 Muhammad Sabbah
Muhammad Sabbah Thomas Engstrøm
Thomas Engstrøm Jacob Lønborg
Jacob Lønborg- Department of Cardiology, Rigshospitalet, Copenhagen University Hospital, Copenhagen, Denmark
Transcutaneous aortic valve implantation (TAVI) has led to a paradigm shift in the treatment of severe aortic stenosis (AS) in the elderly and is expanding to still younger and lower-risk patients with severe AS as an alternative to surgical aortic valve replacement (SAVR). While the role of coronary artery bypass grafting with SAVR is well-documented, the analog of percutaneous coronary intervention with TAVI is less so. The aim of this review is to provide an overview of the important challenges in treating severe AS and co-existing coronary artery disease in patients planned for TAVI.
Introduction
Aortic stenosis (AS) is the most common valvular heart disease in the Western world, affecting 2–7% of all people older than 65 years (1, 2). Surgical aortic valve replacement (SAVR), introduced in the 1960s (3), was for many years the only treatment available for severe AS, but excluded a considerable number of patients due to high surgical risk. The advent of transcatheter aortic valve replacement (TAVI) in 2002 has led to a paradigm shift in the treatment of severe AS (4). TAVI has been demonstrated to confer better survival compared with conservative treatment in inoperable patients (5–8). Moreover, it has been shown to be at least non-inferior to SAVR in elderly patients across all surgical risk profiles (9–15). According to the recently updated American and European guidelines, TAVI is the recommended treatment of symptomatic severe AS in patients aged 80 years or more and may be considered in patients aged 65–80 years based on patient/anatomical characteristics and shared decision-making (16, 17). As a result, more patients are currently treated with TAVI than with SAVR in the Western world. In parallel with this increasing number of (now also younger) patients treated with TAVI, there is an increasing focus on dealing with co-existing coronary artery disease (CAD).
Prevalence, Importance, and Challenges of Coronary Artery Disease in Patients With AS
AS and CAD share several common cardiovascular risk factors such age, hypertension, hypercholesterolemia, and smoking (18). Likewise, there is an important overlap in the symptomatology of AS and CAD with exertional dyspnea and angina pectoris seen in both. Frequently, no angina is reported in patients with severe AS, but significant CAD is incidentally found in the coronary angiogram. In other cases, patients report classical angina but have no significant CAD, the cause likely being microvascular dysfunction (19). Thus, the relative contribution from each disease to the symptom burden is often hard to discern. The prevalence of CAD in patients undergoing TAVI is reported to range from 38.0 to 74.9% (5–7, 12, 13, 20–31). This broad range reflects a large variation in the definition of CAD between studies (Table 1). However, as both previous coronary artery bypass graft (CABG) and percutaneous coronary intervention (PCI) are included in the definition of CAD in these studies as well as the coronary stenosis visually on the coronary angiogram without physiology to assess the importance of the CAD has been used to define co-existing CAD, the prevalence of significant CAD that may warrant revascularization in addition to TAVI is likely much lower. This is supported by registry data in which only 15% of a TAVI population underwent revascularization with PCI before TAVI (24).
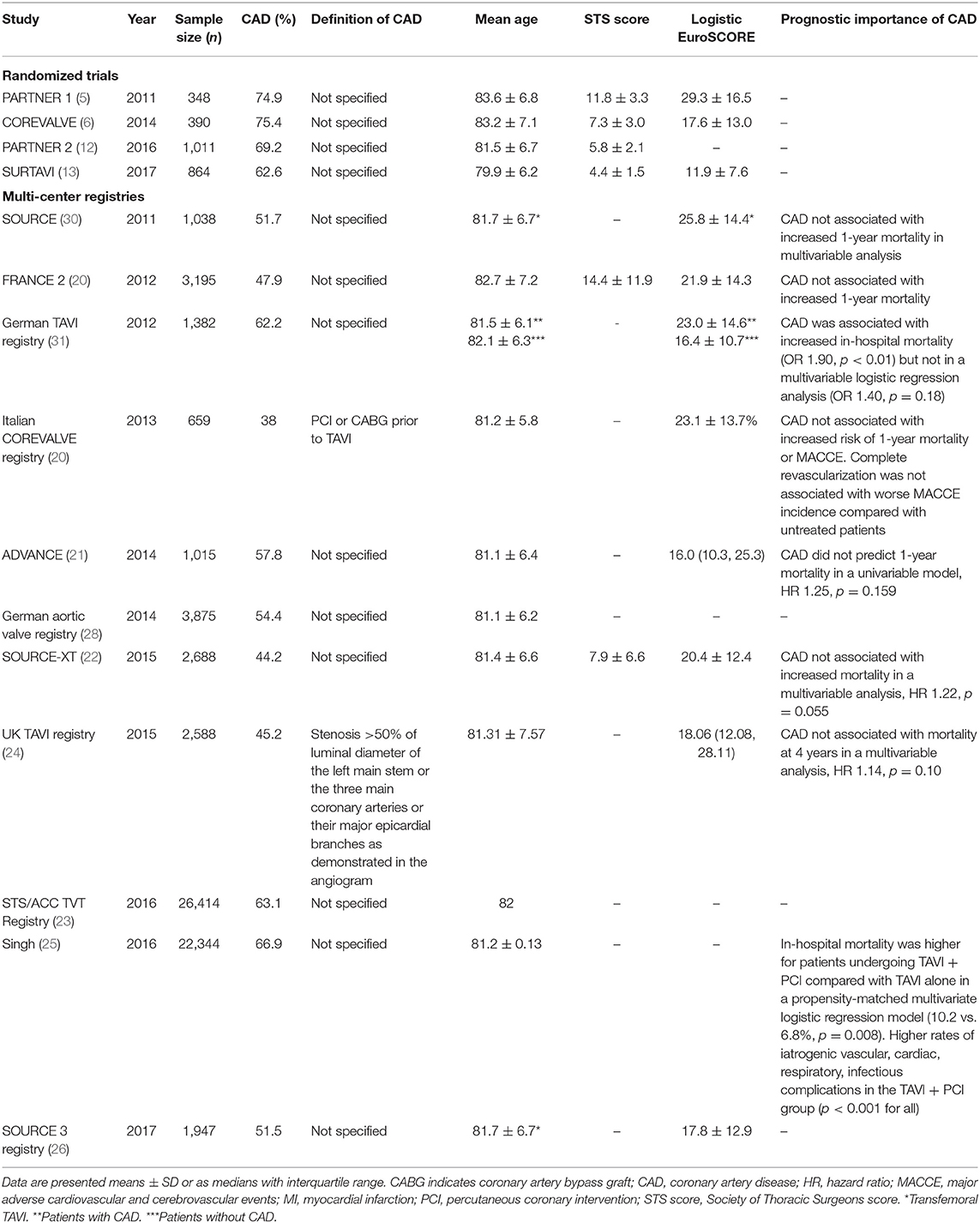
Table 1. Prevalence, definition, and importance of CAD in TAVI reported in randomized trials and real-world multi-center registries.
