Elliott BA, McGregor DG, et al. Preoperative antiplatelet therapy does not increase the risk of spinal hematoma associated with regional anesthesia. Anesth Analg. (1995) 80:303–9. doi: 10.1097/00000539-199502000-00017
106. CLASP collaborative group. CLASP: a randomised trial of low-dose aspirin for the prevention and treatment of pre-eclampsia among 9364 pregnant women. CLASP (Collaborative Low-dose Aspirin Study in Pregnancy) Collaborative Group. Lancet Lond Engl. (1994) 343:619–29. doi: 10.1016/S0140-6736(94)92633-6
107. Horlocker TT, Vandermeuelen E, Kopp SL, Gogarten W, Leffert LR, Benzon HT. Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (Fourth Edition). Reg Anesth Pain Med. (2018) 43:263–309. doi: 10.1097/AAP.0000000000000763
108. Tielleman T, Bujanda D, Cryer B. Epidemiology and risk factors for upper gastrointestinal bleeding. Gastrointest Endosc Clin N Am. (2015) 25:415–28. doi: 10.1016/j.giec.2015.02.010
109. Alli O, Smith C, Hoffman M, Amanullah S, Katz P, Amanullah AM. Incidence, predictors, and outcomes of gastrointestinal bleeding in patients on dual antiplatelet therapy with aspirin and clopidogrel. J Clin Gastroenterol. (2011) 45:410–4. doi: 10.1097/MCG.0b013e3181faec3c
110. Laine L, Jensen DM. Management of patients with ulcer bleeding. Am J Gastroenterol. (2012) 107:345–60; quiz 361. doi: 10.1038/ajg.2011.480
111. Chan FKL, Ching JYL, Hung LCT, Wong VWS, Leung VKS, Kung NNS, et al. Clopidogrel versus aspirin and esomeprazole to prevent recurrent ulcer bleeding. N Engl J Med. (2005) 352:238–44. doi: 10.1056/NEJMoa042087
112. Khan MY, Siddiqui WJ, Alvarez C, Aggarwal S, Hasni SF, Ahmad A, et al. Reduction in postpercutaneous coronary intervention angina in addition to gastrointestinal events in patients on combined proton pump inhibitors and dual antiplatelet therapy: a systematic review and meta-analysis. Eur J Gastroenterol Hepatol. (2018) 30:847–53. doi: 10.1097/MEG.0000000000001125
113. Sehested TSG, Carlson N, Hansen PW, Gerds TA, Charlot MG, Torp-Pedersen C, et al. Reduced risk of gastrointestinal bleeding associated with proton pump inhibitor therapy in patients treated with dual antiplatelet therapy after myocardial infarction. Eur Heart J. (2019) 40:1963–70. doi: 10.1093/eurheartj/ehz104
114. Gilard M, Arnaud B, Cornily J-C, Le Gal G, Lacut K, Le Calvez G, et al. Influence of omeprazole on the antiplatelet action of clopidogrel associated with aspirin: the randomized, double-blind OCLA (Omeprazole CLopidogrel Aspirin) study. J Am Coll Cardiol. (2008) 51:256–60. doi: 10.1016/j.jacc.2007.06.064
115. Vaduganathan M, Cannon CP, Cryer BL, Liu Y, Hsieh W-H, Doros G, et al. Efficacy and safety of proton-pump inhibitors in high-risk cardiovascular subsets of the COGENT trial. Am J Med. (2016) 129:1002–5. doi: 10.1016/j.amjmed.2016.03.042
116. Siller-Matula JM, Spiel AO, Lang IM, Kreiner G, Christ G, Jilma B. Effects of pantoprazole and esomeprazole on platelet inhibition by clopidogrel. Am Heart J. (2009) 157:148.e1–e5. doi: 10.1016/j.ahj.2008.09.017
117. Small DS, Farid NA, Payne CD, Weerakkody GJ, Li YG, Brandt JT, et al. Effects of the proton pump inhibitor lansoprazole on the pharmacokinetics and pharmacodynamics of prasugrel and clopidogrel. J Clin Pharmacol. (2008) 48:475–84. doi: 10.1177/0091270008315310
118. Zakko L, Rustagi T, Douglas M, Laine L. No benefit from platelet transfusion for gastrointestinal bleeding in patients taking antiplatelet agents. Clin Gastroenterol Hepatol. (2017) 15:46–52. doi: 10.1016/j.cgh.2016.07.017
