 Min Shen
Min Shen Jinke Huang3
Jinke Huang3 Tao Qiu
Tao Qiu- 1Department of Neurology, The First Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, China
- 2Department of Neurology, The First Affiliated Rehabilitation Hospital of Zhejiang Chinese Medical University, Hangzhou, China
- 3Xiyuan Hospital, China Academy of Chinese Medical Science, Beijing, China
Background: To systematically appraise and synthesize evidence, we conducted an overview of systematic reviews/meta-analyses (SRs/MAs) on acupuncture for stable angina pectoris (SAP).
Methods: Eight databases were searched for SRs/MAs of acupuncture on SAP. The methodological quality, reporting quality, and evidence quality were evaluated by Assessing the Methodological Quality of Systematic Reviews 2 (AMSTAR-2), the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist, and the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system, respectively.
Results: A total of seven published SRs/MAs met the inclusion criteria. According to the evaluation results of AMSTAR-2, two studies were considered as of moderate quality; the remaining five were considered as of very low quality. According to the evaluation results of the PRISMA checklist, only one study reported the checklist in its entirety, while others had reporting deficiencies. According to GRADE, a total of 18 outcome indicators extracted from the included studies were evaluated. The evidence quality was very low in three, low in three, moderate in eight, and high in four.
Conclusion: Acupuncture may be beneficial for SAP from the currently published evidence. However, this conclusion must be interpreted cautiously due to the generally low methodological quality, reporting quality, and evidence quality of the included studies. More rigorous, more standardized and comprehensive SRs/MAs are needed to provide strong evidence for convincing conclusions.
Introduction
Stable angina pectoris (SAP) is a highly prevalent ischemic cardiovascular disease characterized by left anterior chest pain or discomfort in adjacent areas (1). SAP has become a public health concern worldwide, which affects more than 560,000 individuals per year in America (2). In most European countries, the prevalence of SAP is estimated to be 20,000–40,000 people per million (3). In China, the incidence of SAP is estimated to be 2.4% in men and 3.2% in women (4). Antiplatelet drugs, nitrates, statins, and β-receptor blockers as anti-ischemic treatments are recommended by guidelines as conventional medication (CM) for SAP (5). Despite optimal medical treatment, recurrent angina pectoris is not rare. Thus, patients with SAP resort to complementary and alternative medicine for symptom relief.
Acupuncture, as an important component of traditional Chinese medicine, has been reported to treat cardiovascular diseases, including heart failure (6) and angina (7). According to the reports of published systematic reviews/meta-analyses (SRs/MAs), acupuncture may benefit patients with SAP (8–14). However, the conclusions of these studies regarding the effectiveness of acupuncture in relieving angina symptoms or reducing angina frequency in patients with SAP are not always consistent. To systematically appraise and synthesize these results, we conducted an overview of SRs/MAs. This overview also intended to identify the deficiencies and provide recommendations for achieving high-quality SRs/MAs.
Methods
Study Registration
We have registered this overview under the PROSPERO registry (CRD42020188107). The methodology followed the guidelines stated in the Cochrane Handbook, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist (15), and some high-quality methodological overviews (16, 17).
Criteria for Inclusion
Type of Study
This overview only included SRs/MAs of randomized controlled trials (RCTs) on acupuncture for SAP.
Type of Subjects
Subjects diagnosed with SAP according to national or international criteria, regardless of age, race, or sex, were included.
Type of Interventions
The intervention method in the experimental group was acupuncture or acupuncture plus conventional medication (e.g., antiplatelet drugs, statins, β-receptor blockers, and nitrates). The intervention method in the control group was CM.
Types of Outcome Measurements
The following are the outcome measurements: frequency, intensity of angina, number of patients with changes on the electrocardiogramme (ECG), effective rate, adverse events, and nitroglycerin use.
Search Methods for Identification of Studies
PubMed, Cochrane Library, Embase, Web of Science, China National Knowledge Infrastructure, Wanfang database, Chinese Biomedical Literature database, and the Chinese Science Journals Database were searched from their inception to December 2020. The following keywords were used in the search: angina pectoris, acupuncture, systematic review, and meta-analysis. The search strategy for PubMed is shown in Table 1.
