 Daniel L. Underberg
Daniel L. Underberg Adovich S. Rivera
Adovich S. Rivera Arjun Sinha
Arjun Sinha Matthew J. Feinstein
Matthew J. Feinstein- 1Division of Cardiology, Department of Medicine, Chicago, IL, United States
- 2Department of Preventive Medicine, Chicago, IL, United States
- 3Department of Pathology, Northwestern University Feinberg School of Medicine, Chicago, IL, United States
Objective: Characterize incident heart failure (HF) phenotypes among patients with various chronic inflammatory diseases (CIDs).
Background: Several CIDs are associated with increased HF risk, but differences in HF phenotypes across CIDs are incompletely understood. No prior studies to our knowledge have manually adjudicated HF phenotypes across a CID spectrum.
Methods: We screened for patients with—and controls without—CIDs who had possible HF, then hand-adjudicated HF endpoints. Possible HF resulted from a single HF administrative code; HF was deemed definite/probable vs. absent using standardized, validated criteria. We queried adjudicated HF patients' charts to define specific HF phenotypes, then compared clinical, demographic, and HF phenotypic characteristics for HF patients with specific CIDs vs. non-CID controls using Fisher's exact test.
Results: Out of 415 possible HF patients, 192 had definite/probable HF. Significant differences in HF phenotypes existed across CIDs. Isolated right-sided HF was present in 27.8% of patients with SSc and adjudicated HF, which is more than twice as common as it was in any other CID. Left ventricular systolic dysfunction was most common in patients with HIV and lupus (SLE); mean LVEF was 45.0% ± 18.6% for HIV and 41.3% ± 17.1% for SLE, but was 57.7% ± 10.7% for SSc. Those with HIV and multiple CIDs were most likely to have coronary artery disease.
Conclusions: Different CIDs present with different phenotypes of physician-adjudicated HF, potentially reflecting different underlying inflammatory pathophysiologies. Larger studies are needed to confirm these findings, as are mechanistic studies focused on understanding specific immunoregulatory contributors to HF.
Introduction
Chronic inflammation plays a central role in the pathogenesis of myocardial dysfunction and heart failure (HF) (1). Yet, despite accumulating scientific evidence of the role of inflammation in HF, therapies targeting inflammation in HF treatment (2) and prevention (3) have yielded mixed results. Several reasons for this gap between scientific knowledge and practice exist, including biologic heterogeneity of heart failure phenotypes and the heterogeneity of inflammatory processes in time (even within an individual) and space (e.g., systemic vs. tissue-specific inflammation). Disentangling this heterogeneity offers the potential for useful diagnostic and therapeutic targets in HF prevention and treatment. Several human “models” of systemic and tissue-specific inflammation—chronic inflammatory diseases (CIDs) including but not limited to systemic lupus erythematosus (SLE), systemic sclerosis (SSc), and human immunodeficiency virus (HIV)—are associated with increased HF risk (4). While prior studies have yielded useful general insights into specific CIDs and incident HF, none to our knowledge have adjudicated HF subtypes and phenotypic presentations [which are essential for confirming accurate HF diagnoses given the discordance between administrative codes for HF and physician-adjudicated HF (5, 6)] to produce phenotype-specific insights. In this study, we individually adjudicated incident HF events and compared incident HF phenotypes in a large cohort of CID patients and controls.
Methods
Cohort Creation and Validation
Using electronic health record-based data stored in the Northwestern Medicine Enterprise Data Warehouse (NMEDW) (Northwestern University Clinical and Translational Sciences Institute, Chicago, Illinois), a large cohort of patients with CIDs and non-CID controls receiving regular outpatient care was created. Regular outpatient care was defined as at least one in-person outpatient visit every 2 years during the period of observation (1/1/2000 to 1/1/2019) in a large urban medical system. The NMEDW stores clinical observations of >6.6 million people, and its external validity is demonstrated by the fact that previous investigations of HIV-associated cardiovascular disease using this database yielded findings comparable to those of multicenter U.S. HIV cohorts (7–10). The institutional review board at Northwestern University approved the cohort creation and research protocol for this study.
