 Roberto Orofino Giambastiani
Roberto Orofino Giambastiani Rodrigo Sáenz
Rodrigo Sáenz Guido Lahitte
Guido Lahitte Juan Umaran
Juan Umaran- 1Department of Pediatric Cardiovascular Anesthesiology, Hospital General de Niños “Dr. Pedro de Elizalde”, Buenos Aires, Argentina
- 2Department of Anesthesiology, Hospital General “HIGA. Gral. San Martín”, La Plata, Argentina
- 3Department of Pediatric Anesthesiology, Hospital General de Niños “Sor María Ludovica”, La Plata, Argentina
- 4Independent Author, La Plata, Argentina
Patient safety is acknowledged as a primary aim of anesthesiology. Anesthesia records constitute the main document of the intraoperative course of anesthesia administration. In this paper, we postulate that anesthesia record systems should be based on an integral tamper-proof design and provide specific technology characteristics to ensure data immutability, accessibility and transparency. Issues and limitations regarding current anesthesia record technologies are reviewed. We introduce a novel anesthesia record system designed for patient safety optimization which integrates dedicated hardware, blockchain technology and decentralized storage solutions. We propose an oracle network in which anesthesiologists run independent Sybil-resistant nodes which broadcast biosensor time series to decentralized storage systems and generate proofs of existence on public blockchains. Records are biometrically signed and incorporate information on the temporo-spatial relation between the anesthetized patient and the professional in charge through a unique personal-transponder wearable device. Compatibility for data science and machine learning implementation are discussed. Finally, we evaluate future impact and technological potential.
1 Introduction
Intraoperative anesthesia procedures can be considered a “control system” from a cybernetic perspective (Aström and Murray, 2008). The patient can thus be contemplated as a complex system controlled by the anesthesiologist who performs as a non-deterministic controller.
Anesthetized patients are peculiar components of this system as they remain in a state of maximum vulnerability: they are unable to take care of themselves, delegating their safety to professionals and medical institutions.
The aim of anesthesia records is to register measurements and interpretations for research or audit purposes. They have evolved from manually confected paper sheets to electronic records registered by anesthesia machines and monitors. However, current technology implementations are based on models that are vulnerable to data tampering, destruction, and access limitation, and therefore provide suboptimal mechanisms for ensuring data integrity.
Although individuals and institutions are expected to comply with safety regulations and standards, we believe that anesthesia record systems should operate with trustless and independent mechanisms in order to provide immutable data from sampling and transmission, to the storage and recovery processes. A simple heuristic is: if someone had to choose between boarding one of two identical aircrafts for the same price, one lacking a flight recorder, the other having one installed onboard; it is logical to assume that the latter would be the best choice as it relies on mechanisms that provide evidence regardless of any outcome. In this way, data transparency and availability is guaranteed by a system which is independent of pilots and flight companies.
Anesthesiologists are on the forefront of ensuring the highest possible quality and safest care for every patient (Gaba, 2000). A cornerstone of the discipline is continuous improvement based on iterative reevaluation of metrics, review of processes, and learning from mistakes (Valentine and Falk, 2018). In this context, we believe that performance analysis has the potential to improve the outcomes of dynamical systems and should therefore be a pivotal implementation for control systems in which human life is at stake.
We propose a record system architecture based on two fundamental principles: “data integrity” and “data completeness”. “Data integrity” refers to the preservation of accuracy, consistency, transparency and immutability throughout the data lifecycle. “Data completeness” refers to the presence of necessary information that must be incorporated within the register to contextualize the recorded time series. A scientific record system should bolster data analysis and the exchange of standardized information between anesthesia providers on a global level (Colquhoun et al., 2020).
2 Outline
In Section A, we begin by framing the anesthesiological scenario as a control system. We continue by elucidating the meaning of “safety”, reviewing the causes of suboptimal performance and the limitations for record rebuilding. Next, we expose the drawbacks of current recording methods.
In Section B, we introduce our proposed solution. We first describe what we consider to be the necessary features of an ideal anesthesia record system. We define its components and delineate their interactions. We then describe methods for generating, updating and rebuilding anesthesia records. The section culminates by recapping how this architecture addresses each proposed feature of the ideal system.
In Section C, we discuss the innovation and future vision of this technology. We highlight how the system can proliferate a decentralized oracle network and describe its potential applications. We point out emerging characteristics that are expected to benefit patients, anesthesiologists and the global community. Internal details about the system´s governance, sustainability and self-audit are illustrated. We explain how the proposed system can be coordinated with different fields such as artificial intelligence, neuroscience and anesthesia simulation. Finally, we conclude by mentioning expected limitations.
3 Section A: Background
3.1 The control system model approach
We propose to analyze the intraoperative scenario in a reductionist way by considering it as a cybernetic model (Novikov, 2016).
The set of the anesthetized patient being controlled by the anesthesiologist can be interpreted as a control system consisting of four basic components:
1) A controlled component, represented by the patient, which can be considered a complex dynamical system (Ladyman et al., 2013).
2) A controller component, represented by the anesthesiologist who is in charge of observing the patient, interpreting measurements, and making decisions to maintain or correct patient variables within safe limits (Klocke et al., 1986). Anesthesiologists can be considered non-deterministic controllers as they may exhibit different reactions to identical situations at different times.
3) A channel from the controlled component towards the controller, which transmits the sampled measurements.
4) A channel from the controller to the controlled component, composed of the collection of interfaces through which the anesthesiologist can intervene over the patient, such as endovenous lines, infusion pumps, ventilators, pacemakers, or direct contact with the patient.
3.2 Safety
We consider a “safe performance” to be the active maintenance of the patient’s physiological and biochemical parameters within ranges considered normal by scientific consensus (Joyce et al., 2017). To achieve this, anesthesiologists must take effective action to recover parameters when they deviate from these reliable limits. Lack of timely correction of such deviations can threaten the integrity of the patient and generate potential harm.
The concept of “harm” is broad and can range from general eventualities such as hypoxia, hypoperfusion, pain, acidosis or hypothermia; to specific damage caused by burns, cuts or compressions. Harm can be reversible, irreversible (generating sequelae or disability) or even cause death.
As a controller, the role of the anesthesiologist is to preserve situational awareness (McIlvaine, 2007; Schulz et al., 2013; Schulz et al., 2015) to efficiently prevent harm and ensure patient safety during the entire anesthetic procedure until self-control is regained or exerted by another controller (such as an intensive care service).
3.3 Causes of suboptimal performance and suboptimal record rebuilding
Similarly to pilots, anesthesiologists are in charge of detecting anomalies and resolving complications efficiently (Toff, 2010). To understand the causes of suboptimal performance and undesired outcomes during intraoperative anesthesia, failure scenarios should be outlined. The term “anomaly” refers to any actual or potential inconsistency, irregularity or deviation of parameters which could expose patients to risk or harm.
From the controller perspective, suboptimal performance can be framed in four main failure scenarios:
A) Detection Failure: an anomaly is not detected or detection is delayed.
B) Diagnostic Failure: an anomaly is detected but incorrectly identified or categorized.
C) Failure in Therapeutic Selection: an anomaly is detected and correctly identified, but there is an erroneous choice of the treatment to be applied.
D) Failure in Therapeutic Implementation: an anomaly is detected and correctly identified; the correct treatment is recognized but executed inefficiently or incorrectly.
The root causes of main failure scenarios can be traced to:
1-Controller Absence
2-Controller Distraction
3-Controller Inexperience
4-Insufficient Professional Training
5-Ineffective Supervision of Trainees
6-Resource Unavailability
7-Resource Malfunction
Within this framework, causes of suboptimal record rebuilding must be also recognized:
A) Incomplete/Interrupted Registration
B) Record System Failure
C) Record Adulteration
D) Record Destruction
E) Record Access Limitation
Anesthesia records should enable easy contextualization of any outcome of the control system. Although record immutability is an intimidating concept, technology should protect professionals and institutions from liability risks by providing objective evidence of compliance with quality and safety standards (Feldman, 2004). Genuine commitment to patient safety must involve full transparency for patients and society. Record rebuilding should be guaranteed by a solid tamper-resistant architecture.
3.4 Drawbacks of current anesthesia records
Paper-based anesthesia records present several disadvantages: difficult legibility of handwritten information, asynchrony between measurement and data registration, susceptibility to inaccuracies, loss of relevant data, and user distraction from the environment surveillance (Reich et al., 2000; van Schalkwyk et al., 2011; Edwards et al., 2013; Anderson and Merry, 2015). Paper sheets are easy to tamper, their authenticity relies on sensitive mechanisms such as handwritten signatures or classic stamping. Finally, being physical objects, they are prone to damage or loss.
Prevailing electronic anesthesia records provide many advantages over handwritten registers (Ehrenfeld and Rehman, 2011), however, some aspects of their design can still be improved. For example, data is locally stored on the sampling devices or in centralized institutional networks, which can lead to data vulnerability or access limitation. Authentication relies on local mechanisms such as passwords for the monitor hardware or for local networks. User profiles can generally be created readily and can also be issued and withdrawn by individuals or centralized administrations, providing a technologically weak mechanism for validating user legitimacy.
Current record traceability and timestamping do not depend on public networks, nor do they count on mechanisms to generate public proof of existence or immutability. Data provenance is not endorsed by network-based geolocation.
Finally, there is a general lack of compatibility and interoperability between electronic systems for the integration of data in real time.
4 Section B: Solution
4.1 Proposed anesthesia record features for system optimization
In order to optimize the “control process”, the quality of the generated data should be maximized. An ideal record system should provide unbiased data and ensure the immutability of information, precluding the influence of particular interests of individuals or institutions. In addition, mechanisms to generate evidence about the performance of the system components and their interactions must be provided by the architecture itself.
We propose a model based on the application of open-source hardware and software for the registration of sensor time series as a fundamental principle for case analysis and reconstructions. Decentralization and technological independence ensure an impartial and immutable data outflow. The records integrate real-time information on the spatio-temporal relation between the patient and the anesthesiologist, generating evidence of the entire anesthesia control system. To enhance the interpretation of the time series, manual incorporation of supplemental data related to the anesthesia case is invited by the system.
A global anesthesiologist ecosystem can be assembled over a record technology based on specific features to ensure scientific rigor in the data generation process. While these characteristics define the system as a whole, we divide them into three main categories for an intelligible exposition:
a) Features of the data generation process
b) Features of the system network
c) Features for interacting with data
4.1.1 Features of the data generation process
1-Automaticity: Data sampling and registration should be automated in order to eliminate bias and prevent legibility issues or ambiguity resulting from manual data transfer. An automated record should avoid distractions for the anesthesiologist (Dutton and DuKatz, 2011; Kadry et al., 2012; Tse et al., 2020).
2-Synchronicity: Asynchrony between real events and their registration may lead to inaccuracies and loss of information. Sampled data should be recorded simultaneously (or with minimum delay) with respect to the sensors’ measurement process (Vigoda and Lubarsky, 2006).
3-Decentralized Storage: Relying on local hardware or centralized services for record storage may lead to potential vulnerabilities such as access limitation, data tampering or permanent loss.
We believe that data integrity and accessibility can be ensured by delegating the storage to decentralized systems. This would maximize fault tolerance and attack resistance, and would also avoid reliance on critical points of failure related to hardware malfunction and central control over databases. While “architectural decentralization” would enable data to be saved and distributed globally, “political decentralization” would avoid dependence on the control of individual organizations over data storage (Buterin, 2017).
Storage redundancy should be manageable according to the ecosystem requirements.
4-Accessibility: Records should be permanently available for consultation worldwide. Data retrieval must be guaranteed avoiding any type of territorial or institutional access restriction. Patients can thus benefit from the availability of previous records for use in prospective anesthesiological procedures or emergency scenarios.
5-Encryption: Data must be transmitted securely between nodes, the protection from decryption in the case of malicious interception must be technically ensured (Fernández-Alemán, 2013).
6-Real-Time Transmission: To minimize record vulnerability at data generation sites, sampling should be transmitted to remote storage systems instantly or with minimum delay.
7-Biometric Authentication: Record systems should count on signatures or authentication mechanisms to validate that the data has been generated by whoever claims to have done so. Biometric authentication, such as fingerprint reading, provides a reliable method for the identification of the anesthesiologist and also generates an active proof of proximity to the patient. Biometric signatures would provide objectivity in determining anesthesia times, eliminate inaccuracies in billing systems, and provide a formal method for handovers between professionals. Furthermore, these would impede fraudulent authentication and discourage simultaneous anesthesia procedures.
Ideally, the patient’s consent to record their data should also be obtained through a biometric method. We propose a raw voice recording system to document the patient’s authorization before the anesthesia procedure begins. This would allow its incorporation into the anesthesia record without compromising privacy.
8-Traceability: Information on procedure geolocation and timestamps should not rely on manual labeling. This must be automatically generated by network connectivity and embedded within the register as evidence of the data origin.
9-Confidentiality/Privacy: Paper anesthesia records can easily be mishandled, compromising sensitive data. Most electronic records from anesthesia machines and monitors rely on manually introduced passwords which can be easily revealed or shared. Biometric authentication certifies signer legitimacy and ensures data protection through a non-shareable mechanism. It also enables the implementation of ledgers containing chronological data of biometrically-signed access to records.
To ensure privacy, records should not contain personally identifiable information about patients (Coorevits et al., 2013; Kayaalp, 2018). If necessary, records could be paired to specific cases using codes owned by the patients, or by matching tracking tags (previously authorized by them) such as geolocation, timestamps, type of intervention or medical history.
10-Availability of Data on the Interaction between System Components: The performance record of a control system should include information about the dynamic interactions of its components. In addition to the sampled data from patients and the equipment interacting with them, anesthesia records should include measurements of the spatio-temporal relation between the patient and the anesthesiologist.
In order to prevent record discontinuity or the generation of unsupervised datasets, the system should provide incentives to maximize data completeness and should discourage the absence of the anesthesiologist in the operating room.
Spatio-temporal data from professional trainees should also be available in the form of peer-to-peer dynamic interactions between the trainee, the main anesthesiologist and the anesthetized patient.
