
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 30 November 2022
Sec. Cardiac Rhythmology
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.1032633
 Yan-Guang Li1†
Yan-Guang Li1† Peng-Xin Xie1†
Peng-Xin Xie1† Alawi A. Alsheikh-Ali2
Alawi A. Alsheikh-Ali2 Wael AlMahmeed3Kadhim Sulaiman4
Wael AlMahmeed3Kadhim Sulaiman4 Nidal Asaad5Shu-Wang Liu1*Mohammad Zubaid6
Nidal Asaad5Shu-Wang Liu1*Mohammad Zubaid6 Gregory Y. H. Lip7,8*
Gregory Y. H. Lip7,8*Background: The prognostic impact of obesity on patients with atrial fibrillation (AF) remains under-evaluated and controversial.
Methods: Patients with AF from the Gulf Survey of Atrial Fibrillation Events (Gulf SAFE) registry were included, who were recruited from six countries in the Middle East Gulf region and followed for 12 months. A multivariable model was established to investigate the association of obesity with clinical outcomes, including stroke or systemic embolism (SE), bleeding, admission for heart failure (HF) or AF, all-cause mortality, and a composite outcome. Restricted cubic splines were depicted to illustrate the relationship between body mass index (BMI) and outcomes. Sensitivity analysis was also conducted.
Results: A total of 1,804 patients with AF and recorded BMI entered the final analysis (mean age 56.2 ± 16.1 years, 47.0% female); 559 (31.0%) were obese (BMI over 30 kg/m2). In multivariable analysis, obesity was associated with reduced risks of stroke/systematic embolism [adjusted odds ratio (aOR) 0.40, 95% confidence interval (CI), 0.18–0.89], bleeding [aOR 0.44, 95%CI, 0.26–0.74], HF admission (aOR 0.61, 95%CI, 0.41–0.90) and the composite outcome (aOR 0.65, 95%CI, 0.50–0.84). As a continuous variable, higher BMI was associated with lower risks for stroke/SE, bleeding, HF admission, all-cause mortality, and the composite outcome as demonstrated by the accumulated incidence of events and restricted cubic splines. This “protective effect” of obesity was more prominent in some subgroups of patients.
Conclusion: Among patients with AF, obesity and higher BMI were associated with a more favorable prognosis in the Gulf SAFE registry. The underlying mechanisms for this obesity “paradox” merit further exploration.
Atrial fibrillation (AF) is the most common sustained arrhythmia in clinical practice, with a prevalence of approximately 2–4% in adults (1). Attributing to the aging population (2), accumulation of risk factors (3), and the advancement of diagnostic techniques (4), the incidence of AF will continue to surge in the next decades (5, 6). AF significantly increases the risk of stroke (7), heart failure (HF)(8), dementia (9), and all-cause mortality (8), imposing a heavy burden on society and family (10) and healthcare costs (11).
As a well-known contributing factor to the development of AF (12–14), obesity has become a global problem in the past few decades. The number of overweight and obese people increased by 50% (from 26.5% in 1980 to 39% in 2015) and 80% (from 7% in 1980 to 12.5% in 2015), respectively, (15). However, the impact of obesity on AF prognosis is under-evaluated, and some studies suggest that weight loss can help reduce the burden of AF and delay AF progression (13, 16, 17). In contrast, other studies have indicated that the changes in body mass index (BMI) do not affect AF prognosis (18). Interestingly, obesity has also been associated with favorable AF prognosis in some reports (19–21), which is contrary to common sense and has been termed the “obesity paradox”(22).
Obesity is also prevalent in the Middle East region, which has attracted much attention recently (23). As revealed by a recent systematic analysis involving the Middle East region, the prevalences of obesity and overweight were 23% and over 30%, respectively,(24); which is comparative to the rest part of the globe, such as Asia (25), Europe (26), and America (27, 28).
However, insights into the prognostic role of obesity in patients with AF in this region are scarce. The present study aimed to investigate the prognostic impact of obesity and higher BMI on patients with AF in the Middle East Gulf region.
In the present study, the Gulf Survey of Atrial Fibrillation Events (Gulf-SAFE) registry was applied. The Gulf-SAFE registry is a multicenter, prospective, and observational study with a 12-month follow-up, aimed at providing insights into AF management and outcomes in the Gulf region of the Middle East (29). The inclusion criteria and follow-up methods for the Gulf-SAFE registry have been previously published (29). Briefly, Gulf-SAFE included adult patients from 23 hospitals in 6 countries in the Middle East Gulf region who presented to the Emergency Room from 15th October 2009 to 30th June 2010 with AF on electrocardiogram or heart rhythm strips recorded over 30 s of adult patients. All patients who agreed to be included were required to sign an informed consent form. Exclusion criteria were patients who were not expected to be followed up regularly. This study excluded patients who died in hospital (n = 81), lacked height (n = 106) or weight data (n = 3) to calculate BMI, and those who did not complete 12 follow-up visits (n = 52), enabling analysis in a total of 1,804 patients. The treatment plan of the patients included in the study was decided by the treating physician, without the intervention of the investigator. Outpatient or telephone follow-up was performed at 1, 6, and 12 months after enrollment. The study protocols were approved by each national or institutional ethics committee.
Continuous variables were expressed as mean and standard deviation, and categorical variables as frequencies and percentages. When comparing the differences between the two groups, the chi-square test was used for categorical variables, the independent samples t-test for normally distributed continuous variables and the Mann-Whitney U test for non-normally distributed continuous variables. The BMI was calculated as the body weight (Kg) divided by the square of height in meters. Obesity was defined as BMI ≥ 30 kg/m2. Per the protocol design of the Gulf SAFE registry, we do not have time-to-event variable, therefore we could only conduct risk-related analysis based on Logistic regression model. A logistic regression model was established to analyze the influence of obesity on AF prognosis, and the results were expressed as crude and adjusted odds ratio (aOR). The model was adjusted for the following covariates: sex, type of AF, hypertension, diabetes, coronary artery disease, HF, history of previous stroke or major bleeding, peripheral vascular disease, abnormal renal function, alcohol and smoking history, and baseline medications [aspirin, clopidogrel, angiotensin-converting enzyme inhibitors, angiotensin receptor blockers (ARBs), digoxin, statins, and warfarin]. The annual incidences of all available outcomes were calculated and expressed as per 100 patient years. Different BMIs were divided into four groups (BMI at < 25, 25–30, 30–35, and > 35 kg/m2) as ordered categorical variables, the incidence of different outcome events was the dependent variable, and the P-value obtained by Linear-by-Linear Association was the P for trend value. Restricted cubic splines were drawn for demonstrating the OR and 95% confidence interval (CI) of BMI for clinical outcomes, including stroke/systematic embolism (SE), bleeding (major or clinically relevant non-major bleeding), admission for AF or HF, all-cause mortality, and composite outcome events (a summary all above events). If any of the above-mentioned outcomes occurred, the composite outcome events were treated as positive. Sensitivity analysis was conducted to explore the impact of obesity on subgroups of patients with classified by gender, age, the presence of diabetes and hyperlipidemia. All analyses were performed using R (4.1.2 version). Two-sided P < 0.05 was considered statistically significant.