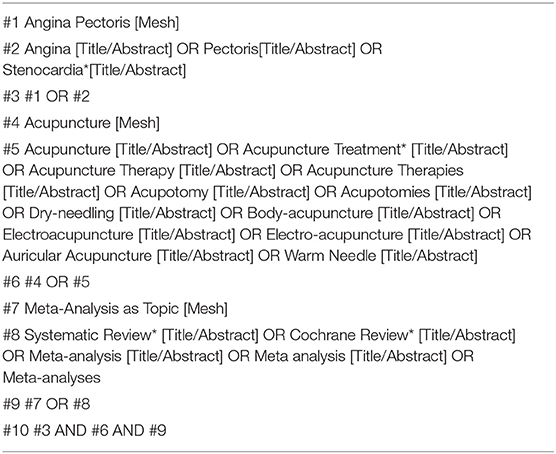
Table 1. The search strategy for Pubmed.
Study Selection and Data Extraction
Two independent reviewers assessed the literature for inclusion and abstracted the data based on details. Any disagreements were resolved by consensus through discussion. The following details were extracted: author(s), publication year, simple size, interventions, outcomes relevant to this overview, quality assessment methods, and the summary estimate of the intervention effects.
Evaluation of the Methodological Quality of the Included Studies
Two independent reviewers assessed the methodological quality of the included studies using Assessing the Methodological Quality of Systematic Reviews 2 (AMSTAR-2) (18). According to the information provided in the included studies, each of the 16 standards of AMSTAR-2 is given a rating of “Yes,” “No,” or “Partial Yes.” Any disagreements were resolved by consensus through discussion.
Evaluation of the Reporting Quality of the Included Studies
Two independent reviewers assessed the reporting quality of the included studies using the PRISMA checklist (15). According to the information provided in the included studies, each of the items in the PRISMA checklist is given a rating of “Yes,” “No,” or “Partial Yes.” Any disagreements were resolved by consensus through discussion.
Evaluation of the Evidence Quality of the Included Studies
Two reviewers independently assessed the evidence quality using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) (19). Evaluation of the evidence quality mainly considers the following aspects: risk of bias, inconsistency, indirectness, imprecision, and publication bias. Disagreements were resolved by discussion or consensus with a third-party reviewer.
Results
Literature Search
The initial database search yielded 128 potentially relevant published studies; 10 publications were retrieved after reviewing the titles and abstracts. Following the review of full texts, seven published SRs/MAs (8–14) met the inclusion criteria. Figure 1 shows details of the flow diagram.

Figure 1. Flow diagram of the review selection process.
Description of the Included Studies
All included studies were published between 2012 and 2019. Six of the studies were published in English; the rest are in Chinese (8). The number of trials ranged from 4 to 25, and the sample size ranged from 254 to 2,058. The intervention methods were mostly acupuncture therapy plus CM in the experimental group and CM and sham acupuncture in the control group. For the assessment of methodological quality, six studies used the Cochrane criteria and the rest used the Jadad scale (9). Details are presented in Table 2.
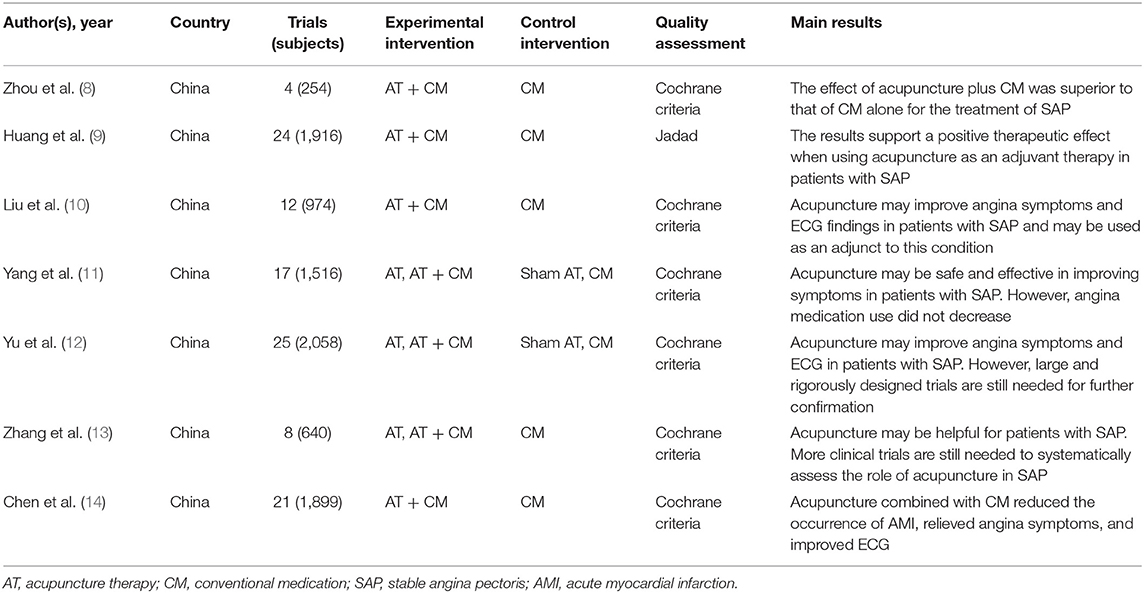
Table 2. Characteristics of the studies.