11-Data Immutability: Measurements should be invulnerable to adulteration from sampling to retrieval processes. Modification or addition of new data should be implemented in a “persistent data structure”, preserving historical data entries (Kaplan, 2018).
12-Blockchain Data Stamping: Proof-of-existence can be generated by registering information of the anesthesia record on blocks from public blockchains. Stamped information should encode: anesthesiologist ID, record identifier, version, time window of its creation and geolocation. It should also include a content hash and the storage addresses of the record and its previous versions.
4.1.2 Features of the system network
13-Universal Instrument Identification: System components and sensors should be universally identifiable by an electronic method. Technical identifiers must be transmitted within the record to allow the performance evaluation and quality of its components. Also, as a policy to ensure scientific reproducibility, data compression and processing should be performed by open-source algorithms.
14-Technology Independence: In order to provide an impartial architecture, the record system should be a dedicated and independent technology implementation. Instrument electronic-identifiers and open-source design should be technically required for external device compatibility.
15-Bidirectional Communication Support for Wearable Devices: Current anesthesia monitoring systems lack mechanisms to measure and record the proximity of the anesthesiologist. Neither do they provide remote communication between the professional and the monitors.
Two-way communication between wearable devices and the record system can generate spatio-temporal data between the anesthesiologist and the patient. Additionally, wearables can allow users to manipulate system parameters remotely, generate biometric signatures, and create voice recordings.
The wearable should be able to alert users through vibration or sound, when the system measurements are interpreted as unsafe conditions for the anesthetized patient (such as anesthesiologist motion inactivity or continuous absence within a safe surveillance distance). Wearable devices should be able to self-alert users even when no connection to the record system is available.
Wearables can also be used to unlock system functions and accredit system manipulation by the actual user through very close radio frequency communication.
Data generated from wearable devices should be integrated into the anesthesia record.
16-Anti-Sybil Backed System1: The system should count on a mechanism to prevent the creation of arbitrary, fraudulent or duplicate user profiles (Douceur, 2002). Integration of blockchain unique human identity proposals (Liu et al., 2020) and the implementation of biometric signatures can lead to a globally interoperable anesthesiologist reputation system (Hoffman et al., 2009).
17-Decentralized Governance: Consensus for system implementations should be managed by a distributed network with no central control (Reijers et al., 2016). Decentralized governance is important for optimizing patient safety as a global anesthesiologist community can reach consensus on standards, guidelines and protocols in an open and transparent way, eliminating any potential risk for institutional coercion. On this basis, compliance with safety protocols, monitoring guidelines, professional certification requirements, and procedure classification for billing systems could be globally assessed by a decentralized community of professionals.
Decentralized governance would also contribute to safety by providing a democratic way for the system community to evaluate its users’ compliance with the established standards. Finally, a network of self-audited users can openly report and alert the global community about labor regimes that may compel anesthesiologists to work in conditions in which patient safety is undermined or deviated from the scientific approach.
18-Output Data Interoperability: Records should facilitate the organized data exchange between diverse information systems, in this context, data must be ideally structured for effectively feeding blockchain oracles (Al-Breiki et al., 2020). Datasets should be easily tokenizeable and embeddable in programmable environments such as smart contracts (Mohanta et al., 2018; Buterin, 2022a).
19-Synchronizable Records: Data streams should be easily synchronized with data from third party devices. In the same way that clapperboards are used in filmmaking to adjust and integrate recorded audio with video, anesthesia records should provide a mechanism for self synchronization with any type of external data gathered from peripheral devices. For example, video from the surgical field could be integrated with the time series to generate multimedia content for research, educational or legal purposes.
Although video recordings of the operating room could be a valid solution for registering events and team performance, this type of information entails potential issues concerning privacy. Native video recording falls outside the scope of this architecture. However, since the system logic seeks to achieve scientific interoperability, synchronization mechanisms for external video must be provided.
20-Dedicated System: The system should be exclusively tailored to patient safety, performance analysis and quality improvement in the field of anesthesiology. In order to mitigate errors and improve the safety of human tasks, it should facilitate the use of checklists and the easy access to protocols and guidelines (Phipps et al., 2008). The architecture should support real time consultation with colleagues worldwide through the system’s professional network.
21-Open-Source Framework: Medical devices can be potentially overpriced in relation to their provided technology. Programmed obsolescence can be used immoderately to maximize profitability by electronically limiting usage time of technological supplies. Closed-source developments restrain the community from auditing hardware and software. This also limits performance evaluation and benchmarking of internal components and processes. The technical design of system components should remain openly available for the community to review, report issues, and suggest improvements.
4.1.3 Features for interacting with data
22-Predictive Analytics and Machine Learning Compatibility: Generated datasets should provide a quality standard for applied research in technology. Extracted statistical information from big data can be used for real-time performance evaluation and predictive analytics (Liem et al., 2018). Sampling and recording processes should generate optimized data streams for feeding artificial intelligence-driven technologies and also for enabling their continuous surveillance. Closed-loop anesthesia infusion systems are examples of emerging technologies that could leverage this system as a data source (Connor, 2019).
23-Compatibility and Interoperability for Supplementary Data Incorporation: Users should be able to integrate supplementary data to the time series records. This feature should be available during the anesthesia procedure or in deferred scenarios such as the preanesthetic visit or extra operative medical consultation.
The input of supplementary information is considered to support the interpretation of time series and should therefore be encouraged. Supplementary data should be incorporated manually and may include patient medical information, device settings, medication details, intraoperative comments and voice notes. In addition, electronic interoperability with authorized third-party devices and extrinsic software platforms should allow the embedding of external data such as video, images, or files containing valuable information (Weininger et al., 2017).
24-Customizable Screen System Interface: A front-end interface should enable users to customize the data flow representation for efficient real-time data analysis (Simpao and Rehman, 2020).
A standardized display configuration must be available through a fast switching mechanism to facilitate the communication of critical information between colleagues during handovers (Saager et al., 2014; Jones et al., 2019) or in emergency scenarios.
25-Software Tool Compatibility: Predictive analytics software is expected to improve decision making-processes (Nair et al., 2017; Rozental and White, 2019). Current anesthesia monitors do not admit the installation of accessory applications. The system should allow users to install and implement their preferred data extraction tools. Also, individuals should be free to develop and deploy their own applications. Audited open-source software validated by scientific consensus can be made available to the ecosystem for use, continuous testing and improvement.
4.2 Implementation
We introduce a model to resolve current issues and comply with the proposed features. In the following section we describe hardware components and their interactions (Figure 1). We outline the aim of the system software and the integration of blockchains with decentralized storage systems. We also describe methods for generating, updating and retrieving anesthesia records.
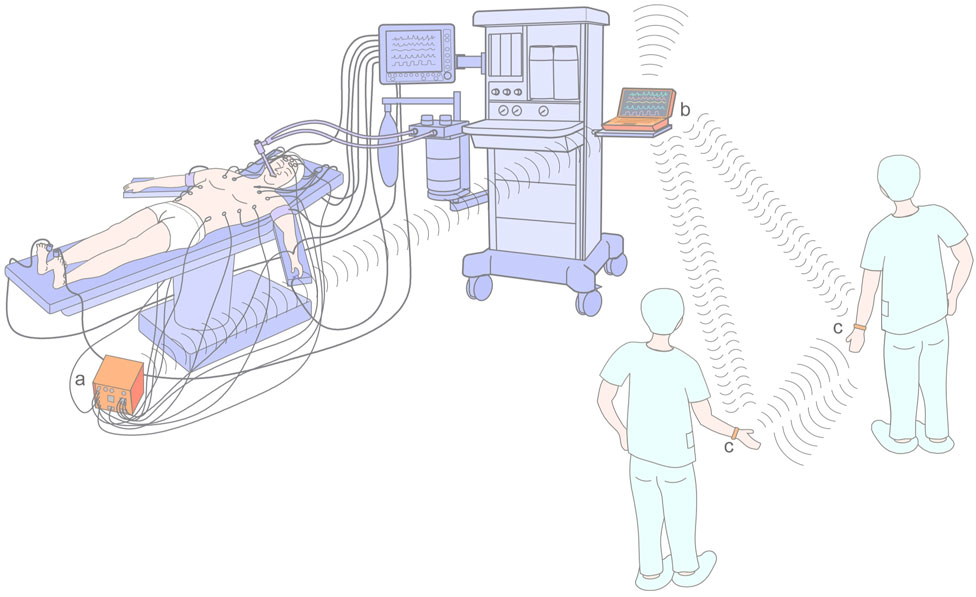
FIGURE 1. Interaction between system components. (A) Sampling unit, (B) specific application computer device, (C) wearable transponders. The computer device (connected to the peer-to-peer governance network) transmits the collected data in real time to the decentralized storage systems.
The descriptions refer to what the authors consider to be the best system configuration, but since various possibilities in component design and connectivity are compatible with the main objective, alternative implementations are mentioned.
We envision that this proof of concept should be initially implemented as a physically independent system from the anesthesia ventilator and multiparameter monitor. This is because it is a technically simpler way to evaluate its performance and adoption during early stages. It should be noted that the initial implementation as a stand-alone system can contribute to safety by being available as a second multiparameter monitor in the operating room, providing backup in complex scenarios where sensor malfunction, disconnection or interference may hamper decision-making processes.
5 Hardware
5.1 Sampling unit
The device consists of a module that contains an array of sockets into which cables from different sensors are connected. Its function is to collect data from sensors and deliver it to a dedicated computer device that broadcasts the data streams to remote storage systems. To provide a mechanism for tracking and measuring instrument performance, the sensors are equipped with an electronic identifier through which the system is able to register their specifications such as model, developer, serial number and time of use. Since the system is intended to be suited for research purposes, several sockets may be present for the same type of sensors.
Each channel receives a specific type of input consisting of biosignals from patients or data from electromechanical devices connected to them. These may include signals from pulse oximetry, electrocardiography, noninvasive blood pressure, invasive pressure, electroencephalography (EEG), near-infrared spectrometry, temperature, and data from the respiratory circuit (capnography, flow, volume, pressure, and gas analysis). Signals that require invasive instruments, such as intravascular sensors, can be electronically split and delivered to the sampling unit and main multi-parameter monitors from a unique transducer.
Data streams are preferably transferred to the computer device via wireless connectivity in order to prevent cables interfering with staff circulation in the operating room.
To maximize electrical safety for patients, this device is ideally powered by rechargeable batteries.
5.2 Specific-application computer device
This module is a personal specific-application computer, equipped with a screen and input devices such as keyboard, moused, knobs and buttons for easy user interaction. It contains the front-end software that allows the anesthesiologist to log into the system, authenticate, generate case registers, consult them and introduce supplementary information to the records.
This device receives the sensors’ time series from the sampling unit and transmits data streams to the remote storage systems via Internet connection. The sampled data is displayed in real time enabling users to interact with it through visualization tools and analytics software.
It is equipped with a fingerprint reader for generating biometric signatures during the anesthesia procedure. Geolocation and synchronization with universal coordinated time (UTC) is established through Internet connectivity.
A set of antennas built into the unit allows bidirectional connectivity with other devices maintaining constant communication with the wearable transponder2. In addition, an integrated very short-range radio frequency identification system (RFID) allows the detection of the wearable device in close proximity, providing a mechanism to validate operations on the computer device performed by the transponder holder.
5.3 Wearable transponder
This device consists of a unique personal smart bracelet equipped with accelerometers, fingerprint reader, vibration motor, sound emitting system, microphone and a magnetic clasp with an electronic contact. Its function is to provide the anesthesiologist with a self-authentication mechanism and generate evidence on the active vigilance of the anesthetized patient. This is done by measuring irregular acceleration patterns on the wearable and estimating the distance between this device, the computer, and the sampling unit through the wireless connectivity.
A very short-range RFID verifies the close proximity of the wearable during the computer device operation.
Bidirectional communication enables the user to remotely interact with the computer device through buttons and a touch-sensitive scrolling surface on the smart bracelet. The device is also able to receive signals from the computer which can trigger vibrations or sound alerts on it.
The built-in microphone allows the incorporation of voice notes to the records. Although the system is not conceived to incorporate personally identifiable information from patients, brief timestamped voice statements from individuals consenting to have their data recorded, can be integrated into the anesthesia record to provide a biometric proof of voluntary acceptance for their data processing.
5.4 Video synchronizer
This is a complementary device designed to synchronize third-party video recordings with the sampled data. It provides a precise mechanism to create multimedia content integrated with anesthesia data streams.
The device consists of an array of lasers which are pointed toward the surgical field or a site of interest. It is connected to the sampling unit or to the computer device and synchronized with the system´s native chronometer. A variable dot pattern is generated intermittently and projected by the lasers in synchrony with the time series clock. The dot pattern code embedded within the record, provides a way for any video content that includes the dynamic pattern in the filmed plane to be synchronized with the data streams by matching the visual time pattern with the one in the time series (Figures 2, 3).