We identified adults 18 years of age and older with CIDs during the above stated period of observation by using the following validated criteria: for SSc (11), inflammatory bowel disease (IBD) (12–15) and psoriasis (Pso) (16, 17), 2 or more International Classification of Diseases-9th Edition (ICD-9) or ICD-10 diagnostic codes were required within a 2-year period; for SLE, 3 diagnostic codes were required in 3 separate months (18, 19); for RA, 2 diagnostic codes and a prescription for a disease-modifying antirheumatic drug were required (20–22). To diagnose HIV, we adapted a previous approach (23) that factored in plasma HIV RNA (viral load), serology, and/or at least 3 instances in which both HIV viral load and CD4 T lymphocyte cell count (CD4) were ordered on the same date. We frequency matched non-CID controls with patients with CIDs based on several demographic factors (age, sex, insurance status) as well as baseline year and the presence or absence of hypertension and/or diabetes at baseline.
We obtained demographic and insurance data from patients' most recent clinical visits. We used an evidence-based approach to define baseline hypertension as the presence of 1 administrative code (ICD-9 401 to 405 and ICD-10 I10 to I15) anytime prior to 1 year after the baseline date (24, 25). Given the heterogeneity of practice settings and potential for sphygmomanometer miscalibration that has been demonstrated in prior studies (26, 27), blood pressure values themselves were not used to define hypertension. We identified baseline diabetes using a combination of validated ICD-9 or ICD-10 administrative codes (ICD-9 250 and ICD-10 E10-, E11, and E13) and either hemoglobin A1c >6.5% or prescription of antidiabetic medications anytime prior to 1 year after the baseline date (28). The presence of coronary artery disease (CAD) was determined by manual chart review, and was defined as present if it was mentioned in at least 1 note written by either an Internal Medicine or Cardiology specialist in the patient's electronic health record.
Adjudication
Our adjudication protocol was based on a method we previously adapted from the Multi-Ethnic Study of Atherosclerosis for adjudicating events in electronic health records-based cohorts (29). As incident HF was the primary outcome of interest in this study, we used intentionally sensitive screening criteria in our CID and non-CID cohorts to define this; patients were deemed to have “possible heart failure” based on a single inpatient or outpatient administrative code (ICD-9 codes 398.91, 402.01, 402.11, 402.91, 404.01, 404.03, 404.11, 404.13, 404.91, 404.93, 425, 428, 429 or ICD-10 codes I42, I43, or I50). Only HF events coded >1 year after baseline were consideredw incident diagnoses in order to minimize the likelihood of misclassifying prevalent but not yet recorded HF as incident HF; importantly, HF events coded within the first year after baseline were considered baseline. Patients deemed to have HF at baseline and those with missing baseline demographic data were excluded.
Patients who screened positive for “possible heart failure” subsequently underwent manual chart review to determine whether “probable heart failure” was present at the time of incident HF diagnosis. This designation was based on fulfilling all 3 of the following criteria: (1) the patient had signs or symptoms of HF (shortness of breath, lower extremity swelling, or jugular venous distension not attributable to a clear other cause); (2) the physician diagnosed HF (by mentioning “heart failure” or “volume/fluid overload” in the setting of objective criteria on echocardiogram [EF <55% or ≥ grade II diastolic diastolic dysfunction] or other superseding diagnoses including “severe valvular disease” or other “cardiomyopathy”); and (3) the patient was prescribed medication for HF (beta-blockers, angiotensin II converting enzyme inhibitors, angiotensin receptor blockers, mineralocorticoid antagonists, angiotensin receptor-neprilysin inhibitors, or diuretics).