119. ASGE ASGE Standards of Practice Committee, Acosta RD, Abraham NS, Chandrasekhara V, Chathadi KV, Early DS, et al. The management of antithrombotic agents for patients undergoing GI endoscopy. Gastrointest Endosc. (2016) 83:3–16. doi: 10.1016/j.gie.2015.09.035
120. Scott MJ, Veitch A, Thachil J. Reintroduction of anti-thrombotic therapy after a gastrointestinal haemorrhage: if and when? Br J Haematol. (2017) 177:185–97. doi: 10.1111/bjh.14599
121. Frontera JA, Lewin JJ, Rabinstein AA, Aisiku IP, Alexandrov AW, Cook AM, et al. Guideline for reversal of antithrombotics in intracranial hemorrhage: a statement for healthcare professionals from the Neurocritical Care Society and Society of Critical Care Medicine. Neurocrit Care. (2016) 24:6–46. doi: 10.1007/s12028-015-0222-x
122. Qiu J, Ye H, Wang J, Yan J, Wang J, Wang Y. Antiplatelet therapy, cerebral microbleeds, and intracerebral hemorrhage: a meta-analysis. Stroke. (2018) 49:1751–4. doi: 10.1161/STROKEAHA.118.021789
123. Wilson D, Ambler G, Shakeshaft C, Brown MM, Charidimou A, Al-Shahi Salman R, et al. Cerebral microbleeds and intracranial haemorrhage risk in patients anticoagulated for atrial fibrillation after acute ischaemic stroke or transient ischaemic attack (CROMIS-2): a multicentre observational cohort study. Lancet Neurol. (2018) 17:539–47. doi: 10.1016/S1474-4422(18)30145-5
124. Scott M, Low R, Swan D, Thachil J. Reintroduction of anticoagulant therapy after intracranial haemorrhage: if and when? Blood Rev. (2018) 32:256–63. doi: 10.1016/j.blre.2017.12.002
125. Ward SA, Raniga P, Ferris NJ, Woods RL, Storey E, Bailey MJ, et al. ASPREE-NEURO study protocol: a randomized controlled trial to determine the effect of low-dose aspirin on cerebral microbleeds, white matter hyperintensities, cognition, and stroke in the healthy elderly. Int J Stroke. (2017) 12:108–13. doi: 10.1177/1747493016669848
126. Baharoglu MI, Cordonnier C, Al-Shahi Salman R, de Gans K, Koopman MM, Brand A, et al. Platelet transfusion versus standard care after acute stroke due to spontaneous cerebral haemorrhage associated with antiplatelet therapy (PATCH): a randomised, open-label, phase 3 trial. Lancet Lond Engl. (2016) 387:2605–13. doi: 10.1016/S0140-6736(16)30392-0
127. Spahn DR, Bouillon B, Cerny V, Duranteau J, Filipescu D, Hunt BJ, et al. The European guideline on management of major bleeding and coagulopathy following trauma: fifth edition. Crit Care Lond Engl. (2019) 23:98. doi: 10.1186/s13054-019-2347-3
128. Ohmori T, Kitamura T, Ishihara J, Onishi H, Nojima T, Yamamoto K, et al. Early predictors for massive transfusion in older adult severe trauma patients. Injury. (2017) 48:1006–12. doi: 10.1016/j.injury.2016.12.028
129. Levine GN, Jeong Y-H, Goto S, Anderson JL, Huo Y, Mega JL, et al. Expert consensus document: World Heart Federation expert consensus statement on antiplatelet therapy in East Asian patients with ACS or undergoing PCI. Nat Rev Cardiol. (2014) 11:597–606. doi: 10.1038/nrcardio.2014.104
130. Corpataux N, Spirito A, Gragnano F, Vaisnora L, Galea R, Svab S, et al. Validation of high bleeding risk criteria and definition as proposed by the academic research consortium for high bleeding risk. Eur Heart J. (2020) 41:3743–9. doi: 10.1093/eurheartj/ehaa671
