 Aleksander Dokollari1
Aleksander Dokollari1 Basel Ramlawi2,3
Basel Ramlawi2,3 Gianluca Torregrossa2,3
Gianluca Torregrossa2,3 Michel Pompeu Sá2,3Serge Sicouri2,3
Michel Pompeu Sá2,3Serge Sicouri2,3 Edvin Prifti4Sandro Gelsomino5,6
Edvin Prifti4Sandro Gelsomino5,6 Massimo Bonacchi7*
Massimo Bonacchi7*- 1St. Michael's Hospital, Toronto, ON, Canada
- 2Department of Cardiac Surgery, Lankenau Heart Institute, Wynnewood, PA, United States
- 3Department of Cardiac Surgery Research, Lankenau Institute for Medical Research, Wynnewood, PA, United States
- 4Mother Teresa Hospital, University of Tirana, Tirana, Albania
- 5Department of Cardiac Surgery, Maastricht University Medical Center, Maastricht, Netherlands
- 6Department of Cardiothoracic Surgery, Cardiovascular Research Institute Maastricht—CARIM, Maastricht, Netherlands
- 7Cardiac Surgery Unit, Department of Experimental and Clinical Medicine, University of Florence, Florence, Italy
Objective: To highlight the main target points covered by clinical studies on the Perceval sutureless valve for surgical aortic valve replacement (SAVR) and raise a point of discussion for further expansion of its use when compared with stented bioprostheses (SB) and transcatheter aortic valve replacement (TAVR).
Methods: We reviewed clinical trials and retrospective studies published up to date and compared the outcomes in terms of mortality, myocardial infarction (MI) stroke, paravalvular leak (PVL), permanent pacemaker implantation (PPI), bleeding and long-term outcomes.
Results: Clinical studies showed that 30-day mortality ranged from 0–4% for Perceval and 2.9–7% for TAVR. The incidence of PVL (Perceval 1.9–19.4 vs. TAVR 9–53.5%), PPI (Perceval 2–11.2 vs. TAVR 4.9–25.5%), stroke (Perceval 0 vs. TAVR 0–2.8%), MI (Perceval 0 vs. TAVR 0–3.5%), were all higher in the TAVR group. Compared to other SB, mortality ranged from 0–6.4% for Perceval and 0–5.9% for SB. The incidence of PVR (Perceval 1–19.4 vs. SB 0–1%), PPI (Perceval 2–10.7 vs. SB 1.8–8.5%), stroke (Perceval 0–3.7 vs. SB 1.8–7.3%) and MI (Perceval 0–7.8 vs. SB 0–4.3%) were comparable among the groups. In patients with a bicuspid aortic valve, mortality rate was (0–4%) and PVL incidence was (0–2.3%). However, there was a high incidence of PPI (0–20%), and stroke (0–8%). Long-term survival ranged between 96.7–98.6%.
Conclusions: The Perceval bioprosthesis has proved to be a reliable prosthesis for surgical aortic valve replacement due to its implantation speed, the reduced cardiopulmonary bypass time, the reduced aortic cross-clamp time and the shorter intensive care unit and hospital length of stay.
Introduction
Surgical aortic valve replacement (SAVR) with the sutureless self-expanding Perceval aortic bioprosthesis (LivaNova Group, Milan, Italy) was developed to combine the advantages of the transcatheter aortic valve replacement (TAVR) procedure, allowing for a fast implantation with no need for suturing, with the benefits of a conventional surgical approach owing to the possibility of removing the native valve along with the calcifications. The valve has grown in popularity mostly due to the reduced cardiopulmonary bypass (CPB) time (1), the improved myocardial recovery time and its application in minimally invasive cardiac surgery (MICS) procedures (2). In addition, the three PARTNER clinical trials' (3–5), the SURTAVI trial (6) and other observational cohort studies (7, 8) have evidenced the non-inferiority of TAVR vs. SAVR. In this context, some reports of successful valve-in-valve TAVR in bioprostheses with structural valve deterioration (SVD) have generated enthusiasm particularly for future applications (9, 10). In addition, other outcomes of the valve include improved hemodynamics, a self-expanding radial force, usage in hostile roots, enhanced surgical and recovery speed, and enabling minimally invasive cardiac surgery procedures. However, many points deserve to be highlighted such as the impact of permanent pacemaker implantation (PPI) after SAVR, the application of the sutureless bioprostheses in patients with bicuspid aortic valves (BAV), the impact of thrombocytopenia on the survival rate and the implantation of this bioprostheses in patients with small aortic annuli.
The goal of this review is to highlight the main target points covered by clinical studies and raise a point of discussion for further expansion of the use of Perceval.
Materials and Methods
Inclusion Criteria
Studies were included if any of the following criteria were met: (1) reported outcomes of Perceval compared with other heart valve prostheses or procedures; (2) reported analysis of complications using the Perceval; (3) reported off-label experience; (4) reported learning curve analysis; (5) reported one or more case of SAVR with Perceval.
Exclusion Criteria
Studies were excluded if any of the following criteria were met: (1) reported outcomes of exclusively other sutureless valves; (2) grouped outcomes of Perceval with other prostheses in the same cohort; (3) not published in the English language; (4) not published in a peer-reviewed journal; and (5) was a conference abstract.
Data Collection
The data collection was done on August 31, 2021. One author (AD) screened the articles and reviewed it three times. The final results were reviewed by another investigator (MPS). The primary reported outcomes of the study included (a) the surgical technique; (b) clinical trials investigating the Perceval valve; (c) the sutureless vs. TAVR; (d) the sutureless vs. other stented bioprostheses (e) Perceval in mini-SAVR; (f) Perceval and bicuspid aortic valves; (g) long-term outcomes of the Perceval valve (valve durability); (h) the incidence of thrombocytopenia after Perceval implantation; (i) the ideal candidate for the prosthesis implantation (Figure 1).
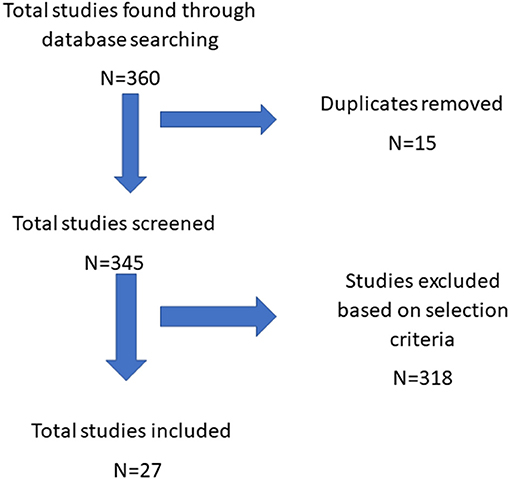
Figure 1. Flowchart study selection process.
