
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CLINICAL TRIAL article
Front. Cardiovasc. Med. , 20 December 2021
Sec. Cardiovascular Therapeutics
Volume 8 - 2021 | https://doi.org/10.3389/fcvm.2021.803979
 Pierre-Grégoire Guinot1,2*
Pierre-Grégoire Guinot1,2* Maxime Nguyen1,2
Maxime Nguyen1,2 Valerian Duclos1
Valerian Duclos1 Vivien Berthoud1Belaid Bouhemad1,2 and The water study group
Vivien Berthoud1Belaid Bouhemad1,2 and The water study groupAim: Little is known about the cardiovascular effects of oral water intake in shock patients. This study was designed to assess the effect of oral water on stroke volume and blood pressure during a 1-h time period.
Method and Results: This open-label, randomized clinical trial included patients admitted to intensive care with acute circulatory failure. Three ICU units at the anesthesia and critical care department of the Dijon Bourgogne University Hospital. Patients were randomized 1:1 to an intervention or standard care group. The intervention group received 500 ml of oral water while the standard care group received intravenous administration of 500 ml of physiological saline solution. Baseline SV did not differ between the two groups (36 ml [28;51] vs. 38 ml [30;51], p = 0.952). The number of patients who were fluid responders did not differ between the two groups [n = 19 (76%) vs. n = 18 (72%), p = 1]. The median change in stroke volume during the three time points did not differ between the two groups (p < 0.05). In the intervention group, blood pressure increased up to 60 min. In the control group, blood pressure quickly increased at the end of fluid expansion, then returned close to baseline value at 60 min.
Conclusion: Shock patients who were administered oral water experienced improvements in blood pressure and blood flow up to 60 min when compared with patients who received intravenous saline solution. Further studies are warranted to confirm these effects.
Clinical Trial Registration: www.clinicaltrials.gov, identifier: NCT03951519.
Volume expansion remains a daily challenge in critically ill patients (1). There is an abundance of published literature on the cardiovascular and metabolic effects of fluid therapies and their side effects in shock (2, 3). Fluid expansion has well-known cardiovascular effects, including increases in venous return, cardiac preload and cardiac output (CO), resulting in improved tissue perfusion (4). These effects are transient seeing as the increase in CO can be seen for a period of a few minutes (4). When administered repeatedly, these solutes lead to haemodilution, sodium overload, and renal failure (3, 5), which are associated with increased morbidity and mortality (2). Despite this abundant literature, to date there are no ideal fluid solution.
Before the development of the intravenous route, oral rehydration solutions were widely used. Oral rehydration was demonstrated to be associated with positive clinical effects such as an improvement in blood pressure, a lower fluid balance and a shorter hospital stay (6, 7). The absorption and homeostasis of water has been thoroughly studied in sports medicine and physiology (8). While the cardiovascular effect of volume expansion by saline has already been investigated in patients admitted to the intensive care unit (ICU), the cardiovascular effects of oral water is unknown. Only one before/after study have demonstrated an increase of stroke volume (9). Cardiologic studies have demonstrated that in non-shocked patients, oral water can change CO and blood pressure through various physiological effects: increase in blood volume, recruitment of splanchnic blood volume, activation of vasomotor tone, or change in heart rate (9–12). Oral water could be used to modulate orthostatic arterial hypotension. Oral water can modulate plasma volume and the response of the cardiovascular system to a stressful situation (13, 14).
Despite an abundant literature on oral feeding, we do not have data on the cardiovascular effects of oral intake of tap water in shock patients. Water is an easily obtained, natural product that can be administered orally, even in shock patients. Because we do not have data on the cardiovascular effects of oral water in shock patients, we designed a longitudinal randomized study over a 60 min period. This study aimed at describing the cardiovascular effects of oral water in patients with acute circulatory failure.