131. Choi SY, Kim MH, Cho Y-R, Sung Park J, Min Lee K, Park T-H, et al. Performance of PRECISE-DAPT score for predicting bleeding complication during dual antiplatelet therapy. Circ Cardiovasc Interv. (2018) 11:e006837. doi: 10.1161/CIRCINTERVENTIONS.118.006837
132. Pelliccia F, Pasceri V, Marazzi G, Cacciotti L, Placanica A, Gragnano F, et al. Predictive ability of longitudinal changes in PRECISE-DAPT score in patients on dual antiplatelet therapy: the RE-SCORE multicentre prospective registry. Eur J Prev Cardiol. (2021) 28:e36–e8. doi: 10.1177/2047487320937846
133. Yeh RW, Secemsky EA, Kereiakes DJ, Normand S-LT, Gershlick AH, Cohen DJ, et al. Development and validation of a prediction rule for benefit and harm of dual antiplatelet therapy beyond 1 year after percutaneous coronary intervention. JAMA. (2016) 315:1735–49. doi: 10.1001/jama.2016.3775
134. Baber U, Mehran R, Giustino G, Cohen DJ, Henry TD, Sartori S, et al. Coronary thrombosis and major bleeding after PCI with drug-eluting stents: risk scores from PARIS. J Am Coll Cardiol. (2016) 67:2224–34. doi: 10.1016/j.jacc.2016.02.064
135. Natsuaki M, Morimoto T, Yamaji K, Watanabe H, Yoshikawa Y, Shiomi H, et al. Prediction of thrombotic and bleeding events after percutaneous coronary intervention: CREDO-Kyoto thrombotic and bleeding risk scores. J Am Heart Assoc. (2018) 7:e008708. doi: 10.1161/JAHA.118.008708
136. Pasea L, Chung S-C, Pujades-Rodriguez M, Moayyeri A, Denaxas S, Fox KAA, et al. Personalising the decision for prolonged dual antiplatelet therapy: development, validation and potential impact of prognostic models for cardiovascular events and bleeding in myocardial infarction survivors. Eur Heart J. (2017) 38:1048–55. doi: 10.1093/eurheartj/ehw683
137. Bohula EA, Bonaca MP, Braunwald E, Aylward PE, Corbalan R, De Ferrari GM, et al. Atherothrombotic risk stratification and the efficacy and safety of vorapaxar in patients with stable ischemic heart disease and previous myocardial infarction. Circulation. (2016) 134:304–13. doi: 10.1161/CIRCULATIONAHA.115.019861
138. Généreux P, Giustino G, Witzenbichler B, Weisz G, Stuckey TD, Rinaldi MJ, et al. Incidence, predictors, and impact of post-discharge bleeding after percutaneous coronary intervention. J Am Coll Cardiol. (2015) 66:1036–45. doi: 10.1016/j.jacc.2015.06.1323
139. Mehran R, Pocock SJ, Nikolsky E, Clayton T, Dangas GD, Kirtane AJ, et al. A risk score to predict bleeding in patients with acute coronary syndromes. J Am Coll Cardiol. (2010) 55:2556–66. doi: 10.1016/j.jacc.2009.09.076
140. Subherwal S, Bach RG, Chen AY, Gage BF, Rao SV, Newby LK, et al. Baseline risk of major bleeding in non-ST-segment-elevation myocardial infarction: the CRUSADE (Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA Guidelines) Bleeding Score. Circulation. (2009) 119:1873–82. doi: 10.1161/CIRCULATIONAHA.108.828541
141. Alfredsson J, Neely B, Neely ML, Bhatt DL, Goodman SG, Tricoci P, et al. Predicting the risk of bleeding during dual antiplatelet therapy after acute coronary syndromes. Heart Br Card Soc. (2017) 103:1168–76. doi: 10.1136/heartjnl-2016-310090
142. Lopes RD, Leonardi S, Neely B, Neely ML, Ohman EM, Ardissino D, et al. Spontaneous MI after non-ST-segment elevation acute coronary syndrome managed without revascularization: the TRILOGY ACS trial. J Am Coll Cardiol. (2016) 67:1289–97. doi: 10.1016/j.jacc.2016.01.034