The Most Appropriate Surgical Technique for Valve Implantation
The aortic incision is performed at the distal portion at the sinotubular junction to preserve a segment of ascending aorta above the prosthetic valve. The aortic valve should be excised at a position corresponding to the incision line of the native leaflets and the aortic annulus should be decalcified to prepare the implant site. A complete decalcification of the aortic annulus is not necessary. To ensure the correct positioning and orientation of the prosthesis, three guiding sutures are placed to act as reference for accurate alignment of the inflow portion of the prosthesis with the insertion plane of the native leaflets. For each valve sinus, one stitch is positioned immediately 2–3 mm below the lowest portion of the native leaflet resection line. On the prosthesis, each guiding suture is passed into a dedicated thread loop located at the midlevel of the inflow ring and aligned to the median part of the prosthetic sinuses. Once the prosthesis is connected to the three guiding suture, the release device is introduced into the aorta (11). In this context, the Perceval Livanova company recommend placing the guiding sutures 2–3 mm below the leaflet insertion line. Using this technique, Yanagawa et al. (12) found a PPI rate of 28%. Therefore, they modified the technique by placing the guiding sutures at the nadir of each cusp and not 2 to 3 mm below. After the modification, the PPI rate dropped to 0%. Nguyen et al. (13), recommend performing the transverse aortotomy ~3.5 cm above the level of the aortic annulus, and 0.5 cm above the sinotubular junction, to leave a free edge for closure of the aortotomy. In bicuspid aortic valves, the surgeon must recreate 3 nadirs that are positioned at ~120° to better manage the asymmetry of each cusp. To achieve this, the surgeon can use a commercial sizer with 120° markings to recreate a normal nadir. In addition, a dedicated balloon should be inserted into the prosthesis and inflated at a pressure of 4 atm for 30 sec.
Clinical Trials
The “PERCEVAL TRIAL—Perceval S valve pilot study was performed in 30 high-risk patients who were scheduled for isolated SAVR due to severe aortic stenosis (14). This prospective analysis was undertaken at three European Centers from April 2007 to February 2008 and concentrated on perioperative and 1-year outcomes. Operative mortality was 3.3% and moderate paravalvular leak (PVL) was present in two patients. The PERCEVAL-AVR clinical trial evidenced the non-inferiority for the sutureless vs. stented for major adverse cerebral and cardiovascular events at 1 year, whereas aortic valve hemodynamics improved equally in both groups. Perceval significantly reduced surgical times (mean CPB: 71.0 ± 34.1 vs. 87.8 ± 33.9 mins; mean aortic cross-clamp times: 48.5 ± 24.7 vs. 65.2 ± 23.6; both p-values < 0.001), but resulted in a higher rate of permanent pacemaker implantation (PPI – 11.1 vs. 3.6% at 1 year). Incidences of PVL and central leak were similar.
The CAVALIER clinical trial (15) reported a mean cross-clamp time of 41.5 ± 20.3 mins and a mean CPB time of 39.0 ± 12.5 mins while the mean hospital length of stay was 12.0 ± 7.4 days. There were three reported cardiac valve-related deaths, and eight cases were cardiac related but not valve related. There were five early explanted valves 13.8 days post-implant due to PVL discovered at follow-up.
Perceval vs. Tavr. When Enemies Become Allies
SVD has been reported in many case series and the treatment in these patients has successfully been delivered through valve-in-valve TAVR using both the Evolut Pro and the Corevalve (16) (Figure 2). With respect to Perceval vs. TAVR, the SURTAVI trial (6) showed that TAVR with the self-expanding CoreValve was non-inferior to SAVR for the primary endpoint at 2 years for the treatment of severe aortic stenosis in intermediate-risk patients (STS-PROM, 3–15%; median 4.5%). The Perceval valve benefits, may render ViV-TAVR second procedure easier and safer. This includes a self-expanding nitinol stage, a radio-opaque frame, and sinusoidal struts that “push” coronary ostia and sinuses away from prosthesis leaflets. In addition, eight retrospective clinical studies showed that 30-day mortality was higher in the TAVR group which may be explained with the higher preoperative risk in this population (16–24). The most used prosthesis in TAVR were the Corevalve, Sapien, Lotus and Portico. The CPB and aortic cross-clamp time for the Perceval ranged between 54 and 73.4/SD = 23.1–25 mins and 32–43.4/SD = 13.4–17, respectively. Mortality ranged from 0 to 4% for Perceval and 2.9–7% for TAVR. The incidence of PVL (Perceval 1.9–19.4 vs. TAVR 9–53.5%), PPI (Perceval 2–11.2 vs. TAVR 4.9–25.5%), stroke (Perceval 0 vs. TAVR 0–2.8%), and myocardial infarction (MI) (Perceval 0 vs. TAVR 0–3.5%), were all higher in the TAVR group (Table 1).
Figure 2. Sutureless aortic valve in the aortic annulus.
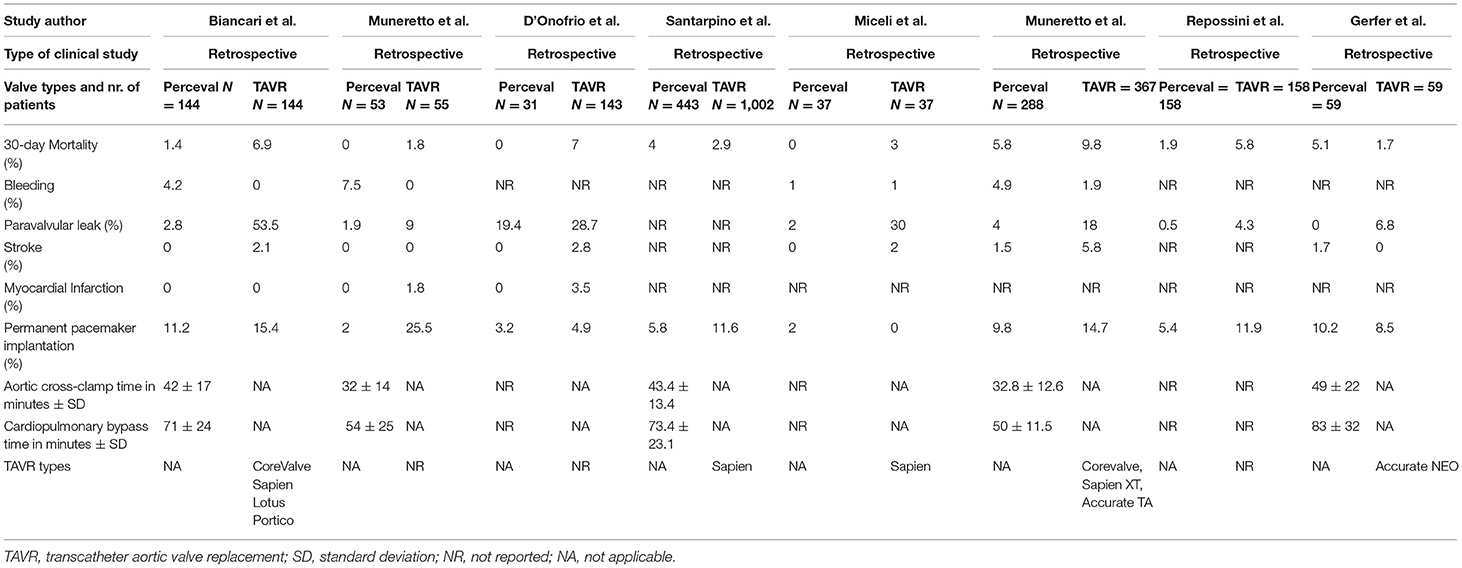
Table 1. Sutureless aortic valve replacement vs. transcatheter aortic valve replacement.