Methodological Quality of the Included Studies
Among the included studies, two (11, 12) were rated as of moderate quality; the rest were of very low quality. Items 2 and 7 were rated as of particularly low quality. Only two studies (11, 12) established a prior study protocol. No study provided a complete list of excluded studies with reasons or explained the reasons for the selection of study types. Details are shown in Table 3.
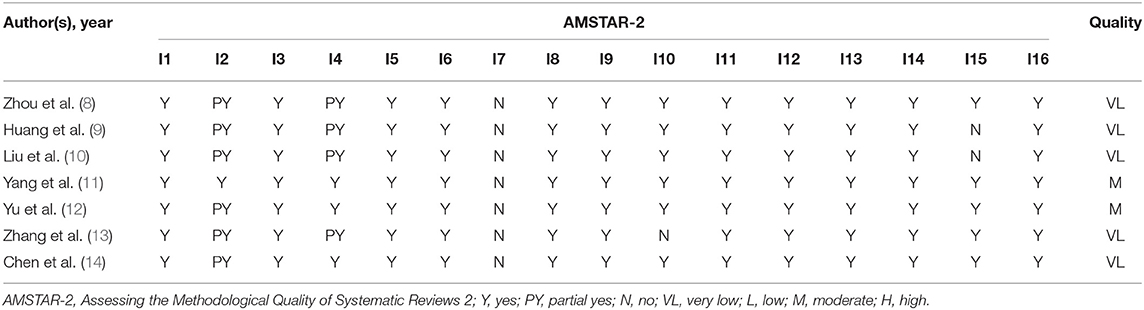
Table 3. Results of the AMSTAR-2 assessment.
Reporting Quality of the Included Studies
With the PRISMA checklist, only one study (11) reported all items in the checklist, while others had reporting deficiencies. The checklist items incomplete