 Muhannad J. Ababneh1*
Muhannad J. Ababneh1* Abdullah Al-Kasasbeh1
Abdullah Al-Kasasbeh1 Mohamad Jarrah1
Mohamad Jarrah1 Lujain Malkawi2
Lujain Malkawi2 Omar Sanduka3
Omar Sanduka3 Areje M. Smadi3
Areje M. Smadi3 Mahmoud M. Smadi4
Mahmoud M. Smadi4- 1Division of Cardiology, Department of Internal Medicine, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan
- 2Department of Internal Medicine, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan
- 3Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan
- 4Department of Mathematics and Statistics, Jordan University of Science and Technology, Irbid, Jordan
Purpose: This retrospective observational study was conducted to assess the clinical characteristics and outcomes of hospitalized COVID-19 patients with positive cardiac enzymes in the King Abdullah University Hospital (KAUH) in Irbid, Jordan.
Patients and methods: A total of 676 patients admitted to KAUH for moderate-to-severe COVID-19 were included in the study. Clinical and mortality data were collected from patients’ electronic medical records.
Results: A significant association was found between myocardial injury and In-hospital mortality. Seven comorbidities were identified as risk factors for myocardial injury: Hypertension, diabetes mellitus (DM), previous cerebrovascular accident (CVA), ischemic heart disease (IHD), heart failure, chronic kidney disease (CKD), and cardiac arrhythmias. The need for intensive care unit (ICU) for invasive ventilation was also associated with myocardial injury. Acute kidney injury (AKI) during hospitalization had a significantly higher incidence of myocardial injury and mortality. Acute myocardial infarction (MI) and acute peripheral vascular disease (PVD) were also associated with higher mortality.
Conclusion: Myocardial injury is an important predictor of mortality in patients with moderate-to-severe COVID-19 disease. Patients with a history of hypertension, diabetes mellitus, any vascular diseases, cardiac arrhythmias or heart failure are considered high-risk for adverse outcome. Additionally, COVID-19 patients with myocardial injury and acute kidney injury were recognized with the highest mortality rate.
Introduction
The COVID-19 pandemic remains to be a global health crisis. Attempts from the scientific community to better understand this disease continue to reveal new characteristics of the novel coronavirus (SARS-CoV-2), ranging from diagnostic challenges to disease mechanisms. Initially thought of as a solely respiratory disease, manifestations of COVID-19 in different organ systems are constantly being reported. While several healthcare professionals and institutions have described vascular thrombotic complications (1), other studies reporting gastrointestinal (2), neurological (3), and cardiac (4) events have emerged. Despite the growing body of literature on the cardiovascular manifestations of moderate-to-severe COVID-19 disease, many questions remain unanswered. More research is needed to better understand the risk, mechanisms, and outcomes of cardiac disease associated with COVID-19 infections.
In the current literature, there has been increasing evidence suggesting cardiovascular involvement in COVID-19 disease. A recent meta-analysis of 35 studies has estimated the frequency of newly developed acute cardiac injury in COVID-19 patients to be more than 25%, in addition to other manifestations such as heart failure and arrhythmias (5). Similar evidence has led other studies to investigate elevation in cardiac biomarkers, such as troponin I, as a potential prognostic factor. A meta-analysis of 10 studies found that 51% of patients with poor outcomes had elevated serum troponin I levels, suggesting that troponin I, and possibly other cardiac biomarkers, could be utilized as a valuable predictor of severe COVID-19 disease (6). Poor outcomes were defined by need for intensive care unit (ICU) admission, oxygen saturation below 90%, invasive mechanical ventilation and in-hospital mortality (6). Another study of 100 patients who had echocardiographic investigations found that 39% of patients had right ventricular dilation and dysfunction and that elevated troponin I levels were associated with worse right ventricular function (7). The mechanisms of myocardial injury in COVID-19 infections remain unclear. There have been a few case reports of COVID-19 infections complicated by myocarditis, though there is no evidence ruling out other pathologies such as supply/demand mismatch and systemic inflammation (8, 9). It is important to note that myocardial injury has been observed in cases of acute respiratory distress syndrome (ARDS) unrelated to the novel coronavirus. A prospective cohort study in 2017 revealed that high-sensitivity troponin I (hsTroponin I) was detectable in 94% of patients with ARDS (10). This suggests that direct cardiotoxicity may not be necessary for myocardial injury in COVID-19 patients, since ARDS in general can cause an elevation in serum hsTroponin I. Despite the increasing evidence of myocardial injury in COVID-19 infections, current understanding of the prognostic value of such findings is quite poor. This calls for further research to assess both the outcomes and initial clinical characteristics of those patients. Additionally, none of the studies assessing cardiac biomarkers in COVID-19 patients was conducted in the MENA region (Middle East and North Africa), which indicates that studies in the region are needed to improve our understanding of this disease and its impacts on this population, and to make similar results obtained from other researcher generalisable.
Materials and methods
In this work, the retrospective cohort study approach was adopted for analysis of COVID-19 patients hospitalized in King Abdullah University Hospital (KAUH). King Abdullah University Hospital (affiliated with Jordan University of Science and Technology), is a tertiary referral center that serves patients from North of Jordan, the majority of them are Arabs. The indication for admission were the existing of severe hypoxia defined as O2 saturation below 90% or patients with other comorbidities and clinical instability. The targeted group were investigated for elevated troponin I levels and/or electrocardiogram (ECG) abnormalities during the period between 1 September and 31 December 2020. Data were collected from the patients’ electronic medical records. The parameters used in the study included demographic information, hospital admission duration, full medical history including presenting illness, past medical and surgical history, physical exam findings, vital signs, ECG findings, serum troponin I (normal range 0.0–0.02 ng/ml) and other biomarker levels [c reactive protein (CRP), and creatine kinase MB (CK-MB)], intensive care unit (ICU) admission, use of mechanical ventilation, occurrence of acute complications during hospitalization (cardiac infarction, cerebral or peripheral vascular complications, and acute kidney injury), and in-hospital mortality.
Descriptive statistics were used to summarize and determine the sample patients’ characteristics and distribution of patients’ data. Among descriptive statistics, we determined the range, mean, standard deviation (S.D), and median for the continuous variables and counts, percentages, and cross tabulation for the categorical variables. Also, we presented visual examination of data using clustered bar charts and error bar charts. Inferential statistics were also used to assess associations between categorical variables and group comparisons between quantitative variables. Associations between two or more qualitative data variables were assessed using Fishers exact test and Cramer’s V test. Quantitative data between more independent groups were analyzed using two independent samples t-test and One-way ANOVA procedure. Multivariate binary logistic regression was conducted to assess the influence of different qualitative and quantitative risk variables associated with different outcomes. All P-values presented were two-tailed, and P-values < 0.05 were considered as statistically significant. All statistical analyses were performed using statistical package SPSS 21.0 (SPSS Inc., Chicago, IL).