Perceval vs. Other Stented Bioprostheses. New Generation vs. Old Style
Compared to other stented bioprostheses (SB), the Perceval valve had similar outcomes. Four prospective and four retrospective clinical studies showed that 30-day mortality was higher in the Perceval group which may be explained with the higher preoperative risk in this population (24–31). Mortality ranged from 0 to 6.4% for Perceval and 0–5.9% for SB. The aortic cross-clamp time in minutes (Perceval 30.8–65.3/SD = 13.6–29.1 vs. SB 59–90/SD = 23–30.3) and CPB time in minutes (Perceval 47–88/SD = 11–34.9 vs. SB 87.8–120/SD = 20.4–37.9) were all significantly higher in the SB group (p < 0.05). The incidence of PVL (Perceval 1–19.4 vs. SB 0–1%), PM (Perceval 2–10.7 vs. SB 1.8–8.5%), stroke (Perceval 0–3.7 vs. SB 1.8–7.3%), MI (Perceval 0–7.8 vs. SB 0–4.3%), were comparable among the groups (Table 2). The most used stented valves were the CE Perimount, Magna Ease and Triflecta valves.
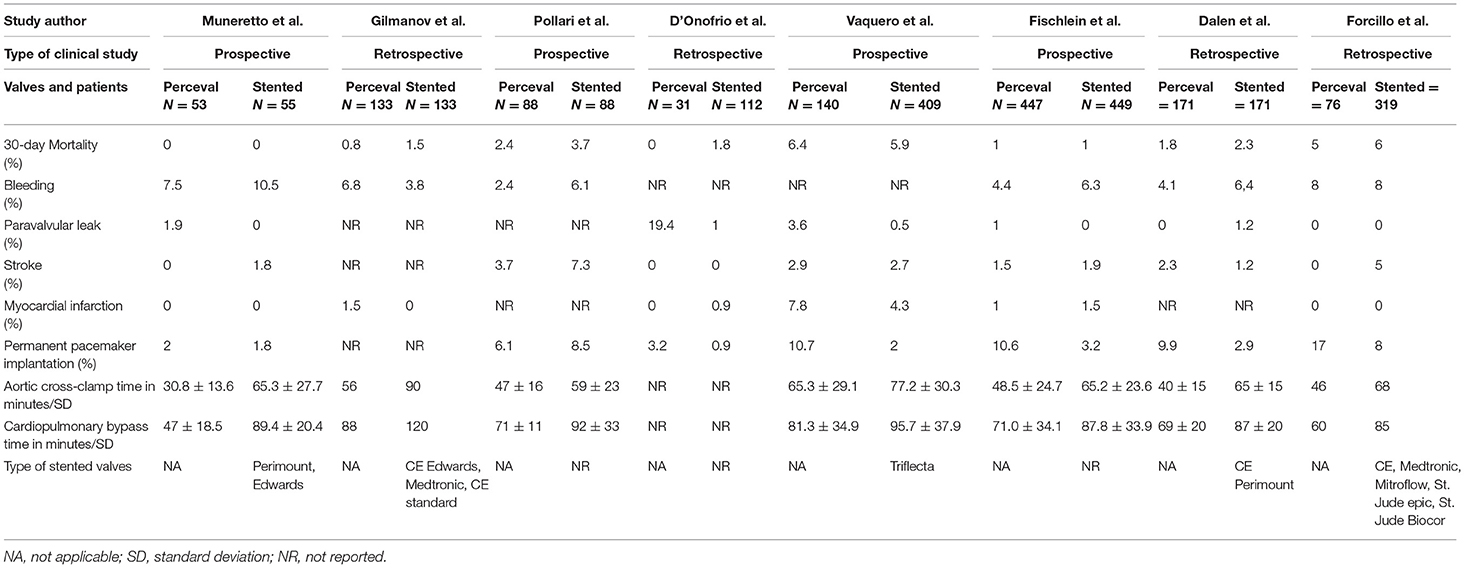
Table 2. Sutureless aortic valve replacement vs. other stented bioprostheses.
Perceval for Mics and Mini-Savr
One of the benefits of the Perceval bioprosthesis is its widespread usage in mini-SAVR. Perceval has been developed in order to combine the best of two worlds, as they could facilitate the implantation while maintaining the benefits of SAVR. Currently, the upper ministernotomy (MS) and the right anterior thoracotomy (RAT) are the most common approaches for (mini-SAVR). Bonacchi et al. (32) evidenced the benefits of the valve in both MS and RAT. In addition, the international prospective registry (33) comparing MS with RAT showed an aortic cross-clamp time of 43 vs. 55 mins (p < 0.01), cardiopulmonary bypass time of 67 vs. 89 mins (p < 0.01) and a prosthesis implantation time of 15.5 vs. 12 mins (p = 0.014), respectively. In this context, the Sutureless and Rapid Deployment International Registry (34), pointed out the efficacy of the Perceval bioprosthesis in redo operations showing a mean cardiopulmonary bypass time of 95 ± 34.3 mins, an aortic cross-clamp time 57.8 ± 23.2 mins with 0% in hospital mortality, a 3.6% incidence of new PPI and 2.5% incidence of PVL. Recent technological developments have led to endoscopic aortic valve replacement. Vola et al. (35) reported the endoscopic SAVR with Perceval. Exposure was provided by four ports in the second, third, and fifth intercostal spaces with fem-fem CPB. Perceval was implanted with an aortic cross-clamp and CPB time of 80 and 166 mins, respectively. At 5-month follow-up, echocardiography was satisfactory. Balkhy et al. (36) reported the first in human robotic SAVR with Perceval. The patient was a 76-year-old male who underwent a combined procedure of coronary artery bypass surgery and SAVR. Two 8-mm arm ports were placed in the 1st and 3rd intercostal space at the midclavivular line. Aortic cross clamp lasted 86 mins. The patient was discharged on postoperative day 2 and at 6-month follow-up the patient was in good health.