A total of 1,804 patients with AF (47.0% female, mean age 56.2 ± 16.1 years) were included in this study. According to the criteria of BMI ≥ 30 kg/m2, 559 people (31.0%) were identified as obese, of which 58.7% were female, and the average age was 59.1 ± 13.3 years. The clinical data and demographic characteristics of the patients are shown in Table 1.
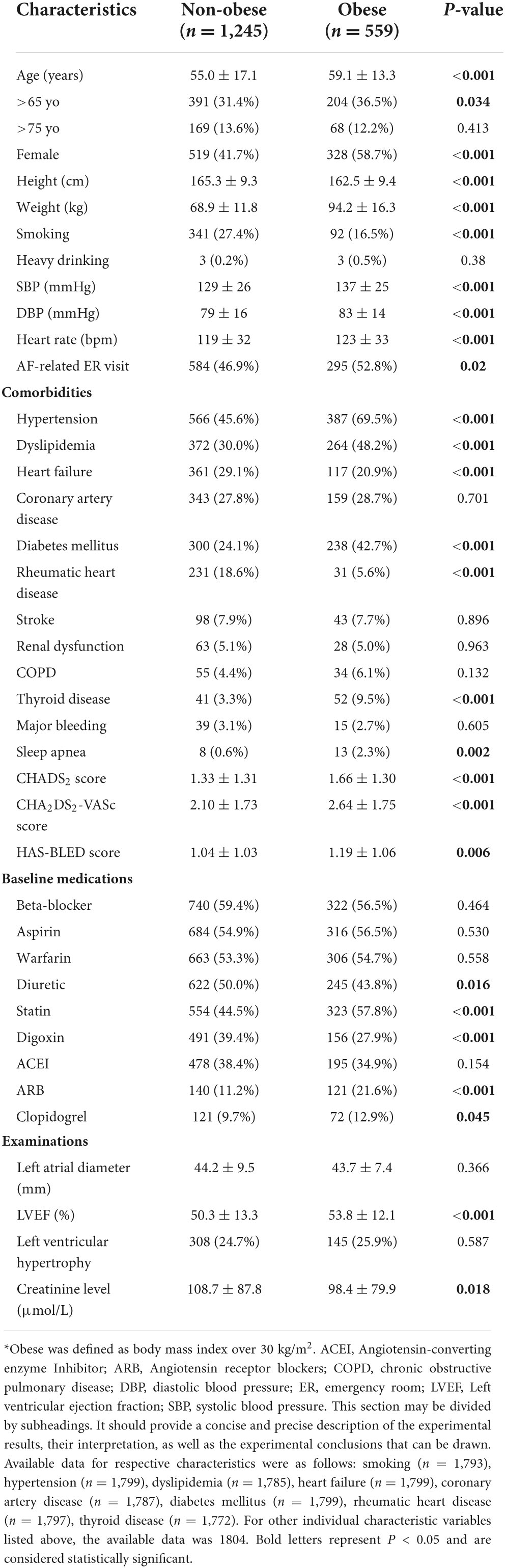
Table 1. Baseline characteristics of obese and non-obese patients with atrial fibrillation.
Obese patients were older, more female, less likely to smoke, and had faster heart rates and higher blood pressure on presentation (all P < 0.05). In addition, patients with obesity had higher prevalences of hypertension, dyslipidemia, diabetes, thyroid disease, and sleep apnea (P < 0.05, respectively). Some comorbidities were less common in obese patients, such as HF and rheumatic heart disease (see Table 1). Obese patients had higher mean CHADS2 (1.66 ± 1.30 vs. 1.33 ± 1.31), CHA2DS2-VASc (2.64 ± 1.75 vs. 2.10 ± 1.73) and HAS-BLED (1.19 ± 1.06 vs. 1.04 ± 1.03) scores (all P < 0.05). Patients with obesity were more likely to receive statins, ARBs, and clopidogrel, but less likely to use diuretics and digoxin (see Table 1).
During the 12-month follow-up period, there was a significant inverse association between BMI and the incidence of stroke/SE, bleeding, admission for HF, all-cause mortality, and the composite outcome showed a decreasing trend (see Table 2 and Figure 1) (P for trend < 0.001, respective), which were more prominent regarding the events of bleeding, HF admission, all-cause mortality, and the composite outcome. For patients with BMI at < 25, 25–30, 30–35 kg/m2, and > 35 kg/m2, the incidences of the composite outcome were 37.1 (32.2–42.6), 33.3 (29.2–38.9), 28.3 (22.6–34.8), and 24.3 (18.6–31.2) per 100 patient-years, respectively, (see Figure 1) (P for trend < 0.001).
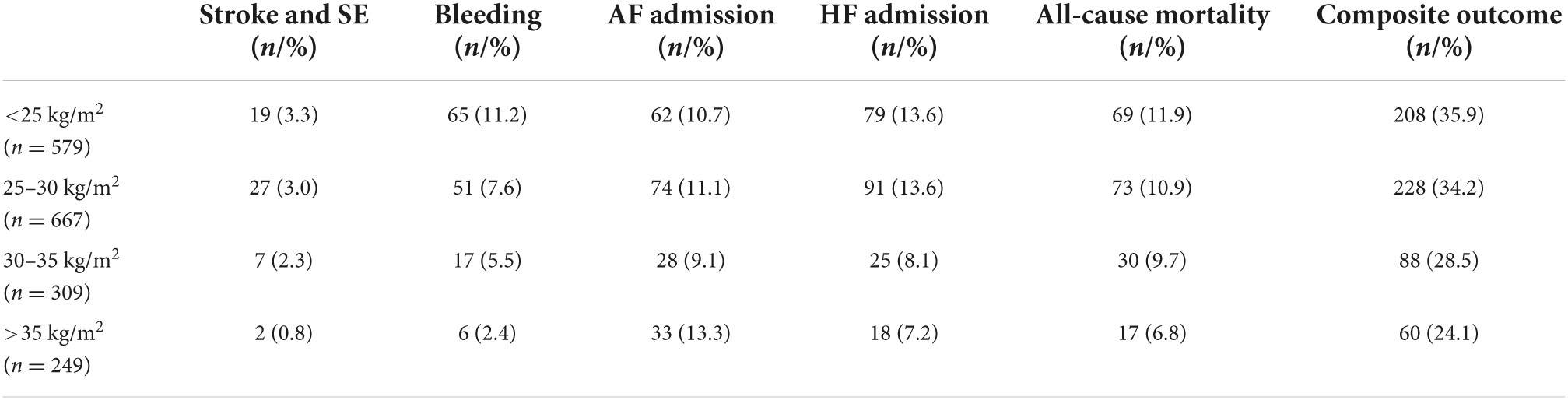
Table 2. BMI category and outcome events.