reported were mainly Q5 (protocol and registration), Q8 (search), Q16 (additional analyses of methods), and Q23 (additional analyses of results). Details are shown in Table 4.
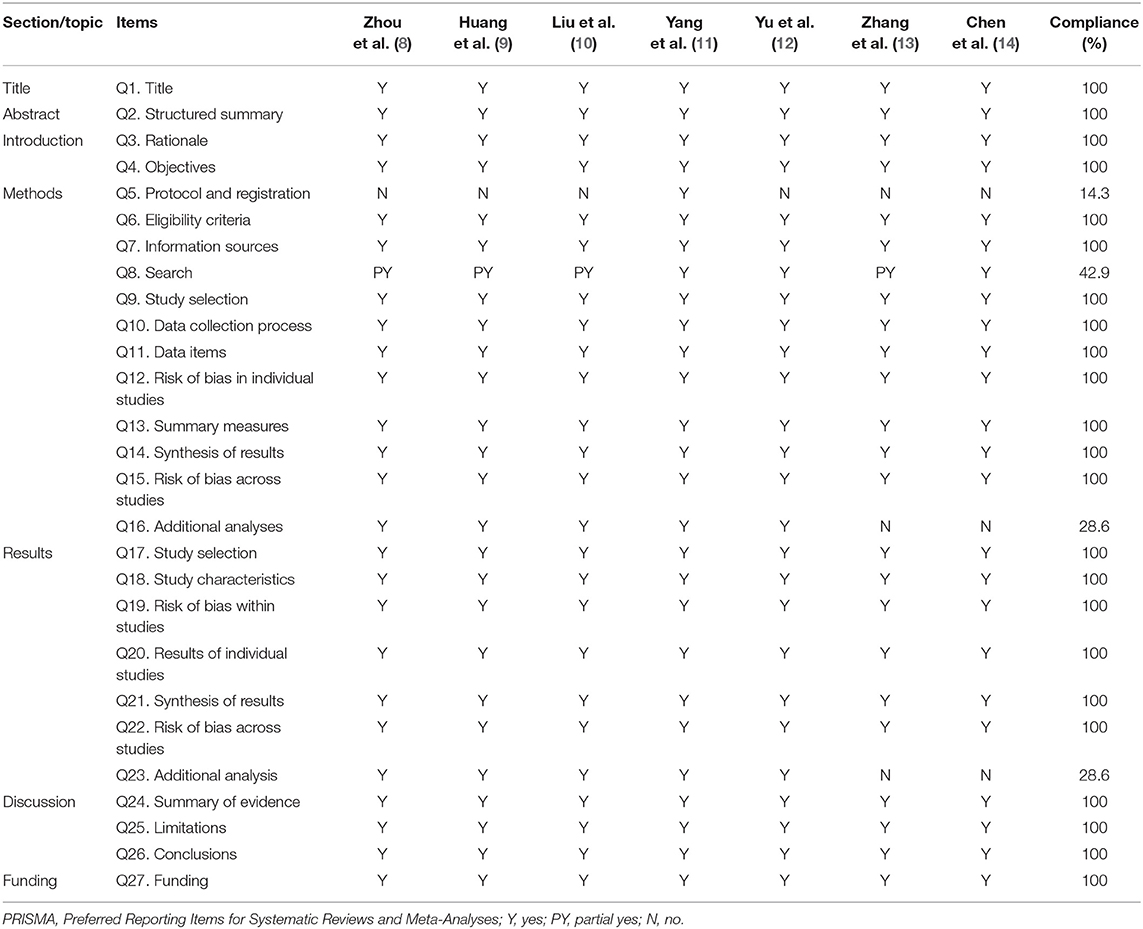
Table 4. Results of the PRISMA checklist.
Evidence Quality of the Included Studies
A total of 18 outcome indicators extracted from the included studies were evaluated; the evidence quality was very low in three, low in three, moderate in eight, and high in four. Risk of bias was the most common downgrading factor, followed by imprecision, inconsistency, publication bias, and indirectness. Details are shown in Table 5.
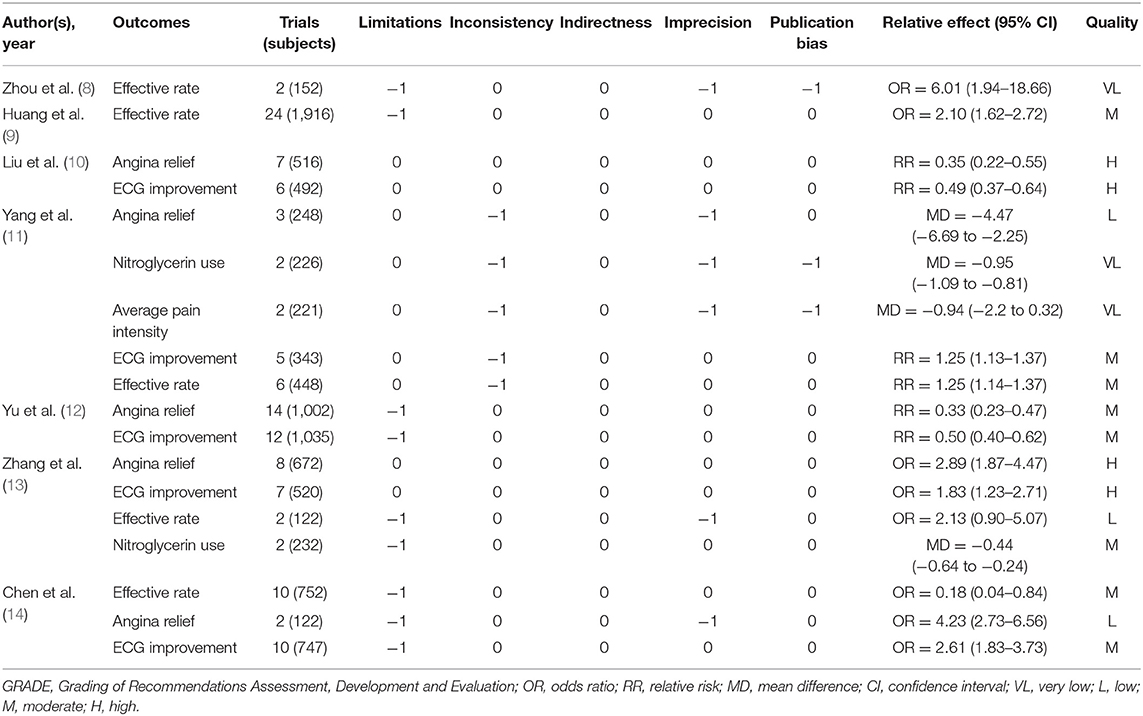
Table 5. Results of GRADE assessment.