Bicuspid Aortic Valves and Perceval
This topic remains controversial among surgeons. Many clinical studies, including the PERSIST-AVR clinical trial (37), excluded patients with a congenital bicuspid aortic valve. Some reports suggested that the sutureless valves may increase the risk of PVL and/or potential dislocation related to BAV aortic root asymmetry (38). Nguyen et al. (13) emphasized that the most crucial point during surgery is to recreate three natural nadirs points positioned at 120° with the aim of recreating a circular annulus. Four retrospective clinical studies (13, 34, 39, 40) with a small population ranging between 11 and 88 patients evidenced a low mortality rate (0–4%) and PVL incidence (0–2.3%). However, there was a high incidence of PPI (0–20%), and stroke (0–8%) (Table 3). The mean aortic cross clamp time in minutes (39–55/SD = 3.1–14) and CPB time in minutes (54.5–80/SD = 4.4–22) were higher compared to non BAV procedures. These outcomes mean that despite recent surgical technique developments, PPI remain a hurdle for BAV patients undergoing SAVR with sutureless bioprostheses.
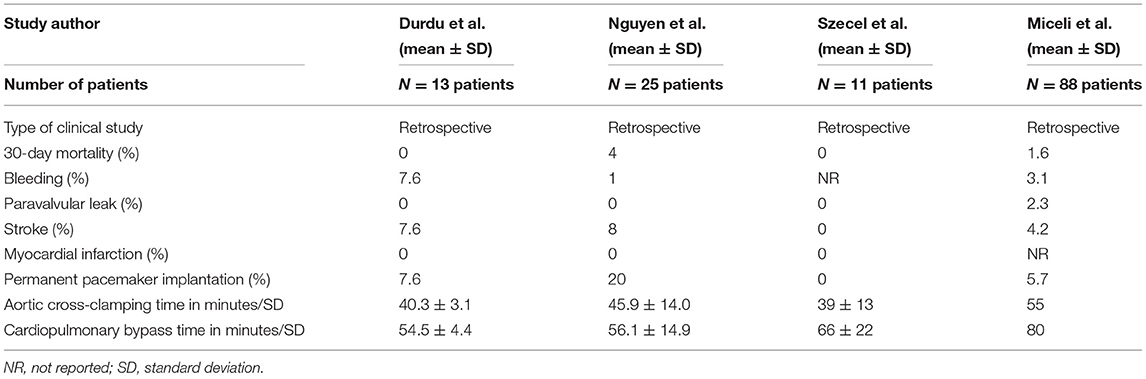
Table 3. Clinical outcomes of bicuspid aortic valve stenosis treated with sutureless valve.
Thrombocytopenia. Do We Really Need to Correct It?
Several causes of platelet dysfunction have been speculated: (1) the detoxification process with homocysteic acid and the storage aldehyde-free solution; (2) the naked alloy stent; and (3) mechanical stress and turbulence, especially in small valve sizes (41). At the end of the day, Vendramin and Bortolotti correctly pose the following questions: Do we really need to solve it and why should we still be worried (42)? In this context, Stegmeier et al. (43) showed that Perceval, when compared to other prostheses, is more prone to causing thrombocytopenia, however, no detrimental clinical effect of this phenomenon was found. The mean minimum platelets count was 47,000 μm and upon discharge the platelets level was 166,000 μm. Can medical therapy have an impact on thrombocytopenia? The result from the study showed a non-significant difference among patients on aspirin and dual antiplatelet medical therapy. In addition, there was no significant change in platelets and red blood cells transfusion. However, the reoperation for bleeding rate (20%) was higher than in the other two groups (Labcor TLPB-A = 4% and Hancock valve = 8%). Moreover, a sub-analysis of the PERSIST-AVR clinical trial evidenced that the Perceval group had a higher platelet reduction than the control group (46 vs. 32%) (44). The phenomenon was transient in both groups, with a slow recovery of the platelet count by hospital discharge. No differences were observed between groups regarding need of transfusions, blood loss, major bleeding and stroke events. While comparing the Intuity valve with its Perceval counterpart, Jiritano et al. (41) found that no risk factors that may have predisposed to platelet dysfunction were found in either group. More red blood cell transfusions were given to the Perceval group as compared with the Intuity group (10 vs. 7 units, p = 0.012) as well as platelets (4 vs. 0 units, P < 0.01). Platelet count at discharge for Perceval was 102.18 ± 29.34 μm. In addition, mean platelet volume was significantly larger in the Perceval group on postoperative days 1, 3, and 5 (P = 0.04, P = 0.001, P = 0.015), whereas platelet distribution width was significantly larger in the Perceval group on postoperative days 3 and 5 (P = 0.018, P = 0.026). Looking at the clinical studies outcomes the answer to Vendramin and Bortolotti is the following: “no, we do not need to correct the transient thrombocytopenia, but we should be cautious.”
Hemodynamic Changes, Ventricular Mass Regression, and Porcelain Aorta
We found nine clinical studies but only eight were reporting data with standard deviations. Six of the studies were retrospective observational cohort studies and two were prospective non-randomized clinical trials (Table 4) (11, 21–23, 35, 36). The effective orifice area (EOA) ranged between 1.5 and 1.7 cm2/SD = 0.3–0.5 since discharge up to 2 years of follow-up. The mean transvalvular gradient ranged between 10.1 and 14 mmHg/ SD = 4.3–6.4 at discharge, 8.9 mmHg/ SD = 3.2–4.2 at 6 months, 8.7–9.9 mmHg/SD = 3.7–5 at 1 year and 8–9 mmHg/SD = 3.4–4.1 at 2 years follow-up. The peak transvalvular gradient was 19.4–27 mmHg/SD = 8.1–11 at discharge, 16.8–19.6 mmHg/SD = 6.7–7.6 at 6 months, 17.1–20.9 mmHg/SD 7.6–9.2 at 1 year, 16.6–18.3 mmHg/SD 5.6–7.2 mmHg at 2 years follow-up. With respect to the ventricular mass regression, Santarpino et al. (45) found that the mean ± SD left ventricular mass index decreased from 148.4 ± 48.4 g/m2 to 119.7 ± 38.5 g/m2 (P = 0.002) whereas interventricular septum and posterior wall thickness decreased from 13.9 ± 2.3 mm to 12.1 ± 2.8 mm (P = 0.02) and 12.1 ± 1.6 mm to 11.3 ± 1.3 mm (P = 0.04) at follow-up. In addition, there have been sporadic reports of the implantation of the Perceval in porcelain aortas. Santarpino et al. (46) reported a 72-year-old woman with severe AS, coronary artery disease, and porcelain aorta. The patient underwent CABG, removal of the ascending aorta, and implantation of a 23-mm Perceval and FlowWeave Bioseal 24-mm prosthesis (Jotec, Hechingen, Germany). Gatti et al. (47) reported the use of Perceval in four patients with porcelain aorta. All patients were discharged within postoperative day 20 and, at 1 to 6-month, were alive with improvements in symptoms.
