
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Cardiovasc. Med., 11 October 2021
Sec. Heart Failure and Transplantation
Volume 8 - 2021 | https://doi.org/10.3389/fcvm.2021.738496
 Stefan Andrei1,2*Maxime Nguyen1,3Vivien Berthoud1Marie-Catherine Morgant4Belaid Bouhemad1,3Pierre-Grégoire Guinot1,3 and the ECMORIX Study Group
Stefan Andrei1,2*Maxime Nguyen1,3Vivien Berthoud1Marie-Catherine Morgant4Belaid Bouhemad1,3Pierre-Grégoire Guinot1,3 and the ECMORIX Study GroupBackground: Veno-arterial extracorporeal membrane oxygenation (VA-ECMO) is the rescue treatment proposed to patients with refractory cardiogenic shock. The VA-ECMO implantation promotes inflammation and ischemia-reperfusion injuries through the VA-ECMO flow, causing digestive mucosa barrier disrupture and inducing translocation of bacterial wall components—Lipopolysaccharides (LPS) with further inflammation and circulatory impairment. LPS is a well-studied surrogate indicator of bacterial translocation. Oxiris membrane is a promising and well-tolerated device that can specifically remove LPS. The main study aim is to compare the LPS elimination capacity of Oxiris membrane vs. a non-absorbant classical renal replacement (RRT) membrane in patients with cardiogenic shock requiring VA-ECMO.
Methods: ECMORIX is a randomized, prospective, single-center, single-blind, parallel-group, controlled study. It compares the treatment with Oxiris membrane vs. the standard continuous renal replacement therapy care in patients with cardiogenic shock support by peripheral VA-ECMO. Forty patients will be enrolled in both treatment groups. The primary endpoint is the value of LPS serum levels after 24 h of treatment. LPS serum levels will be monitored during the first 72 h of treatment, as clinical and cardiac ultrasound parameters, biological markers of inflammation and 30-day mortality.
Discussion: Oxiris membrane appears to be beneficial in controlling the VA-ECMO-induced ischemia-reperfusion inflammation by LPS removal. ECMORIX results will be of major importance in the management of severe cases requiring VA-ECMO and will bring pathophysiological insights about the LPS role in this context.
Clinical Trial Registration: www.ClinicalTrials.gov, identifier: NCT04886180.
Cardiogenic shock is associated with high morbidity and mortality due to impaired tissue perfusion (1). Approximately, 10% of the patients with refractory shock to medical treatment require circulatory support (2). In this case, veno-arterial extracorporeal membrane oxygenation (VA-ECMO) is the bridge-to-recovery treatment of choice. Despite VA-ECMO support, patients with cardiogenic shock have high morbidity and mortality (≥50%) (3). Morbidity and mortality are due to several interconnected mechanisms: tissue hypoperfusion, ischemia-reperfusion phenomenon, and systemic inflammatory response following the cardiogenic shock and VA-ECMO implantation (4–7). These conditions are responsible for multiple organ failure (MOF) and death (1, 8).
The digestive tract mucosa barrier function is affected during the ischemia-reperfusion phase, being a catalyst for systemic inflammation and MOF progression (9, 10). Lipopolysaccharides (LPS) are bacterial wall components that can be found in the intestinal lumen. From animal model and human neonates' studies, it was demonstrated that ECMO-related SIRS may disrupt the intestinal mucosa (11–13), favoring LPS translocation into the plasmatic sector (8, 10, 14). Acute ischemic heart failure also induces intestinal hypoperfusion and intestinal mucosal injury thus LPS translocation (14). LPS translocation promotes systemic inflammation through the activation of toll-like receptors, then it worsens vasoplegia and MOF with further mucosal barrier disruptions entering a positive feedback loop (15). Systemic inflammation with LPS translocation and digestive barrier disruption plays a pivotal role in patient's evolution to MOF and death (12).
The Oxiris filter set has a 3-layer structure with a polyethyleneimine surface-treated and heparin-coated enhanced AN-69 membrane. This particular structure allows for several cytokines and LPS elimination (16). In vitro and human studies demonstrated that LPS adsorption decrease the cytokine, systemic inflammation, vasoplegia, with less harmful adverse effects on splanchnic perfusion (16, 17). Furthermore, Oxiris membrane may not be associated with more complications than the usual continuous venovenous hemofiltration membrane (17). The ability of the Oxiris membrane to eliminate cytokine and bind LPS suggests that it might be a potential candidate to control the magnitude of the ischemia-reperfusion-induced inflammation, in order to impair the bacterial translocation and progression to MOF. To our knowledge, there is no published or ongoing clinical trial evaluating the Oxiris membrane in patients with cardiogenic shock support by VA-ECMO.
