 Lina Wang
Lina Wang Yangli Sun1†
Yangli Sun1† Jie Zhan
Jie Zhan Zhiyuan Wu
Zhiyuan Wu Peiming Zhang
Peiming Zhang Xu Han
Xu Han Liming Lu
Liming Lu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Cardiovasc. Med., 11 October 2021
Sec. Coronary Artery Disease
Volume 8 - 2021 | https://doi.org/10.3389/fcvm.2021.730155
Objective: The purpose of this review was to evaluate the effect of exercise therapy on anxiety and depression symptoms in patients with coronary heart disease (CHD).
Methods: A systematic review of papers published between January 2000 and February 2021 was conducted. MEDLINE, Embase, the Cochrane Library and Web of Science were searched. Meta-analysis was used to compare the results of the included studies. Bias risk assessment was performed using the Cochrane Collaboration bias risk tool. If half or more of the seven items in Randomized controlled trials (RCTs) were low-risk, then the RCT was considered low-risk research; otherwise, it was high-risk. Statistical analyses were performed using RevMan version 5.3 and STATA version 12.0.
Results: We performed a meta-analysis of 11 randomized clinical studies including 771 subjects. Eight studies (73%) were of high quality. Compared with the control group, the exercise group showed a significant improvement in anxiety [standard mean difference (SMD) = −0.61; 95% confidence interval (CI): −0.86, −0.35]. The depression level in the exercise group was also significantly reduced (SMD = −0.48; 95% CI: −0.92, −0.04). Aerobic fitness and athletic endurance also improved [mean difference (MD) = 0.77; 95% CI: 0.58, 0.95; and MD = 20.69; 95% CI: 6.91, 34.46; respectively].
Conclusions: This meta-analysis suggests that exercise therapy may be effective in alleviating anxiety and depression symptoms in patients with coronary heart disease. Due to methodological weaknesses, rigorous research needs to be designed to further confirm the effectiveness of exercise therapy in improving the mental health of patients with coronary heart disease.
Systematic Review Registration: https://inplasy.com/projects/, identifier: INPLASY202160017.
Partial or complete blockage of the coronary artery due to atherosclerosis, which leads to myocardial ischemia, hypoxia or necrosis, is called coronary heart disease (CHD) together with coronary spasm, and it is one of the main causes of death and life reduction worldwide (1). Depression and anxiety are recognized as social and psychological risk factors for coronary heart disease (2); ~15–20% of patients with coronary heart disease suffer from depression, resulting in increased mortality and decreased quality of life (3). The prevalence of anxiety in patients with coronary heart disease is ~15%, and a meta-analysis by Roest et al. has suggested that post-myocardial infarction anxiety increases the risk of adverse cardiac outcomes by 36% (4, 5). However, epidemiological studies have shown that <20% of patients with depression have been properly treated (6), and the rate of anxiety and depression symptoms after coronary heart disease is even lower, which will result in a higher recurrence and mortality rate of coronary heart disease, as well as high health care expenditures. The American Heart Association (AHA) published a scientific recommendation in 2008 to screen all patients with CHD for depression, and European clinical guidelines for cardiovascular diseases also recommend the treatment of depression and anxiety (7).
At present, the psychological and psychiatric intervention recommended by the guidelines seems to improve the degree of depression in patients with coronary heart disease (8–11). However, in the case of patients with coronary heart disease combined with anxiety symptoms, the effect of psychological treatment and psychotropic drugs is still unclear, indicating the need for other interventions. For patients with coronary heart disease combined with anxiety and depression, exercise may be a promising, flexible and easy-to-implement treatment option. Exercise can reduce anxiety and depression in patients without coronary heart disease as well as improve cardiac prognosis (12, 13). A meta-analysis by Kugler et al. before 2,000 suggested that exercise therapy might be beneficial to improve the mood of patients with coronary heart disease (14). However, another systematic evaluation report (15) found it impossible to definitively conclude that exercise is effective for anxiety and depression symptoms in patients with ischemic heart disease due to the general lack of data on the effect of exercise. In recent years, studies have shown that inspiratory muscle training can significantly improve anxiety symptoms after coronary artery bypass surgery (CABG) (16). In contrast, some studies have concluded that exercise-based cardiac rehabilitation has no obvious effect on improving patients' depression (17). Due to current conflicting evidence, we performed a meta-analysis to evaluate the efficacy of exercise therapy on depression and anxiety symptoms in patients with coronary heart disease.
All available randomized controlled trials (RCTs) met the following criteria: participants were over 18 years old and diagnosed with coronary heart disease (including acute coronary syndrome, angina pectoris, coronary artery disease confirmed by coronary angiography, percutaneous coronary intervention or coronary artery bypass grafting). An RCT was included if there were elevated levels of anxiety and depression (clinically diagnosed as anxiety and depression or scores higher than the threshold on the effective scale) as the primary or secondary outcome and there was an effective score on the anxiety and depression scale at baseline or before and after the intervention.
We included studies that received exercise therapy alone or as part of a comprehensive cardiac rehabilitation program that included psychological interventions or health education. Exercise could be any combination of aerobic, strength, or balance training. There were no restrictions on the length of time, frequency or method. Exercise-based cardiac rehabilitation, deep breathing exercises or inspiratory muscle training were also included.
If the exercise intervention was compared with standard medical care or any other intervention (such as psychological education, antidepressant drugs, or stress management), the study was included.
The primary outcomes were depression and anxiety severity. Anxiety was assessed by the HADS-A, GAD 7, HAMA, and DASS-A. Depression was assessed by the HADS-D, HAMD, SDS, PHQ-9, BDI, DASS-D, and CDS, all of which are effective self-reporting tools. For example, the Hospital Anxiety and Depression Scale (HADS) consists of 14 items, seven measuring anxiety and seven measuring depression (18). According to the literature, the cutoff point for elevated anxiety and depression as measured by the HADS is eight. For example, the SDS consists of 20 items that describe depressive symptoms. Respondents describe how often they experience each symptom on a 4-level scale, from “no or few” to “most or all.” Lower scores represent a more favorable psychological state. Secondary outcomes were the 6-min walk test and peak oxygen consumption.
We searched MEDLINE, Embase, the Cochrane Library and Web of Science from 1 January 2000 to 1 February 2021. This period was chosen to select recent studies that reflect contemporary clinical cardiology practice. We established search strategies that combined medical subject headings and free-text terms that contained subjects with coronary heart disease, anxiety, depression, exercise therapy, and randomized clinical trials. The citations retrieved from these four electronic databases were further screened for potentially eligible studies. A manual search of published meta-analyses, review articles, and handbooks of meeting minutes was also performed to ensure inclusion of all relevant studies for preliminary review. The searches were limited to studies published in English. Detailed search strategies are described in Appendix 1.
Two reviewers (LNW, PMZ) independently screened all titles and abstracts for potential eligible publications. Articles that passed the initial screening underwent full text review by both reviewers. Disagreement about study eligibility was resolved by discussion with the last author (JZ).