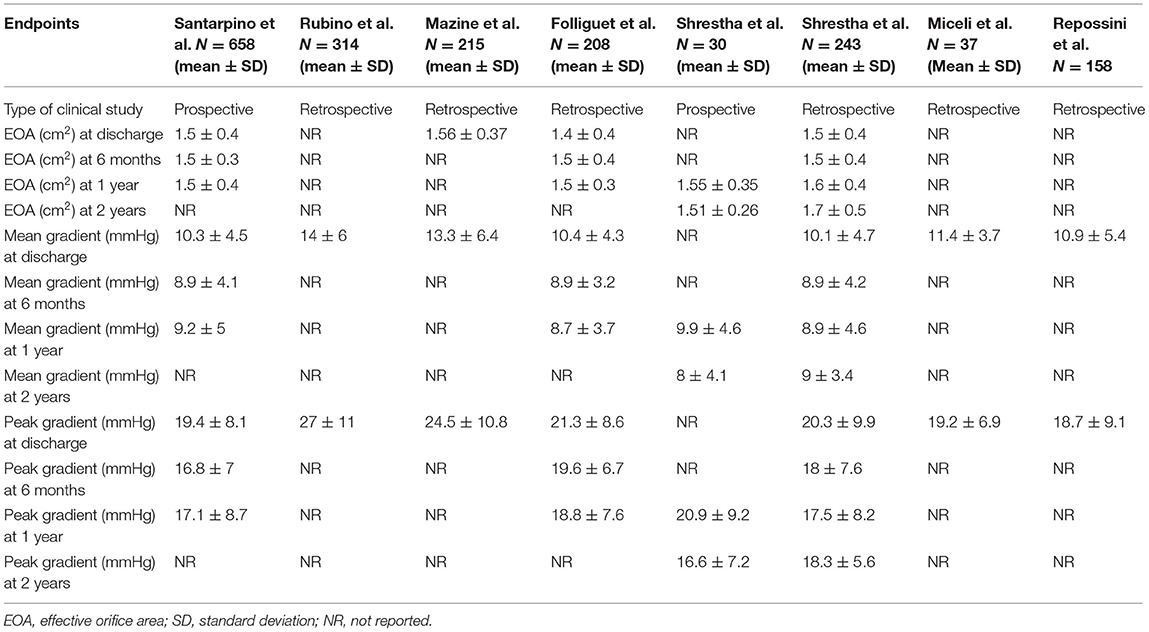
Table 4. Hemodynamic outcomes.
Long-Term Outcomes Of The Perceval Valve
The Perceval aortic valve has proven to be a reliable bioprosthesis with excellent early and midterm outcomes. However, the long-term outcomes of the valve have not been studied and results are coming from some clinical studies. Our literature research found one retrospective study and one clinical trial with a 5-year follow-up period (Table 5). Shrestha et al. (48) reported the outcomes of 720 patients evidencing a 1.4% of cardiac deaths, 1,5% of valve explants, 1% of major paravalvular leak, 1.4% of A-V block III and 0.8% of stroke. The 5-year outcomes of a prospective clinical trial (14) with only 30 patients evidenced a cardiac mortality of 3.3%, an A-V block type III of 3.3% but no stroke, paravalvular leak, valve thrombosis or structural valve deterioration was noticed. The echocardiographic outcomes at 3, 4, and 5-year follow-up evidenced an EOA of 1.64–1.68 (SD 0.4–0.42), 1.68 (SD 0.43), 1.69–1.8 (SD 0.3–0.42), respectively. In addition, the mean transvalvular gradient across the valve at 3, 4, and 5 years was 7.7–8.3 mmHg (SD 2.5–2.8), 7.6–7.8 mmHg (SD 3.6–3.8), 8.8–9.3 mmHg (SD 4.6–5.5), respectively. These results once more confirm the usefulness of the Perceval valve (Table 6).
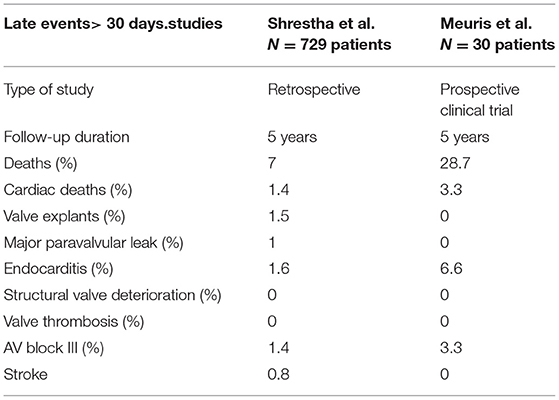
Table 5. Long-term outcomes of the Perceval bioprosthesis.
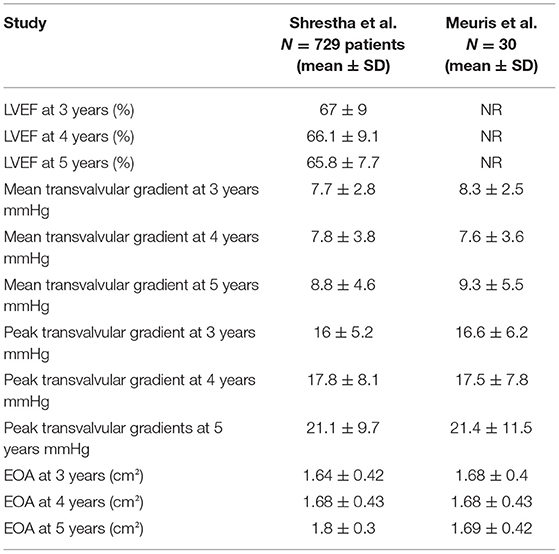
Table 6. Long-term echocardiographic outcomes (5-year follow-up) of the Perceval bioprosthesis.
The Ideal Candidate for Sutureless Aortic Valve Replacement
Many studies have evidenced the benefits of Perceval aortic bioprosthesis, especially in the following three situations:
(a) High-risk patients undergoing a combined surgical procedure
(b) Hostile aortic root
(c) A small aortic annulus.
In the first situation, the use of sutureless and rapid-deployment valves allows economy of precious CPB time by alleviating the need to place and tie sutures around the aortic annulus, while still allowing native valve excision and annular decalcification. In a systematic review and meta-analysis that included 12 observational studies, Phan et al. (49) demonstrated that the pooled durations of cardiopulmonary bypass and aortic cross-clamp for isolated SAVR were 57 and 33 min, respectively. These values are nearly half of those reported in the Society of Thoracic Surgeons National Database1 for conventional SAVR.
In hostile aortic roots and redo operations, Perceval may become the bioprosthesis of choice. In addition to the time-saving procedure and to the non-necessity of complete annular decalcification, it allows valve replacement after graft infection. In the last scenario, the benefits include less foreign material used (pledgets/sutures), less manipulation of friable tissues, and radial force of Perceval solidifies root repair. During reoperations and extensive decalcification of the annulus, clefts in the mitral valve/left atrium can form. In this situation, the Perceval valve can be easily compressed and removed (without the necessity of removing all the sutures as in the stented valves), the cleft repaired, and the valve redeployed again (50). However, neither the CAVALIER nor the PERSISTENT-AVR clinical trials mentioned the hostile aortic root.
