 Hessah A. Alsalamah1,2*
Hessah A. Alsalamah1,2* Ghada Alsuwailem1
Ghada Alsuwailem1 Fatima Bin Rajeh1Samar Alharbi1Salmah AlQahtani1Razan AlArifi1Shaden AlShargi1Sara A. Alsalamah3
Fatima Bin Rajeh1Samar Alharbi1Salmah AlQahtani1Razan AlArifi1Shaden AlShargi1Sara A. Alsalamah3 Shada Alsalamah1,4,5
Shada Alsalamah1,4,5- 1Information Systems Department, College of Computer and Information Sciences, King Saud University, Riyadh, Saudi Arabia
- 2Computer Engineering Department, College of Engineering and Architecture, Al Yamamah University, Riyadh, Saudi Arabia
- 3College of Computer and Information Sciences, Imam Muhammad Ibn Saud Islamic University, Riyadh, Saudi Arabia
- 4Digital Health and Innovation, Science Division, World Health Organization, Geneva, Switzerland
- 5National Health Information Center, Saudi Health Council, Riyadh, Saudi Arabia
The pandemic has triggered an unprecedented global demand for home caregiving to manage asymptomatic and mild COVID-19 cases. Older people and others with pre-existing medical conditions (including diabetes) appear to be more vulnerable to severe illness caused by the severe acute respiratory syndrome coronavirus 2. Approximately 25% of Saudis suffer from diabetes; these 4 million patients require 5.5 million consultations and follow-up visits each year to manage their disease. Furthermore, with the increasing number of patients with diabetes and their need for professional care, it is difficult and time consuming to share patient-care information among caregivers in a traditional way; this increases the financial and psychological burden of home caregivers. Although the pandemic has also triggered a global demand for digital health technology adoption worldwide to achieve higher standards of health, recent developments in advanced technologies and mobile health (mHealth) applications have failed to equip the caregivers with the right ecosystem for patient-centered information sharing to allow for informed care decisions. Therefore, there is a gap in the literature as the current solutions fall short of facilitating an effective communication channel among caregivers and between them and their patients, supporting diverse caregiving groups with multiple languages, distributing tasks between caregivers to alleviate the burden on one caregiver, providing a treatment plan by a specialized care team to be viewed and followed by caregivers and patients, and alerting everyone in case of an emergency. Based on the need for empowering home caregivers to cope with the pressure, we propose eHomeCaregiving, an mHealth solution that can build a transparent blockchain-based patient-centered family caregiving ecosystem. eHomeCaregiving facilitates care continuity in patients with type 2 diabetes in Saudi Arabia by integrating care, saving time and efforts of all caregivers, and improving the patient’s quality of life and outcomes, particularly in terms of facing emerging challenges amid the pandemic.
Introduction
According to the WHO, the COVID-19 pandemic has triggered an unprecedented global demand for home caregiving to manage the 80% of COVID-19 cases with minimal flu-like symptoms (International Diabetes Federation, 2020) and for digital health technology adoption to achieve higher standards of health (World Health Organization, 2020a). Furthermore, according to the International Diabetes Federation (IDF), older people and others with chronic diseases, including diabetes, appear to be more vulnerable to severe illness caused by the severe acute respiratory syndrome coronavirus (International Diabetes Federation, 2020). When patients with diabetes develop a viral infection, it can be difficult to treat because of fluctuations in their blood glucose levels and the possible presence of diabetes complications (International Diabetes Federation, 2020). Moreover, COVID-19 patients who are asymptomatic or those with mild or moderate disease could be suitable for home isolation and care without any need for emergency interventions or hospitalization (World Health Organization, 2020b). This requires home caregiving and increases the number of unpaid family caregivers.
A caregiver, whether unpaid or paid, is a member of the person’s social network that helps patients with their daily life activities (Hunt, 2003). Caregiving is commonly used to address impairments related to aging and disabilities, diseases, conditions, injuries, or mental disorders. Supporting caregivers is an important issue that has been neglected worldwide whereas the demand for caregiving has been increasing. According to recently published data, 25% of the global population will be over 65 years old in the next 5–7 years (United Nations Population Fund, 2020). Furthermore, there are no hospitals or nursing homes that can accommodate this large and growing number of patients. There are many communication-related difficulties between caregivers and between caregivers and the care team regarding the accurate timestamped order in which to share informed decisions regarding the patients. Thus, it is necessary to improve the issues caregivers are facing. Moreover, the care team faces many difficulties in managing and controlling a large number of patients. The patients also face many difficulties, such as waiting times, and the need to see more than one doctor on the same day to receive full treatment. Furthermore, if they have disabilities, this process may be stressful for them.