Patients screening positive for “probable heart failure” underwent further manual chart review to determine whether “definite heart failure” was present at the time of incident HF diagnosis. This designation was made by fulfilling at least 1 of the following criteria: (1) chest x-ray showed signs of volume overload; (2) echocardiogram showed evidence of HF; or (3) BNP or NT-proBNP was consistent with HF (using age-adjusted cutoff values of ≥450 for age <50, ≥900 for age 50–75, and ≥1,800 for age >75). Echocardiographic evidence of HF was defined as meeting at least 1 of the following criteria, based on the lowest values seen on echocardiogram within 1 month of incident HF diagnosis: (1) left ventricular ejection fraction <50; (2) wall motion abnormalities; (3) left ventricular systolic dysfunction (chamber dilation or left ventricular end diastolic volume index >97 ml/m2); (4) diastolic dysfunction (left ventricular end diastolic pressure >16mmHg, pulmonary capillary wedge pressure >12mmHg, E/E' >15, or left atrial volume index >34ml/m2); (5) moderate-severe valvular disease; or (6) evidence of right ventricular failure (depressed systolic function, dilation, or evidence of pressure/volume overload). Definite and probable HF events were combined and considered HF events for the purpose of these analyses. In addition to determining whether HF was present or absent, we adjudicated phenotype-related factors, such as the presence or absence of CAD (as previously specified) and right vs. left-sided HF (based on echocardiographic parameters), as well as whether or not the patient received a cardiac MRI.
Statistical Analyses
Our analyses focused on phenotypic differences among individuals with HF, which we determined by physician adjudication, rather than factors associated with incident HF. Therefore, our entire sub-cohort analyzed had adjudicated HF; our central analyses were performed without additional adjustment for HF risk factors because all individuals had HF, and because the stratified, CID-specific nature of the analyses limited our power for additional stratification or adjustment. Nevertheless, key demographic and clinical covariates were reviewed to assist with interpretation; these are provided along with the central analyses in Table 1 and are discussed in the results. The co-primary endpoints, compared across CIDs and vs. non-CID controls, were percentage (%) of individuals