Results and discussion
Patients’ characteristics
A total of 676 patients were included in the study, 56.8% of which were males. Their ages ranged between 16 and 96 years, with a mean of 64.50 ± 13.99 years. Analysis of the data showed that 38 patients are smokers (5.7%), including 6 female smokers (2.1%) out of 292 female patients and 32 male smokers (8.4%) out of 384 male patients. The recorded comorbidity rates of hypertension (HTN), diabetes mellitus (DM), pre-diabetes mellitus (pre-DM), pulmonary disease, hypercholesterolemia, ischemic heart disease (IHD), previous cerebrovascular accident (CVA), peripheral vascular disease (PVD), and chronic kidney disease (CKD) are shown in Table 1. Patients with positive cardiac enzymes were 50% of all included patients; 5% were in the myocardial infarction group including STEMI and NSTEMI (infarction group), and 45% were considered as myocardial injury group (injury group), the remaining 50% without elevation in cardiac enzymes were considered as no injury group. The Pie chart in Figure 1 demonstrates the distribution in the three study groups.
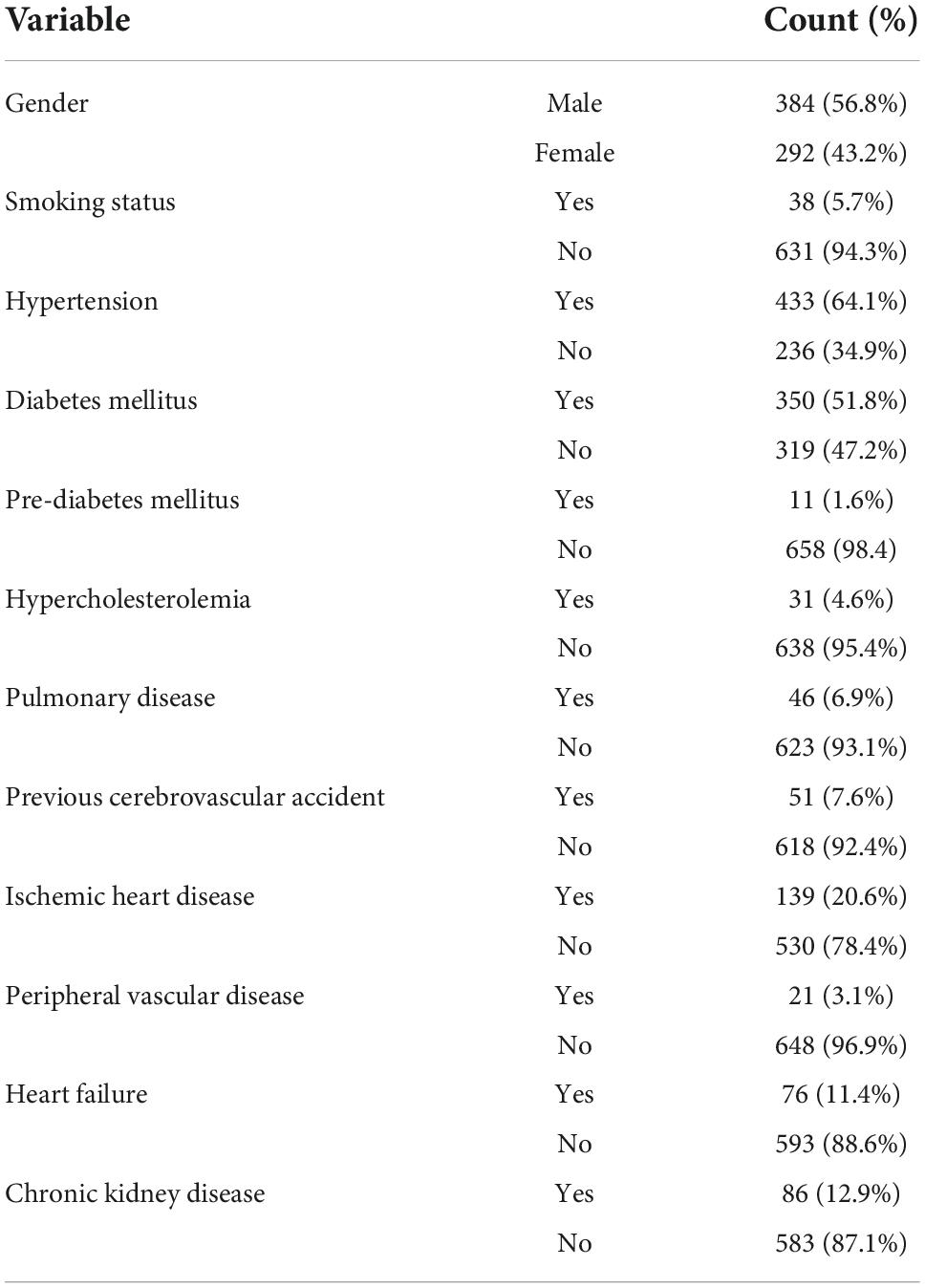
Table 1. Demographic characteristics of patients.