Regardless, co-existing CAD is frequent in patients with severe AS undergoing TAVI, but the clinical importance is uncertain (Table 1). Registry data suggest that co-existing CAD is not independently related to a reduced 1-year survival rate (24). However, these data may be confounded as a substantial number of patients underwent revascularization with percutaneous coronary intervention (PCI) before TAVI. Moreover, the definition of CAD was based solely on visual assessment of the coronary angiogram. Today, it is well-known that angiography by itself is an inaccurate method for evaluation of the physiological severity of coronary stenoses (32). Instead, fractional flow reserve (FFR)–guided revascularization is the gold standard (33–36). Data from another registry using SYNTAX score for evaluation of CAD indicate that patients with severe and anatomically complex CAD undergoing TAVI have an increased cardiovascular mortality compared with patients with no or mild to moderate CAD (37). In the most recent meta-analysis addressing the impact of CAD in patients undergoing TAVI, 15 non-randomized studies were included for analysis (nine studies were retrospective and six prospective) totaling more than 5,000 patients (38). The main findings were as follows: (1) 30-day all-cause mortality was similar for patients with and without CAD, but 1-year mortality was significantly higher in patients with CAD; (2) procedural complications such as myocardial infarction (MI), cardiovascular mortality, stroke, bleeding, and vascular complications were not different between groups. Conversely, recently published data show that almost 10% of patients treated with TAVI are readmitted with acute coronary syndrome after a median of 25 months, which is related to the presence of CAD (39). However, these results should be interpreted with caution due to heterogeneity in the definition of CAD, lack of physiological assessment of CAD severity or use of SYNTAX score, incomplete reporting of endpoints based on CAD status in some studies, as well as the observational nature of these studies which rules out assessment of causality between CAD and outcome. Moreover, as the patients selected for TAVI are getting younger with a longer life expectancy, the clinical importance of CAD may also change.
Non-invasive Evaluation of CAD
Exercise and dipyridamole stress echocardiography have a high sensitivity for CAD in patients with AS but a specificity of only 61–74% with thallium-201 scintigraphy or coronary angiography as reference (40, 41). When adenosine is used as stressor, specificity is higher at 97% with a sensitivity of 85% (42). Other modalities such as stress SPECT, PET, and cardiac MR have been tested in small patient series (n = 23–50) with reported sensitivity ranging from 91 to 100% with specificity of 80–91% when compared against coronary angiography (43, 44). The utility of coronary CT angiography (CTA) has also been investigated in patients planned for TAVI (45, 46). In one registry, CTA done before TAVI identified significant CAD in 93.3% of patients who underwent PCI (46). However, the definition of significant CAD was a luminal narrowing of ≥50%, and only 10% had FFR measured. Another study reported CTA to have a negative predictive value of 96% for detection of significant CAD (45). Again, significant CAD was defined as ≥50% luminal narrowing, and the use of FFR was not reported. These data confirm that CTA is nearly as good as coronary angiography at identifying anatomical characteristics of CAD. Although, CTA by itself is not enough for accurate assessment of the functional significance of CAD, especially in intermediate coronary stenoses, it does offer a high negative predictive value, which can spare some patients the risks of invasive testing. As TAVI is moving toward still younger patients—with a lower prevalence of CAD—CTA could contribute to better cost-effectiveness. The accuracy of CTA can be improved further by post-processing using computational fluid dynamics which allows for derivation of FFR non-invasively (FFRCT) (47). The CAST-FFR study evaluated FFRCT against invasive FFR in patients with severe AS (48) and reported better accuracy than CTA alone. Unfortunately, clinical implementation of FFRCT has been limited by its dependence on the quality of source data, added cost, and requirement for time-consuming computation (49).
Invasive Evaluation of CAD
Fractional Flow Reserve
The use of physiological testing in addition to standard coronary angiography ensures the most accurate assessment of CAD severity (34). Of the currently available pressure-derived indices of stenosis severity, FFR is the only one that has been validated against a true gold standard (prospective multi-testing Bayesian methodology) (50) and is therefore the gold standard for invasive assessment in patients without AS. Although, FFR has never been validated in patients with severe AS, registry data indicate that FFR may also be applicable in patients with AS (51). FFR appears to change only slightly when measured immediately after TAVI (52). Positive FFR values tend to worsen, whereas, negative values tend to improve. In 6% (8 out of 133 lesions), FFR crossed the threshold for treatment indication (52). However, as others have pointed out, the prevailing systemic hemodynamic conditions during TAVI call for caution in interpretation of FFR values measured peri-procedurally (53). Physiologically, the main factor thought to alter FFR in AS patients is increased microvascular resistance due to the extravascular compression caused by high ventricular pressures (Figure 1). In a small observational study, FFR was measured in 23 lesions all with FFR values >0.75 (14 patients) before TAVI and 14 months later (54). Abnormally low values tended to worsen at follow-up while lesions with a FFR >0.80 remained stable. Only one lesion crossed the ≤0.80 cut-off from baseline to follow-up. However, this study only included patients with FFR >0.75 and not the full spectrum of FFR values. The bottom line, however, is that the standard FFR cut-off of ≤0.80 in severe patients with AS is unproven. Likewise, it is unknown if deferral of PCI in lesions with FFR > 0.80 is safe in this patient group. The ongoing FAITAVI trial (ClinicalTrials.gov Identifier: NCT03360591) is designed to address some of these questions. It is planned to randomize 320 patients referred to TAVI to revascularization guided by either angiography or FFR.
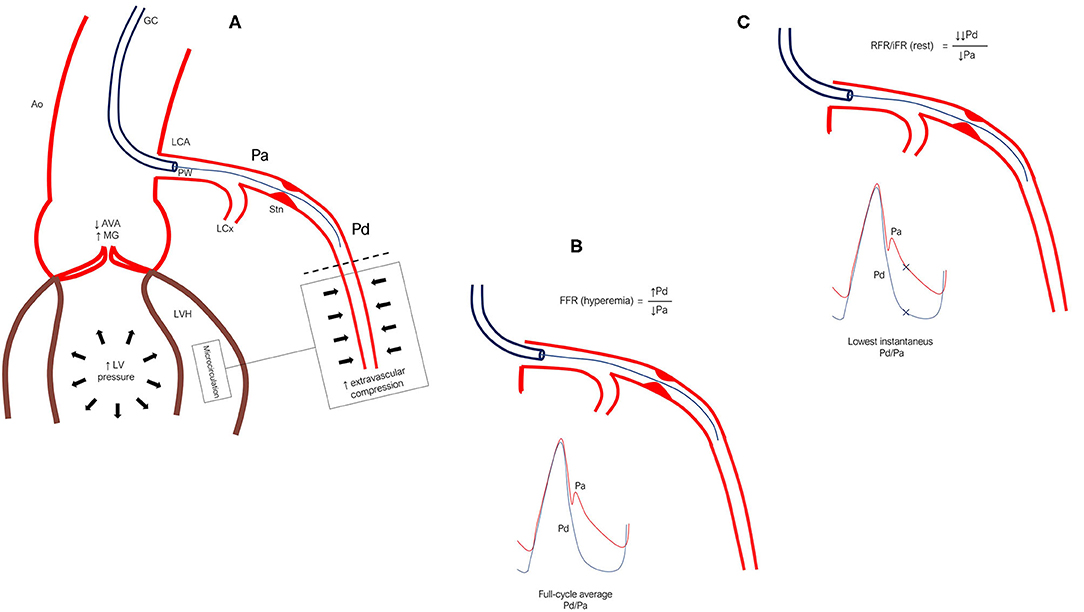
Figure 1. (A) In severe aortic stenosis, systemic, and thus aortic pressure, Pa, is often reduced due to pressure loss across the aortic valve. Meanwhile, elevated LV pressure and increased contraction force due to LVH causes intramyocardial compression of the microcirculation, driving up mean distal coronary pressure, Pd (back-pressure). (B) FFR is measured as the ratio of full-cycle mean Pd/Pa during maximal hyperemia. As such, flow rate and subsequent pressure loss across the epicardial stenosis would not be expected to vary much before vs. after TAVI. However, relief from extravascular compression (LVH and high LV pressure especially during systole) after TAVI may cause Pd to fall, thus lowering FFR. (C) The major difference between FFR and iFR/RFR is that the latter are measured during rest and are calculated as the lowest instantaneous Pd/Pa, which typically occurs during diastole. This is a potential source of error in severe AS because resting flow rate is elevated due to increased myocardial workload. Therefore, when pressure is sampled only in diastole—where pressure separation is very large in AS patients—the calculated Pd/Pa can turn out to be lower than that calculated from the full-cycle averages of Pd/Pa even during maximal hyperemia (i.e., FFR). As pressure loss across a stenosis is closely related to flow rate, measuring IFR/RFR before TAVI likely overestimates the significance of a stenosis as compared with evaluation after TAVI where resting flow and subsequent pressure loss are drastically reduced. Ao, indicates aorta; AVA, aortic valve area; FFR, fractional flow reserve; GC, guide catheter; iFR, instantaneous wave-free ratio; LCA, left coronary artery; LCx, left circumflex artery; LV, left ventricle; LVH, left ventricular hypertrophy; MG, mean gradient; Pa, aortic pressure; Pd, distal coronary pressure; PW, pressure wire; RFR, resting full cycle ratio; Stn, stenosis.
