
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Cardiovasc. Med. , 06 January 2023
Sec. Cardiac Rhythmology
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.1099014
This article is part of the Research Topic Wearable Devices for Cardiac Rhythm Monitoring, Volume II View all 11 articles
 Maarten A. Koole1,2,3
Maarten A. Koole1,2,3 Dirkjan Kauw4
Dirkjan Kauw4 Kirsten M. Kooiman1
Kirsten M. Kooiman1 Joris R. de Groot1
Joris R. de Groot1 Danielle Robbers-Visser1Igor I. Tulevski2Barbara J. Mulder1
Danielle Robbers-Visser1Igor I. Tulevski2Barbara J. Mulder1 Berto J. Bouma1
Berto J. Bouma1 Mark J. Schuuring1,5,6*
Mark J. Schuuring1,5,6*Background: The European Society of Cardiology (ESC) guidelines for the management of adult congenital heart disease (ACHD) recommend screening in patients at risk for arrhythmic events. However, the optimal mode of detection is unknown.
Methods: Baseline and follow-up data of symptomatic ACHD patients who received an implantable loop recorder (ILR) or who participated in a smartphone based single-lead electrocardiogram study were collected. The primary endpoint was time to first detected arrhythmia.
Results: In total 116 ACHD patients (mean age 42 years, 44% male) were studied. The ILR group (n = 23) differed from the smartphone based single-lead electrocardiogram group (n = 93) in having a greater part of males and had more severe CHD and (near) syncope as qualifying diagnosis. In the smartphone based single-lead electrocardiogram group history of arrhythmia and palpitations were more frequent (all p < 0.05). Monitoring was performed for 40 and 79 patient-years for the ILR- and smartphone based single-lead electrocardiogram group, respectively. Arrhythmias occurred in 33 patients with an equal median time for both groups to first arrhythmia of 3 months (HR of 0.7, p = 0.81). Furthermore, atrial fibrillation occurred most often (n = 16) and common therapy changes included medication changes (n = 7) and implantation of pacemaker or Implantable Cardioverter Defibrillator (ICD) (N = 4). Symptoms or mode of detection were not a determinant of the first event.
Conclusion: Non-invasive smartphone based single-lead electrocardiogram monitoring could be an acceptable alternative for ILR implantation in detecting arrhythmia in symptomatic ACHD patients in respect to diagnostic yield, safety and management decisions, especially in those without syncope.
Congenital heart disease has a worldwide prevalence of ∼9 per 1000 newborns. Nowadays, the number of adult congenital heart disease (ACHD) patients exceeds the number of children with congenital heart disease and the population of ACHD patients is still increasing by 5% per year (1, 2). These ACHD patients are under lifelong surveillance in specialized centers. Although their prognosis has significantly improved compared to only a few decades ago, these patients are not cured. Data from the Dutch National CONCOR registry showed that the median age of death is 49 years and that two third of adult patients with CHD die from a cardiac cause (3–6). One of the most common causes of death is sudden cardiac death (19%), which occurs at a median age of 39 years (3, 4, 7). It is estimated that 1 out of 6 ACHD patients develops bradycardias or tachyarrhythmia during life, that often precede syncope and/or sudden death (3). Over one-third of tetralogy of Fallot (ToF) patients develop symptomatic atrial tachyarrhythmia by adulthood, 10% develop high-grade ventricular arrhythmia, and 5% require a pacemaker implantation for surgically acquired atrioventricular block or sinus node dysfunction. After Senning or Mustard repairs for Transposition of the Great Arteries (TGA), loss of sinus rhythm occurs in 60% of patients in the 20-year period after surgery (8).
The European Society of Cardiology (ESC) guidelines recommend periodical screening in symptomatic ACHD patients, without arrhythmia documentation at presentation, evaluation for arrhythmia (1). Subgroups of patients who are at increased risk are identified in the guideline. In patients with pacemakers or implantable cardioverter defibrillators (ICDs), device interrogation is used to screen for arrhythmias (9, 10). In patients without implantable device, short term screening is commonly performed with Holter studies, and prolonged screening with Implantable Loop Recorders (ILR). However, smartphone based single-lead electrocardiogram solutions may provide new alternatives (11, 12). Mobile devices for heart rhythm monitoring, defined as ambulant diagnostics, is rapidly evolving as wearables, mobile health applications (apps) and smartphone possibilities are improving, and increasing in number (13–15). ACHD patients seem particularly eligible to benefit from these alternative solutions, as these patients have a higher burden of arrhythmia compared to the general population and having their first arrhythmia at younger age. So they are generally well motivated to apply eHealth. However, data on smartphone based single-lead electrocardiogram are scarce. Therefore, the study aimed to explore whether smartphone based single-lead electrocardiogram can be a good alternative to ILR in detecting arrhythmia.
Baseline and follow-up data were collected of two cohorts of ACHD patients with symptoms which could be caused by arrhythmia. One cohort were patients who participated in a smartphone based single-lead electrocardiogram study and the other cohort are patients gathered by a retrospective chart review of patients with an ILR. Indications for ILR implantation were symptoms which could be related to arrhythmia. The smartphone based single-lead electrocardiogram group of patients participated in a prospective study in two medical centers in the Netherlands (Haga Teaching Hospital and Amsterdam UMC, location AMC). The study protocol required routine evaluation of heart rhythm using a wireless pocket-sized single lead EKG recording device that could record a 30 s single lead EKG (Kardia, AliveCor). After a 1-week run-in period, a single lead EKG was recorded once every week. Patients could perform extra measurements in case of symptoms. Data of events were sent by the application of the smartphone to our telemedicine center and within 48 h judged by specialized nurses. Data of the ILR were read as soon as possible after an event at our outpatient clinic. All patients were explained to contact a physician directly in case of emergency. Detailed description of the study has been published elsewhere (15). A retrospective chart review has been performed to collect ILR data of all symptomatic ACHD patients having an ILR implanted between 2003 and 2019 (Amsterdam UMC, location AMC).