Summary of Results of the Included Studies
Efficacy of Acupuncture for SAP
The outcome indicators extracted from the included studies are presented in Table 4. Five studies (10–14) reported the outcome indicator for angina relief; meta-analysis revealed a more significant effect of combination therapy than of CM alone. Five studies (10–14) reported the outcome indicator for ECG improvement; meta-analysis showed a more significant effect of combination therapy. Five studies (10–14) reported the outcome indicator for ECG improvement; meta-analysis revealed a more significant effect of combination therapy. Two studies (11, 13) reported the outcome indicator for nitroglycerin use; meta-analysis showed a more significant effect of acupuncture than of CM. Similarly, one study (11) reported the outcome indicator for average pain intensity; the results revealed a more significant effect of combination therapy. Five studies (8, 9, 11, 13, 14) reported the outcome indicator for effective rate; meta-analysis revealed a more significant effect of acupuncture in four studies. However, another study (13) reported no significant difference.
Safety of Acupuncture for SAP
Adverse events were mentioned in five studies (10–14), and no adverse effects related to acupuncture were reported.
Discussion
SRs/MAs are regarded as the gold standard for assessing the effects of an intervention. Despite the strengths of SRs/MAs, bias may arise in the implementation process. An increasing number of SRs/MAs have begun to investigate the effectiveness of acupuncture for SAP. Under the circumstances, to systematically appraise and synthesize these results, we performed this overview.
Summary of Quality
Through a comprehensive search, seven SRs/MAs on the effectiveness of acupuncture for SAP were identified. According to the results of the AMSTAR-2 assessment, only two of which were regarded as of moderate methodological quality; the rest were of very low methodological quality. Items 2 (protocol registration) and 7 (list of excluded studies) were rated as of particularly low quality. In performing SR/MA, a pre-registration protocol is quite essential, which helps to promote processing transparency and avoid methodological bias (20). In this context, registration platforms, such as PROSPERO, have been highlighted and advocated. Therefore, more attention should be paid to registering the work. Future investigators should register protocols in advance, before the SRs/MAs are carried out. For study selection, all the included studies were selected in duplicate, resolving disagreements by discussion or consensus with a third author. However, none of the studies provided a list of excluded trials, which made it difficult to guarantee the reproducibility of the results (21). Similar to the results of the AMSTAR-2 evaluation, assessment using the PRISMA checklist found that only one study (11) reported the checklist in its entirety, while others had reporting deficiencies. Incomplete reports of checklist items were mainly missed information on protocol and registration, literature search, and additional analyses.
The evidence quality was assessed by the GRADE system. Among the 17 outcome indicators, the evidence quality was very low in three, low in three, moderate in eight, and high in four. Risk of bias was the most common downgrading factor, followed by imprecision, inconsistency, publication bias, and indirectness. Through further analysis, it was found that the limitation in this area was mainly due to the inability of acupuncture therapy to blind the implementer. Thus, there are issues that should be paid attention to. With the development of evidence-based acupuncture, it is hoped that researchers will continue to promote standardization of the techniques and operating procedures of acupuncture in the future in order to provide more high-quality evidence.
Of the included studies, it is worth noting that, although almost all indicated that acupuncture is an effective approach in treating SAP, most authors did not want to draw firm conclusions because of the small sample sizes or the low methodological quality of the included studies. Meanwhile, given that the results assessed in this overview suggest that neither the methodological quality of the included studies nor the evidence quality of the reported outcome indicators is satisfactory, we cannot draw firm conclusions regarding acupuncture for SAP based on the currently published evidence. Therefore, in the future, RCTs with adequate blinding and large simple sizes are still needed to determine whether acupuncture or combination therapies are more effective than other treatments. Furthermore, strict adherence to the Cochrane Handbook for the design and implementation of SRs/MAs needs to be encouraged and advocated in order to be able to provide more convincing evidence.