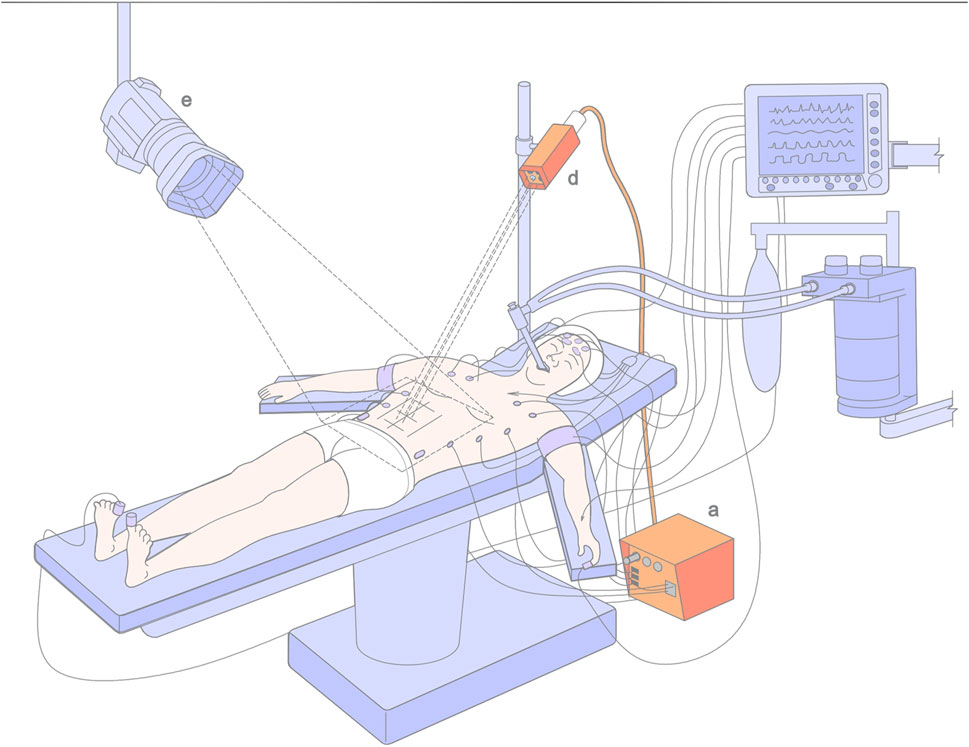
FIGURE 2. Method for synchronizing third party video. The (d) video synchronizer is connected to the system timer through the (a) sampling unit. It projects through its lasers a dynamic dot pattern synchronized with the system´s internal chronometer to the area being filmed by a (e) third party video camera.
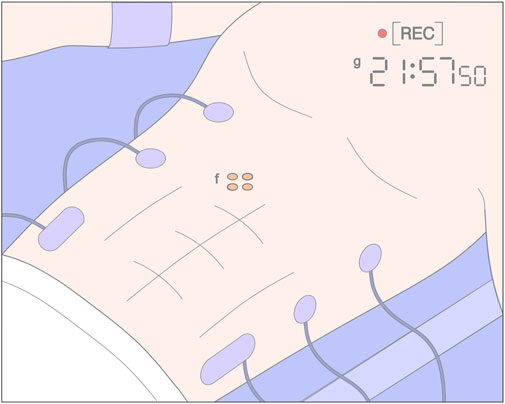
FIGURE 3. Filmed plane recorded by a third party video camera. The (f) dynamic dot pattern projected by the video synchronizer enables synchronization of the system internal timer (and therefore, the recorded time series) with the (g) third party video chronometer.
6 Software
The system software interconnects the hardware with distributed storage systems, blockchains and decentralized computing services. It provides a front-end interface on the computer device for logging into the online system and for interacting with the “governance layer”: a peer-to-peer network which coordinates the system components and in which decisions about the system infrastructure, flow of data and permissions are resolved by consensus.
The software facilitates data management and communication between devices. It allows users to customize data visualization and run applications to explore sampled information. In addition, it provides the interface to interact with machine learning tools such as artificial neural networks. Global data statistics are delivered for real-time visual juxtaposition with time series enhancing surveillance through trend extrapolations, Bayesian inference or the application of deep learning predictive models (Emmert-Streib et al., 2020).
7 Blockchain technology
Blockchain technology is implemented to provide a public register of the anesthesia records. Information such as record ID, anesthesiologist authentication, personal blockchain address signatures, record content hash, storage addresses, versioning, geolocation and timestamping; is embodied on blocks of public blockchains generating an immutable proof of record existence.
Users connect to the system through their unique accounts based on blockchain addresses (wallets) that provide proof of personhood and possess certain useful features such as Sybil attack resistance and community recovery (Siddarth et al., 2020). These accounts are also referred to as “Souls” in the context of Web 3.0 (Chohan, 2022) and are used to hold the professional´s commitments, credentials and affiliations in the form of “soulbond tokens” (Weyl et al., 2022). The application of this methodology is expected to be consistent with the future global adoption of universal identity systems based on distributed ledger technologies (Goodell and Aste, 2019; Zwitter et al., 2020). Anesthesiologists can thus take advantage of blockchain use cases to prove provenance, reputation and establish decentralized governance through innovative polling mechanisms such as quadratic voting (Lalley and Weyl, 2018).
8 Decentralized storage
Data streams are directly transmitted to distributed remote storage systems, initially saving the anesthesia records relying on architectural decentralization. To ensure data integrity and permanent accessibility, records are then retransmitted to one or more distributed storage networks structured on political decentralization.
Although an optimal implementation would involve transmitting data streams directly to politically decentralized storage networks, current technologies present slow upload and download speeds and do not allow information to be recorded in real time. To overcome this limitation, we propose to apply a remote storage system consisting of one or more architecturally decentralized (but politically centralized) databases for efficiently receiving the transmitted data in real time.
Once the anesthesia case is over and the record transmission to the remote databases is completed, it is integrated into a unique register and automatically retransmitted to architecturally and politically decentralized storage systems for permanent and immutable preservation.
Multiple types of databases can be implemented simultaneously to deliver streamed data: regular SQL, NonSQL or databases built specifically for time series (such as InfluxDB3 and TimescaleDB4). These can also provide efficient data access for machine learning model training, real-time analytics and data mining. Selected data can be filtered, categorized and saved in repositories in order to be readily available and interoperable for data science (Sessler, 2014; Epstein and Dexter, 2018).
“Content-addressable storage” (CAS) qualifies as an optimal scalable approach to store and reference permanent anesthesia records in architecturally and politically decentralized systems (Hinsen, 2020; Kumar and Tripathi, 2020). CAS delivered by peer-to-peer networks (as proposed by IPFS5) can further contribute to persistent data structures by providing logical decentralization (Benet, 2014; Buterin, 2017). This technology allows the long-term immutable storage of electronic objects using cryptographic hashes (calculated from the object content) as references to retrieve the original data. Hash-based IDs are unique identifiers that provide a permanent and unalterable address for future record reconstruction. Content-addressing guarantees that the links always return exactly the same content even though it may be redundantly partitioned and replicated onto arrays situated at different locations. Even if someone destroys all the copies on the network, it would only take one node adding the content in order to restore the global availability.
The CAS system is impervious to technological changes since the data remains accessible as long as an application server is able to map the address of the original content. It also prevents the data from being duplicated or modified once stored, therefore guaranteeing its legitimacy and integrity. A CAS-based end storage can simplify data communication between different software used in research and facilitate distributed computations.
In order to keep records always available, the content must be stored at least at one location. This is referred to as “pinning” in the IPFS protocol (Guidi et al., 2021). Objects can be pinned on local nodes or delegated to third-party pinning services. To provide scalable, cost effective and permanent storage, diverse storage services could be implemented concurrently or alternated if necessary; in this way storage redundancy can also be dynamically regulated according to the ecosystem´s needs.
Although native blockchains could theoretically be used to store data within blocks, the method would be impractical due to the extreme block size that would be required.
Since a primary goal of the system is to save an immutable copy of the record with the lowest possible latency in politically decentralized (and ideally, logically decentralized) storage networks; intermittent transmission of partial data sets could be considered as an alternative strategy.
9 Hyperscale computational network
The internal hardware of the specific-application computer devices, connected through a peer-to-peer network, may deliver a suitable computational power for coordinating the data flows according to the instructions on the governance layer. However, processing power may be limited as the system and data throughput scalate. Specific tasks regarding high-performance networking, big data processing and deep learning will require large-scale computations (Panda et al., 2022). To meet the needs, computing power, communication, memory and storage can be outsourced to decentralized services orchestrated from the governance layer.
9.1 System architecture
The network of peer-to-peer specific-application computer nodes, integrates into a governance layer. This structure exerts parallel control over the different system components: storage services, blockchains, and outsourced computational networks (Figures 4, 5). Its functions are:
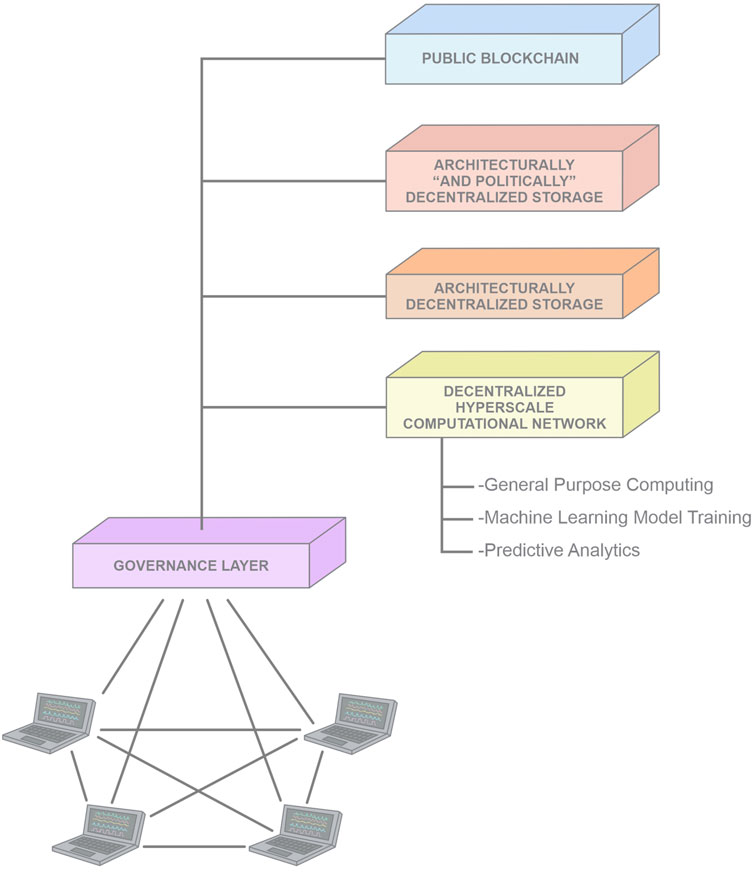
FIGURE 4. System Architecture: Component Diagram. The Governance Layer exerts parallel control over each component and coordinates the flow of the data.
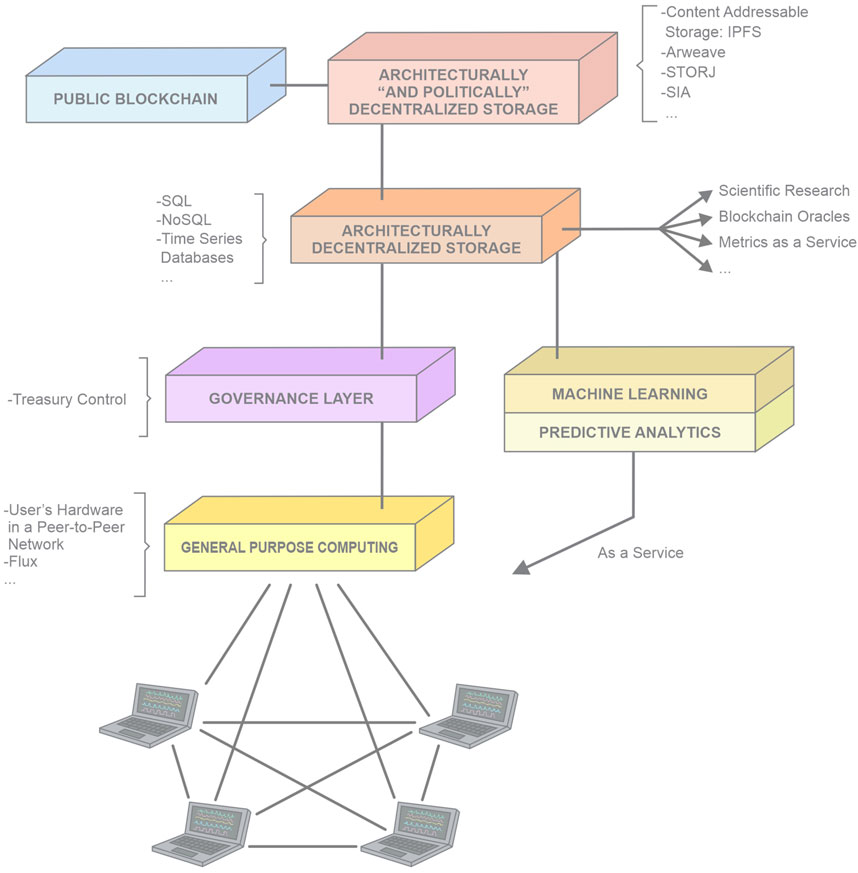
FIGURE 5. Interaction Diagram: the scheme represents a simplification of the data flow. It should be noted that every interaction is coordinated through the Governance Layer. The computational power is segregated into different independent systems which perform specific tasks.
Data Management:
- Verify the legitimacy of its users
- Certify the generated records
- Direct the data transmission to the storage systems
- Coordinate the flow of data between different storage systems
- Write the blockchain registers
Coordination for the Participation of Nodes:
- Conduct the voting system for: network consensus, use of the decentralized-treasury funds, improvement proposals, community consultation, insurance resolutions.
System Administration:
- System maintenance
- Accountability
- Outsourcing relationship management (for data storage, computational power, machine learning model training, and blockchain fees)
- Quality control of the generated information
- Accreditation of its members’ compliance
- Custody of internal system data (for example,; the distribution of split keys, information about members, internal registry of anesthesia records, history of queries to registers).
An inherent value of the system is that as a result of its processes, anesthesia records (which are encrypted and certified by the system) are stored and always available through content addressable storage, evidencing their existence on a public blockchain.
This implies that even if the system architecture ceases to exist, the records and the evidence of their generation and immutability would remain available. In this hypothetical case, since the system´s treasury is aimed to cover the costs for the pinning services of the records though smart contracts; these would remain pinned for a considerable period, allowing anesthesiologists and patients to download their records and pin them themselves to ensure their permanent availability.
Access to the content of the records, and thus the preservation of their privacy, would rely on the holders of their respective decryption keys. Interestingly, techniques for content erasure have been proposed for CAS in order to meet the “right to be forgotten” requirement for personal data protection regimes (Politou et al., 2020).