Our hypothesis is that the early treatment by the Oxiris membrane in patients with cardiogenic shock support by VA-ECMO would allow the removal of LPS and pro-inflammatory cytokines, thus controlling systemic inflammation, vasoplegia, MOF, and death.
ECMORIX is a randomized, prospective, single-center, single-blind, parallel-group, controlled study. It compares the Oxiris membrane vs. the standard RRT care in patients with cardiogenic shock support by VA-ECMO. The study was approved by an independent ethics committee (Ethics Committee No. 2-21-005 id11120, French CPP Sud-Ouest et Outre-Mer 2) and was registered on Clinicaltrials.gov (NCT04886180). The study is conducted at the cardio-vascular ICU of the university-affiliated tertiary hospital of Dijon, France. All patients or their next of kin received written information about the study and gave their written consent to participate. The study design adheres to the requirements of the Medical Research Involving Human Subjects Act and of the Declaration of Helsinki.
The Standard Protocol Items: the study follows the SPIRIT Recommendations for Interventional Trials, and the SPIRIT protocol chronology is presented in Table 1. The first patient was included in May 2021, and the last patient follow-up is planned for June 2024.
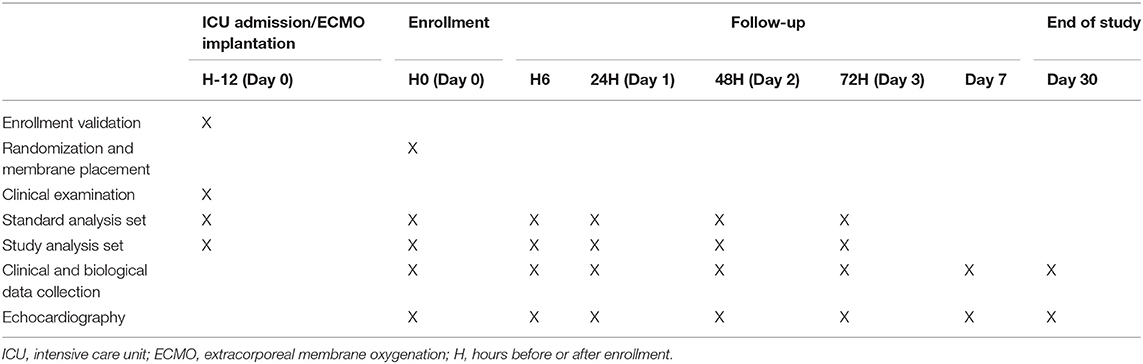
Table 1. Protocol chronology of the study.
Adult patients are considered for enrolment if they have cardiogenic shock support by VA-ECMO, with an indication for renal replacement therapy (RRT). The inclusion, non-inclusion and exclusion criteria are provided in Table 2.
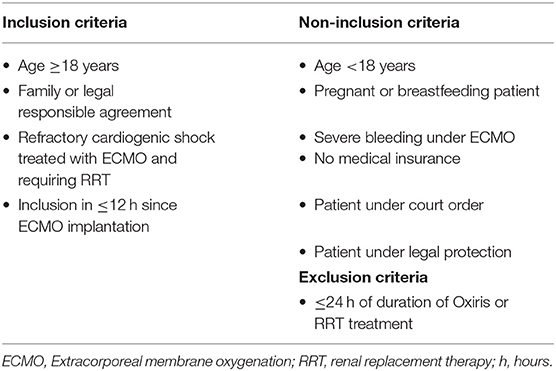
Table 2. Inclusion, non-inclusion and exclusion criteria of the study.
All patients are treated with peripheral venous-arterial femoro-femoral ECMO. Care for patients supported by VA-ECMO is standardized, as previously described (18, 19), and follow patients care practice ESLO guidelines1.
Enteral nutrition is started within 24 h of ECMO starting after obtaining hemodynamic stabilization. The enteral nutrition rate follows international guidelines (20). The feeding dose and flow rate is progressively increase on several days (20).
