 Atul Kumar Singh1
Atul Kumar Singh1 Abdulelah Aljohani2*
Abdulelah Aljohani2* Pshtiwan Shakor3Bankole Osita Awuzie4
Pshtiwan Shakor3Bankole Osita Awuzie4 S. M. Jamil Uddin5B. T. Shivendra1
S. M. Jamil Uddin5B. T. Shivendra1- 1Department of Civil Engineering, Dayananda Sagar College of Engineering, Bengaluru, India
- 2Department of Civil Engineering, Faculty of Engineering, Al-Baha University, Al-Baha, Saudi Arabia
- 3Technical College of Engineering, Sulaimani Polytechnic University, Sulaymaniyah, Iraq
- 4Construction Management and Quantity Surveying, Faculty of Engineering and Built Environment, University of Johannesburg, Johannesburg, South Africa
- 5Department of Construction Management, Colorado State University, Fort Collins, CO, United States
In the construction industry, irregular schedules and long hours disrupt workers’ circadian rhythms, adversely affecting their safety and health. While studies have shown that sleep timing influences safety and health, they often overlook sleep quantity, work-shift start time, and a broad range of safety and health outcomes. To fill this gap, this study examines the relationship between circadian rhythm and safety health factors, including psychological issues, wellbeing, behavioral issues, altruistic behaviors, sleep quantity, starting hours at work, and parental care in 1,400 construction workers using a questionnaire. We investigated safety health using scales for psychological issues (0–34), wellbeing (0–24), behavioral issues (0–29), and altruistic behaviors (0–27). Midsleep time on weekends estimated circadian rhythm, with multilevel regressions adjusting for sleep quantity, work start time, and various characteristics. Results showed average midsleep at 04:11 h, with a 1 h delay associated with increased psychological issues (0.37), behavioral issues (3.0%), decreased wellbeing (0.19), and decreased altruistic behaviors (0.18). These findings highlight a correlation between early circadian rhythm and poor safety health, independent of sleep quantity and work-shift start time. Addressing circadian rhythm disruptions could be crucial for improving safety health outcomes, suggesting that work schedule adjustments and better sleep practices may mitigate adverse effects on workers’ health and wellbeing.
1 Introduction
The construction industry plays an important role in the global economy, employing millions of workers worldwide and contributing significantly to economic growth and development (Abdul Azeez and Jawed Akhtar, 2019). However, the physically demanding nature of construction work, which often involves long hours, physically and safety daunting tasks, and irregular schedules, can negatively impact the safety health and wellbeing of workers (Boschman et al., 2013; Turner and Lingard, 2020). In recent years, there has been growing recognition of the high prevalence of safety health problems among construction workers and the need for targeted interventions and strategies to address this issue (Chan et al., 2016; Fagbenro et al., 2023; Greiner et al., 2022; Kotera et al., 2020; Turner and Lingard, 2020).
Safety health problems, such as depression, anxiety, and stress, are common among construction workers and can have significant negative impacts on both individual workers and the industry as a whole. Recent studies have highlighted that construction workers have significantly higher rates of depression and anxiety compared to the general population (Gómez-Salgado et al., 2023; Jacobsen et al., 2013; Langdon and Sawang, 2018; Palaniappan et al., 2022). These safety health problems can lead to a range of adverse outcomes, including reduced productivity, increased absenteeism, and a higher risk of accidents and injuries on the job site (Chan et al., 2020; Jacobsen et al., 2013).
Several factors have been identified as contributing factors to the high rates of safety health problems among construction workers. These include job-related stressors, such as high workload, time pressure, and job insecurity, as well as individual factors, such as unhealthy lifestyle behaviors and limited access to safety health services (Chan et al., 2020; Langdon and Sawang, 2018). However, one factor that has received relatively little attention in the literature is the role of circadian rhythm disruption in the development of safety health problems among construction workers.
Circadian rhythms are internal biological processes that regulate various physiological functions, including the sleep-wake cycle, on a roughly 24-hour schedule (Mohawk et al., 2012). These rhythms are essential for maintaining optimal physical and safety health of an individual. Disruption of circadian rhythms, such as that experienced by shift workers or those with irregular sleep schedules, has been linked to a range of negative health outcomes, including sleep disturbances, metabolic disorders, and safety health problems (Kecklund and Axelsson, 2016; Sharma et al., 2008).
Construction workers may be particularly vulnerable to circadian rhythm disruption due to the nature of their work schedules and the demands of the industry (Singh and Kumar, 2022; Singh and Prasath Kumar, 2022; Singh and Kumar, 2023; Singh and Kumar, 2024a; Singh and Kumar, 2024b). Long work hours, early morning starts, overtime, and irregular schedules are common in construction, all of which can interfere with the body’s natural circadian rhythms (Dong, 2005). This disruption may, in turn, contribute to the high rates of safety and health problems observed among construction workers.
Despite the potential link between circadian rhythm disruption and safety health in construction workers, there has been limited research on this topic to date. While some studies have examined the relationship between shift work and safety health in construction workers (Zhao et al., 2019; Kotera et al., 2020), few have explored the broader impact of circadian rhythm disruption on a range of safety health outcomes. Moreover, there is a need for research that takes into account other relevant factors, such as sleep duration and work schedule characteristics, to better understand the independent effects of circadian rhythm on safety and health.
The current study aims to address these gaps in the literature by examining the relationship between circadian rhythm and a comprehensive set of safety health indicators in a large sample of construction workers in India. India has one of the largest construction industries in the world, employing over 70 million workers (Chellappa et al., 2021; Statista, 2024), however, research on the safety health of Indian construction workers is limited, despite the high prevalence of safety health problems among construction workers.
To fill the above-mentioned gap, The objectives of this research are:
1. To examine the relationship between circadian rhythm and various safety health factors in construction workers, including psychological issues, wellbeing, behavioral issues, altruistic behaviors, sleep quantity, and starting hours at work.
2. To investigate the specific impact of midsleep time on weekends as an estimate of circadian rhythm on safety health outcomes, adjusting for sleep quantity, initial work start time, and individual, family, and geographical characteristics.
3. To provide insights that can inform potential interventions, such as work schedule adjustments and sleep practice improvements, aimed at enhancing the safety and health of construction workers.