While the application of a second set of sensors connected to the patient could be considered as an over-engineering approach, it should be understood that this is implemented in this way to allow the gradual operation and testing of the concept without affecting the validated monitors of the operating room. We foresee that, if adopted, some components of future versions of the system could be simplified or even dispensed with. For example, the sampling unit could be reduced to a small module which may capture raw data wirelessly from multiparameter monitors and anesthesia machines. These in turn, should be able to transmit their raw data and the technical identifiers of their components. The wireless sampling unit could be further integrated into the specific application computer device, which may become a main multiparameter monitor in the operating room.
9.2 Methods
9.2.1 How is a record generated?
- Certified anesthesiologists use the specific-application computer, connected to the Internet, to log into the system through their password and biometric authentication. A blockchain-based personal identification account can also be paired to the system. This can be done by connecting a software cryptocurrency wallet (such as Metamask6) to the user interface or by signing a specific message with the private key of a proof of personhood wallet: for example, generating a signature containing the case record ID and its geolocation with the private key of a Proof of Humanity7 (PoH) Ethereum8 address (Buterin, 2014).
- The sampling unit is wirelessly paired with the computer device. Cables from sensors needed for the procedure are connected to their sockets. Each channel sampling rate is configured according to specific needs. For example, higher temporal resolution may be required for EEG channels in surgical procedures that generate useful data for neuroscience research.
- The wearable device is paired with the specific-application computer and sampling unit. The user puts the device on their wrist, closes the electronic clasp and self-authenticates using the fingerprint reader.
- Sensors are connected to the patient. A case register is created in the system using the specific-application computer device. Information related to patient medical history, procedure plan and professional team is introduced.
- A brief recording of the patient’s voice is obtained through the microphone on the wearable device. This provides a biometric consent declaration which is incorporated within the anesthesia record.
- Checklists are run to verify procedure details and check resource functionality and availability.
- Geolocalization and UTC synchronization are established.
- The user starts the recording by generating a fingerprint signature on the computer and wearable device. Sampled data is transmitted from the sampling unit to the computer device where time series are displayed on screen.
- Datasets are streamed in real time to the remote storage system via Internet connection. An internal memory stores the sampled data within the device to provide a buffer for transmitting deferred data in situations where Internet connection quality becomes low or interrupted.
- Generated information from the wearable and sensors is streamed in a time series format. Supplementary data expected to enhance the interpretation of the anesthetic procedure is manually incorporated into the register through the computer device. These data may include: sensor placements, medications administered, infusion rates, ventilator settings, comments, observations, voice recordings and photos or videos from authorized devices.
- At the conclusion of the anesthesia procedure, the anesthesiologist confirms the end of the recording with a new biometric signature.
- Once the complete set of data from the anesthesia procedure is received by the remote databases, it is then integrated, packed and retransmitted with the lowest possible latency to an architecturally and politically decentralized storage system (such as IPFS3, Arweave9, Storj10, Sia11) where they are permanently stored.
- Blockchains are implemented to automatically generate a public timestamped proof of record existence, certifying the provenance and authenticity of purported factual recordings. An automatic register is generated on a block of a public blockchain consisting in a digital signature encoding specific information such as:
- anesthetic case record identifier
- anesthesiologist identifier
- signature from an anti-Sybil personal address (or from a related dedicated address)
- record version
- timestamps (defining case time interval)
- geolocation
- addresses of the decentralized databases in which the record is stored
- hash of the record content (to validate data immutability and to retrieve records from CAS)
- Keys for decrypting the stored files containing the records are generated for the anesthesiologist and the patient. Additionally, a special split key, such as a Shamir key (Shamir, 1979), is randomly and redundantly distributed among users to provide a mechanism for record decryption through the system consensus. This enables a democratic community retrieval of the record information in situations where neither the patient nor the anesthesiologist can provide the decryption keys (Benzekki et al., 2017).
- On completion of the anesthetic procedure, the system generates an electronic certificate which is sent to the anesthesiologist´s computer device. It incorporates the record identifier, the encoded register uploaded to the blockchain and the block header. This certificate can be attached to the hospital medical record and delivered to the patient.
- As a result of the described processes, a register for each case is generated in a public blockchain certifying the existence, storage and authenticity of the anesthesia record. Blockchain scanners can be used to verify registers and are therefore essential to support a universal logbook containing blockchain-certified professional cases. A system internal ledger available off-chain can facilitate data accesibility avoiding the need to scan entire blockchains to search and retrieve records.
- Anesthesia records authorized by patients can be made available for use in data science and research. Patients can provide customs permissions to use or restrict specific types of information from their records.
9.2.2 How is new information added to an existing record?
The system architecture is conceived so that the original data cannot be modified or deleted. Amendments and additions are allowed to the creator of the record, in a timestamped and layered structure, preserving the historical data always accessible.
Data can be corrected or added by recovering the record from the decentralized databases through the system software. Once modifications have been made, the new complete record is uploaded to the architecturally and politically decentralized database and a new blockchain register is generated. As an alternative implementation, the system could upload just the new record layer, referencing in the blockchain register the entire set of layers prior to the original.
9.2.3 How is a record retrieved?
Records can be retrieved autonomously using their blockchain identifiers which specify versions, storage addresses, and content hashes. Decryption is performed using the keys of the patient or the anesthesiologist.
Retrieval can also be done through the system by requesting the data recovery from the computer device of the record creator. After verifying the identity of the user, data packages are downloaded, and the record content is decrypted. Anesthesiologists can thus consult and review previous anesthesia records from their patients without the need to handle the specific decryption keys. A history of record queries is automatically generated by the system.
Community recovery can be achieved with the randomly distributed key through the consensus of users. These are randomly selected and subjected to consultation in order to establish whether the retrieval and decryption of the anesthesia record for each particular case is justified and in accordance with ethics and law.
9.2.4 Wearable device operation
The interconnection between the wearable transponder, the sampling unit and the computing device allows the dynamic estimation of distances between them and, therefore, the extrapolation of spatio-temporal information between the patient and the anesthesiologist. Accelerometers built into the wearable device sample acceleration patterns which are expected to be irregular when worn by a person. Movement patterns can be automatically detected by the system but also efficiently verified using artificial intelligence. Measurements from the wearable sensors are transmitted along with the time series, thereby generating an automated proof of active permanence within a safe distance from the patient.
As a routine protocol, the system stochastically requests biometric authentications on the wearable. To improve the verification mechanisms, the device can be linked to a personal-identity blockchain address (such as the proposed by PoH) so that when a biometric authentication is produced, signatures or non-interactive zero-knowledge proofs12 (Blum et al., 1988; Buterin, 2022b) are delivered to the system.
To avoid the risks of dealing with private keys of a personal ID public address, the user can link it to a dedicated address. For example, the governance layer can issue a soulbond token (ideally a non-transferable token) which exhibits: a) a PoH address (or similar service), where this soulbond token is delivered and expected to be held; b) an anesthesiology dedicated address (generated by the user) and; c) a signature emitted from a system official address (as a membership certificate) having both addresses (a+b) as the input content of the signed message. The user incorporates the secret key of the dedicated address into the wearable transponder which enables it to generate off-chain signatures or zero knowledge proofs (ZKP). This method would provide evidence that the fingerprint signer is in physical possession of the cryptographic seed of the dedicated address. This public address has an inherent value for the user as it is used as a unique account for the system and as the identifier for the professional log, the generation of reports, and the issue of certifications (Figure 6).
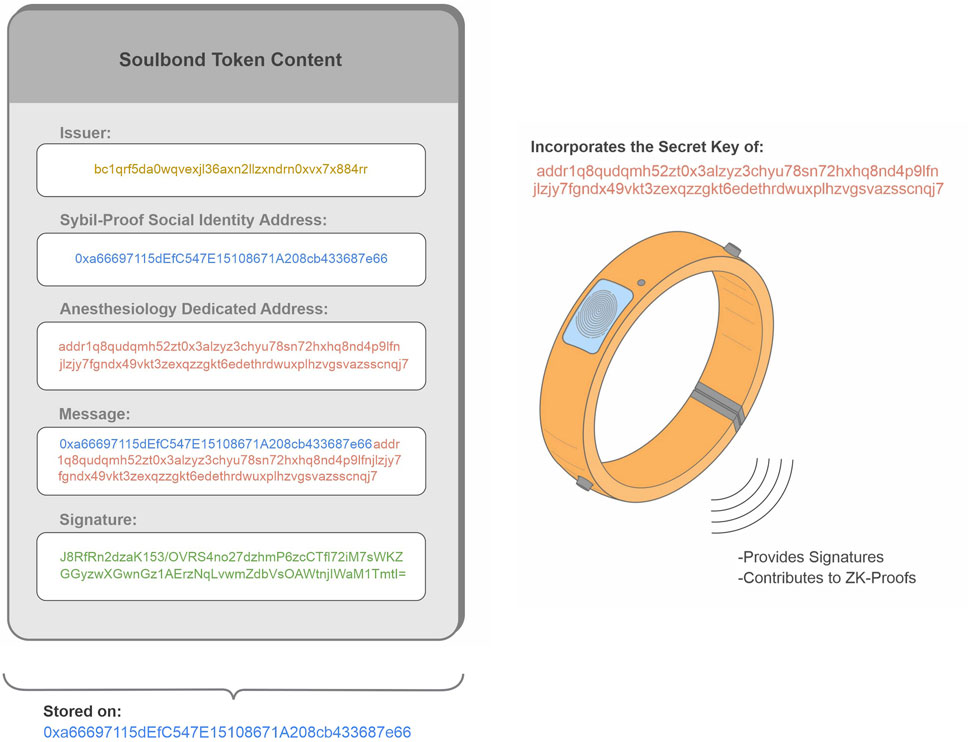
FIGURE 6. Soulbond Token containing a signature13 (in green) emitted from a system official address14 (in yellow: a bech32 Bitcoin address). The message contains a personal ID address15 (in blue: an Ethereum Externally-Owned account such as used in PoH), and an anesthesiology dedicated address16 (in red: a Cardano Shelley address). The token is stored in the user’s personal ID address. The secret key of the dedicated address is incorporated in the wearable device, allowing it to provide signatures or generate non-interactive zero knowledge proofs. Different blockchains were used to demonstrate the implementation versatility. The signature can be verified at https://www.verifybitcoinmessage.com/.
13 J8RfRn2dzaK153/OVRS4no27dzhmP6zcCTfl72iM7sWKZGGyzwXGwnGz1AErzNqLvwmZdbVsOAWtnjIWaM1TmtI=
14 bc1qrf5da0wqvexjl36axn2llzxndrn0xvx7x884rr
15 0xa66697115dEfC547E15108671A208cb433687e66
16 addr1q8qudqmh52zt0x3alzyz3chyu78sn72hxhq8nd4p9lfnjlzjy7fgndx49vkt3zexqzzgkt6edethrdwuxplhzvgsvazsscnqj7
To ensure that the wearable device is worn by its legitimate owner, biometric authentications are requested each time its contact is closed. This is because it is expected that the anesthesiologist may need to take the bracelet off during certain procedures, for example, when placing a central line. Successive openings may increase the frequency of stochastic authentication requests.
Alerts on parameters outside normal ranges transmitted from the computer can trigger vibrations and sounds in the wearable device. Also, circumstances automatically interpreted as suboptimal patient surveillance generate alerts and response requests on the wearable. These may include: lack of response to consecutive requests, failure to detect the wearable within a safe distance for a time considered to imply risk for the anesthetized patient, prolonged accelerometers inactivity and, detection of continuous regular motion in the wearable. In these cases, the algorithm may increase the frequency of stochastic authentication requests on the device. Requests and authentications are recorded in real time.
The smart bracelet can be used to remotely interact with the computer device allowing to silence alarms and navigate through menus via a touch-sensitive surface. It can be programmed to generate vibration patterns to indicate attributes of the sampled signals such as heart rate, oxygen saturation, blood pressure and airway compliance among others.
As a safety feature, the wearable device can autonomously alert the user through vibrations or sounds when it senses permanent motion inactivity or loses connection with the computer device due to excessive distance or poor signal quality.
The very short-range radio frequency system, integrated in the wearable and in the computer device, functions as an automatic proximity detector that differentiates computer manipulations done by the user carrying the wearable. This connection can be used as an additional mechanism for unlocking special functions by close proximity such as alarm settings and display customization.
9.3 Overview
The proposed system architecture addresses the aforementioned features in the following way:
1) Automaticity: Sampling and recording is done automatically, reducing distractions and allowing anesthesiologists to focus on patient care. Sensor measurements are transmitted directly avoiding the inaccuracies of manual data transcriptions.
2) Synchronicity: Data is simultaneously recorded in the electronic system as it is sampled by sensors, eliminating asynchrony between what is happening and what is being registered.
3) Decentralized Storage: Definitive storage of the records takes place in architecturally and politically decentralized databases. The system is able to delegate the storage to the most convenient services and regulate data redundancy based on needs.
4) Accessibility: Record availability is ensured through storage decentralization allowing censorship-resistant data retrieval worldwide. Patients benefit from having their anesthesiological history instantly available globally.
5) Encryption: Data is encrypted from sampling to storage processes. Different decryption keys are delivered to the patient and the anesthesiologist. A special redundantly partitioned key is randomly distributed among users to enable community recovery of records.
6) Real-Time Transmission: Data received by the computer device is transmitted immediately or with minimal latency to remote databases.
7) Biometric Authentication: Anesthesiologists sign their records through the fingerprint readers on the computer and wearable device. Patients incorporate their consent to sample and save their data through a short recording of their voice (not mentioning personally identifiable information) via the microphone built into the wearable. Instantly hashed, time-stamped raw audio verifies that voice recordings are not generated at a later time. In addition, open source signal processing facilitates the application of synthetic-speech detection methods to ensure that recordings are not created by a voice generator or impersonator software (Dinkel et al., 2017; Borrelli et al., 2021). In this way, each anesthesia record incorporates a biometric signature of its creator and a biometric proof of the patient’s authorization and permissions for the generation and processing of their data.
It should be noted that biometrically generated information is enclosed within the encrypted records and is not made publicly available as part of the metadata.
8) Traceability: Data is recorded with a certification of their respective geolocation and UTC timestamps which are determined through the network connectivity. This information is also embedded and publicly available on the blockchain register.