The study treatment consists of either continuous RRT using the Oxiris membrane or an ST150 PrismaFlex membrane for 72 h, respecting the randomization. The continuous RRT is initiated and managed according to the usual practice, only the type of RRT filter membrane is different. The RRT is standardized to continuous veno-venous hemofiltration (CVVH), with a patient dose of 30 ml/kg/h, a predilution of 1/3, and a postdilution of 2/3. The blood flow rate is set between 150 and 350 ml/min to obtain a filtration fraction ratio of 20%. Ultrafiltration rate is set according to patient volemia status. For both groups, the RRT system is incorporated to the VA-ECMO system, as part of routinely process in our ICU.
The 1:1 ratio randomization is performed by the investigator after the patient's enrollment, using a dedicated e-platform made with CleanWeb TM. This process is controlled by individual usernames and newly created passwords for each enrollment. A second checkup for the inclusion, non-inclusion and exclusion criteria is done at this point. Technical support is provided by the Research Methodology Support Unit from our university-affiliated hospital, which also keeps a record of the full randomization process.
The primary objective is to compare the LPS concentration at 24 h between Oxiris membrane vs. a non-absorbent classical membrane (ST150) in patients with cardiogenic shock support by VA-ECMO.
The secondary objectives are (1) to evaluate the effect of Oxiris membrane treatment on the severity of vasoplegic circulatory failure assessed by the vasoactive-inotropic score (VIS); (2) to evaluate the effect of Oxiris membrane treatment on organ failure using the Sequential organ failure assessment (SOFA) score; (3) to evaluate the effect of Oxiris membrane treatment on inflammation and digestive tract barrier disruptor; (4) to describe the Oxiris membrane LPS elimination kinetic profile; (5) to evaluate the Oxiris membrane treatment on the intensive care unit (ICU) length of stay and 30-day mortality.
The primary endpoint is the LPS serum level after 24 h of continuous RRT with Oxiris membrane.
The secondary endpoints are: (1) the VIS score [defined using the formula: Dopamine infusion rate (mcg/kg/min) + Dobutamine infusion rate (mcg/kg/min) + 100 x Epinephrine infusion rate (mcg/kg/min) + 10 x Milrinone infusion rate (mcg/kg/min) + 10,000 x Vasopressin infusion rate (units/kg/min) + 100 x Norepinephrine infusion rate (mcg/kg/min)]; (2) the SOFA score at day 1, 2, 3 and 7; (3) Serum levels kinetic of cytokines (IL1, IL6, IL 4, IL10, TNF-alpha, interferon gamma, MCP1), CRP, procalcitonin, I-FABP, GLP-1, zonuline, citrulline from RRT initiation, to 6 h after initiation, day 1, day 2, and day 3 of treatment; (4) LPS plasma concentration, (5), ICU length of stay and 30-day mortality. Patients' follow-up is 30 days after initiation of VA-ECMO.
Serial standard usual blood analysis set is drawn at several time points: at the enrollment moment (before RRT membrane placement), after 6, 24, 48, and 72 h of continuous RRT. The study-specific blood analyses are performed at the same time moments. The reference time (T0) is the start of RRT for all group (control and intervention).
At each time point, one EDTA tube of 5 ml is taken via the arterial catheter, and 2 sets of EDTA tubes of 5 ml and are taken on the RRT circuit (one before and one after the filter membrane).
All data will be collected by a non-managing investigator blind to treatment therapy. All analyzes will be performed blind to treatment therapy.
Data will be collected and recorded on eCRF. All patient-related data are anonymously and numerically coded.
Data are as follows: age, sex, weight, SOFA score, SAPS II score, hospital and ICU admission reason, past medical history, comorbidities, VIS score, sedation drugs (type and infusion rate), hourly urinary output, amount of fluid, fluid balance, respiratory parameters (tidal volume, respiratory rate, positive end-expiratory pressure, inspiratory O2 fraction, plateau pressure), enteral nutrition (flow rate and kcal/kg/d), hemodynamic (heart rate, arterial blood pressure, pulse pressure), transthoracic echocardiographic evaluation, VA-ECMO parameters [flow rate, FmO2, O2 flow rate (l /min)].