The significance of this study lies in its comprehensive examination of the relationship between circadian rhythm and a broad range of safety and health factors in construction workers. By controlling potential confounding variables, such as sleep duration and work schedule factors, this study seeks to isolate the specific effects of circadian rhythm on safety health outcomes. By addressing gaps in previous research, which often overlooked sleep quantity and work-shift start times, this study provides a more holistic understanding of how disrupted circadian rhythms impact psychological issues, wellbeing, behavioral issues, and altruistic behaviors. The findings highlight the importance of considering circadian rhythms in workplace health and safety strategies, offering evidence that could lead to targeted interventions such as adjusting work schedules and promoting better sleep practices. These insights have the potential to inform the development of targeted interventions and policies to promote the safety, health, and wellbeing of construction workers, both in India and globally. Ultimately, improving the overall safety, health, and wellbeing of construction workers could enhance productivity and reduce workplace accidents and health issues.
2 Literature review
2.1 Circadian rhythms
Circadian rhythms are endogenous biological processes that oscillate on a roughly 24-hour cycle, regulating numerous physiological functions and behaviors (Mohawk et al., 2012). These rhythms are generated by a central pacemaker in the suprachiasmatic nucleus (SCN) of the hypothalamus and are synchronized to the external environment primarily through light exposure (Golombek and Rosenstein, 2010; Mieda, 2020). Circadian rhythms play a crucial role in regulating sleep-wake cycles, hormone secretion, body temperature, and cognitive performance (Albrecht, 2012). Individual differences in circadian timing, known as chronotypes, range from early types (“larks”) to late types (“owls”) (Adan et al., 2012). Several studies have identified different internal factors such as genetics, age, etc. and external factors such as work schedule, temperature, light etc. that help determine the chronotype (Duffy et al., 2001; Roenneberg et al., 2004; Roenneberg et al., 2007; Nováková et al., 2013). Misalignment between an individual’s circadian rhythm and external time cues, such as work schedules or social demands, can lead to circadian disruption and associated health problems (Baron and Reid, 2014; Sletten et al., 2020). Shift work, jet lag, and irregular sleep schedules are common causes of circadian disruption (Chellappa et al., 2020; Vetter, 2020). In the construction industry, workers often face early morning starts and long work hours, which can lead to misalignment of their circadian rhythms (Dong, 2005; Sathvik et al., 2023). Studies demonstrated that construction workers have significantly lower sleep efficiency and more fragmented sleep compared to office workers, likely due to early work start times and physical demands of the job (Juda et al., 2013).
Chronic circadian disruption has been linked to numerous health issues, including sleep disorders, cardiovascular disease, metabolic disorders, cancer, and safety health problems (Kecklund and Axelsson, 2016; James et al., 2017). A meta-analysis by Kecklund and Axelsson (2016) found that shift work was associated with a 17% increased risk of cardiovascular disease and a 25%–40% increased risk of diabetes. In the construction industry, workers with poor sleep quality have a significantly higher risk of occupational injuries compared to those with good sleep quality (Cheng et al., 2012). Strategies to minimize circadian disruption and promote healthy circadian rhythms include maintaining a regular sleep schedule, minimizing light exposure before bedtime, and optimizing work schedules to align with natural circadian preferences (Arendt, 2010). In the construction industry, implementing interventions such as flexible work hours and educating workers about sleep hygiene could help mitigate the negative effects of circadian disruption (Järnefelt et al., 2012).
2.2 Safety health in construction workers
The construction industry is a high-risk sector for safety health problems, with workers facing numerous stressors that can contribute to the development of psychiatric disorders and psychological distress issues (Chan et al., 2016; Kotera et al., 2020; Turner and Lingard, 2020). Studies found that construction workers have significantly higher rates of depression, anxiety, and stress than other industries and professions (Milner et al., 2017; Harris et al., 2022). Several work-related factors have been identified as contributing to poor safety health among construction workers. Long and irregular work hours, physically demanding tasks, high job strain, and low job control are common stressors in the industry (Boschman et al., 2013). Construction workers who report high physical demands and low job control usually show a significantly higher risk of safety health problems compared to those with low physical demands and high job control (Boschman et al., 2013).
Shift work and circadian rhythm disruption are also prevalent in the construction industry and have been linked to safety and health issues. A systematic review by Zhao et al. (2019) found that shift workers had a significantly higher risk of depression compared to day workers. Studies also reported that construction workers who worked night shifts had a higher prevalence of depressive symptoms compared to day shift workers (Kawabe et al., 2015; Angerer et al., 2017). Sleep disturbances, which are often associated with circadian rhythm disruption, have also been identified as a risk factor for safety health problems in construction workers (Dong et al., 2017). Dong et al. (2017) also found that construction workers who reported shorter sleep duration (<7 h per night) and poor sleep quality had a significantly higher risk of depression compared to those with adequate sleep duration and good sleep quality. The consequences of poor safety and health in the construction industry are significant. Safety health problems have been associated with increased risk of accidents and injuries, higher construction costs, absenteeism, presenteeism, and reduced productivity (Gosselin et al., 2013; Jacobsen et al., 2013).
2.3 Research gap
Despite the high prevalence and significant consequences of safety health problems, construction workers often face barriers to accessing safety health services, including stigma, low safety health literacy, and a lack of industry-specific support programs (Roche et al., 2016). There is a clear need for targeted interventions and policies to promote safety health and wellbeing in this vulnerable population. Given the links between circadian rhythm disruption, sleep disturbances, and safety health problems in construction workers, there is a need for further research to better understand these relationships and develop effective interventions. The current study aims to address this gap by comprehensively examining the associations between circadian rhythm, sleep duration, work schedules, and a broad range of safety health outcomes in a large sample of construction workers in India.
3 Research methodology
A longitudinal study was conducted among 1,400 workers aged 20–49 years recruited from five construction companies in India. Surveys were conducted using a two-stage cluster sampling approach and a weighted probability method to ensure a balanced representation of company characteristics, such as religion, the size of the community, the size of the company, and the language of instruction (Singh and Kumar, 2024a). Questionnaires were distributed to construction workers who voluntarily participated in the study. Workers who were younger than 20 years (n = 30) and older than 50 years (n = 45) and those whose survey weights were unavailable (n = 120) were excluded. Figure 1 provides a summary of the adopted research methodology. The subsequent subsections offer detailed explanations of the implemented research approach.