9) Confidentiality/Privacy: The identity of the patients remains confidential since the records do not contain personally identifiable information. However, if a patient register ID is forgotten or lost, it can be traced back by matching previously patient-authorized tracking tags such as type of procedure, anesthesiologist ID, date, geolocation or specific patient characteristics. The implementation of smart contracts to support data usage consent can further ensure the confidentiality of personal information shared with multiple data controllers and processors (Kaaniche et al., 2020).
10) Availability of Data on the Interaction between System Components: Anesthesia records contain information on the dynamic interaction between the anesthesiologist and their patient, which is extrapolated from distance and acceleration data from the wearable transponder.
Wearable devices provide trainees with a mechanism to record and certify their actively supervised anesthesia cases. Data collected throughout the anesthesiologist career can support an updated interoperable register to provide proof of training and proficiency worldwide (Simpao et al., 2011). Similarly professionals who supervise anesthesiologists in training can provide objective evidence of their involvement and expertise as instructors through their personal records.
11) Data Immutability: Content hashes certify the immutability of records. A persistent data structure ensures access to historical information by adding corrections and new data without overwriting the original entries. Modifications to records are incorporated in a layered structure, on top of previous data, so that information from all versions is preserved.
12) Blockchain Data Stamping: Proof-of-existence is available on-chain embedded on blockchain blocks as public evidence of the generated records. It encodes information about:
- record identifier
- record version
- anesthesiologist identifier
- hash of the content (for retrieval of records saved as CAS and for verifying record immutability)
- geolocation
- time window within which the record was generated
- file storage addresses (path for file reconstruction)
- blockchain block headers containing registers from previous versions
- file storage addresses of previous versions
13) Universal Instrument Identification: Sensors and system components provide their electronic identifiers which are incorporated in the record and enable the tracing of their use time and their performance evaluation. Signal processing algorithms are also electronically referenced and transmitted within the records.
14) Technology Independence: System sensors are independent and autonomous from those provided by the anesthesia machine and its multiparametric monitors.
Alternative third-party sensors may be compatible with the system as long as they are based on open-source technology and provide electronic instrument identifiers.
15) Bidirectional Communication Support for Wearable Devices: Wearable transponders maintain two-way communication with the computer device enabling remote operation, self-authentication and voice recording.
Users can be alerted through the wearable via vibration or sound whenever the system interprets measurements consistent with situations of risk for the patient. The wearable can alert the user autonomously even when it has no connection to the computer device.
Short-range RFID validates computer manipulations carried out in close proximity to the transponder worn on the wrist of the user.
Information generated by the wearable is included in the anesthesia record.
16) Anti-Sybil Backed System: Blockchain-based “unique human identity systems” can be integrated by linking blockchain accounts to the user profile or by incorporating signed messages within the anesthesia record. As an example of the latter case, signatures can be generated with the private key of a personal identity blockchain address and embodied in the record. Alternatively, a system dedicated address, linked to the user´s personal identity address can be utilized to generate signatures or ZKP.
17) Decentralized Governance: System improvements, planning and policy making can be decided through system community voting. Blockchain based user profiles provide trustless mechanisms for democratic consensus.
18) Output Data Interoperability: The system advocates the exchange of electronic information. It generates an organized information outflow ready to provide off-chain data to blockchain oracles (such as Chainlink17). Records can be tokenized and integrated into smart contracts for automated execution of programmable agreements.
19) Synchronizable Records: An output channel is available for synchronization with the system´s internal timer. A mechanism to synchronize third party video recordings is provided through the projection of lasers in the vicinity of the surgical field.
20) Dedicated System: The system is custom designed for the exclusive use of anesthesiologists. Soulbound tokens can be issued (and potentially removed) by a decentralized community of anesthesiologists as a method for certifying membership and ethical compliance.
21) Open-Source Framework: Hardware, firmware, and software components are open-source by default and therefore technically auditable.
22) Predictive Analytics and Machine Learning Compatibility: Statistical information generated by the system is available for real time juxtaposition with sampled data during anesthesia procedures. Machine learning delivered as a decentralized service (as proposed by Gensyn18), can potentiate system data analysis.
The scientifically rigorous data generated by the system is technically ideal for feeding artificial neural networks. In this framework, it should be noted that the system could leverage the application of “federated learning” and “federated analytics”: machine learning techniques that train algorithms for generating models and predictions across multiple decentralized nodes without the need to exchange or centralize data sets (Rieke et al., 2020; Short et al., 2022). These may become essential implementations in the field of anesthesiology, as they would address critical issues concerning data privacy, data security, and access rights while taking advantage of distributed computation.
Interestingly, distributed learning may coexist with decentralized storage as nodes could train their local data while permanently storing it on politically decentralized storage systems. In this way, each node could retain governance rights over its generated data while preserving a mechanism for the system community to access it through the consensus of the decentralized governance layer.
Since reliance on data is essential to generate accurate models; the need for a governance layer to ensure data integrity and filter out unacceptable nodes seems critical.
Live-streamed data can be used for modeling, calibrating and auditing technologies based on artificial intelligence such as automatic closed-loop infusion systems.
23) Compatibility and Interoperability for Supplementary Data Incorporation: Users are incentivized to generate rigorous and exhaustive records as these are cataloged according to their completeness. Datasets incorporating accurate supplementary information are expected to be valuable for researchers from different fields. Records utilized for scientific research can be publicly certified by the system. These can be used to establish a reputation of users as research contributors.
24) Customizable Screen System Interface: The computer interface enables anesthesiologists to customize the screen according to personal preferences. Sampled data can be displayed with innovative visualization modes such as tridimensional representations or tunnel navigation. A rapid, standardized display mode is available for emergency consultation with colleagues who may not be used to a personalized screen configuration.
25) Software Tool Compatibility: Software tools run over a failsafe firmware layer allowing users to perform measurements on the data shown on-screen and to apply predictive analytics algorithms.
Users are able to create their own applications and share them with the system community for testing. Innovative software tools that prove useful and are validated by scientific consensus can be made available to the ecosystem.
10 Section C: Innovation, future vision and limitations
10.1 Innovation
Blockchain technology is increasingly gaining adoption in several environments. Aviation (Ahmad et al., 2021), robotics (Lopes and Alexandre, 2019; Strobel et al., 2020), agriculture (Xiong et al., 2020), healthcare (Saeed et al., 2022; Thakur, 2022) and supply chain management (Munir et al., 2022) are examples of activities where this technology is explored. The idea of blockchain applicability in the field of anesthesiology has been proposed (Bellini et al., 2019; Jain, 2019). While specific implementations to use blockchain for the anesthesia records have been suggested (Figar Gutiérrez et al., 2021), our technology concept differs in two fundamental aspects: a) the proposed architecture seeks to not depend on monolithic private services and instead, use them if needed, as replaceable modules; and b) we propose to rely on layer-one blockchains to take technological advantage of the security and decentralization of their consensus mechanisms. That is, implement “real blockchains” and “real politically decentralized storage systems” and not depend on “storage services with blockchain characteristics”.
Conceptually, we seek to develop an integral architecture that minimizes systemic over encapsulated complexity (Buterin, 2022c) while preserving decentralized governance, data immutability and accessibility. On this basis, fully decentralized computing networks (as proposed by Flux19 and Internet Computer20) should be conceived as a plausible implementation to allocate the computing power infrastructure of the system. Also in this context, decentralized wireless networks (as proposed by Helium21) should be considered as an ideal global communication technology for the devised architecture.
10.2 Anesthesia records as a blockchain oracle
The work of anesthesiologists within health systems is exceptional since they objectively measure multiple parameters related to patients, machines, medications, and diverse technological resources. The proposed system provides continuous data streams whose inherent characteristics make them suitable for feeding analytics systems and for supplying off-chain data to blockchain oracles (Caldarelli, 2020; Ezzat et al., 2022). The generated data is technically valuable as it originates from a complex control system in which many variables are measured and whose different components have distinctive reasons to support the quality of the registration process. These components are naturally coordinated to generate a robust and coherent data flow. The concept should be explained from four different perspectives, each of which presents specific incentives for preserving data integrity and for preventing other parties from colluding against the system:
Patients: Patients logically demand safe anesthesia and quality of care. They expect their anesthesiologist to be qualified and trained to resolve any potential complication. Patients are aligned with the preservation of data integrity, since it prevails as evidence in cases of harm or death. Records are also valuable as documentation of their anesthesiology history for future interventions.
Anesthesiologists: Although practitioners are naturally motivated to provide safe anesthesia to their patients, they are also expected to benefit from data integrity and legitimacy as it feeds their professional log and builds their reputation in the system. In addition, the recorded evidence of compliance with safety standards is a technological protective factor against liability risks.
Society: Data integrity contributes to society by improving anesthesiology outcomes and quality through scientific research. Data tampering is expected to be repelled and reported, as adulterated data can undermine patient safety.
Companies: Companies are expected to appreciate transparent data as they can leverage metrics, supply chain analytics and pharmacovigilance. Rigorous data drives free and fair competition and provides a major incentive for companies to oppose data fraud.
The described system components interact so that each party is encouraged to take advantage of legitimate data and motivated to verify the reliability and validity of the other components. This mechanism of cross auditable interactions provides a collusion resistant system optimized to provide accurate data flows.
10.3 Safety of human life as a measurable asset
Human life can be considered the worthiest asset. Estimating its intrinsic value is analytically complex and objectively unfeasible due to the myriad of variables that should be taken into consideration. However, anesthesiology provides scenarios in which human life is in a standardized state of potential vulnerability due to the lack of self control. Here, the costs and performance associated with the safe care of human life can be objectively measured.
The value of human “health” is also difficult to calculate due to the subjectivity of considering the specific characteristics of patients and of measuring isolated variables from health systems. For example, it would be impractical to establish a standard health value based on a surgeon’s skills, or on a tangible item such as a specific medication or treatment. Both approaches would result in deviations due to interindividual skill disparities in the former, and medication price volatility over time in the latter.
We propose that real-time multivariable recordings can be used to objectively determine the costs related to intraoperative anesthesia procedures through the integration of biosensor time series (and hence data on the performance of the anesthesiologist) with information related to case complexity, medical resource requirements, pharmacological consumption and use of technology. Global statistics can reduce variability and eliminate bias and inconsistencies.
A decentralized blockchain oracle can rule an open-access standard price in health systems which can be used as a financial reference value. This can provide a mechanism to scientifically determine minimum ethical wages for anesthesiologists (and extensively for other health professionals). The latter should be understood as the minimum payment rate that professionals should ethically receive during a specific procedure for health systems to coherently guarantee compliance with safety standards. This can prevent detrimental consequences from unfair or distorted billing systems which, through professional overload (West et al., 2018; Afonso et al., 2021; De Hert, 2021), can lead to decreased situational awareness (Schulz et al., 2017), sleep deprivation (Howard et al., 2003; Neuschwander et al., 2017; Wong et al., 2018) or indirectly induce unsafe practices such as simultaneous anesthesia (Burns et al., 2022), absence from the operating room, or protocol circumvention.
Oracles can automatically classify anesthesiological procedures based on analytical criteria such as patient characteristics, case complexity, procedure duration, incidence of complications, professional proficiency and training requirements. An updated categorization of anesthesiological procedures can improve patient safety by establishing a scientific scale for professional fees, so that cases that are more sophisticated or require more complex skills, are higher ranked. We believe that anesthesia billing structures should position the economic incentives to reward continuous professional education, training and deliberate practice (Hastings and Rickard, 2015), overcoming schemes that can potentially lead to academic outdating or competency obsolescence.
An “anesthesiology blockchain oracle” fed with continuous multivariable data streams can theoretically engender a token tied to healthcare. Global intraoperative sampling could provide a formal way to estimate the value of assuming the responsibility for taking care of human life.
Interestingly, the performance evaluation of intraoperative anesthesia through the proposed measurement system may contribute to practical solutions for some crypto-economic problems termed as “Proof of Excellence” and “Decentralized Success Metrics” (Buterin, 2019). The former refers to token distribution and involves creating a task that only humans can do (or are the only ones authorized to do) but that computers can easily verify. The latter problem consists in implementing a decentralized method for measuring numerical real-world variables.
Finally, it should be noted that an anesthesiology oracle could provide a useful source of entropy (such as League of Entropy22 and Random.org23), operating as a publicly verifiable randomness beacon (Stipčević and Koç, 2014).
10.4 Professional interoperable CaseLog
The interrelation between blockchain technology and distributed storage should provide anesthesiologists with a universal professional record. A personal logbook can be made globally available supplying interoperable evidence of professional proficiency and expertise. Quantities, types and performances of cases carried out during an anesthesiologist´s professional career could be verified on the decentralized and immutable register.
Wearable transponders enable professionals in training stages to formally register their actively supervised cases. Similarly, those in charge of academic training are able to accredit their activity as supervisors.
The envisaged system should contribute to the anesthesiologist community by providing a transparent tool to issue evidence of professional suitability and thus facilitate transnational interoperability. Work experience involving geographical exchanges should enhance the spread of knowledge and professional development.
10.5 Academic incentives
The system aims to foster individuals to seek excellence in their generated data. Records can be categorized according to the quality of their measurements and their completeness. Targeted incentives can be granted for provenance-rich data, uninterrupted sampling, interference-free datastreams, continuous proximity to the supervised patient and for the quality of the supplementary information. Users can be referenced according to the suitability of their records for use in scientific research. Greater demand is expected for high-quality data generated by better referenced users.
10.6 Governance
User profiles linked to unique blockchain anti-Sybil identities provide the means for a voting system, enabling affiliates to reach consensus and take decisions collectively without relying on a central authority (Honkanen et al., 2021). Decisions on the direction of the ecosystem, such as improvement proposals and technology implementations can be achieved through the decentralized polling mechanism (Zwitter and Hazenberg, 2020).
A scheme of challenges can incentivize the network to verify the professional performance, accreditation fulfillment, and safety compliance of its participants, thus ensuring the scientific and ethical integrity of the system. In this way, the admission and rejection of users is constantly determined by the consensus of the ecosystem. Scalability and global adoption can drive a “network state” (Srinivasan, 2022): a translational online community of anesthesiologists organized around the values of Science (Bunge, 2018).