Two reviewers (LNW, JZ) independently extracted data from each study using a predefined data extraction sheet. The information we collected included research characteristics (such as the author's name, publication year, research design, country, and sample size), population characteristics (such as average age, gender, baseline anxiety level (HADS-A, GAD7, HAMA, and DASS-A), baseline depression level (HAMD, SDS, PHQ-9, BDI, HADS-D, DASS-D, and CDS), and intervention characteristics (movement type, frequency, and duration). If studies presented insufficient data or uncertain information, we contacted the corresponding authors. Discrepancies were resolved by discussion with the third reviewer (LL).
Using the Cochrane Collaboration bias risk tool, we identified the following domains as relevant for assessing the RCTs: sequence generation, allocation concealment, blinding of participants and personnel, incomplete outcome data, selective outcome reporting, and other sources of bias. Blinding was assessed at the outcome level. Two reviewers (LNW, JZ) independently classified each domain as having a low, high or unclear risk of bias. If half or more of the seven items in an RCT are low-risk, the RCT can be considered low-risk research; otherwise, it is high-risk. Disagreement about the risk of bias was resolved by discussion with the third reviewer (LL).
The statistical analyses were performed using RevMan version 5.3 (Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014) and STATA version 12.0. The mean difference (MD) or standardized mean difference (SMD) with 95% CI was used to analyze continuous outcomes. The SMD statistic was selected when the outcome was assessed by the different scales. I2 statistics were calculated to assess the heterogeneity and to choose the effect model. If I2 > 50% and the P-value of X2 was <0.1, meaning that statistical heterogeneity existed among studies, a random-effects model was selected. Otherwise, a fixed-effects model was used. If the pooled result included clinical heterogeneity, subgroup analysis was performed to search for the source of heterogeneity. Moreover, to examine the stability of the analysis result, we also conducted a sensitivity analysis by removing one study at a time. In studies that reported multiple depression results, to prevent double counting in the meta-analysis, we randomly selected one. If a study included multiple intervention groups (with different treatments), we combined all relevant experimental interventions from the study into a single group (comparison format: all exercise groups vs. control group) and combined the mean and SD using the continuous outcome formula in the Cochrane manual (19).
In total, 856 citations were obtained by searching 4 electronic databases along with reference lists (one citation). Overall, 158 repetitive citations were eliminated. Based on the abstracts and titles of these studies, 676 citations were excluded. Twenty-two citations passed the full-text review, and 11 were excluded because they did not meet the eligibility criteria. The remaining 11 randomized controlled trials, including 771 participants, met the eligibility criteria. In the end, 11 studies met the inclusion criteria and were included in the meta-analysis (see Figure 1).
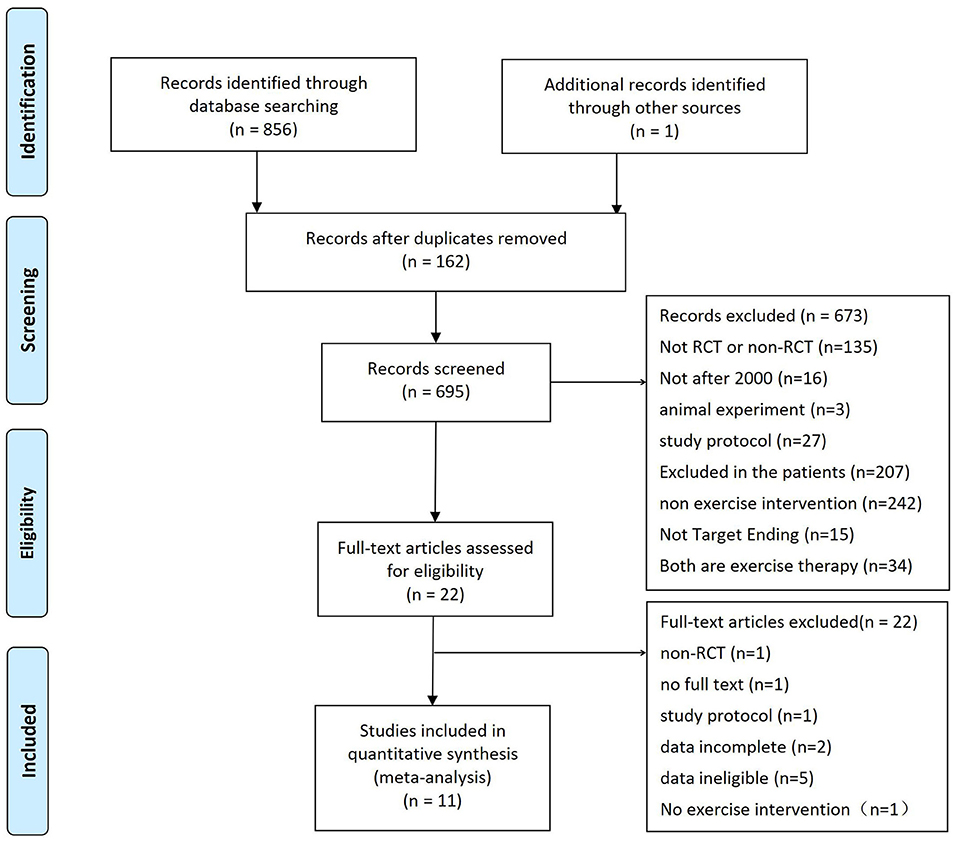
Figure 1. Flow of the trial selection process.
The baseline characteristics of the 11 eligible RCT studies are summarized in Table 1. Eleven studies were randomized controlled studies, 10 studies (91%) reported a primary outcome of depression, five studies (45%) reported a primary outcome of anxiety, the average age of patients ranged from 51.51 to 72.46 years old, and the majority of the patients were male. Treatment ranged from 10 days to 24 weeks. All the experimental treatment groups were treated with exercise therapy, while the control group was treated with non-exercise therapy.