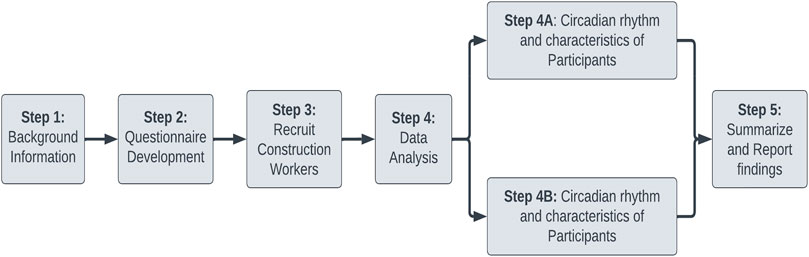
Figure 1. Adopted research methodology.
3.1 Measures of sleep
Construction workers were asked for their normal wake and bedtimes during the previous week, both on company workdays and weekends (Xu et al., 2016; Liang et al., 2018). The circadian rhythm was estimated by considering the phase of entrainment from the calculated local time at mid-sleep on free nights. This study was conducted on a free night to represent the natural internal clock more accurately. On free nights, a person who falls asleep at midnight and wakes up at 8 am has an estimated circadian rhythm of 4 am, which represents the midpoint between sleep and wake. Sleep debt accrued during the construction company week was corrected using the weekend as a proxy for free nights. Moreover, values that were greater than three standard deviations from the mean were excluded (n = 221). A three-group analysis was conducted to compare the early, intermediate, and late circadian rhythms. The average number of hours of sleep per day on company days was calculated by subtracting the reported bedtime from the reported waking time. Means were excluded when the deviation exceeded three standard deviations (n = 515).
3.2 Indicators of safety health
Four indices of safety health were included in the questionnaire: psychological issues (ten items; Cronbach’s alpha = 0.89; score sum range 0–34), psychological wellbeing (six items; Cronbach’s alpha = 0.74; score sum range 0–24), behavioural issues (eight items; Cronbach’s alpha = 0.81; score sum range 0–29), and altruistic behaviors (six items; Cronbach’s alpha = 0.89; score sum range 0–27) (Liang et al., 2017; Saxena et al., 2020). A panel of experts developed these indicators for the questionnaire survey, and they were found to possess both concurrent and content validity.
3.3 Covariates
Several potential confounding variables were considered in this analysis. Adjustments were made for worker characteristics, such as age, sex, travel time to work (<4, 3–13, 14–28, 29–60, or >60 min), sedentary time, level of physical activity, daily cigarette consumption (no/yes), daily alcohol consumption (no/yes), family responsibilities, type of worker (skilled/semi-skilled/unskilled), and company information, such as the initial time, and latitude. The participant’s level of physical activity was determined by measuring the number of days in the past week they were physically active for an hour or more (0–7). The number of hours spent watching TV or using the telephone per day during the week was used to estimate the amount of sedentary time (>3 h vs. 3 h). Family responsibility was assessed using the Family Responsibility Scale IV, which has seven items that reflect common indicators of family wealth (range of total scores: 7–20). Family support items (1 = agree to 7 = disagree) and family equation frequency (1 = never to 6 = daily) were used as substitute measures of parental involvement in the daily schedule, as reported previously (Gulliver et al., 2010; Morgan et al., 2014). The work-shift start time of a construction company was obtained from the company’s website or by directly contacting the company.
3.4 Statistical analysis
Safety health indicators among the companies were regressed on circadian rhythms using multilevel generalized linear regression models. The models were adjusted to consider the characteristics of the worker, their family, type of employee, company, and survey season. For each safety health indicator, three models were developed, adjusting for individual characteristics, family characteristics, worker type, company characteristics, and the season. Model 1 comprised of circadian rhythm, Model 2 comprised of circadian rhythm, Model 3 comprised of circadian rhythm, and Model 4 comprised of sleep quantity. The generalized linear models were fitted with Gaussian family identities, except for behavioral issues, which were fitted with log links because the distribution of data was right-skewed. Behavioural issues were expressed as a percentage change in the score of behavioral issues for every unit change in the covariates. The Wald test was used to determine how the company’s work-shift start time interacted with the length of sleep to determine the effects of each on circadian rhythms.
Multiple sensitivity analyses confirmed the validity of the primary findings. There was a slight difference in the distribution of sleep quantity on company days between those with an initial circadian rhythm and those with a late circadian rhythm. The analyses were conducted using only those participants (n = 1,400) whose sleep duration was between 07:00 and 11:00 h (5th and >95th percentile) on company days. The “fp” command in STATA [21] was used to model the circadian rhythm as a fractional polynomial of the first order to investigate nonlinearity. Few covariates had missing data, except for circadian rhythm (15%), sleep quantity (13%), family equations (13%), parental support (9%), and sedentary time (8%). In STATA, the “mi” command was used to impute missing values using multiple imputations through chained equations. All analyses were conducted in STATA version 14.2 and weighted using post-stratification weights to ensure that the results are representative of construction companies in India.
4 Results
The sleep-mid phase lasted 05:22 hr (SD = 02:34 h). The sample characteristics are shown in Table 1, using the initial (23:45–03:47 h), intermediate (03:47–04:58 h), and late (04:58–08:45 h) circadian rhythms. In addition to being older, skilled, and having shorter sleep than others, workers with a late circadian rhythm reported fewer family dinners and less family support. There was a negative correlation between circadian rhythm and sleep quantity on company days (r = −0.30) and a weak correlation between circadian rhythm and the company work-shift start time (r = 0.06). The average scores for psychological issues, psychological wellbeing, behavioral issues, and altruistic behaviors ranged from 29.7 (SD = 7.2) to 19.0 (SD = 4.2). There was an average sleep duration of 9:45 h on company days (SD = 1:17 h, range 5:08 to 14:00 h), and an average initial time of 09:45 h (SD = 0:18 h, range 08:59–10:46 h).