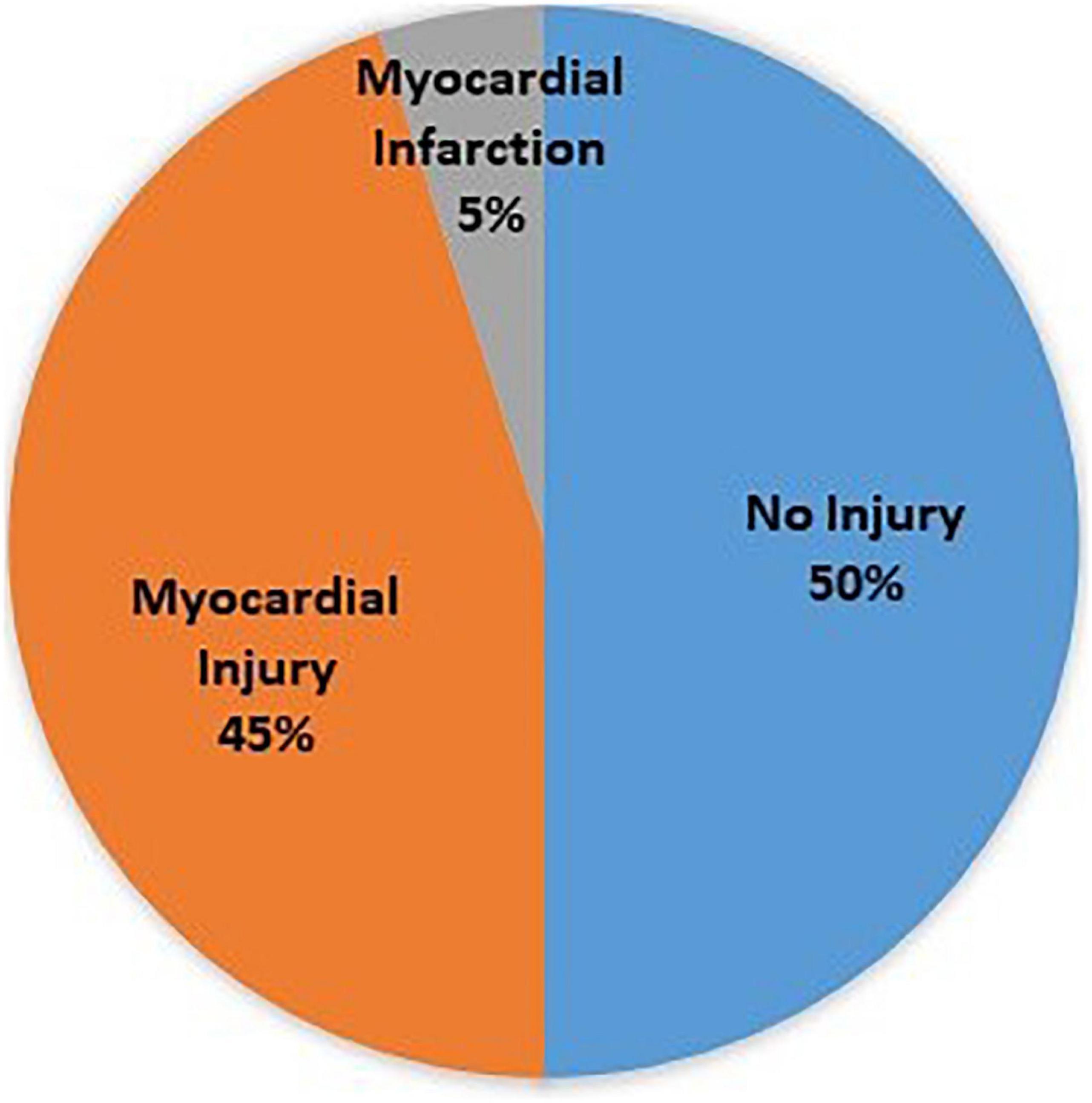
Figure 1. Pie chart of patient groups (no injury, injury, and infarction).
Characteristics of patients with positive cardiac enzymes
The patients were categorized into three groups according to their serial cardiac enzymes levels and clinical history notes. Patients with elevation in their cardiac enzymes without evidence of Myocardial infarction (MI) were categorized into the “injury” group. Patients with elevation in their cardiac enzymes in addition to clinical evidence of MI were classified as the “infarction” group. Clinical evidence of MI is defined as the presence of typical chest pain with ST elevation in ECG, ischemic ECG changes or changes in myocardial function (echocardiography). Patients who did not have elevation in their cardiac enzymes or evidence of infarction were set as the “no injury” group. A univariate analysis was conducted to assess the effect of different predictors on myocardial injury using Fisher exact test; the results are shown in Table 2. The following predictors were found to be statistically significant in predicting myocardial injury: Hypertension (p-value < 0.001), diabetes mellitus (p-value = < 0.001), previous CVA (p-value = 0.008), IHD (p-value < 0.001), HF (p-value < 0.001), CKD (p-value < 0.001), and pre-existing arrhythmia (p-value = 0.005).
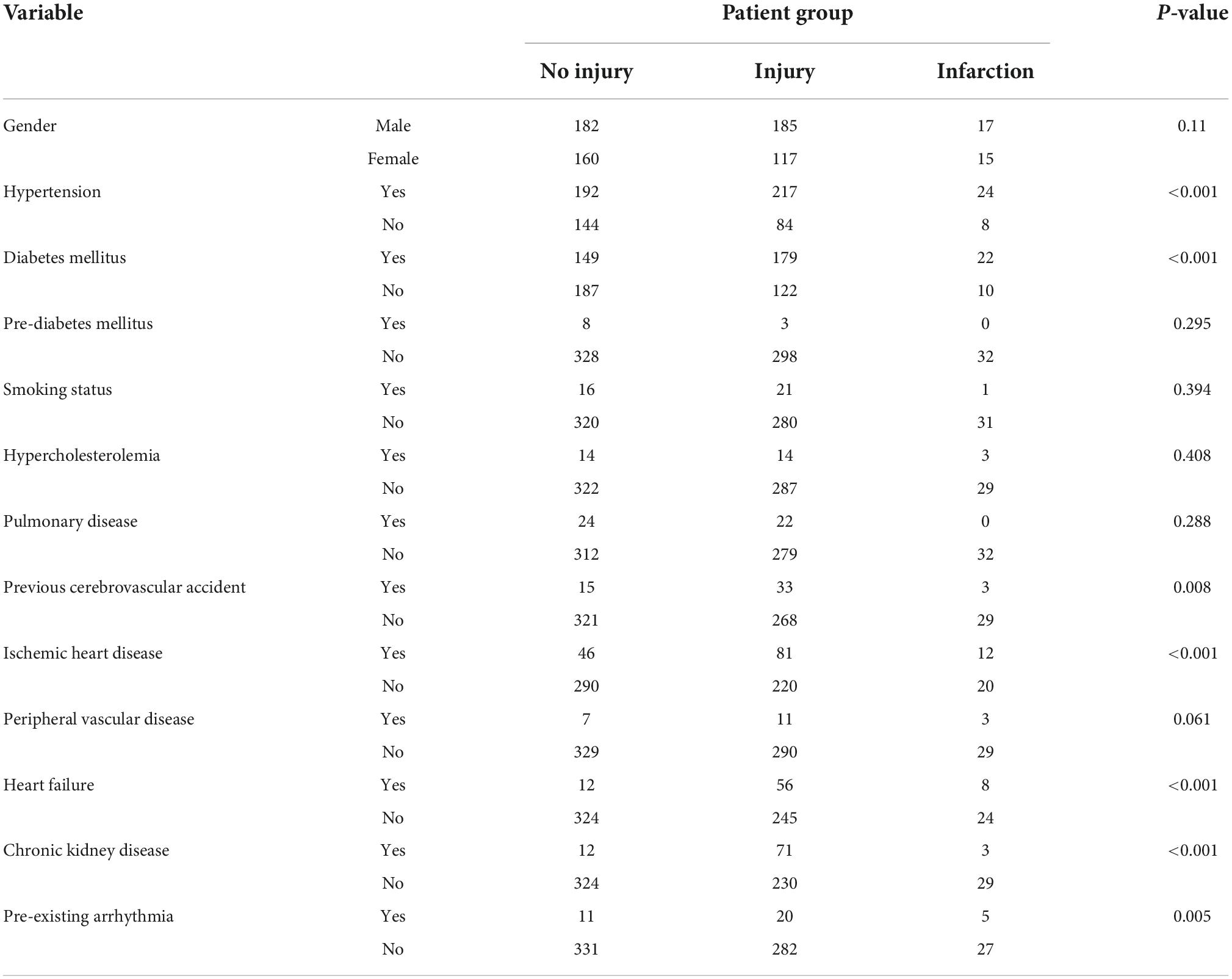
Table 2. Association between patient groups (no injury, injury, and infarction) and patients’ characteristics.