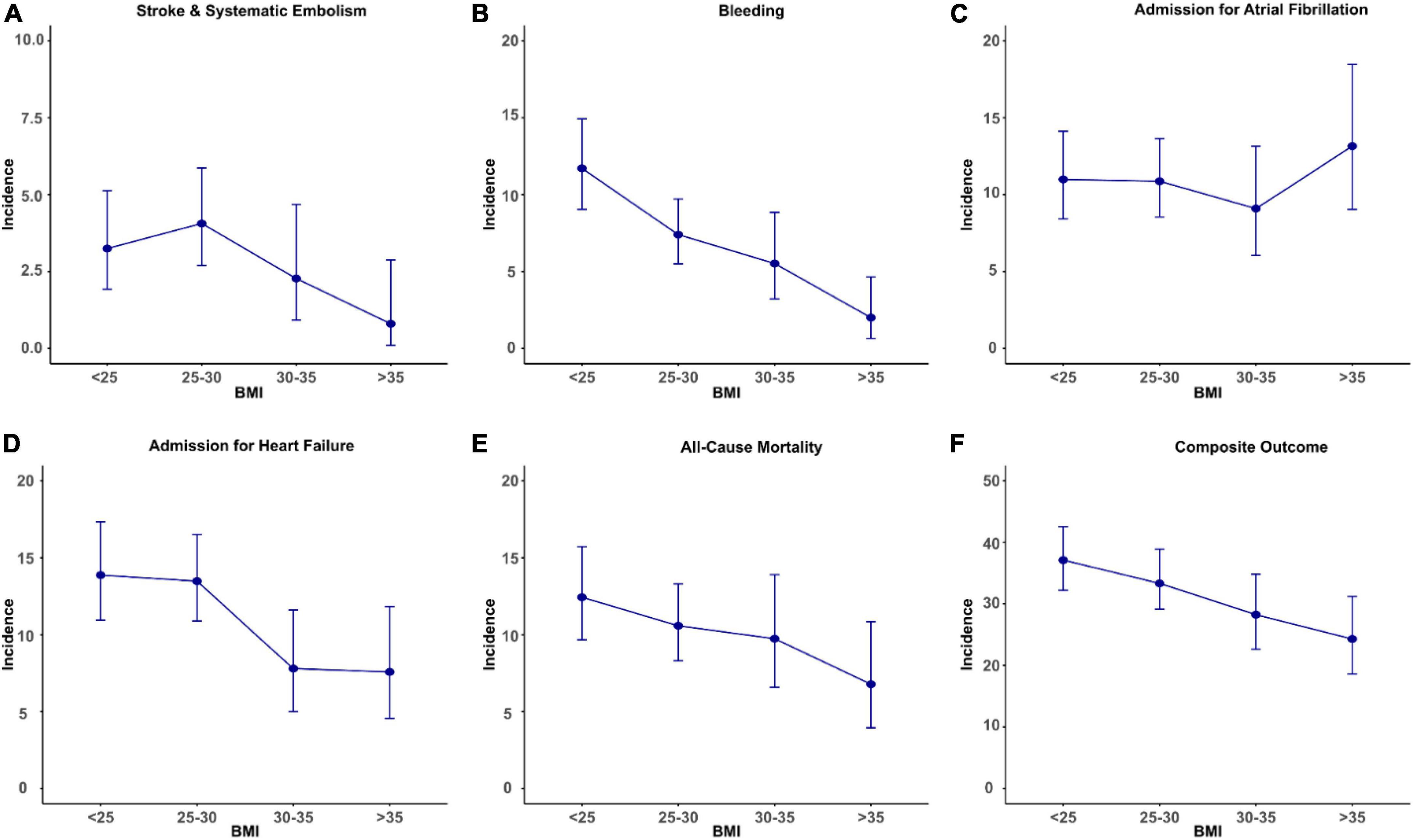
Figure 1. Body mass index and incident rates of clinical outcomes [(A) stroke and systematic embolism; (B) bleeding; (C) admission for atrial fibrillation; (D) admission for heart failure; (E) all-cause mortality; (F) composite outcome] per 100 patient-years. The bar represents confidence interval of incident rate.
When dividing patients into obese and non-obese groups, obese patients were less likely to have stroke/SE [crude odds ratio (OR) = 0.43], bleeding (OR = 0.42), admission for HF (OR = 0.53), all-cause mortality (OR = 0.69), and the composite outcome (OR = 0.69) (P < 0.05, respectively). In the multivariable logistic regression model, after adjusting with other cofounders including medical history, baseline medication, etc., the result was generally the same for stroke/SE [adjusted OR (aOR) = 0.40], bleeding (aOR = 0.44), admission for HF (aOR = 0.61), and the composite outcome (aOR = 0.65) (all P < 0.05) (see Table 3).
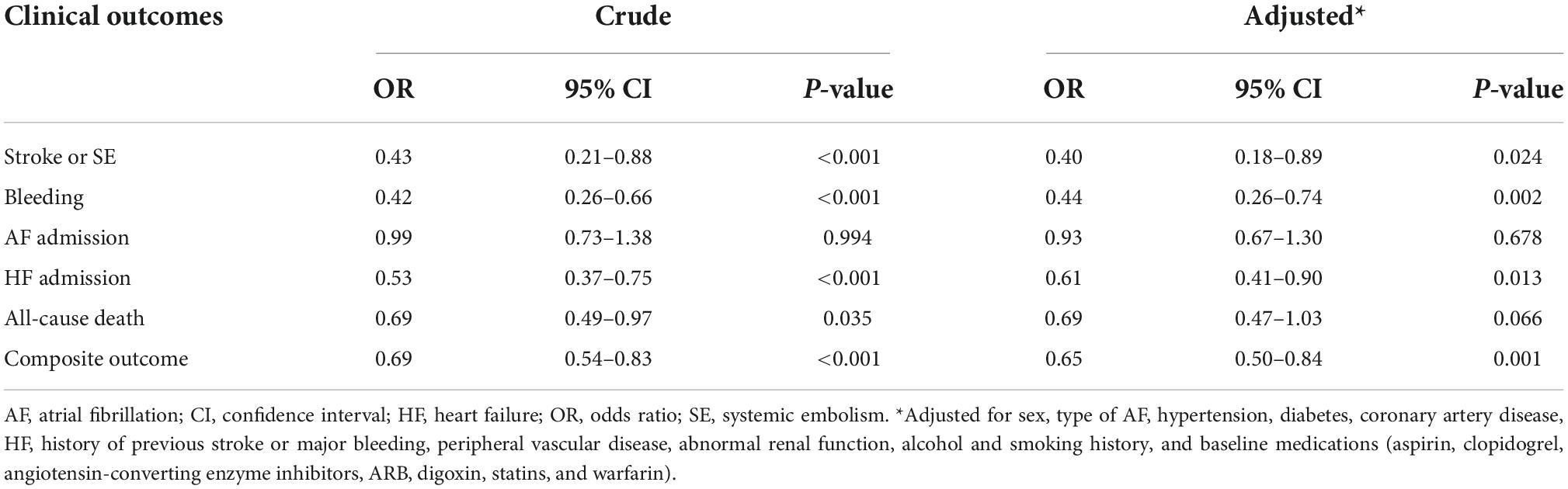
Table 3. Odds ratio of clinical outcomes comparing obese and non-obese patients.