This paper is focused on patients with type 2 diabetes, which occurs in patients over 40 years of age, and according to the consulting family physician we interviewed, it is the most prevalent type of diabetes in Saudi Arabia. This category was selected because of the increasing number of patients with diabetes in Saudi Arabia. According to previously published data, 25% of Saudis suffer from diabetes; therefore, 4 million patients with diabetes require 5.5 million consultations and follow-up visits a year (International Medical Travel Journal, 2018). In addition, based on the interviews we conducted with a patient with diabetes and his caregiver it is clear that there is a lack of Arabic platforms that facilitate the connectedness between caregivers and their patients with diabetes. Therefore, this article introduces a novel approach to build a patient-centered family caregiving ecosystem, which collects all patient-centered information within a single blockchain-based mobile healthcare (mHealth) application, named eHomeCaregiving, to help doctors, nurses, patients, and inexperienced caregivers to easily communicate with more experienced caregivers. This is intended to provide each member of the team the necessary support, whether emotional, physical, or medical, to track the patient’s care for continuity. In this article, we present the special home care requirements of a patient with diabetes and COVID-19, the problem definition, the proposed blockchain-based solution, the design and implementation of the solution, and user perspectives.
Diabetes and COVID-19
Diabetes is one of the fastest-growing health problems in the world which is now reaching epidemic proportions in some countries. It is primarily a consequence of lifestyle behaviors, such as lack of exercise, unhealthy diet, and obesity. Over the past 4 decades, major socioeconomic changes have occurred in Saudi Arabia. Growth and prosperity have led to pronounced changes in the lifestyles of people. In particular, eating habits have become less healthy, and the level of physical activity has declined. Globally, in 2013, it was estimated that almost 382 million people suffered from diabetes, with a prevalence of 8.3%. The top ten countries with the highest prevalence of diabetes were Tokelau (37.5%), Federated States of Micronesia (35%), Marshall Islands (34.9%), Kiribati (28.8%), Cook Islands (25.7%), Vanuatu (24%), Saudi Arabia (23.9%), Nauru (23.3%), Kuwait (23.1%), and Qatar (22.9%). Therefore, Saudi Arabia is among the top ten countries in the world with the highest prevalence (Florenica et al., 2013). In Saudi Arabia, the national healthcare burden resulting from diabetes is likely to exceed $0.87 billion, but this figure does not consider the indirect costs associated with diabetes, such as absenteeism, loss of productivity from disease-related complications, unemployment due to disability, and premature mortality (Alhowaish, 2013). Furthermore, the social costs, such as pain and suffering, and the cost of care provided by caregivers as well as healthcare system administrative costs, cost of medications, clinician training programs, and research and infrastructure development were omitted from this research study. Further studies are needed to confirm the present findings and to improve our understanding of the economic costs of diabetes and its related complications (Alhowaish, 2013). Diabetes should be treated in a close collaboration between patients and healthcare providers to prevent long-term complications, such as damage to the eyes, kidneys, feet, and heart, and early death. Aggressive promotion of public awareness, continued screening, and early intervention are pivotal in boosting a positive response. Special attention should also be given to the role of diabetes awareness programs, community-based screening campaigns, and different health educational programs in reducing health problems caused by diabetes, which in the long run help reduce the national burden of this disease (Al-Hazzaa et al., 2011).
Patients with diabetes are more vulnerable to severe illness when infected by the severe acute respiratory syndrome coronavirus 2 (International Diabetes Federation, 2020). According to IDF, the viral infection can be difficult to treat because of fluctuations in blood glucose levels and, possibly, the presence of diabetes complications (International Diabetes Federation, 2020). Therefore, the IDF published special guidance for patients with diabetes who were infected with the virus (Figure 1) (International Diabetes Federation, 2020). The guidance in Figure 1 requires caregivers to manage the patient’s food supply and water intake (diet), to ensure sufficient medication supply, and to monitor glucose levels. This should be performed by the patients, especially during the self-quarantine period, or by a family member if the patient is not able to. Furthermore, caregivers (including the patient and their family) need to be equipped with tools that can help them manage and share vital information with each other in a trusted ecosystem to better manage the case while applying physical distancing measures.