Multivariate binary logistic regression analysis was performed to assess the significance of a combination of different risk factors on myocardial injury (1: injury, 0: no injury). The candidate risk factors considered in the analysis were: Age, Hypertension (HTN), diabetes mellitus (DM), Smoking status, Hypercholesterolemia, pulmonary disease, previous cerebrovascular accident (CVA), ischemic heart disease (IHD), peripheral vascular disease (PVD), heart failure (HF), chronic kidney injury (CKD), and Pre-existing arrhythmia. A significant logistic regression equation was found using 14 predictors with an Nagelkerke R2 = 39.3%. The significant predictors for myocardial injury were gender, age, HF, DM, and CKD.
A univariate analysis was conducted to assess the effect of different predictors (patient admission for >24 h, ICU admission, and invasive ventilation) on the patient groups (injury, infarction, and no injury) using Cramer’s V test. The results are shown in Table 3. The following variables were found to be statistically significant predictors of myocardial injury: ICU admission and invasive ventilation with p-values < 0.001. Using one-WAY ANOVA procedure, significant differences were found for O2 saturation on admission, while no significant differences for the remaining vital signs on admission (respiratory rate, temperature, systolic blood pressure, and diastolic blood pressure), as depicted in Table 3.
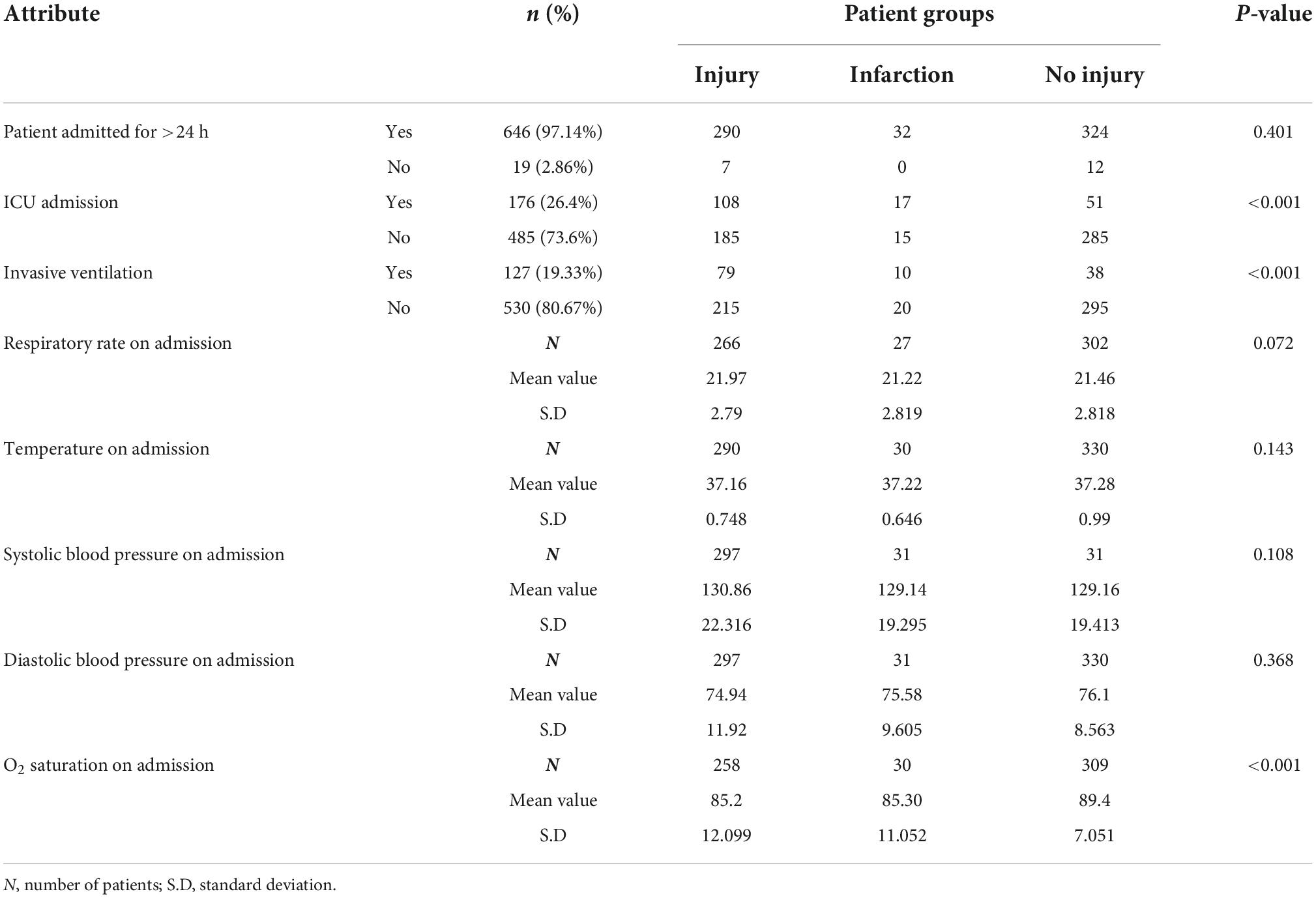
Table 3. Association and group comparisons between patient groups (injury, infarction, and no injury) and ICU admission, hospital admission for >24 h, invasive ventilation, and vital signs on admission.
In the stacked bar chart in Figure 2 we can demonstrate a significant correlation for the need of invasive mechanical ventilation in patients with myocardial involvement (injury of infarction).