within a particular CID group with each of the following phenotypic presentations of HF: Isolated (1) left- or (2) right-sided HF, (3) combined left- and right-sided HF, and (4) left ventricular ejection fraction on echocardiography. For each of these variables, we performed analysis of variance (ANOVA) across CID/non-CID control groups with subsequent post-hoc Fisher's exact tests due to limited sample size for each CID/HF sub-group.
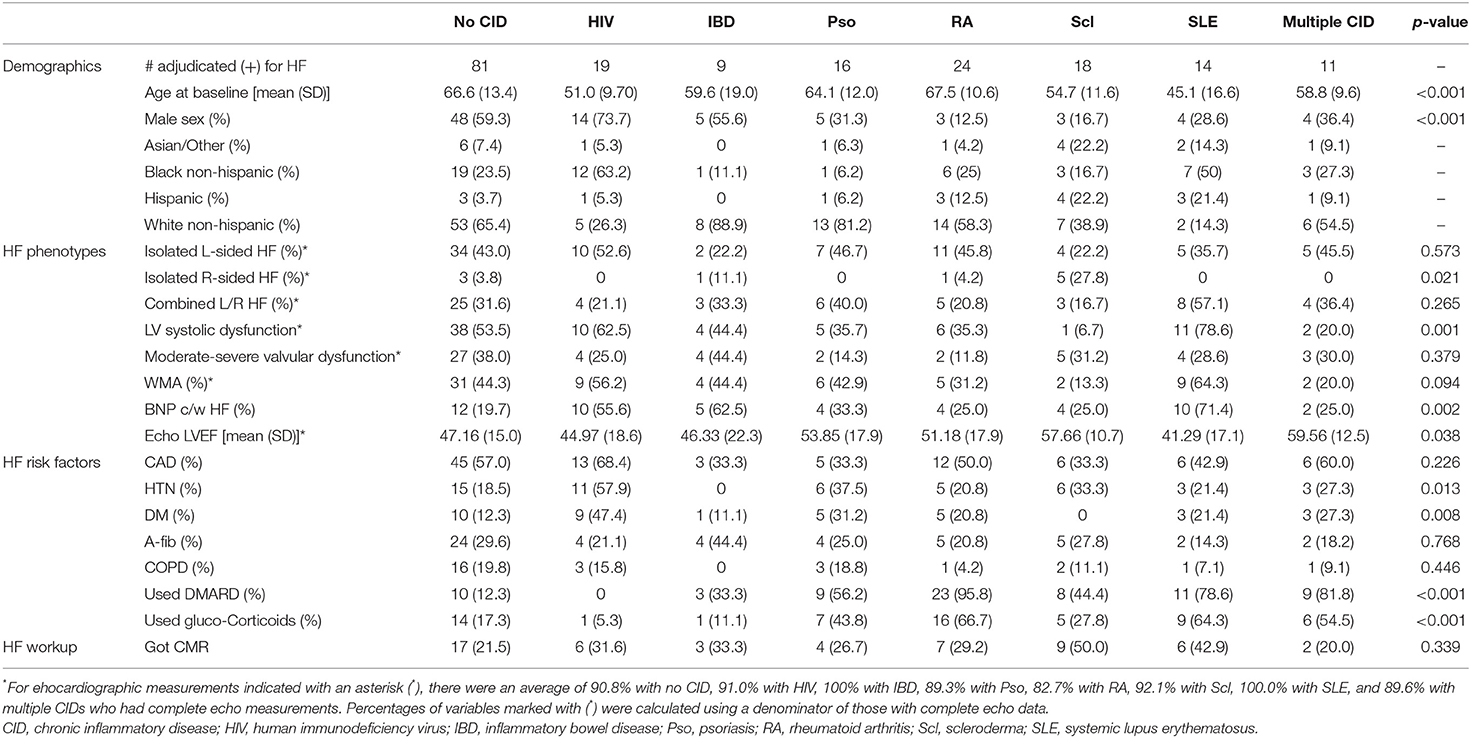
Table 1. Heart failure demographics, phenotypes, risk factors, and workup among patients with and without chronic inflammatory diseases who adjudicated positive for heart failure.
Results
Out of 415 patients with CIDs and controls with at least one administrative code for HF, 192 had definite/probable HF, consistent with expected high false positivity screening rates of our intentionally sensitive approach to screening for possible HF events. We observed significant differences in HF phenotypes across CIDs (Table 1). Isolated right-sided HF was present in 27.8% of patients with SSc and adjudicated HF, which is more than twice as common as it was in any other CID. Left ventricular systolic dysfunction was most common in patients with HIV and SLE; mean LVEF was 45.0 ± 18.6% for HIV and 41.3 ± 17.1% for SLE, whereas it was 57.7 ± 10.7% for SSc. CAD was most prevalent in those with adjudicated HF who had HIV (68.4% of patients with HIV and HF had CAD) and multiple CIDs (60% of patients with multiple CIDs had CAD). Hypertension and diabetes were also most common in adjudicated HF patients with HIV (present in 57.9 and 47.4% of patients with HIV, respectively). We did not observe significant differences in the prevalence of isolated left-sided HF or atrial fibrillation between the various CIDs.
In a secondary analysis comparing proportions of each CID group that had HF with preserved ejection fraction (HFpEF) as the presentation of HF, SSc (in which 66.7% of HF cases were adjudicated as HFpEF) and Pso (60.0%) had the highest proportion of HFpEF, whereas only 38.0% of non-CID controls with HF had HFpEF.
Discussion
We adjudicated HF events in a large cohort of CID patients and controls and identified significant differences in adjudicated HF subtypes across CIDs. This represents the first study to our knowledge that individually adjudicated HF events and phenotypes in a cohort examining patients with a spectrum of CIDs.