Limitations
To the best of our knowledge, this is the first study using the method of overview to systematically appraise and synthesize evidence of acupuncture for SAP. The results of this overview will be beneficial to evidence users and help researchers improve the quality of their studies. However, limitations should be acknowledged, especially the differences involving populations, interventions, comparators, outcomes, and study designs (PICOS). Firstly, all included SRs/MAs mentioned that the included patients were diagnosed with SAP according to national or international standards. However, only one study (12) mentioned the use of the WHO criteria, while other studies did not account for the specific diagnostic criteria used. Moreover, patients were heterogeneous in terms of age, disease duration, and complications. The above heterogeneity from the patient aspect may affect the credibility of the conclusions. Secondly, some studies have looked at the use of acupuncture to combine other interventions on a control group basis, which is easily mixed with the effects of acupuncture. Thus, experimental measures of acupuncture alone or plus a control group may increase credibility. Thirdly, the diversity of the acupuncture treatment protocols has resulted in heterogeneity, including acupoint selection, stimulation methods, and the frequency of treatment. Although the use of some acupoints was concentrated, the overall differences in the acupuncture treatment regimens in the included studies were large. Moreover, the CM used in the control group was different. This may have caused some deviation. Fourthly, the measurement scales used in the RCTs were subjective clinical assessment tools based on the observations of assessors and may not be accurate for the assessment of treatment effects. The use of effective rate or the number of patients with no improvements in ECG also limited the generalization of the results. A fifth limitation is that, although all SRs/MAs were based on RCTs, inadequate reporting of randomization, allocation concealment, blinding, intention-to-treat analysis, and dropout interpretation in most RCTs may have contributed to the risk of bias. Finally, all the included studies in this overview were performed in China, so whether the conclusions of this study can be generalized to other populations remains to be studied further.
Conclusions
Acupuncture may be beneficial for SAP based on the currently published evidence. However, this conclusion must be interpreted with caution due to the generally low methodological quality, reporting quality, and evidence quality of the included studies. More rigorous, more standardized and comprehensive SRs/MAs are needed to provide strong evidence for convincing conclusions.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Author Contributions
MS and JH wrote the original draft. TQ reviewed and edited the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
SR, systemic review; SAP, stable angina pectoris; MA, meta-analysis; AMSTAR-2, Assessing the Methodological Quality of Systematic Reviews 2; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; GRADE, Grading of Recommendations Assessment Development and Evaluation; RCTs, randomized controlled trials; CM, conventional medication; ECG, electrocardiogram; PICOS, populations, interventions, comparators, outcomes and study designs.
References
1. Kones R. Recent advances in the management of chronic stable angina I: approach to the patient, diagnosis, pathophysiology, risk stratification, gender disparities. Vasc Health Risk Manage. (2010) 6:635. doi: 10.2147/VHRM.S7564
2. Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, et al. Heart disease and stroke statistics−2017 update: a report from the American Heart Association. Circulation. (2017) 135:e146–03. doi: 10.1161/CIR.0000000000000491
3. Authors/Task Force Members, Fox K, Garcia MA, Ardissino D, Buszman P, Camici PG, et al. Guidelines on the management of stable angina pectoris: executive summary: the Task Force on the Management of Stable Angina Pectoris of the European Society of Cardiology. Eur Heart J. (2006) 27:1341–81. doi: 10.1093/eurheartj/ehl001
4. Lam TH, Liu LJ, Janus ED, Lau CP, Hedley AJ. Fibrinogen, angina and coronary heart disease in a Chinese population. Atherosclerosis. (2000) 149:443–9. doi: 10.1016/S0021-9150(99)00347-0
5. Jneid H, Anderson JL, Wright RS, Adams CD, Bridges CR, Casey DE Jr., et al. ACCF/AHA focused update of the guideline for the management of patients with unstable angina/Non-ST-elevation myocardial infarction (updating the 2007 guideline and replacing the 2011 focused update): a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. (2012) 126:875–910. doi: 10.1161/CIR.0b013e318256f1e0
6. Middlekauff HR. Acupuncture in the treatment of heart failure. Cardiol Rev. (2004) 12:171–3. doi: 10.1097/01.crd.0000103650.71735.f0
7. Ballegaard S, Karpatschoff B, Holck JA, Meyer CN, Trojaborg W. Acupuncture in angina pectoris: do psycho-social and neurophysiological factors relate to the effect? Acupunct Electrother Res. (1995) 20:101–16. doi: 10.3727/036012995816357113
8. Zhou JU, Huang We, Deng J, Tang YH. Meta analysis of the therapeutic effect of acupuncture on stable angina pectoris. J Hubei Univ Chin Med. (2018) 20:40–3.