All patients treated with VA-ECMO have daily transthoracic echocardiography until ECMO withdraw. Cardiac echocardiographic parameters are anonymously recorded at each time points and analyzed in a second time by an investigator non-involved in the patient's clinical management and blind to allocation treatment. Echocardiography is performed by an investigator with cardiac ultrasound certificate. Echocardiography parameters are: right and left cardiac chamber size, right and left systolic cardiac function, left and right diastolic parameters (mitral inflow, mitral annular velocities, tricuspid inflow, tricuspid annular velocities), cardiac output, inferior vena cava diameter, portal flow. The analysis will be performed offline in a simple blind manner.
Adverse events will be recorded in detail during both the follow-up periods. The reporting and documentation of adverse events will be classified as IMT-related or non-IMT-related. This safety analysis will be conducted at the end of our research.
Based on a LPS mean value of 110 ± 40 pmol/l (21), 34 patients should be randomized, 17 in each treatment arm will be necessary to demonstrate a decrease over 35% (16), with a bilateral alpha risk of 5% and a power of 80%. Assuming that 15% of patients would not be evaluable due to early death, we fixed the sample size to 40 patients, 20 patients in each treatment arm.
The data will be analyzed in intention-to-treat and per-protocol. The variables will be presented as mean ± SD, or as median [25–75% IQR], as appropriate. The treatment groups will be presented comparatively after the randomization. The qualitative variables will be compared using the Chi-square test or Fisher's exact test. The quantitative variables will be compared using the Student's test or a non-parametric test, as appropriate. Longitudinal data will be processed using mixed-models. The normality will be checked graphically, with histograms and QQ plots and using the Shapiro-Wilk normality test.
The evaluation of the primary endpoint will be considered as a comparison of means. The statistical analysis will be performed using R Studio software. A p < 0.05 will be considered statistically significant.
The results of this study will bring insights into the potential use of the Oxiris membrane in managing cardiogenic shock supported by VA-ECMO. Furthermore, the particular focus on the LPS serum levels profile will provide a better understanding of the mechanisms of therapeutical benefit of Oxiris membrane.
Blood purifications is a subject of rising interest, and some authors proposed a rationale for blood purifiers use to control VA-ECMO-induced systemic inflammation (22). However, the use of cytokine absorbent filters is still controversial and lacking scientific evidence. The Cytosorb membrane (Cytosorbents, NJ, USA) has been studied in various settings (23–26). The Cytosorb membrane is able to eliminate a large diversity of cytokines, but also other plasmatic molecules like DAMP, PAMP, complement factors (27–29). However, Cytosorb did not improve clinical outcomes when used during the cardio-pulmonary bypass (30). Moreover, in patients suffering of SARS-Cov2 supported by ECMO, Cytosorb was unable to decrease interleukin 6 concentrations, and was associated with higher mortality (31). These findings suggest that inflammation is insufficiently controlled by the Cystosorb membrane and one hypothesis is that an alternative pathway might be involved.
The Oxiris membrane (Baxter Investment Co., Ltd., Shanghai, China) is another adsorbing membrane that has been less studied. One important difference between those 2 membranes is that the Oxiris membrane is able to remove both interleukins and LPS (16, 28). Those properties seem to promote hemodynamic stabilization and even organs failure improvement during states of sepsis-related circulatory failure (17, 32–35). Because LPS might play a pivotal role in enhancing inflammation during the ischemia-reperfusion phase, the additional LPS removal properties of the Oxiris membrane by reducing the triggering of the TLR-4 pathway could provide a clinical benefit. As this clinical benefit has not yet been demonstrated in our population those hypotheses remain speculative and randomized trials are needed to provide robust answers.
Indeed, the literature on the subject is parse and mainly performed in human neonates or animals with immature gastrointestinal tract and/or different immune system (7, 11). No study has evaluated the effect of retrograde VA-ECMO flow on intestinal perfusion and intestinal barrier. Despite cardiogenic shock is associated with intestinal translocation and high level of LPS, few studies have demonstrated this point in cardiogenic shock supported with VA-ECMO. In addition, our study doesn't include a control group of cardiogenic shock patients without VA-ECMO support. All these points could be a limit of the study. Nevertheless, by focusing on LPS removal kinetic our study will allow clarifying for the first time whether the Oxiris device lowers the LPS burden in refractory cardiogenic shock supported by ECMO (10–12).
