 Josep Redon1*
Josep Redon1* Tomas Seeman2
Tomas Seeman2 Dénes Pall3
Dénes Pall3 Lagle Suurorg4
Lagle Suurorg4 Konstantinos Kamperis5Serap Erdine6
Konstantinos Kamperis5Serap Erdine6 Elke Wühl7
Elke Wühl7 Giuseppe Mancia8
Giuseppe Mancia8- 1INCLIVA Research Institute, CIBERObn Institute of Health Charles III, University of Valencia, Madrid, Spain
- 2Department of Pediatrics, 2nd Faculty of Medicine, Charles University Prague, Prague, Czechia
- 3Department of Medical Clinical Pharmacology, University of Debrecen, Debrecen, Hungary
- 4Tallinn Children's Hospital, Tallinn, Estonia
- 5Department of Paediatrics and Adolescent Medicine, Aarhus University Hospital, Aarhus, Denmark
- 6Hypertension and Atherosclerosis Center, Marmara University School of Medicine, Istanbul, Turkey
- 7Division of Pediatric Nephrology, Center for Pediatrics and Adolescent Medicine, Heidelberg University Hospital, Heidelberg, Germany
- 8University of Milano-Bicocca, Milan, Italy
Introduction: To date, our knowledge on antihypertensive pharmacological treatment in children and adolescents is still limited because there are few randomized clinical trials (CTs), hampering appropriate management. The objective was to perform a narrative review of the most relevant aspects of clinical trials carried out in primary and secondary hypertension.
Methods: Studies published in PubMed with the following descriptors: clinical trial, antihypertensive drug, children, adolescents were selected. A previous Cochrane review of 21 randomized CTs pointed out the difficulty that statistical analysis could not assess heterogeneity because there were not enough data. A more recent meta-analysis, that applied more stringent inclusion criteria and selected 13 CTs, also concluded that heterogeneity, small sample size, and short follow-up time, as well as the absence of studies comparing drugs of different classes, limit the utility.
Results: In the presented narrative review, including 30 studies, there is a paucity of CTs focusing only on children with primary or secondary, mainly renoparenchymal, hypertension. In trials on angiotensin converting enzyme inhibitors (ACEI), angiotensin receptor blockers (ARBs), calcium channel blockers (CCBs) and diuretics, a significant reduction of both SBP and DBP in mixed cohorts of children with primary and secondary hypertension was achieved. However, few studies assessed the effect of antihypertensive drugs on hypertensive organ damage.
Conclusions: Given the increasing prevalence and undertreatment of hypertension in this age group, innovative solutions including new design, such as ‘n-of-1', and optimizing the use of digital health technologies could provide more precise and faster information about the efficacy of each antihypertensive drug class and the potential benefits according to patient characteristics.
Introduction
Globally, and particularly in developing countries, hypertension (HTN) is the most common disease of adulthood (1) and low rates of antihypertensive treatment and blood pressure (BP) control are the most important cause of the high cardiovascular morbidity and mortality worldwide (2). Even though its prevalence is much lower in children and adolescents than in adults, HTN has a great clinical importance also at a young age because BP elevation in young people makes the development of sustained HTN in adulthood more likely (3). Furthermore, in recent decades the number of young patients with a diagnosis of hypertension has been found to increase. This is in part because of the wider use of BP measurements (4) but unquestionably also to the increase of overweight and obesity in younger populations (5). Because HTN in adulthood has its roots in childhood, it is important to measure BP appropriately and diagnose pediatric HTN in a timely manner (6). Diagnostic criteria for elevated BP in children and adolescents are based on the concept that BP increases with age and body size, making it impossible to utilize a single BP level to define HTN, as done in adults. Hypertension is defined as systolic and/or diastolic BP persistently ≥95th percentile of the normative BP distribution, adjusted by age, sex and height measured on at least three separate occasions. Consistent with the physiological body growth adult cut-points 140/90 mmHg are applied for adolescents 16 years and older (Table 1) (4).
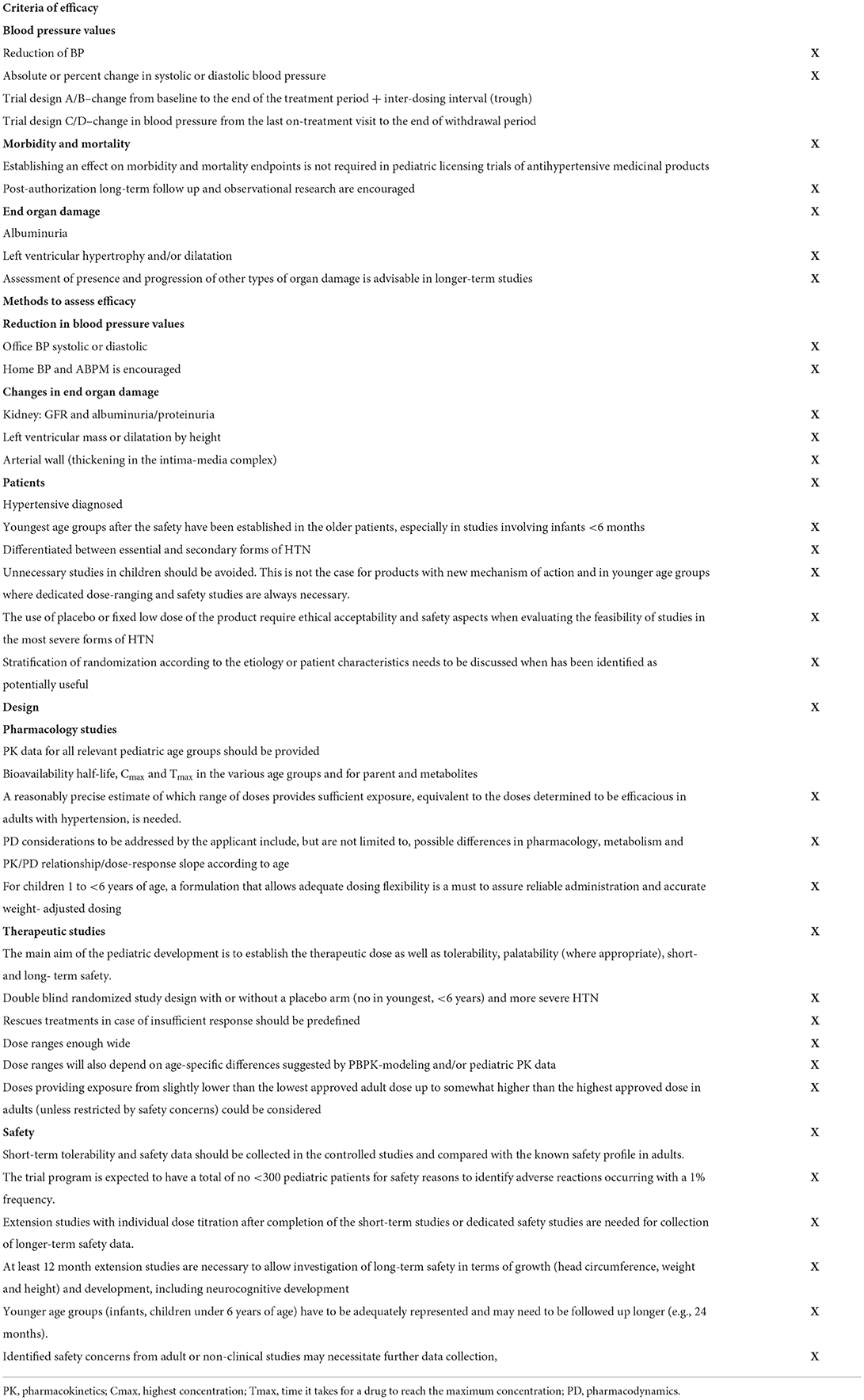
Table 1. Criteria for the methods to establish dosing recommendation and safety of antihypertensives from EMA (15).