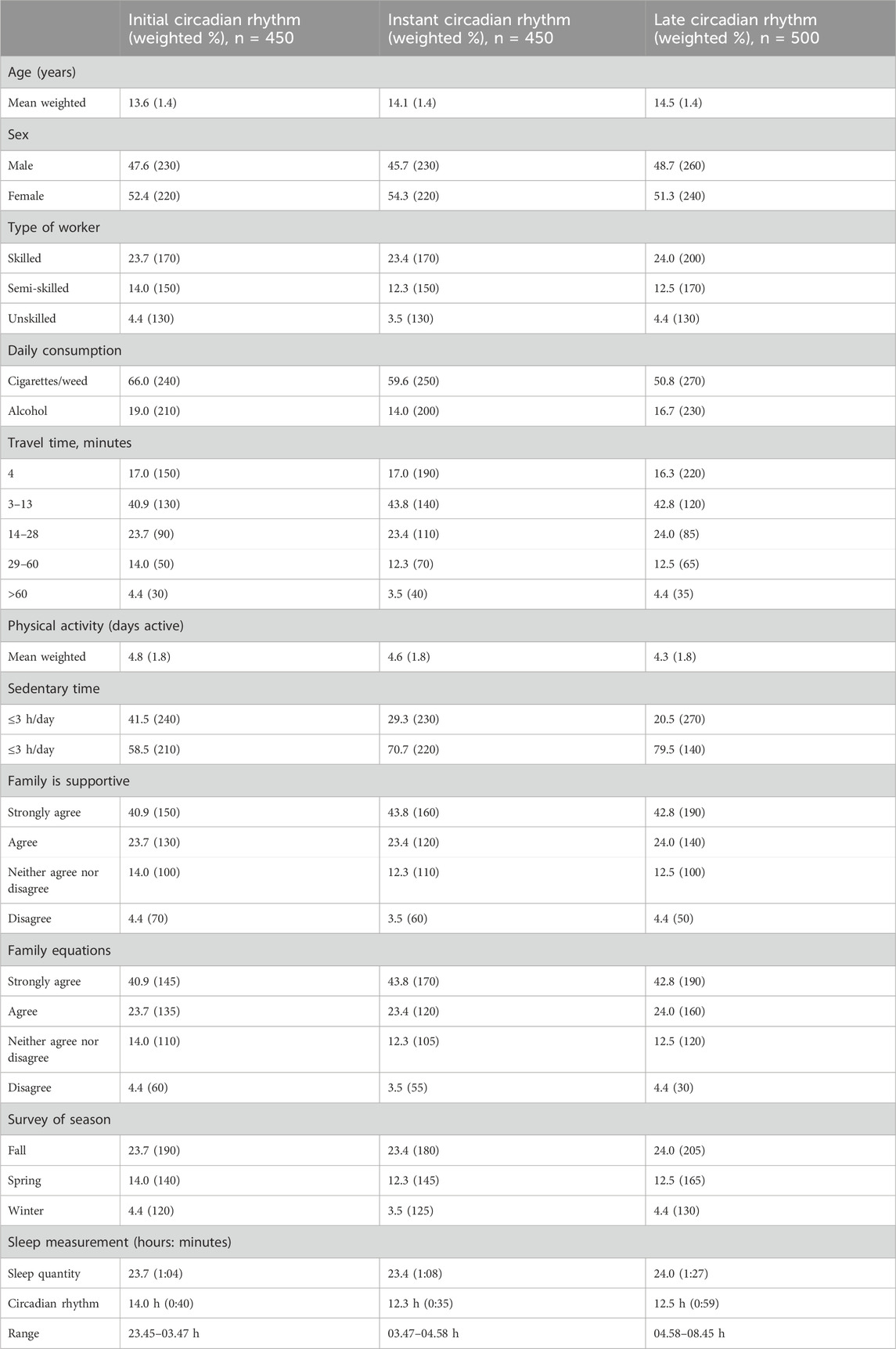
Table 1. Circadian rhythm and characteristics of participants of the questionnaire survey (n = 1,400).
To ensure the robustness of this analysis, all covariates as detailed in Tables 2, 3 were systematically controlled for. The presence of psychological problems, psychological wellbeing, behavioral problems, and altruistic behaviors was associated with a later circadian rhythm. Model 3 was fully adjusted. A 1 hr delay in midsleep was associated with a high score of 0.43 (95% CI: 0.32–0.54) for psychological issues, a low score of 0.20 (95% CI: 0.10–0.21) for psychological wellbeing, a low score of 0.19 (95% CI: 0.09–0.30) for altruistic behavior, and a high score of 3.0% for behavioral issues (95% CI: 1.6–0.31).

Table 2. Construction workers internalizing safety health indicators and 95% confidence intervals from regression analysis.
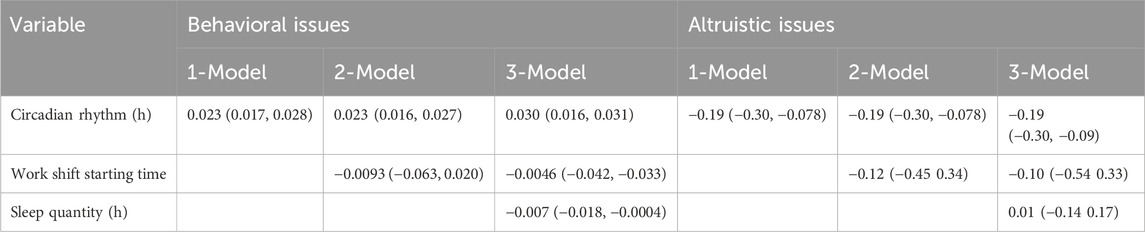
Table 3. Construction workers externalizing safety health indicators and their 95% confidence intervals.
Additionally, sleep quality on company days had a significant effect on psychological issues (0.49 low score, 95% CI: 0.39–0.67), greater psychological wellbeing (0.29 high score, 95% CI: 0.19–0.39), and fewer behavioral issues (0.7% low score, 95% CI: 0.3–1.5), but not altruistic behaviors (0.01 high score, 95% CI: 0.14–0.17). There was no correlation between the initial time and the safety outcomes of the workers.
Psychological wellbeing was marginally correlated with an earlier circadian rhythm and longer sleep duration (p = 0.04), but this interaction disappeared (p = 0.70) when the sample was restricted to employees who slept between 7:00 and 11:00 h on workdays. Sleep quantity or company work-shift start time had no impact on other safety health outcomes. Primary analyses were largely unaffected by restricting the sample to workers who slept between 7:00 and 11:00 on workdays or imputed missing data. We derived evidence of nonlinearity by employing fractional polynomials to model circadian rhythm. Safety health predictions were based on circadian rhythms derived from the linear and fractional polynomial models. Fractional polynomial models suggest that a circadian rhythm earlier than 03:00 hr. may be less detrimental to psychological performance than fractional polynomial models.