The smartphone based single-lead electrocardiogram study ACHD patients were eligible for inclusion if they met the following inclusion criteria: palpitations within the last 3 years (with or without arrhythmia diagnosis) or HF NYHA class ≥ II, and possession of a smartphone. Patients with impaired cognition, as assessed by their treating physician, tremors or patients with an insurance not covering costs of the smartphone based single-lead electrocardiogram program, were excluded. Patients were recruited from the outpatient clinic and clinical wards. Enrollment in this study followed after informed consent for the use of their clinical data was acquired. The local medical ethics committees of both institutions issued a waiver for this study. This included a waived consent for the retrospective chart review, because data were processed anonymously by the investigator.
The primary endpoint was time to first arrhythmia detected (AF, SVT, VT, sinus node defect, or AV block) in both study groups. Device implantation and change in medication were not an outcome but also registered as a result of detecting arrhythmia for both groups. Data were analyzed with Kaplan-Meier survival curves and Cox proportional hazard analysis (SPSS version 28, IBM, Armonk, New York, NY, USA). Chi-square test or independent t-test were used to assess differences between patient-groups.
In total 116 ACHD patients were studied, see Table 1. Mean age was 42 years and 44% were male. There were 25 (22%) patients with mild CHD, 45 (39%) patients with moderate CHD, and 46 (39%) patients with severe CHD. The rate of hypertension (n = 16, 14%) or coronary artery disease was low (n = 7, 6%). The ILR group consisted of 23 patients and the smartphone based single-lead electrocardiogram consisted of 93 patients.
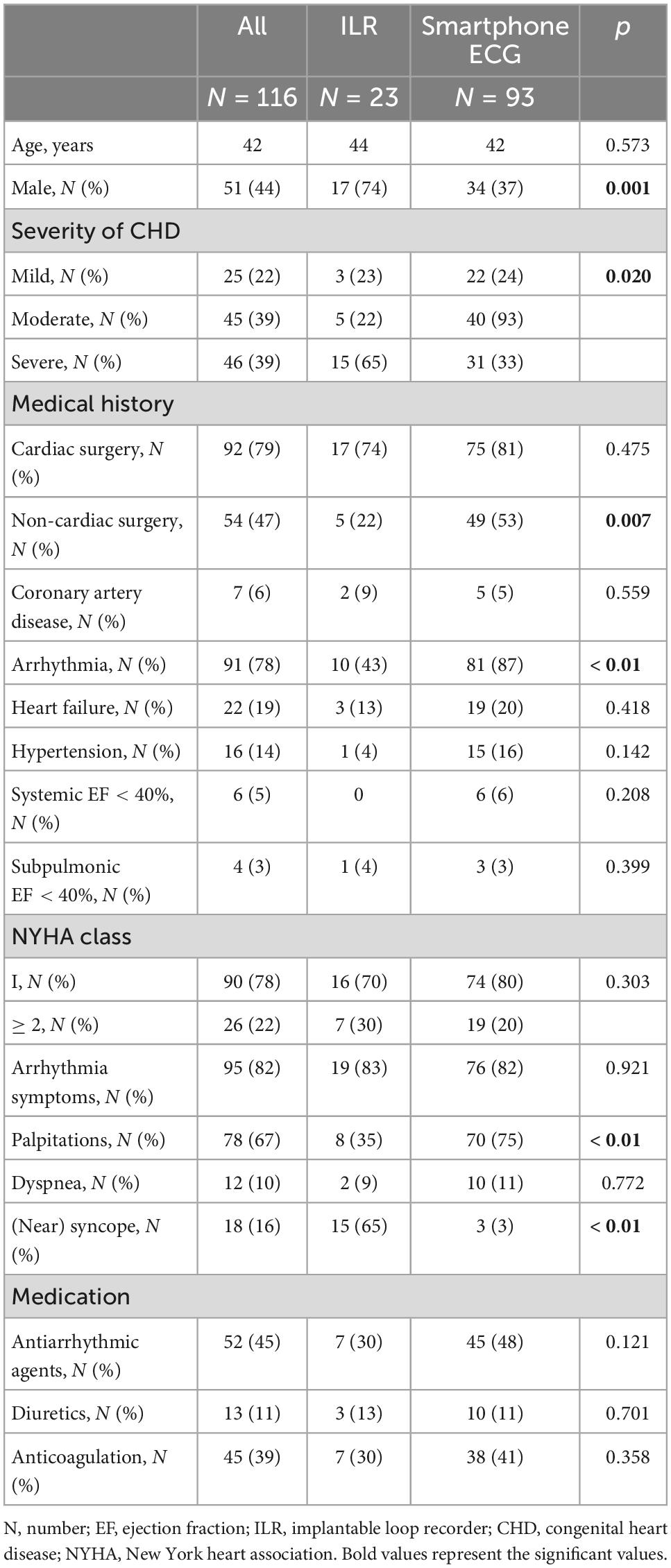
Table 1. Baseline characteristics.