Currently primary HTN is the most frequent cause of high BP in children and adolescents with a close association with overweight and obesity (7). As in adulthood, the first therapeutic step to adopt under these circumstances should be non-pharmacological treatment, i.e., modifications of incorrect lifestyles that may contribute to BP elevation (8, 9). However, in children where such a strategy fails, pharmacological treatment is indicated (4) and in young people with symptomatic HTN, secondary HTN, target organ damage, chronic kidney disease or diabetes mellitus, pharmacological treatment should be considered as first line therapy. Unfortunately, however, knowledge of what should be the optimal first step drug or drugs in children and adolescents is much more limited than in adults (4, 8). In addition, no or few good-quality long-term outcome data are available to guide pediatricians in selecting medication to treat HTN, which means, that treatment is often based on experience rather than on evidence. In the absence of evidence, use of “off-label” drugs is also common (10), further complicating the appropriate management of pediatric HTN and making it a challenging task for pediatricians. Many of whom feel uncomfortable treating a hypertensive child, also because recognition of a HTN state is more difficult than in adults. Nevertheless, during the last decades, childhood HTN has been studied more rigorously, to optimize BP measurements, collect normative data and establish diagnostic work-up guidelines. To-date the development of worldwide adopted recommendations has improved our ability to diagnose pediatric HTN to an extent superior to that of HTN management, which has made much less progress (4).
Clinical trials of antihypertensive drugs in the adult population have yielded in-depth information about their pharmacokinetics and pharmacodynamics, including BP lowering efficacy, effects on hypertension-related outcomes and safety for all major classes of antihypertensive medication. Data on optimal drug doses, best combinations, and differences in efficacy among the different drug classes have also been obtained. In contrast, in the pediatric population, paucity of studies is the rule, which is a major shortcoming because what works in adults does not necessarily work in children and adolescents. Furthermore, most drug formulations are not adapted for use in the pediatric age.
The present review focuses on CTs of antihypertensive drugs in primary and secondary HTN of children and adolescents, with emphasis on future research needed in this age population. PRISMA system have been used (11) to select the studies to be included with descriptors: clinical trials, antihypertensive drugs and children and adolescents, in PubMed. The flow diagram is in Figure 1.
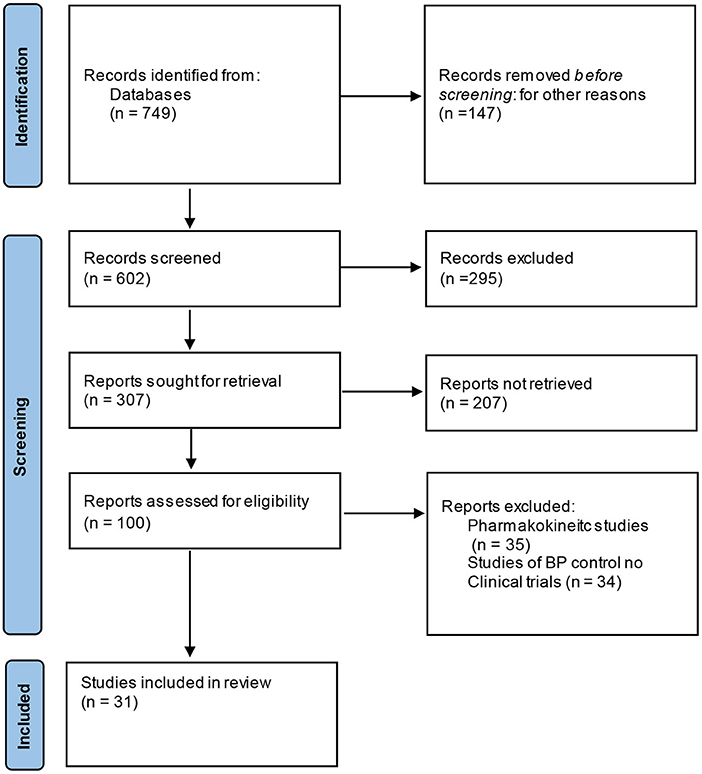
Figure 1. Flow-chart of the studies selected.
Regulatory agencies and hypertension drug treatment
During the last three decades, Regulatory Agencies have effectively acted to provide better information about the use of drugs for pediatric treatment and to promote their availability. In the US, incentives were first authorized by the Food and Drug Modernization Act of 1997 such as the 6 month prolongation of the market patent for drugs which were tested by clinical trials in children, as well as the possibility to perform clinical trials with off-patent drugs. This was reauthorized in 2002 by the Best Pharmaceuticals for Children Act (BPCA) (12), and permanently reauthorized by FDA in 2012 under the FDA Safety and Innovation Act (13).