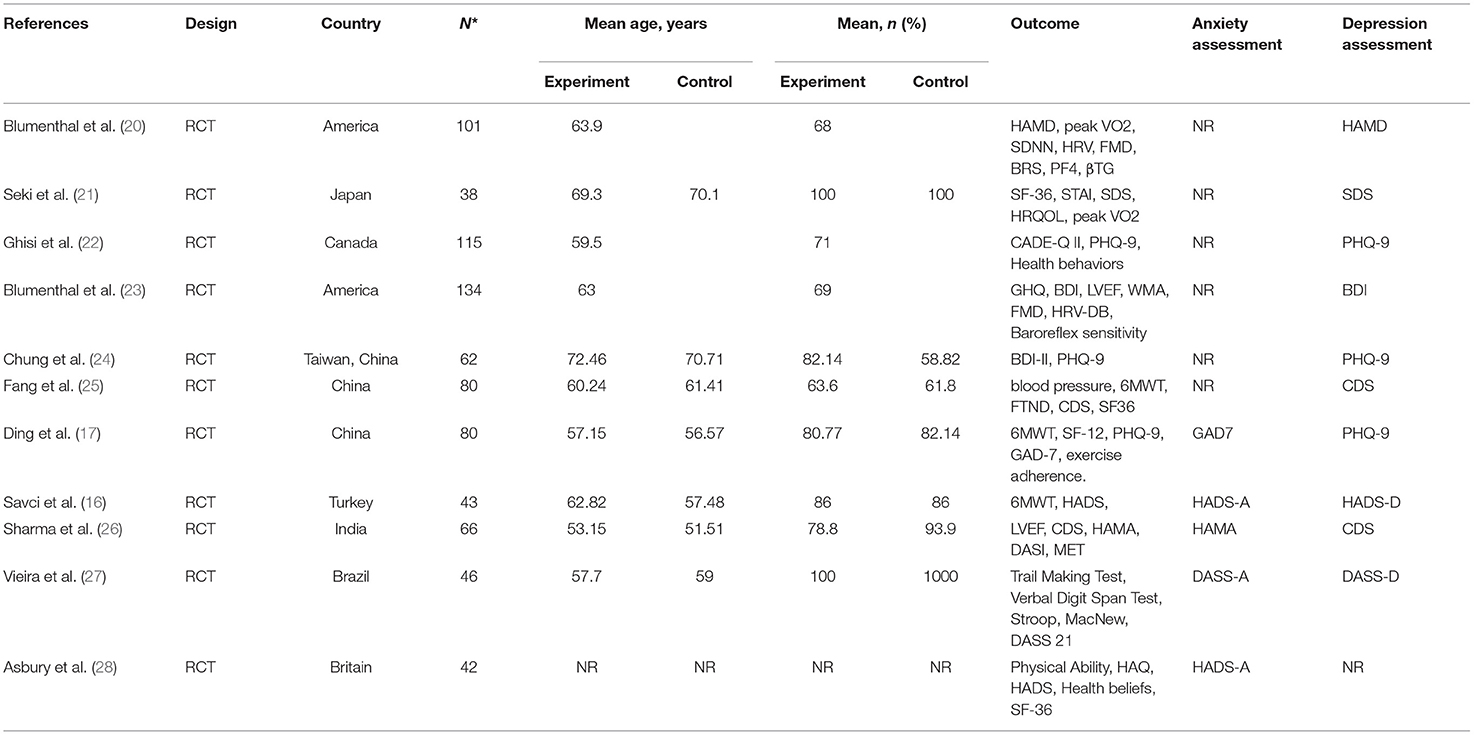
Table 1. Characteristics of included studies.
Eight of the 11 RCTs assessed the risk of bias, where half or more of the seven items were low risk, resulting in eight (73%) of the RCTs being low risk studies. Two (18%) studies were judged to be biased due to insufficient reporting of allocation concealment, blinding of participants, blinding of outcome evaluation, and selective reporting. In addition, in one study (9%), due to issues related to obtaining fully informed consent, the local ethics committee explicitly prohibited the use of group blindness (Figures 2, 3).
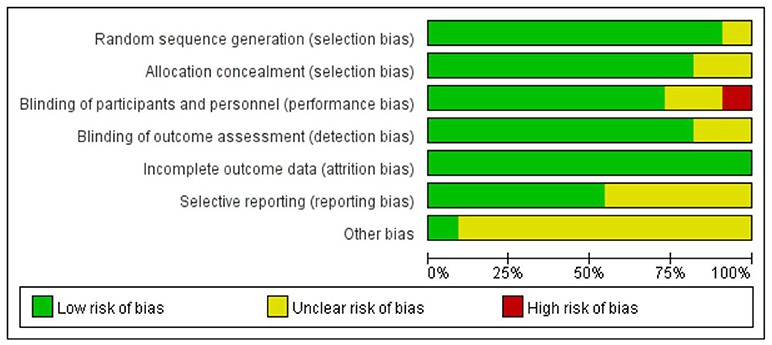
Figure 2. Demonstrate the risk of bias in the included studies.
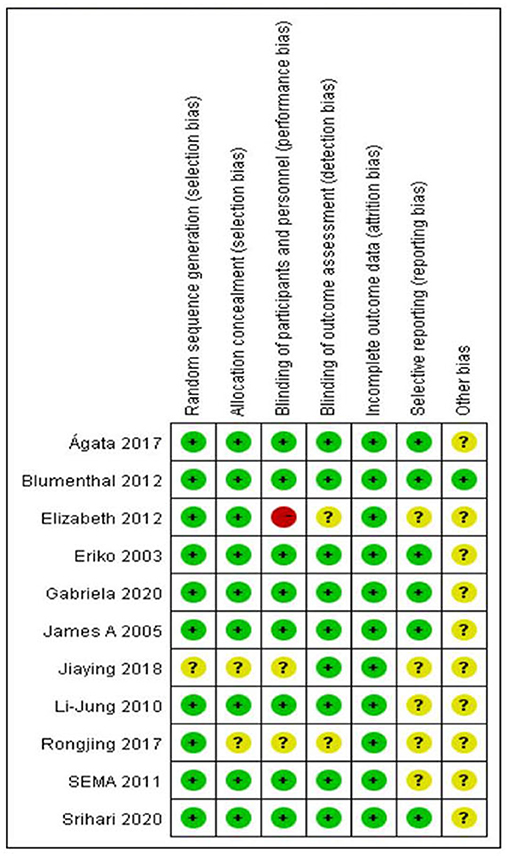
Figure 3. Risk of bias summary review authors' judgements about each risk of bias item for each included study.
In total, 260 participants in five randomized controlled studies (16, 17, 26–28) evaluated the effect of exercise therapy on anxiety in patients with coronary heart disease (Figure 4). Using evaluation methods, including GAD7, HADS-A, HAMA, and DASS-A, due to the diversity of dimensions, we used SMD to aggregate the anxiety symptom data, and the fixed-effect model was chosen because the combined results had no obvious statistical heterogeneity. The results showed that compared with the control group, the intervention group had a significant overall effect in improving anxiety of patients with coronary heart disease.
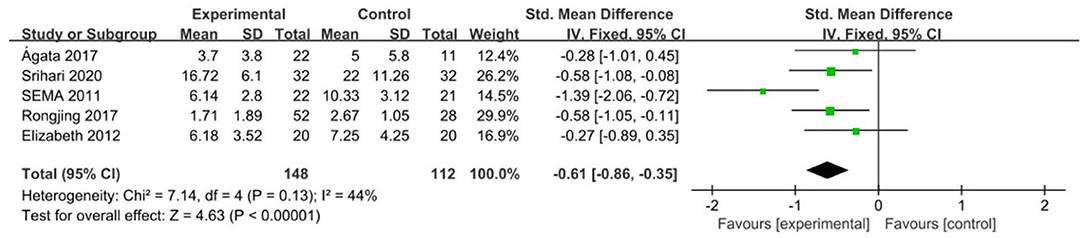
Figure 4. Meta-analysis: anxiety in coronary heart disease patients.
