
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 18 January 2022
Sec. Cardiovascular Epidemiology and Prevention
Volume 8 - 2021 | https://doi.org/10.3389/fcvm.2021.800458
This article is part of the Research Topic Insights in Cardiovascular Epidemiology and Prevention: 2021 View all 21 articles
 Sheng Hu1†
Sheng Hu1† Tian Lan2†
Tian Lan2† Silin Wang1
Silin Wang1 Lang Su1Sheng Zou1
Lang Su1Sheng Zou1 Jiayue Ye1Yang Zhang1Deyuan Zhang1
Jiayue Ye1Yang Zhang1Deyuan Zhang1 Qiang Guo1
Qiang Guo1 Wenxiong Zhang1Dongliang Yu1Jianjun Xu1Yiping Wei1*Jinhua Peng1*
Wenxiong Zhang1Dongliang Yu1Jianjun Xu1Yiping Wei1*Jinhua Peng1*Background: Abdominal aortic calcification is a potentially important independent risk factor for cardiovascular health. The aim of this study was to determine the relationship between serum chloride level and abdominal artery calcification.
Methods: We obtained the data of 3,018 individuals from the National Health and Nutrition Examination Survey database and analyzed the relationship between serum chloride and abdominal artery calcification. We performed stratified and single factor analysis, multiple equation regression analysis, smooth curve fitting, and threshold effect and saturation effect analysis. R and EmpowerStats were used for data analysis.
Results: Serum chloride is independently related to the AAC total 24 score (AAC-24). The smooth curves fitted were all inverted-U shaped. Below a cutoff value of 92 mmol/L, increase in serum chloride level was associated with increase in AAC-24; however, above that cutoff, increase in serum chloride level was associated with decrease in AAC-24.
Conclusions: At serum levels below 92 mmol/L, chloride is a risk factor for abdominal aortic calcification but levels above 92 mmol/L appear to protect against abdominal aortic calcification.
Aortic calcification is a risk marker for cardiovascular diseases such as coronary artery disease and stroke (1–4). Factors known to be strongly associated with abdominal aortic calcification (AAC) include old age, chronic kidney disease, sex, diabetes mellitus (5), and osteoporosis (6, 7). Several other factors are also probably involved; their identification is essential for effective prevention of AAC.
Serum chloride level has complex effects in humans. It is associated with several diseases, including hypertension (8), heart failure (9), acute pancreatitis (10), acute kidney injury (10), chronic kidney disease (11), pulmonary arterial hypertension (11), cardiorenal syndrome (12), and neuromyelitis optica (13). Changes in serum chloride level—especially increase in serum level—during hospitalization has been shown to be associated with increased in-hospital mortality in patients with chronic kidney disease and pulmonary arterial hypertension (11, 14). In addition, there are studies showing that lanthanum chloride influences bovine vascular smooth muscle cell calcification bi-directionally (15) and that magnesium chloride can block tissue valve calcification (16). However, the relationship between serum chloride and AAC in humans has not been well-studied. We speculate that serum chloride could be one such factor.
The aim of this study was to evaluate the relationship between serum chloride and abdominal aortic calcification using a representative sample of elderly individuals from the National Health and Nutrition Examination Survey (NHANES) (17).
The study population was selected from the database of the NHANES—a population-based cross-sectional survey designed to collect information about the health and nutrition of the population of the US. The project surveys a nationally representative sample each year. These populations are located in counties across the country. NHANES interviews collect demographic, socioeconomic, dietary, and health-related information. Physical examinations conducted during the survey include physiological measurements and laboratory examinations (18).
In this study, we retrospectively analyzed the data recorded for the period 2013–2014, which represents one cycle of the NHANES. From among the 10,175 individuals registered in the NHANES database during this period, we eliminated 7,035 because of missing data on AAC Total 24 score (AAC-24) and another 122 because of missing data on serum chloride level. The data of the remaining 3,018 individuals were included in this analysis. Figure 1 is a flowchart for screening participants.
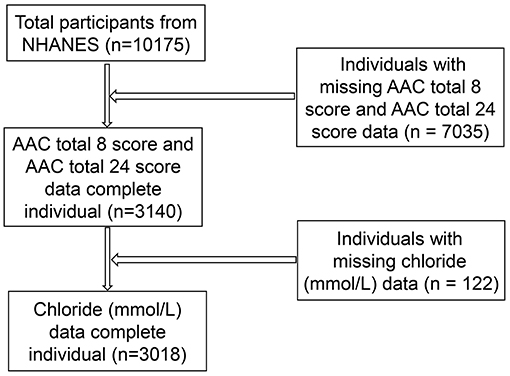
Figure 1. Flowchart of screening participants.
This study was approved by the Ethics Review Board of the National Center for Health Statistics. Informed consent was not considered necessary as this was an analysis of a database.
The exposure variable for this study was serum chloride level (mmol/L). Blood specimens were processed and stored in the mobile examination center laboratory, and shipped to the Johns Hopkins University Lipoprotein Analytical Laboratory for analysis. The outcome variable was AAC-24, which was used to describe the amount of calcification. Several studies have shown that lateral spine images obtained with dual-energy X-ray absorptiometry (DXA) for vertebral fracture assessment can detect AAC with reasonably good sensitivity and specificity. The image resolution of lateral spine scans obtained with DXA is close that of a standard radiograph, and radiation exposure is much lower (19, 20). For scoring AAC-24, the anterior and posterior aortic walls were each divided into four segments, corresponding to the areas in front of lumbar vertebrae L1–L4. Within each of the eight segments, aortic calcification was recognized visually as either a diffused white stippling of the anterior and/or posterior aortic walls, or as white linear calcification of the anterior and/or posterior walls. Aortic calcification was scored as “0” if there was no calcification in that segment; “1” if one-third or less of the aortic wall in that segment was calcified; “2” if more than one-third but <two-thirds was calcified; or “3” if more than two-thirds was calcified. The scores were obtained separately for the anterior and posterior aortic wall; thus, the score at each vertebral level ranged from “0” to “6,” and the total score from “0” to “24” (20, 21), see Supplementary Table S1 for details of AAC-24 calculations.