143. Capodanno D, Angiolillo DJ. Tailoring duration of DAPT with risk scores. Lancet Lond Engl. (2017) 389:987–9. doi: 10.1016/S0140-6736(17)30591-3
144. Marquis-Gravel G, Neely ML, Valgimigli M, Costa F, Van Klaveren D, Altner R, et al. Long-term bleeding risk prediction with dual antiplatelet therapy after acute coronary syndromes treated without revascularization. Circ Cardiovasc Qual Outcomes. (2020) 13:e006582. doi: 10.1161/CIRCOUTCOMES.120.006582
145. Iqbal J, Gunn J, Serruys PW. Coronary stents: historical development, current status and future directions. Br Med Bull. (2013) 106:193–211. doi: 10.1093/bmb/ldt009
146. McFadden EP, Stabile E, Regar E, Cheneau E, Ong ATL, Kinnaird T, et al. Late thrombosis in drug-eluting coronary stents after discontinuation of antiplatelet therapy. Lancet Lond Engl. (2004) 364:1519–21. doi: 10.1016/S0140-6736(04)17275-9
147. Cassese S, Byrne RA, Ndrepepa G, Kufner S, Wiebe J, Repp J, et al. Everolimus-eluting bioresorbable vascular scaffolds versus everolimus-eluting metallic stents: a meta-analysis of randomised controlled trials. Lancet Lond Engl. (2016) 387:537–44. doi: 10.1016/S0140-6736(15)00979-4
148. Mangieri A, Gallo F, Sticchi A, Khokhar AA, Laricchia A, Giannini F, et al. Dual antiplatelet therapy in coronary artery disease: from the past to the future prospective. Cardiovasc Interv Ther. (2020) 35:117–29. doi: 10.1007/s12928-020-00642-w
149. O'Connor CT, Kiernan TJ, Yan BP. The genetic basis of antiplatelet and anticoagulant therapy: a pharmacogenetic review of newer antiplatelets (clopidogrel, prasugrel and ticagrelor) and anticoagulants (dabigatran, rivaroxaban, apixaban and edoxaban). Expert Opin Drug Metab Toxicol. (2017) 13:725–39. doi: 10.1080/17425255.2017.1338274
150. Lordkipanidzé M, Diodati JG, Palisaitis DA, Schampaert E, Turgeon J, Pharand C. Genetic determinants of response to aspirin: appraisal of 4 candidate genes. Thromb Res. (2011) 128:47–53. doi: 10.1016/j.thromres.2011.02.019
151. Hulot J-S, Bura A, Villard E, Azizi M, Remones V, Goyenvalle C, et al. Cytochrome P450 2C19 loss-of-function polymorphism is a major determinant of clopidogrel responsiveness in healthy subjects. Blood. (2006) 108:2244–7. doi: 10.1182/blood-2006-04-013052
152. Strom CM, Goos D, Crossley B, Zhang K, Buller-Burkle A, Jarvis M, et al. Testing for variants in CYP2C19: population frequencies and testing experience in a clinical laboratory. Genet Med. (2012) 14:95–100. doi: 10.1038/gim.0b013e3182329870
153. Scott SA, Sangkuhl K, Stein CM, Hulot J-S, Mega JL, Roden DM, et al. Clinical Pharmacogenetics Implementation Consortium guidelines for CYP2C19 genotype and clopidogrel therapy: 2013 update. Clin Pharmacol Ther. (2013) 94:317–23. doi: 10.1038/clpt.2013.105
154. Desta Z, Zhao X, Shin J-G, Flockhart DA. Clinical significance of the cytochrome P450 2C19 genetic polymorphism. Clin Pharmacokinet. (2002) 41:913–58. doi: 10.2165/00003088-200241120-00002
155. Gower MN, Ratner LR, Williams AK, Rossi JS, Stouffer GA, Lee CR. Clinical utility of CYP2C19 genotype-guided antiplatelet therapy in patients at risk of adverse cardiovascular and cerebrovascular events: a review of emerging evidence. Pharmacogenomics Pers Med. (2020) 13:239–52. doi: 10.2147/PGPM.S231475
156. Mega JL, Close SL, Wiviott SD, Shen L, Hockett RD, Brandt JT, et al. Cytochrome P450 genetic polymorphisms and the response to prasugrel: relationship to pharmacokinetic, pharmacodynamic, and clinical outcomes. Circulation. (2009) 119:2553–60. doi: 10.1161/CIRCULATIONAHA.109.851949