The study was approved by an Independent Ethics Committee (CPP 3 Nord-ouest CHU de Caen. 2018-A03368-47, NCT03951519). This study is a second part of an investigation aimed at describing the value of oral water in shock patients (9). All patients or their next of kin received written information about the study and gave their written consent to participate. This prospective, open-label, randomized, controlled, parallel-arm, monocentric clinical trial was conducted from May 2019 to February 2020 in three ICU units at the anesthesia and critical care department of the Dijon Bourgogne University Hospital (France).
Inclusion criteria were participants who were aged 18 years or older, suffering from acute circulatory failure (systolic blood pressure < 90 mmHg, and/or mean blood pressure < 65 mmHg, and need for infusion of vasopressor amines, and/or skin mottling, and/or diuresis < 0.5 ml kg−1 h−1 for 2 h ≥, and/or arterial lactate level > 2 mmol/l), with stroke volume change following passive leg raising over 10% (preload dependency), and with no contraindication to a nasogastric tube. The exclusion criteria included permanent atrial fibrillation, hypothermia, concurrent participation in another study, and pregnant women.
The intervention consisted of oral tap water with a low mineral content (Cristaline™; Ca2+: 64 mg/l; Mg2−: 10 mg/l; Na+: 89 mg/l; K+: 3 mg/l; :245 mg/l; :17 mg/l; Cl−: 140 mg/l) at room temperature (22°C). Over a period of 15 min, 500 ml of this water was administered to the patient through the nasogastric tube by using a pump. Standard care consisted of intravenous administration of 500 ml of physiologic saline solution (NaCl 9%) over a period of 15 min.
All patients had been sedated by continuous infusion of propofol and opioid, and were fully adapted to volume-controlled mode with a tidal volume (Vt) set at 7-9 ml/kg of ideal body weight, and a positive end-expiratory pressure (PEEP) of 5-15 cmH2O. Ventilator settings, catecholamines, and sedation were not modified during the study period. The following clinical parameters were recorded: age, gender, weight, sedation, vasoactive agents, ventilation parameters, and main diagnosis. When a subject met the inclusion criteria, measurements of heart rate, blood pressure, respiratory variation of pulse pressure, echocardiography, and arterial/venous blood gas levels were obtained at each step of the study: baseline (time 1), immediately after administration (time 2), 30 min after administration (time 3), 60 min after administration (time 4).
Echocardiography was performed by a physician with echocardiographic certification (15). Tissue perfusion parameters were calculated from arterial/venous blood gas, as previously described (16) (Supplementary Material).
The main outcome was the kinetic of stroke volume change between baseline (time 1) and 60 min after the end of fluid expansion (time 4). The secondary outcomes were the change of mean arterial blood pressure (delta MAP, %), the kinetics of arterial blood pressure, gap CO2, gap CO2/oxygen arteriovenous difference ratio, oxygen delivery (DO2), oxygen consumption (VO2), arterial lactate, hematocrit, sodium, and chloremia over a period of 60 min.
The plasma volume changes were evaluated by using the following formula: 100 * (Hctpre/Hctpost – 1)/(1 – Hctpre) at time 2, time 3, and time 4 (17).
Study participants were randomly assigned to one of two groups using a computer-generated randomization code (CleanWeb® software). The randomization procedure was stratified by stroke volume change following passive leg raising with a 1:1 ratio. Although the research staff who collected data could not be blinded to group assignments, much attention was given to ensuring strict blinding during the data collection and echocardiography data analysis.
Endpoints and adverse events (vomiting, arrythmia, abdominal distention, worsening arterial lactate) were recorded by physicians affiliated with the hospital's clinical research division.