For illustrating the relationship between continuous BMI and AF prognosis, restricted cubic splines were depicted (see Figure 2). The risk of stroke/SE was highest at a BMI of 28 kg/m2, followed by a decreasing trend with a higher BMI. The risk of admission for AF did not show significant changes. While, the risks of bleeding, HF admission, all-cause mortality, and composite outcomes decreased with higher BMI (Figure 2).
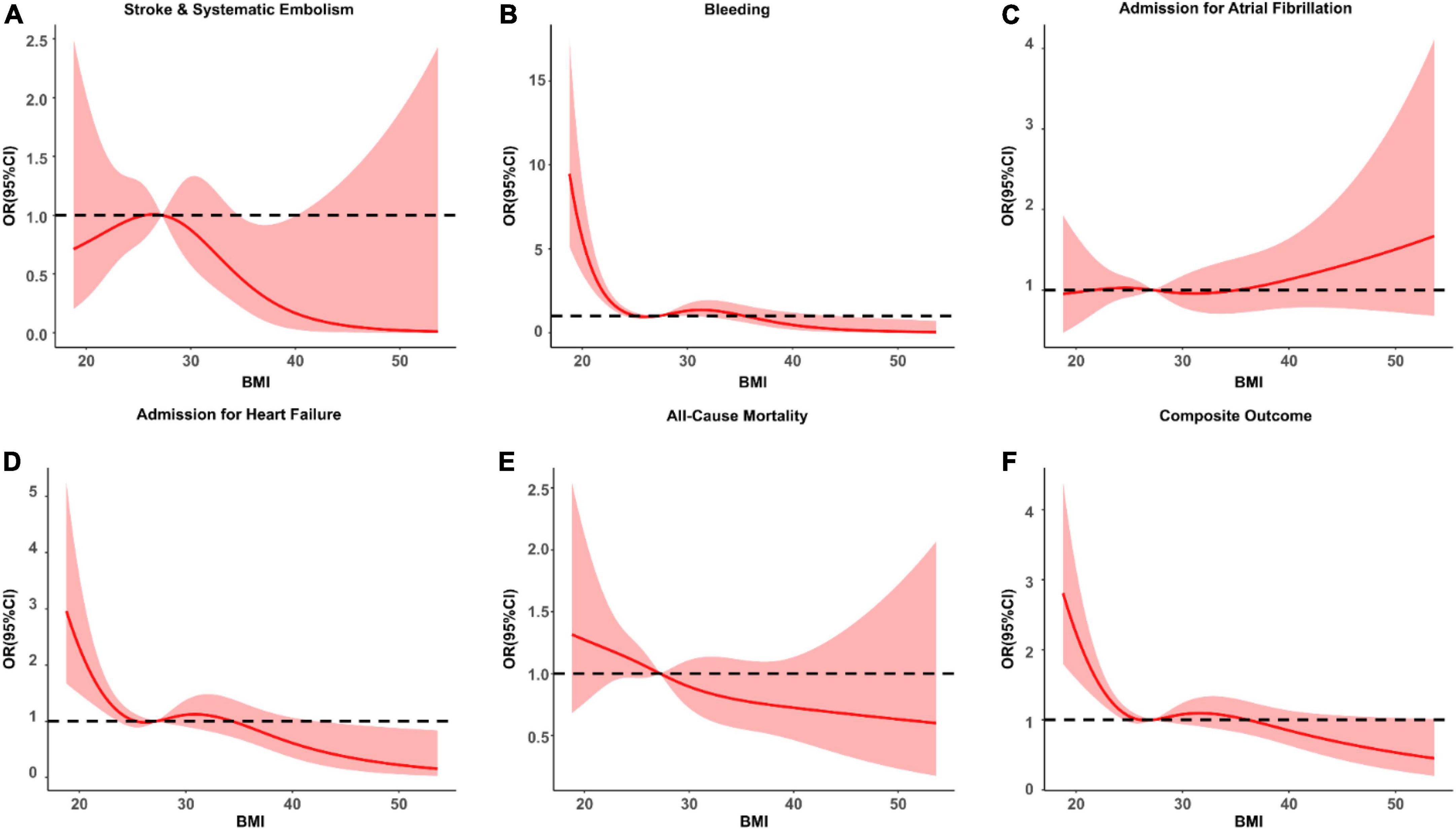
Figure 2. The hazard ratio (95% CI) BMI as a continuous variable for clinical outcomes [(A) stroke and systematic embolism; (B) bleeding; (C) admission for atrial fibrillation; (D) admission for heart failure; (E) all-cause mortality; (F) composite outcome]. The solid red line is the multivariate adjusted odds ratio, and the pink shade represents the 95% confidence interval. Unrelated reference lines are represented by dotted lines.
To show the impact of obesity on outcomes in subgroups of patients, we have conducted a sensitivity analysis and depicted forest plots for comparison. For stroke/SE events, obesity showed a significantly lower OR in patients with hyperlipidemia (OR = 0.20) and diabetes (OR = 0.26). For bleeding events, obese patients had a significantly lower OR in all subgroups except in those aged ≥ 65 years. The risk of AF admission did not show significance. For HF admission, obesity showed lower OR for all subgroups except in males. For obesity, the risk of all-cause mortality was significantly lower in males (OR = 0.54), elderly (OR = 0.62), and non-diabetes (OR = 0.53) compared with the non-obese population. For the risk of composite outcomes, obesity showed significantly lower OR for all subgroups, except those without hyperlipidemia (see Figure 3).