Resting Indices
Adenosine infusion is considered safe (55) and causes no significant change in cardiac work (56). However, adenosine frequently causes systemic hypotension, chest pain, and shortness of breath. These adverse effects can be an issue in frail patients hemodynamically challenged by severe AS and CAD. Efforts to circumvent the use of adenosine lead to the development of the resting full-cycle ratio (RFR) and instantaneous wave-free ratio (iFR). Resting indices are appealing as they offer a simpler, cheaper, and faster stenosis evaluation without the adverse effects of adenosine. However, they have an important potential limitation when used in patients with AS. In severe AS, resting myocardial workload is increased due to increased afterload (57). Accordingly, resting myocardial blood flow and subsequent trans-stenotic pressure-drop are large, falsely decreasing RFR/iFR (Figure 1). After valve replacement, afterload is abruptly reduced and left ventricular hypertrophy gradually regresses (58). Consequently, resting flow and trans-stenotic pressure-drop must decrease. It thus follows that the appropriate time for stenosis evaluation may be after TAVI. Using a resting flow index before TAVI, one may probe a physiologically significant lesion which after valve replacement becomes non-significant. In the only published study reporting long-term changes in FFR and iFR (14 months after TAVI), iFR showed a higher reclassification rate at 21.7 vs. 4.3% for FFR (54). Reclassification was due to lesions becoming non-significant after TAVI. Published data on changes in FFR and iFR before and after TAVI are summarized in Table 2.
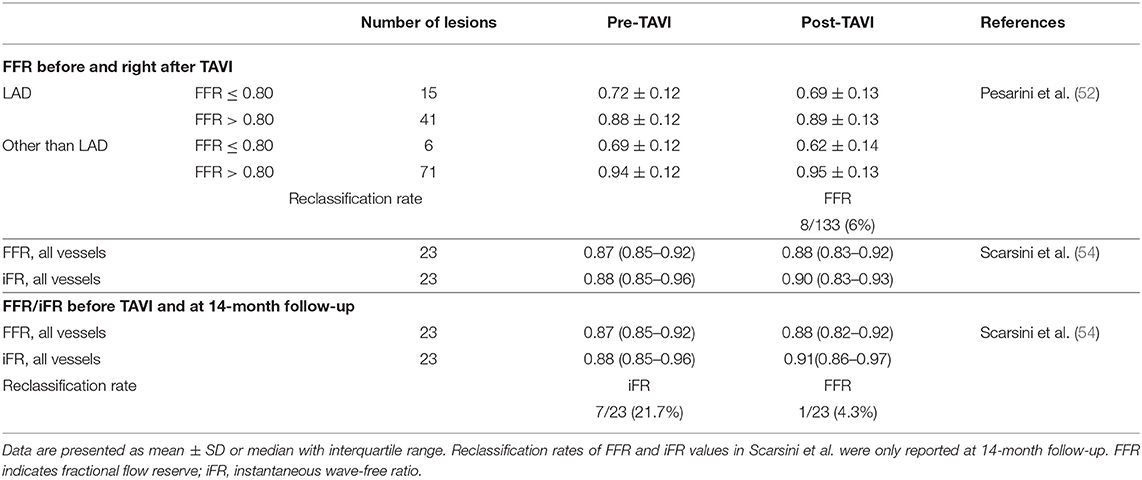
Table 2. FFR and iFR measured before and right after TAVI and after 14-month follow-up.
Revascularization in Patients Treated With TAVI
There are several uncertainties regarding revascularization of CAD before TAVI: (1) Should patients selected for TAVI with significant CAD undergo PCI?; (2) the optimal order in which to do PCI and TAVI is unknown; (3) consequences of PCI on anti-thrombotic therapy; (4) the choice of treatment for patients with more complex CAD (complex PCI + TAVI or CABG + SAVR).
Is Revascularization Necessary?
Revascularization may provide symptom relief and prevent future events such as acute coronary syndrome, as has been demonstrated in patients with stable CAD without AS and in the treatment of non-culprit lesions in patients with STEMI (59–64). Revascularization may also help to hemodynamically stabilize the patients during TAVI, as discussed later. The obvious downside of PCI before TAVI is the necessary temporary treatment with dual antiplatelet therapy (DAPT) which increases bleeding risk, particularly in the elderly, that is, in patients currently undergoing TAVI. Even short-term DAPT is associated with a higher rate of serious adverse events as compared with single antiplatelet therapy, which is now the standard post-procedural anti-thrombotic therapy after TAVI (65, 66). Another concern regarding PCI in patients with AS is the risk of stent-thrombosis and target lesion failure, but recent data have shown that these events are rare in patients treated with PCI before TAVI (67). The scarcity of controlled data from patients with AS and CAD leaves one to rely on data from isolated CAD (68–72), from which may be extrapolated that factors such as left main stenosis, very proximal stenoses, and multi-vessel disease should mandate revascularization at some point, be it before or after TAVI. For example, there is little doubt that physiologically significant left main lesions are certainly important to treat. Conversely, very distal stenoses with a small downstream subtended myocardial mass and FFR values in the gray zone, i.e., 0.75–0.80, might not be worth the risks of PCI neither before nor after TAVI. Because patients with severe AS are typically old, one may argue that the combined prognostic impact of age itself and severity of AS significantly outweighs that of co-existing CAD, making the benefit of revascularization increasingly irrelevant. For example, in the PARTNER 2 trial, the event rate (death + stroke) at 2-year follow-up was 20% while the event rate (death + myocardial infarction) at 5-year follow-up in the FAME-2 trial was only 8% (12, 73). In a retrospective analysis of the DANAMI-3-PRIMULTI study, increasing age, ≥75 years, diminished the prognostic benefit of revascularization of non-culprit arteries in patients with STEMI (68). On the other hand, the After 80 trial showed a benefit of revascularization vs. medical treatment of NSTEMI or unstable angina in patients ≥80 years (74). However, that trial also found that increasing age diminished this benefit.