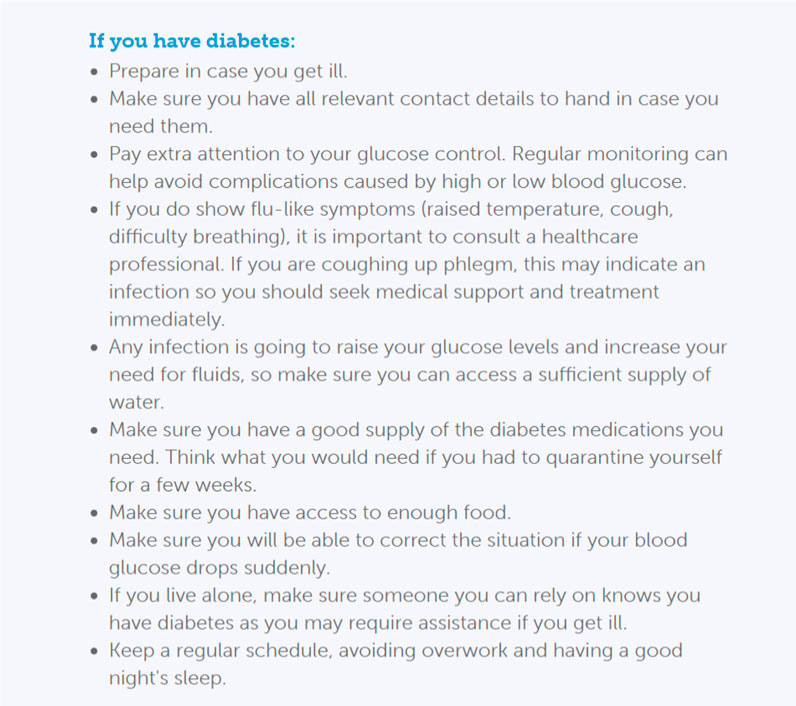
FIGURE 1. IDF instructions for COVID-19 and diabetes (International Diabetes Federation, 2020).
All aspects mentioned in the IDF instructions should be considered when managing or caring for a patient with diabetes and COVID-19. This defines the scope of the patient-centered family caregiving ecosystem introduced here. These include diet, training, treatment, and sugar-level monitoring, as illustrated in Figure 2. Each aspect is managed by a specialist that collaborates with the team for the implementation of patient-centric home caregiving. We present the scope of diabetes care in Figure 2.
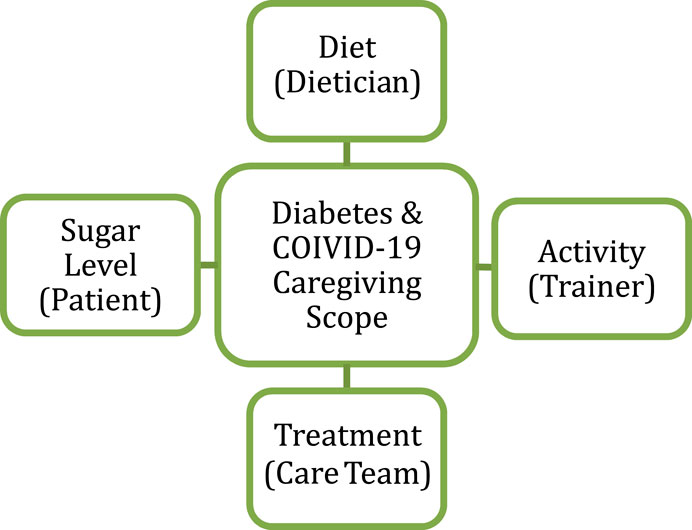
FIGURE 2. Diabetes and COVID-19 caregiving scope.
The caregiving needs of a patient with diabetes might vary depending on their medical condition, age, and ability. Some patients require home care, which provides the patient with appropriate and complete care. Meanwhile, other patients may need a licensed professional caregiver to attend to the their care needs.
We can define caregiving support applications as mHealth and pHealth. “mHealth is a general term for the use of mobile phones and other wireless technology in medical care; mHealth is the most common application to educate the users about several services in health care; mHealth is also used for disease surveillance, treatment support, epidemic outbreak tracking, and chronic disease management” (Rouse, 2018). Meanwhile, “pHealth increasingly combines medical services with public health and epidemiological monitoring, prevention, social and elderly care, in addition to the feeding and wellness to build full care and protection” (pHealth, 2017).