10.7 Sustainability
The costs of system maintenance, processing power, data storage, audit incentives and blockchain fees must be covered by a sustainable contribution mechanism. While a payment system analysis is beyond the scope of this paper, potential implementations of blockchain technology should be considered.
We believe that from an ethical perspective the system’s cost should be covered by users themselves and patients should not be charged. A real-time blockchain micropayment system (Klein and Stummer, 2021) applied during the data transmission process can provide a fair alternative to the subscription model, such that users are charged only by their transmitted data and can freely decide whether to record their specific cases on the system.
Taking advantage of blockchain transparency and traceability, a cryptocurrency treasury can be established and controlled by the governance layer through the voting system. Smart contracts can be programmed to automatically pay the costs for storing and pinning services directly from the system reserves. The treasury can provide funds according to the ecosystem´s investment interests such as scientific research, production of educational content, simulation training, technology development and provision of resources for anesthesiologists in areas of need (Warner et al., 2022). Also, in return for generating the anesthesia record, patients and anesthesiologists can be insured by the system treasury (Shetty et al., 2022). In this way, costs of potential legal demands and compensation for injuries or sequelae during recorded anesthesia procedures can be covered directly by the system.
Users can be randomly requested to audit anonymous records in order to interpret cases which need clarification. Worldwide users with diverse professional backgrounds can determine through recorded measurements whether the execution of the audited anesthesia was carried out competently in accordance with safety protocols. Through this mechanism, the ecosystem consensus can resolve the release of funds for each particular case in a fair and impartial way.
Part of the system liquidity can be collectively managed to generate income through the investment in projects or protocols enabling users to reduce (and potentially eliminate) their system usage expenses. Not only this could result in a feasible cost-free service and professional insurance, but also in a potential retirement fund system (Sarker and Datta, 2022). Furthermore, utility tokens can be minted by the system mechanics contributing to its sustainability through the application of strategic tokenomics (Freni et al., 2022).
10.8 Record audit structure
It is expected that any anesthesia record may require an audit or an expert opinion emitted by a third party or legal entity. The system can contribute by providing a mechanism for cooperative issuance of formal interpretations.
Users with different backgrounds and diverse professional expertise can be incentivized to review records and submit their findings and conclusions. Sustainability of the audit structure can be achieved by paying contributors according to professional expertise.
In order to guarantee confidentiality and impartiality throughout the entire review process, traceable content is hidden and records are kept anonymous. Reports on records are authenticated by their reviewers and made openly available enabling the ecosystem to audit and object to the review process. Users can be randomly incentivized to create and inject fake records with incorrect, imprecise or unreliable information in order to reward reviewers who consistently detect inaccuracies.
In addition to auditing purposes, a report system should be available to communicate accidents, near misses and rare events related to patients, medications, surgical procedures, or equipment performance. In this way colleagues can evaluate, provide suggestions and validate data for its correct interpretation. A library of scientific case reports selected by the ecosystem can be created for educational purposes.
10.9 Artificial intelligence
Feedback control systems have potential application in the field of anesthesiology. Artificial intelligence algorithms can integrate datastreams in real time and efficiently anticipate the physiological and biochemical evolution of patients (Hashimoto et al., 2020).
Upcoming technology will likely provide automated control of drug infusion systems and anesthesia machine parameters, leading to more precise and accurate performance (Zaouter et al., 2020). Although from a safety perspective automated systems are not expected to replace human anesthesiologists, new technologies will probably expand their tasks and require professionals to operate and supervise automatic control systems (Lonsdale et al., 2020). This will propel professional development of future anesthesiologists into formal science fields such as mathematics, computing and engineering.
The development of control systems driven by artificial intelligence will require implementation stages in real scenarios (Magrabi et al., 2019; Canales et al., 2020). The immutable, authenticated and timestamped data generated by our proposed architecture is theoretically applicable for optimally feeding these systems and for providing continuous technological surveillance of innovative implementations (Parvinian et al., 2018). We believe that systems which exert control over humans through artificial intelligence should be auditable through an open science framework (Paton and Kobayashi, 2019).
10.10 Neuroscience and neurotechnology
Intraoperative anesthesia provides exceptional opportunities for the sampling of EEG data. Diverse cases require different types of anesthesia; from sedation to deep hypothermic circulatory arrest (Mavroudis et al., 2018; Alkhatip et al., 2021). Open source neurotechnology and standardized protocols can provide vast datasets for neuroscience research.
We believe that anesthesiology should play a leading role in addressing fundamental problems of neuroscience. There is arguably no medical specialty better positioned to pursue a comprehensive explanatory framework for understanding how the electrochemical activity of the brain generates perception; also known as “the hard problem of consciousness” (Chalmers, 1995). Assessment of the activity and interactivity of neural structures during different states of anesthesia can elucidate the core requirements for conscious experience.
Coordinating efforts through a collective “laboratory” composed of operating rooms around the world measuring information processes about conscious state transitions is expected to generate valuable data to consolidate physiological knowledge of neural encoding (Mashour, 2022). Making foundational scientific contributions to understanding the neural basis for consciousness is important for anesthesiology since solving this challenge will provide insights into what brains are naturally engineered to do (Alkire et al., 2008). Ultimately, this knowledge will help in understanding how to improve patient safety.
10.11 Software for simulation
Simulation-based education in anesthesiology has gained wide integration over time (Higham and Baxendale, 2017). However, development of anesthesia software simulators has been limited and scarce evidence of their implementation is available in the current literature. We believe that the potential of software simulation is under-exploited. Unfriendly operability, outdated graphics, limited scenarios and expensive subscriptions for individuals can negatively affect their widespread adoption (Edwards and Lampotang, 2020).
The system treasury can fund and sustain a continuously updated high fidelity software simulator.
Next-generation game engines (such as Unreal Engine 524) can deliver photorealistic point-of-view simulation environments (El-Wajeh et al., 2022). Furthermore, virtual and augmented reality technologies may be adopted over time if their generated immersive experiences prove to be superior in cost/effectiveness terms over screen-based simulation (Alam and Matava, 2022).
To provide evidence-based scenarios, simulations can be fed by global data generated by real cases. Intraoperative physiology and biochemistry can be simulated by integrating big data from anesthesia records enhanced by machine learning technology.
Anesthesiologists can learn and train with a high-fidelity software simulation platform and test their proficiency through automatic system examinations which generate blockchain certifications. Pushing this idea further, official examinations can be enhanced by compensating users with system retributions (such as credits or storage capacity), for the simulated time according to payment rates consistent with actual anesthesia cases, therefore mitigating the obstacle of prolonged times required to perform truthful scenarios. This would reduce the bias of “short latency times” generating a realistic length simulation in which subjects do not tend to become hypervigilant while aware of being in a simulation, expecting critical events to be triggered imminently in the first minutes.
The wearable transponder can be used to validate users performing simulations by matching their acceleration patterns with movements in the virtual environment.
10.12 Academic content production
A decentralized educational platform can be created by funding high quality multimedia content creators through community voting (Leible et al., 2019; Rahardja et al., 2021). Educational content may include lectures, tutorials, anesthesiological metrics, case reports, measurements on specific procedures, near-misses and accident reconstructions.
System governance can democratically fund research and scientific publishing in accordance with the ecosystem academic objectives (Mackey et al., 2019).
10.13 Limitations
Although this proof-of-concept advocates decentralization, it is important to note that a governance layer is necessary in order to ensure scientific rigor. This implies that a self-governed community should be able to determine which professionals are admitted or rejected, based on accreditation of professional certifications, compliance with patient safety and adherence to quality standards for data generation. It should be noted that decentralized governance may introduce potential drawbacks to the system that will require its definitive implementation to be a meticulous process (Buterin, 2021).
A decentralized autonomous organization (DAO) can potentially be assembled on top of the system (Ziolkowski et al., 2020; Liu et al., 2021); however, since there is no precedent for similar implementations in anesthesiology, we believe that full decentralization should be achieved gradually if possible (Buterin, 2022d; Henrik et al., 2022).
Whereas different blockchains may be implemented (Tasca and Tessone, 2019), it would be opportune to materialize their functionalities through projects founded on peer-reviewed research (such as Cardano)25 and developed through evidence-based methods consistent with our system’s inherent philosophy.
We anticipate adoption resistance as a primary limitation to scalability. Unfamiliarity about novel technologies and the need to use additional hardware may restrain acceptance by professionals (Lustenberger et al., 2021). However, we foresee that as the global community gradually assimilate the benefits of decentralization and data immutability, the proposed system architecture may become a new paradigm in the way data is recorded in operating rooms (Pandya et al., 2021). In the long run, global adoption is expected to be driven by patient demand for modern safety technologies.
10.14 Closing thoughts
Keeping control of patients’ parameters in all scenarios is a central goal of anesthesiologists. We believe that health professionals who work with control systems should stream and record immutable data as proof of transparency and respect for human life. Great progress in the field can be driven by generating accurate records and making measurements openly available to science.
The proposed architecture seeks to provide a transformative path for anesthesiology, assuming as a guiding principle that “better information makes for better decisions”. In summary, this is how we believe technology should be implemented to scientifically improve patient safety, outcomes, and quality.
“Whereas science elicits changes in order to know, technology knows in order to elicit changes.”
- Mario Bunge
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author. Authors declare the following official manuscript blockchain address: bc1qrf5da0wqvexjl36axn2llzxndrn0xvx7x884rr
Author contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Acknowledgments
Special thanks to Matias Ramos, Lisandro Valente, Ignacio Lugones, Ayelén Barreto, Máximo Salvarezza and Fernando Cucchietti for substantial feedback, review and discussion of ideas. We are also grateful to Luis Segura, Octavio Atun and Oscar Regalado for their invaluable support and technical advice. This article was submitted as a preprint to SSRN as Orofino Giambastiani et al. (2022).
Conflict of interest
Authors declare that they hold patent applications for the proposed system and are the co-founders of “Euclidean: Time Series for Science ™”; a technology development project based on the exposed ideas, and of which this document should be considered its theoretical paper.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1https://en.wikipedia.org/wiki/Sybil_attack [Accessed 12 November 2022].
2https://en.wikipedia.org/wiki/Transponder [Accessed 12 November 2022].
7https://www.proofofhumanity.id/
12https://en.wikipedia.org/wiki/Zero-knowledge_proof [Accessed 12 November 2022].
20https://internetcomputer.org/
22https://www.cloudflare.com/leagueofentropy/
24https://www.unrealengine.com/
References
Afonso, A. M., Cadwell, J. B., Staffa, S. J., Zurakowski, D., and Vinson, A. E. (2021). Burnout rate and risk factors among anesthesiologists in the United States. Anesthesiology 134 (5), 683–696. doi:10.1097/ALN.0000000000003722
Ahmad, R. W., Salah, K., Jayaraman, R., Hasan, H. R., Yaqoob, I., and Omar, M. (2021). The role of blockchain technology in aviation industry. IEEE Aerosp. Electron. Syst. Mag. 36 (3), 4–15. doi:10.1109/MAES.2020.3043152
Al-Breiki, H., Rehman, M. H. U., Salah, K., and Svetinovic, D. (2020). Trustworthy blockchain oracles: Review, comparison, and open research challenges. IEEE Access 8, 85675–85685. doi:10.1109/ACCESS.2020.2992698
Alam, F., and Matava, C. (2022). A new virtual world? The future of immersive environments in anesthesiology. Anesth. Analgesia 135 (2), 230–238. doi:10.1213/ANE.0000000000006118
Alkhatip, A. A. A. M. M., Kamel, M. G., Farag, E. M., Elayashy, M., Farag, A., Yassin, H. M., et al. (2021). Deep hypothermic circulatory arrest in the pediatric population undergoing cardiac surgery with electroencephalography monitoring: A systematic review and meta-analysis. J. Cardiothorac. Vasc. Anesth. 35 (10), 2875–2888. doi:10.1053/j.jvca.2021.01.039
Alkire, M. T., Hudetz, A. G., and Tononi, G. (2008). Consciousness and anesthesia. Science 322 (5903), 876–880. doi:10.1126/science.1149213
Anderson, B. J., and Merry, A. F. (2015). Paperless anesthesia: Uses and abuses of these data’, pediatric anesthesia. A. Davidson 25 (12), 1184–1192. doi:10.1111/pan.12782
Aström, K. J., and Murray, R. M. (2008). Feedback systems: An introduction for scientists and engineers. New Jersey, United States: Princeton University Press. doi:10.1515/9781400828739
Bellini, V., Petroni, A., Palumbo, G., and Bignami, E. (2019). Data quality and blockchain technology. Anaesth. Crit. Care & Pain Med. 38 (5), 521–522. doi:10.1016/j.accpm.2018.12.015
Benet, J. (2014). IPFS - content addressed, versioned, P2P file system. Ithaca: Cornell University. doi:10.48550/ARXIV.1407.3561
Benzekki, K., El Fergougui, A., and Elalaoui, A. E. (2017). “A verifiable secret sharing approach for secure MultiCloud storage,” in Ubiquitous networking. Editor E. Sabir (Cham: Springer International Publishing), 225–234. doi:10.1007/978-3-319-68179-5_20
Blum, M., Feldman, P., and Micali, S. (1988). “Non-interactive zero-knowledge and its applications,” in Proceedings of the twentieth annual ACM symposium on Theory of computing - stoc ’88 (Chicago, Illinois, United States: ACM Press), 103–112. doi:10.1145/62212.62222
Borrelli, C., Bestagini, P., Antonacci, F., Sarti, A., and Tubaro, S. (2021). Synthetic speech detection through short-term and long-term prediction traces. EURASIP J. Inf. Secur. 2021 (1), 2. doi:10.1186/s13635-021-00116-3
Burns, M. L., Saager, L., Cassidy, R. B., Mentz, G., Mashour, G. A., and Kheterpal, S. (2022). Association of anesthesiologist staffing ratio with surgical patient morbidity and mortality. JAMA Surg. 157, 807. doi:10.1001/jamasurg.2022.2804
Buterin, V. (2022d). DAOs are not corporations: Where decentralization in autonomous organizations matters. Vitalik Buterin's website. Available at: https://vitalik.ca/general/2022/09/20/daos.html (Accessed November 12, 2022).