The central question of whether PCI before TAVI is beneficial or even necessary at all was addressed in the recently completed, but not yet published, ACTIVATION trial (75). They randomized patients with severe AS and at least one coronary stenosis >70% in a major epicardial coronary artery to either PCI or medical therapy before TAVI. CAD was evaluated by angiography only, and patients in CCS class III–IV were excluded. Unfortunately, the trial was stopped prematurely due to low enrollment rate, with only 235 out of planned 310 patients included. The rate of the primary endpoint of mortality and rehospitalization was 41.5% in patients treated with PCI and 44.0% in the control group, which did not meet the non-inferiority margin. Patients treated with PCI had more bleeding events (44.5 vs. 28.4%, p = 0.021) with no statistical difference in major bleedings (26.1 vs. 18.1%, p = 0.19). However, the trial did not include myocardial infarction and urgent revascularization in the primary endpoint—outcomes which arguably are more relevant in this patient group than all-cause mortality. Also, information on effect on symptom relief is warranted. Another concern is the use of angiography to guide treatment in the ACTIVATION trial, as FFR is the most optimal method to guide revascularization in patients without AS (34) and probably also in patients with AS (51). Although ACTIVATION provided important evidence, the role of revascularization and especially FFR-guided PCI in patients with severe AS is still unresolved. The ongoing NOTION-3 trial (ClinicalTrials.gov Identifier: NCT03058627) may provide additional information; it is planned to randomize a total of 452 patients with severe AS and CAD to either FFR-guided full revascularization before TAVI in a staged approach or TAVI alone. Primary endpoints are all-cause mortality, MI, or urgent revascularization until the last included patient has been followed for a year after the TAVI. Another trial, COMPLETE TAVR (ClinicalTrials.gov Identifier: NCT04634240), will randomize 4,000 patients referred for TAVI to either angiography-guided PCI after TAVI or medical treatment.
When Is the Optimal Time for Revascularization?
Revascularization done before, or in conjunction with TAVI, may help to avoid myocardial ischemia related to hemodynamic instability during the TAVI procedure, but experience with the TAVI procedure has shown us that this issue is a lesser concern (Figure 3). Another issue is the easier coronary access before compared with after TAVI (76). Coronary access after TAVI is subject to growing concern in patients with long life expectancy and therefore a higher risk of a second TAVI (valve-in-valve). Commissural alignment of the transcatheter heart valve may help in overcoming this issue (77), just as use of a transcatheter heart valve with a low frame and intra-annular leaflets allows easier coronary access as demonstrated in the RE-ACCESS study (76) (Figures 2, 3). There are no randomized data demonstrating whether concomitant TAVI and PCI is superior to a staged approach, or vice versa. In the only published meta-analysis including four observational studies with a total of 209 patients, there was no difference between groups in terms of 30-day mortality, renal failure, periprocedural MI, life-threatening bleeding, or major stroke (78). In the SURTAVI trial, 128 patients underwent TAVI and PCI of whom 76 (56.4%) were treated through a staged approach, whereas 52 (40.6%) had TAVI and PCI performed concomitantly. The staged approach was associated with significantly higher contrast load and acute kidney injury compared with the concomitant procedure (79). Although, patients were not randomized to either approach, this sample is the largest from a single published study. Contrarily, in patients with complex CAD and reduced left ventricular function, TAVI is generally recommended before revascularization. These patients, in turn, are disadvantaged by the dependence on the blood supply from a compromised coronary circulation during the TAVI procedure. The optimal order in which to do PCI and TAVI is currently under investigation in the TAVI-PCI Trial (ClinicalTrials.gov Identifier: NCT04310046) in which patients will be randomized to FFR-guided PCI before or after TAVI.
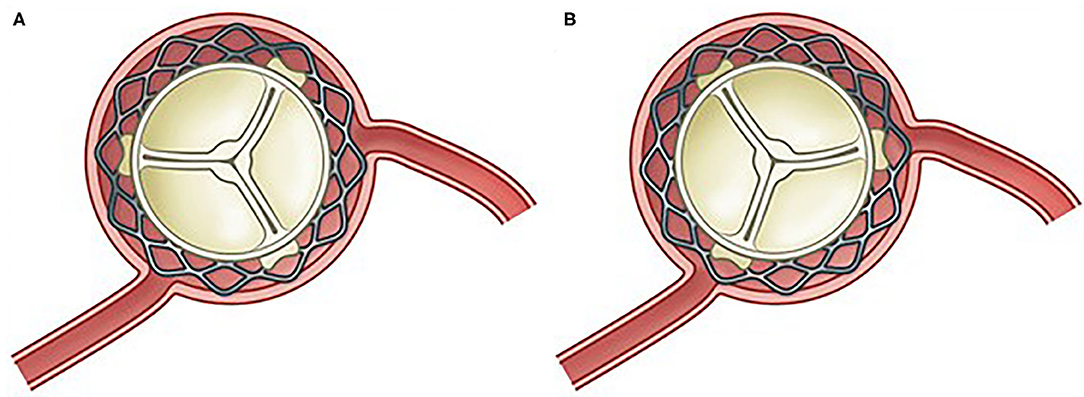
Figure 2. Commissural alignment between native and TAVI valve makes for easy coronary access (A) compared with commissural misalignment (B).
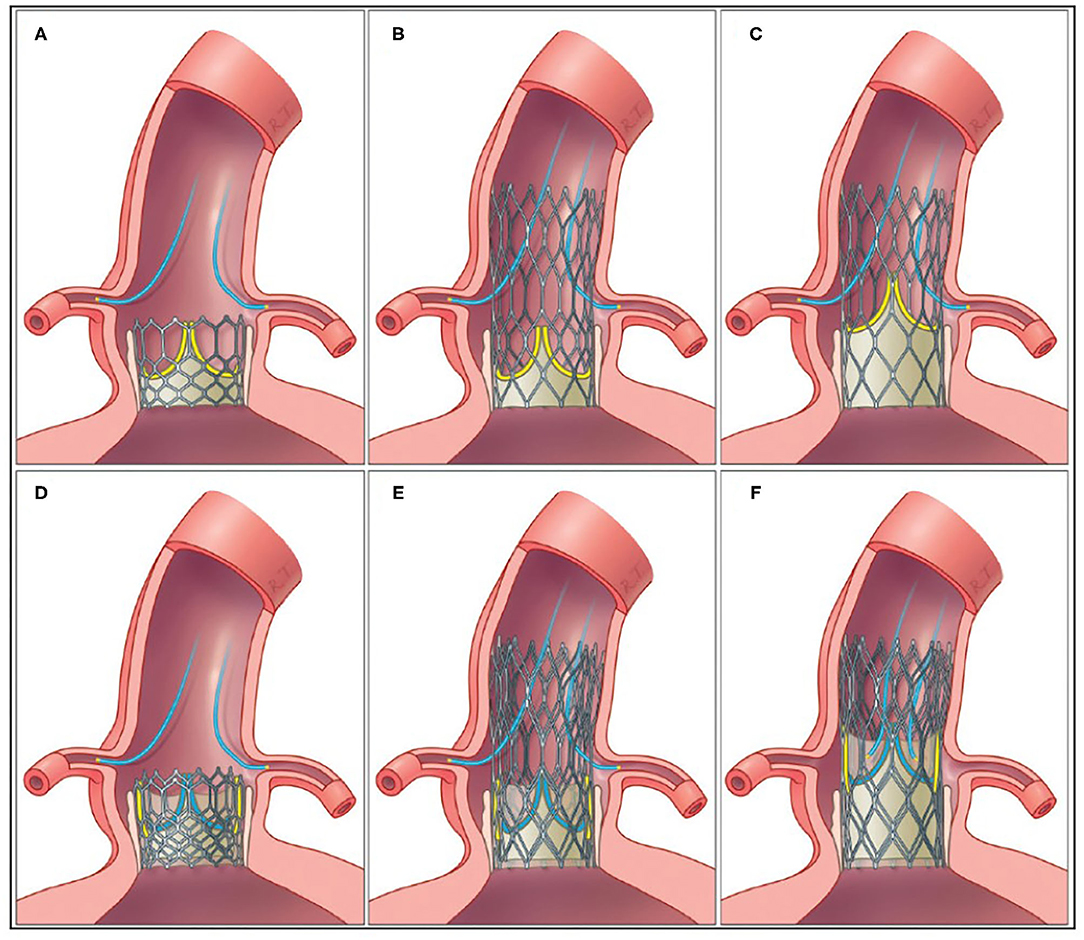
Figure 3. Coronary access after first TAVI with low-frame and intra-annular leaflet position (A), high-frame and intra-annular leaflet position (B), and high-frame and supra-annular leaflet position (C). After TAVI-in-TAVI, access to the coronary arteries may be possible in patients with low-frame and intra-annular leaflet position (D) and high-frame and intra-annular leaflet position (E), whereas, access may be compromised in high-frame and supra-annular leaflet position (F). Yellow leaflets = leaflets in the first implanted THV; blue leaflets = leaflets in the second implanted THV; yellow/gray shading = tissue tunnel.