Similar actions were taken in Europe by the Regulation of Medical Products for Pediatric Use (14). The Pediatric Committee of the European Medicines Agency (PDCO) is the scientific committee responsible for activities connected with medicines to be used in pediatrics and for their development in the European Union via scientific support and help to data analysis in the area of pediatrics. The PDCO was created by the pediatric regulations that came into force in 2007, with the aim of improving the health of the European Union's pediatric population via development and increasing the availability of ad hoc medicines. A Pediatric Investigation Plan (PIP) promoting research activities has also been launched, including PIPs for treatment of cardiovascular disease, HTN in particular (15), although at present the numbers of PIPs in this area lags behind other therapeutic areas.
As shown in Tables 1, 2 the two Regulatory Agencies have also established the requirements for the approval and conduction of CTs. Although some requirements are in agreement, others differ between the two Agencies (16, 17), with the main differences involving methods of measuring BP, assessment of organ damage, range of drug dose to be used, and time for extended observation after completion of a trial.
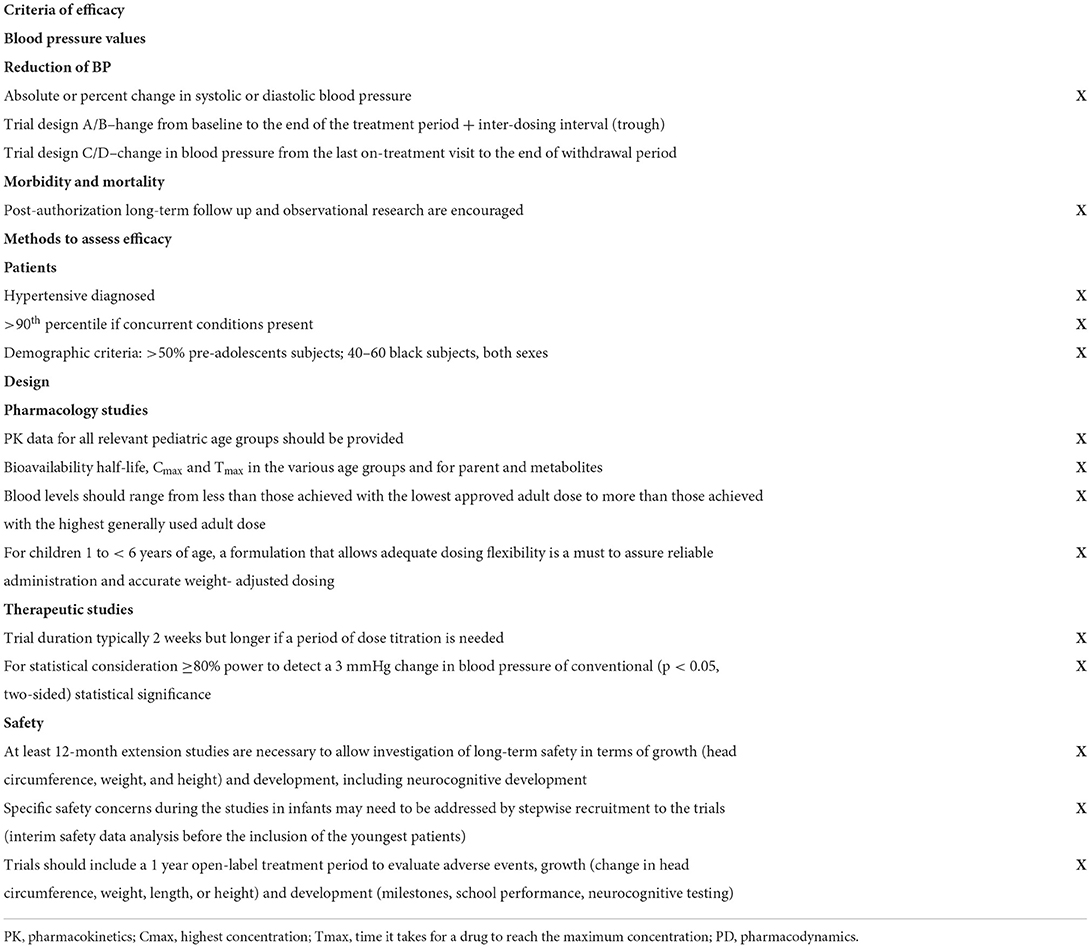
Table 2. Criteria for the methods to establish dosing recommendation and safety of antihypertensives from FDA agencies (16).
Clinical trial challenges
Barriers
Research on children in CTs faces ethical, epidemiological, and economic difficulties or barriers, which have some special characteristics in the case of antihypertensive drugs. Research failures may occur because the results do not reach statistical significance and thus the efficacy of a tested drug cannot be proven. Other reasons are inconsistent results, controversial results or project failure because the budget has been overspent, the project targets have not been achieved or deadlines haven't been met (18).
In a review of CTs on failure rates and causes of the use of drugs for hypertension care in children and adolescents since 2000 (search keywords “pediatric drug therapy,” “hypertension,” “clinical trials” and “fail of trials”) nine of the sixteen pediatric antihypertensive drug trials failed to show a dose response (19) due to unskilled project manager, unproductive team, complexity of protocol, the dilemma of “Project Completion Targets” vs. “Eligibility of the Volunteers,” poor training and poor verification, ethical issues and data quality (20, 21).
Finally, early discontinuation and lack of publication of study findings are common in registered pediatric CTs. Targeted efforts are needed to support trial completion and timely result dissemination to strengthen evidence-based pediatric medicine (22).
Previous analysis assessing BP lowering effect and safety
As in adults, in children and adolescents the BP-lowering effect of drug treatment may be influenced by several factors, including age, sex, weight, and severity of baseline hypertension, which makes achievement of conclusive information on between-drug differences in efficacy far from simple.
In a Cochrane review article (23) including 21 randomized CTs, a total of 3,454 hypertensive children and adolescents were enrolled when at least a 2 week comparison was made between (a) monotherapy or combination therapy with either placebo or another medication or (b) different doses of the same drug. Despite use of random effect models the authors emphasized that safe conclusions could not be made due to lack of sufficient data. Nevertheless, they stated that the agents tested, i.e., ACEIs, ARBs and CCBs did not exhibit a consistent dose-response relationship, although all of them appeared to be safe, at least within the short-term context of the studies.
A more recent meta-analysis (24) tried to assess more uniform and higher clinical quality CTs by selecting 13 trials with a randomized placebo-controlled design, more than 50 patients enrolled, and a follow-up of at least 4 weeks. Patients affected by secondary forms of hypertension, which may benefit from specific and targeted therapies, were not systematically excluded. The results were rather inconclusive because, despite the more demanding selection of the studies, the results remined heterogeneous and the follow-up time short. The authors highlighted that the observations nevertheless increased the available experience with drugs that block the renin angiotensin system (i.e., ACEIs and ARBs), because these drugs accounted for the greater proportion of treatment in the patients recruited.