5 Discussion
5.1 Findings
A representative sample of construction workers was studied to examine the relationship between safety health and circadian rhythm. As previously reported, a later circadian rhythm is often associated with high levels of psychological difficulties and behavioral issues (Altamura et al., 2010; Kobayashi et al., 2019). Furthermore, a later circadian rhythm was associated with lower psychological wellbeing and fewer altruistic behaviours, supporting the notion that circadian rhythm affects safety and health (Agahi et al., 2018; Siswanto et al., 2020; Analizi and Loganathan, 2022). Numerous controls, including sleep quantity, parenting behaviour, and work-shift start time at the construction company, did not impact these findings. A growing body of evidence suggests that sleep timing plays an important role in the safety and health of construction workers (Wallis et al., 2018; Hwang et al., 2019). However, the mechanisms underlying this association are not well understood. It was observed that the sleep quantity of construction workers with a later circadian rhythm did not influence the association between poor safety health and later circadian rhythms. In addition, the effects of sleep quantity and circadian rhythm were found to be independent in two studies conducted on young people (Kobayashi et al., 2019). A small expert safety study found that construction workers with a late circadian rhythm reported fewer positive emotions than those with a circadian rhythm that had an initial rhythm under both resting and sleep-deprived conditions (Kineber et al., 2022; Singh et al., 2023c). Furthermore, a previous observational study found that late circadian rhythms were associated with poor self-regulation among construction workers regardless of their sleep quantity or levels of daytime sleepiness (Singh et al., 2023b; Singh et al., 2023e). These results are extended to various safety health domains in this study. The current study’s findings indicate that circadian rhythm, rather than sleep quantity, is associated with altruistic behaviours (Altamura et al., 2010; Liang et al., 2018). Although this finding is new in construction workers, similar associations have been reported in previous studies in adults (Kobayashi et al., 2019).
Also, a company’s work-shift start time does not affect the correlation between circadian rhythms and safety health (Agahi et al., 2018; Siswanto et al., 2020). Construction workers with an early and late circadian rhythm showed distinct health disparities. Other studies, including the current study, have found that construction workers sleep more when their company begins operations later in the day. Construction workers with a later circadian rhythm may benefit from this, but their safety and health may not necessarily improve (Tempesta et al., 2016; Lamrhari et al., 2022). Thus, to improve their wellbeing, it may be necessary to investigate ways to better align construction workers’ social schedules to their circadian rhythm throughout the day rather than just during the company’s work-shift start hours (Singh et al., 2023a; Singh et al., 2023d; Kineber et al., 2023).
5.2 Implications
This study has profound and multifaceted implications, spanning both theoretical insights and practical applications. On a theoretical level, this research advances our understanding of circadian rhythms by highlighting their specific effects on a wide array of safety and health outcomes among construction workers. By meticulously controlling for variables such as sleep duration and work schedule factors, the study delineates the intricate interplay between these elements and circadian rhythms. This comprehensive approach enriches the existing theoretical framework and paves the way for future research to build upon these nuanced findings. Additionally, by broadening the spectrum of safety and health outcomes to include psychological issues, wellbeing, behavioural issues, and altruistic behaviours, this study provides a more holistic view of occupational health dynamics.
Practically, the findings offer invaluable insights for shaping workplace policies that mitigate the adverse effects of disrupted circadian rhythms. Employers can use this research to implement flexible work schedules and promote sleep health programs, directly addressing the specific safety and health concerns identified. These evidence-based interventions, such as educational programs on sleep hygiene and adjustments to work shift timings, can significantly enhance the wellbeing of construction workers. Furthermore, the study’s implications extend beyond the local context, offering a globally applicable framework. International construction companies can leverage these insights to improve worker safety and productivity by better managing work schedules and promoting healthier sleep practices. Ultimately, this study not only contributes to academic discourse but also provides practical solutions to enhance the health and safety of construction workers worldwide.
6 Conclusion
This study examined the relationship between young people’s safety health and circadian rhythm, as well as the role of sleep quantity, company work-shift start time, and parenting characteristics in this association. An association between a later circadian rhythm, a greater likelihood of safety health issues and a lower level of positive wellbeing, regardless of the amount of sleep or the work shift starting time was discovered. Although a later circadian rhythm has no independent negative consequences, it appears to be detrimental to young people as they struggle more than others.
There were some limitations to this study. Sleep quantity and circadian rhythm were estimated using self-reported sleep times. Even though these measures have been validated, objective sleep measurement studies would strengthen this evidence. In addition, the estimates of circadian rhythms based on weekend sleep patterns assumed that workers had unrestricted sleep on company-free days, which is not the case for all employees. In this case, misclassification could result in an underestimation of the results, which would indicate that the actual associations are stronger. The puberty stage, however, may better capture differences in biological maturation among workers. The onset of puberty is a marker for circadian shifts in the phase of life, and pubertal status is correlated with youth safety and health, regardless of age.