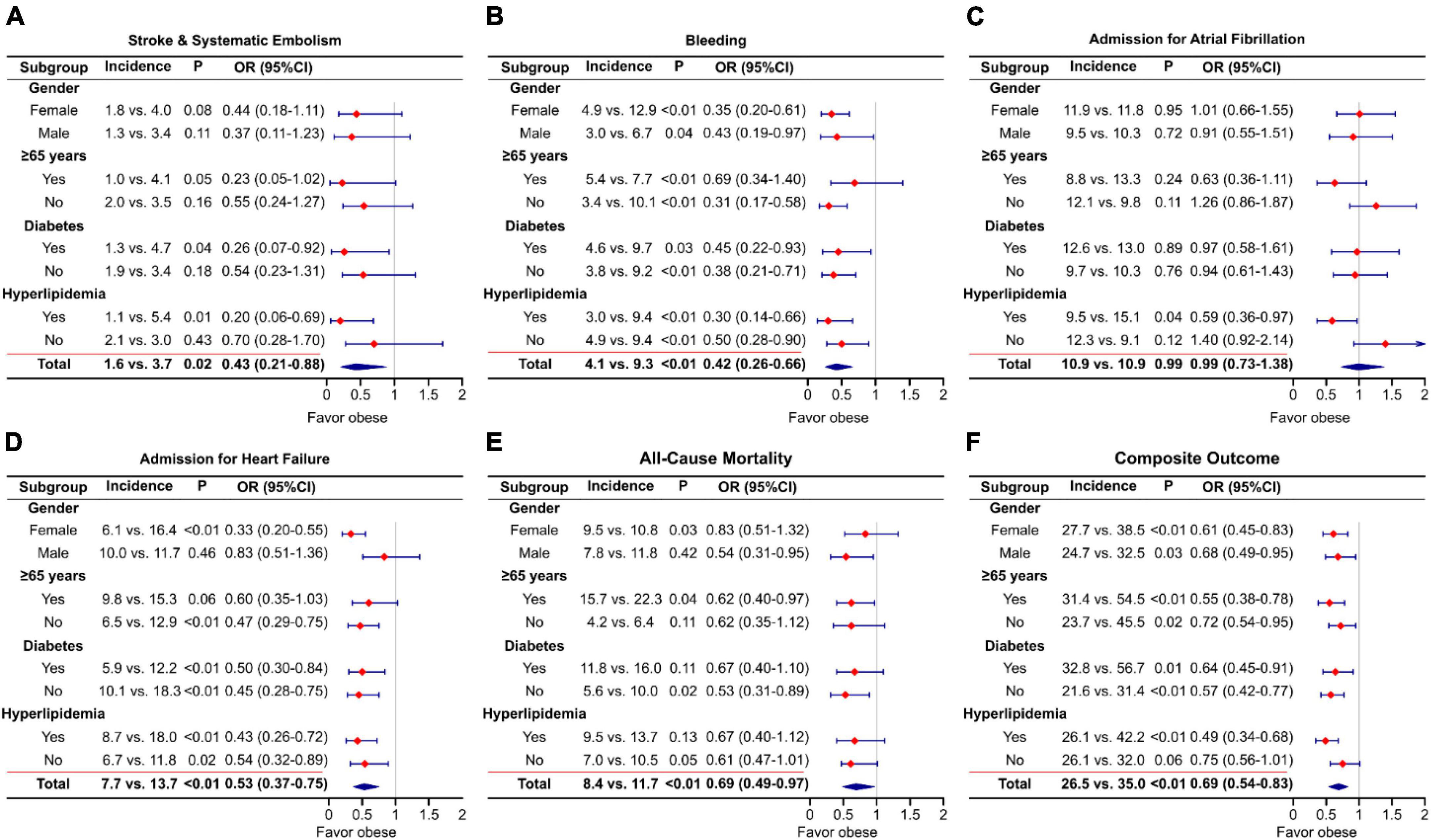
Figure 3. Odds ratio and forest plots of outcomes [(A) stroke and systematic embolism; (B) bleeding; (C) admission for atrial fibrillation; (D) admission for heart failure; (E) all-cause mortality; (F) composite outcome] in subgroups of patients.
This is the first study assessing the impact of obesity on the prognosis of AF patients from the Middle East Gulf region. We found that obesity is prevalent among AF patients, with nearly one-third of all enrolled subjects. Obesity was independently associated with lower risks of stroke/SE, bleeding, HF admission, all-cause mortality, and composite outcomes, consistent with what has been termed the “obesity paradox.” With the increase in BMI, the risks of these multiple outcome events showed a decreasing trend.
The prevalence of obesity is increasing in the general population and those with AF. In a recently published study in Spain which included 14,849 patients with AF, 46% of patients were obese (30). In the EORP-AF (EURObservational Research Programme AF) General Pilot Registry, among the 2,540 AF patients included, 42.7% were overweight and 29.0% were obese (18). This is roughly the same as the proportion in the present study. Obesity is one of the major contributors to the development of AF (3), and weight loss was associated with an improved prognosis for AF patients (17, 31). In the reports from Patti et al. (n = 9,330), obesity was associated with worse outcomes regarding thromboembolic and bleeding risks (32). Despite the well-established causal associations between obesity and AF, some studies have demonstrated controversial results suggesting a favorable effect of higher BMI. For instance, in the ARISTOTLE (Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation) trial, which is a large prospective cohort study including 17,913 AF patients with at least one risk factor for stroke, BMI > 25 kg/m2 and high waist circumference (>102 cm for men, > 88 cm for women) were associated with lower risks of stroke and all-cause mortality (19). In a systematic analysis enrolling 13 randomized trials on AF, Proietti et al. also found evidence for an obesity paradox, whereby both overweight (OR 0.75, 95%CI, 0.66–0.84) and obese (OR 0.62, 95%CI, 0.54–0.70) patients had a lower risk for stroke/SE (21). The risk of major bleeding was lower in obese patients compared with normal-weight individuals (OR, 0.84; 95% CI, 0.72–0.98) (21).
In the present study, with increasing BMI, the risks of stroke/SE, bleeding risk, admission for HF, all-cause mortality, and the composite outcome were reduced; which is contrary to our common belief, and has been termed as “obesity paradox.” When treating BMI as a continuous variable as demonstrated by restricted cubic splines (Figure 2), we found that multiple outcome events showed higher risks when BMI is lower than < 28 kg/m2. More importantly, for the risk of stroke and SE, the highest risk was presented at the level of BMI = 28 kg/m2. Similar pattern was seen for the risk of AF admission. This phenomenon has attracted much attention in recent years (18, 19, 33, 34). In the ENGAGE AF-TIMI 48 study (n = 21,028), higher BMI (per 5 kg/m2 increase) was associated with lower risks of stroke/SE (hazard ratio = 0.88, P = 0.0001) and mortality (hazard ratio = 0.91, P = 0.0001) (33). In the EORP-AF study (n = 2,540), the risk of all-cause mortality in female overweight and obese AF patients was lower than that of normal-weight AF patients (18). Similarly, in a multicenter, longitudinal, observational study with 12 months of follow-up, which included 1,193 patients with AF, higher basal BMI was associated with a lower fatality rate (35). With a higher BMI category, mortality risk decreased by 26.4% (35). This was also seen in a generally well-anticoagulated AF population. In a recent large, multicenter, retrospective study involving 15 centers and 6,164 patients with AF on anticoagulants in China, higher BMI was negatively associated with major bleeding (OR = 0.353), total bleeding (OR = 0.664), and all-cause death (OR = 0.370) (36).