Since one of the trials did not study the target outcome of depression and could not be included in the meta-analysis, 731 participants in 10 randomized controlled studies (16, 17, 20–27) evaluated the effect of exercise therapy on depression in patients with coronary heart disease (Figure 5). Using evaluation methods, including HAMD, SDS, PHQ-9, BDI, CDS, HADS-D, CDS, and DASS-D, the random effects model was chosen because the combined results were highly statistically heterogeneous. The comprehensive results showed that, compared with the control group, the intervention group had a significant overall effect in improving the depression of patients with coronary heart disease.
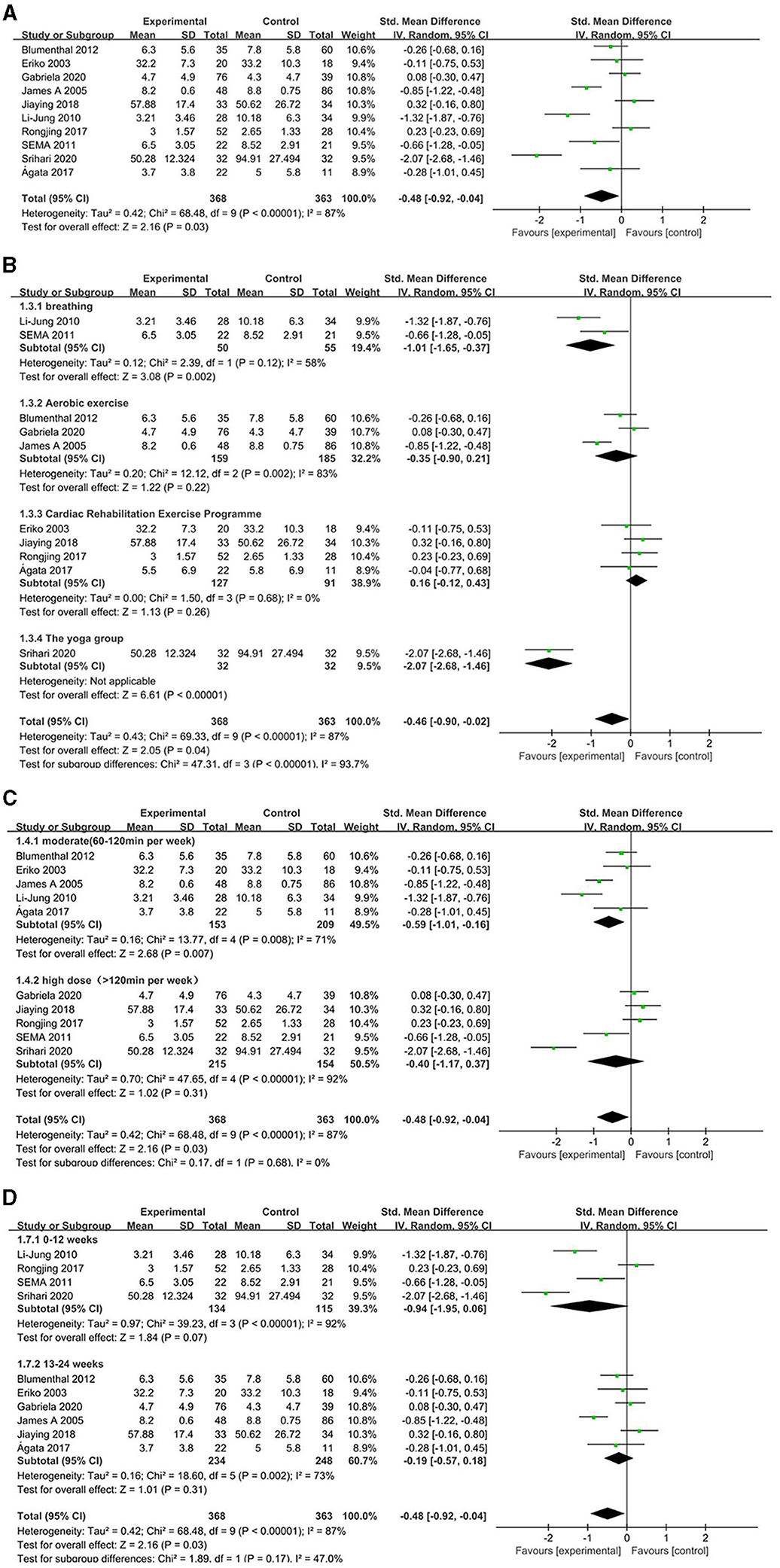
Figure 5. Comparison of acupuncture related therapies in terms of UPDRS-II. (A) The effect of exercise therapy on depression in patients with coronary heart disease. (B) The effect of different exercise types on depression in patients with coronary heart disease. (C) The effect of different exercise time on depression in patients with coronary heart disease. (D) According to the length of intervention, exercise therapy the impact of depression in patients with coronary heart disease.
Subgroup analysis: Four exercise-focused cardiac rehabilitation studies and three studies on aerobic exercise reached no conclusions. The statistical heterogeneity of the combined results from the two studies on respiratory motion was small, and a significant difference was found between the intervention group and the control group, suggesting that the intervention group had a significant overall effect at improving the degree of depression in patients with coronary heart disease (Figure 5B). According to different intervention doses, we divided the frequency and duration of exercise therapy, and divided it into medium dose (60–120 min per week) and high dose (120 min per week). Comprehensive results of different doses show that there are differences between the exercise therapy group and the control group. There are subgroup differences, and compared with the control group, moderate-dose exercise therapy can improve depression in patients with coronary heart disease (Figure 5C). According to the length of the intervention, the treatment time is divided into 0–12 and 13–24 weeks. The results of the length of the comprehensive intervention time show that there is a difference between the exercise therapy group and the control group (Figure 5D).
Sensitivity analysis: A sensitivity analysis was performed by excluding one study at a time, and the results showed that after excluding one study, the combined result was stable and not affected by any single data set (Figures 6, 7).