How to Revascularize Patients Undergoing TAVI?
Revascularization with PCI vs. CABG is another field in cardiovascular medicine of complexity that has gained much attention. In patients with AS and significant CAD the decision of performing CABG + SAVR or TAVI + PCI is even more complex. In the patients already selected for TAVI, percutaneous revascularization with PCI is undeniably the method of choice for revascularization. However, in patients without AS, CABG is preferred over PCI in patients with left main stenosis, three-vessel disease, and SYNTAX score >22, multivessel disease and diabetes or reduced LV function. Thus, as the complexity of CAD increases, the beneficial effect of PCI may be counterbalanced by increasing risk of complications and CABG + SAVR may be superior to PCI + TAVI in these patients. A recent meta-analysis comparing SAVR + CABG vs. TAVI + PCI found only three eligible studies out of 425 screened references (80). Of these, only one study was a randomized trial (79). The meta-analysis found no differences in 30-day safety outcomes (MI, stroke) and 2-year mortality. However, the authors reported differences in revascularization strategies, inaccuracies in surgical risk assessment, and non-uniformity in CAD grading according to SYNTAX score between studies (80). Nevertheless, this evidence suggests that TAVI + PCI is comparable with SAVR + CABG.
Taken together, patients with AS and co-existing CAD are heterogeneous in terms of risk profiles, comorbidities, life expectancy, severity of AS, and CAD as well as symptom burden. Importantly, both the functional severity of CAD (extent of coronary ischemia) and anatomical complexity (SYNTAX score) are highly variable and may both impact on the optimal of treatment and decision-making. Thus, Heart Team decisions focusing on individual patient–orientated treatment are important with contributions from invasive (coronary and structural) and non-invasive cardiologists as well as thoracic surgeons. Future studies may also help in addressing some of these pivotal questions in current Cardiology.
Anti-thrombotic Treatment After PCI?
DAPT is no longer recommended after TAVI as bleeding rates are higher without clear benefits (65, 66). However, TAVI patients who undergo PCI cannot avoid DAPT without increasing the risk of stent thrombosis in exchange for the lower bleeding risk. Moreover, longer DAPT treatment is especially recommended in the case of complex PCI, e.g., of bifurcations or venous grafts. In addition, more than one third of TAVI patients have concomitant atrial fibrillation with an indication for oral anticoagulation therapy (81). As such, the typically frail TAVI patient with atrial fibrillation and a need for complex PCI is exposed to an increased bleeding risk.
Conclusions
TAVI has revolutionized the treatment of severe AS and the indication for TAVI is expanding to still younger and lower-risk patient groups. Important unresolved questions are if, how, and when to treat co-existing CAD. To date, data on these pivotal questions are few, but ongoing clinical trials are greatly awaited and will provide important evidence.
Author Contributions
All authors have read and approved the manuscript and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet. (2006) 368:1005–11. doi: 10.1016/S0140-6736(06)69208-8
2. Iung B, Baron G, Butchart EG, Delahaye F, Gohlke-Bärwolf C, Levang OW, et al. A prospective survey of patients with valvular heart disease in Europe: The Euro Heart Survey on valvular heart disease. Eur Heart J. (2003) 24:1231–43. doi: 10.1016/S0195-668X(03)00201-X
3. Ionescu MI, Pakrashi BC, Mary DAS, Bartek IT, Wooler GH. Replacement of heart valves with frame mounted tissue grafts. Thorax. (1974) 29:56–67. doi: 10.1136/thx.29.1.56
4. Cribier A, Eltchaninoff H, Bash A, Borenstein N, Tron C, Bauer F, et al. Percutaneous transcatheter implantation of an aortic valve prosthesis for calcific aortic stenosis: First human case description. Circulation. (2002) 106:3006–8. doi: 10.1161/01.CIR.0000047200.36165.B8
5. Smith CR, Leon MB, Mack MJ, Miller DC, Moses JW, Svensson LG, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. (2011) 364:2187–98. doi: 10.1056/NEJMoa1103510
6. Adams DH, Popma JJ, Reardon MJ, Yakubov SJ, Coselli JS, Deeb GM, et al. Transcatheter aortic-valve replacement with a self-expanding prosthesis. N Engl J Med. (2014) 370:1790–8. doi: 10.1056/NEJMoa1400590
7. Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. (2010) 363:1597–607. doi: 10.1056/NEJMoa1008232
8. Kapadia SR, Leon MB, Makkar RR, Tuzcu EM, Svensson LG, Kodali S, et al. 5-year outcomes of transcatheter aortic valve replacement compared with standard treatment for patients with inoperable aortic stenosis (PARTNER 1): a randomised controlled trial. Lancet. (2015) 385:2485–91. doi: 10.1016/S0140-6736(15)60290-2
9. Mack MJ, Leon MB, Thourani VH, Makkar R, Kodali SK, Russo M, et al. Transcatheter aortic-valve replacement with a balloon-expandable valve in low-risk patients. N Engl J Med. (2019) 380:1695–705. doi: 10.1056/NEJMoa1814052
10. Popma JJ, Deeb GM, Yakubov SJ, Mumtaz M, Gada H, O'Hair D, et al. Transcatheter aortic-valve replacement with a self-expanding valve in low-risk patients. N Engl J Med. (2019) 380:1706–15. doi: 10.1056/NEJMoa1816885
11. Thyregod HGH, Ihlemann N, Jørgensen TH, Nissen H, Kjeldsen BJ, Petursson P, et al. Five-year clinical and echocardiographic outcomes from the NOTION randomized clinical trial in patients at lower surgical risk. Circulation. (2019) 139:2714–23. doi: 10.1161/CIRCULATIONAHA.118.036606
12. Leon MB, Smith CR, Mack MJ, Makkar RR, Svensson LG, Kodali SK, et al. Transcatheter or surgical aortic-valve replacement in intermediate-risk patients. N Engl J Med. (2016) 374:1609–20. doi: 10.1056/NEJMoa1514616
13. Reardon MJ, Van Mieghem NM, Popma JJ, Kleiman NS, Søndergaard L, Mumtaz M, et al. Surgical or transcatheter aortic-valve replacement in intermediate-risk patients. N Engl J Med. (2017) 376:1321–31. doi: 10.1056/NEJMoa1700456
14. Mack MJ, Leon MB, Smith CR, Miller DC, Moses JW, Tuzcu EM, et al. 5-year outcomes of transcatheter aortic valve replacement or surgical aortic valve replacement for high surgical risk patients with aortic stenosis (PARTNER 1): a randomised controlled trial. Lancet. (2015) 385:2477–84. doi: 10.1016/S0140-6736(15)60308-7