Update of present knowledge
A total of 31 (25–55) CTs have been summarized in the present review, the majority (n = 20), (26, 29–38, 40, 41, 45, 47–53) (Table 3) including children with both primary and secondary HTN. Fewer CTs investigated antihypertensive drugs focusing only on children with primary HTN and taking into account concomitant obesity (48) or race (46). The majority children participating in CTs on secondary HTN had renal disease as the first cause of HTN (27, 31, 34–40, 42, 43, 47, 49–55). Some of the CTs in renal disease assessed changes in albuminuria or proteinuria (35, 36, 52, 53).
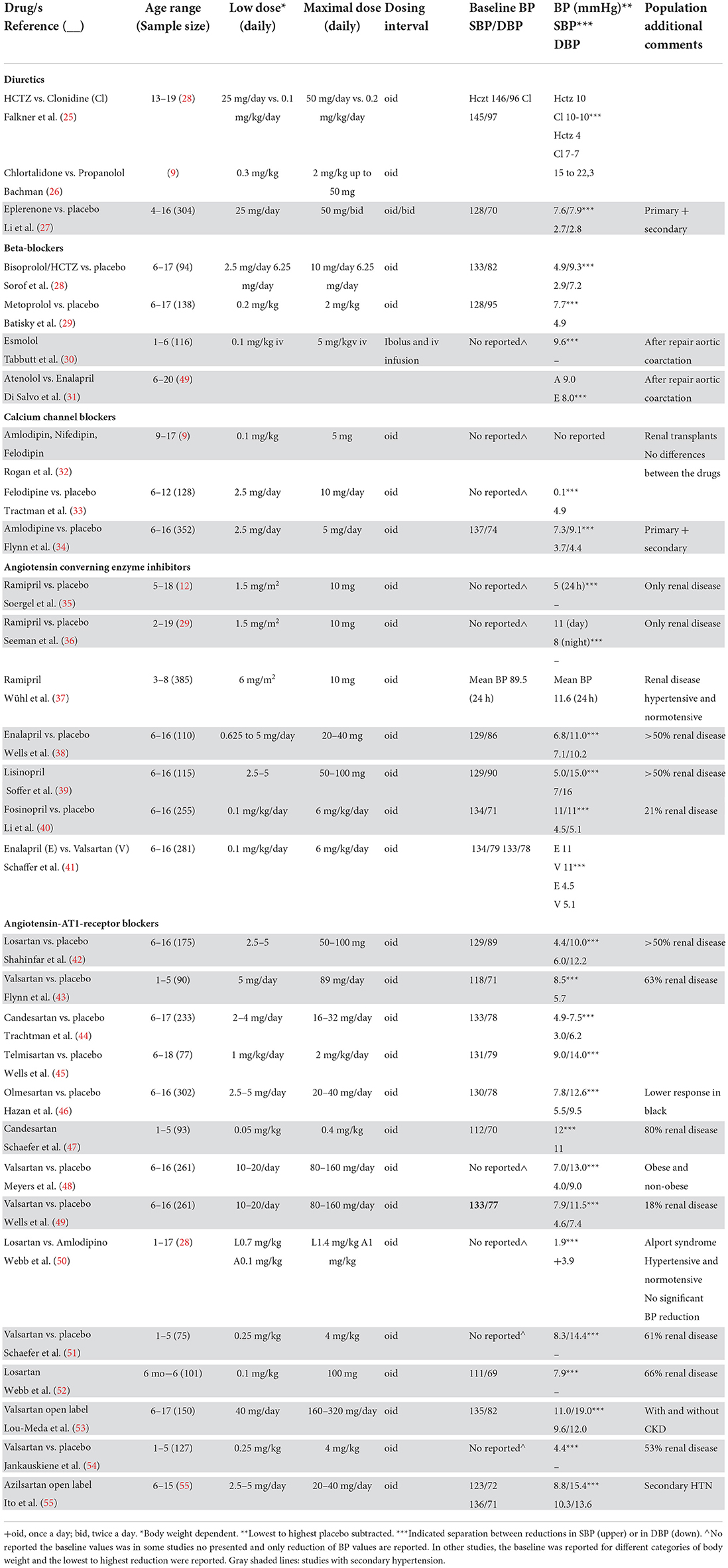
Table 3. Main characteristics of clinical trials in blood pressure reduction.
Among the CTs specifically addressing primary HTN, one study analyzed the antihypertensive efficacy of Valsartan (48) in obese and non-obese hypertensives, and found that BP reduction was similar in the two groups. In another specific CT on primary HTN, Olmesartan, an angiotensin receptor blocker, was less effective in reducing BP in African American children compared to Caucasians (46), a result in line with data available in the adult population.
Regarding secondary vs. primary HTN, most CTs did not perform a separate analysis of the BP lowering effect of study medication in children with primary and secondary HTN.
In the mixed cohorts, in which ACEI, ARBs or diuretics were used a significant reduction of both systolic (SBP) and diastolic BP (DBP) was observed. This was the case also in the only study in which amlodipine was used. In this study however, a separate analysis of children with primary and secondary HTN was made. The results showed that there was no effect of the underlying cause of HTN on BP response (34). Thus, the authors concluded that, at least with regard to amlodipine, the BP lowering effect of drug treatment in children with secondary HTN is not different from that in children with primary HTN. Taken together, the data suggest that in children with primary vs. secondary HTN there may be no significantly different BP lowering effect of a variety of antihypertensive drugs, a conclusion supported by data in adults.
Four studies analyzed the impact of antihypertensive drug treatment only in secondary HTN. In renal posttransplant patients one study compared three CCBs, i.e., amlodipine, nifedipine and felodipine, and found no difference in the BP-lowering effect among them (32). In the second study losartan and amlodipine both resulted in a significant decrease of SBP but not of diastolic BP compared to placebo in children with Alport syndrome (51). In the last two studies, esmolol and atenolol, beta-blockers, effectively reduced BP in the post-operative phase of surgery for aortic coarctation (30, 31).