Buterin, V. (2022c). Encapsulated vs systemic complexity in protocol design. Vitalik Buterin's website. Available at: https://vitalik.ca/general/2022/02/28/complexity.html (Accessed November 12, 2022).
Buterin, V. (2014). Ethereum: A next-generation smart contract and decentralized application platform. Available at: https://ethereum.org/669c9e2e2027310b6b3cdce6e1c52962/Ethereum_Whitepaper_-_Buterin_2014.pdf (Accessed November 12, 2022).
Buterin, V. (2019). Hard problems in cryptocurrency: Five years later. Vitalik Buterin's website. Available at: https://vitalik.ca/general/2019/11/22/progress.html (Accessed November 12, 2022).
Buterin, V. (2021). Moving beyond coin voting governance. Vitalik Buterin's website. Available at: https://vitalik.ca/general/2021/08/16/voting3.html (Accessed November 12, 2022).
Buterin, V. (2022b). Some ways to use ZK-SNARKs for privacy. Vitalik Buterin's website. Available at: https://vitalik.ca/general/2022/06/15/using_snarks.html (Accessed November 12, 2022).
Buterin, V. (2017). The meaning of decentralization. Medium. Available at: https://medium.com/@VitalikButerin/the-meaning-of-decentralization-a0c92b76a274 (Accessed November 12, 2022).
Buterin, V. (2022a). Where to use a blockchain in non-financial applications. Vitalik Buterin's website. Available at: https://vitalik.ca/general/2022/06/12/nonfin.html (Accessed November 12, 2022).
Caldarelli, G. (2020). Understanding the blockchain oracle problem: A call for action. Information 11 (11), 509. doi:10.3390/info11110509
Canales, C., Lee, C., and Cannesson, M. (2020). Science without conscience is but the ruin of the soul: The ethics of big data and artificial intelligence in perioperative medicine. Anesth. Analgesia 130 (5), 1234–1243. doi:10.1213/ANE.0000000000004728
Chohan, U. W. (2022). Web 3.0: The future architecture of the Internet? SSRN Electron. J. 2022, 4037693. doi:10.2139/ssrn.4037693
Colquhoun, D. A., Shanks, A. M., Kapeles, S. R., Shah, N., Saager, L., Vaughn, M. T., et al. (2020). Considerations for integration of perioperative electronic health records across institutions for research and quality improvement: The approach taken by the multicenter perioperative outcomes group. Anesth. Analgesia 130 (5), 1133–1146. doi:10.1213/ANE.0000000000004489
Connor, C. W. (2019). Artificial intelligence and machine learning in anesthesiology. Anesthesiology 131 (6), 1346–1359. doi:10.1097/ALN.0000000000002694
Coorevits, P., Sundgren, M., Klein, G. O., Bahr, A., Claerhout, B., Daniel, C., et al. (2013). Electronic health records: New opportunities for clinical research. J. Intern. Med. 274 (6), 547–560. doi:10.1111/joim.12119
De Hert, S. (2021). Human factors affecting intraoperative patient safety. Curr. Opin. Anaesthesiol. 34 (6), 735–743. doi:10.1097/ACO.0000000000001059
Dinkel, H., Chen, N., Qian, Y., and Yu, K. (2017). “End-to-end spoofing detection with raw waveform CLDNNS,” in 2017 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), New Orleans, LA, 05-09 March 2017, 4860–4864. IEEE. doi:10.1109/ICASSP.2017.7953080
Douceur, J. R. (2002). “The Sybil attack,” in Peer-to-Peer systems. Editors P. Druschel, F. Kaashoek, and A. Rowstron (Berlin, Heidelberg: Springer Berlin Heidelberg), 251–260. doi:10.1007/3-540-45748-8_24
Dutton, R. P., and DuKatz, A. (2011). Quality improvement using automated data sources. Anesthesiology Clinics: The Anesthesia Quality Institute’, S1932227511000395. doi:10.1016/j.anclin.2011.05.002
Edwards, D. A., and Lampotang, S. (2020). “Computer- and web-based simulators and virtual environments,” in Comprehensive healthcare simulation: Anesthesiology. Editors B. Mahoney, R. D. Minehart, and M. C. M. Pian-Smith (Cham: Springer International Publishing), 117–125. doi:10.1007/978-3-030-26849-7_12
Edwards, K.-E., Hagen, S. M., Hannam, J., Kruger, C., Yu, R., and Merry, A. F. (2013). A randomized comparison between records made with an anesthesia information management system and by hand, and evaluation of the Hawthorne effect. Can. J. Anesthesia/Journal Can. d’anesthésie 60 (10), 990–997. doi:10.1007/s12630-013-0003-y
Ehrenfeld, J. M., and Rehman, M. A. (2011). Anesthesia information management systems: A review of functionality and installation considerations. J. Clin. Monit. Comput. 25 (1), 71–79. doi:10.1007/s10877-010-9256-y
El-Wajeh, Y. A. M., Hatton, P. V., and Lee, N. J. (2022). Unreal engine 5 and immersive surgical training: Translating advances in gaming technology into extended-reality surgical simulation training programmes. Br. J. Surg. 109 (5), 470–471. doi:10.1093/bjs/znac015
Emmert-Streib, F., Yang, Z., Feng, H., Tripathi, S., and Dehmer, M. (2020). An introductory review of deep learning for prediction models with big data. Front. Artif. Intell. 3, 4. doi:10.3389/frai.2020.00004
Epstein, R. H., and Dexter, F. (2018). Database quality and access issues relevant to research using anesthesia information management system data. Anesth. Analgesia 127 (1), 105–114. doi:10.1213/ANE.0000000000003324
Ezzat, S. K., Saleh, Y. N. M., and Abdel-Hamid, A. A. (2022). Blockchain oracles: State-of-the-Art and research directions. IEEE Access 10, 67551–67572. doi:10.1109/ACCESS.2022.3184726
Feldman, J. M. (2004). Do anesthesia information systems increase malpractice exposure? Results of a survey. Anesth. Analgesia 99 (3), 840–843. doi:10.1213/01.ANE.0000130259.52838.3B
Fernández-Alemán, J. L., Señor, I. C., Lozoya, P. Á. O., and Toval, A. (2013). Security and privacy in electronic health records: A systematic literature review. J. Biomed. Inf. 46 (3), 541–562. doi:10.1016/j.jbi.2012.12.003
Figar Gutiérrez, A., Garbino, J. A. M., Burgos, V., and Rajah, T. (2021). Anesthesia inmutable registry of real-time vital signs and waveforms using blockchain. preprint. Health Informatics. doi:10.1101/2021.12.18.21267876
Freni, P., Ferro, E., and Moncada, R. (2022). Tokenomics and blockchain tokens: A design-oriented morphological framework. Blockchain Res. Appl. 3 (1), 100069. doi:10.1016/j.bcra.2022.100069
Gaba, D. M. (2000). Anaesthesiology as a model for patient safety in health care. BMJ 320 (7237), 785–788. doi:10.1136/bmj.320.7237.785
Goodell, G., and Aste, T. (2019). A decentralized digital identity architecture. Front. Blockchain 2, 17. doi:10.3389/fbloc.2019.00017
Guidi, B., Michienzi, A., and Ricci, L. (2021). “Data persistence in decentralized social applications: The IPFS approach,” in 2021 IEEE 18th Annual Consumer Communications & Networking Conference (CCNC). 2021 IEEE 18th Annual Consumer Communications & Networking Conference (CCNC), Las Vegas, NV, USA, 09-12 January 2021, 1–4. doi:10.1109/CCNC49032.2021.9369473
Hashimoto, D. A., Witkowski, E., Gao, L., Meireles, O., and Rosman, G. (2020). Artificial intelligence in anesthesiology. Anesthesiology 132 (2), 379–394. doi:10.1097/ALN.0000000000002960
Hastings, R. H., and Rickard, T. C. (2015). Deliberate practice for achieving and maintaining expertise in anesthesiology. Anesth. Analgesia 120 (2), 449–459. doi:10.1213/ANE.0000000000000526
Henrik, A., Johannes, R. J., and Ross, O. (2022). When is a DAO Decentralized? Complex Syst. Inf. Model. Q. 31, 51–75. doi:10.7250/csimq.2022-31.04
Higham, H., and Baxendale, B. (2017). To err is human: Use of simulation to enhance training and patient safety in anaesthesia. Br. J. Anaesth. 119, i106–i114. doi:10.1093/bja/aex302
Hinsen, K. (2020). The magic of content-addressable storage. Comput. Sci. Eng. 22 (3), 113–119. doi:10.1109/MCSE.2019.2949441
Hoffman, K., Zage, D., and Nita-Rotaru, C. (2009). A survey of attack and defense techniques for reputation systems. ACM Comput. Surv. 42 (1), 1–31. doi:10.1145/1592451.1592452
Honkanen, P., Nylund, M., and Westerlund, M. (2021). Organizational building blocks for blockchain governance: A survey of 241 blockchain white papers. Front. Blockchain 4, 613115. doi:10.3389/fbloc.2021.613115
Howard, S. K., Gaba, D., Smith, B., Weinger, M., Herndon, C., Keshavacharya, S., et al. (2003). Simulation study of rested versus sleep-deprived anesthesiologists. Anesthesiology 98 (6), 1345–1355. doi:10.1097/00000542-200306000-00008
Jones, P. M., Cherry, R. A., Allen, B. N., Jenkyn, K. M. B., Shariff, S. Z., Flier, S., et al. (2019). Association between handover of anesthesia care and adverse postoperative outcomes among patients undergoing major surgery. JAMA 319 (2), 143. doi:10.1001/jama.2017.20040
Joyce, M. F., Careskey, H. E., Barach, P., and Azocar, R. J. (2017). “The science of delivering safe and reliable anesthesia care,” in Surgical patient care. Editor J. A. Sanchez (Cham: Springer International Publishing), 327–347. doi:10.1007/978-3-319-44010-1_21
Kaaniche, N., Laurent, M., and Levallois-Barth, C. (2020). ID-based user-centric data usage auditing scheme for distributed environments. Front. Blockchain 3, 17. doi:10.3389/fbloc.2020.00017
Kadry, B., Feaster, W. W., Macario, A., and Ehrenfeld, J. M. (2012). Anesthesia information management systems: Past, present, and future of anesthesia records. Mt. Sinai J. Med. A J. Transl. Personalized Med. 79 (1), 154–165. doi:10.1002/msj.21281
Kaplan, H. (2018). “Persistent data structures,” in Handbook of data structures and applications. Second Edition (Chapman and Hall/CRC), 511–528. doi:10.1201/9781315119335
Kayaalp, M. (2018). Patient privacy in the era of big data. Balkan Med. J. 35 (1), 8–17. doi:10.4274/balkanmedj.2017.0966
Klein, M., and Stummer, C. (2021). Feeless micropayments as drivers for new business models: Two exemplary application cases. Front. Blockchain 4, 641508. doi:10.3389/fbloc.2021.641508
Klocke, H., Trispel, S., Rau, G., Hatzky, U., and Daub, D. (1986). An anesthesia information system for monitoring and record keeping during surgical anesthesia. J. Clin. Monit. 2 (4), 246–261. doi:10.1007/BF02851173
Kumar, R., and Tripathi, R. (2020). “Blockchain-based framework for data storage in peer-to-peer scheme using interplanetary file system,” in Handbook of research on blockchain technology (Amsterdam, Netherlands: Elsevier), 35–59. doi:10.1016/B978-0-12-819816-2.00002-2
Ladyman, J., Lambert, J., and Wiesner, K. (2013). What is a complex system? Eur. J. Philosophy Sci. 3 (1), 33–67. doi:10.1007/s13194-012-0056-8
Lalley, S. P., and Weyl, E. G. (2018). Quadratic voting: How mechanism design can radicalize democracy. AEA Pap. Proc. 108, 33–37. doi:10.1257/pandp.20181002
Leible, S., Schlager, S., Schubotz, M., and Gipp, B. (2019). A review on blockchain technology and blockchain projects fostering open science. Front. Blockchain 2, 16. doi:10.3389/fbloc.2019.00016
Liem, V. G. B., Hoeks, S. E., van Lier, F., and de Graaff, J. C. (2018). What we can learn from Big Data about factors influencing perioperative outcome. Curr. Opin. Anaesthesiol. 31 (6), 723–731. doi:10.1097/ACO.0000000000000659
Liu, L., Zhou, S., Huang, H., and Zheng, Z. (2021). From technology to society: An overview of blockchain-based DAO. IEEE Open J. Comput. Soc. 2, 204–215. doi:10.1109/OJCS.2021.3072661
Liu, Y., He, D., Obaidat, M. S., Kumar, N., Khan, M. K., and Raymond Choo, K. K. (2020). Blockchain-based identity management systems: A review. J. Netw. Comput. Appl. 166, 102731. doi:10.1016/j.jnca.2020.102731
Lonsdale, H., Jalali, A., Gálvez, J. A., Ahumada, L. M., and Simpao, A. F. (2020). Artificial intelligence in anesthesiology: Hype, hope, and hurdles. Anesth. Analgesia 130 (5), 1111–1113. doi:10.1213/ANE.0000000000004751
Lopes, V., and Alexandre, L. A. (2019). An overview of blockchain integration with robotics and artificial intelligence. Ledger 2019, 171. doi:10.5195/ledger.2019.171
Lustenberger, M., Malešević, S., and Spychiger, F. (2021). Ecosystem readiness: Blockchain adoption is driven externally. Front. Blockchain 4, 720454. doi:10.3389/fbloc.2021.720454
Mackey, T. K., Shah, N., Miyachi, K., Short, J., and Clauson, K. (2019). A framework proposal for blockchain-based scientific publishing using shared governance. Front. Blockchain 2, 19. doi:10.3389/fbloc.2019.00019
Magrabi, F., Ammenwerth, E., McNair, J. B., De Keizer, N. F., Hyppönen, H., Nykänen, P., et al. (2019). Artificial intelligence in clinical decision support: Challenges for evaluating ai and practical implications: A position paper from the imia technology assessment & quality development in health informatics working group and the efmi working group for assessment of health information systems. Yearb. Med. Inf. 28 (01), 128–134. doi:10.1055/s-0039-1677903
Mashour, G. A. (2022). Consciousness. Anesth. Analgesia 134 (6), 1118–1125. doi:10.1213/ANE.0000000000005983
Mavroudis, C. D., Mensah-Brown, K. G., Ko, T. S., Boorady, T. W., Massey, S. L., Abend, N. S., et al. (2018). Electroencephalographic response to deep hypothermic circulatory arrest in neonatal swine and humans. Ann. Thorac. Surg. 106 (6), 1841–1846. doi:10.1016/j.athoracsur.2018.06.036
McIlvaine, W. B. (2007). Situational awareness in the operating room: A primer for the anesthesiologist. Seminars Anesth. Perioper. Med. Pain 26 (3), 167–172. doi:10.1053/j.sane.2007.06.001
Mohanta, B. K., Panda, S. S., and Jena, D. (2018). “An overview of smart contract and use cases in blockchain technology,” in 2018 9th International Conference on Computing, Communication and Networking Technologies (ICCCNT). 2018 9th International Conference on Computing, Communication and Networking Technologies (ICCCNT), Bengaluru, India, 10-12 July 2018, 1–4. doi:10.1109/ICCCNT.2018.8494045
Munir, M. A., Habib, M. S., Hussain, A., Shahbaz, M. A., Qamar, A., Masood, T., et al. (2022). Blockchain adoption for sustainable supply chain management: Economic, environmental, and social perspectives. Front. Energy Res. 10, 899632. doi:10.3389/fenrg.2022.899632
Nair, B. G., Gabel, E., Hofer, I., Schwid, H. A., and Cannesson, M. (2017). Intraoperative clinical decision support for anesthesia: A narrative review of available systems. Anesth. Analgesia 124 (2), 603–617. doi:10.1213/ANE.0000000000001636
Neuschwander, A., Job, A., Younes, A., Mignon, A., Delgoulet, C., Cabon, P., et al. (2017). Impact of sleep deprivation on anaesthesia residents’ non-technical skills: A pilot simulation-based prospective randomized trial. Br. J. Anaesth. 119 (1), 125–131. doi:10.1093/bja/aex155
Novikov, D. A. (2016). “Studies in systems, decision and control, volume 47,” in Cybernetics: From past to future (Cham: Springer).