The categorical variables included as covariates in our analysis were sex, race/ethnicity, and education level. The continuous covariates included in our analysis were age, body mass index (BMI), systolic blood pressure, diastolic blood pressure, total serum calcium (mmol/L), serum cholesterol (mmol/L), serum albumin (g/L), serum glucose, and refrigerated serum glucose (mmol/L). All data on serum chloride, AAC-24 score, and the covariates are available at http://www.cdc.gov/nchs/nhanes/.
We performed weighted and variance estimation analyses to account for significant variance in our data set. Weighted multiple logistic regression models were used to assess the association between serum chloride and AAC-24. Weighted chi-square test was used to analyze differences in categorical variables between groups, and a weighted linear regression model was used to analyze differences in continuous variables. Stratified multiple regression was used for subgroup analysis. In addition, smooth curve fitting and generalized additive models were used to address the non-linear relationship between serum chloride and AAC-24. A recursive algorithm was used to calculate the inflection point in the relationship between serum chloride and AAC-24 when non-linearity was detected, with a bi-segmented linear regression model on either side of the inflection point. Data analysis was performed using R 3.6.3 (http://www.r-project.org) and EmpowerStats (www.empowerstats.net, X&Y Solutions Inc., Boston, MA, USA). P < 0.05 was considered statistically significant.
Serum chloride was divided into three tertile groups: low: ≥87 mmol/L to 103 mmol/L; medium: ≥103 mmol/L to <105 mmol/L; and high: ≥105 mmol/L to <119 mmol/L. As Table 1 shows, there were significant differences in baseline characteristics between the three tertile groups. Mean age, systolic blood pressure, serum cholesterol, serum albumin, serum calcium, and serum glucose were all significantly higher in the low tertile group than in the other tertile groups. AAC-24 was lowest in the medium tertile group. Mean BMI was highest in the high tertile group. Race/ethnicity, sex, and diastolic blood pressure were not significantly different between the three tertile groups.
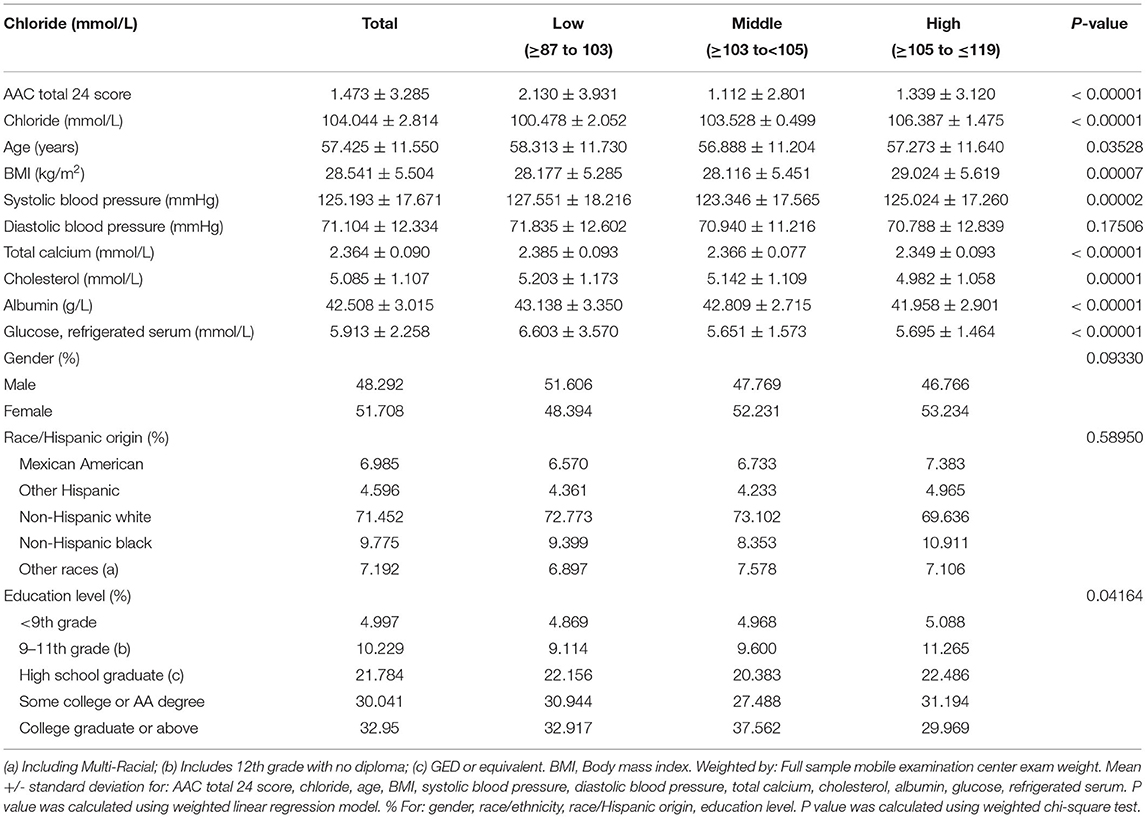
Table 1. Baseline characteristics of participants (N = 3,018).
Table 2 shows the results of univariate analysis. Beta value >0 indicates that the factor is a risk factor for AAC, and beta value <0 indicates that the factor is a protective factor. Compared with the low tertile group of serum chlorine levels, the β value (CI) of the serum chlorine level middle tertile group is −1.017 (−1.333, −0.702), and the β value of the serum chlorine level high tertile group is −0.791 (−1.079, −0.502). P values are <0.001. The beta value, P value, 95% confidence interval and P for trend value of different covariates are shown in Table 2 (gender, age, race/Hispanic origin, education level recoded, BMI, systolic blood pressure, diastolic blood pressure, total calcium, cholesterol, albumin, glucose, refrigerated serum).