The ILR group (n = 23) differed from the smartphone based single-lead electrocardiogram group (n = 93) in having a greater part of males. They had more severe CHD and (near) syncope (65 vs. 3%) as qualifying symptom of possible arrhythmia. In the smartphone based single-lead electrocardiogram group history of arrhythmia and suffering from palpitations were more frequent.
In total patients were monitored for 119 patient years. Monitoring was performed for 40 and 79 patient years, respectively, in the ILR and smartphone based single-lead electrocardiogram groups. The median time to first arrhythmia was 92 (16–233) days for the complete study cohort, for the ILR group 40 (15–681) days and for the smartphone based single-lead electrocardiogram group 102 (21–232) days (p = 0.80, HR of 0.7) (Figure 1 and Table 2). Arrhythmias occurred in 33 patients, of which 11 (48%) were documented in the ILR group and 22 (24%) in the smartphone based single-lead electrocardiogram group (p = 0.021). In both groups atrial fibrillation was the most frequently documented arrhythmia and no patient died.
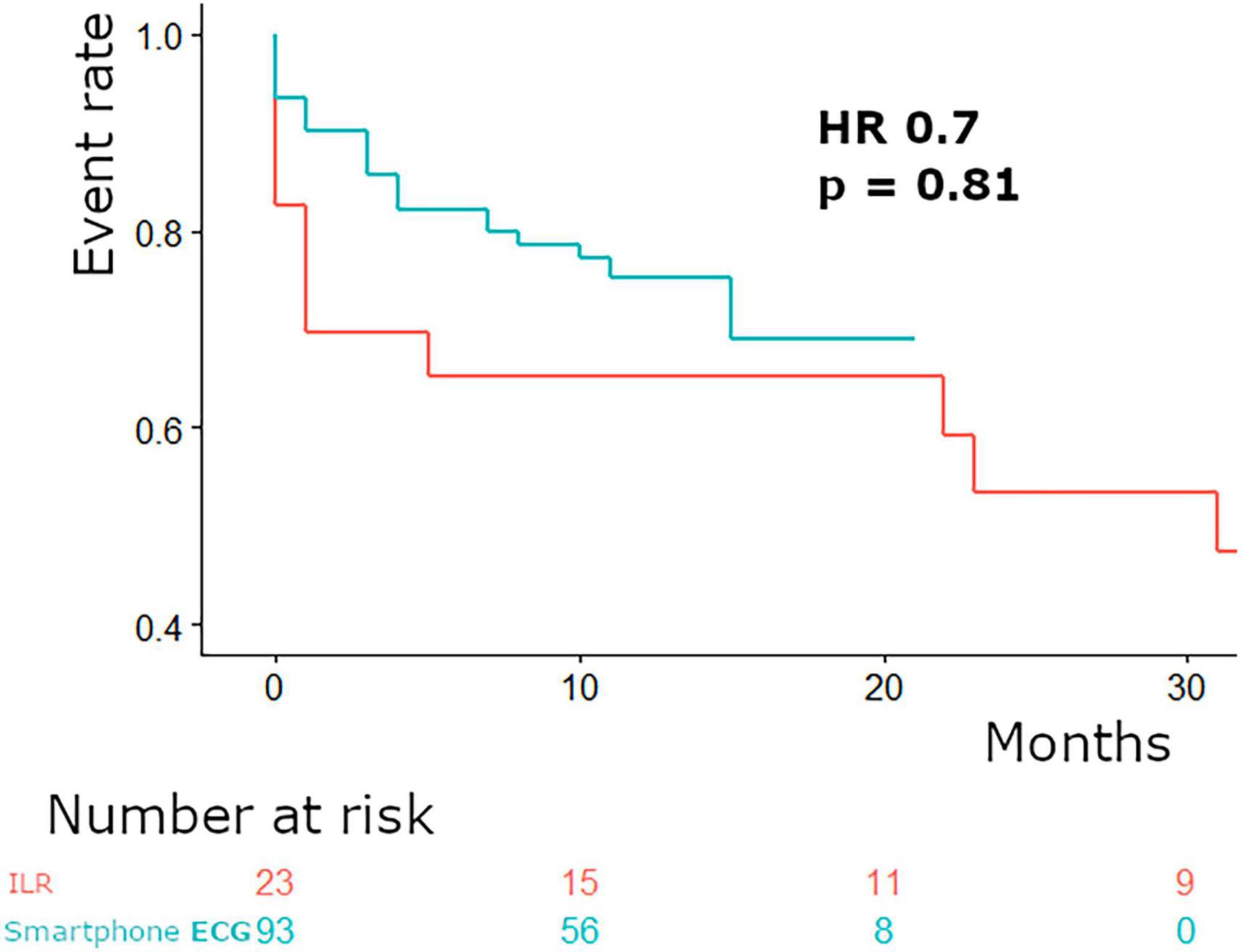
Figure 1. Time to first arrhythmia.