We observed that isolated right-sided HF was much more common in SSc than in any other CID, and that left ventricular systolic dysfunction was more common in HIV and SLE. There was no significant difference in the rate of isolated left-sided HF across the spectrum of CIDs, however. Our findings substantiate previously postulated (4, 30, 31) CID-specific HF phenotypes, with our study adding the value of enabling comparison across CIDs in a single cohort and presenting physician-adjudicated assessment and phenotyping of HF, which may be more accurate than administrative code-based definitions (32). Additionally, although pulmonary hypertension—a key contributor to right-sided HF—is common in several CIDs including SSc, HIV, and SLE, we observed a stark difference whereby SSc patients with HF had a several-fold higher likelihood of isolated right-sided HF than patients with any other CID and HF. Whether these differences reflect unique heart-lung physiology and fibrotic mediators arising in SSc warrants further study. Moreover, although several CIDs (including HIV, RA, and SLE) are associated with heightened atherothrombotic risk, HF patients with HIV had an especially high prevalence of underlying CAD; this adds to recently reported data revealing a higher rate of CAD in patients with SLE and SSc (33), and substantiates prior reports highlighting HIV's association with acute coronary syndrome (34).
Although these findings yield interesting CID-specific insights into HF presentation and, perhaps, underlying pathophysiologies, they require confirmation in larger, multi-center studies as one of the limitations of our current work is the relatively small sample size. Such analyses would offer the benefit of providing CID-specific insights into HF risk and pathophysiology.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Northwestern University IRB. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
DU, AS, and MF constituted the team that conceptualized the project, collected and reviewed the data, and wrote and edited the final manuscript. AR assisted with statistical analyses. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by the National Institutes of Health R01 HL 156592 (to MF).
Conflict of Interest
MF was employed by Consultant/Advisory Board, Novartis AG.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We thank the Northwestern Medicine Enterprise Data Warehouse.
References
1. Paulus WJ, Tschope C. A novel paradigm for heart failure with preserved ejection fraction. JACC. (2013) 62:263–71. doi: 10.1016/j.jacc.2013.02.092
2. Mann DL. Innate immunity and the failing heart: the cytokine hypothesis revisited. Circ Res. (2015) 116:1254–68. doi: 10.1161/CIRCRESAHA.116.302317
3. Adamo L, Rocha-Resende C, Prabhu SD, Mann DL. Reappraising the role of inflammation in heart failure. Nat Rev Cardiol. (2020) 17:269–85. doi: 10.1038/s41569-019-0315-x
4. Prasada S, Rivera A, Nishtala A, Pawlowski AE, Sinha A, Bundy JD, et al. Differential association of chronic inflammatory diseases with incident heart failure. JACC: Heart Failure. (2020) 8:489–98. doi: 10.1016/j.jchf.2019.11.013
5. Quach S, Blais C, Quan H. Administrative data have high variation in validity for recording heart failure. Can J Cardiol. (2010) 26:306–12. doi: 10.1016/S0828-282X(10)70438-4
6. Steverson AB, Pawlowski AE, Schneider D, Nannapaneni P, Sanders JM, Achenbach CJ, et al. Clinical characteristics of HIV-infected patients with adjudicated heart failure. Eur J Prev Cardiol. (2017) 24:1746–58. doi: 10.1177/2047487317732432