Further research on the causal mechanisms linking chronobiology with safety and health is required. Future research should consider the age at maturation. In addition, the study design made it impossible to determine the direction of causality. Numerous psychiatric disorders are associated with circadian disruptions, and evidence from studies on adults suggests a reciprocal relationship. There is a possibility that residual confounding may still occur despite controlling for several confounders, including personality traits or genes that are shared by both circadian rhythms and safety health problems.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by this research study was conducted according to the Declaration of Helsinki guidelines. The Institutional Review Board of Dayananda Sagar University has approved the study. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AS: Conceptualization, Formal Analysis, Methodology, Resources, Validation, Writing–original draft, Writing–review and editing. AA: Conceptualization, Data curation, Supervision, Validation, Writing–original draft, Writing–review and editing. PS: Formal Analysis, Investigation, Methodology, Validation, Writing–original draft, Writing–review and editing. BA: Data curation, Formal Analysis, Software, Supervision, Writing–original draft, Writing–review and editing. SU: Data curation, Formal Analysis, Investigation, Supervision, Writing–original draft, Writing–review and editing. BS: Conceptualization, Formal Analysis, Methodology, Resources, Visualization, Writing–original draft, Writing–review and editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Abdul Azeez, N. P., and Jawed Akhtar, S. M. (2019). Analysis of Female Work Participation Rate in India. Financial and Inclusion in India. Availabel at: https://www.researchgate.netpublication/331702688_Analysis_of_Female_Work_Participation_Rate_in_India#fullTextFileContent
Adan, A., Archer, S. N., Hidalgo, M. P., Di Milia, L., Natale, V., and Randler, C. (2012). Circadian typology: a comprehensive review. Chronobiology Int. 29 (9), 1153–1175. doi:10.3109/07420528.2012.719971
Agahi, A., Hamidi, G. A., Daneshvar, R., Hamdieh, M., Soheili, M., Alinaghipour, A., et al. (2018). Does severity of alzheimer ’ s disease contribute to its responsiveness to modifying gut microbiota ? A double blind clinical trial. Front. Neurol. 9, 662–669. doi:10.3389/fneur.2018.00662
Albrecht, U. (2012). Timing to perfection: the biology of central and peripheral circadian clocks. Neuron 74 (2), 246–260. doi:10.1016/J.NEURON.2012.04.006
Altamura, A. C., Dell, B., Berlin, H. A., Buoli, M., Bassetti, R., and Mundo, E. (2010). Duration of untreated illness and suicide in bipolar disorder: a naturalistic study. Eur. Arch. Psychiatry Clin. Neurosci. 260, 385–391. doi:10.1007/s00406-009-0085-2
Analizi, N. B., and Loganathan, K. (2022). A quantitative analysis between sleep and psychological behaviour of Indian construction workers. J. Turkish Sleep Med. 9 (3), 221–231. doi:10.4274/jtsm.galenos.2022.64426
Angerer, P., Schmook, R., Elfantel, I., and Li, J. (2017). Night work and the risk of depression: a systematic review. Dtsch. Ärzteblatt Int. 114 (24), 404–411. doi:10.3238/ARZTEBL.2017.0404
Arendt, J. (2010). Shift work: coping with the biological clock. Occup. Med. 60 (1), 10–20. doi:10.1093/OCCMED/KQP162
Baron, K. G., and Reid, K. J. (2014). Circadian misalignment and health. Int. Rev. Psychiatry 26 (2), 139–154. doi:10.3109/09540261.2014.911149
Boschman, J. S., van der Molen, H. F., Sluiter, J. K., and Frings-Dresen, M. H. W. (2013). Psychosocial work environment and mental health among construction workers. Appl. Ergon. 44 (5), 748–755. doi:10.1016/J.APERGO.2013.01.004
Chan, I. Y. S., Leung, M. Y., and Liu, A. M. M. (2016). Occupational health management system: a study of expatriate construction professionals. Accid. Analysis and Prev. 93, 280–290. doi:10.1016/J.AAP.2015.11.003
Chan, A. P. C, Nwaogu, J. M., and Naslund, J. A. (2020). Mental Ill-Health Risk Factors in the Construction Industry: Systematic Review. J. Constr. Eng. Manag. 146 (3), 04020004. doi:10.1061/(asce)co.1943-7862.000177
Chellappa, S. L., Morris, C. J., and Scheer, F. A. J. L. (2020). Circadian misalignment increases mood vulnerability in simulated shift work. Sci. Rep. 10 (1), 18614–18710. doi:10.1038/s41598-020-75245-9
Chellappa, V., Srivastava, V., and Salve, U. R. (2021). A systematic review of construction workers’ health and safety research in India. Journal of Engineering, Design and Technology 19 (6), 1488–1504. doi:10.1108/JEDT-08-2020-0345
Cheng, W. J., Cheng, Y., Huang, M. C., and Chen, C. J. (2012). Alcohol dependence, consumption of alcoholic energy drinks and associated work characteristics in the taiwan working population. Alcohol Alcohol. 47 (4), 372–379. doi:10.1093/ALCALC/AGS034
Dong, H., Zhang, Q., Sun, Z., Sang, F., and Xu, Y. (2017). Sleep disturbances among Chinese clinical nurses in general hospitals and its influencing factors. BMC Psychiatry 17 (1), 241–249. doi:10.1186/s12888-017-1402-3
Dong, X. (2005). Long workhours, work scheduling and work-related injuries among construction workers in the United States. Scand. J. Work, Environ. and Health 31, 329–335. doi:10.5271/sjweh.915
Duffy, J. F., Rimmer, D. W., and Czeisler, C. A. (2001). Association of intrinsic circadian period with morningness-eveningness, usual wake time, and circadian phase. Behav. Neurosci. 115 (4), 895–899. doi:10.1037/0735-7044.115.4.895
Fagbenro, R. K., Sunindijo, R. Y., Illankoon, C., and Frimpong, S. (2023). Influence of Prefabricated Construction on the Mental Health of Workers: Systematic Review. Eur. J Investig. Health Psychol. Educ. 13 (2), 345–363. doi:10.3390/ejihpe13020026
Golombek, D. A., and Rosenstein, R. E. (2010). Physiology of circadian entrainment. Physiol. Rev. 90 (3), 1063–1102. doi:10.1152/physrev.00009.2009
Gómez-Salgado, C., Camacho-Vega, J. C., Gómez-Salgado, J., García-Iglesias, J. J., Fagundo-Rivera, J., Allande-Cussó, R., et al. (2023). Stress, fear, and anxiety among construction workers: a systematic review. Front. Public Health 11, 1226914. doi:10.3389/fpubh.2023.1226914
Gosselin, E., Lemyre, L., and Corneil, W. (2013). Presenteeism and absenteeism: differentiated understanding of related phenomena. J. Occup. Health Psychol. 18 (1), 75–86. doi:10.1037/A0030932