Orofino Giambastiani, R. E., Sáenz, R., Lahitte, G., and Umaran, J. (2022). Technology optimization for patient safety: a blockchain-based anesthesia record system architecture. SSRN Electronic Journal [Preprint]. doi:10.2139/ssrn.4275953
Panda, D. K., Lu, X., and Shankar, D. (2022). High-performance big data computing. Cambridge, Massachusetts London: The MIT Press (Scientific and engineering computation.
Pandya, A. N., Majid, S. Z., and Desai, M. S. (2021). The origins, evolution, and spread of anesthesia monitoring standards: From boston to across the world. Anesth. Analgesia 132 (3), 890–898. doi:10.1213/ANE.0000000000005021
Parvinian, B., Scully, C., Wiyor, H., Kumar, A., and Weininger, S. (2018). Regulatory considerations for physiological closed-loop controlled medical devices used for automated critical care: Food and drug administration workshop discussion topics. Anesth. Analgesia 126 (6), 1916–1925. doi:10.1213/ANE.0000000000002329
Paton, C., and Kobayashi, S. (2019). An open science approach to artificial intelligence in healthcare: A contribution from the international medical informatics association open source working group. Yearb. Med. Inf. 28 (01), 047–051. doi:10.1055/s-0039-1677898
Phipps, D., Meakin, G., Beatty, P., Nsoedo, C., and Parker, D. (2008). Human factors in anaesthetic practice: Insights from a task analysis. Br. J. Anaesth. 100 (3), 333–343. doi:10.1093/bja/aem392
Politou, E., Alepis, E., Patsakis, C., Casino, F., and Alazab, M. (2020). Delegated content erasure in IPFS. Future Gener. Comput. Syst. 112, 956–964. doi:10.1016/j.future.2020.06.037
Rahardja, U., Ngadi, M. A., Budiarto, R., Aini, Q., Hardini, M., and Oganda, F. P. (2021). Education exchange storage protocol: Transformation into decentralized learning platform. Front. Educ. 6, 782969. doi:10.3389/feduc.2021.782969
Reich, D. L., Wood, R. K., Mattar, R., Krol, M., Adams, D. C., Hossain, S., et al. (2000). Arterial blood pressure and heart rate discrepancies between handwritten and computerized anesthesia records. Anesth. Analgesia 91, 612–616. doi:10.1097/00000539-200009000-00022
Reijers, W., O’Brolcháin, F., and Haynes, P. (2016). Governance in blockchain technologies & social contract theories. Ledger 1, 134–151. doi:10.5195/ledger.2016.62
Rieke, N., Hancox, J., Li, W., Milletarì, F., Roth, H. R., Albarqouni, S., et al. (2020). The future of digital health with federated learning. npj Digit. Med. 3 (1), 119. doi:10.1038/s41746-020-00323-1
Rozental, O., and White, R. S. (2019). Anesthesia information management systems: Evolution of the paper anesthetic record to a multisystem electronic medical record network that streamlines perioperative care. J. Anesth. Hist. 5 (3), 93–98. doi:10.1016/j.janh.2019.04.001
Saager, L., Hesler, B. D., You, J., Turan, A., Mascha, E. J., Sessler, D. I., et al. (2014). Intraoperative transitions of anesthesia care and postoperative adverse outcomes. Anesthesiology 121 (4), 695–706. doi:10.1097/ALN.0000000000000401
Saeed, H., Malik, H., Bashir, U., Ahmad, A., Riaz, S., Ilyas, M., et al. (2022). Blockchain technology in healthcare: A systematic review. PLOS ONE 17 (4), e0266462. doi:10.1371/journal.pone.0266462
Sarker, I., and Datta, B. (2022). Re-Designing the pension business processes for achieving technology-driven reforms through blockchain adoption: A proposed architecture. Technol. Forecast. Soc. Change 174, 121059. doi:10.1016/j.techfore.2021.121059
Schulz, C. M., Burden, A., Posner, K. L., Mincer, S. L., Steadman, R., Wagner, K. J., et al. (2017). Frequency and type of situational awareness errors contributing to death and brain damage. Anesthesiology 127 (2), 326–337. doi:10.1097/ALN.0000000000001661
Schulz, C. M., Endsley, M., Kochs, E., Gelb, A., and Wagner, K. (2013). Situation awareness in anesthesia. Anesthesiology 118 (3), 729–742. doi:10.1097/ALN.0b013e318280a40f
Schulz, C. M., Krautheim, V., Hackemann, A., Kreuzer, M., Kochs, E. F., and Wagner, K. J. (2015). Situation awareness errors in anesthesia and critical care in 200 cases of a critical incident reporting system. BMC Anesthesiol. 16 (1), 4. doi:10.1186/s12871-016-0172-7
Sessler, D. I. (2014). Big Data - and its contributions to peri-operative medicine. Anaesthesia 69 (2), 100–105. doi:10.1111/anae.12537
Shetty, A., Pai, R. Y., Rao, R. R., Bhandary, R., and Shetty, J., (2022). Block chain application in insurance services: A systematic review of the evidence. SAGE Open 12 (1), 215824402210798. doi:10.1177/21582440221079877
Short, J. E., Miyachi, K., Toouli, C., and Todd, S. (2022). A field test of a federated learning/federated analytic blockchain network implementation in an HPC environment. Front. Blockchain 5, 893747. doi:10.3389/fbloc.2022.893747
Siddarth, D., Ivliev, S., Siri, S., and Berman, P. (2020). Who watches the watchmen? A review of subjective approaches for sybil-resistance in proof of personhood protocols. Front. Blockchain 3, 590171. doi:10.3389/fbloc.2020.590171
Simpao, A. F., and Rehman, M. A. (2020). “Electronic anesthesia records: Anesthesia information management systems,” in Gregory’s pediatric anesthesia. Editors D B Andropoulos, and G A Gregory. 1st edn (New Jersey, United States: Wiley), 1227–1242. doi:10.1002/9781119371533.ch49
Simpao, A., Heitz, J. W., McNulty, S. E., Chekemian, B., Brenn, B. R., and Epstein, R. H. (2011). The design and implementation of an automated system for logging clinical experiences using an anesthesia information management system. Anesth. Analgesia 112 (2), 422–429. doi:10.1213/ANE.0b013e3182042e56
Srinivasan, B. (2022). The network state. Available at: https://thenetworkstate.com/(Accessed November 12, 2022).
Stipčević, M., and Koç, Ç. K. (2014). “True random number generators,” in Open problems in mathematics and computational science. Editor Ç. K. Koç (Cham: Springer International Publishing), 275–315. doi:10.1007/978-3-319-10683-0_12
Strobel, V., Castelló Ferrer, E., and Dorigo, M. (2020). Blockchain technology secures robot swarms: A comparison of consensus protocols and their resilience to byzantine robots. Front. Robotics AI 7, 54. doi:10.3389/frobt.2020.00054
Tasca, P., and Tessone, C. J. (2019). A taxonomy of blockchain technologies: Principles of identification and classification. Ledger 4. doi:10.5195/ledger.2019.140
Thakur, A. (2022). A comprehensive study of the trends and analysis of distributed ledger technology and blockchain technology in the healthcare industry. Front. Blockchain 5, 844834. doi:10.3389/fbloc.2022.844834
Toff, N. J. (2010). Human factors in anaesthesia: Lessons from aviation. Br. J. Anaesth. 105 (1), 21–25. doi:10.1093/bja/aeq127
Tse, M.-K., Li, S. Y. W., Chiu, T. H., Lau, C. W., Lam, K. M., and Cheng, C. P. B. (2020). Comparison of the effects of automated and manual record keeping on anesthetists’ monitoring performance: Randomized controlled simulation study. JMIR Hum. Factors 7 (2), e16036. doi:10.2196/16036
Valentine, E. A., and Falk, S. A. (2018). Quality improvement in anesthesiology — leveraging data and analytics to optimize outcomes. Anesthesiol. Clin. 36 (1), 31–44. doi:10.1016/j.anclin.2017.10.006
van Schalkwyk, J. M., Lowes, D., Frampton, C., and Merry, A. (2011). Does manual anaesthetic record capture remove clinically important data? Br. J. Anaesth. 107 (4), 546–552. doi:10.1093/bja/aer163
Vigoda, M. M., and Lubarsky, D. A. (2006). The medicolegal importance of enhancing timeliness of documentation when using an anesthesia information system and the response to automated feedback in an academic practice. Anesth. Analgesia 103 (1), 131–136. doi:10.1213/01.ane.0000221602.90315.49
Warner, M. A., Arnal, D., Cole, D. J., Hammoud, R., Haylock-Loor, C., Ibarra, P., et al. (2022). Anesthesia patient safety: Next steps to improve worldwide perioperative safety by 2030. Anesth. Analgesia 135 (1), 6–19. doi:10.1213/ANE.0000000000006028
Weininger, S., Jaffe, M. B., and Goldman, J. M. (2017). The need to apply medical device informatics in developing standards for safe interoperable medical systems. Anesth. Analgesia 124 (1), 127–135. doi:10.1213/ANE.0000000000001386
West, C. P., Dyrbye, L. N., and Shanafelt, T. D. (2018). Physician burnout: Contributors, consequences and solutions. J. Intern. Med. 283 (6), 516–529. doi:10.1111/joim.12752
Weyl, E. G., Ohlhaver, P., and Buterin, V. (2022). Decentralized society: Finding Web3’s soul. SSRN Electron. J. 2022, 4105763. doi:10.2139/ssrn.4105763
Wong, L. R., Flynn-Evans, E., and Ruskin, K. J. (2018). Fatigue risk management: The impact of anesthesiology residents’ work schedules on job performance and a review of potential countermeasures. Anesth. Analgesia 126 (4), 1340–1348. doi:10.1213/ANE.0000000000002548
Xiong, H., Dalhaus, T., Wang, P., and Huang, J. (2020). Blockchain technology for agriculture: Applications and rationale. Front. Blockchain 3, 7. doi:10.3389/fbloc.2020.00007
Zaouter, C., Joosten, A., Rinehart, J., Struys, M. M. R. F., and Hemmerling, T. M. (2020). Autonomous systems in anesthesia: Where do we stand in 2020? A narrative review. Anesth. Analgesia 130 (5), 1120–1132. doi:10.1213/ANE.0000000000004646
Ziolkowski, R., Miscione, G., and Schwabe, G. (2020). “Exploring decentralized autonomous organizations: Towards shared interests and “code is constitution”,” in Forty-First International Conference on Information Systems (ICIS). doi:10.5167/UZH-193663
Zwitter, A., and Hazenberg, J. (2020). Decentralized network governance: Blockchain technology and the future of regulation. Front. Blockchain 3, 12. doi:10.3389/fbloc.2020.00012
Keywords: anesthesia record, blockchain technology, machine learning, patient safety, decentralized storage, control systems, soulbond tokens
Citation: Orofino Giambastiani R, Sáenz R, Lahitte G and Umaran J (2023) Technology optimization for patient safety: a blockchain-based anesthesia record system architecture. Front. Blockchain 6:1116124. doi: 10.3389/fbloc.2023.1116124
Received: 05 December 2022; Accepted: 19 June 2023;
Published: 13 July 2023.
Edited by:
Zulfiqar Ali, Sher-I-Kashmir Institute of Medical Sciences, IndiaReviewed by:
Alexander Vladimirovich Bogdanov, Saint Petersburg State University, RussiaEdouard Lansiaux, Université de Lille, France
Copyright © 2023 Orofino Giambastiani, Sáenz, Lahitte and Umaran. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Roberto Orofino Giambastiani, cm9iZXJ0by5vcm9maW5vQGFuZXN0aC50ZWNo