15. Gleason TG, Reardon MJ, Popma JJ, Deeb GM, Yakubov SJ, Lee JS, et al. 5-year outcomes of self-expanding transcatheter versus surgical aortic valve replacement in high-risk patients. J Am Coll Cardiol. (2018) 72:2687–96. doi: 10.1016/j.jacc.2018.08.2146
16. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, Gentile F, et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease. J Am Coll Cardiol. (2020) 77:450–500. doi: 10.1016/j.jacc.2020.11.018
17. Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, et al. 2017 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J. (2017) 38:2739–86. doi: 10.5603/KP.2018.0013
18. Stewart BF, Siscovick D, Lind BK, Gardin JM, Gottdiener JS, Smith VE, et al. Clinical factors associated with calcific aortic valve disease. Cardiovascular health study. J Am Coll Cardiol. (1997) 29:630–4. doi: 10.1016/S0735-1097(96)00563-3
19. Ahn JH, Kim SM, Park SJ, Jeong DS, Woo MA, Jung SH, et al. Coronary microvascular dysfunction as a mechanism of angina in severe AS: prospective adenosine-stress CMR study. J Am Coll Cardiol. (2016) 67:1412–22. doi: 10.1016/j.jacc.2016.01.013
20. Gilard M, Eltchaninoff H, Iung B, Donzeau-Gouge P, Chevreul K, Fajadet J, et al. Registry of transcatheter aortic-valve implantation in high-risk patients. N Engl J Med. (2012) 366:1705–15. doi: 10.1056/NEJMoa1114705
21. Hamm CW, Möllmann H, Holzhey D, Beckmann A, Veit C, Figulla HR, et al. The german aortic valve registry (GARY): in-hospital outcome. Eur Heart J. (2014) 35:1588–98. doi: 10.1093/eurheartj/eht381
22. Thomas M, Schymik G, Walther T, Himbert D, Lefèvre T, Treede H, et al. Thirty-day results of the SAPIEN aortic bioprosthesis European outcome (SOURCE) registry: a European registry of transcatheter aortic valve implantation using the edwards SAPIEN valve. Circulation. (2010) 122:62–9. doi: 10.1161/CIRCULATIONAHA.109.907402
23. Thomas M, Schymik G, Walther T, Himbert D, Lefèvre T, Treede H, et al. One-year outcomes of cohort 1 in the edwards Sapien aortic bioprosthesis european outcome (SOURCE) registry: The European registry of transcatheter aortic valve implantation using the edwards Sapien valve. Circulation. (2011) 124:425–33. doi: 10.1161/CIRCULATIONAHA.110.001545
24. Abdel-Wahab M, Zahn R, Horack M, Gerckens U, Schuler G, Sievert H, et al. Transcatheter aortic valve implantation in patients with and without concomitant coronary artery disease: Comparison of characteristics and early outcome in the German multicenter TAVI registry. Clin Res Cardiol. (2012) 101:973–81. doi: 10.1007/s00392-012-0486-5
25. Ussia GP, Barbanti M, Colombo A, Tarantini G, Petronio AS, Ettori F, et al. Impact of coronary artery disease in elderly patients undergoing transcatheter aortic valve implantation: Insight from the Italian CoreValve Registry. Int J Cardiol. (2013) 167:943–50. doi: 10.1016/j.ijcard.2012.03.089
26. Linke A, Wenaweser P, Gerckens U, Tamburino C, Bosmans J, Bleiziffer S, et al. Treatment of aortic stenosis with a self-expanding transcatheter valve: the International Multi-centre ADVANCE Study. Eur Heart J. (2014) 35:2672–84. doi: 10.1093/eurheartj/ehu162
27. Schymik G, Lefèvre T, Bartorelli AL, Rubino P, Treede H, Walther T, et al. European experience with the second-generation Edwards SAPIEN XT transcatheter heart valve in patients with severe aortic stenosis: 1-year outcomes from the SOURCE XT registry. JACC Cardiovasc Interv. (2015) 8:657–69. doi: 10.1016/j.jcin.2014.10.026
28. Holmes DR, Nishimura RA, Grover FL, Brindis RG, Carroll JD, Edwards FH, et al. Annual outcomes with transcatheter valve therapy. From the STS/ACC TVT registry. Ann Thorac Surg. (2015) 101:789–800. doi: 10.1016/j.athoracsur.2015.10.049
29. Snow TM, Ludman P, Banya W, DeBelder M, MacCarthy PM, Davies SW, et al. Management of concomitant coronary artery disease in patients undergoing transcatheter aortic valve implantation: the United Kingdom TAVI registry. Int J Cardiol. (2015) 199:253–60. doi: 10.1016/j.ijcard.2015.06.166
30. Singh V, Rodriguez AP, Thakkar B, Patel NJ, Ghatak A, Badheka AO, et al. Comparison of outcomes of transcatheter aortic valve replacement plus percutaneous coronary intervention versus transcatheter aortic valve replacement alone in the United States. Am J Cardiol. (2016) 118:1698–704. doi: 10.1016/j.amjcard.2016.08.048
31. Wendler O, Schymik G, Treede H, Baumgartner H, Dumonteil N, Ihlberg L, et al. SOURCE 3 registry: design and 30-day results of the european postapproval registry of the latest generation of the sapien 3 transcatheter heart valve. Circulation. (2017) 135:1123–32. doi: 10.1161/CIRCULATIONAHA.116.025103
32. Sant'Anna FM, Silva EER, Batista LA, Ventura FM, Barrozo CAM, Pijls NHJ. Influence of routine assessment of fractional flow reserve on decision making during coronary interventions. Am J Cardiol. (2007) 99:504–8. doi: 10.1016/j.amjcard.2006.09.097
33. Tonino PAL, Fearon WF, De Bruyne B, Oldroyd KG, Leesar MA, Ver Lee PN, et al. Angiographic versus functional severity of coronary artery stenoses in the FAME study. Fractional flow reserve versus angiography in multivessel evaluation. J Am Coll Cardiol. (2010) 55:2816–21. doi: 10.1016/j.jacc.2009.11.096
34. Tonino PAL, De Bruyne B, Pijls NHJ, Siebert U, Ikeno F, Van't Veer M, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. (2009) 360:213–24. doi: 10.1056/NEJMoa0807611
35. De Bruyne B, Fearon WF, Pijls NHJ, Barbato E, Tonino P, Piroth Z, et al. Fractional flow reserve-guided PCI for stable coronary artery disease. N Engl J Med. (2014) 371:1208–17. doi: 10.1056/NEJMoa1408758
36. De Backer O, Biasco L, Lønborg J, Pedersen F, Holmvang L, Kelbaek H, et al. Long-term outcome of FFR-guided PCI for stable coronary artery disease in daily clinical practice: A propensity scorematched landmark analysis. EuroIntervention. (2016) 11:e1257–66. doi: 10.4244/EIJV11I11A247
37. Stefanini GG, Stortecky S, Cao D, Rat-Wirtzler J, O'Sullivan CJ, Gloekler S, et al. Coronary artery disease severity and aortic stenosis: Clinical outcomes according to SYNTAX score in patients undergoing transcatheter aortic valve implantation. Eur Heart J. (2014) 35:2530–40. doi: 10.1093/eurheartj/ehu074
38. Sankaramangalam K, Banerjee K, Kandregula K, Mohananey D, Parashar A, Jones BM, et al. Impact of coronary artery disease on 30-day and 1-year mortality in patients undergoing transcatheter aortic valve replacement: a meta-analysis. J Am Heart Assoc. (2017) 6:e006092. doi: 10.1161/JAHA.117.006092