From the above review it is clear that data on antihypertensive drugs in the young age are scarce. Beside the limited information on the BP lowering effect of different drugs and the probable similarity of antihypertensive drug treatment effects in primary and secondary HTN, no adequate data are available on the effect of different timing of drug administration, the relationship with food intake, the effect on BP reduction during sleep and the comparison of different agents within the same drug class. Data about the effect of antihypertensive drugs on hypertensive target organ damage are also very limited and the safety profile of the antihypertensive drug administration, although addressed by some CTs, almost entirely lacks of longer-term information as well as of information in children with other health problems such as lung disease, cardiac disease, and others.
Overall, the available evidence appears to allow a relatively safe choice of at least the class of antihypertensive drugs in children with secondary HTN. Most other clinical considerations, however, are still largely depending on the underlying pathophysiology and the presence of concurrent disorders such as diabetes mellitus, chronic kidney disease, proteinuria, overweight and more.
The studies available in the ClinicalTrials.gov Search Results (56) (consulted 07/05/2022) include only six studies in different stages of conduction but not published yet (Table 4). The design does not seem to cover the previously mentioned issues.
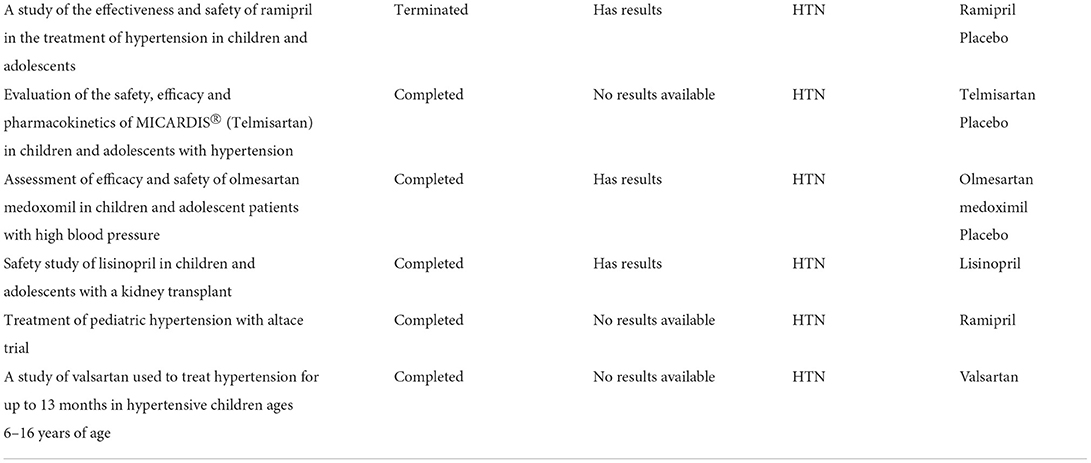
Table 4. ClinicalTrials.gov search results 07/05/2022 (56).
n-of-1 trials
Given the limitations of the CTs performed in the last 20 years, new research approaches are needed to provide evidence on how to select appropriate antihypertensive medications in children, in terms of efficacy and tolerance as well as persistence of the effect over prolonged time periods.
The n-of-1 trial (a.k.a. single-patient trials) is a promising approach to identify the most successful treatment for diseases that require treatment during prolonged periods of time. Based on a document released in 2014 by the Agency for the Health Care Research and Qualities (57), n-of-1 trials, is a form of prospective research in which different treatments are evaluated in an individual patient over time.
The approach has been applied to HTN using ambulatory blood pressure monitoring (ABPM). In a randomized trial (58), three drugs from different classes were selected and started in patients in whom HTN had been confirmed by ABPM. The first drug was given during the first 2 weeks, the second drug during weeks 3 and 4 and the third drug during weeks 5 and 6. At the end of each 2 week period a 24 h ABPM was performed. Once the first circle (6 weeks) was finished, the drug with unacceptable side effect profile or minimal BP reduction was discarded and the procedure was repeated for the remaining two drugs. In the end the drug with the best treatment adherence, patient satisfaction, and BP control was selected. It should be noted that the above design does not meet with universal agreement because compliance can be challenging for both patients and physicians, although the results can be useful in patients who require long-term BP control.
Future perspectives
Innovative solutions are needed to optimize the traditional testing of drugs. The application of rapidly evolving digital health technologies and artificial intelligence in HTN healthcare and research (digital hypertension) holds promise to provide further insights into the understanding of pathophysiology as well as the identification of therapeutic targets and efficacy of antihypertensive drugs.
The stringent isolation measures adopted during the pandemic have strongly promoted telemedicine practices that provide information via communication technologies that use several distinct methods (59).
A prospective study evaluating 263 interviews between health care professionals and children with chronic diseases suggests that telemedicine applications are useful tools not only during pandemics but also in daily practice (60). One application now frequently used in managing HTN is BP telemonitoring (BPT) (61). Although patients' compliance might be a potential limitation, a systematic review article points out that all current studies regarding the efficacy of BPT exhibit several benefits for long-term follow-ups, including reduction of health care costs and improvement of outcomes in the pediatric population (62). This opens also opportunities to improve drugs.
Artificial intelligence (AI) is another promising tool for the management of patients with high blood pressure and can also improve the assessment of drug efficacy (63). Machine learning methods differ significantly from traditional statistical methods. While conventional statistics focuses mainly on the conclusions, AI-derived statistics generally concentrates on prediction and decision-making. Therefore, they are commonly used as risk-stratifying and scoring tools (64, 65). However, the role of AI techniques in the management of HTN remains unclear and controversial due to several limitations, such as requiring large amounts of data, lack of data quality, lack of standardized models that can be reliably used for different populations, dependence mostly on laboratory findings without adequate environmental factor assessments, necessity to retrain the neural network whenever a significant change is made in the target population, and insufficient training of clinicians in bioinformatics and data science (63, 66, 67).
Conclusions
Despite the traditional belief that HTN is a rare condition in children, there is accumulating evidence that elevated BP is increasingly common in both children and adolescence. Despite the abundance of different pharmacological agents designed to treat HTN these are mostly studied in adults and only over the last years industry and authorities have identified the need of well conducted randomized trials of pharmacological treatment in childhood HTN.
Legislation changes have pushed for pediatric studies, but we are still far from establishing a confident level of knowledge in HTN management for children. CTs available today lack hard evidence to recommend any class of antihypertensive medication over the others as first line in children. Furthermore, the impact of pharmacological therapy on cognitive development and growth is not sufficiently studied.