In absence of data, we performed a pilot study. The sample size calculation was based on volume expansion, where 500 ml of saline is usually associated with a mean SV change of 25% (+/−10%) for a mean baseline of 40 ± 10 ml (16). The inclusion of 25 patients can demonstrate a 10% difference in SV variation between the two groups with a power of 80% and a two-tailed p-value of 0.05. The normality of the data distribution was assessed using the Shapiro–Wilk test. Quantitative data were expressed as means ± standard deviation or medians [interquartile range], as appropriate, and qualitative data were expressed as numbers (percentages). Quantitative variables were analyzed by using bi-variate mixed linear modeling. The response variable was modeled depending on the group of randomization and the time of sampling (used as fixed effect) and the individual (used as random, intercept, effect). Normality of the random effect and of residuals distribution was checked graphically. When the fixed effect was significant for between group comparisons, a pairwise testing was carried out with Bonferroni post hoc correction. Statistical analysis was adjusted to baseline amount of fluid before randomization. Qualitative variables were analyzed by using Wilcoxon test or Chi-2 test. All hypothesis tests were two-sided, and the threshold for statistical significance was set at P < 0.05. All analyses were performed using R software (Version 1.1.447).
Fifty patients were included; there were no exclusions. The baseline characteristics were similar between the two groups (Table 1). Patients were admitted to ICU because of septic shock, cardiac arrest, cardiac failure, haemorrhagic shock, and following cardio-vascular surgery (Table 1). At baseline the mean amount of fluid did not differ between the two groups (20 ml Kg−1 [10;34] vs. 25 ml Kg−1 [12;41], p = 0.290). The number of patients with fluid responsiveness (i.e., SV increase of more than 15% between baseline and end of fluid expansion) did not differ between the two groups [n = 19 (76%) vs. n = 18 (72%), p = 1].

Table 1. Baseline characteristics of the study population.
Baseline SV did not differ between the two groups (36 ml [28;51] vs. 38 ml [30;51], p = 0.952). The intervention and standard care groups exhibited significant differences in blood pressure over time (Table 2; Figure 1). In the intervention group, blood pressure, SV and CO increased up to the end of the study (time 4). In the control group, blood pressure, SV, CO quickly increased at the end of fluid expansion (time 2), then returned close to baseline value at 60 min (time 4).
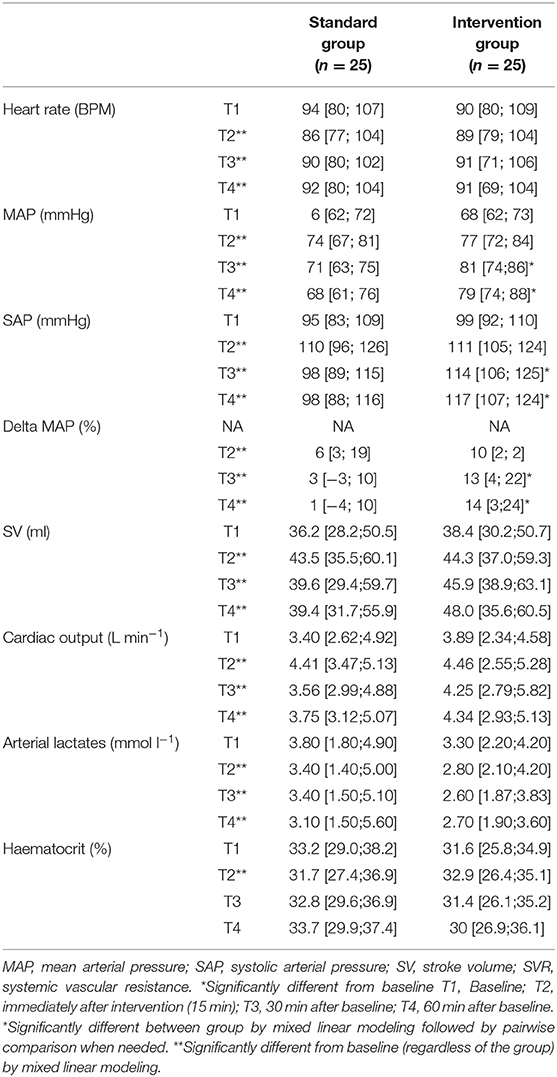
Table 2. Change over time in the haemodynamic and tissue perfusion parameters.