Problem Definition
A study on the use of primary healthcare services and satisfaction by elderly people in Asir, Saudi Arabia, reported that the three leading causes of dissatisfaction were poor transportation to healthcare and communication (65.1%), long time spent in the center (46.4%), and insufficient number of specialty clinics (42.5%) (Kronfol, 2012). This study demonstrated the challenges and burdens that elderly people, most of them diagnosed with diabetes or other chronic illnesses, face when receiving care. As mentioned earlier, 4 million patients with diabetes in Saudi Arabia require 5.5 million consultations and follow-up visits each year. A large number of these visits are not important, but patients go because of the absence of caregiving staff or insufficient home caregiving (International Medical Travel Journal, 2018). During the patient’s visits, the communication language between the care team and their patients while providing or updating the treatment plan and explaining this to the patient can be a barrier. Diabetes is the most prevalent disease in Saudi Arabia; 25% of Saudis have diabetes (International Medical Travel Journal, 2018). Furthermore, when it comes to home caregiving, patients and their caregivers face a number of key challenges. For example, there are challenges related to communicating informed, shared decisions between caregivers when a family member needs special care at home and the family provides care to the patient by sharing the caregiving time between the family members, hiring a nurse, or asking neighbors or friends to check the patient’s status. This is mainly determined by the type of caregiving the patient needs. Patients with diabetes are also challenged in their ability to communicate important information with their caregivers and to remember to track changes in their blood sugar measurements. Caregivers for such patients are challenged in balancing between providing their care and allowing them to live their regular lives. Most caregivers are left with no option but to leave their jobs to provide effective caring services for their loved ones, which adds many financial barriers and an increasing burden of responsibilities. This negatively impacts their financial status, possibly leading to depression and mental health problems.
Therefore, caregivers need to be equipped with tools that can help them share vital information with each other in a trusted ecosystem to successfully facilitate informed care decisions. This can only be achieved if caregivers can track important changes, such as blood sugar measurements, treatment updates, and patient status. Moreover, they should be aware of who entered specific information and make correct care decisions depending on the provided data. Such challenges have not been fully addressed by current related applications in the literature (Kronfol, 2012).
eHomeCaregiving: A Blockchain-Based Solution
The proposed eHomeCaregiving solution is a patient-centered mHealth designed for family caregiving, which aims to address caregivers’ burnout manifesting in isolation and unpreparedness using a blockchain-based technology solution. eHomeCaregiving empowers caregivers by allowing them to track and record their patients’ care management changes, health status, and psychological status on a continuous basis. Caregivers have access to the treatment plan for diabetes that is decided by the care team. The treatment plan may include associated disease treatments for the patient. It also provides information regarding the availability of authorized persons as well as management of the nurses’ and families’ time. The most important benefit is that it offers an opportunity to continuously care for the patient by connecting related caregivers to build an ecosystem using blockchain technology. By using this application, the financial issues and efforts of one caregiver are reduced by connecting the caregivers around the patient. In this study, we utilized blockchain technology to provide good support. Blockchain technology is a digital ledger that allows caregivers to securely connect with each other without the need for third-party intermediaries (Crawford, 2017). Furthermore, blockchain technology creates an immutable, timestamped, and trusted chain of components (changes in care continuity) that are distributed in a ledger among the network of caregivers, and each caregiver receives the same ledger (Crawford, 2017). There are four classes of accessibility and visibility in blockchains (Al-Megren et al., 2018; Alsalamah and Nuzzolese, 2020) (illustrated in Figure 3): the permissionless private class provides access so that only specific people can visit; the permissionless public class is accessible and visible to everyone; the permission private class is such that a specific person can access and visit; and finally, the permission public class is visible to anyone but only specified people can access.