Overall, it is beyond any doubt that we lack important knowledge when it comes to pharmacological antihypertensive treatment in children. The increasing number of children to be treated rises the need for large multicenter randomized trials to investigate the best treatment strategies for each child, to identify optimal dosage regimes and improve the long-term safety of antihypertensive medication in children. In addition to classical CTs, new approaches will contribute to get more grounded information.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
JR, GM, and SE contributed to conception and design of the study. JR wrote the first draft of the manuscript. JR, SE, EW, GM, DP, TS, LS, and KK wrote sections of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Funding
This article is based upon work from COST Action HyperChildNET (CA19115), supported by COST (European Cooperation in Science and Technology).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Mancia G, Fagard R, Narkiewicz K, Redón J, Zanchetti A, Böhm M, et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. (2013) 31:1281–357. doi: 10.1097/01.hjh.0000431740.32696.cc
2. Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. (2018) 39:3021–104. doi: 10.1093/eurheartj/ehy339
3. Lurbe E, Cifkova R, Cruickshank JK, Dillon MJ, Ferreira I, Invitti C, et al. Management of high blood pressure in children and adolescents: recommendations of the European society of hypertension. J Hypertens. (2009) 27:1719–42. doi: 10.1097/HJH.0b013e32832f4f6b
4. Lurbe E, Agabiti-Rosei E, Cruickshank JK, Dominiczak A, Erdine S, Hirth A, et al. 2016 European society of hypertension guidelines for the management of high blood pressure in children and adolescents. J Hypertens. (2016) 34:1887–920. doi: 10.1097/HJH.0000000000001039
5. Drozdz D, Alvarez-Pitti J, Wójcik M, Borghi C, Gabbianelli R, Mazur A, et al. Obesity and cardiometabolic risk factors: from childhood to adulthood. Nutrients. (2021) 13:4176. doi: 10.3390/nu13114176
6. Stabouli S, Kotsis V, Toumanidis S, Papamichael C, Constantopoulos A, Zakopoulos N. White-coat and masked hypertension in children: association with target-organ damage. Pediatr Nephrol. (2005) 20:1151–5. doi: 10.1007/s00467-005-1979-5
7. Gupta-Malhotra M, Banker A, Shete S, Hashmi SS, Tyson JE, Barratt MS, et al. Essential hypertension vs. secondary hypertension among children. Am J Hypertens. (2015) 28:73–80. doi: 10.1093/ajh/hpu083
8. Lurbe E, Litwin M, Pall D, Seeman T, Stabouli S, Webb NJA, et al. Insights and implications of new blood pressure guidelines in children and adolescents. J Hypertens. (2018) 36:1456–9. doi: 10.1097/HJH.0000000000001761
9. Páll D, Zrínyi M. Non-pharmacological treatment of hypertension. In: Lurbe E, Wühl E, editors. Hypertension in Children and Adolescents. Springer Nature Switzerland AG 2019. pp. 211–24. doi: 10.1007/978-3-030-18167-3_13
10. Redon J, Redon P. Evidences from clinical trials and use of antihypertensive drugs in children and adolescents. In: Lurbe E, Wühl E, editors. Hypertension in children and adolescents. Springer Nature Switzerland AG 2019. p. 263–77. doi: 10.1007/978-3-030-18167-3_17
11. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
12. Best Pharmaceuticals for Children Act and Pediatric Research Equity Act. Available online at https://www.fda.gov/ScienceResearch/SpecialTopics/PediatricTherapeuticsResearch/ucm509707.htm (accessed 11 June, 2022).
13. Food Drug Administration Safety Innovation Act (FDASIA). Available online at https://www.fda.gov/RegulatoryInformation/LawsEnforcedbyFDA/SignificantAmendmentstotheFDCAct/FDASIA/default.htm (accessed 11 June, 2022).
14. European Medicines Agency Addendum to the Guideline on Clinical Investigation of Medicinal Products in the Treatment of Hypertension (EMA/238/1995/Rev. 3, 18 November 2010 released in 26 February 2015. EMA/CHMP/206815/2013 Committee for Medicinal Products for Human Use (CHMP).
15. Faulkner B, Delgado-Charro MB. Cardiovascular paediatric medicines development: have paediatric investigation plans lost heart? Pharmaceutics. (2020) 12:1176. doi: 10.3390/pharmaceutics12121176
16. Paediatric addendum to the note for guidance on the clinical investigation on medicinal products in the treatment of hypertension. (2015). Available online at: https://www.ema.europa.eu/en/paediatric-addendum-guideline-clinical-investigation-medicinal-products-treatment-hypertension
17. Principles for Clinical Evaluation of New Antihypertensive Drugs. (2000). Available online at: https://www.ema.europa.eu/en/ich-e12-principles-clinical-evaluation-new-antihypertensive-drugs-scientific-guideline
18. Geoffrey, Banks Why Do Clinical Trials Fail? Available online at: https://www.nuventra.com/resources/blog/why-do-clinical-trials-fail/
19. Hill PYC, li JS, Hornik CP. Pediatric trials of antihypertensive agents: impact of trial design and unique pediatric factors on efficacy end points. Clin Invest. (2014) 4:1031–41. doi: 10.4155/cli.14.98
20. Seven Reasons Why Clinical Trials Fail. By Artem Andrianov. (2014). Available online at: https://cyntegrity.com/7-reasons-clinical-trials-fail/
21. Why Do Clinical Trials Fail? By Geoffrey Banks. (2018). Available online at: https://www.nuventra.com/resources/blog/ why-do-clinical-trials-fail/
22. Brewster R, Wong M, Magnani CJ, Gunningham H, Hoffer M, Showalter S, et al. Early discontinuation, results reporting, and publication of pediatric clinical trials. Pediatrics. (2022) 149:e2021052557. doi: 10.1542/peds.2021-052557
23. Chaturvedi S, Lipszyc DH, Licht C, Craig JC, Parekh R. Pharmacological interventions for hypertension in children. Cochrane Database Syst Rev. (2014) 2:CD008117. doi: 10.1002/14651858.CD008117.pub2
24. Burrello J, Erhardt EM, Saint-Hilary G, Veglio F, Rabbia F, Mulatero P, et al. Pharmacological treatment of arterial hypertension in children and adolescents: a network meta-analysis. Hypertension. (2018) 72:306–13. doi: 10.1161/HYPERTENSIONAHA.118.10862
25. Falkner B, Onesti G, Lowenthal DT, Affrime MB. Use of clonidine monotherapy (versus diuretics) in adolescent hypertension. Chest. (1983) 83:425–7. doi: 10.1378/chest.83.2.425
26. Bachmann H. Propranolol versus chlorthalidone—a prospective therapeutic trial in children with chronic hypertension. Helv Paediatr Acta. (1984) 39:55–61.