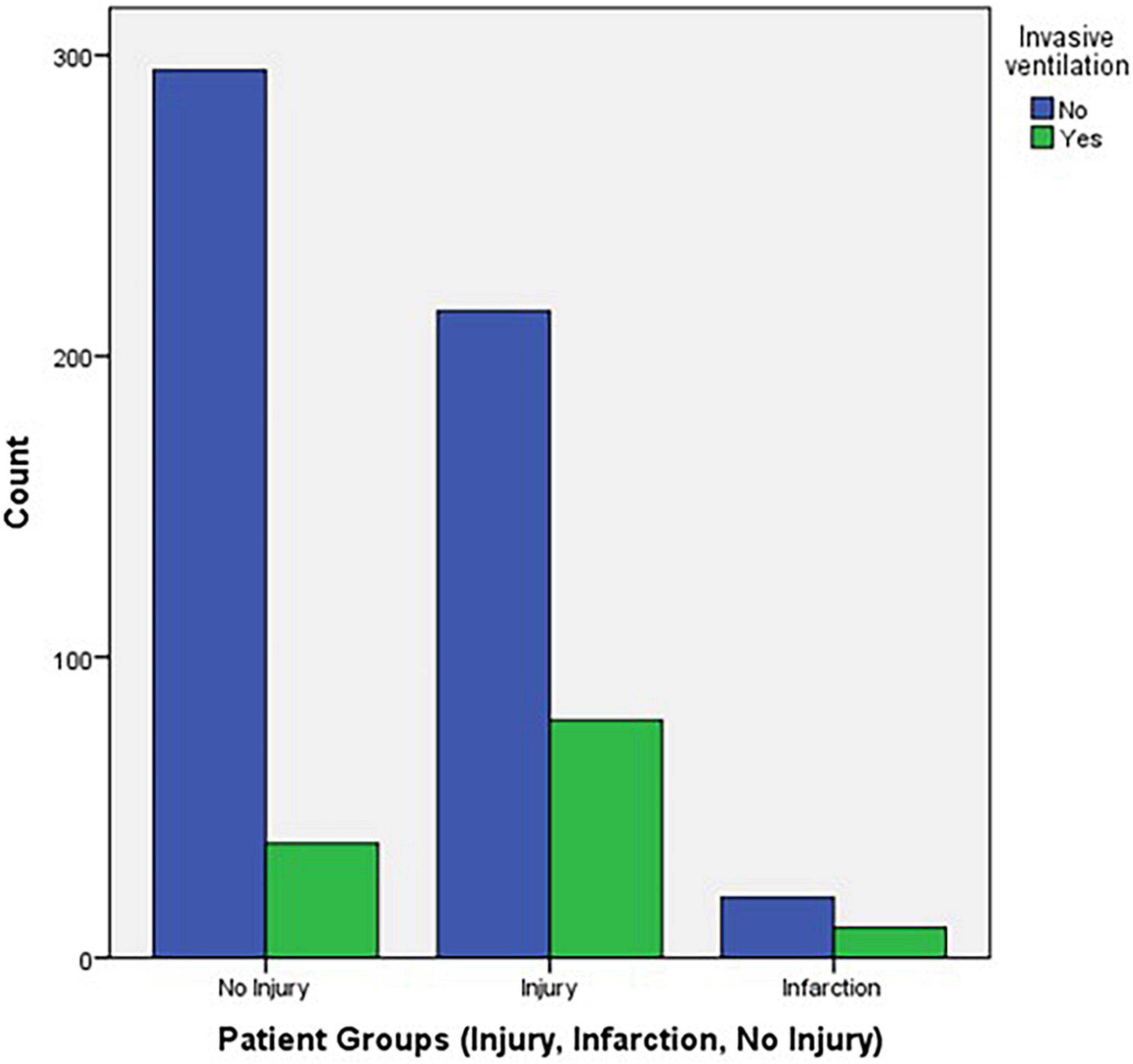
Figure 2. Stacked bar chart of invasive ventilation vs. patient groups.
Error bar plot of O2 saturation on admission in the different patient groups is also shown in Figure 3.
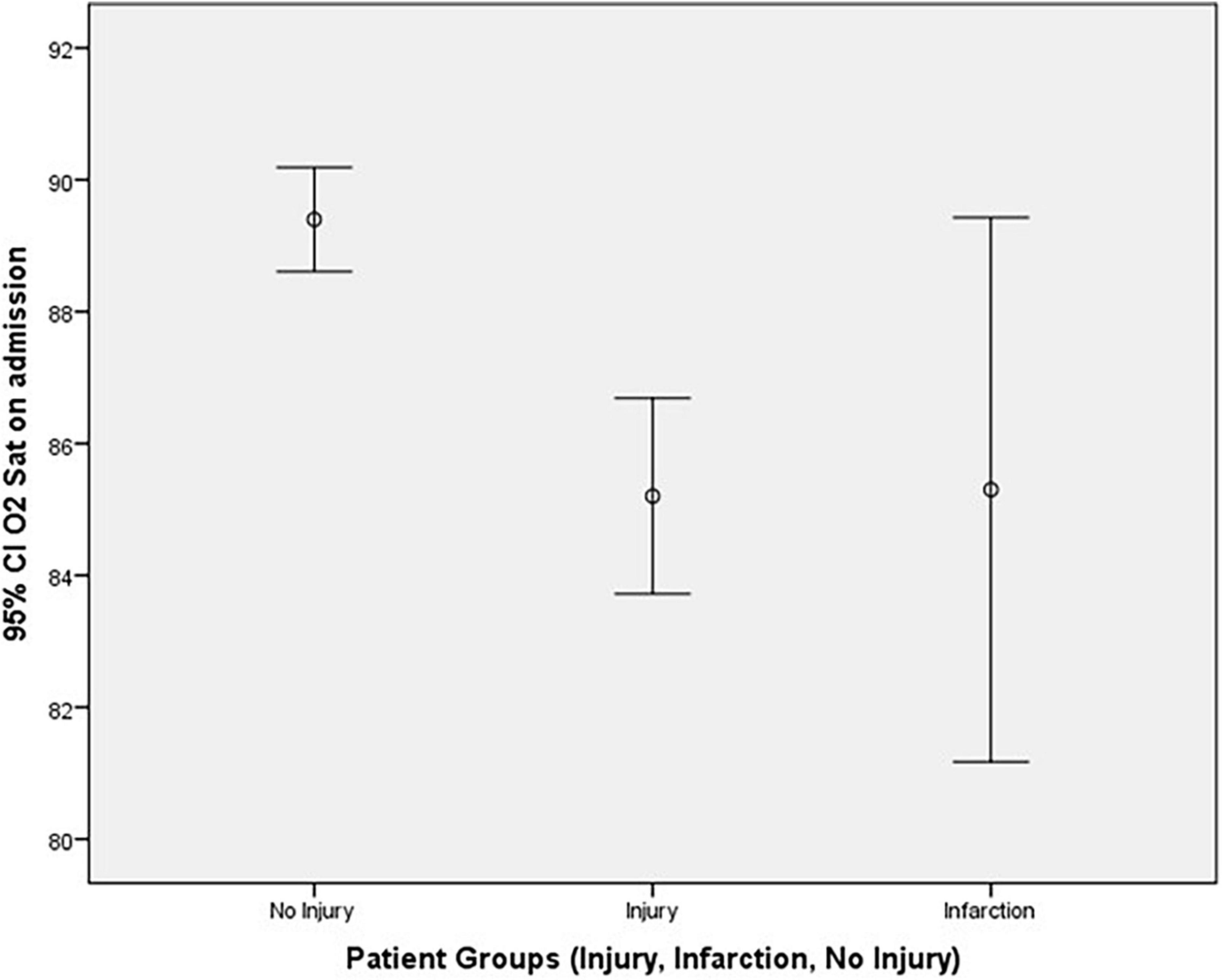
Figure 3. Error bar plot of O2 saturation on admission against patient groups.