One aspect of particular interest in our population is the predictability of the timing of the injury that allows early treatment before the irreversible consequences of ischemia-reperfusion. This fact represents an advantage comparing to medical conditions-induced cytokine storm. Nevertheless, the right initiation timing during VA-ECMO is debatable and to be determined (22). One should also consider the more extensive ICU discussion about the adequate RRT initiation moment (29). We chose to enroll the patients no later than 12 h after VA-ECMO implantation in order to anticipate the irreversibility of ischemia-reperfusion injury.
The adding of an extracorporeal circuit seems to be clinically tolerated, but it is difficult to propose it for patients who do not need RRT. Because Oxiris membrane is used on VA-ECMO, RRT blood flow rate may be low and the LPS clearance rate may be insufficient. Broman et al. demonstrated that RRT with a mean blood flow rate of 132 ± 69 ml min−1 is able to significantly decrease endotoxin level (17). This blood flow rate is below the blood flow rate in our study. The main concern is the risk of hemorrhage due to vascular access, extracorporeal-induced coagulopathy, and the immune reactions to the heparin-coated circuit. Regarding this concern, the patients on VA-ECMO are already at risk with a larger extracorporeal circuit, large cannulae for vascular access and already on heparin anticoagulation. The addition of the RRT circuit can be performed on the VA-ECMO circuit, as already shown (36).
In conclusion, the study results will be of significant importance in the management of refractory cardiogenic shock support by VA-ECMO, and will bring pathophysiological insights about the intestinal barrier and LPS role in this context.
The studies involving human participants were reviewed and approved by Ethics Committee French CPP Sud-Ouest et Outre-Mer 2, No. 2-21-005 id11120. The patients/participants provided their written informed consent to participate in this study.
P-GG, MN, and VB contributed to the conception and design. P-GG, MN, SA, and M-CM searched the associated data. SA, MN, and P-GG drafted the manuscript. BB provided the supervision support. MN performed data analysis. All authors contributed to the critical revisions and final approval of the manuscript.
The authors performed this study in the course of their normal duties as full-time employees of public healthcare institutions.
Audrey Martin, Mohamed Radhouani, Tiberiu Constandache, Sandrine Grosjean, Pierre Voizeux, Emel Rafrafi, Chloe Bernard, Saed Jazayeri, Ghislain Malapert, Olivier Bouchot.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Vahdatpour C, Collins D, Goldberg S. Cardiogenic shock. J Am Heart Assoc. (2019) 8:e011991. doi: 10.1161/JAHA.119.011991
2. Hamm CW, Bassand JP, Agewall S, Bax J, Boersma E, Bueno H, et al. ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: the Task Force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. (2011) 32:2999–3054. doi: 10.1093/eurheartj/ehr236
3. Kolte D, Khera S, Aronow WS, Mujib M, Palaniswamy C, Sule S, et al. Trends in incidence, management, and outcomes of cardiogenic shock complicating ST-elevation myocardial infarction in the United States. J Am Heart Assoc. (2014) 3:e000590. doi: 10.1161/JAHA.113.000590
4. Debrunner M, Schuiki E, Minder E, Straumann E, Naegeli B, Mury R, et al. Proinflammatory cytokines in acute myocardial infarction with and without cardiogenic shock. Clin Res Cardiol. (2008) 97:298–305. doi: 10.1007/s00392-007-0626-5
5. Prondzinsky R, Unverzagt S, Lemm H, Wegener N, Heinroth K, Buerke U, et al. Acute myocardial infarction and cardiogenic shock: prognostic impact of cytokines: INF-γ, TNF-α, MIP-1β, G-CSF, and MCP-1β. Medizinische Klinik Intensivmedizin Notfallmedizin. (2012) 107:476–84. doi: 10.1007/s00063-012-0117-y