Table 2. Univariate analysis for AAC total 24 score.
Table 3 shows the results of stratified analysis between serum chloride and AAC-24. The medium and high serum chloride groups were all negative by using the low serum chloride group as a reference. The absolute value of beta for female in the middle and high serum chloride groups were higher than those for male. The absolute value of beta was highest in the other Hispanic group, followed by the non-Hispanic White group and the Mexican-American group. In the stratification of different education levels, the absolute value of beta was highest in the <9th grade group. In the age stratification, the 64–80-year age-group had the highest absolute value of beta, which was significantly higher than the other age-groups. The absolute value of beta was maximum in the 0–64 mmHg diastolic blood pressure group. The absolute value of beta was maximum in the 1.9–2.3 mmol/L total calcium group. The absolute value of beta was maximum in the 4.577–5.456 mmol/L total cholesterol group. The absolute value of beta was maximum in the 24–40 g/L serum albumin group. The absolute value of beta was maximum in the 5.11–5.77 mmol/L refrigerated serum glucose group.
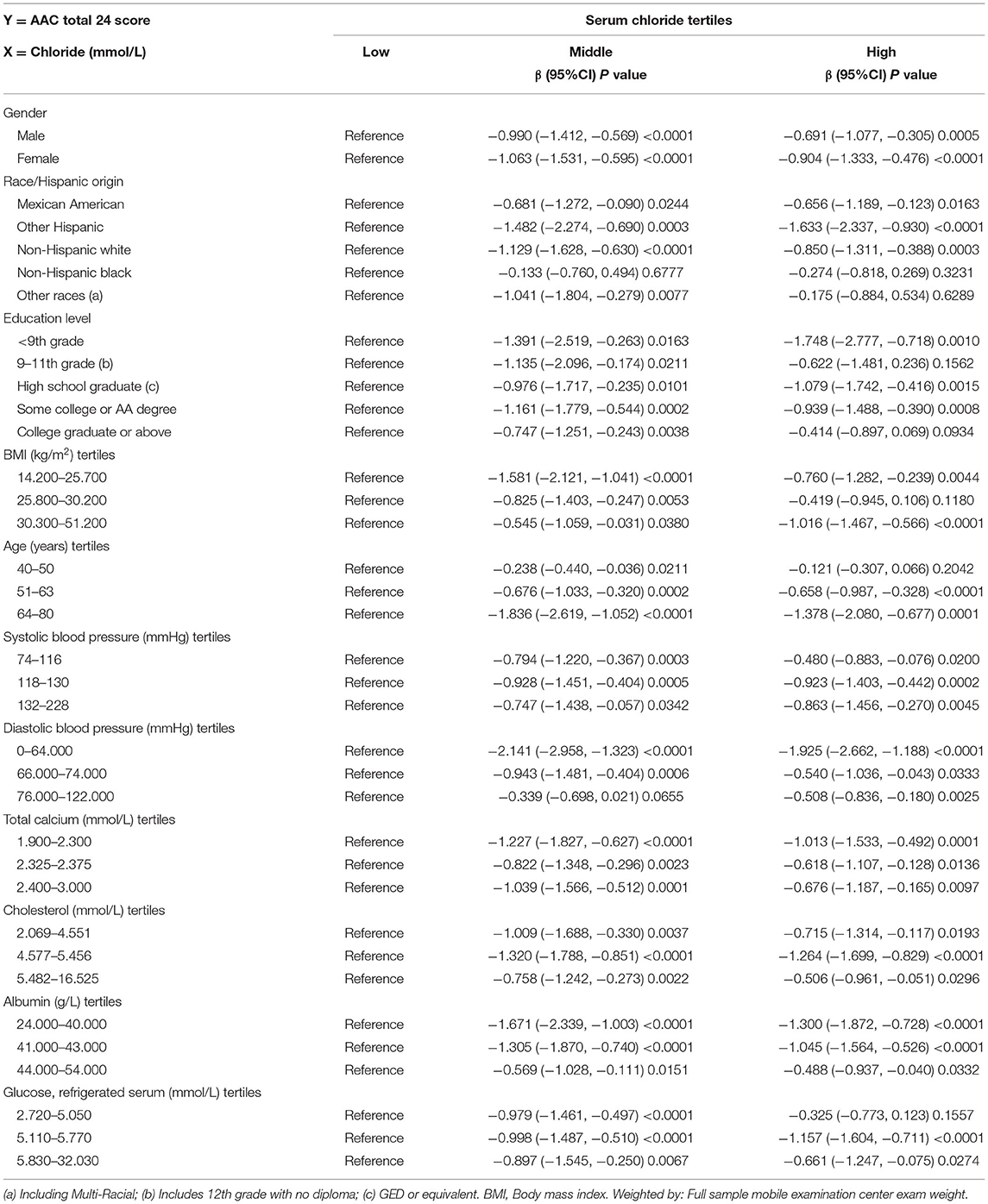
Table 3. Stratified analysis between Chloride (mmol/L) and AAC total 24 score.
Table 4 shows the results of the multiple regression equation analysis. The outcome variable was AAC-24, and the exposure variable was serum chloride. Weighted by: Full sample mobile examination center examination. The crude model was unadjusted; model I adjusted for age, sex, and race/Hispanic origin; model II adjusted for age, sex, race/Hispanic origin, education level, BMI, systolic blood pressure, diastolic blood pressure, total calcium, cholesterol, albumin, and refrigerated serum glucose; and model III adjusted for age (smooth), sex, race/Hispanic origin, education level, BMI (smooth), systolic blood pressure (smooth), diastolic blood pressure (smooth), total calcium (smooth), cholesterol (smooth), albumin (smooth), and refrigerated serum glucose (smooth). The beta value for model III was −0.110. We stratified by chloride tertiles and, additionally, by the following covariates: sex, age, race/Hispanic origin, education level, BMI, systolic blood pressure, diastolic blood pressure, total calcium, cholesterol, albumin, and adjusted serum glucose (Table 4).