Interestingly, the obesity “paradox” is not only present in AF but also observed in coronary artery disease, HF, hypertension and other non-cardiovascular diseases (37–40). For instance, in the TOPCAT (Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist) trial with 1,749 patients with HF, both overweight (HR, 0.51; 95% CI, 0.27–0.95) and obesity (HR, 0.64; 95% CI, 0.43–0.98) were associated with reduced risk of all-cause death (41).
The phenomenon of high BMI increasing the risk of incident cardiovascular disease initially and reduces the risk of composite outcomes after cardiovascular disease occurred has been called the “obesity paradox”(22). However, it could be problematic to consider obesity as a protecting factor from the perspective of epidemiological standpoints. A reasonable explanation may be that obese patients tend to receive more aggressive treatment and follow-up regimens, which could improve cardiovascular disease prognosis (42). For instance, in the ARISTOTLE trial, the medication usage rates of statin and beta-blockers were 50%, and 68% for obese AF patients, compared to 34% and 56% for non-obesity patients (19). This phenomenon appears to be seen in the present study as well that obese patients received more statin and ARBs compared with non-obese individuals. Importantly, in the present study, obese patients were more treated with warfarin during follow-up time points. By categorizing patients into BMI < 30 kg/m2 and ≥ 30 kg/m2 groups, we found the following warfarin usage rates during follow-up: 48.9% vs. 51.7% (1st month), 42.8% vs. 47.4% (6th month), and 41.6% vs. 44.0% (12th month). This is a proof of the theory that obese patients received more treatment leading to better outcomes. In the present study, we found that obesity population were more prone to visit ER due to AF. Probably this is a reason why this group of patients were associated with more favorable AF-related outcome events. Further, in the Middle East region, relatively higher BMI may suggest better nutrition conditions and more available economical and medical resources, which could be transferred to better treatment selection. In addition, obese patients may receive more cardiorespiratory fitness exercise, which is beneficial in improving AF prognosis (43).
Nonetheless, BMI might not be an optimal index to describe obesity, which did not fully consider body composition, such as central obesity or visceral obesity. At present, some researchers have proposed the definition of metabolically healthy obese (MHO): systolic blood pressure < 130 mmHg and no antihypertensive drugs and waist-to-hip ratio < 0.95 (female)/1.03 (male) and self-reported without type 2 diabetes of obese people. The results showed that the cardiovascular risk of MHO patients was not significantly increased (44). This indicates that if we only use BMI to define obese, the prognosis judgment for some diseases could be misleading. The MHO may represent specialized adipose tissue composition with biologically protective functions (45).
Our study has several limitations. First, the body weight in this study was the data of the patients when they were included in the study, and the patients’ usual exercise and weight change trends were not recorded during the following follow-up period, which may have influenced our results. Second, despite the strict inclusion criteria and follow-up schedule of this study, its conclusions may be influenced by unmeasured and residual confounding factors, such as dietary habits and rest schedule. The Gulf SAFE registry did not provide the severity of AF during the enrollment procedure, which may have impact on AF prognosis. In addition, the anticoagulants used by the patients in this study did not include Non-vitamin K antagonists, and the quality of anticoagulation in the vitamin K antagonist population was not available, which would affect our assessment of AF prognosis, especially the stroke/SE and bleeding risk. Finally, one should not treat this as a distraction toward our endeavor of fighting obesity considering its culprit role in multiple cardiovascular disorders as recommended by guidelines (1). Ultimately, the contemporary management of AF needs a holistic or integrated care approach (46), which is recommended in guidelines (47), given the improved outcomes by adherence to such a strategy (48).
In the Gulf-SAFE registry, obesity is prevalent among AF patients and associated with favorable outcomes. With the increase of BMI, the risks of stroke/SE, bleeding, admission for HF, all-cause mortality, and composite outcomes decreased significantly. The underlying mechanisms merit further investigation.
The data analyzed in this study was obtained from the authorization of PIs from individual center involved in this study. The datasets presented in this article are not readily available because of copyright. Requests to access the datasets should be directed to all PIs in this study.
The study protocols were approved by each National or Institutional Ethics Committee. The patients/participants provided their written informed consent to participate in this study.
Y-GL and P-XX: drafting manuscript. GL and S-WL: designing study and editing manuscript. AA-A, WA, KS, NA, and MZ: participated in processing data and quality control. All authors have read and agreed to the published version of the manuscript.
We thank the patients who volunteered to participate in this study.