Mortality and patient groups (injury, no injury, STEMI, and NSTEMI)
The “infarction” patient group was subdivided into two further groups according to their ECG findings: ST segment elevation MI (STEMI) and non-ST segment elevation MI (NSTEMI). A contingency table of mortality vs. patient groups (injury, no injury, STEMI, and NSTEMI) is shown in Table 4. A significant association between mortality and patient groups was detected with p-value < 0.001 using Cramer’s V test.

Table 4. Contingency table of mortality and patient groups (injury, no injury, STEMI, and NSTEMI).
Mortality with intensive care unit admission and invasive ventilation
To study the association between mortality and patients’ clinical findings, a univariate analysis was conducted to assess the effect of different predictors (patient admission for >24 h, ICU admission, and invasive ventilation) on the mortality using Fishers exact test. The results are shown in Table 5. The following predictors were found to be statistically significant in predicting mortality: Patient admission for >24 h (p-value = 0.025), ICU admission, and invasive ventilation with p-values < 0.001.
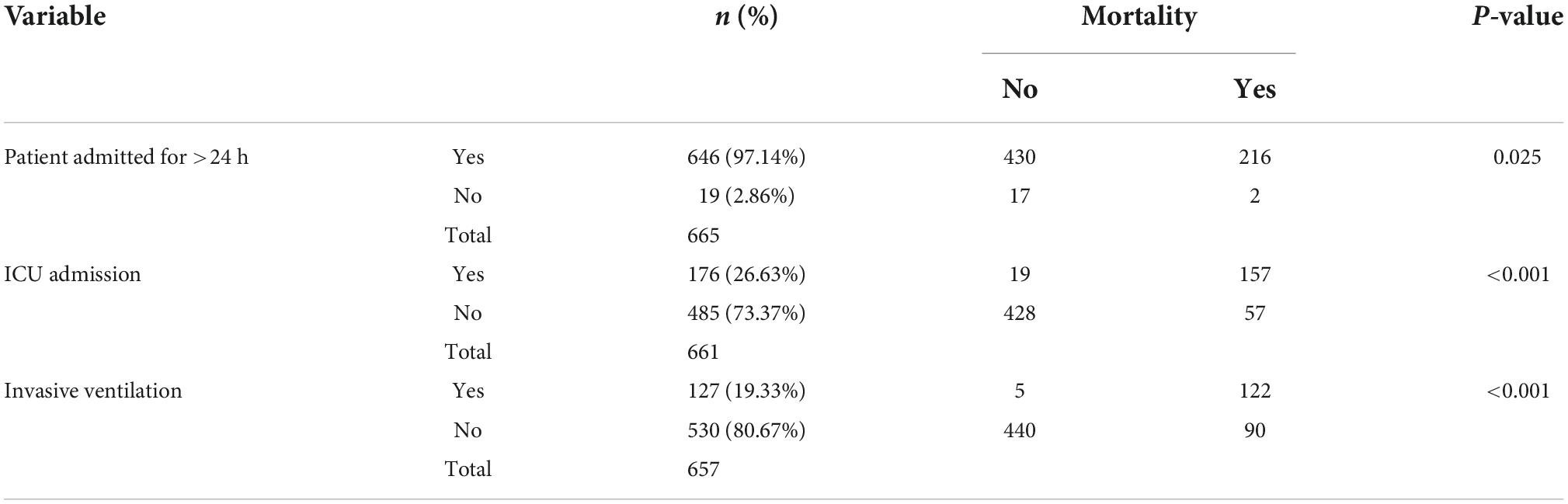
Table 5. Association and group comparisons of mortality with hospital admission for >24 h, ICU admission, and invasive ventilation.
Multivariate binary logistic regression analysis shows the significance of the risk factors patient admission for >24 h, ICU admission, and invasive ventilation on mortality and yields Nagelkerke measure of R2 = 67.9%.
Mortality and myocardial injury in patients with acute complications
The incidence of acute MI, acute kidney injury (AKI), acute peripheral vascular disease (PVD), and acute CVA was recorded. Table 6 demonstrates the incidence of acute complications and mortality during patients’ hospital stay:
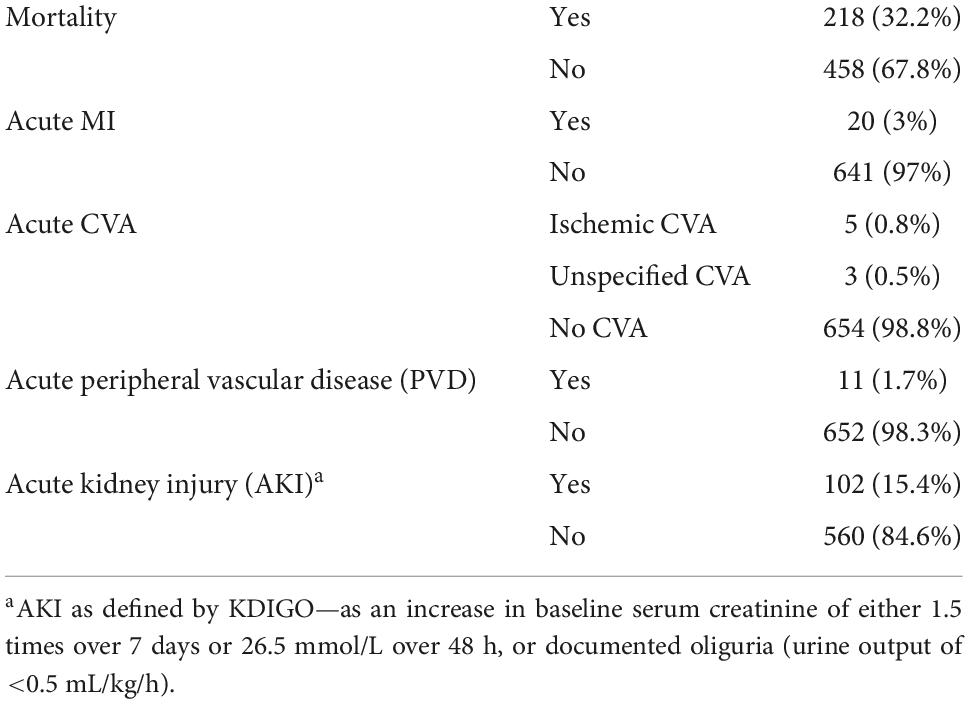
Table 6. Incidence of acute complications and mortality.