27. Li JS, Flynn JT, Portman R, Davis I, Ogawa M, Shi H, et al. The efficacy and safety of the novel aldosterone antagonist eplerenone in children with hypertension: a randomized, double-blind, dose-response study. J Pediatr. (2010) 157:282–7. doi: 10.1016/j.jpeds.2010.02.042
28. Sorof JM, Cargo P, Graepel J, Humphrey D, King E, Rolf C, et al. Beta-blocker/thiazide combination for treatment of hypertensive children: a randomized double-blind, placebocontrolled trial. Pediatr Nephrol. (2002) 17:345–50. doi: 10.1007/s00467-002-0851-0
29. Batisky DL, Sorof JM, Sugg J, Llewellyn M, Klibaner M, Hainer JW, et al. Efficacy and safety of extended-release metoprolol succinate in hypertensive children 6 to 16 years of age: a clinical trial experience. J Pediatr. (2007) 150:134–9. doi: 10.1016/j.jpeds.2006.09.034
30. Tabbutt S, Nicolson SC, Adamson PC, Zhang X, Hoffman ML, Wells W, et al. The safety, efficacy, and pharmacokinetics of esmolol for blood pressure control immediately after repair of coarctation of the aorta in infants and children: a multicenter, double-blind, randomized trial. J Thorac Cardiovasc Surg. (2008) 136:321–8. doi: 10.1016/j.jtcvs.2007.09.086
31. Di Salvo G, Castaldi B, Gala S, Baldini L, Del Gaizo F, D'Aiello FA, et al. Atenolol vs enalapril in young hypertensive patients after successful repair of aortic coarctation. J Hum Hypertens. (2016) 30:363–7. doi: 10.1038/jhh.2015.87
32. Rogan JW, Lyszkiewicz DA, Blowey D, Khattak S, Arbus GS, Koren G, et al. randomized prospective crossover trial of amlodipine in pediatric hypertension. Pediatr Nephrol. (2000) 14:1083–7. doi: 10.1007/s004670000400
33. Trachtman H, Frank R, Mahan JD, Portman R, Restaino I, Matoo TK, et al. Clinical trial of extended-release felodipine in pediatric essential hypertension. Pediatr Nephrol. (2003) 18:548–53. doi: 10.1007/s00467-003-1134-0
34. Flynn JT, Newburger JW, Daniels SR, Sanders SP, Portman RJ, Hogg RJ, et al. A randomized, placebo-controlled trial of amlodipine in children with hypertension. J Pediatr. (2004) 145:353–9. doi: 10.1016/j.jpeds.2004.04.009
35. Soergel M, Verho M, Wühl E, Gellermann J, Teichert L, Schärer K. Effect of ramipril on ambulatory blood pressure and albuminuria in renal hypertension. Pediatr Nephrol. (2000) 15:113–8. doi: 10.1007/s004670000422
36. Seeman T, Dusek J, Vondrák K, Flögelová H, Geier P, Janda J. Ramipril in the treatment of hypertension and proteinuria in children with chronic kidney diseases. Am J Hypertens. (2004) 17:415–20. doi: 10.1016/j.amjhyper.2004.01.008
37. ESCAPE Trial Group, Wühl E, Trivelli A, Picca S, Litwin M, Peco-Antic A, et al. Strict blood-pressure control and progression of renal failure in children. N Engl J Med. (2009) 361:1639–50. doi: 10.1056/NEJMoa0902066
38. Wells T, Frame V, Soffer B, Shaw W, Zhang Z, Herrera P, et al. A double-blind, placebo-controlled, dose-response study of the effectiveness and safety of enalapril for children with hypertension. J Clin Pharmacol. (2002) 42:870–80. doi: 10.1177/009127002401102786
39. Soffer B, Zhang Z, Miller K, Vogt BA, Shahinfar S, A. double-blind, placebo-controlled, dose-response study of the effectiveness and safety of lisinopril for children with hypertension. Am J Hypertens. (2003) 16:795–800. doi: 10.1016/S0895-7061(03)00900-2
40. Li JS, Berezny K, Kilaru R, Hazan L, Portman R, Hogg R, et al. Is the extrapolated adult dose of fosinopril safe and effective in treating hypertensive children? Hypertension. (2004) 44:289–93. doi: 10.1161/01.HYP.0000138069.68413.f0
41. Schaefer F, Litwin M, Zachwieja J, Zurowska A, Turi S, Grosso A, et al. Efficacy and safety of valsartan compared to enalapril in hypertensive children: a 12-week, randomized, double-blind, parallel-group study. J Hypertens. (2011) 29:2484–90. doi: 10.1097/HJH.0b013e32834c625c
42. Shahinfar S, Cano F, Soffer BA, Ahmed T, Santoro EP, Zhang Z, et al. A double-blind, dose-response study of losartan in hypertensive children. Am J Hypertens. (2005) 18:183–90. doi: 10.1016/j.amjhyper.2004.09.009
43. Flynn JT, Meyers KE, Neto JP, de Paula Meneses R, Zurowska A, Bagga A, et al. Efficacy and safety of the angiotensin receptor blocker valsartan in children with hypertension aged 1 to 5 years. Hypertension. (2008) 52:222–8. doi: 10.1161/HYPERTENSIONAHA.108.111054
44. Trachtman H, Hainer JW, Sugg J, Teng R, Sorof JM, Radcliffe J, et al. Efficacy, safety, and pharmacokinetics of candesartan cilexetil in hypertensive children aged 6 to 17 years. J Clin Hypertens. (2008) 10:743–50. doi: 10.1111/j.1751-7176.2008.00022.x
45. Wells TG, Portman R, Norman P, Haertter S, Davidai G, Wang F. Safety, efficacy, and pharmacokinetics of telmisartan in pediatric patients with hypertension. Clin Pediatr. (2010) 49:938–46. doi: 10.1177/0009922810363609
46. Hazan L, Hernández Rodriguez OA, Bhorat AE, Miyazaki K, Tao B, Heyrman R, et al. A double-blind, dose-response study of the efficacy and safety of olmesartan medoxomil in children and adolescents with hypertension. Hypertension. (2010) 55:1323–30. doi: 10.1161/HYPERTENSIONAHA.109.147702