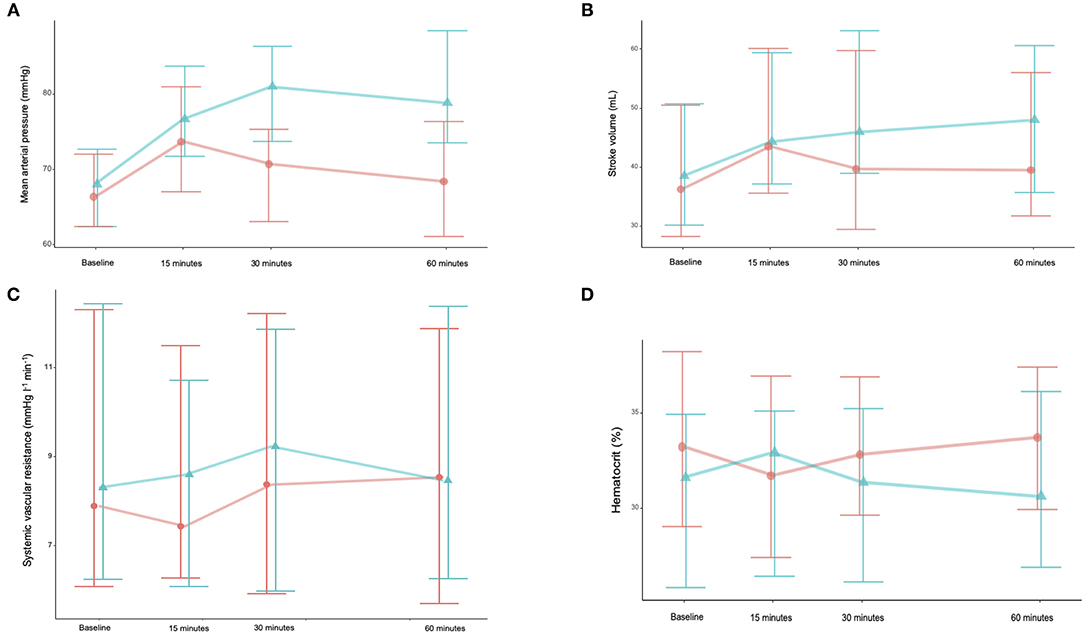
Figure 1. Changes over time in mean arterial pressure (MAP) (A), stroke volume (SV) (B), stroke systemic vascular resistance (SVR) (C), and haematocrit (D). Orange line is saline group, and green line is water group.
The evolution of oxygen delivery and oxygen consumption did not significantly differ between the two groups (Table 2, Supplementary Table 1 and Figure 2). They remained higher until the 60th minute in the intervention group. Arterial lactates decreased over time in both groups. The gapCO2 and gapCO2/DavO2 ratios did not change.
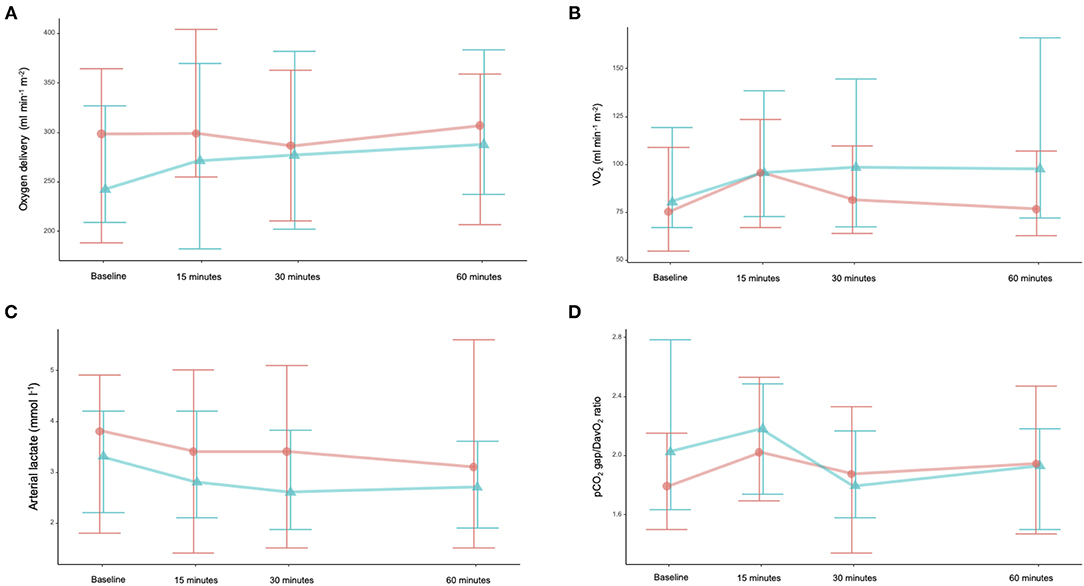
Figure 2. Changes over time in oxygen delivery (DO2) (A), oxygen consumption (VO2) (B), arterial lactate (C), and gapCO2/DavO2 ratio (D). Orange line is saline group, and green line is water group.