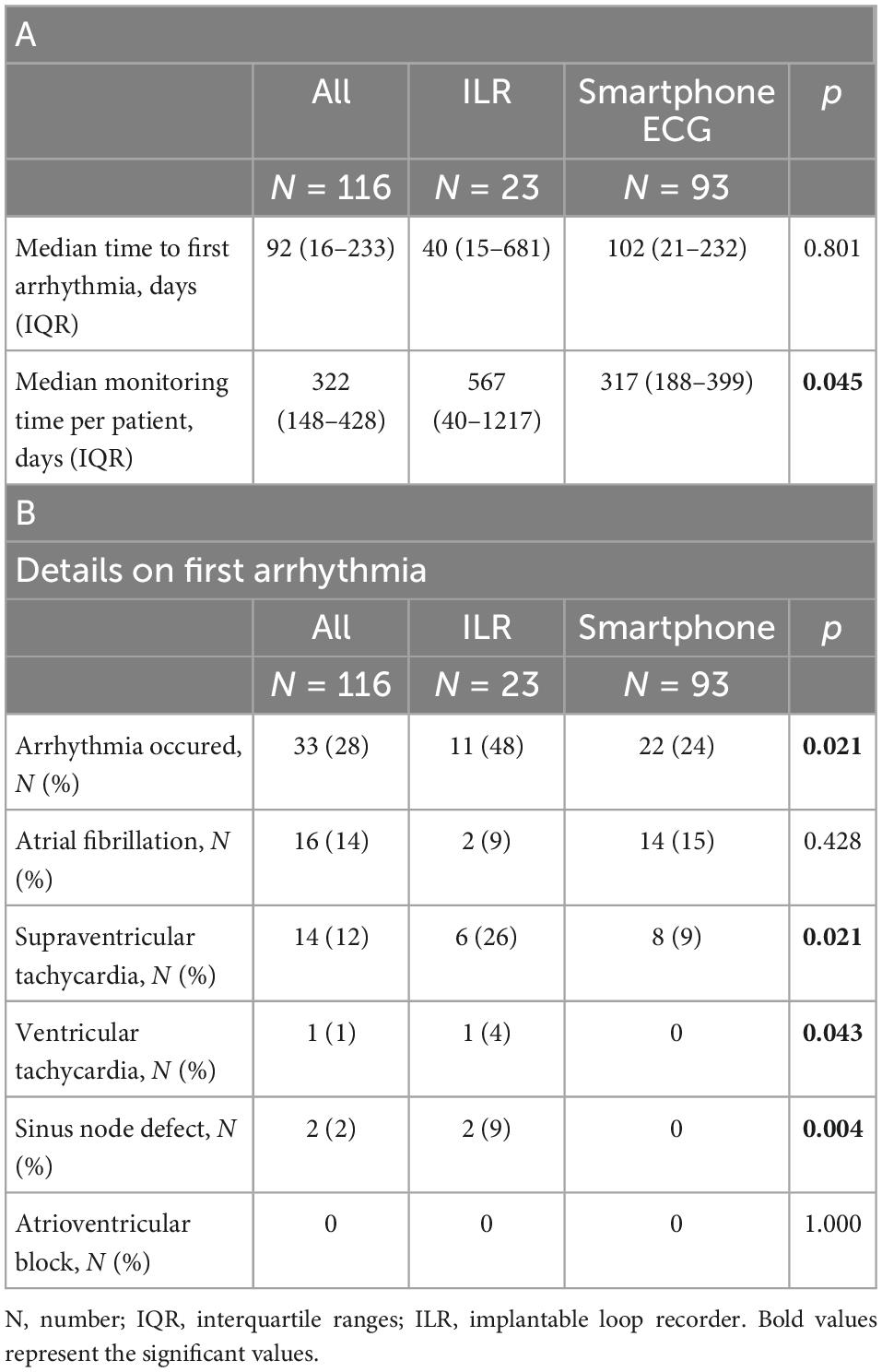
Table 2. Details on monitoring.
Arrhythmia detection led to the important care changes, displayed in Figure 2. In the ILR group device implantation to treat arrhythmia was performed in four patients (three pacemaker and one ICD) and medication changes were performed in two patients (start of beta-blocker). Furthermore, in the ILR group a wait and see strategy was chosen in five patients. In the smartphone based single-lead electrocardiogram group ablation was performed in one patient and electrical cardioversion was performed in three patients. In five patients monitored with smartphone based single-lead electrocardiogram medication changes were performed, including start of a direct oral anticoagulant, start of amiodarone, and both start and increase of beta blocker. In one patient it was decided to perform additional Holter monitoring and in 12 patients no change in management was initiated.