47. Schaefer F, van de Walle J, Zurowska A, Gimpel C, van Hoeck K, Drozdz D, et al. Efficacy, safety and pharmacokinetics of candesartan cilexetil in hypertensive children from 1 to less than 6 years of age. J Hypertens. (2010) 28:1083–90. doi: 10.1097/HJH.0b013e328336b86b
48. Meyers KEC, Lieberman K, Solar-Yohay S, Han G, Shi V. The efficacy and safety of valsartan in obese and nonobese pediatric hypertensive patients. J Clin Hypertens. (2011) 13:758–66. doi: 10.1111/j.1751-7176.2011.00502.x
49. Wells T, Blumer J, Meyers KE, Neto JP, Meneses R, Litwin M, et al. Effectiveness and safety of valsartan in children aged 6 to 16 years with hypertension. J Clin Hypertens. (2011) 13:357–65. doi: 10.1111/j.1751-7176.2011.00432.x
50. Webb NJ, Lam C, Shahinfar S, Strehlau J, Wells TG, Gleim GW, et al. Efficacy and safety of losartan in children with Alport syndrome–results from a subgroup analysis of a prospective, randomized, placebo- or amlodipine-controlled trial. Nephrol Dial Transplant. (2011) 26:2521–6. doi: 10.1093/ndt/gfq797
51. Schaefer F, Coppo R, Bagga A, Senguttuvan P, Schlosshauer R, Zhang Y, et al. Efficacy and safety of valsartan in hypertensive children 6 months to 5 years of age. J Hypertens. (2013) 31:993–1000. doi: 10.1097/HJH.0b013e32835f5721
52. Webb NJ, Wells TG, Shahinfar S, Massaad R, Dankner WM, Lam C, et al. A randomized, open-label, dose-response study of losartan in hypertensive children. Clin J Am Soc Nephrol. (2014) 9:1441–8. doi: 10.2215/CJN.11111113
53. Lou-Meda R, Stiller B, Antonio ZL, Zielinska E, Yap HK, Kang HG, et al. Long-term safety and tolerability of valsartan in children aged 6 to 17 years with hypertension. Pediatr Nephrol. (2019) 34:495–506. doi: 10.1007/s00467-018-4114-0
54. Jankauskiene A, Drozdz D, Wasilewska A, de Paula-Bernardes R, Glazer R, Valentin M, et al. Efficacy and safety of valsartan in children aged 1-5 years with hypertension, with or without chronic kidney disease: a randomized, double-blind study followed by open-label phase. Curr Med Res Opin. (2021) 37:2113–22. doi: 10.1080/03007995.2021.1982681
55. Ito S, Nishiyama Y, Sugiura K, Enya K. Safety and efficacy of azilsartan in paediatric patients with hypertension: a phase 3, single-arm, open-label, prospective study. Clin Exp Nephrol. (2022) 26:350–8. doi: 10.1007/s10157-021-02159-9
57. Kravitz RL, Duan N eds the DEcIDE Methods Center N-of-1 Guidance Panel. Design and Implementation of N-of-1 Trials: A User's Guide. AHRQ Publication No. 13(14)-EHC122-EF. Rockville, MD: Agency for Healthcare Research and Quality (2014).
58. Samuel JP, Tyson JE, Green C, Bell CS, Pedroza C, Molony D, et al. Treating hypertension in children with n-of-1 trials. Pediatrics. (2019) 143:e20181818. doi: 10.1542/peds.2018-1818
59. Omboni S, McManus RJ, Bosworth HB, Chappell LC, Green BB, Kario K, et al. Evidence and recommendations on the use of telemedicine for the management of arterial hypertension: an international expert position paper. Hypertension. (2020) 76:1368–83. doi: 10.1161/HYPERTENSIONAHA.120.15873
60. Aydemir S, Ocak S, Saygili S, Hopurcuoglu D, Haşlak F, Kiykim E, et al. Telemedicine applications in a tertiary pediatric hospital in turkey during COVID-19 pandemic. Telemed J E Health. (2021) 27:1180–7. doi: 10.1089/tmj.2020.0381
61. Omboni S, Caserini M, Coronetti C. Telemedicine and M-Health in hypertension management: technologies, applications and clinical evidence. High Blood Press Cardiovasc Prev. (2016) 23:187–96. doi: 10.1007/s40292-016-0143-6
62. Purcell R, McInnes S, Halcomb EJ. Telemonitoring can assist in managing cardiovascular disease in primary care: a systematic review of systematic reviews. BMC Fam Pract. (2014) 15:43. doi: 10.1186/1471-2296-15-43
63. Krittanawong C, Zhang H, Wang Z, Aydar M, Kitai T. Artificial intelligence in precision cardiovascular medicine. J Am Coll Cardiol. (2017) 69:2657–64. doi: 10.1016/j.jacc.2017.03.571
64. Bzdok D, Altman N, Krzywinski M. Statistics versus machine learning. Nat Methods. (2018) 15:233–4. doi: 10.1038/nmeth.4642
65. Bzdok D, Krzywinski M, Altman N. Points of significance: machine learning: a primer. Nat Methods. (2017) 14:1119–20. doi: 10.1038/nmeth.4526
66. Niel O, Bastard P, Boussard C, Hogan J, Kwon T, Deschênes G. Artificial intelligence outperforms experienced nephrologists to assess dry weight in pediatric patients on chronic hemodialysis. Pediatr Nephrol. (2018) 33:1799–803. doi: 10.1007/s00467-018-4015-2
Keywords: clinical trial (2.172), children, adolescents, antihypertensive drug, pharmacological treatment
Citation: Redon J, Seeman T, Pall D, Suurorg L, Kamperis K, Erdine S, Wühl E and Mancia G (2022) Narrative update of clinical trials with antihypertensive drugs in children and adolescents. Front. Cardiovasc. Med. 9:1042190. doi: 10.3389/fcvm.2022.1042190
Received: 12 September 2022; Accepted: 04 November 2022;
Published: 21 November 2022.
Edited by:
Giuseppe Maiolino, University Hospital of Padua, ItalyReviewed by:
Skaiste Sendzikaite, Vilnius University, LithuaniaLorenzo A. Calò, University of Padua, Italy
Copyright © 2022 Redon, Seeman, Pall, Suurorg, Kamperis, Erdine, Wühl and Mancia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Josep Redon, am9zZXAucmVkb25AdXYuZXM=