7. Feinstein MJ, Hsue PY, Benjamin LA, Bloomfield GS, Currier JS, Frieberg MS, et al. Characteristics, prevention, and management of cardiovascular disease in people living with HIV: a scientific statement from the American Heart Association. Circulation. (2019) 140:e98–124. doi: 10.1161/CIR.0000000000000695
8. Sanders JM, Steverson AB, Pawlowski AE, Schneider D, Achenbach CJ, Lloyd-Jones DM, et al. Atrial arrhythmia prevalence and character- istics for human immunodeficiency virus-infected persons and matched uninfected controls. PLoS ONE. (2018) 13:e0194754. doi: 10.1371/journal.pone.0194754
9. Freiberg MS, Chang CH, Skanderson M, Patterson OV, DuVall SL, Brandt CA, et al. Association between HIV infection and the risk of heart failure with reduced ejection fraction and preserved ejection fraction in the antiretroviral therapy era: results from the Veterans Aging Cohort study. JAMA Cardiol. (2017) 2:536–46. doi: 10.1001/jamacardio.2017.0264
10. Hsu JC Li Y, Marcus GM, Hsue PY, Scherzer R, Grunfield C, et al. Atrial fibrillation and atrial flutter in human immunodeficiency virus-infected persons: incidence, risk factors, and association with markers of HIV disease severity. J Am Coll Cardiol. (2013) 61:2288–95. doi: 10.1016/j.jacc.2013.03.022
11. Valenzuela A, Yaqub A, Fiorentino D, Krishnan E, Chung L. Validation of the ICD-9-CM code for systemic sclerosis using updated ACR/EULAR classification criteria. Scand J Rheumatol. (2015) 44:253–5. doi: 10.3109/03009742.2015.1008038
12. Ma C, Moran GW, Benchimol EI, Targownik LE, Heitman SJ, Hubbard JN, et al. Surgical rates for Crohn's disease are decreasing: a population-based time trend analysis and validation study. Am J Gastroenterol. (2017) 112:1840–8. doi: 10.1038/ajg.2017.394
13. Thirumurthi S, Chowdhury R, Richardson P, Abraham NS. Validation of ICD-9-CM diagnostic codes for inflammatory bowel disease among veterans. Dig Dis Sci. (2010) 55:2592–8. doi: 10.1007/s10620-009-1074-z
14. Hou JK, Tan M, Stidham RW, Colozzi J, Adams D, El-Serag H, et al. Accuracy of diagnostic codes for identifying patients with ulcerative colitis and Crohn's disease in the Veterans Affairs Health Care System. Dig Dis Sci. (2014) 59:2406–10. doi: 10.1007/s10620-014-3174-7
15. Park S, Chun J, Han KD, Soh H, Choi K, Kim JH, et al. Increased end-stage renal disease risk in patients with inflammatory bowel disease: a nationwide population-based study. World J Gastroenterol. (2018) 24:4798–808. doi: 10.3748/wjg.v24.i42.4798
16. Lofvendahl S, Theander E, Svensson A, Carlsson KS, Englund M, Petersson IF. Validity of diagnostic codes and prevalence of physician- diagnosed psoriasis and psoriatic arthritis in southern Sweden—a population-based register study. PLoS ONE. (2014) 9:e98024. doi: 10.1371/journal.pone.0098024
17. Asgari MM, Wu JJ, Gelfand JM, Salman C, Curtis JR, Harrold LR, et al. Validity of diagnostic codes and prevalence of psoriasis and psoriatic arthritis in a managed care population, 1996–2009. Pharmacoepidemiol Drug Saf. (2013) 22:842–9. doi: 10.1002/pds.3447
18. Walunas TL, Jackson KL, Chung AH, Mancera-Cuevas KA, Erickson DL, Ramsey-Goldman R, et al. Disease outcomes and care fragmentation among patients with systemic lupus erythematosus. Arthritis Care Res (Hoboken). (2017) 69:1369–76. doi: 10.1002/acr.23161
19. Chibnik LB, Massarotti EM, Costenbader KH. Identification and validation of lupus nephritis cases using administrative data. Lupus. (2010) 19:741–3. doi: 10.1177/0961203309356289
20. Jafri K, Taylor L, Nezamzadeh M, Baker JF, Mehta NN, Bartels C, et al. Management of hyperlipidemia among patients with rheumatoid arthritis in the primary care setting. BMC Musculoskelet Disord. (2015) 16:237. doi: 10.1186/s12891-015-0700-5