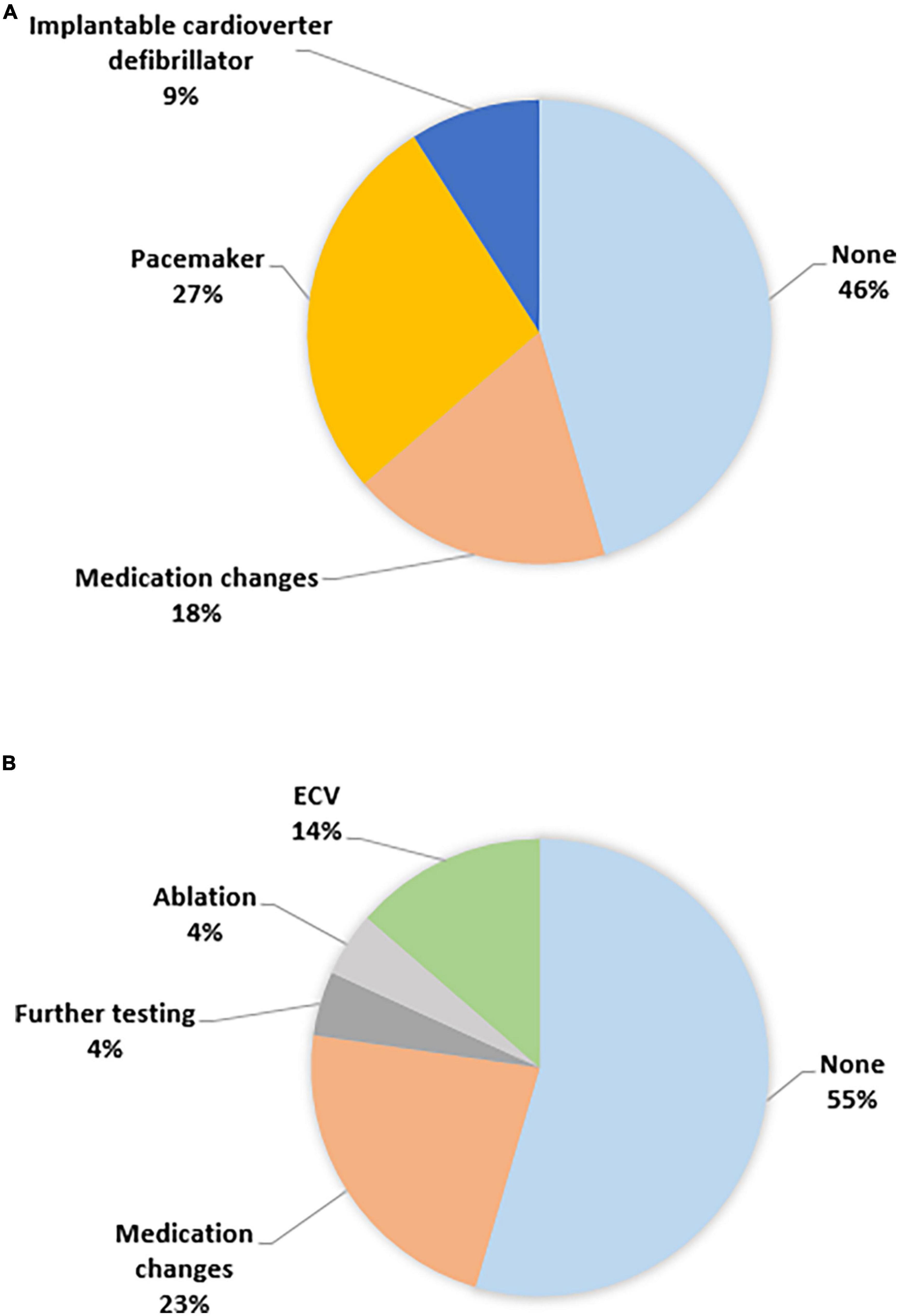
Figure 2. Care changes (A) ILR and (B) smartphone ECG.
The mode of detection (HR 0,688 95% CI 0.3–1.6, 0,371) appeared not to be associated with the first detection of arrhythmia in the study period (HR 3.2, 95% CI 1.5–6.8, p = 0.002). The use of anti-arrhythmic drugs was associated with an arrhythmia event because patients with anti-arrhythmic drugs are at high risk of arrhythmia.
Rhythm monitoring is important in ACHD patients as they are at high risk for arrhythmic and brady-arrhythmic events, but with the currently expanded possibilities of diagnostics no optimal diagnostic strategy has been defined yet. To our knowledge this is the first study that performed a comparison of ILR and smartphone based single-lead electrocardiogram for heart rhythm monitoring in ACHD patients. Smartphone based single-lead electrocardiogram seems to be a reasonable non-invasive alternative diagnostic tool for symptomatic patients instead of an invasive ILR for detecting arrhythmia.
Our findings of a high burden of arrhythmia in selected ACHD patients is comparable to the literature. Dodeja et al. evaluated traditional ILR monitoring in ACHD patients and showed a useful adjunct with clinically relevant events in 41% of patients (9). Schultz et al. performed a retrospective cohort study on remote ambulatory monitoring in 307 ACHD patients with symptoms, a history of arrhythmia or screening due to an increased risk. Their 14-day screening detected arrhythmia in 153 (50%) ACHD patients. Management changes, including medication changes (30%), further testing or imaging (10%), and procedures (6%), were made based on results of these prolonged monitoring strategy (16). Huntgeburth et al. performed a single center, retrospective observational study in which all CHD-patients with an ILR who were under care of the German Heart Center Munich between February 2015 and January 2019 were identified (17). The authors found a considerable complementary diagnostic value of ILR for the detection and differentiation of benign and malignant arrhythmias. Huntgeburth et al. concluded that ILR implantation should be considered in patients with CHD of any complexity who need medium or long-term arrhythmia monitoring, especially if short-term Holter monitoring cannot provide sufficient diagnostic certainty.
Smartphone based single-lead electrocardiogram is a promising tool to improve care and detect arrhythmia in ACHD patients (18–21). Smartphone based single-lead electrocardiogram has been shown to enable early detection of recurrences and new diagnosis of arrhythmia, which led to swift therapeutic response or remote reassurance. Furthermore, smartphone based single-lead electrocardiogram was well accepted in ACHD patients with high adherence and positive patient experience (15, 22). The risk of ILR implantation such as need for re-implantation, wound dehiscence or device erosion of 1–9% can be avoided (17, 23, 24). Smartphone based single-lead electrocardiogram as a non-invasive diagnostic tool has no such risk of surgical complications. In our analysis smartphone based single-lead electrocardiogram proofed to be an effective tool in detecting arrhythmia. In our study there was a lower rate of arrhythmia detection in the smartphone based single-lead electrocardiogram group, potentially due to the fact that this group had less patients with severe ACHD. Although ILR is better at detecting arrhythmias in patients because the window of measurement is continuous, it has the before mentioned disadvantage of being an invasive tool. So, we suggest in symptomatic patients, if symptoms occur on daily basis, 24 Holter monitoring for diagnosing arrhythmia is a good option. If symptoms occur less frequently smartphone based single-lead electrocardiogram could be an alternative option and save the ILR for patients where no diagnosis could be found with these modalities and for whom detecting arrhythmia is important to their prognosis. Furthermore, new wearables with smart algorithms can monitor patients continuous and alert patient and physician if arrhythmia is detected (25, 26).