Finally, in case of a small aortic annulus, an aortic root enlargement should be performed to implant an adequately sized bioprosthesis. However, this is not always feasible as newly minted surgeons do not have sufficient technical experience to perform these procedures. In this scenario, the sutureless prosthesis have shown good outcomes when implanted with low post-procedural transvalvular gradients (45). In addition, Perceval is a proven option for high-risk patients and for those at risk of prosthesis-patient mismatch (51).
Contraindications for the prosthesis implantation are (a) subjects with aortic root enlargement, where the ratio between observed and expected diameters (calculated as a function of age and patient body surface area) is ≥1.3; (b) subjects with known hypersensitivity to nickel alloys, (c) subjects with aneurysmal dilation or dissection of the ascending aortic wall needing surgical correction.
Potential Pitfalls of Perceval
Limitations and drawbacks of the Perceval bioprosthesis are the following;
(a) PVL.
(b) Acquired conduction disorders and PPI.
(c) SVD and need for reintervention.
PVL has shown an increased incidence in the TAVR and the sutureless bioprostheses with the latter being the highest (52). Surgeons came to understand that the Achilles heel of these bioprostheses is the non-coronary sinus which is slightly lower compared to the left and right sinuses. During the deployment phase, the valve must be positioned in a lower angle of 15–30° at the level of the non-coronary sinus, on the side of the surgeon. When the valve is accurately positioned, and no gap exists on visual inspection than it should be deployed. This technique avoids the incidence of PVL. However, it has been shown that these results are related to a learning curve and experienced surgeons tend to have a lower incidence of PVL (53).
The PPI trend has shown a slow but steadily decrease since the introduction by Yanagawa et al. (12) of their modification of the implantation height. They found that a higher implantation of the valve (2–3 mm) decreases the incidence of conduction abnormalities requiring a pacemaker. This is in contrast with the first prescription given from the company to implant the valve below the annular plane. SVD happens continuously and Perceval is not exempt from it.
Conclusions
The Perceval bioprosthesis has proved to be a reliable prosthesis for conventional SAVR and mini-SAVR due to its implantation speed, the reduced CPB time, the reduced aortic cross-clamp time and the shorter intensive care unit and hospital length of stay. In addition, its adoption in hostile roots, and the usage in reinterventions coupled with the low profile render it a formidable tool in the surgical armamentarium.
Author Contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Conflict of Interest
BR has received financial support from Medtronic, LivaNova, and AtriCure.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
TAVR, transcatheter aortic valve replacement; CPB, cardiopulmonary bypass; PPI, permanent pacemaker implantation; BAV, bicuspid aortic valve; MI, myocardial infarction; PVL, paravalvular leak; SAVR, surgical aortic valve replacement; MS, mini-sternotomy; RAT, right anterior thoracotomy.
Footnotes
References
1. Santarpino G, Pfeiffer S, Concistre G, Grossmann I, Hinzmann M, Fischlein T. The Perceval S aortic valve has the potential of shortening surgical time: does it also result in improved outcome? Ann Thorac Surg. (2013) 96:77–81. doi: 10.1016/j.athoracsur.2013.03.083
2. Solinas M, Bianchi G, Chiaramonti F, Margaryan R, Kallushi E, Gasbarri T, et al. Right anterior mini-thoracotomy and sutureless valves: the perfect marriage. Ann Cardiothorac Surg. (2020) 9:305–13. doi: 10.21037/acs-2019-surd-172
3. Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. (2010) 363:1597–607. doi: 10.1056/NEJMoa1008232
4. Leon MB, Smith CR, Mack MJ, Makkar RR, Svensson LG, Kodali SK, et al. Transcatheter or surgical aortic-valve replacement in intermediate-risk patients. N Engl J Med. (2016) 374:1609–20. doi: 10.1056/NEJMoa1514616
5. Mack MJ, Leon MB, Thourani VH, Makkar R, Kodali SK, Russo M, et al. Transcatheter aortic-valve replacement with a balloon-expandable valve in low-risk patients. N Engl J Med. (2019) 380:1695–705. doi: 10.1056/NEJMoa1814052
6. Reardon MR, Mieghem NMV, Pompa JJ, Kleiman NS, Sondergaard L, Mumtaz M, et al. Surgical or transcatheter aortic-valve replacement in intermediate-risk patients. (2017) 376:1321–31. doi: 10.1056/NEJMoa1700456
7. Virtanen MPO, Eskola M, Jalava MP, Husso A, Laakso T, Niemela M et al. Comparison of outcomes after transcatheter aortic valve replacement vs. surgical aortic valve replacement among patients with aortic stenosis at low operative risk. JAMA Netw Open. (2019) 2:e195742. doi: 10.1001/jamanetworkopen.2019.5742
8. Dokollari A, Cameli M, Mandoli GE, Kalra DS, Poston R, Coku L et al. Early and midterm clinical outcomes of transcatheter valve-in-valve implantation vs. redo surgical aortic valve replacement for aortic bioprosthetic valve degeneration: two faces of the same medal. J Cardiothorac Vasc Anesth. (2021) 24:29. doi: 10.1053/j.jvca.2021.05.029
9. Andreas M, Coti J, Laufer G, Kastner J. Valve-in valve transcatheter aortic valve implantation into a novel, sutureless bioprosthesis: technical considerations. Eurointervention. (2018) 13:1902–3. doi: 10.4244/EIJ-D-17-00578
10. Suleiman T, Tanseco K, Arunothayaraj S, Michail M, Cockburn J, Hadjivassilev S, et al. Valve-in-valve transcatheter aortic valve implantation for the failing surgical Perceval bioprosthesis. Cardiovasc Revasc Med. (2021) 21:S1553–8389. doi: 10.1016/j.carrev.2021.07.023
11. Folliguet TA, Laborde F, Zannis K, Ghorayeb G, Haverich A, Shrestha M. Sutureless perceval aortic valve replacement: results of two European centers. Ann Thorac Surg. (2012) 93:1483–8. doi: 10.1016/j.athoracsur.2012.01.071