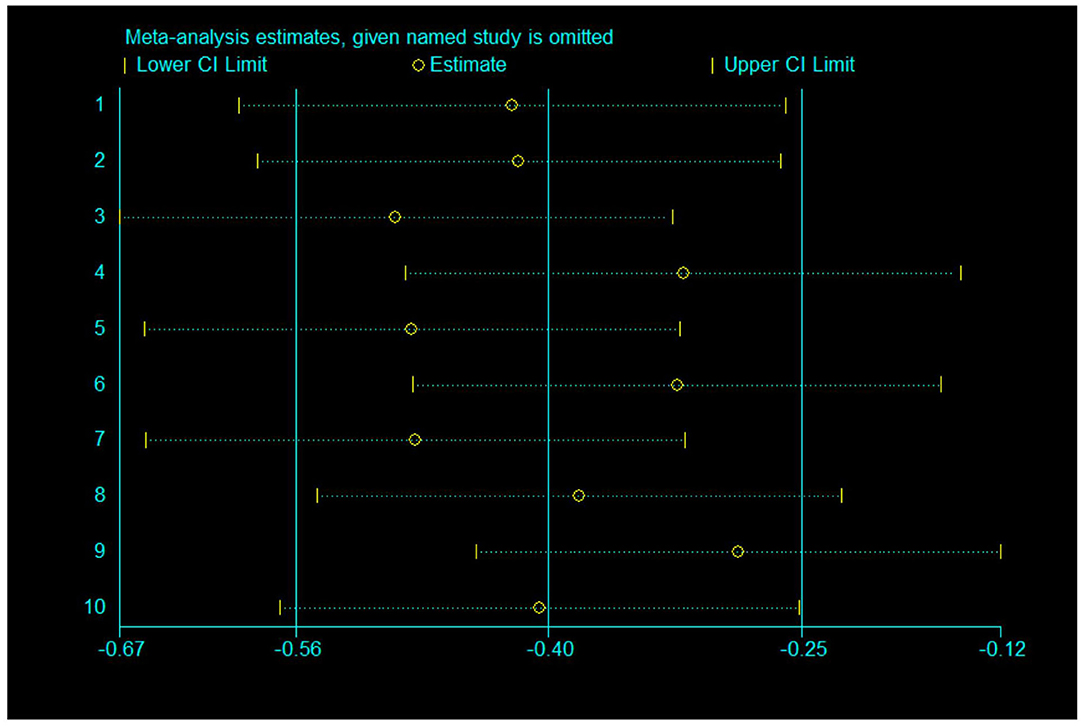
Figure 6. Sensitivity analysis of 10 items for depression.
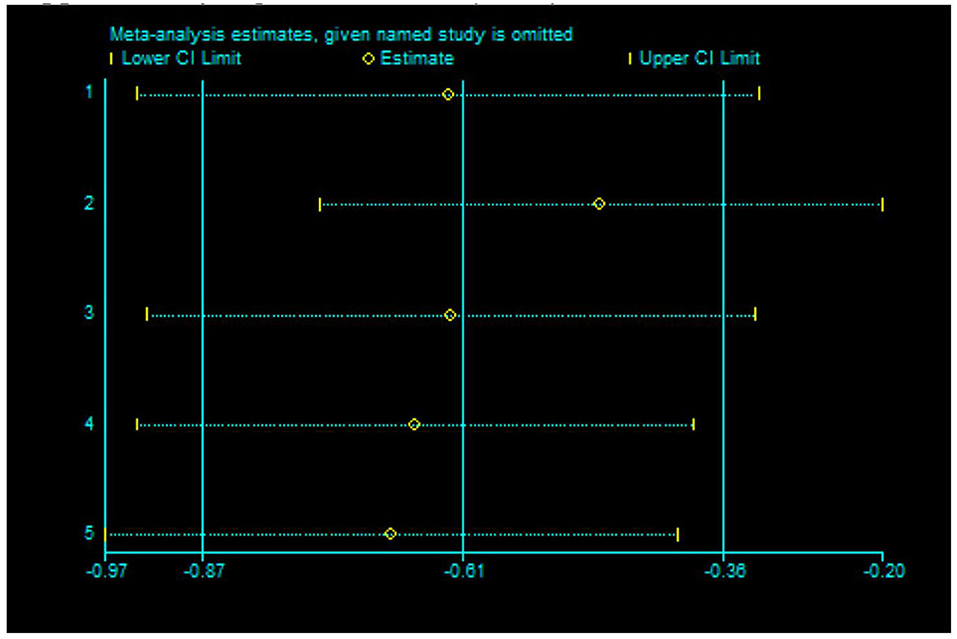
Figure 7. Sensitivity analysis of 5 items to the effect of anxiety.
The cardiopulmonary function test (CPET), as the core assessment technique of cardiac rehabilitation, is a necessary condition for ensuring precise exercise prescription. In the cardiopulmonary exercise test, the peak oxygen uptake (VO2 peak) was one of the most important parameters (Figure 8). Eight of the 11 randomized controlled studies did not report the target outcome peak oxygen concentration; thus, we included 3 studies with a total of 267 participants. A meta-analysis was performed to evaluate the exercise tolerance and aerobic adaptability of exercise therapy in patients with coronary heart disease. The fixed-effects model was chosen because there was no significant statistical heterogeneity in the combined results. Compared with the control group, the intervention group had a significant difference in peak oxygen uptake.

Figure 8. Meta-analysis: a 6-minute walk trial of exercise therapy in patients with coronary heart disease.
The 6-min walk test was used to assess functional exercise ability. Of the 11 randomized controlled studies, seven studies did not report the target outcome of the 6-min walk test. One of the studies had inappropriate data. Therefore, we included three studies with a total of 190 participants for a meta-analysis to evaluate the effect of exercise therapy on coronary heart disease (Figure 9). The fixed-effects model was chosen because there was no significant statistical heterogeneity in the combined results. Compared with the control group, the intervention group had a significant difference in the 6-min walk test.

Figure 9. Meta-analysis: peak oxygen uptake with exercise therapy in patients with coronary heart disease.
We performed a meta-analysis of 11 randomized clinical studies including 771 subjects. We evaluated the impact of exercise therapy on anxiety and depressive symptoms in patients with coronary heart disease, and most studies focused on patients with coronary heart disease with anxiety and/or depression at baseline. We have drawn several conclusions. First, the combined results of exercise therapy on anxiety symptom scores of patients with coronary heart disease show that the exercise group is superior to the control group in improving anxiety. Second, the combined results of exercise therapy and depression symptom scores of patients with coronary heart disease showed that the exercise group was superior to the control group in improving depression. Due to the high heterogeneity of the combined results, we conducted a subgroup analysis on different exercise methods, and the results showed that the overall effect of respiratory exercise on improving the depression degree of patients with coronary heart disease was significant, while the differences between the exercise-based cardiac rehabilitation and aerobic exercise subgroups were not statistically significant. Sensitivity analysis was performed on all main results, indicating that the results were durable and stable. Third, exercise therapy can significantly improve peak oxygen uptake in patients with coronary heart disease according to the results of the 6-min walk test. In summary, exercise therapy can improve the anxiety and depression symptoms, aerobic adaptability and functional exercise ability of patients with coronary heart disease.
Previous related studies have suggested that long-term, moderate-intensity exercise therapy can effectively alleviate depression symptoms and is widely used in the treatment of depression (29, 30). Among them, the relationship between anxiety, depression and cardiovascular disease has become an important area of research and therapeutic intervention. This relationship may affect the onset of cardiovascular disease, and the prognosis is unclear (31). The mechanism by which exercise reduces anxiety and depression symptoms may be multifactorial. Physiological effects may be an important mechanism, including (32) a reduction in inflammation, improvement in endothelial function, reduction in platelet aggregation, and sympathetic-vagal balance. Social interaction may also be an important mechanism. Most importantly, exercise therapy reduced the risk factors by improving depressive mood, which was associated with significant reductions in morbidity and mortality from coronary heart disease (33).