157. Claassens DMF, Vos GJA, Bergmeijer TO, Hermanides RS, van't Hof AWJ, van der Harst P, et al. A genotype-guided strategy for oral P2Y12 inhibitors in primary PCI. N Engl J Med. (2019) 381:1621–31. doi: 10.1056/NEJMoa1907096
158. Hulot J-S, Wuerzner G, Bachelot-Loza C, Azizi M, Blanchard A, Peyrard S, et al. Effect of an increased clopidogrel maintenance dose or lansoprazole co-administration on the antiplatelet response to clopidogrel in CYP2C19-genotyped healthy subjects. J Thromb Haemost. (2010) 8:610–3. doi: 10.1111/j.1538-7836.2009.03729.x
159. Collet J-P, Hulot J-S, Anzaha G, Pena A, Chastre T, Caron C, et al. High doses of clopidogrel to overcome genetic resistance: the randomized crossover CLOVIS-2 (Clopidogrel and Response Variability Investigation Study 2). JACC Cardiovasc Interv. (2011) 4:392–402. doi: 10.1016/j.jcin.2011.03.002
160. Wallentin L, James S, Storey RF, Armstrong M, Barratt BJ, Horrow J, et al. Effect of CYP2C19 and ABCB1 single nucleotide polymorphisms on outcomes of treatment with ticagrelor versus clopidogrel for acute coronary syndromes: a genetic substudy of the PLATO trial. Lancet Lond Engl. (2010) 376:1320–8. doi: 10.1016/S0140-6736(10)61274-3
161. Sibbing D, Koch W, Gebhard D, Schuster T, Braun S, Stegherr J, et al. Cytochrome 2C19*17 allelic variant, platelet aggregation, bleeding events, and stent thrombosis in clopidogrel-treated patients with coronary stent placement. Circulation. (2010) 121:512–8. doi: 10.1161/CIRCULATIONAHA.109.885194
162. Craig R, Lee, Cameron D, Thomas, Amber L, Beitelshees, Sony, Tuteja, Philip E, Empey, James C, Lee, et al. Impact of the CYP2C19* 17 Allele on Outcomes in Patients Receiving Genotype-Guided Antiplatelet Therapy After Percutaneous Coronary Intervention. Available online at: https://pubmed-ncbi-nlm-nih-gov.proxy.insermbiblio.inist.fr/32897581/ (accessed September 27, 2021).
163. Simon T, Verstuyft C, Mary-Krause M, Quteineh L, Drouet E, Méneveau N, et al. Genetic determinants of response to clopidogrel and cardiovascular events. N Engl J Med. (2009) 360:363–75. doi: 10.1056/NEJMoa0808227
164. Taubert D, von Beckerath N, Grimberg G, Lazar A, Jung N, Goeser T, et al. Impact of P-glycoprotein on clopidogrel absorption. Clin Pharmacol Ther. (2006) 80:486–501. doi: 10.1016/j.clpt.2006.07.007
165. Notarangelo FM, Maglietta G, Bevilacqua P, Cereda M, Merlini PA, Villani GQ, et al. Pharmacogenomic approach to selecting antiplatelet therapy in patients with acute coronary syndromes: the PHARMCLO trial. J Am Coll Cardiol. (2018) 71:1869–77. doi: 10.1016/j.jacc.2018.02.029
166. Pereira NL, Farkouh ME, So D, Lennon R, Geller N, Mathew V, et al. Effect of genotype-guided oral P2Y12 inhibitor selection vs conventional clopidogrel therapy on ischemic outcomes after percutaneous coronary intervention: the TAILOR-PCI randomized clinical trial. JAMA. (2020) 324:761–71. doi: 10.1001/jama.2020.12443
167. Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, Funck-Brentano C, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. (2020). 41:407–77. doi: 10.1093/eurheartj/ehz425
168. Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation. (2011) 124:e574–e651. doi: 10.1161/CIR.0b013e31823a5596
169. Kernan WN, Ovbiagele B, Black HR, Bravata DM, Chimowitz MI, Ezekowitz MD, et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. (2014) 45:2160–236. doi: 10.1161/STR.0000000000000024