Oral water slightly increased hematocrit whereas saline infusion decreased hematocrit; both groups returned to baseline values at 60 min. After fluid administration, plasma volume changes differed between the two groups [8% (2-18%) vs. −2% (−5-4), p = 0.01). Then plasma volume decreased in the control group and increased in the intervention group [−4% (−6-0) vs. 2% (−2-4), p = 0.01].
The incidence of adverse events did not differ between the two groups (Supplementary Table 2). 18 patients (9 vs. 9, p > 0.99) died during their stay in the ICU. Natremia and chloremia did not changed.
The main result of the present study is that oral tap water increases CO and blood pressure up to 60 min. These effects do not differ in term of amplitude, but they are longer with administration of oral water than with the infusion of a saline solution.
These results may be explained by several known physiological mechanisms of oral water. The first and main effect is related to the pressor effect of tap water (10, 12, 18, 19). In the 2000's, Jordan et al. demonstrated that oral water has a pressor effect in patients with autonomic failure (20). Ingestion of water rapidly raises sympathetic activity, and norepinephrine plasma levels, which increases blood pressure (19–21). In the present study, blood pressure increased immediately after oral water administration because of the increase in CO and in systemic vascular resistance. The initial increase of CO may be due to the pressor effect of oral water. Hence, we noted hematocrit kinetics similar to what was previously observed with infusion of vasoactive agents, and plasma volume change was negative (17). Sympathetic activation may be due to several mechanisms such as distention of the abdominal viscera, osmolarity and temperature of the fluids (21–23). We choose to give tap water at room temperature because cold water has been demonstrated to be associated with lower pressor effects (22).
The second mechanism may be in relation to the absorption of water and its effect on plasma volume (24). Water was demonstrated to be quickly absorbed in the proximal part of small intestine. In healthy subjects, tap water is absorbed quickly, with a peak effect at around 15 min (24). On the contrary, we observed a delayed effect in our group of patients, with a peak effect 15-30 min after administration. The delayed gut absorption may be explained by shock-associated gut dysmotility (25). Despite this delay, we observed sustained hemodynamic effects 60 min after oral ingestion. In the same way, hematocrit kinetics inversely followed these of blood pressure.
Since water increases CO and blood pressure, we observed an increase in oxygen delivery. Oral water was associated with an increase in VO2 up to the final time point of the study, and this effect was not observed in the control group. It may be explained by several factors: DO2-VO2 dependency, the effect of oral water on gut oxygen balance, or body thermogenesis following water ingestion (26). It was previously demonstrated that feeding ICU burn patients is associated with a rise in gapCO2 that can be diminished by decreasing the amount of enteral nutrition (27). Oral water is able to increase thermogenesis through b-adrenergic stimulation, as observed with intravenous infusion of epinephrine (26). Increasing gut oxygen consumption could be a limitation of the hemodynamic effects of oral water.