9. Huang X, Guo S, Li F, Tan X, Cai Q, Wang H, et al. Acupuncture as an adjunctive treatment for angina due to coronary artery disease: a meta-analysis. Med Sci Monit. (2019) 25:1263–74. doi: 10.12659/MSM.913379
10. Liu Y, Meng HY, Khurwolah MR, Liu JB, Tang H, Aa N, et al. Acupuncture therapy for the treatment of stable angina pectoris: an updated meta-analysis of randomized controlled trials. Complement Ther Clin Pract. (2019) 34:247–53. doi: 10.1016/j.ctcp.2018.12.012
11. Yang M, Sun M, Du T, Long H, Chen J, Liang F, et al. The efficacy of acupuncture for stable angina pectoris: a systematic review and meta-analysis. Eur J Prev Cardiol. (2019). doi: 10.1177/2047487319876761
12. Yu C, Ji K, Cao H, Wang Y, Jin HH, Zhang Z, et al. Effectiveness of acupuncture for angina pectoris: a systematic review of randomized controlled trials. BMC Complement Altern Med. (2015) 15:90. doi: 10.1186/s12906-015-0586-7
13. Zhang Z, Chen M, Zhang L, Zhang Z, Wu W, Liu J, et al. Meta-analysis of acupuncture therapy for the treatment of stable angina pectoris. Int J Clin Exp Med. (2015) 8:5112–20.
14. Chen J, Ren Y, Tang Y, Li Z, Liang F. Acupuncture therapy for angina pectoris: a systematic review. J Trad Chin Med. (2012) 32:494–501. doi: 10.1016/S0254-6272(13)60061-8
15. Moher D, Liberati A, Tetzlaff J, Altman D. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. (2009) 339:b2535. doi: 10.1136/bmj.b2535
16. Huang J, Wu M, Liang S, Qin X, Shen M, Li J, et al. A critical overview of systematic reviews and meta-analyses on acupuncture for poststroke insomnia. Evid Based Complement Alternat Med. (2020) 2020:2032575. doi: 10.1155/2020/2032575
17. Huang J, Qin X, Shen M, Xu Y, Huang Y. The effects of Tai Chi exercise among adults with chronic heart failure: an overview of systematic review and meta-analysis. Front Cardiovasc Med. (2021) 8:589267. doi: 10.3389/fcvm.2021.589267
18. Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomized or non-randomized studies of healthcare interventions, or both. BMJ. (2017) 358:j4008. doi: 10.1136/bmj.j4008
19. Pollock A, Farmer SE, Brady MC, Langhorne P, Mead GE, Mehrholz J, et al. An algorithm was developed to assign grade levels of evidence to comparisons within systematic reviews. J Clin Epidemiol. (2016) 70:106–10. doi: 10.1016/j.jclinepi.2015.08.013
20. Zhang F, Sun M, Han S, Shen X, Luo Y, Zhong D, et al. Acupuncture for primary dysmenorrhea: an overview of systematic reviews. Evid Based Complement Alternat Med. (2018) 2018:8791538. doi: 10.1155/2018/8791538
Keywords: acupuncture, stable angina pectoris, AMSTAR 2, grade, overview
Citation: Shen M, Huang J and Qiu T (2021) Quality of the Evidence Supporting the Role of Acupuncture for Stable Angina Pectoris: An Umbrella Review of Systematic Reviews. Front. Cardiovasc. Med. 8:732144. doi: 10.3389/fcvm.2021.732144
Received: 28 June 2021; Accepted: 26 August 2021;
Published: 30 September 2021.
Edited by:
Xiaofeng Yang, Temple University, United StatesReviewed by:
Gerard Kennedy, Federation University Australia, AustraliaYan Guo, China Academy of Chinese Medical Sciences, China
Copyright © 2021 Shen, Huang and Qiu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tao Qiu, cWl1dGFvMjAwMjIwMDJAMTYzLmNvbQ==