12. Yanagawa B, Cruz J, Boisvert L, Bonneau D. A simple modification to lower incidence of heart block with sutureless valve implantation. J Thorac Cardiovasc Surg. (2016) 152:630–2. doi: 10.1016/j.jtcvs.2016.02.034
13. Nguyen A, Fortin W, Mazine A, Bouchard D, Carrier M, El-Hamamsy I, et al. Sutureless aortic valve replacement in patients who have bicuspid aortic valve. J Thorac Cardiovasc Surg. (2015) 150:851–7. doi: 10.1016/j.jtcvs.2015.05.071
14. Meuris B, Flameng WJ, Laborde F, Folliguet TA, Haverich A, Shrestha M. Five-year results of the pilot trial of a sutureless valve. J Thorac Cardiovasc Surg. (2015) 150:84–8. doi: 10.1016/j.jtcvs.2015.03.040
15. Laborde F, Fischlein T, Hakim-Meibodi K, Misfeld M, Carrel T, Zambala M, et al. Clinical and haemodynamic outcomes in 658 patients receiving the Perceval sutureless aortic valve: early results from a prospective European multicentre study (the Cavalier Trial). Eur J Cardiothorac Surg. (2016) 49:978–86. doi: 10.1093/ejcts/ezv257
16. Misfeld M, Abdel-Wahab M, Thiele H, Borger MA, Holzhey D. A series of four transcatheter aortic valve replacement in failed Perceval valves. Ann Cardiothorac Surg. (2020) 9:280–8. doi: 10.21037/acs-2020-surd-20
17. Biancari F, Barbanti M, Santarpino G, Deste W, Tamburrino C et al. Immediate outcome after sutureless vs. transcatheter aortic valve replacement. Heart Vessels. (2016) 31:427–33. doi: 10.1007/s00380-014-0623-3
18. Muneretto C, Solinas M, Folliguet T, Di Bartolomeo R, Repossini A, Laborde F, et al. Sutureless vs. transcatheter aortic valves in elderly patients with aortic stenosis at intermediate risk: a multi-institutional study. J Thorac Cardiovasc Surg. (2020) 4:179. doi: 10.1016/j.jtcvs.2020.04.179
19. D'Onofrio A, Messina A, Lorusso R, Alfieri O, Fusari M, Rubino P, et al. Sutureless aortic valve replacement as an alternative treatment for patients belonging to the “gray zone” between transcatheter aortic valve implantation and conventional surgery: a propensity-matched, multicenter analysis. J Thorac Cardiovasc Surg. (2012) 144:1010–6. doi: 10.1016/j.jtcvs.2012.07.040
20. Santarpino G, Pfeiffer S, Jessl J, Dell'Aquila AM, Pollari F, Pauschinger M, et al. Sutureless replacement vs. transcatheter valve implantation in aortic valve stenosis: a propensity matched analysis of 2 strategies in high-risk patients. J Thorac Cardiovasc Surg. (2014) 147:561–7. doi: 10.1016/j.jtcvs.2013.10.025
21. Miceli A, Gilmanov D, Murzi M, Marchi F, Ferrarini M, Cerillo AG, et al. Minimally invasive aortic valve replacement with a sutureless valve through a right anterior mini-thoracotomy vs. transcatheter aortic valve implantation in high-risk patients. Eur J Cardiothorac Surg. (2016) 49:960–5. doi: 10.1093/ejcts/ezv210
22. Muneretto C, Alfieri O, Cesana BM, De Bonis M, Di Bartolomeo R, et al. A comparison of conventional surgery, transcatheter aortic valve replacement, and sutureless valves in “real-world” patients with aortic stenosis and intermediate- to high-risk profile. J Thorac Cardiovasc Surg. (2015) 150:1570–7; discussion 1577–9. doi: 10.1016/j.jtcvs.2015.08.052
23. Repossini A, Fischlein T, Solinas M, Di Bacco L, Passaretti B, Grubitzsch H, et al. Stentless sutureless and transcatheter valves: a comparison of the hemodynamic performance of different prostheses concept. Minerva Cardioangiologica. (2018) 66:180–90. doi: 10.23736/S0026-4725.17.04564-9
24. Gerfer S, Mauri V, Kuhn E, Adam M, Djordevic I, Ivanov B, et al. Comparison of Self-expanding RDV perceval S vs. TAVI ACURATE neo/TF. Thorac Cardiovasc Surg. (2021) 69:420–7. doi: 10.1055/s-0040-1722692
25. Muneretto C, Bisleri G, Moggi A, Di Bacco L, Tespili M, Repossini A, et al. Treating the patients in the 'grey-zone' with aortic valve disease: a comparison among conventional surgery, sutureless valves and transcatheter aortic valve replacement. Interact Cardiovasc Thorac Surg. (2015) 20:90–5. doi: 10.1093/icvts/ivu340
26. Gilmanov D, Miceli A, Ferrarini M, Farneti P, Murzi M, Solinas M, et al. Aortic valve replacement through right anterior minithoracotomy: can sutureless technology improve clinical outcomes? Ann Thorac Surg. (2014) 98:1585–92. doi: 10.1016/j.athoracsur.2014.05.092
27. Pollari F, Santarpino G, Dell'Aquila AM, Gazdag L, Alnahas H, Vogt F, et al. Better short-term outcome by using sutureless valves: a propensity-matched score analysis. Ann Thorac Surg. (2014) 98:616–7. doi: 10.1016/j.athoracsur.2014.04.072
28. D'Onofrio A, Rizzoli G, Messina A, Alfieri O, Lorusso R, Salizzoni S, et al. Conventional surgery, sutureless valves, and transapical aortic valve replacement: what is the best option for patients with aortic valve stenosis? a multicenter, propensity-matched analysis. J Thorac Cardiovasc Surg. (2013) 146:1065–70; discussion 1070–1. doi: 10.1016/j.jtcvs.2013.06.047
29. Hernandez-Vaquero D, Vigil-Escalera C, Persia Y, Morales C, Pascual I, Dominguez-Rodriguez A, et al. Perceval or trifecta to prevent patient-prosthesis mismatch. J Clin Med. (2020) 9:2964. doi: 10.3390/jcm9092964
30. Fischlein T, Folliguet T, Meuris B, Shrestha ML, Roselli EE, McGlothlin A, et al. Sutureless vs. conventional bioprostheses for aortic valve replacement in severe symptomatic aortic valve stenosis. J Thorac Cardiovasc Surg. (2021) 161:920–932. doi: 10.1016/j.jtcvs.2020.11.162
31. Dalen M, Biancari F, Rubino AS, Santarpino G, Glaser N, Praetere HD, et al. Aortic valve replacement through full sternotomy with a stented bioprosthesis vs. minimally invasive sternotomy with a sutureless bioprosthesis. Eur J Cardithorac Surg. (2016) 49:220–7. doi: 10.1093/ejcts/ezv014
32. Bonacchi M, Dokollari A, Parise O, Sani G, Prifti E, Bisleri G, et al. Ministernotomy compared with right anterior minithoracotomy for aortic valve surgery. J Thorac Cardiovasc Surg. (2021) 22:125. doi: 10.1016/j.jtcvs.2021.03.125