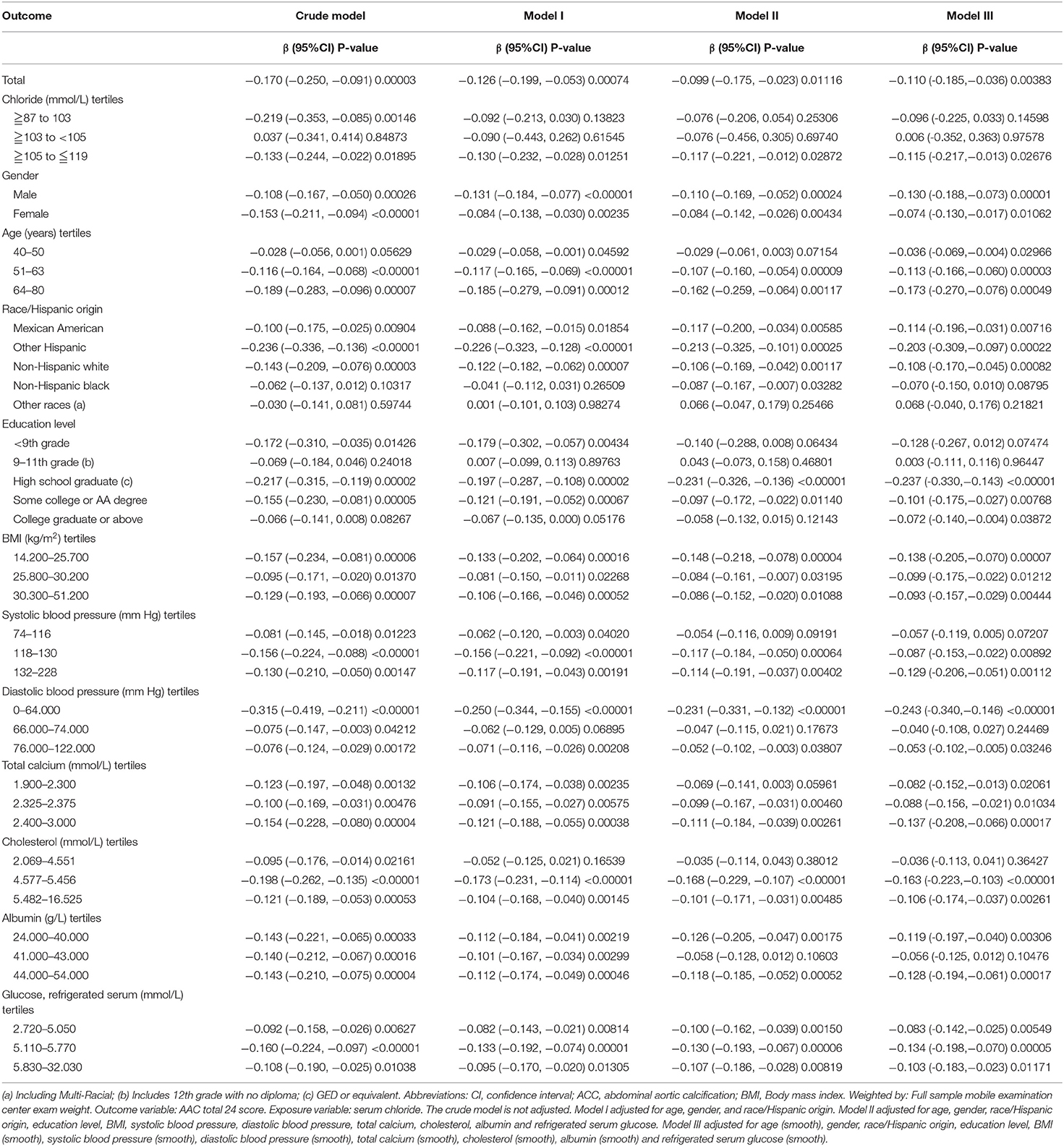
Table 4. Relationship between serum chloride and abdominal aortic calcification (multiple regression equation analysis).
Figure 2 shows the smooth fitting curves of serum chloride and AAC-24. The curve increases first and then decreases gradually, with inflection point being at serum chloride level of 92 mmol/L. We also analyzed the threshold effect and saturation effect using serum chloride of 92 mmol/L as the fold point (Table 5). Weighted by: Full sample mobile examination center exam weight. Outcome variable: AAC-24. Exposure variable: serum chloride (mmol/L). Table 5 shows the adjustment covariates 5. Model I showed a straight-line effect, with a beta value of −0.099 and P < 0.0001. Model II: serum chloride equal to 92 mmol/L was used as the fold point, and the results were statistically significant. Log likelihood ratio tests 0.003. The curve rose after 113 mmol/L. We performed the threshold effect and saturation effect analysis with 113, 114, and 115 mmol/L as folding points; the results are presented in Supplementary Tables S2–S4, respectively. However, the P values after folding point were all >0.05. Figures 3, 4 show the smoothed fitted curves of serum chloride and AAC-24, stratified by different covariates. The curves differed across different strata of individual covariates.