Greiner, B. A., Leduc, C., O'Brien, C., Cresswell-Smith, J., Rugulies, R., Wahlbeck, K., et al. (2022). The effectiveness of organisational-level workplace mental health interventions on mental health and wellbeing in construction workers: A systematic review and recommended research agenda. PLoS One. 17 (11), e0277114. doi:10.1371/journal.pone.0277114
Gulliver, A., Griffiths, K. M., and Christensen, H. (2010). Perceived barriers and facilitators to mental health help-seeking in young people: a systematic review. BMC Psychiatry 10, 113. doi:10.1186/1471-244X-10-113
Harris, E. J., Khoo, I. H., and Demircan, E. (2022). A survey of human gait-based artificial intelligence applications. Front. Robotics AI 8, 749274. doi:10.3389/frobt.2021.749274
Hwang, Y., Park, S., Paik, J., Chae, S., Kim, D., Jeong, D., et al. (2019). Efficacy and safety of lactobacillus plantarum C29-fermented soybean (DW2009) in individuals with mild cognitive impairment: a 12-week, multi-center, randomized, double-blind, placebo-controlled clinical trial. Nutrients 11, 305. doi:10.3390/nu11020305
Jacobsen, H. B., Caban-Martinez, A., Onyebeke, L. C., Sorensen, G., Dennerlein, J. T., and Reme, S. E. (2013). Construction workers struggle with a high prevalence of mental distress, and this is associated with their pain and injuries. J. Occup. Environ. Med. 55 (10), 1197–1204. doi:10.1097/JOM.0B013E31829C76B3
James, S. M., Honn, K. A., Gaddameedhi, S., and Van Dongen, H. P. A. (2017). Shift work: disrupted circadian rhythms and sleep—implications for health and well-being. Curr. Sleep. Med. Rep. 3 (2), 104–112. doi:10.1007/s40675-017-0071-6
Järnefelt, H., Lagerstedt, R., Kajaste, S., Sallinen, M., Savolainen, A., and Hublin, C. (2012). Cognitive behavioral therapy for shift workers with chronic insomnia. Sleep. Med. 13 (10), 1238–1246. doi:10.1016/J.SLEEP.2012.10.003
Juda, M., Vetter, C., and Roenneberg, T. (2013). Chronotype modulates sleep duration, sleep quality, and social jet lag in shift-workers. J. Biol. Rhythms 28 (2), 141–151. doi:10.1177/0748730412475042
Kawabe, Y., Nakamura, Y., Kikuchi, S., Suzukamo, Y., Murakami, Y., Tanaka, T., et al. (2015). Relationship of type of work with health-related quality of life. Qual. Life Res. 24 (12), 2927–2932. doi:10.1007/s11136-015-1024-5
Kecklund, G., and Axelsson, J. (2016). Health consequences of shift work and insufficient sleep. BMJ 355, i5210. doi:10.1136/BMJ.I5210
Kineber, A. F., Mohandes, S. R., Hamed, M. M., Singh, A. K., and Elayoty, S. (2022). Identifying and assessing the critical criteria for material selection in storm drainage networks: a stationary analysis approach. Sustainability 14 (21), 13863. doi:10.3390/su142113863
Kineber, A. F., Singh, A. K., Fazeli, A., Mohandes, S. R., Cheung, C., Arashpour, M., et al. (2023). Modelling the relationship between digital twins implementation barriers and sustainability pillars: insights from building and construction sector. Sustain. Cities Soc. 99, 104930. doi:10.1016/j.scs.2023.104930
Kobayashi, Y., Kuhara, T., Oki, M., and Xiao, J. Z. (2019). Effects of Bifidobacterium breve A1 on the cognitive function of older adults with memory complaints: a randomised, double-blind, placebo-controlled trial. Benef. Microbes 10 (5), 511–520. doi:10.3920/BM2018.0170
Kotera, Y., Green, P., and Sheffield, D. (2020). Work-life balance of UK construction workers: relationship with mental health. Constr. Manag. Econ. 38 (3), 291–303. doi:10.1080/01446193.2019.1625417
Lamrhari, S., El, H., Oubrich, M., and El, A. (2022). Technological Forecasting and Social Change A social CRM analytic framework for improving customer retention, acquisition, and conversion. Technol. Forecast. and Soc. Change 174, 121275. doi:10.1016/j.techfore.2021.121275
Langdon, R. R., and Sawang, S. (2018). Construction workers’ well-being: what leads to depression, anxiety, and stress?. J. Constr. Eng. Manag. 144, 04017100. doi:10.1061/(ASCE)CO.1943-7862.0001406
Liang, D., Mays, V. M., and Hwang, W. (2017). Integrated mental health services in China: challenges and planning for the future. Health Policy Plan. 33, 107–122. doi:10.1093/heapol/czx137
Liang, D., Mays, V. M., and Hwang, W. (2018). Integrated mental health services in China: challenges and planning for the future. Health Policy Plan. 33, 107–122. doi:10.1093/heapol/czx137
Mieda, M. (2020). The central circadian clock of the suprachiasmatic nucleus as an ensemble of multiple oscillatory neurons. Neurosci. Res. 156, 24–31. doi:10.1016/J.NEURES.2019.08.003
Milner, A., Krnjacki, L., and LaMontagne, A. D. (2017). Psychosocial job quality and mental health among young workers: a fixed-effects regression analysis using 13 waves of annual data. Scand. J. Work, Environ. and Health 43, 50–58. doi:10.5271/sjweh.3608
Mohawk, J. A., Green, C. B., and Takahashi, J. S. (2012). Central and peripheral circadian clocks in mammals. Annu. Rev. Neurosci. 35 (35), 445–462. doi:10.1146/annurev-neuro-060909-153128
Morgan, A. J., Reavley, N. J., and Jorm, A. F. (2014). Beliefs about mental disorder treatment and prognosis: comparison of health professionals with the Australian public. Aust. N. Z. J. Psychiatry 48 (5), 442–451. doi:10.1177/0004867413512686
Nováková, M., Sládek, M., and Sumová, A. (2013). Human chronotype is determined in bodily cells under real-life conditions. Chronobiology Int. 30 (4), 607–617. doi:10.3109/07420528.2012.754455
Palaniappan, K., Natarajan, R., and Dasgupta, C. (2022). Prevalence and risk factors for depression, anxiety and stress among foreign construction workers in Singapore - a cross-sectional study. Int. J. Constr. Manag. 24, 1–9. doi:10.1080/15623599.2022.2070343
Roche, A. M., Pidd, K., Fischer, J. A., Lee, N., Scarfe, A., and Kostadinov, V. (2016). Men, work, and mental health: a systematic review of depression in male-dominated industries and occupations. Saf. Health A. T. Work 7 (4), 268–283. doi:10.1016/J.SHAW.2016.04.005
Roenneberg, T., Kuehnle, T., Pramstaller, P. P., Ricken, J., Havel, M., Guth, A., et al. (2004). A marker for the end of adolescence. Curr. Biol. 14 (24), R1038–R1039. doi:10.1016/j.cub.2004.11.039
Roenneberg, T., Kuehnle, T., Juda, M., Kantermann, T., Allebrandt, K., Gordijn, M., et al. (2007). Epidemiology of the human circadian clock. Sleep. Med. Rev. 11 (6), 429–438. doi:10.1016/J.SMRV.2007.07.005
Sathvik, S., Krishnaraj, L., and Awuzie, B. O. (2023). An assessment of prevalence of poor sleep quality among construction workers in Southern India. Built Environ. Proj. Asset Manag. 13 (2), 290–305. doi:10.1108/bepam-03-2022-0041
Saxena, S., Funk, M. K., and Chisholm, D. (2020). Comprehensive mental health action plan 2013 –2015.