33. Glauber M, Di Bacco L, Cuenca J, Di Bartolomeo R, Baghai M, Zakova D, et al. Minimally invasive aortic valve replacement with sutureless valves: results from an international prospective registry. Innovation. (2020) 15:120–30. doi: 10.1177/1556984519892585
34. Miceli A, Berretta P, Fiore A, Andreas M, Solinas M, Santarpino G, et al. Sutureless and rapid deployment implantation in bicuspid aortic valve: results from the sutureless and rapid-deployment aortic valve replacement international registry. Ann Cardiothorac Surg. (2020) 9:298–304. doi: 10.21037/acs-2020-surd-33
35. Vola M, Fuzellier JF, Campisi S, Grinberg D, Albertini JN, Morel J et al. Total endoscopic sutureless aortic valve replacem rationale, development, perspectives. Ann Cardiothorac Surg. (2015) 4:170–4. doi: 10.3978/j.issn.2225-319X.2014.11.04
36. Balkhy S, Kitahara H. First human totally endoscopic robotic-assisted sutureless aortic valve replacement. Ann Thorac Surg. (2020) 109:e9–e11. doi: 10.1016/j.athoracsur.2019.04.093
37. Lorusso R, Folliguet T, Shrestha M, Meuris B, Kappetein AP, Roselli E, et al. Sutureless vs. stented bioprostheses for aortic valve replacement: the randomized PERSIST-avr study design. Thorac Cardiovasc Surg. (2020) 68:114–23. doi: 10.1055/s-0038-1675847
38. Jug J, Stor Z, Gersak B. Anatomical circumstances and aortic cross-clamp time in minimally invasive aortic valve replacement. Interact Cardiovasc Thorac Surg. (2021) 32:204–12. doi: 10.1093/icvts/ivaa251
39. Durdu MS, Gumus F, Ozcinar E, Cakici M, Bermede O, Dincer I et al. Sutureless valve replacement through a right anterior mini-thoracotomy in elderly patients with stenotic bicuspid aortic valve. Semin Thorac Cardiovasc Surg. (2019) 31:458–64. doi: 10.1053/j.semtcvs.2018.09.025
40. Szecel D, Eurlings R, Rega F, Verbrugghe P, Meuris B. Perceval sutureless aortic valve implantation: mid-term outcomes. Ann Thorac Surg. (2020) 6:64. doi: 10.1016/j.athoracsur.2020.06.064.
41. Jiritano F, Cristodoro L, Malta E, Mastroroberto P. Thrombocytopenia after sutureless aortic valve implantation: comparison between Intuity and Perceval bioprosthesis. J Thorac Cardiovasc Surg. (2016) 152:1631–3. doi: 10.1016/j.jtcvs.2016.07.054
42. Vendramin I, Bortolotti U. The thrombocytopenia conundrum after aortic bioprosthetic implantation: do we really need to solve it? J Thorac Cardiovasc Surg. (2021) 161:e21–2. doi: 10.1016/j.jtcvs.2020.06.129
43. Stegmeier P, Schlomicher M, Stiegler H, Straucht JT, Bechtel JFM. Thrombocytopenia after implantation of the Perceval S aortic bioprosthesis. J Thorac Cardiovasc Surg. (2020) 160:61–8. doi: 10.1016/j.jtcvs.2019.07.046
44. Lorusso R, Jiritano F, Roselli E, Shrestha M, Folliguet T, Meuris B, et al. Perioperative platelet reduction after sutureless or stented valve implantation: results from the PERSIST-AVR controlled randomized trial. EJCTS. (2021) 21:175. doi: 10.1093/ejcts/ezab175
45. Santarpino G, Pfeiffer S, Pollari F, Concistré G, Vogt F, Fischlein F. Left ventricular mass regression after sutureless implantation of the perceval S aortic valve bioprosthesis: preliminary results. Interact Cardiovasc Thorac Surg. (2014) 18:38–42. doi: 10.1093/icvts/ivt362
46. Santarpino G, Pfeiffer S, Fischlein T. Perceval sutureless approach in a patient with porcelain aorta unsuitable for transcatheter aortic valve implantation. Int J Cardiol. (2012) 155:168–70. doi: 10.1016/j.ijcard.2011.09.025
47. Gatti G, Benussi B, Camerini F, Pappalardo A. Aortic valve replacement within an unexpected porcelain aorta: the sutureless valve option. Interact Cardiovasc Thorac Surg. (2014) 18:396–8. doi: 10.1093/icvts/ivt494
48. Shrestha M, Fischlein T, Meuris B, Flameng W, Carrel T, Madonna F, et al. European multicentre experience with the sutureless Perceval valve: clinical and haemodynamic outcomes up to 5 years in over 700 patients. Eur J Cardiothorac Surg. (2016) 49:234–41. doi: 10.1093/ejcts/ezv040
49. Phan K, Tsai Y, Ninjaran N, Bouchard D, Carrel T, Dapunt O, et al. Sutureless aortic valve replacement: a systematic review and meta-analysis. Ann Cardiothorac Surg. (2015) 4:100–11. doi: 10.3978/j.issn.2225-319X.2014.06.01
50. Mork C, Koechlin L, Schaeffer T, Eckstein F, Ruthebuch O. Long-term follow-up after sutureless Perceval S valve implantation as bail-out strategy in a hostile environment. Cardiovasc Med. (2020) 23:w02093. doi: 10.4414/cvm.2020.02093
51. Meco M, Montisci A, Miceli A, Panisi P, Donatelli F, Cirri D, et al. The Perceval valve is a supportive option for high-risk patients and for those at risk of patient–prosthesis mismatch. Sutureless perceval aortic valve vs. conventional stented bioprostheses: meta-analysis of postoperative and midterm results in isolated aortic valve replacement. J Am Heart Assoc. (2018) 7:e006091. doi: 10.1161/JAHA.117.006091
52. Genereux P, Head SJ, Hahn R, Deneault B, Kodali S, Williams MR, et al. Paravalvular leak after transcatheter aortic valve replacement: the new Achilles' heel? a comprehensive review of the literature. J Am Coll Cardiol. (2013) 61:1125–36. doi: 10.1016/j.jacc.2012.08.1039
Keywords: benefits, pitfalls, Perceval, sutureless, review, sutureless valve replacement
Citation: Dokollari A, Ramlawi B, Torregrossa G, Sá MP, Sicouri S, Prifti E, Gelsomino S and Bonacchi M (2022) Benefits and Pitfalls of the Perceval Sutureless Bioprosthesis. Front. Cardiovasc. Med. 8:789392. doi: 10.3389/fcvm.2021.789392
Received: 04 October 2021; Accepted: 29 November 2021;
Published: 05 January 2022.
Edited by:
Hendrik Tevaearai Stahel, Bern University Hospital, SwitzerlandReviewed by:
Giuseppe Santarpino, Nürnberg Hospital, GermanyAntonio Lio, San Camillo-Forlanini Hospital, Italy
Copyright © 2022 Dokollari, Ramlawi, Torregrossa, Sá, Sicouri, Prifti, Gelsomino and Bonacchi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Massimo Bonacchi, bWJvbmFjY2hpQHVuaWZpLml0