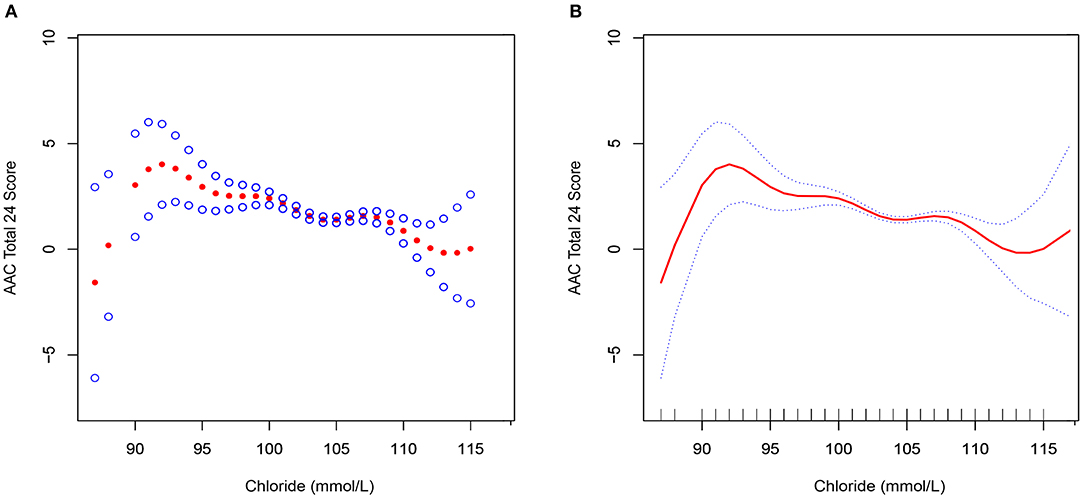
Figure 2. Association between serum chloride and abdominal aortic calcification. The red line represents the smooth curve fit between the variables. The blue bar represents the 95% confidence interval of the fit. Weighted by: full sample mobile examination center examination weight. Adjusted for age (smooth), sex, race/Hispanic origin, education level, BMI (smooth), systolic blood pressure (smooth), diastolic blood pressure (smooth), total calcium (smooth), cholesterol (smooth), albumin (smooth), and refrigerated serum glucose (smooth). (A) Scatter plot of curve fit. (B) Solid line plot of curve fit.
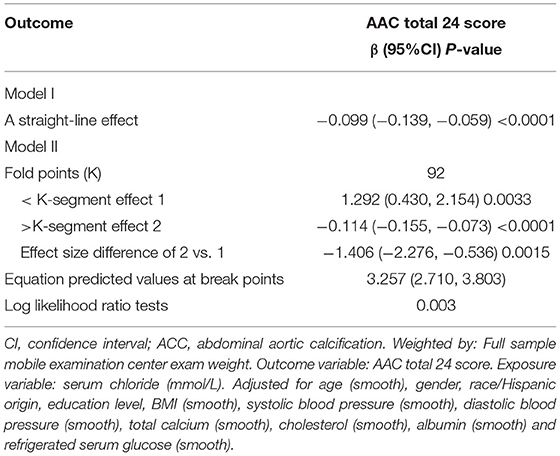
Table 5. Analysis of threshold effect and saturation effect with 92 mmol/L as cutoff serum chloride value point.
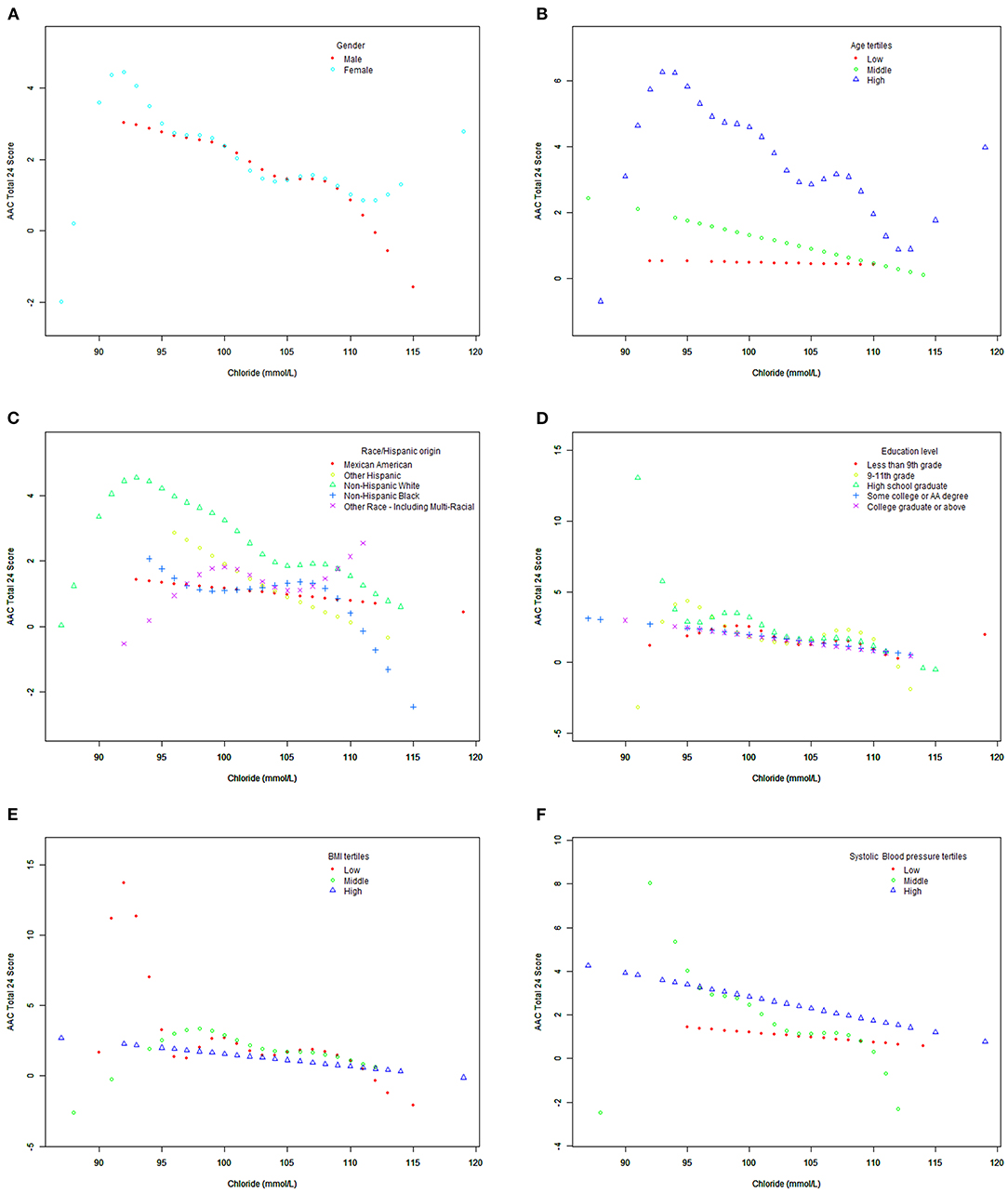
Figure 3. Association between serum chloride and abdominal aortic calcification, stratified by covariates (sex, age, race/Hispanic origin, education level, BMI, systolic blood pressure). Weighted by: full sample mobile examination center examination weight. Adjusted for age (smooth), sex, race/Hispanic origin, education level, BMI (smooth), systolic blood pressure (smooth), diastolic blood pressure (smooth), total calcium (smooth), cholesterol (smooth), albumin (smooth), and refrigerated serum glucose (smooth). (A) Stratified by sex. (B) Stratified by age tertiles. (C) Stratified race/Hispanic origin. (D) Stratified by education level. (E) Stratified by BMI tertiles. (F) Stratified by systolic blood pressure tertiles.