The present results demonstrated the effectiveness of oral water to improve blood flow and tissue perfusion. But these effects differ in term of duration from those observed with saline infusion. To date there are countless literature on fluid therapy, with a focus on renal effect and acid-base disturbance. No ideal fluid solution has been demonstrated. Interesting most of the literature has focused on fluid during shock resuscitation but maintenance fluid therapy and creep fluid may account for 30% of fluid balance (28). Oral water may not replace iv fluid but it's long-acting cardiovascular effects may be of interest during optimization and weaning process of shock patients supported by vasopressor and fluid (29). In addition, using oral tap water may be of interest in term of fluid balance because plasma volume effect and body elimination can be modulated by adding glucose or combining different type of water (tap, saline, sugar). According to Zdolsek et al. this approach can be associated with an increase of plasma volume up to 400 min with a limited volume (24).
Oral water may be harmful in specific subgroup such as acute heart failure, hemorrhage, or digestive ischemia. Few of the included patients were suffering of acute heart failure. Because the main underlying mechanism is the mobilization of the unstressed volume though pressor effect, giving oral water in hemorrhage shock may not be associated with fast hemodynamic effects. On contrary it could be associated with opposite effects (20, 30). Heart failure patients are very sensitive to preload and afterload status. Giving oral water during acute heart failure may be of caution because it can precipitate heart failure by increasing preload and afterload. Further studies evaluating different type of oral solute and their place in fluid therapy in ICU must be performed. These studies must focus on the type of oral solution (tap, saline, mixed…) and the group of ICU patients (sepsis, heart failure, hemorrhagic shock…).
We did not perform a double-blind study. This study must be considered as a preliminary study that provides data on cardiovascular effects of oral water. We assessed hemodynamic changes by using echocardiography and not cardiac output device. Echocardiography has already used in several studies to evaluate the hemodynamic effect of intravenous solutions with good accuracy (31, 32). We measured blood gas parameters from a central venous catheter and not from a pulmonary artery catheter. Since we performed repeated measurements of blood gas levels, mathematical coupling cannot be ruled out. But VO2 calculated from hemodynamic data is a valid alternative to VO2 derived from respiratory gas measurements.
In conclusion, the administration of oral tap water is associated with a sustained improvement in blood pressure when compared with patients who received intravenous saline solution. These results may be mainly explained by the vasopressor effects of oral water. Further studies are warranted to confirm these effects.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Comité de Protection des Personnes Nord-ouest 3, Centre hospitalier universitaire de Caen. The patients/participants provided their written informed consent to participate in this study.
Mohamed Radhouani, Tiberiu Constandache, Sandrine Grosjean, Pierre-Alain Bar, Pierre Voizeux, Emel Rafrafi, Audrey Martin.
P-GG, MN, and VB contributed to the conception and design. P-GG and MN searched the associated data and drafted the manuscript. BB provided the supervision support. MN performed data analysis. All authors contributed to the critical revisions and final approval of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Thank you to Suzanne Rankin for proofreading and reviewing the English.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2021.803979/full#supplementary-material
1. Perner A, Hjortrup PB, Arabi Y. Focus on fluid therapy in critically ill patients. Intensive Care Med. (2019) 45:1469–71. doi: 10.1007/s00134-019-05703-0
2. Frazee E, Kashani K. Fluid management for critically ill patients: a review of the current state of fluid therapy in the intensive care unit. Kidney Dis Basel Switz. (2016) 2:64–71. doi: 10.1159/000446265
3. Martin C, Cortegiani A, Gregoretti C, Martin-Loeches I, Ichai C, Leone M, et al. Choice of fluids in critically ill patients. BMC Anesthesiol. (2018) 18:200. doi: 10.1186/s12871-018-0669-3
4. Bennett VA, Vidouris A, Cecconi M. Effects of fluids on the macro- and microcirculations. Crit Care. (2018) 22:74. doi: 10.1186/s13054-018-1993-1
5. Hahn RG. Adverse effects of crystalloid and colloid fluids. Anaesthesiol Intensive Ther. (2017) 49:303–8. doi: 10.5603/AIT.a2017.0045
6. Harris E, Pérez L, Phares CR, Pérez M de los A, Idiaquez W, Rocha J, et al. Fluid intake and decreased risk for hospitalization for dengue fever, Nicaragua. Emerg Infect Dis. (2003) 9:1003–6. doi: 10.3201/eid0908.020456
7. Moghazy AM, Adly OA, Elbadawy MA, Hashem RE. Evaluation of who oral rehydration solution (ORS) and salt tablets in resuscitating adult patients with burns covering more than 15% of total body surface area (TBSA). Ann Burns Fire Disasters. (2016) 29:43–7.