Statistical analyses were performed to investigate the association between the incidence of acute complications during hospitalization with myocardial injury (described as the three patient groups) (Table 7) and mortality (Table 8). Using Cramer’s V test, the incidence of acute kidney injury (AKI) was significantly associated with myocardial injury (p-value = <0.001).
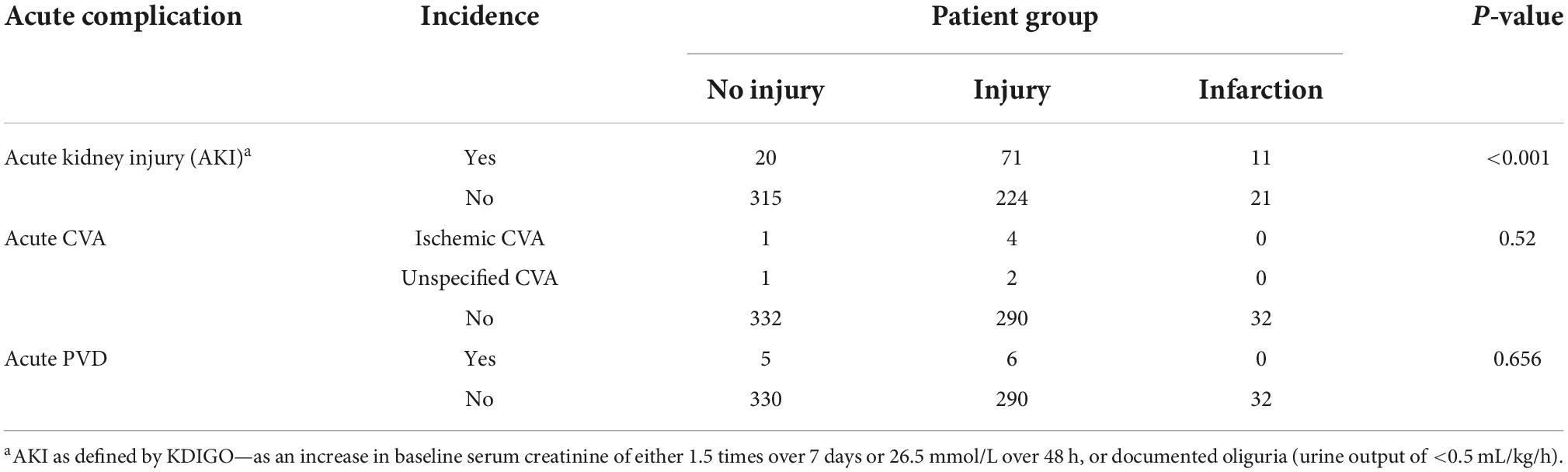
Table 7. Acute complications and patient groups (no injury, injury, and infarction).
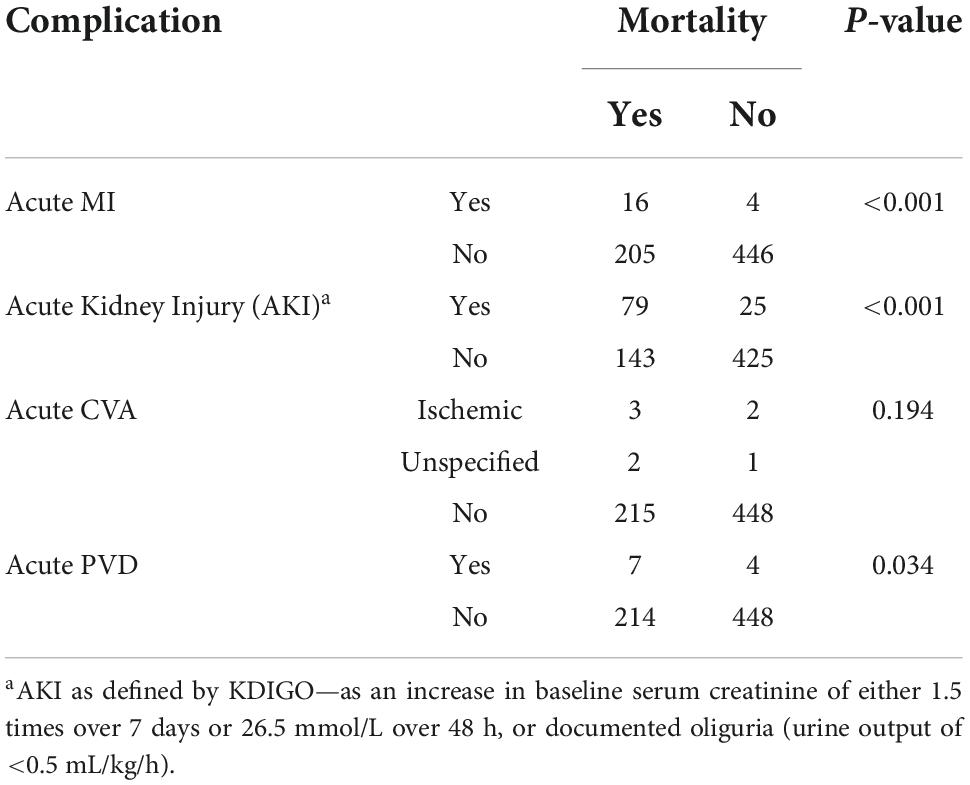
Table 8. Acute complications and mortality.
Using Fisher’s exact test, a significant association was found between mortality and the incidence of acute MI, AKI, and acute PVD. No significant association was found between mortality and acute CVA using Cramer’s V test. The results are displayed in Table 8.