21. Kim SY, Servi A, Polinski JM, Mogun H, Weinblatt ME, Katz JN, et al. Validation of rheumatoid arthritis diagnoses in health care utilization data. Arthritis Res Ther. (2011) 13:R32. doi: 10.1186/ar3260
22. Singh JA, Holmgren AR, Noorbaloochi S. Accuracy of Veterans Administration databases for a diagnosis of rheumatoid arthritis. Arthritis Rheum. (2004) 51:952–7. doi: 10.1002/art.20827
23. Felsen UR, Bellin EY, Cunningham CO, Zingman BS. Development of an electronic medical record-based algorithm to identify patients with unknown HIV status. AIDS Care. (2014) 26:1318–25. doi: 10.1080/09540121.2014.911813
24. Pace R, Peters T, Rahme E, Dasgupta K. Validity of health administrative database definitions for hypertension: a systematic review. Can J Car- diol. (2017) 33:1052–9. doi: 10.1016/j.cjca.2017.05.025
25. Teixeira PL, Wei WQ, Cronin RM, Mo H, VanHouten JP, Carroll RJ, et al. Evaluating electronic health record data sources and algorithmic approaches to identify hypertensive individuals. J Am Med Inform Assoc. (2017) 24:162–71. doi: 10.1093/jamia/ocw071
26. Ali S, Rouse A. Practice audits: reliability of sphygmomanometers and blood pressure recording bias. J Hum Hypertens. (2002) 16:359–61. doi: 10.1038/sj.jhh.1001384
27. Rouse A, Marshall T. The extent and implications of sphygmomanometer calibration error in primary care. J Hum Hypertens. (2001) 15:587–91. doi: 10.1038/sj.jhh.1001241
28. Wilke RA, Berg RL, Peissig P, Kitchner T, Sijercic B, McCarty CA, et al. Use of an electronic medical record for the identification of research subjects with diabetes mellitus. Clin Med Res. (2007) 5:1–7. doi: 10.3121/cmr.2007.726
29. Patel RB, Colangelo LA, Bielinski SJ, Larson NB, Ding J, Allen NB, et al. Circulating vascular cell adhesion molecule-1 and incident heart failure: the Multi-Ethnic Study of Atherosclerosis (MESA). J Am Heart Assoc. (2020) 9:e019390. doi: 10.1161/JAHA.120.019390
30. Wright K, Crowson CS, Gabriel SE. Cardiovascular comorbidity in rheumatic diseases: a focus on heart failure. Heart Failure Clin. (2014) 10:339–52. doi: 10.1016/j.hfc.2013.10.003
31. Dimitroulas T, Giannakoulas G, Karvounis H, Garyfallos A, Settas L, Kitas GD. Micro- and macrovascular treatment targets in scleroderma heart disease. Curr Pharm Des. (2014) 20:536–44. doi: 10.2174/13816128113199990555
32. Feinstein MJ, Steverson AB, Ning H, Pawlowski AE, Schneider D, Ahmad FS, et al. Adjudicated heart failure in HIV-infected and un-infected men and women. J Am Heart Assoc. (2018) 7:e009985. doi: 10.1161/JAHA.118.009985
33. Sinha A, Rivera AS, Chadha SA, Prasada S, Pawlowski AE, Thorp E, et al. Comparative risk of incident coronary heart disease across chronic inflammatory diseases. Front Cardiovasc Med. (2021) 8:757738. doi: 10.3389/fcvm.2021.757738
Keywords: heart failure, coronary artery disease, chronic inflammation, adjudication, HIV
Citation: Underberg DL, Rivera AS, Sinha A and Feinstein MJ (2022) Phenotypic Presentations of Heart Failure Among Patients With Chronic Inflammatory Diseases. Front. Cardiovasc. Med. 9:784601. doi: 10.3389/fcvm.2022.784601
Received: 28 September 2021; Accepted: 24 January 2022;
Published: 16 March 2022.
Edited by:
Günther Silbernagel, Medical University of Graz, AustriaReviewed by:
Aitor Aguirre, Michigan State University, United StatesErik Josef Behringer, Loma Linda University, United States
Copyright © 2022 Underberg, Rivera, Sinha and Feinstein. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Matthew J. Feinstein, bWF0dGhld2pmZWluc3RlaW5Abm9ydGh3ZXN0ZXJuLmVkdQ==