In this study, the therapeutic effect of exercise on depressive symptoms is affected by the way of exercise. The characteristics of different exercise interventions are shown in Table 2. A different finding is that inspiratory muscle training and home deep breathing therapy suggest improvement in depression symptoms in patients with coronary heart disease, but the antidepressant effects of exercise-based cardiac rehabilitation and aerobic exercise have not been confirmed, which is in line with previous meta-analysis The results are inconsistent (34). This inconsistency might be related to the sample size or the type of articles included. Second, in this study, the depressive symptoms were mostly mild and moderate, and failure to select RCTs with patients with high depressive symptoms might have affected the evaluation of exercise intervention, thus making it impossible to detect clinically significant changes in the entire study sample. The baseline levels of anxiety and depression in the study are shown in Tables 3, 4. Five of 11 RCTs included exercise as part of a multicomponent intervention. These results are difficult to explain because not all treatment-related changes can be attributed to exercise. Methodologically, depression and anxiety symptoms were secondary results in some studies. This issue may have affected our results, as the study may have adequately supported the primary outcome but not necessarily the secondary outcome (35). Due to the high heterogeneity of the results, we conducted a subgroup analysis based on the effect of different exercise time on depression in patients with coronary heart disease. Medium-dose exercise therapy (60–120 min per week) may be the best treatment to improve depression symptoms in patients with coronary heart disease time. For the improvement of exercise tolerance and aerobic fitness, according to previous studies, moderate intensity and frequent exercise may reduce the potential risk factors for coronary heart disease (36). The update of the American Heart Association's Scientific Statement (AHA) in 2020 also pointed out that regular exercise can bring cardiovascular benefits to most people, but it may bring harm to those who exercise intensively or are incompetent (37). The exercise intensity of the studies in this paper was mostly moderate, which is consistent with the basic recommendations of previous guidelines for exercise.
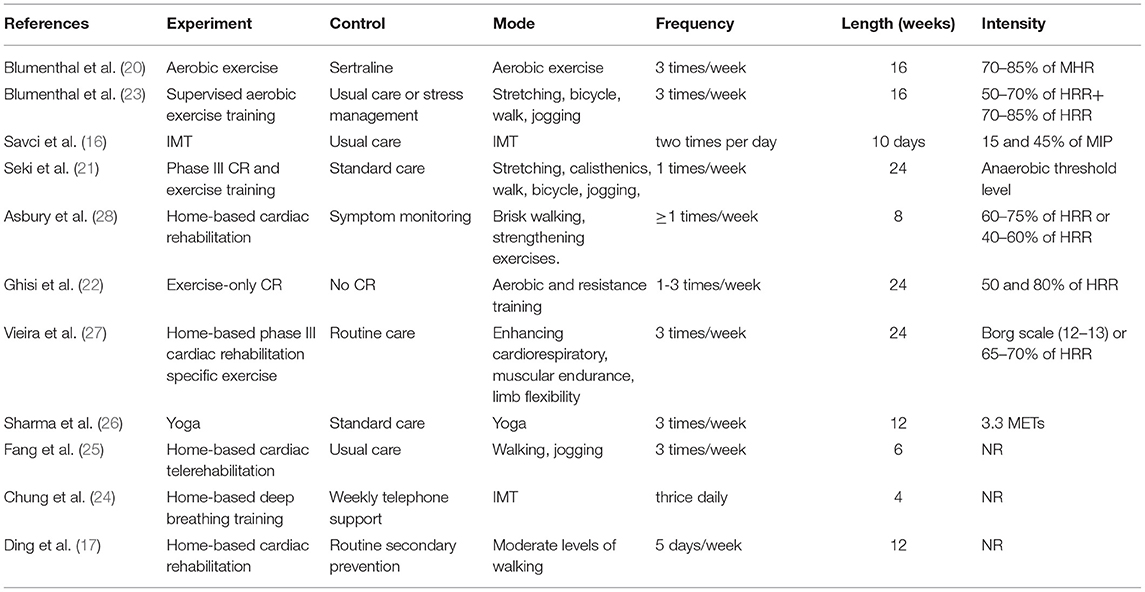
Table 2. Characteristics of different exercise interventions.

Table 3. Baseline of anxiety included in the study.
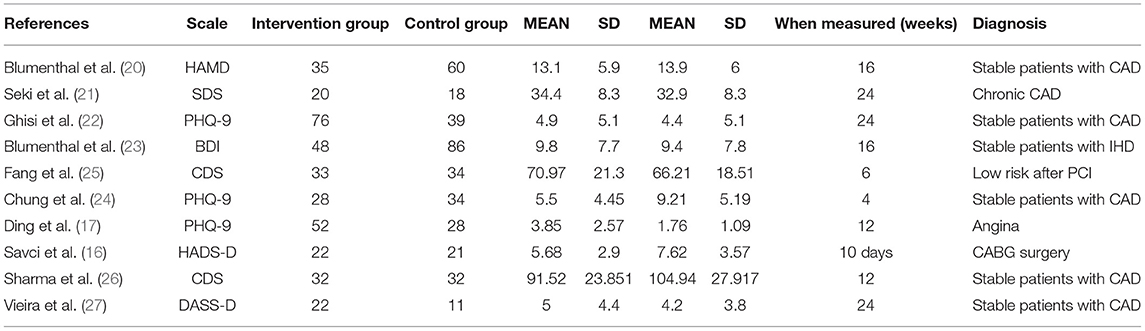
Table 4. Baseline of depression included in the study.
Anxiety disorder is very common in patients with coronary heart disease (CHD), and there is increasing evidence that high levels of anxiety disorder are associated with poor prognosis. However, few studies have evaluated the efficacy of relieving anxiety symptoms and thus improving clinical outcomes in patients with coronary heart disease (38). As far as we know, for the first time we conducted this meta-analysis, exercise therapy significantly improved the anxiety symptom scores of patients with coronary heart disease, verifying the previous systematic reviews (6). In another meta-analysis (7), it was concluded that exercise-based cardiac rehabilitation can significantly improve anxiety, but the heterogeneity of the combined results was high, which affected the interpretation of the results. In the five anxiety studies, one on deep breathing exercise, one on inspiratory muscle training, and the other three on exercise-based cardiac rehabilitation. In terms of the quality of the included studies, 65.6% were evaluated as high-quality studies, but concealment and blindness remained, which might have weakened the robustness of the evidence to some extent.