Sharma, H. R., Appadurai, S., Wubshet, M., and Tadesse, T. (2008). Occupational Exposures and Related Health Effects among Construction Workers. Ethiopian Journal of Health and Biomedical Sciences, 1 (1), 6. doi:10.20372/ejhbs.v1i1.10
Singh, A. K., and Kumar, V. R. P. (2022). Conceptual model of quality management based on blockchain in construction industry.
Singh, A. K., and Kumar, V. R. P. (2023). Analyzing the barriers for blockchain-enabled BIM adoption in facility management using best-worst method approach. Built Environ. Proj. Asset Manag. 14, 164–183. doi:10.1108/BEPAM-04-2023-0080
Singh, A. K., and Kumar, V. R. P. (2024a). Analyzing the barriers for blockchain-enabled BIM adoption in facility management using best-worst method approach. Built Environ. Proj. Asset Manag. 14, 164–183. doi:10.1108/BEPAM-04-2023-0080
Singh, A. K., and Kumar, V. R. P. (2024b). Establishing the relationship between the strategic factors influencing blockchain technology deployment for achieving SDG and ESG objectives during infrastructure development: an ISM-MICMAC approach. Smart Sustain. Built Environ. 13 (3), 711–736. doi:10.1108/SASBE-12-2023-0405
Singh, A. K., and Prasath Kumar, V. R. (2022). Smart contracts and supply chain management using blockchain. J. Eng. Res. (Kuwait) 9, 1–11. doi:10.36909/jer.ACMM.16307
Singh, A. K., Kumar, V. R. P., Dehdasht, G., Mohandes, S. R., Manu, P., and Pour Rahimian, F. (2023a). Investigating barriers to blockchain adoption in construction supply chain management: a fuzzy-based MCDM approach. Technol. Forecast. Soc. Change 196, 122849. doi:10.1016/j.techfore.2023.122849
Singh, A. K., Kumar, V. R. P., Irfan, M., Mohandes, S. R., and Awan, U. (2023b). Revealing the barriers of blockchain technology for supply chain transparency and sustainability in the construction industry: an application of pythagorean FAHP methods. Sustain. Switz. 15 (13), 10681. doi:10.3390/su151310681
Singh, A. K., Kumar, V. R. P., Shoaib, M., Adebayo, T. S., and Irfan, M. (2023c). A strategic roadmap to overcome blockchain technology barriers for sustainable construction: a deep learning-based dual-stage SEM-ANN approach. Technol. Forecast. Soc. Change 194, 122716. doi:10.1016/j.techfore.2023.122716
Singh, A. K., Sathvik, S. C., Krishnaraj, L., Irfan, M., Kumar, V. R. P., and Işik, C. (2023d). Assessing thermo-physical products’ efficiency in the building and construction industry: a bibliometric analysis approach. Environ. Sci. Pollut. Res. 30 (7), 16867–16877. doi:10.1007/s11356-022-25103-0
Singh, A. K., Kumar, V. G. R. P., Hu, J., and Irfan, M. (2023e). Investigation of barriers and mitigation strategies to blockchain technology implementation in construction industry: an interpretive structural modeling approach. Environ. Sci. Pollut. Res. 30, 89889–89909. doi:10.1007/s11356-023-28749-6
Siswanto, D., Iridiastadi, H., and Muslim, K. (2020). A case study on impact of labours sleep deprivation in construction project using application method. IOP Conf. Ser. Mater. Sci. Eng. 912 (6), 062055. doi:10.1088/1757-899X/912/6/062055
Sletten, T. L., Cappuccio, F. P., Davidson, A. J., Van Cauter, E., Rajaratnam, S. M. W., and Scheer, F. A. J. L. (2020). Health consequences of circadian disruption. Sleep 43 (1), zsz194. doi:10.1093/SLEEP/ZSZ194
Statista, (2024). U.S. construction sector employment reaches highest level in the 21st century. Available at: https://www.statista.com/statistics/183715/employment-in-the-us-construction-industry-since-1990/
Tempesta, D., Socci, V., Coppo, M., Dello, G., Nepa, V., Gennaro, L. D., et al. (2016). The effect of sleep deprivation on the encoding of contextual and non-contextual aspects of emotional memory. Neurobiol. Learn. Mem. 131, 9–17. doi:10.1016/j.nlm.2016.03.007
Turner, M., and Lingard, H. (2020). Examining the interaction between bodily pain and mental health of construction workers. Constr. Manag. Econ. 38 (11), 1009–1023. doi:10.1080/01446193.2020.1791920
Vetter, C. (2020). Circadian disruption: what do we actually mean? Eur. J. Neurosci. 51 (1), 531–550. doi:10.1111/EJN.14255
Wallis, A., Ball, M., Butt, H., Lewis, D. P., Mckechnie, S., Paull, P., et al. (2018). Open - label pilot for treatment targeting gut dysbiosis in myalgic encephalomyelitis/chronic fatigue syndrome: neuropsychological symptoms and sex comparisons. J. Transl. Med. 16, 24–16. doi:10.1186/s12967-018-1392-z
Xu, J., Wang, J., Wimo, A., and Qiu, C. (2016). The economic burden of mental disorders in China, 2005 – 2013: implications for health policy. BMC Psychiatry 16, 137–139. doi:10.1186/s12888-016-0839-0
Keywords: safety health, construction industry, workers, psychological wellbeing, circadian rhythm
Citation: Kumar Singh A, Aljohani A, Shakor P, Awuzie BO, Uddin SMJ and Shivendra BT (2024) Study on safety health of construction workers at workplace: a sustainable perspective approach. Front. Built Environ. 10:1451727. doi: 10.3389/fbuil.2024.1451727
Received: 19 June 2024; Accepted: 09 August 2024;
Published: 26 August 2024.
Edited by:
V. R. Prasath Kumar, SRM Institute of Science and Technology, IndiaReviewed by:
Ahmed Kineber, Prince Sattam Bin Abdulaziz University, Saudi ArabiaRakesh Kumar, National Institute of Technology Patna, India
Copyright © 2024 Kumar Singh, Aljohani, Shakor, Awuzie, Uddin and Shivendra. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Abdulelah Aljohani, YWFsam9oYW5pQGJ1LmVkdS5zYQ==