170. Ahmed N, Audebert H, Turc G, Cordonnier C, Christensen H, Sacco S, et al. Consensus statements and recommendations from the ESO-Karolinska Stroke Update Conference, Stockholm 11-13 November 2018. Eur Stroke J. (2019) 4:307–17. doi: 10.1177/2396987319863606
171. Siller-Matula JM, Francesconi M, Dechant C, Jilma B, Maurer G, Delle-Karth G, et al. Personalized antiplatelet treatment after percutaneous coronary intervention: the MADONNA study. Int J Cardiol. (2013) 167:2018–23. doi: 10.1016/j.ijcard.2012.05.040
172. Mayer K, Schulz S, Bernlochner I, Morath T, Braun S, Hausleiter J, et al. A comparative cohort study on personalised antiplatelet therapy in PCI-treated patients with high on-clopidogrel platelet reactivity. Results of the ISAR-HPR registry. Thromb Haemost. (2014) 112:342–51. doi: 10.1160/TH13-10-0874
173. Aradi D, Tornyos A, Pintér T, Vorobcsuk A, Kónyi A, Faluközy J, et al. Optimizing P2Y12 receptor inhibition in patients with acute coronary syndrome on the basis of platelet function testing: impact of prasugrel and high-dose clopidogrel. J Am Coll Cardiol. (2014) 63:1061–70. doi: 10.1016/j.jacc.2013.12.023
174. Sibbing D, Aradi D, Jacobshagen C, Gross L, Trenk D, Geisler T, et al. Guided de-escalation of antiplatelet treatment in patients with acute coronary syndrome undergoing percutaneous coronary intervention (TROPICAL-ACS): a randomised, open-label, multicentre trial. Lancet Lond Engl. (2017) 390:1747–57. doi: 10.1016/S0140-6736(17)32155-4
175. Tang Y-D, Wang W, Yang M, Zhang K, Chen J, Qiao S, et al. Randomized comparisons of double-dose clopidogrel or adjunctive cilostazol versus standard dual antiplatelet in patients with high posttreatment platelet reactivity: results of the CREATIVE trial. Circulation. (2018) 137:2231–45. doi: 10.1161/CIRCULATIONAHA.117.030190
176. Cayla G, Cuisset T, Silvain J, Leclercq F, Manzo-Silberman S, Saint-Etienne C, et al. Platelet function monitoring to adjust antiplatelet therapy in elderly patients stented for an acute coronary syndrome (ANTARCTIC): an open-label, blinded-endpoint, randomised controlled superiority trial. Lancet Lond Engl. (2016) 388:2015–22. doi: 10.1016/S0140-6736(16)31323-X
177. Trenk D, Stone GW, Gawaz M, Kastrati A, Angiolillo DJ, Müller U, et al. A randomized trial of prasugrel versus clopidogrel in patients with high platelet reactivity on clopidogrel after elective percutaneous coronary intervention with implantation of drug-eluting stents: results of the TRIGGER-PCI (Testing Platelet Reactivity In Patients Undergoing Elective Stent Placement on Clopidogrel to Guide Alternative Therapy With Prasugrel) study. J Am Coll Cardiol. (2012) 59:2159–64. doi: 10.1016/j.jacc.2012.02.026
178. Price MJ, Berger PB, Teirstein PS, Tanguay J-F, Angiolillo DJ, Spriggs D, et al. Standard- vs high-dose clopidogrel based on platelet function testing after percutaneous coronary intervention: the GRAVITAS randomized trial. JAMA. (2011) 305:1097–105. doi: 10.1001/jama.2011.290
179. Collet J-P, Cuisset T, Rangé G, Cayla G, Elhadad S, Pouillot C, et al. Bedside monitoring to adjust antiplatelet therapy for coronary stenting. N Engl J Med. (2012) 367:2100–9. doi: 10.1056/NEJMoa1209979
180. Cattaneo M, Cerletti C, Harrison P, Hayward CPM, Kenny D, Nugent D, et al. Recommendations for the standardization of light transmission aggregometry: a consensus of the working party from the platelet physiology subcommittee of SSC/ISTH. J Thromb Haemost. (2013) 11:1183–89. doi: 10.1111/jth.12231