Author NA was employed by Hamad Medical Corporation.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomstrom-Lundqvist C, et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the task force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. (2021) 42:373–498. doi: 10.1093/eurheartj/ehaa612
2. Li YG, Bai J, Zhou G, Li J, Wei Y, Sun L, et al. Refining age stratum of the C2hest score for predicting incident atrial fibrillation in a hospital-based Chinese population. Eur J Intern Med. (2021) 90:37–42. doi: 10.1016/j.ejim.2021.04.014
3. Li Y, Pastori D, Guo Y, Wang Y, Lip GYH. Risk factors for new-onset atrial fibrillation: a focus on Asian populations. Int J Cardiol. (2018) 261:92–8. doi: 10.1016/j.ijcard.2018.02.051
4. Fan YY, Li YG, Li J, Cheng WK, Shan ZL, Wang YT, et al. Diagnostic performance of a smart device with photoplethysmography technology for atrial fibrillation detection: pilot study (Pre-Mafa Ii Registry). JMIR Mhealth Uhealth. (2019) 7:e11437. doi: 10.2196/11437
5. Kornej J, Borschel CS, Benjamin EJ, Schnabel RB. Epidemiology of atrial fibrillation in the 21st century: novel methods and new insights. Circ Res. (2020) 127:4–20. doi: 10.1161/CIRCRESAHA.120.316340
6. Lippi G, Sanchis-Gomar F, Cervellin G. Global epidemiology of atrial fibrillation: an increasing epidemic and public health challenge. Int J Stroke. (2021) 16:217–21. doi: 10.1177/1747493019897870
7. Kotalczyk A, Mazurek M, Kalarus Z, Potpara TS, Lip GYH. Stroke prevention strategies in high-risk patients with atrial fibrillation. Nat Rev Cardiol. (2021) 18:276–90. doi: 10.1038/s41569-020-00459-3
8. Al-Khatib SM, Benjamin EJ, Albert CM, Alonso A, Chauhan C, Chen PS, et al. Advancing research on the complex interrelations between atrial fibrillation and heart failure: a report from a US National Heart, Lung, and Blood Institute Virtual Workshop. Circulation. (2020) 141:1915–26. doi: 10.1161/CIRCULATIONAHA.119.045204
9. Madhavan M, Hu TY, Gersh BJ, Roger VL, Killian J, Weston SA, et al. Efficacy of warfarin anticoagulation and incident dementia in a community-based cohort of atrial fibrillation. Mayo Clin Proc. (2018) 93:145–54. doi: 10.1016/j.mayocp.2017.09.021
10. Chen LY, Chung MK, Allen LA, Ezekowitz M, Furie KL, McCabe P, et al. Atrial fibrillation burden: moving beyond atrial fibrillation as a binary entity: a scientific statement from the American Heart Association. Circulation. (2018) 137:e623–44. doi: 10.1161/CIR.0000000000000568
11. Burdett P, Lip GYH. Atrial fibrillation in the UK: predicting costs of an emerging epidemic recognizing and forecasting the cost drivers of atrial fibrillation-related costs. Eur Heart J Qual Care Clin Outcomes. (2022) 8:187–94. doi: 10.1093/ehjqcco/qcaa093
12. Asad Z, Abbas M, Javed I, Korantzopoulos P, Stavrakis S. Obesity is associated with incident atrial fibrillation independent of gender: a meta-analysis. J Cardiovasc Electrophysiol. (2018) 29:725–32. doi: 10.1111/jce.13458
13. Chung MK, Eckhardt LL, Chen LY, Ahmed HM, Gopinathannair R, Joglar JA, et al. Lifestyle and risk factor modification for reduction of atrial fibrillation: a scientific statement from the American Heart Association. Circulation. (2020) 141:e750–72. doi: 10.1161/CIR.0000000000000748
14. Feng T, Vegard M, Strand LB, Laugsand LE, Morkedal B, Aune D, et al. Weight and weight change and risk of atrial fibrillation: the hunt study. Eur Heart J. (2019) 40:2859–66. doi: 10.1093/eurheartj/ehz390
15. Chooi YC, Ding C, Magkos F. The epidemiology of obesity. Metabolism. (2019) 92:6–10. doi: 10.1016/j.metabol.2018.09.005
16. Middeldorp ME, Pathak RK, Meredith M, Mehta AB, Elliott AD, Mahajan R, et al. Prevention and regressive effect of weight-loss and risk factor modification on atrial fibrillation: the Reverse-AF study. Europace. (2018) 20:1929–35. doi: 10.1093/europace/euy117
17. Lavie CJ, Pandey A, Lau DH, Alpert MA, Sanders P. Obesity and atrial fibrillation prevalence, pathogenesis, and prognosis: effects of weight loss and exercise. J Am Coll Cardiol. (2017) 70:2022–35. doi: 10.1016/j.jacc.2017.09.002
18. Boriani G, Laroche C, Diemberger I, Fantecchi E, Meeder J, Kurpesa M, et al. Overweight and obesity in patients with atrial fibrillation: sex differences in 1-year outcomes in the EORP-AF general pilot registry. J Cardiovasc Electrophysiol. (2018) 29:566–72. doi: 10.1111/jce.13428
19. Sandhu RK, Ezekowitz J, Andersson U, Alexander JH, Granger CB, Halvorsen S, et al. The “obesity paradox” in atrial fibrillation: observations from the aristotle (apixaban for reduction in stroke and other thromboembolic events in atrial fibrillation) trial. Eur Heart J. (2016) 37:2869–78. doi: 10.1093/eurheartj/ehw124
20. Liu X, Guo L, Xiao K, Zhu W, Liu M, Wan R, et al. The obesity paradox for outcomes in atrial fibrillation: evidence from an exposure-effect analysis of prospective studies. Obes Rev. (2020) 21:e12970. doi: 10.1111/obr.12970
21. Proietti M, Guiducci E, Cheli P, Lip GY. Is there an obesity paradox for outcomes in atrial fibrillation? a systematic review and meta-analysis of non-vitamin K antagonist oral anticoagulant trials. Stroke. (2017) 48:857–66. doi: 10.1161/STROKEAHA.116.015984
22. Badheka AO, Rathod A, Kizilbash MA, Garg N, Mohamad T, Afonso L, et al. Influence of obesity on outcomes in atrial fibrillation: yet another obesity paradox. Am J Med. (2010) 123:646–51. doi: 10.1016/j.amjmed.2009.11.026
23. Atoofi MK, Qorbani M, Asayesh H, Rezaei N, Moghaddam SS, Djalalinia S. Obesity researches in youth: a scientometrics study in Middle East Countries. J Res Med Sci. (2021) 26:54. doi: 10.4103/jrms.JRMS_415_19
24. Okati-Aliabad H, Ansari-Moghaddam A, Kargar S, Jabbari N. Prevalence of obesity and overweight among adults in the Middle East countries from 2000 to 2020: a systematic review and meta-analysis. J Obes. (2022) 2022:8074837. doi: 10.1155/2022/8074837
25. Fan JG, Kim SU, Wong VW. New trends on obesity and Nafld in Asia. J Hepatol. (2017) 67:862–73. doi: 10.1016/j.jhep.2017.06.003
26. Balakrishnan VS. Europe’s obesity burden on the rise: WHO Report. Lancet Diabetes Endocrinol. (2022) 10:488. (22) 00165-6 doi: 10.1016/S2213-8587