Some limitations to this analysis should be noted. First, our analysis of anxiety and depression symptom data was limited to SMD because many different anxiety and depression scales were used in the included trials (The application of different psychological scales is shown in Table 5). Second, gender differences between populations with coronary heart disease need to be considered, as the majority of participants in this study were male, which may limit the universality of the results, especially when considering older women with coronary heart disease. Studies have shown that participation in exercise therapy can help to reduce depression and anxiety in women after myocardial infarction, while men's depression and anxiety do not change significantly. Third, due to the relatively wide range of coronary atherosclerotic heart disease, the World Health Organization divides coronary heart disease into five major categories. The research included in this META analysis may not be enough to support classification based on severity. The research has a certain pointing effect. Finally, there is a lack of tests to examine the effects of exercise alone on anxiety and depression. Large-scale, high-quality randomized controlled trials (RCTs) are needed to determine the benefits of exercise in the treatment of anxiety and depression in patients with coronary heart disease, especially in elderly patients and patients with different types of coronary heart disease.

Table 5. Application of different psychological scales.
From our aggregated results, we have obtained the potential impact on clinical practice. First of all, medical staff can recommend exercise therapy as an intervention to improve anxiety and depression in patients with coronary heart disease, which may reduce potential risk factors for coronary heart disease. Second, among all major exercise therapies, deep breathing training and inspiratory muscle training may be more suitable for improving the anxiety and depression symptoms of patients with coronary heart disease as a whole. Third, moderate-intensity exercise (60–120 min per week) may be the best exercise intensity to improve depression symptoms in patients with coronary heart disease.
In summary, exercise therapy may be effective in alleviating the anxiety and depression symptoms of patients with coronary heart disease. However, these findings need to be interpreted with caution given the methodological limitations within the included studies. In order to further confirm the effectiveness of exercise therapy in improving anxiety and depression symptoms in patients with coronary heart disease, large-scale, randomized, rigorous and high-quality methodological and long-term follow-up trials are urgently needed.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
LW wrote the manuscript. LL and YS contributed to the conception. PZ and SG search the literature. LW, JZ, and LL extracted data. ZW, XW, and XH contributed to the acquisition. All authors have read and approved the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Thanks are due to all authors for contributions for this paper and we appreciate the reviewers valuable comments.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2021.730155/full#supplementary-material
1. GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2018) 392:10159. doi: 10.1016/S0140-6736(18)32203-7
2. Pogosova N, Kotseva K, De Bacquer D, von Känel R, De Smedt D, Bruthans J, et al. Psychosocial risk factors in relation to other cardiovascular risk factors in coronary heart disease: Results from the EUROASPIRE IV survey. A registry from the European Society of Cardiology. Eur J Prev Cardiol. (2017) 24:1371–80. doi: 10.1177/2047487317711334
3. Jha MK, Qamar A, Vaduganathan M, Charney DS, Murrough JW. Screening and management of depression in patients with cardiovascular disease. J Am Coll Cardiol. (2019) 73:1827–45. doi: 10.1016/j.jacc.2019.01.041
4. Roest AM, Martens EJ, Denollet J, de Jonge P. Prognostic association of anxiety post myocardial infarction with mortality and new cardiac events: a meta-analysis. Psychosom Med. (2010) 72:563–9. doi: 10.1097/PSY.0b013e3181dbff97
5. Farquhar JM, Stonerock GL, Blumenthal JA. Treatment of anxiety in patients with coronary heart disease: a systematic review. Psychosomatics. (2018) 59:318–32. doi: 10.1016/j.psym.2018.03.008
6. Kessler RC, Berglund P, Demler O, Jin R, Koretz D, Merikangas KR, et al. The epidemiology of major depressive disorder: results from the national comorbidity survey replication (NCS-R). J Am Med Assoc. (2003) 289:3095. doi: 10.1001/jama.289.23.3095
7. Montalescot G, Sechtem U, Achenbach S, Andreotti F, Arden C, Task Force Members, et al. 2013 ESC guidelines on the management of stable coronary artery disease: the Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J. (2013) 2013:2949. doi: 10.1093/eurheartj/eht296
8. Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C, Catapano AL, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention &Rehabilitation (EACPR). Atherosclerosis. (2016) 252:207–74. doi: 10.1016/j.atherosclerosis.2016.05.037
9. Ski CF, Jelinek M, Jackson AC, Murphy BM, Thompson DR. Psychosocial interventions for patients with coronary heart disease and depression: a systematic review and meta-analysis. Eur J Cardiovasc Nurs. (2016) 15:305–16. doi: 10.1177/1474515115613204
10. Fernandes N, Prada L, Rosa MM, Ferreira JJ, Costa J, Pinto FJ, et al. The impact of SSRIs on mortality and cardiovascular events in patients with coronary artery disease and depression: systematic review and meta-analysis. Clin Res Cardiol. (2021) 110:183–93. doi: 10.1007/s00392-020-01697-8
11. Whalley B, Rees K, Davies P, Bennett P, Ebrahim S, Liu Z, et al. Psychological interventions for coronary heart disease. Cochr Datab Systemat Rev. (2011) 21:CD002902. doi: 10.1002/14651858.CD002902.pub3
12. Kandola A, Stubbs B. Exercise and anxiety. Adv Exp Med Biol. (2020) 1228:345–52. doi: 10.1007/978-981-15-1792-1_23
13. Bueno-Antequera J, Munguía-Izquierdo D. Exercise and depressive disorder. Adv Exp Med Biol. (2020) 1228:271–87. doi: 10.1007/978-981-15-1792-1_18
14. Kugler J, Seelbach H, Krüskemper GM. Effects of rehabilitation exercise programmes on anxiety and depression in coronary patients: a meta-analysis. Br J Clin Psychol. (1994) 33:401–10. doi: 10.1111/j.2044-8260.1994.tb01136.x
15. Verschueren S, Eskes AM, Maaskant JM, Roest AM, Latour CHM, Op Reimer WS. The effect of exercise therapy on depressive and anxious symptoms in patients with ischemic heart disease: a systematic review. J Psychosomat Res. (2018) 105:80. doi: 10.1016/j.jpsychores.2017.11.018
16. Savci S, Degirmenci B, Saglam M, Arikan H, Inal-Ince D, Turan HN, et al. Short-term effects of inspiratory muscle training in coronary artery bypass graft surgery: a randomized controlled trial. Scand Cardiovasc J Scj. (2011) 45:286–93. doi: 10.3109/14017431.2011.595820
17. Ding R, Li J, Gao L, Liang Z, Xie W, Wang X, et al. The effect of home-based cardiac rehabilitation on functional capacity, behavior, and risk factors in patients with acute coronary syndrome in China. Cardiovasc Innov Appl. (2017) 2017:4. doi: 10.15212/CVIA.2017.0004
18. Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the hospital anxiety and depression scale: an updated literature review. J Psychosom Res. (2002) 52:0–77. doi: 10.1016/S0022-3999(01)00296-3