Conclusion
The study demonstrates that myocardial injury, represented by elevation in serum troponin I, is an important predictor of mortality in patients with moderate-to-severe COVID-19 disease. Specifically, patients who are expected to suffer myocardial injury according to the findings are those with a medical history of hypertension, DM, CVA, IHD, heart failure, CKD, or cardiac arrhythmias. An early testing for elevated cardiac biomarkers (troponin I) can be used as a predictor for adverse outcome and complications and help in patients triage and need for admission.
The study also suggests that patients who require ICU admission, invasive ventilation, or both should have their serum troponin I levels monitored regularly during their hospital stay, as these readings can be a significant predictor of mortality.
The incidence of AKI during hospitalization was identified as a poor prognostic factor, as it was highly associated with myocardial injury and a higher In-hospital mortality. Other complications that were associated with higher In-hospital mortality were acute MI and acute PVD.
According to the findings of this study and considering the reports of cardiac complications of COVID-19 in the literature, a thorough investigation into the mechanisms of myocardial injury in COVID-19 disease would be recommended. We would also suggest further research of the incidence, pathophysiology, and potential predictors of AKI in COVID-19 patients.
Limitations
The authors believe that the prevalence of smokers in this study (5.7%) was underreported; a 2014 national survey by the World Health Organization found the prevalence of smokers in the Jordanian population to be around 32.3% (11). We hypothesize that this underestimation was due to underreporting, or incomplete documentation in the electronic records. The authors also believe that the prevalence of hypercholesterolemia in the study (4.6%) was below the actual figure due to lack of primary screening in the local community.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The collection and use of patients’ data was approved by the Institutional Review Board (IRB) of Jordan University of Science and Technology (JUST) and King Abdullah University Hospital (KAUH). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
MA: primary investigator, IRB proposal, supervising data collection and analysis, and manuscript writing and editing. AA-K and MJ: supervising data collection and manuscript preparation. LM: IRB proposal, supervising data collection and manuscript preparation. OS: data collection, and manuscript writing and editing. AS: statistical analysis and manuscript editing. MS: supervising data collection, statistical analysis, and manuscript preparation. All authors contributed to the article and approved the submitted version.
Acknowledgments
We would like to thank our dedicated colleagues and students for their valuable contribution in data collection: Abdallah M. S. Aljabeiti, Noor A. Qasem, Rama S. K. Alqatarneh, and Qusai A. K. A. Ali (Jordan University of Science and Technology—Graduate Students—School of Medicine).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
KAUH, King Abdullah University Hospital; HTN, hypertension; DM, diabetes mellitus; MI, myocardial infarction; CKD, chronic kidney disease; IHD, ischemic heart disease; PVD, peripheral vascular disease; CVA, cerebrovascular accident; AKI, acute kidney injury; ICU, intensive care unit; STEMI, ST elevation myocardial infarction; NSTEMI, non-ST elevation myocardial infarction.
References
1. Al-Ani F, Chehade S, Lazo-Langner A. Thrombosis risk associated with COVID-19 infection. A scoping review. Thromb Res. (2020) 192:152–60. doi: 10.1016/j.thromres.2020.05.039
2. Cha MH, Regueiro M, Sandhu DS. Gastrointestinal and hepatic manifestations of COVID-19: a comprehensive review. World J Gastroenterol. (2020) 26:2323–32. doi: 10.3748/wjg.v26.i19.2323
3. Wang L, Shen Y, Li M, Chuang H, Ye Y, Zhao H, et al. Clinical manifestations and evidence of neurological involvement in 2019 novel coronavirus SARS-CoV-2: a systematic review and meta-analysis. J Neurol. (2020) 267:2777–89. doi: 10.1007/s00415-020-09974-2
4. Kunutsor SK, Laukkanen JA. Cardiovascular complications in COVID-19: a systematic review and meta-analysis. J Infect. (2020) 81:e139–41. doi: 10.1016/j.jinf.2020.05.068
5. Momtazmanesh S, Shobeiri P, Hanaei S, Mahmoud-Elsayed H, Dalvi B, Malakan Rad E. Cardiovascular disease in COVID-19: a systematic review and meta-analysis of 10,898 patients and proposal of a triage risk stratification tool. Egypt Heart J. (2020) 72:41. doi: 10.1186/s43044-020-00075-z
6. Malik P, Patel U, Patel NH, Somi S, Singh J. Elevated cardiac troponin i as a predictor of outcomes in COVID-19 hospitalizations: a meta-analysis. Infez Med. (2020) 28:500–6.
7. Szekely Y, Lichter Y, Taieb P, Banai A, Hochstadt A, Merdler I, et al. Spectrum of cardiac manifestations in COVID-19: a systematic echocardiographic study. Circulation. (2020) 142:342–53. doi: 10.1161/CIRCULATIONAHA.120.047971
8. Zeng J-H, Liu Y-X, Yuan J, Wang F-X, Wu W-B, Li J-X, et al. First case of COVID-19 complicated with fulminant myocarditis: a case report and insights. Infection. (2020) 48:773–7. doi: 10.1007/s15010-020-01424-5
9. Doyen D, Moceri P, Ducreux D, Dellamonica J. Myocarditis in a patient with COVID-19: a cause of raised troponin and ECG changes. Lancet. (2020) 395:1516. doi: 10.1016/S0140-6736(20)30912-0
10. Metkus TS, Guallar E, Sokoll L, Morrow D, Tomaselli G, Brower R, et al. Prevalence and prognostic association of circulating troponin in the acute respiratory distress syndrome. Crit Care Med. (2017) 45:1709–17. doi: 10.1097/CCM.0000000000002641
Keywords: SARS-CoV-2, COVID-19, troponin, myocardial infarction, acute kidney injury, risk stratification
Citation: Ababneh MJ, Al-Kasasbeh A, Jarrah M, Malkawi L, Sanduka O, Smadi AM and Smadi MM (2022) Myocardial injury and its correlation to mortality in hospitalized COVID-19 patients: A retrospective cohort study. Front. Cardiovasc. Med. 9:1039655. doi: 10.3389/fcvm.2022.1039655
Received: 09 September 2022; Accepted: 03 November 2022;
Published: 23 November 2022.
Edited by:
Amit K. Dey, National Institutes of Health (NIH), United StatesReviewed by:
Kumar Ashish, CarolinaEast Medical Center, United StatesAnubhav Jain, Michigan State University, United States
Copyright © 2022 Ababneh, Al-Kasasbeh, Jarrah, Malkawi, Sanduka, Smadi and Smadi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Muhannad J. Ababneh, bWphYmFibmVoQGp1c3QuZWR1Lmpv