Diagnostic yield of prolonged monitoring is also well established in AF screening in cryptogenic stroke patients (27). Longer durations of monitoring were associated with the highest diagnostic yield in these patients (28, 29). However, the optimal monitoring method and duration of monitoring is unclear (30–32). Solbiati et al. performed a systematic Cochrane review on ILR performance and concluded that available data are non-conclusive. The authors therefore recommended further research on ILR with clinically relevant outcomes (33). Our study suggests our smartphone based single-lead electrocardiogram protocol compared to ILR can be a good alternative in detecting arrhythmia in patients with symptoms other than syncope. Especially if these complaints are less frequent than once a day for which 24–48-h Holter monitoring is still a good alternative option.
Beside clinical effectiveness other aspects of implementation include amongst others: cost evaluation, governance, patient, and technological factors. Studies on costs of smartphone based single-lead electrocardiogram are scarce. In the first study that compared eHealth with the standard outpatient clinic setting it was suggested that eHealth was likely cost-effective (34). That study was performed in patients who suffered from acute myocardial infarction. Hypothetically, smartphone based single-lead electrocardiogram is more cost-effective than ILR because it saves on the costs of implantation and explantation, but if wearables for heart rhythm monitoring use a service center with medical personnel, the costs for this solution could also become significant. Furthermore, health system governance, health provider, patient and technological factors may complicate implementation. However, tools to identify barriers to implementing digital health and recommendations for overcoming them are increasingly available (35–37).
Our study was limited by a combination of two datasets, without randomization of patients between the two monitoring strategies. Moreover, short arrhythmia and asymptomatic arrhythmia or bradycardias may remain unnoticed in both groups. Despite we screened all ACHD patients visiting our outpatient clinic between 2003 and 2019 for having an ILR, the number of patients we found having an ILR was much smaller compared to the smartphone based single-lead electrocardiogram group. We postulate that the threshold for using an invasive diagnostic tool to find arrhythmia in symptomatic patients is higher compared to non-invasive Holter monitoring. The decision to implant an ILR to detect arrhythmia was most often reserved for ACHD patients with unexplained syncope or cerebral vascular accident after unsuccessful period of Holter monitoring. However, in the emerging field of non-invasive wearable heart rhythm monitoring solutions we are the first to report a comparison in this high-risk patient population. Matching was not performed in the study. The smartphone based single-lead electrocardiogram has a significantly higher number of patients with a history of previous arrhythmia. Previous arrhythmia could make arrhythmia recurrence more likely than no previous arrhythmia. However, arrhythmia could also make arrhythmia recurrence less likely because of the treatment with anti-arrhythmic drugs. Potentially this could have introduced bias the process of arrhythmia detection.
Non-invasive smartphone based single-lead electrocardiogram monitoring could be an acceptable alternative in detecting arrhythmia in symptomatic ACHD patients instead of an ILR in respect to diagnostic yield, safety and management decisions, especially in those patients without syncope.
The data underlying this article will be shared on reasonable request to the corresponding author.
The studies involving human participants were reviewed and approved by the Amsterdam UMC. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements. Written informed consent was not obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
MK, BB, and MS drafted the manuscript, which was critically revised and edited by BM, DR-V, DK, IT, JG, and KK. All authors agree to be accountable for all aspects of the work.
IT was shareholder in ventures supplying hardware and software implemented in the methods of this study.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Baumgartner H, De Backer J, Babu-Narayan SV, Budts W, Chessa M, Diller G-P, et al. 2020 ESC Guidelines for the management of adult congenital heart disease. Eur Heart J. (2021) 42:563–645. doi: 10.1093/eurheartj/ehaa554
2. Stout KK, Daniels CJ, Aboulhosn JA, Bozkurt B, Broberg CS, Colman JM, et al. 2018 AHA/ACC guideline for the management of adults with congenital heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. (2019) 73:e81–192. doi: 10.1016/j.jacc.2018.08.1029
3. Koyak Z, Harris L, de Groot JR, Silversides CK, Oechslin EN, Bouma BJ, et al. Sudden cardiac death in adult congenital heart disease. Circulation. (2012) 126:1944–54. doi: 10.1161/CIRCULATIONAHA.112.104786
4. van der Velde ET, Vander VET, Vriend JWJ, Mannens MMAM, Uiterwaal CSPM, Brand R, et al. CONCOR, an initiative towards a national registry and DNA-bank of patients with congenital heart disease in the Netherlands: rationale, design, and first results. Eur J Epidemiol. (2005) 20:549–57. doi: 10.1007/s10654-005-4264-9
5. Zomer AC, Vaartjes I, Uiterwaal CSPM, van der Velde ET, van den Merkhof LFM, Baur LHB, et al. Circumstances of death in adult congenital heart disease. Int J Cardiol. (2012) 154:168–72.