19. GSe HJPT. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The Cochrane Collaboration (2011).
20. Blumenthal JA, Sherwood A, Babyak MA, Watkins LL, Smith PJ, Hoffman BM, et al. Exercise and pharmacological treatment of depressive symptoms in patients with coronary heart disease: results from the UPBEAT (Understanding the Prognostic Benefits of Exercise and Antidepressant Therapy) study. J Am Coll Cardiol. (2012) 60:1053–63. doi: 10.1016/j.jacc.2012.04.040
21. Seki E, Watanabe Y, Sunayama S, Iwama Y, Shimada K, Kawakami K, et al. Effects of phase III cardiac rehabilitation programs on health-related quality of life in elderly patients with coronary artery disease: Juntendo Cardiac Rehabilitation Program (J-CARP). Circul J. (2003) 67:73–7. doi: 10.1253/circj.67.73
22. Ghisi GLM, Chaves GSS, Ribeiro AL, Oh P, Britto RR, Grace SL. Comprehensive cardiac rehabilitation effectiveness in a middle-income setting: a randomized controlled trial. J Cardiopul Rehabil Prev. (2020) 40:512. doi: 10.1097/HCR.0000000000000512
23. Blumenthal JA, Sherwood A, Babyak MA, Watkins LL, Waugh R, Georgiades A, et al. Effects of exercise and stress management training on markers of cardiovascular risk in patients with ischemic heart disease: a randomized controlled trial. Acc Curr J Rev. (2005) 14:2–3. doi: 10.1016/j.accreview.2005.06.008
24. Chung LJ, Tsai PS, Liu BY, Chou KR, Lin WH, Shyu YK, et al. Home-based deep breathing for depression in patients with coronary heart disease: a randomised controlled trial. Int J Nurs Stud. (2010) 47:1346–53. doi: 10.1016/j.ijnurstu.2010.03.007
25. Fang J, Huang B, Xu D, Li J, Au WW. Innovative application of a home-based and remote sensing cardiac rehabilitation protocol in chinese patients after percutaneous coronary intervention. Telemed J E Health. (2019) 25:288–93. doi: 10.1089/tmj.2018.0064
26. Sharma KNS, Pailoor S, Choudhary NR, Bhat P, Shrestha S. Integrated yoga practice in cardiac rehabilitation program: a randomized control trial. J Alternat Complement Med. (2020) 26:250. doi: 10.1089/acm.2019.0250
27. Vieira Á, Melo C, Machado J, Gabriel J. Virtual reality exercise on a home-based phase III cardiac rehabilitation program, effect on executive function, quality of life and depression, anxiety and stress: a randomized controlled trial. Disabil Rehabil Assist Technol. (2018) 13:112–23. doi: 10.1080/17483107.2017.1297858
28. Asbury EA, Webb CM, Probert H, Wright C, Barbir M, Fox K, et al. Cardiac rehabilitation to improve physical functioning in refractory angina: a pilot study. Cardiology. (2012) 122:170–7. doi: 10.1159/000339224
29. Toups M, Carmody T, Greer T, Rethorst C, Grannemann B, Trivedi MH. Exercise is an effective treatment for positive valence symptoms in major depression. J Affect Disord. (2017) 209:188–94. doi: 10.1016/j.jad.2016.08.058
30. Luan X, Tian X, Zhang H, Huang R, Li N, Chen P, et al. Exercise as a prescription for patients with various diseases. J Sport Health Sci. (2019) 4:2. doi: 10.1016/j.jshs.2019.04.002
31. Allgulander C. Anxiety as a risk factor in cardiovascular disease. Curr Opin Psychiatry. (2016) 29:13. doi: 10.1097/YCO.0000000000000217
32. Korzeniowska-Kubacka I, Bilińska M, Piotrowska D, Stepnowska M, Piotrowicz R. The impact of exercise-only-based rehabilitation on depression and anxiety in patients after myocardial infarction. Eur J Cardiovasc Nurs J Working Group Cardiovasc Nurs Eur Soc Cardiol. (2017) 2017:147451511668212. doi: 10.1177/1474515116682123
33. Peterson JC, Charlson ME, Wells MT, Altemus M. Depression, coronary artery disease, and physical activity: how much exercise is enough? Clin Therapeut. (2014) 36:1518–30. doi: 10.1016/j.clinthera.2014.10.003
34. Zheng X, Zheng Y, Ma J, Zhang M, Zhang Y, Liu X, et al. Effect of exercise-based cardiac rehabilitation on anxiety and depression in patients with myocardial infarction: a systematic review and meta-analysis. Heart Lung. (2019) 48:1–7. doi: 10.1016/j.hrtlng.2018.09.011
35. Li J, Mehrotra DV. An efficient method for accommodating potentially underpowered primary endpoints. Stat Med. (2008) 27:5377–91. doi: 10.1002/sim.3369
36. Currie KD, Bailey KJ, Jung ME, McKelvie RS, MacDonald MJ. Effects of resistance training combined with moderate-intensity endurance or low-volume high-intensity interval exercise on cardiovascular risk factors in patients with coronary artery disease. J Sci Med Sport. (2015) 2015:637–42. doi: 10.1016/j.jsams.2014.09.013
37. Franklin BA, Thompson PD, Al-Zaiti SS, Albert CM, Hivert MF, Levine BD, et al. Exercise-related acute cardiovascular events and potential deleterious adaptations following long-term exercise training: placing the risks into perspective–an update: a scientific statement from the american heart association. Circulation. (2020) 2020:749. doi: 10.1161/CIR.0000000000000749
38. Blumenthal JA, Feger BJ, Smith PJ, Watkins LL, Jiang W, Davidson J, et al. Treatment of anxiety in patients with coronary heart disease: rationale and design of the UNderstanding the benefits of exercise and escitalopram in anxious patients WIth coroNary heart Disease (UNWIND) randomized clinical trial. Am Heart J. (2016) 176:53–62. doi: 10.1016/j.ahj.2016.03.003
39. Santos IS, Tavares BF, Munhoz TN, Almeida LS, Silva NT, Tams BD. Sensitivity and specificity of the Patient Health Questionnaire-9 (PHQ-9) among adults from the general population. Cad Saude Publica. (2013) 29:1533–43. doi: 10.1590/S0102-311X2013001200006
40. Richter P, Werner J, Heerlein A, Kraus A, Sauer H. On the validity of the beck depression inventory. Psychopathology. (1998) 31:160–8. doi: 10.1159/000066239
Keywords: exercise therapy, coronary heart disease, anxiety, depression, meta-analysis
Citation: Wang L, Sun Y, Zhan J, Wu Z, Zhang P, Wen X, Ge S, Han X and Lu L (2021) Effects of Exercise Therapy on Anxiety and Depression in Patients With Coronary Heart Disease: A Meta-Analysis of a Randomized Controlled Study. Front. Cardiovasc. Med. 8:730155. doi: 10.3389/fcvm.2021.730155
Received: 24 June 2021; Accepted: 07 September 2021;
Published: 11 October 2021.
Edited by:
Hao Hu, University of Macau, ChinaReviewed by:
Matthias Bossard, Luzerner Kantonsspital, SwitzerlandCopyright © 2021 Wang, Sun, Zhan, Wu, Zhang, Wen, Ge, Han and Lu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Liming Lu, bHVsaW1pbmdsZW9uQDEyNi5jb20=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.