8. Leiper JB. Intestinal water absorption–implications for the formulation of rehydration solutions. Int J Sports Med. (1998) 19(Suppl 2):S129-32. doi: 10.1055/s-2007-971977
9. Guinot P-G, Nguyen M, Duclos V, Soudry-Faure A, Bouhemad B, Water Study Group. Oral water ingestion in the treatment of shock patients: a prospective randomized study. Intensive Care Med. (2020) 46:2111–2. doi: 10.1007/s00134-020-06215-y
10. Cariga P, Mathias CJ. Haemodynamics of the pressor effect of oral water in human sympathetic denervation due to autonomic failure. Clin Sci. (2001) 101:313–9. doi: 10.1042/CS20000253
11. Mendonca GV, Teixeira MS, Pereira FD, Fernhall B. Cardiovascular and autonomic effects of water ingestion during postexercise circulatory occlusion. Appl Physiol Nutr Metab Physiol Appl Nutr Metab. (2012) 37:1153–63. doi: 10.1139/h2012-106
12. Young T, Mathias C. The effects of water ingestion on orthostatic hypotension in two groups of chronic autonomic failure: multiple system atrophy and pure autonomic failure. J Neurol Neurosurg Psychiatry. (2004) 75:1737–41. doi: 10.1136/jnnp.2004.038471
13. Fox CL. Oral sodium lactate in the treatment of burn shock. J Am Med Assoc. (1944) 124:207–12. doi: 10.1001/jama.1944.02850040007002
14. Schroeder C, Bush VE, Norcliffe LJ, Luft FC, Tank J, Jordan J, et al. Water drinking acutely improves orthostatic tolerance in healthy subjects. Circulation. (2002) 106:2806–11. doi: 10.1161/01.CIR.0000038921.64575.D0
15. Guinot P-G, Longrois D, Kamel S, Lorne E, Dupont H. Ventriculo-arterial coupling analysis predicts the hemodynamic response to norepinephrine in hypotensive postoperative patients: a prospective observational study. Crit Care Med. (2018) 46:e17–25. doi: 10.1097/CCM.0000000000002772
16. Guinot P-G, Guilbart M, Hchikat AH, Trujillo M, Huette P, Bar S, et al. Association between end-tidal carbon dioxide pressure and cardiac output during fluid expansion in operative patients depend on the change of oxygen extraction. Medicine. (2016) 95:e3287. doi: 10.1097/MD.0000000000003287
17. Nygren A, Redfors B, Thorén A, Ricksten S-E. Norepinephrine causes a pressure-dependent plasma volume decrease in clinical vasodilatory shock. Acta Anaesthesiol Scand. (2010) 54:814–20. doi: 10.1111/j.1399-6576.2010.02244.x
18. Callegaro CC, Moraes RS, Negrão CE, Trombetta IC, Rondon MU, Teixeira MS, et al. Acute water ingestion increases arterial blood pressure in hypertensive and normotensive subjects. J Hum Hypertens. (2007) 21:564–70. doi: 10.1038/sj.jhh.1002188
19. Routledge HC, Chowdhary S, Coote JH, Townend JN. Cardiac vagal response to water ingestion in normal human subjects. Clin Sci. (2002) 103:157–62. doi: 10.1042/CS20010317
20. Jordan J, Shannon JR, Black BK, Ali Y, Farley M, Costa F, et al. The pressor response to water drinking in humans : a sympathetic reflex? Circulation. (2000) 101:504–9. doi: 10.1161/01.CIR.101.5.504
21. Scott EM, Greenwood JP, Gilbey SG, Stoker JB, Mary DA. Water ingestion increases sympathetic vasoconstrictor discharge in normal human subjects. Clin Sci. (2001) 100:335–42. doi: 10.1042/CS20000177