6. van der Bom T, Zomer AC, Zwinderman AH, Meijboom FJ, Bouma BJ, Mulder BJM. The changing epidemiology of congenital heart disease. Nat Rev Cardiol. (2011) 8:50–60.
7. Vehmeijer JT, Koyak Z, Leerink JM, Zwinderman AH, Harris L, Peinado R, et al. Identification of patients at risk of sudden cardiac death in congenital heart disease: the PRospEctiVE study on implaNTable cardIOverter defibrillator therapy and suddeN cardiac death in Adults with Congenital Heart Disease (PREVENTION-ACHD). Heart Rhythm. (2021) 18:785–92. doi: 10.1016/j.hrthm.2021.01.009
8. Bouma BJ, Mulder BJM. Changing landscape of congenital heart disease. Circ Res. (2017) 120:908–22. doi: 10.1161/CIRCRESAHA.116.309302
9. Dodeja AK, Thomas C, Daniels CJ, Kertesz N, Kamp A. Detection of arrhythmias in adult congenital heart disease patients with LINQTM implantable loop recorder. Congenit Heart Dis. (2019) 14:745–51. doi: 10.1111/chd.12815
10. Dussault C, Toeg H, Nathan M, Wang ZJ, Roux J-F, Secemsky E. Electrocardiographic monitoring for detecting atrial fibrillation after ischemic stroke or transient ischemic attack: systematic review and meta-analysis. Circ Arrhythm Electrophysiol. (2015) 8:263–9. doi: 10.1161/CIRCEP.114.002521
11. Jensen MT, Treskes RW, Caiani EG, Casado-Arroyo R, Cowie MR, Dilaveris P, et al. ESC working group on e-cardiology position paper: use of commercially available wearable technology for heart rate and activity tracking in primary and secondary cardiovascular prevention—in collaboration with the European Heart Rhythm Association, European Association of Preventive Cardiology, Association of Cardiovascular Nursing and Allied Professionals, Patient Forum, and the Digital Health Committee. Eur Heart J Digit Health. (2021) 2:49–59. doi: 10.1093/ehjdh/ztab011
12. Schuuring MJ, Kauw D. How to initiate eHealth in congenital heart disease patients? Eur Heart J Digit Health. (2020) 1:83–6. doi: 10.1093/ehjdh/ztaa012
13. Svennberg E, Tjong F, Goette A, Akoum N, Di Biase L, Bordachar P, et al. How to use digital devices to detect and manage arrhythmias: an EHRA practical guide. Europace. (2022) 24:979–1005. doi: 10.1093/europace/euac038
14. Cowie MR, Bax J, Bruining N, Cleland JGF, Koehler F, Malik M, et al. e-Health: a position statement of the European Society of Cardiology. Eur Heart J. (2015) 37:63–6. doi: 10.1093/eurheartj/ehv416
15. Kauw D, Koole MAC, Winter MM, Dohmen DAJ, Tulevski II, Blok S, et al. Advantages of mobile health in the management of adult patients with congenital heart disease. Int J Med Inform. (2019) 132:104011. doi: 10.1016/j.ijmedinf.2019.104011
16. Schultz KE, Lui GK, McElhinney DB, Long J, Balasubramanian V, Sakarovitch C, et al. Extended cardiac ambulatory rhythm monitoring in adults with congenital heart disease: arrhythmia detection and impact of extended monitoring. Congenit Heart Dis. (2019) 14:410–8. doi: 10.1111/chd.12736
17. Huntgeburth M, Hohmann C, Ewert P, Freilinger S, Nagdyman N, Neidenbach R, et al. Implantable loop recorder for monitoring patients with congenital heart disease. Cardiovasc Diagn Ther. (2021) 11:1334–43. doi: 10.21037/cdt-20-677
18. Schuuring MJ, Mischie AN, Caiani EG. Editorial: digital solutions in cardiology. Front Cardiovasc Med. (2022) 9:873991. doi: 10.3389/fcvm.2022.873991
19. Duncker D, Svennberg E. Editorial: wearable devices for cardiac rhythm monitoring. Front Cardiovasc Med. (2022) 9:951769. doi: 10.3389/fcvm.2022.951769
20. Abu-Alrub S, Strik M, Ramirez FD, Moussaoui N, Racine HP, Marchand H, et al. Smartwatch electrocardiograms for automated and manual diagnosis of atrial fibrillation: a comparative analysis of three models. Front Cardiovasc Med. (2022) 9:836375. doi: 10.3389/fcvm.2022.836375
21. Pengel LKD, Robbers-Visser D, Groenink M, Winter MM, Schuuring MJ, Bouma BJ, et al. A comparison of ECG-based home monitoring devices in adults with CHD. Cardiol Young. (2022) [Online ahead of print]. doi: 10.1017/S1047951122002244
22. Koole MAC, Kauw D, Winter MM, Dohmen DAJ, Tulevski II, de Haan R, et al. First real-world experience with mobile health telemonitoring in adult patients with congenital heart disease. Neth Heart J. (2019) 27:30–7. doi: 10.1007/s12471-018-1201-6
23. Lim WY, Papageorgiou N, Sukumar SM, Alexiou S, Srinivasan NT, Monkhouse C, et al. A nurse-led implantable loop recorder service is safe and cost effective. J Cardiovasc Electrophysiol. (2019) 30:2900–6. doi: 10.1111/jce.14206