6. Jentzer JC, Lawler PR, van Diepen S, Henry TD, Menon V, Baran DA, et al. Systemic inflammatory response syndrome is associated with increased mortality across the spectrum of shock severity in cardiac intensive care patients. Circulation. (2020) 13:e006956. doi: 10.1161/CIRCOUTCOMES.120.006956
7. Millar JE, Fanning JP, McDonald CI, McAuley DF, Fraser JF. The inflammatory response to extracorporeal membrane oxygenation (ECMO): a review of the pathophysiology. Crit Care. (2016) 20:387. doi: 10.1186/s13054-016-1570-4
8. Al-Fares A, Pettenuzzo T, Del Sorbo L. Extracorporeal life support and systemic inflammation. Intens Care Med Exp. (2019) 7(Suppl 1):46. doi: 10.1186/s40635-019-0249-y
9. de Jong PR, González-Navajas JM, Jansen NJ. The digestive tract as the origin of systemic inflammation. Crit Care. (2016) 20:279. doi: 10.1186/s13054-016-1458-3
10. Brunkhorst FM, Clark AL, Forycki ZF, Anker SD. Pyrexia, procalcitonin, immune activation and survival in cardiogenic shock: the potential importance of bacterial translocation. Int J Cardiol. (1999) 72:3–10. doi: 10.1016/S0167-5273(99)00118-7
11. Kurundkar AR, Killingsworth CR, McIlwain RB, Timpa JG, Hartman YE, He D, et al. Extracorporeal membrane oxygenation causes loss of intestinal epithelial barrier in the newborn piglet. Pediatr Res. (2010) 68:128–33. doi: 10.1203/PDR.0b013e3181e4c9f8
12. McILwain RB, Timpa JG, Kurundkar AR, Holt DW, Kelly DR, Hartman YE, et al. Plasma concentrations of inflammatory cytokines rise rapidly during ECMO-related SIRS due to the release of preformed stores in the intestine. Lab Investig. (2010) 90:128–39. doi: 10.1038/labinvest.2009.119
13. MohanKumar K, Killingsworth CR, McIlwain RB, Timpa JG, Jagadeeswaran R, Namachivayam K, et al. Intestinal epithelial apoptosis initiates gut mucosal injury during extracorporeal membrane oxygenation in the newborn piglet. Lab Investig. (2014) 94:150–60. doi: 10.1038/labinvest.2013.149
14. Zhou X, Li J, Guo J, Geng B, Ji W, Zhao Q, et al. Gut-dependent microbial translocation induces inflammation and cardiovascular events after ST-elevation myocardial infarction. Microbiome. (2018) 6:66. doi: 10.1186/s40168-018-0441-4
15. Lu YC, Yeh WC, Ohashi PS. LPS/TLR4 signal transduction pathway. Cytokine. (2008) 42:145–51. doi: 10.1016/j.cyto.2008.01.006
16. Malard B, Lambert C, Kellum JA. In vitro comparison of the adsorption of inflammatory mediators by blood purification devices. Intens Care Med Exp. (2018) 6:12. doi: 10.1186/s40635-018-0177-2
17. Broman ME, Hansson F, Vincent JL, Bodelsson M. Endotoxin and cytokine reducing properties of the oXiris membrane in patients with septic shock: a randomized crossover double-blind study. PLoS ONE. (2019) 14:e0220444. doi: 10.1371/journal.pone.0220444
18. Ellouze O, Soudry Faure A, Radhouani M, Abou-Arab O, Besnier E, Moussa M, et al. Levosimendan in venoarterial ECMO weaning. Rational and design of a randomized double blind multicentre trial. ESC Heart Failure. (2021) 8:3339–47. doi: 10.1002/ehf2.13427
19. Ellouze O, Lamirel J, Perrot J, Missaoui A, Daily T, Aho S, et al. Extubation of patients undergoing extracorporeal life support. A retrospective study. Perfusion. (2019) 34:50–7. doi: 10.1177/0267659118791072
20. Reintam Blaser A, Starkopf J, Alhazzani W, Berger MM, Casaer MP, Deane AM, et al. Early enteral nutrition in critically ill patients: ESICM clinical practice guidelines. Intens Care Med. (2017) 43:380–98. doi: 10.1007/s00134-016-4665-0
21. Nguyen M, Tavernier A, Gautier T, Aho S, Morgant MC, Bouhemad B, et al. Glucagon-like peptide-1 is associated with poor clinical outcome, lipopolysaccharide translocation and inflammation in patients undergoing cardiac surgery with cardiopulmonary bypass. Cytokine. (2020) 133:155182. doi: 10.1016/j.cyto.2020.155182
22. Napp LC, Ziegeler S, Kindgen-Milles D. Rationale of hemoadsorption during extracorporeal membrane oxygenation support. Blood Purif. (2019) 48:203–14. doi: 10.1159/000500015