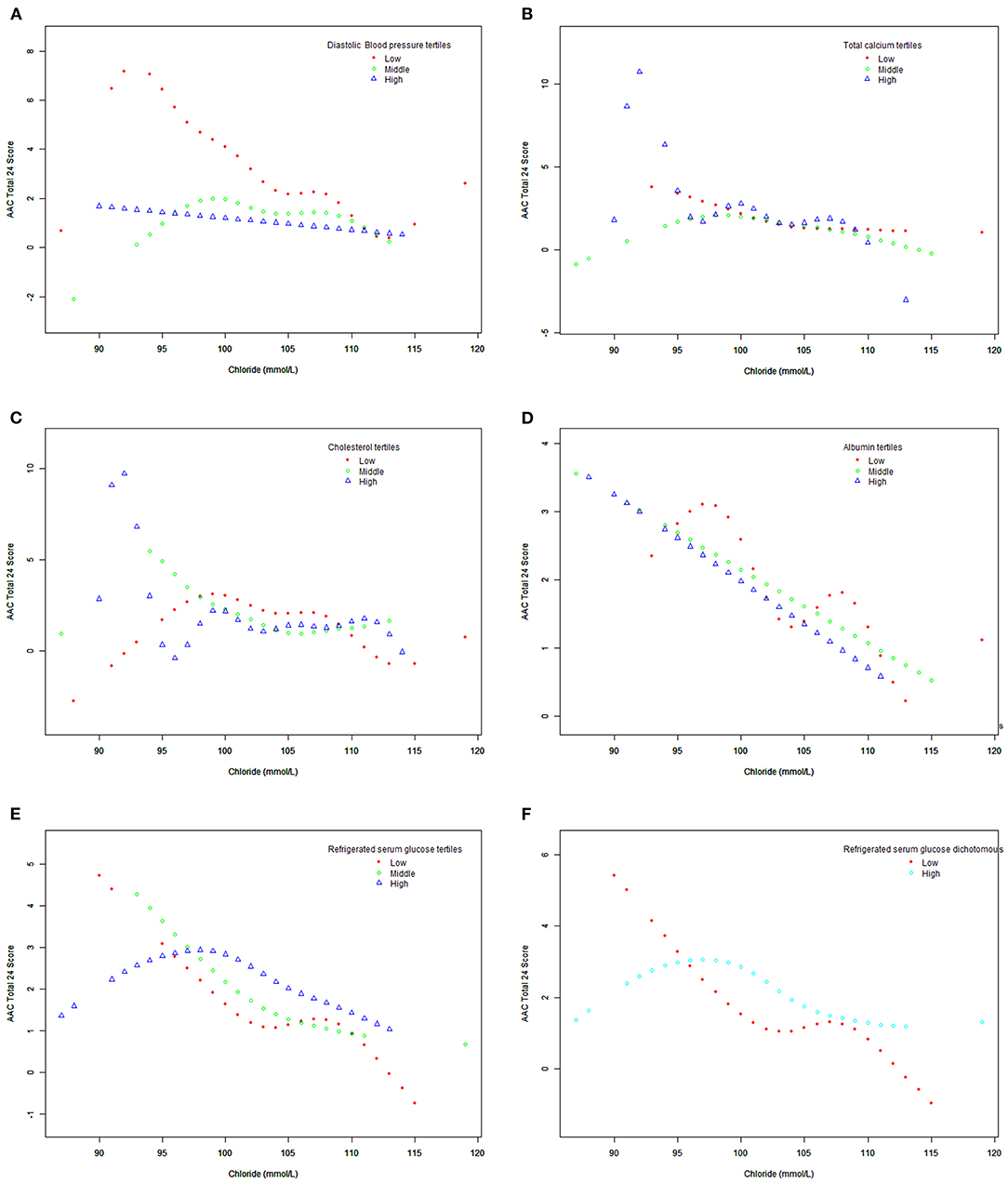
Figure 4. Association between serum chloride and abdominal aortic calcification, stratified by covariates (diastolic blood pressure, total calcium, cholesterol, albumin, refrigerated serum glucose). Weighted by: full sample mobile examination center exam weight. Adjusted for age (smooth), sex, race/Hispanic origin, education level, BMI (smooth), systolic blood pressure (smooth), diastolic blood pressure (smooth), total calcium (smooth), cholesterol (smooth), albumin (smooth), and refrigerated serum glucose (smooth). (A) Stratified by diastolic blood pressure tertiles. (B) Stratified by total calcium tertiles. (C) Stratified cholesterol tertiles. (D) Stratified by albumin tertiles. (E) Stratified by refrigerated serum glucose tertiles. (F) Stratified by refrigerated serum glucose (dichotomous).