24. Bezzerides VJ, Walsh A, Martuscello M, Escudero CA, Gauvreau K, Lam G, et al. The real-world utility of the LINQ implantable loop recorder in pediatric and adult congenital heart patients. JACC Clin Electrophysiol. (2019) 5:245–51. doi: 10.1016/j.jacep.2018.09.016
25. Avram R, Ramsis M, Cristal AD, Nathan V, Zhu L, Kim J, et al. Validation of an algorithm for continuous monitoring of atrial fibrillation using a consumer smartwatch. Heart Rhythm. (2021) 18:1482–90. doi: 10.1016/j.hrthm.2021.03.044
26. Garikapati K, Turnbull S, Bennett RG, Campbell TG, Kanawati J, Wong MS, et al. The role of contemporary wearable and handheld devices in the diagnosis and management of cardiac arrhythmias. Heart Lung Circ. (2022) 31:1432–49. doi: 10.1016/j.hlc.2022.08.001
27. Dilaveris PE, Antoniou CK, Caiani EG, Casado-Arroyo R, Climent AM, Cluitmans M, et al. ESC Working Group on e-Cardiology Position Paper: accuracy and reliability of electrocardiogram monitoring in the detection of atrial fibrillation in cryptogenic stroke patients : in collaboration with the Council on Stroke, the European Heart Rhythm Association, and the Digital Health Committee. Eur Heart J Digit Health. (2022) 3:341–58. doi: 10.1093/ehjdh/ztac026
28. Wachter R, Gröschel K, Gelbrich G, Hamann GF, Kermer P, Liman J, et al. Holter-electrocardiogram-monitoring in patients with acute ischaemic stroke (Find-AFRANDOMISED): an open-label randomised controlled trial. Lancet Neurol. (2017) 16:282–90. doi: 10.1016/S1474-4422(17)30002-9
29. Healey JS, Connolly SJ, Gold MR, Israel CW, Van Gelder IC, Capucci A, et al. Subclinical atrial fibrillation and the risk of stroke. N Engl J Med. (2012) 366:120–9. doi: 10.1056/NEJMoa1105575
30. Kishore A, Vail A, Majid A, Dawson J, Lees KR, Tyrrell PJ, et al. Detection of atrial fibrillation after ischemic stroke or transient ischemic attack: a systematic review and meta-analysis. Stroke. (2014) 45:520–6. doi: 10.1161/STROKEAHA.113.003433
31. Albers GW, Bernstein RA, Brachmann J, Camm J, Easton JD, Fromm P, et al. Heart rhythm monitoring strategies for cryptogenic stroke: 2015 diagnostics and monitoring stroke focus group report. J Am Heart Assoc. (2016) 5:e002944. doi: 10.1161/JAHA.115.002944
32. Steinberg JS, Varma N, Cygankiewicz I, Aziz P, Balsam P, Baranchuk A, et al. 2017 ISHNE-HRS expert consensus statement on ambulatory ECG and external cardiac monitoring/telemetry. Heart Rhythm. (2017) 14:e55–96. doi: 10.1016/j.hrthm.2017.03.038
33. Solbiati M, Costantino G, Casazza G, Dipaola F, Galli A, Furlan R, et al. Implantable loop recorder versus conventional diagnostic workup for unexplained recurrent syncope. Cochrane Database Syst Rev. (2016) 4:CD011637. doi: 10.1002/14651858.CD011637.pub2
34. Treskes RW, van den Akker-van Marle ME, van Winden L, van Keulen N, van der Velde ET, Beeres S, et al. The box-eHealth in the outpatient clinic follow-up of patients with acute myocardial infarction: cost-utility analysis. J Med Internet Res. (2022) 24:e30236. doi: 10.2196/30236
35. Tromp J, Jindal D, Redfern J, Bhatt A, Séverin T, Banerjee A, et al. World heart federation roadmap for digital health in cardiology. Glob Heart. (2022) 17:61. doi: 10.5334/gh.1141
36. Kauw D, Huisma PR, Medlock SK, Koole MAC, Wierda E, Abu-Hanna A, et al. Mobile health in cardiac patients: an overview on experiences and challenges of stakeholders involved in daily use and development. BMJ Innovat. (2020) 6:1–8. doi: 10.1136/bmjinnov-2019-000418
Keywords: arrhythmias, congenital heart disease, electrocardiography, telemedicine, implantable loop recorder, cardiology, pacemaker, eHealth
Citation: Koole MA, Kauw D, Kooiman KM, de Groot JR, Robbers-Visser D, Tulevski II, Mulder BJ, Bouma BJ and Schuuring MJ (2023) An implantable loop recorder or smartphone based single-lead electrocardiogram to detect arrhythmia in adults with congenital heart disease? Front. Cardiovasc. Med. 9:1099014. doi: 10.3389/fcvm.2022.1099014
Received: 15 November 2022; Accepted: 13 December 2022;
Published: 06 January 2023.
Edited by:
David Duncker, Hannover Medical School, GermanyReviewed by:
Sebastian Feickert, Department for Cardiology and Conservative Intensive Care Unit, GermanyCopyright © 2023 Koole, Kauw, Kooiman, de Groot, Robbers-Visser, Tulevski, Mulder, Bouma and Schuuring. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mark J. Schuuring,  TS5KLlNjaHV1cmluZy0xOUB1bWN1dHJlY2h0Lm5s
TS5KLlNjaHV1cmluZy0xOUB1bWN1dHJlY2h0Lm5s
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.