22. Arjunwadekar P, Siddanagoudra SP. Cardioautonomic responses to acute ingestion of ice water and its correlation to body mass index. J Basic Clin Physiol Pharmacol. (2018) 30:259–64. doi: 10.1515/jbcpp-2018-0057
23. Brown CM, Barberini L, Dulloo AG, Montani J-P. Cardiovascular responses to water drinking: does osmolality play a role? Am J Physiol Regul Integr Comp Physiol. (2005) 289:R1687-92. doi: 10.1152/ajpregu.00205.2005
24. Zdolsek J, Metander A, Hahn R. Volume kinetic evaluation of fluid turnover after oral intake of tap water, lemonade and saline in volunteers. BMC Sports Sci Med Rehabil. (2016) 8:22. doi: 10.1186/s13102-016-0045-x
25. Plummer MP, Reintam Blaser A, Deane AM. Gut dysmotility in the ICU: diagnosis and therapeutic options. Curr Opin Crit Care. (2019) 25:138–44. doi: 10.1097/MCC.0000000000000581
26. Boschmann M, Steiniger J, Hille U, Tank J, Adams F, Sharma AM, et al. Water-induced thermogenesis. J Clin Endocrinol Metab. (2003) 88:6015–9. doi: 10.1210/jc.2003-030780
27. Kearney MT, Cowley AJ, Macdonald IA. The cardiovascular responses to feeding in man. Exp Physiol. (1995) 80:683–700. doi: 10.1113/expphysiol.1995.sp003878
28. Van Regenmortel N, Verbrugghe W, Roelant E, Van den Wyngaert T, Jorens PG. Maintenance fluid therapy and fluid creep impose more significant fluid, sodium, and chloride burdens than resuscitation fluids in critically ill patients: a retrospective study in a tertiary mixed ICU population. Intensive Care Med. (2018) 44:409–17. doi: 10.1007/s00134-018-5147-3
29. Guinot P-G, Martin A, Berthoud V, Voizeux P, Bartamian L, Santangelo E, et al. Vasopressor-sparing strategies in patients with shock: a scoping-review and an evidence-based strategy proposition. J Clin Med. (2021) 10:3164. doi: 10.3390/jcm10143164
30. Martini J, Carpentier B, Negrete AC, Frangos JA, Intaglietta M. Paradoxical hypotension following increased hematocrit and blood viscosity. Am J Physiol Heart Circ Physiol. (2005) 289:H2136-43. doi: 10.1152/ajpheart.00490.2005
31. Zhang Y, Wang Y, Shi J, Hua Z, Xu J. Cardiac output measurements via echocardiography versus thermodilution: a systematic review and meta-analysis. PLoS ONE. (2019) 14:e0222105. doi: 10.1371/journal.pone.0222105
Keywords: oral water, shock, sepsis, cardiac failure, plasma volume, fluid therapies, acute circulatory failure, vasopressor
Citation: Guinot P-G, Nguyen M, Duclos V, Berthoud V, Bouhemad B and The water study group (2021) Oral Water Has Cardiovascular Effects Up to 60 min in Shock Patients. Front. Cardiovasc. Med. 8:803979. doi: 10.3389/fcvm.2021.803979
Received: 28 October 2021; Accepted: 29 November 2021;
Published: 20 December 2021.
Edited by:
Michael Lichtenauer, Paracelsus Medical University, AustriaReviewed by:
Bernhard Wernly, Paracelsus Medical University, AustriaCopyright © 2021 Guinot, Nguyen, Duclos, Berthoud, Bouhemad and The water study group. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pierre-Grégoire Guinot, Z3Vpbm90cGllcnJlZ3JlZ29pcmVAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.