The relationship between serum chloride and aortic calcification has not received enough attention. Some studies have found that the Wnt/β-Catenin pathway is involved in arterial calcification via regulation of the osteoprotegerin)/receptor activator of NF-κ B ligand system. The Wnt/β-Catenin pathway is activated or inhibited by lithium chloride in vitro and in vivo (22), implying that chloride may be associated with arterial calcification. Chloride is the cause of arterial calcification. Elastin, a structural protein present in abundance in the arterial wall, is prone to calcification in many diseases; meanwhile, aluminum chloride–pretreated elastin has been shown to be completely resistant to calcification (23, 24). However, none of these earlier studies have directly shown that chloride is associated with arterial calcification; moreover, some of the studies were in animal aortas (23, 24). In this study, we therefore aimed to investigate the association between serum chloride and AAC. We found that serum chloride is independently related to the AAC-24. For serum chloride levels lower than 92 mmol/L, the AAC-24 increased as serum chloride increased, indicating increased risk for calcification; however, for serum chloride levels >92 mmol/L, the AAC-24 decreased as serum chloride increased, indicating a protective effect.
Our large sample size allowed subgroup analysis. When refrigerated serum glucose was 5.38–32.03 mmol/L, the smooth fitting curve between serum chloride and AAC-24 was inverted-U shaped, which is similar to the overall fitting curve between serum chloride and AAC-24, but the inflection point was >92 mmol/L. In the low serum glucose group (2.72–5.33 mmol/L), there was a downward fitting curve. In the low age triad (40–50 years), the smooth fitting curve between serum chloride and AAC-24 score was flat. The smooth fitting curves of low systolic blood pressure (74–116 mmHg) and high systolic blood pressure (76–122 mmHg) were flat.
Since we used a nationally representative sample, our findings are generalizable to the whole US population. Our results suggest that serum chloride levels in adults should be maintained at an appropriate level, and that control of serum chloride level could be a new method for the prevention and control of peripheral artery calcification. Appropriate and individualized measures for prevention for AAC may have to be developed for different ethnic populations, sexes, and age-groups.
It is important to recognize the limitations of our research. First, because of the cross-sectional design of our study, a causal relationship between adult serum chloride level and AAC-24 cannot be inferred. Second, confounding factors not analyzed in this study may affect the results. Third, no attempt has been made to clarify the mechanism by which serum chloride affects abdominal aortic calcification. Fourth, it would be more convincing if the range of the lowest and highest values of serum chloride among the participants examined were larger.
Below a cutoff value of 92 mmol/L, serum chloride appears to be a risk factor for development of abdominal aortic calcification, but serum levels >92 mmol/L may protect against abdominal aortic calcification. Thus, detection of serum chlorine detection could be a simple and accurate method for screening individuals for risk of abdominal aorta calcification and cardiovascular disease.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary Material.
This study was approved by the Ethics Review Board of the National Center for Health Statistics. Informed consent was not considered necessary as this was an analysis of a database.
SH, JP, and YW contributed to data collection, analysis, and writing of the manuscript. SH, TL, WZ, JY, DZ, YZ, SW, QG, LS, DY, JP, YW, and JX contributed to study design and writing of the manuscript. All authors read and approved the final manuscript.
This study was supported by grants from the National Natural Science Foundation of China (81860379 and 82160410) and the Science and Technology Planning Project at the Department of Science and Technology of Jiangxi Province, China (20171BAB 205075).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We hereby thank the participants for their time and energy in the data collection phase of NHANES project.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2021.800458/full#supplementary-material
AAC-24, AAC total 24 score; ACC, abdominal aortic calcification; BMI, body mass index; DXA, dual-energy X-ray absorptiometry; NHANES, National Health and Nutrition Examination Survey.
1. Imaoka Y, Ohira M, Nakano R, Shimizu S, Kuroda S, Tahara H, et al. Impact of abdominal aortic calcification among liver transplantation recipients. Liver Transpl. (2019) 25:79–87. doi: 10.1002/lt.25311
2. Hollander M, Hak AE, Koudstaal PJ, Bots ML, Grobbee DE, Hofman A, et al. Comparison between measures of atherosclerosis and risk of stroke: the Rotterdam Study. Stroke. (2003) 34:2367–72. doi: 10.1161/01.STR.0000091393.32060.0E
3. Wilson PW, Kauppila LI, O'Donnell CJ, Kiel DP, Hannan M, Polak JM, et al. Abdominal aortic calcific deposits are an important predictor of vascular morbidity and mortality. Circulation. (2001) 103:1529–34. doi: 10.1161/01.CIR.103.11.1529