23. Zuccari S, Damiani E, Domizi R, Scorcella C, D'Arezzo M, Carsetti A, et al. Changes in cytokines, haemodynamics and microcirculation in patients with sepsis/septic shock undergoing continuous renal replacement therapy and blood purification with cytosorb. Blood Purif. (2020) 49:107–13. doi: 10.1159/000502540
24. Huber W, Algül H, Lahmer T, Mayr U, Lehmann M, Schmid RM, et al. Pancreatitis cytosorbents (CytoSorb) inflammatory cytokine removal: a prospective study (PACIFIC). Medicine. (2019) 98:e13044. doi: 10.1097/MD.0000000000013044
25. Scharf C, Liebchen U, Paal M, Irlbeck M, Zoller M, Schroeder I. Blood purification with a cytokine adsorber for the elimination of myoglobin in critically ill patients with severe rhabdomyolysis. Crit Care. (2021) 25:41. doi: 10.1186/s13054-021-03468-x
26. Tomescu D, Popescu M, David C, Sima R, Dima S. Haemoadsorption by CytoSorb® in patients with acute liver failure: a case series. Int J Artif Organs. (2020) 44:560–64. doi: 10.1177/0391398820981383
27. Zhang L, Feng Y, Fu P. Blood purification for sepsis: an overview. Precis Clin Med. (2021) 4:45–55. doi: 10.1093/pcmedi/pbab005
28. Monard C, Rimmelé T, Ronco C. Extracorporeal blood purification therapies for sepsis. Blood Purif. (2019) 47(Suppl. 3):1–14. doi: 10.1159/000499786
29. Harm S, Schildböck C, Hartmann J. Cytokine removal in extracorporeal blood purification: an in vitro study. Blood Purif. (2020) 49:33–43. doi: 10.1159/000502680
30. Poli EC, Alberio L, Bauer-Doerries A, Marcucci C, Roumy A, Kirsch M, et al. Cytokine clearance with CytoSorb® during cardiac surgery: a pilot randomized controlled trial. Crit Care. (2019) 23:108. doi: 10.1186/s13054-019-2399-4
31. Supady A, Weber E, Rieder M, Lother A, Niklaus T, Zahn T, et al. Cytokine adsorption in patients with severe COVID-19 pneumonia requiring extracorporeal membrane oxygenation (CYCOV): a single centre, open-label, randomised, controlled trial. Lancet Respirat Med. (2021) 9:755–62. doi: 10.1016/S2213-2600(21)00177-6
32. Turani F, Barchetta R, Falco M, Busatti S, Weltert L. Continuous renal replacement therapy with the adsorbing filter oxiris in septic patients: a case series. Blood Purif. (2019) 47(Suppl. 3):1–5. doi: 10.1159/000499589
33. Zhang H, Zhu G, Yan L, Lu Y, Fang Q, Shao F. The absorbing filter Oxiris in severe coronavirus disease 2019 patients: a case series. Artif Organs. (2020) 44:1296–302. doi: 10.1111/aor.13786
34. Samman KN, Baalbaki H, Bouchard J, Albert M. Continuous renal replacement therapy with oXiris® membrane in severe ebstein-barr virus-mediated hemophagocytic lymphohistiocytosis: a case report. Blood Purif. (2020) 50:578–81. doi: 10.1159/000511724
35. Zhai Y, Pan J, Zhang C. The application value of oXiris-endotoxin adsorption in sepsis. Am J Transl Res. (2021) 13:3839–44.
Keywords: cardiogenic shock, heart failure, extracorporeal membrane oxygenation, artificial membrane, oxiris, endotoxin/blood, cytokines/blood, continuous renal replacement therapy
Citation: Andrei S, Nguyen M, Berthoud V, Morgant M-C, Bouhemad B, Guinot P-G and the ECMORIX Study Group (2021) Evaluation of the Oxiris Membrane in Cardiogenic Shock Requiring Extracorporeal Membrane Oxygenation Support: Study Protocol for a Single Center, Single-Blind, Randomized Controlled Trial. Front. Cardiovasc. Med. 8:738496. doi: 10.3389/fcvm.2021.738496
Received: 08 July 2021; Accepted: 20 September 2021;
Published: 11 October 2021.
Edited by:
Kiyotake Ishikawa, Icahn School of Medicine at Mount Sinai, United StatesReviewed by:
Warwick Wolf Butt, Royal Children's Hospital, AustraliaCopyright © 2021 Andrei, Nguyen, Berthoud, Morgant, Bouhemad, Guinot and the ECMORIX Study Group. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stefan Andrei, stefanmandrei@gmail.com
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.