39. Vilalta V, Asmarats L, Ferreira-Neto AN, Maes F, de Freitas Campos Guimarães L, Couture T, et al. Incidence, clinical characteristics, and impact of acute coronary syndrome following transcatheter aortic valve replacement. JACC Cardiovasc Interv. (2018) 11:2523–33. doi: 10.1016/j.jcin.2018.09.001
40. Clyne CA, Arrighi JA, Maron BJ, Dilsizian V, Bonow RO, Cannon RO. Systemic and left ventricular responses to exercise stress in asymptomatic patients with valvular aortic stenosis. Am J Cardiol. (1991) 68:1469–76. doi: 10.1016/0002-9149(91)90281-O
41. Maffei S, Baroni M, Terrazzi M, Paoli F, Ferrazzi P, Biagini A. Preoperative assessment of coronary artery disease in aortic stenosis: a dipyridamole echocardiographic study. Ann Thorac Surg. (1998) 65:397–402. doi: 10.1016/S0003-4975(97)01177-6
42. Patsilinakos SP, Kranidis AI, Antonelis IP, Filippatos G, Houssianakou IK, Zamanis NI, et al. Detection of coronary artery disease in patients with severe aortic stenosis with non-invasive methods. Angiology. (1999) 50:309–17. doi: 10.1177/000331979905000406
43. Cremer PC, Khalaf S, Lou J, Rodriguez L, Cerqueira MD, Jaber WA. Stress positron emission tomography is safe and can guide coronary revascularization in high-risk patients being considered for transcatheter aortic valve replacement. J Nucl Cardiol. (2014) 21:1001–10. doi: 10.1007/s12350-014-9928-y
44. Burgstahler C, Kunze M, Gawaz MP, Rasche V, Wöhrle J, Hombach V, et al. Adenosine stress first pass perfusion for the detection of coronary artery disease in patients with aortic stenosis: a feasibility study. Int J Cardiovasc Imaging. (2008) 24:195–200. doi: 10.1007/s10554-007-9236-6
45. Hamdan A, Wellnhofer E, Konen E, Kelle S, Goitein O, Andrada B, et al. Coronary CT angiography for the detection of coronary artery stenosis in patients referred fortranscatheter aortic valve replacement. J Cardiovasc Comput Tomogr. (2015) 9:31–41. doi: 10.1016/j.jcct.2014.11.008
46. Case BC, Yerasi C, Forrestal BJ, Musallam A, Chezar-Azerrad C, Hahm J, et al. Utility of routine invasive coronary angiography prior to transcatheter aortic valve replacement. Cardiovasc Revascularization Med. (2020). doi: 10.1016/j.carrev.2020.11.022. [Epub ahead of print].
47. Taylor CA, Fonte TA, Min JK. Computational fluid dynamics applied to cardiac computed tomography for non-invasive quantification of fractional flow reserve: scientific basis. J Am Coll Cardiol. (2013) 61:2233–41. doi: 10.1016/j.jacc.2012.11.083
48. Michail M, Ihdayhid A-R, Comella A, Thakur U, Cameron JD, McCormick LM, et al. Feasibility and validity of computed tomography-derived fractional flow reserve in patients with severe aortic stenosis. Circ Cardiovasc Interv. (2020) 14:e009586. doi: 10.1161/CIRCINTERVENTIONS.120.009586
49. Chen J, Wetzel LH, Pope KL, Meek LJ, Rosamond T, Walker CM. FFR CT : current status. Am J Roentgenol. (2020) 216:640–8. doi: 10.2214/AJR.20.23332
50. Pijls NHJ, de Bruyne B, Peels K, van der Voort PH, Bonnier HJRM, Bartunek J, et al. Measurement of fractional flow reserve to assess the functional severity of coronary-artery stenoses. N Engl J Med. (1996) 334:1703–8. doi: 10.1056/NEJM199606273342604
51. Lunardi M, Scarsini R, Venturi G, Pesarini G, Pighi M, Gratta A, et al. Physiological versus angiographic guidance for myocardial revascularization in patients undergoing transcatheter aortic valve implantation. J Am Heart Assoc. (2019) 8:e012618. doi: 10.1161/JAHA.119.012618
52. Pesarini G, Scarsini R, Zivelonghi C, Piccoli A, Gambaro A, Gottin L, et al. Functional assessment of coronary artery disease in patients undergoing transcatheter aortic valve implantation: influence of pressure overload on the evaluation of lesions severity. Circ Cardiovasc Interv. (2016) 9:e004088. doi: 10.1161/CIRCINTERVENTIONS.116.004088
53. Fournier S, Harbaoui B, Muller O. Letter by fournier et al. regarding article, “functional assessment of coronary artery disease in patients undergoing transcatheter aortic valve implantation: influence of pressure overload on the evaluation of lesions severity.” Circ Cardiovasc Interv. (2017). 10:e004772. doi: 10.1161/CIRCINTERVENTIONS.116.004772
54. Scarsini R, Lunardi M, Venturi G, Pighi M, Tavella D, Pesarini G, et al. Long-term variations of FFR and iFR after transcatheter aortic valve implantation. Int J Cardiol. (2020) 317:37–41. doi: 10.1016/j.ijcard.2020.05.085
55. Cerqueira MD, Verani MS, Schwaiger M, Heo J, Iskandrian AS. Safety profile of adenosine stress perfusion imaging: Results from the adenoscan multicenter trial registry. J Am Coll Cardiol. (1994) 23:384–9. doi: 10.1016/0735-1097(94)90424-3
56. Strååt E, Henriksson P, Edlund A. Adenosine provokes myocardial ischaemia in patients with ischaemic heart disease without increasing cardiac work. J Intern Med. (1991) 230:319–23. doi: 10.1111/j.1365-2796.1991.tb00451.x
57. Strauer BE, Beer K, Heitlinger K, Höfling B. Left ventricular systolic wall stress as a primary determinant of myocardial oxygen consumption: comparative studies in patients with normal left ventricular function, with pressure and volume overload and with coronary heart disease. Basic Res Cardiol. (1977) 72:306–13. doi: 10.1007/BF01906378
58. Monrad ES, Hess OM, Murakami T, Nonogi H, Corin WJ, Krayenbuehl HP. Time course of regression of left ventricular hypertrophy after aortic valve replacement. Circulation. (1988) 77:1345–55. doi: 10.1161/01.CIR.77.6.1345
59. Smits PC, Abdel-Wahab M, Neumann F-J, Boxma-de Klerk BM, Lunde K, Schotborgh CE, et al. Fractional flow reserve–guided multivessel angioplasty in myocardial infarction. N Engl J Med. (2017) 376:1234–44. doi: 10.1056/NEJMoa1701067
60. Pavasini R, Biscaglia S, Barbato E, Tebaldi M, Dudek D, Escaned J, et al. Complete revascularization reduces cardiovascular death in patients with ST-segment elevation myocardial infarction and multivessel disease: systematic review and meta-analysis of randomized clinical trials. Eur Heart J. (2020) 41:4103–10. doi: 10.1093/eurheartj/ehz896
61. Fearon WF, Nishi T, De Bruyne B, Boothroyd DB, Barbato E, Tonino P, et al. Clinical outcomes and cost-effectiveness of fractional flow reserve-guided percutaneous coronary intervention in patients with stable coronary artery disease. Circulation. (2018) 137:480–7. doi: 10.1161/CIRCULATIONAHA.117.031907
62. De Bruyne B, Pijls NHJ, Kalesan B, Barbato E, Tonino PAL, Piroth Z, et al. Fractional flow reserve–guided PCI versus medical therapy in stable coronary disease. N Engl J Med. (2012) 367:991–1001. doi: 10.1056/NEJMoa1205361