181. Gum PA, Kottke-Marchant K, Welsh PA, White J, Topol EJ. A prospective, blinded determination of the natural history of aspirin resistance among stable patients with cardiovascular disease. J Am Coll Cardiol. (2003) 41:961–5. doi: 10.1016/S0735-1097(02)03014-0
182. Bliden KP, DiChiara J, Tantry US, Bassi AK, Chaganti SK, Gurbel PA. Increased risk in patients with high platelet aggregation receiving chronic clopidogrel therapy undergoing percutaneous coronary intervention: is the current antiplatelet therapy adequate? J Am Coll Cardiol. (2007) 49:657–66. doi: 10.1016/j.jacc.2006.10.050
183. Bagoly Z, Homoródi N, Kovács EG, Sarkady F, Csiba L, Édes I, et al. How to test the effect of aspirin and clopidogrel in patients on dual antiplatelet therapy? Platelets. (2016) 27:59–65. doi: 10.3109/09537104.2015.1031098
184. Bouman HJ, Parlak E, van Werkum JW, Breet NJ, ten Cate H, Hackeng CM, et al. Which platelet function test is suitable to monitor clopidogrel responsiveness? A pharmacokinetic analysis on the active metabolite of clopidogrel. J Thromb Haemost. (2010) 8:482–8. doi: 10.1111/j.1538-7836.2009.03733.x
185. Koziński M, Ostrowska M, Adamski P, Sikora J, Sikora A, Karczmarska-Wódzka A, et al. Which platelet function test best reflects the in vivo plasma concentrations of ticagrelor and its active metabolite? The HARMONIC study. Thromb Haemost. (2016) 116:1140–9. doi: 10.1160/TH16-07-0535
186. Lam H, Katyal N, Parker C, Natteru P, Nattanamai P, Newey CR, et al. Thromboelastography with platelet mapping is not an effective measure of platelet inhibition in patients with spontaneous intracerebral hemorrhage on antiplatelet therapy. Cureus. (2018) 10:e2515. doi: 10.7759/cureus.2515
187. Michelson AD, Bhatt DL. How I use laboratory monitoring of antiplatelet therapy. Blood. (2017) 130:713–21. doi: 10.1182/blood-2017-03-742338
188. Jilma B, Fuchs I. Detecting aspirin resistance with the platelet function analyzer (PFA-100). Am J Cardiol. (2001) 88:1348–9. doi: 10.1016/S0002-9149(01)02143-9
189. Mulliez SMN, Hallaert G, Van Roost D, Vantilborgh A, Devreese KMJ. Influence of platelet clumps on platelet function analyser (PFA)-200® testing. Int J Lab Hematol. (2015) 37:e103–e5. doi: 10.1111/ijlh.12337
190. Reny J-L, De Moerloose P, Dauzat M, Fontana P. Use of the PFA-100 closure time to predict cardiovascular events in aspirin-treated cardiovascular patients: a systematic review and meta-analysis. J Thromb Haemost. (2008) 6:444–50. doi: 10.1111/j.1538-7836.2008.02897.x
191. Lordkipanidzé M. Platelet function tests. Semin Thromb Hemost. (2016) 42:258–67. doi: 10.1055/s-0035-1564834
192. Hardy M, Dupuis C, Dincq A-S, Jacqmin H, Lecompte T, Mullier F, et al. Reduction of preoperative waiting time before urgent surgery for patients on P2Y12 inhibitors using multiple electrode aggregometry: a retrospective study. J Clin Med. (2020) 9:E424. doi: 10.3390/jcm9020424
193. Ferguson LP, Duong P, Pearce KF, Murphy P, Biss TT. Monitoring of antiplatelet therapy in children on ventricular assist device support: comparison of multiplate and thromboelastography platelet mapping. ASAIO J. (2019) 65:84–93. doi: 10.1097/MAT.0000000000000768