4. van der Meer IM, Bots ML, Hofman A. del Sol AI, van der Kuip DA, Witteman JC. Predictive value of noninvasive measures of atherosclerosis for incident myocardial infarction: the Rotterdam Study. Circulation. (2004) 109:1089–94. doi: 10.1161/01.CIR.0000120708.59903.1B
5. Jayalath RW, Mangan SH, Golledge J. Aortic calcification. Eur J Vasc Endovasc Surg. (2005) 30:476–88. doi: 10.1016/j.ejvs.2005.04.030
6. Golledge J. Abdominal aortic calcification: clinical significance, mechanisms and therapies. Curr Pharm Des. (2014) 20:5834–8. doi: 10.2174/1381612820666140212195309
7. Rodríguez AJ, Leow K, Szulc P, Scott D, Ebeling P, Sim M, et al. Abdominal aortic calcification, bone mineral density and fractures: a systematic review and meta-analysis protocol. BMJ Open. (2019) 9:e026232. doi: 10.1136/bmjopen-2018-026232
8. Kawada T. Effect of serum chloride on mortality in hypertensive patients. Hypertension. (2014) 63:e14. doi: 10.1161/HYPERTENSIONAHA.113.02877
9. Grodin JL, Simon J, Hachamovitch R, Wu Y, Jackson G, Halkar M, et al. Prognostic role of serum chloride levels in acute decompensated heart failure. J Am Coll Cardiol. (2015) 66:659–66. doi: 10.1016/j.jacc.2015.06.007
10. Mao W, Wu J, Zhang H, Zhou J, Ye B, Li G, et al. Increase in serum chloride and chloride exposure are associated with acute kidney injury in moderately severe and severe acute pancreatitis patients. Pancreatology. (2019) 19:136–42. doi: 10.1016/j.pan.2018.11.006
11. Khatri M, Zitovsky J, Lee D, Nayyar K, Fazzari M, Grant C. The association between serum chloride levels and chronic kidney disease progression: a cohort study. BMC Nephrol. (2020) 21:165. doi: 10.1186/s12882-020-01828-3
12. Kazory A, Costanzo MR. The dynamic relationship between serum chloride and cardiorenal syndrome. Rev Cardiovasc Med. (2020) 21:25–9. doi: 10.31083/j.rcm.2020.01.6
13. Akaishi T, Takahashi T, Himori N, Takeshita T, Nakazawa T, Aoki M, et al. Chloride imbalance is involved in the pathogenesis of optic neuritis in neuromyelitis optica. J Neuroimmunol. (2018) 320:98–100. doi: 10.1016/j.jneuroim.2018.03.010
14. Thongprayoon C, Cheungpasitporn W, Hansrivijit P, Thirunavukkarasu S, Chewcharat A, Medaura J, et al. Association of serum chloride level alterations with in-hospital mortality. Postgrad Med J. (2020) 96:731–6. doi: 10.1136/postgradmedj-2019-137270
15. Zhao WH, Gou BD, Zhang TL, Wang K. Lanthanum chloride bidirectionally influences calcification in bovine vascular smooth muscle cells. J Cell Biochem. (2012) 113:1776–86. doi: 10.1002/jcb.24049
16. Myers DJ. The effect of potassium phosphate, magnesium chloride and T6 as blocking agents on tissue valve calcification. J Cardiovasc Surg (Torino). (1990) 31:130.
17. Ahluwalia N, Dwyer J, Terry A, Moshfegh A, Johnson C. Update on NHANES dietary data: focus on collection, release, analytical considerations, and uses to inform public policy. Adv Nutr. (2016) 7:121–34. doi: 10.3945/an.115.009258
18. Curtin LR, Mohadjer LK, Dohrmann SM, Montaquila JM, Kruszan-Moran D, Mirel LB, et al. The national health and nutrition examination survey: sample design, 1999–2006. Vital Health Stat 2. (2012) 1–39.
19. Schousboe JT, Wilson KE, Kiel DP. Detection of abdominal aortic calcification with lateral spine imaging using DXA. J Clin Densitom. (2006) 9:302–8. doi: 10.1016/j.jocd.2006.05.007
20. Schousboe JT, Lewis JR, Kiel DP. Abdominal aortic calcification on dual-energy X-ray absorptiometry: methods of assessment and clinical significance. Bone. (2017) 104:91–100. doi: 10.1016/j.bone.2017.01.025
21. Kauppila LI, McAlindon T, Evans S, Wilson PW, Kiel D, Felson DT. Disc degeneration/back pain and calcification of the abdominal aorta. A 25-year follow-up study in Framingham. Spine (Phila Pa 1976). (1997) 22:1642–7. discussion 8–9. doi: 10.1097/00007632-199707150-00023
22. Nie B, Zhang SY, Guan SM, Zhou SQ, Fang X. Role of Wnt/β-catenin pathway in the arterial medial calcification and its effect on the OPG/RANKL system. Curr Med Sci. (2019) 39:28–36. doi: 10.1007/s11596-019-1996-4
23. Vyavahare N, Ogle M, Schoen FJ, Levy RJ. Elastin calcification and its prevention with aluminum chloride pretreatment. Am J Pathol. (1999) 155:973–82. doi: 10.1016/S0002-9440(10)65197-8
24. Vyavahare NR, Hirsch D, Lerner E, Baskin JZ, Zand R, Schoen FJ, et al. Prevention of calcification of glutaraldehyde-crosslinked porcine aortic cusps by ethanol preincubation: mechanistic studies of protein structure and water-biomaterial relationships. J Biomed Mater Res. (1998) 40:577–85. doi: 10.1002/(SICI)1097-4636(19980615)40:4<577::AID-JBM9>3.0.CO;2-C
Keywords: serum chloride, abdominal aortic calcification, association, multiple equation regression analysis, smooth curve fitting
Citation: Hu S, Lan T, Wang S, Su L, Zou S, Ye J, Zhang Y, Zhang D, Guo Q, Zhang W, Yu D, Xu J, Wei Y and Peng J (2022) Serum Chloride Level Is Associated With Abdominal Aortic Calcification. Front. Cardiovasc. Med. 8:800458. doi: 10.3389/fcvm.2021.800458
Received: 23 October 2021; Accepted: 16 December 2021;
Published: 18 January 2022.
Edited by:
Chien-Te Lee, Kaohsiung Chang Gung Memorial Hospital, TaiwanReviewed by:
Zhexue Qin, Xinqiao Hospital, ChinaCopyright © 2022 Hu, Lan, Wang, Su, Zou, Ye, Zhang, Zhang, Guo, Zhang, Yu, Xu, Wei and Peng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yiping Wei, d2VpeWlwMjAwMEBob3RtYWlsLmNvbQ==; Jinhua Peng, MzQ1MTM0NzUzNkBxcS5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.