63. van Nunen LX, Zimmermann FM, Tonino PAL, Barbato E, Baumbach A, Engstrøm T, et al. Fractional flow reserve versus angiography for guidance of PCI in patients with multivessel coronary artery disease (FAME): 5-year follow-up of a randomised controlled trial. Lancet. (2015) 386:1853–60. doi: 10.1016/S0140-6736(15)00057-4
64. Engstrøm T, Kelbæk H, Helqvist S, Høfsten DE, Kløvgaard L, Holmvang L, et al. Complete revascularisation versus treatment of the culprit lesion only in patients with ST-segment elevation myocardial infarction and multivessel disease (DANAMI-3—PRIMULTI): an open-label, randomised controlled trial. Lancet. (2015) 386:665–71. doi: 10.1016/S0140-6736(15)60648-1
65. Nijenhuis VJ, Brouwer J, Delewi R, Hermanides RS, Holvoet W, Dubois CLF, et al. Anticoagulation with or without clopidogrel after transcatheter aortic-valve implantation. N Engl J Med. (2020) 382:1696–707. doi: 10.1056/NEJMoa1915152
66. Rodés-Cabau J, Masson JB, Welsh RC, Garcia del Blanco B, Pelletier M, Webb JG, et al. Aspirin versus aspirin plus clopidogrel as antithrombotic treatment following transcatheter aortic valve replacement with a balloon-expandable valve: the ARTE (Aspirin Versus Aspirin + Clopidogrel Following Transcatheter Aortic Valve Implantation) randomized clinical trial. JACC Cardiovasc Interv. (2017) 10:1357–65. doi: 10.1016/j.jcin.2017.04.014
67. Faroux L, Campelo-Parada F, Munoz-Garcia E, Nombela-Franco L, Fischer Q, Donaint P, et al. Procedural characteristics and late outcomes of percutaneous coronary intervention in the workup pre-TAVR. JACC Cardiovasc Interv. (2020) 13:2601–13. doi: 10.1016/j.jcin.2020.07.009
68. Lønborg J, Engstrøm T, Kelbæk H, Helqvist S, Kløvgaard L, Holmvang L, et al. Fractional flow reserve–guided complete revascularization improves the prognosis in patients with ST-segment–elevation myocardial infarction and severe non-culprit disease. Circ Cardiovasc Interv. (2017) 10:e004460. doi: 10.1161/CIRCINTERVENTIONS.116.004460
69. Johnson NP, Tóth GG, Lai D, Zhu H, Açar G, Agostoni P, et al. Prognostic value of fractional flow reserve: Linking physiologic severity to clinical outcomes. J Am Coll Cardiol. (2014) 64:1641–54. doi: 10.1016/j.jacc.2014.07.973
70. Barbato E, Toth GG, Johnson NP, Pijls NHJ, Fearon WF, Tonino PAL, et al. A prospective natural history study of coronary atherosclerosis using fractional flow reserve. J Am Coll Cardiol. (2016) 68:2247–55. doi: 10.1016/j.jacc.2016.08.055
71. Ahn JM, Park DW, Shin ES, Koo BK, Nam CW, Doh JH, et al. Fractional flow reserve and cardiac events in coronary artery disease: data from a prospective IRIS-FFR Registry (Interventional Cardiology Research Incooperation Society Fractional Flow Reserve). Circulation. (2017) 135:2241–51. doi: 10.1161/CIRCULATIONAHA.116.024433
72. Neumann FJ, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur Heart J. (2019) 40:87–165. doi: 10.1093/eurheartj/ehy855
73. Xaplanteris P, Fournier S, Pijls NHJ, Fearon WF, Barbato E, Tonino PAL, et al. Five-year outcomes with PCI guided by fractional flow reserve. N Engl J Med. (2018) 379:250–9. doi: 10.1056/NEJMoa1803538
74. Tegn N, Abdelnoor M, Aaberge L, Endresen K, Smith P, Aakhus S, et al. Invasive versus conservative strategy in patients aged 80 years or older with non-ST-elevation myocardial infarction or unstable angina pectoris (After Eighty study): An open-label randomised controlled trial. Lancet. (2016) 387:1057–65. doi: 10.1016/S0140-6736(15)01166-6
75. Khawaja MZ, Wang D, Pocock S, Redwood SR, Thomas MR. The percutaneous coronary intervention prior to transcatheter aortic valve implantation (ACTIVATION) trial: study protocol for a randomized controlled trial. Trials. (2014) 15:300. doi: 10.1186/1745-6215-15-300
76. Barbanti M, Costa G, Picci A, Criscione E, Reddavid C, Valvo R, et al. coronary cannulation after transcatheter aortic valve replacement: the RE-ACCESS study. JACC Cardiovasc Interv. (2020) 13:2542–55. doi: 10.1016/j.jcin.2020.07.006
77. Tang GHL, Zaid S, Fuchs A, Yamabe T, Yazdchi F, Gupta E, et al. Alignment of transcatheter aortic-valve neo-commissures (ALIGN TAVR): impact on final valve orientation and coronary artery overlap. JACC Cardiovasc Interv. (2020) 13:1030–42. doi: 10.1016/j.jcin.2020.02.005
78. Yang Y, Huang FY, Huang BT, Xiong TY, Pu XB, Chen SJ, et al. The safety of concomitant transcatheter aortic valve replacement and percutaneous coronary intervention. Medicine. (2017) 96:e8919. doi: 10.1097/MD.0000000000008919
79. Søndergaard L, Popma JJ, Reardon MJ, Van Mieghem NM, Deeb GM, Kodali S, et al. Comparison of a complete percutaneous versus surgical approach to aortic valve replacement and revascularization in patients at intermediate surgical risk: results from the randomized SURTAVI trial. Circulation. (2019) 140:1296–305. doi: 10.1161/CIRCULATIONAHA.118.039564
80. Tarus A, Tinica G, Bacusca A, Artene B, Popa IV, Burlacu A. Coronary revascularization during treatment of severe aortic stenosis: a meta-analysis of the complete percutaneous approach (PCI plus TAVR) versus the complete surgical approach (CABG plus SAVR). J Card Surg. (2020) 35:2009–16. doi: 10.1111/jocs.14814
81. Tarantini G, Mojoli M, Windecker S, Wendler O, Lefèvre T, Saia F, et al. Prevalence and impact of atrial fibrillation in patients with severe aortic stenosis undergoing transcatheter aortic valve replacement an analysis from the SOURCE XT prospective multicenter registry. JACC Cardiovasc Interv. (2016) 9:937–46. doi: 10.1016/j.jcin.2016.01.037
Keywords: transcatheter aortic valve implantation, percutaneous coronary intervention, revascualrization, fractional flow reserve, coronary artery diasease
Citation: Sabbah M, Engstrøm T, De Backer O, Søndergaard L and Lønborg J (2021) Coronary Assessment and Revascularization Before Transcutaneous Aortic Valve Implantation: An Update on Current Knowledge. Front. Cardiovasc. Med. 8:654892. doi: 10.3389/fcvm.2021.654892
Received: 17 January 2021; Accepted: 18 March 2021;
Published: 21 May 2021.
Edited by:
Micha Tobias Maeder, Kantonsspital St. Gallen, SwitzerlandReviewed by:
Moritz Seiffert, University Heart and Vascular Center Hamburg (UHZ), GermanyCristina Aurigemma, Catholic University of the Sacred Heart, Italy
Copyright © 2021 Sabbah, Engstrøm, De Backer, Søndergaard and Lønborg. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Muhammad Sabbah, TXVoYW1tYWQuc2FiYmFoLjAxQHJlZ2lvbmguZGs=