194. Li Y, Zhang X, Guo Z, Zhu J, Xu R, He Z, et al. Standard vs. modified antiplatelet therapy based on thromboelastography with platelet mapping for preventing bleeding events in patients undergoing stent-assisted coil for a ruptured intracranial aneurysm. Front Neurol. (2020) 11:615829. doi: 10.3389/fneur.2020.615829
195. Hranjec T, Estreicher M, Rogers B, Kohler L, Solomon R, Hennessy S, et al. Integral use of thromboelastography with platelet mapping to guide appropriate treatment, avoid complications, and improve survival of patients with coronavirus disease 2019-related coagulopathy. Crit Care Explor. (2020) 2:e0287. doi: 10.1097/CCE.0000000000000287
196. Lordkipanidzé M, Diodati JG, Schampaert E, Palisaitis DA, Pharand C. Prevalence of unresponsiveness to aspirin and/or clopidogrel in patients with stable coronary heart disease. Am J Cardiol. (2009) 104:1189–93. doi: 10.1016/j.amjcard.2009.06.025
197. Lordkipanidzé M, Pharand C, Nguyen TA, Schampaert E, Palisaitis DA, Diodati JG. Comparison of four tests to assess inhibition of platelet function by clopidogrel in stable coronary artery disease patients. Eur Heart J. (2008) 29:2877–85. doi: 10.1093/eurheartj/ehn419
198. Lordkipanidzé M, Pharand C, Schampaert E, Turgeon J, Palisaitis DA, Diodati JG. A comparison of six major platelet function tests to determine the prevalence of aspirin resistance in patients with stable coronary artery disease. Eur Heart J. (2007) 28:1702–8. doi: 10.1093/eurheartj/ehm226
199. Bor WL, Zheng KL, Tavenier AH, Gibson CM, Granger CB, Bentur O, et al. Pharmacokinetics, pharmacodynamics, and tolerability of subcutaneous administration of a novel glycoprotein IIb/IIIa inhibitor, RUC-4, in patients with ST-segment elevation myocardial infarction. EuroIntervention. (2021) 17:e401–e10. doi: 10.4244/EIJ-D-21-00287
200. Sinnaeve P, Fahrni G, Schelfaut D, Spirito A, Mueller C, Frenoux J-M, et al. Subcutaneous selatogrel inhibits platelet aggregation in patients with acute myocardial infarction. J Am Coll Cardiol. (2020) 75:2588–97. doi: 10.1016/j.jacc.2020.03.059
201. Voors-Pette C, Lebozec K, Dogterom P, Jullien L, Billiald P, Ferlan P, et al. Safety and tolerability, pharmacokinetics, and pharmacodynamics of ACT017, an antiplatelet GPVI (Glycoprotein VI) fab. Arterioscler Thromb Vasc Biol. (2019) 39:956–64. doi: 10.1161/ATVBAHA.118.312314
202. Schüpke S, Hein-Rothweiler R, Mayer K, Janisch M, Sibbing D, Ndrepepa G, et al. Revacept, a novel inhibitor of platelet adhesion, in patients undergoing elective PCI-design and rationale of the randomized ISAR-PLASTER trial. Thromb Haemost. (2019) 119:1539–45. doi: 10.1055/s-0039-1692423
Keywords: platelets, aspirin, P2Y12 receptor antagonists, cardiovascular disease, precision medicine, bleeding, surgery
Citation: Jourdi G, Godier A, Lordkipanidzé M, Marquis-Gravel G and Gaussem P (2022) Antiplatelet Therapy for Atherothrombotic Disease in 2022—From Population to Patient-Centered Approaches. Front. Cardiovasc. Med. 9:805525. doi: 10.3389/fcvm.2022.805525
Received: 30 October 2021; Accepted: 06 January 2022;
Published: 28 January 2022.
Edited by:
Joseph Aslan, Oregon Health and Science University, United StatesReviewed by:
Felice Gragnano, University of Campania Luigi Vanvitelli, ItalyThomas Pierre Lecompte, Université de Genève, Switzerland
Copyright © 2022 Jourdi, Godier, Lordkipanidzé, Marquis-Gravel and Gaussem. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Georges Jourdi, Z2Vvcmdlcy5lbC5qZXJkaS1qb3VyZGlAdW1vbnRyZWFsLmNh