27. Kivimaki M, Kuosma E, Ferrie JE, Luukkonen R, Nyberg ST, Alfredsson L, et al. Overweight, obesity, and risk of cardiometabolic multimorbidity: pooled analysis of individual-level data for 120 813 adults from 16 cohort studies from the USA and Europe. Lancet Public Health. (2017) 2:e277–85. (17) 30074-9 doi: 10.1016/S2468-2667
28. Jiwani SS, Carrillo-Larco RM, Hernandez-Vasquez A, Barrientos-Gutierrez T, Basto-Abreu A, Gutierrez L, et al. The shift of obesity burden by socioeconomic status between 1998 and 2017 in Latin America and the Caribbean: a cross-sectional series study. Lancet Glob Health. (2019) 7:e1644–54. (19)30421-8 doi: 10.1016/S2214-109X
29. Zubaid M, Rashed WA, Alsheikh-Ali AA, Almahmeed W, Shehab A, Sulaiman K, et al. Gulf Survey of atrial fibrillation events (Gulf SAFE): design and baseline characteristics of patients with atrial fibrillation in the Arab Middle East. Circ Cardiovasc Qual Outcomes. (2011) 4:477–82. doi: 10.1161/CIRCOUTCOMES.110.959700
30. Raposeiras-Roubin S, Abu-Assi E, Lizancos Castro A, Barreiro Pardal C, Melendo Viu M, Cespon Fernandez M, et al. Nutrition status, obesity and outcomes in patients with atrial fibrillation. Rev Esp Cardiol. (2022) 75:825–32. doi: 10.1016/j.rec.2022.01.006
31. Boriani G, Proietti M. Atrial fibrillation prevention: an appraisal of current evidence. Heart. (2018) 104:882–7. doi: 10.1136/heartjnl-2017-311546
32. Patti G, Pecen L, Manu MC, Huber K, Rohla M, Renda G, et al. Thromboembolic and bleeding risk in obese patients with atrial fibrillation according to different anticoagulation strategies. Int J Cardiol. (2020) 318:67–73. doi: 10.1016/j.ijcard.2020.06.010
33. Boriani G, Ruff CT, Kuder JF, Shi M, Lanz HJ, Rutman H, et al. Relationship between Body Mass Index and outcomes in patients with atrial fibrillation treated with edoxaban or warfarin in the engage Af-Timi 48 Trial. Eur Heart J. (2019) 40:1541–50. doi: 10.1093/eurheartj/ehy861
34. Balayah Z, Alsheikh-Ali AA, Rashed W, Almahmeed W, Mulla AA, Alrawahi N, et al. Association of obesity indices with in-hospital and 1-year mortality following acute coronary syndrome. Int J Obes. (2021) 45:358–68. doi: 10.1038/s41366-020-00679-0
35. Rodriguez-Reyes H, Lara-Vaca S, Ochoa-Guzman A, Chiquete E, Registro Mexicano de Fibrilacion Auricular Study Group. Obesity paradox and 12 month outcome in patients with atrial fibrillation. Arch Med Res. (2021) 52:233–9. doi: 10.1016/j.arcmed.2020.10.015
36. Wu S, Huang N, Chen X, Jiang S, Zhang W, Hu W, et al. Association between Body Mass Index and clinical outcomes in patients with non-valvular atrial fibrillation receiving direct oral anticoagulants: a new piece of evidence on the obesity paradox from China. Cardiovasc Drugs Ther. (2022) [Epub ahead of print]. doi: 10.1007/s10557-022-07332-0
37. Lavie CJ, De Schutter A, Parto P, Jahangir E, Kokkinos P, Ortega FB, et al. Obesity and prevalence of cardiovascular diseases and prognosis-the obesity paradox updated. Prog Cardiovasc Dis. (2016) 58:537–47. doi: 10.1016/j.pcad.2016.01.008
38. Oktay AA, Lavie CJ, Kokkinos PF, Parto P, Pandey A, Ventura HO. The interaction of cardiorespiratory fitness with obesity and the obesity paradox in cardiovascular disease. Prog Cardiovasc Dis. (2017) 60:30–44. doi: 10.1016/j.pcad.2017.05.005
39. Zhou D, Wang C, Lin Q, Li T. The obesity paradox for survivors of critically ill patients. Crit Care. (2022) 26:198. doi: 10.1186/s13054-022-04074-1
40. Liu Z, Sanossian N, Starkman S, Avila-Rinek G, Eckstein M, Sharma LK, et al. Adiposity and outcome after ischemic stroke: obesity paradox for mortality and obesity parabola for favorable functional outcomes. Stroke. (2021) 52:144–51. doi: 10.1161/STROKEAHA.119.027900
41. Guo L, Liu X, Yu P, Zhu W. The “Obesity Paradox” in patients with hfpef with or without comorbid atrial fibrillation. Front Cardiovasc Med. (2021) 8:743327. doi: 10.3389/fcvm.2021.743327
42. Proietti M, Boriani G. Obesity paradox in atrial fibrillation: implications for outcomes and relationship with oral anticoagulant drugs. Am J Cardiovasc Drugs. (2020) 20:125–37. doi: 10.1007/s40256-019-00374-0
43. Mishima RS, Verdicchio CV, Noubiap JJ, Ariyaratnam JP, Gallagher C, Jones D, et al. Self-Reported physical activity and atrial fibrillation risk: a systematic review and meta-analysis. Heart Rhythm. (2021) 18:520–8. doi: 10.1016/j.hrthm.2020.12.017
44. Zembic A, Eckel N, Stefan N, Baudry J, Schulze MB. An empirically derived definition of metabolically healthy obesity based on risk of cardiovascular and total mortality. JAMA Netw Open. (2021) 4:e218505. doi: 10.1001/jamanetworkopen.2021.8505
45. Antonopoulos AS, Tousoulis D. The molecular mechanisms of obesity paradox. Cardiovasc Res. (2017) 113:1074–86. doi: 10.1093/cvr/cvx106
46. Lip GYH. The ABC pathway: an integrated approach to improve af management. Nat Rev Cardiol. (2017) 14:627–8. doi: 10.1038/nrcardio.2017.153
47. Chao TF, Joung B, Takahashi Y, Lim TW, Choi EK, Chan YH, et al. 2021 focused update consensus guidelines of the asia pacific heart rhythm society on stroke prevention in atrial fibrillation: executive summary. Thromb Haemost. (2022) 122:20–47. doi: 10.1055/s-0041-1739411
48. Romiti GF, Pastori D, Rivera-Caravaca JM, Ding WY, Gue YX, Menichelli D, et al. Adherence to the“Atrial Fibrillation Better Care” pathway in patients with atrial fibrillation: impact on clinical outcomes-a systematic review and meta-analysis of 285,000 patients. Thromb Haemost. (2021) 122:406–14. doi: 10.1055/a-1515-9630
Keywords: atrial fibrillation, obesity, paradox, body mass index, stroke, prognosis
Citation: Li Y-G, Xie P-X, Alsheikh-Ali AA, AlMahmeed W, Sulaiman K, Asaad N, Liu S-W, Zubaid M and Lip GYH (2022) The “obesity paradox” in patients with atrial fibrillation: Insights from the Gulf SAFE registry. Front. Cardiovasc. Med. 9:1032633. doi: 10.3389/fcvm.2022.1032633
Received: 31 August 2022; Accepted: 17 October 2022;
Published: 30 November 2022.
Edited by:
Danilo Menichelli, Sapienza University of Rome, ItalyReviewed by:
Yuliya Lokhnygina, Duke University, United StatesCopyright © 2022 Li, Xie, Alsheikh-Ali, AlMahmeed, Sulaiman, Asaad, Liu, Zubaid and Lip. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shu-Wang Liu, bGl1c2h1d2FuZzIwMThAMTYzLmNvbQ==; Gregory Y. H. Lip, Z3JlZ29yeS5saXBAbGl2ZXJwb29sLmFjLnVr
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.