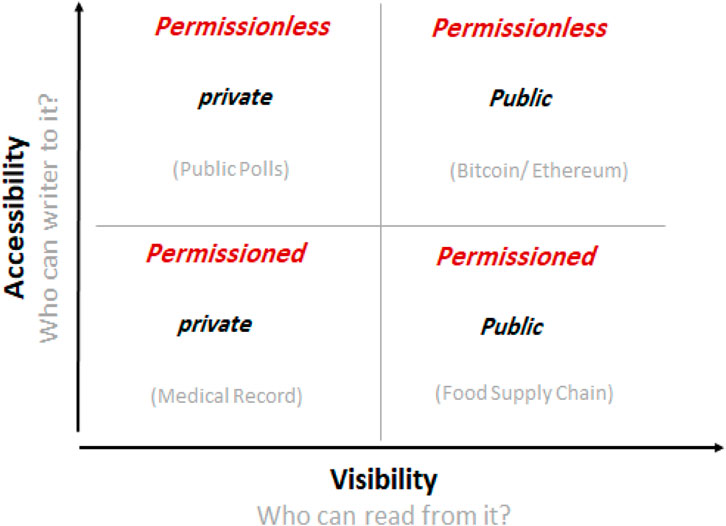
FIGURE 3. Blockchain systems accessibility and visibility matrix (Alsalamah and Nuzzolese, 2020).
Private permission is suitable for this study so that a specific care team can write and read, and only caregivers that the patient knows can access and view the patient’s information. We also chose the Ethereum blockchain platform because Ethereum is an open source that supports blockchain’s advanced versions for general applications beyond cryptocurrency and financial services (Swan, 2015). Regarding the eHomeCaregiving blockchain consensus mechanism type, we apply the proof of identity consensus mechanism because eHomeCaregiving ecosystem requires a role-based access control. The proof of identity is a piece of cryptographic evidence for a user’s private key that is cryptographically attached to a specific transaction. Any identified user (based on their role) from a blockchain network can create a block of data that can be presented to anyone in the network; this is the best fit for private permission classes based on roles. The proof of identity ensures the integrity and authenticity of the data. This consensus mechanism allows eHomeCaregiving to compare the private keys of registered caregivers with an authorized identity.
eHomeCaregiving builds a privately permissioned blockchain solution to address connectivity and patient homecare continuity issues. This is achieved by designing a blockchain-based social network for a patient-centered family caregivers’ support system that can connect the patient's families, friends, and neighbors to build an ecosystem of stakeholders to make shared, informed care decisions. Connected caregivers can exchange information about a patient, such as patient’s treatment, changes in vital sign readings, and time of sleep, to ensure care continuity; they can also confirm administering treatments at specified times. In addition, the caregivers and the patient can add comments that increase the power of interaction and contact between the members of this system. Therefore, the blockchain ledger is shared among all caregivers in this distributed network, and they will know who made the changes or added patient-care information. Blockchain allows multiple participants who need to view common information. It also enables the recording and verification of multiple participants’ actions, so that other participants can trust the validity of the recorded actions. Thus, blockchain has a strong potential to provide a solution (Crawford, 2017). Because these conditions meet the problem requirements, a blockchain is proposed for the platform of the mHealth solution. Through these solutions, we propose a system to track and share patient-centered caregiving transactions in a distributed and immutable caregiving ledger and to connect the caregivers for fast communication and collaboration to make patient-centered care decisions, reduce the errors or inaccurate or incorrect care decisions, track the originator of specific shared information, and provide multiple caregivers access to patients’ needs in order to provide effective care.
eHomeCaregiving mHealth solution targets patients with diabetes and their caregivers. It facilitates care continuity by following up on the patient’s physical, psychological, and nutritional status. Furthermore, eHomeCaregiving solution is suitable for the needs of patients with diabetes. This solution supports home caregivers by enabling them to stay in constant contact and meet their patients’ needs and addresses the need of caregivers to access available information about the patients condition. By using the eHomeCaregiving application, users can record specific information about the patient, especially those related to the measurement of blood sugar. With the adoption of this solution, home caregivers will always be informed regarding their patient’s status, and the application will facilitate making informed care decisions for care continuity. Users will be able to use this application in two languages: the Arabic language because it is the native language, and the English language because it is the second language for Saudi communities.
eHomeCaregiving aims to address key challenges home caregivers face to support their loved ones and focuses particularly on helping patients with diabetes and their caregivers. The increasing number of patients with diabetes has motivated the development of this application to serve or help them. First, this will help Saudi Arabia, which is faced with an increasing number of patients with diabetes and increased pressure on hospitals and skilled nurses. The application will further help by reducing waiting times and the number of patients, as there are no hospitals or nursing facilities that can accommodate their large and growing numbers. In addition, eHomeCaregiving is newly introduced, and according to the interviewed consulting family physician, it should help many in the medical field.
Second, the development of this application will help caregivers manage and control the caregiving process and share informed decisions. Moreover, it will help eliminate difficulties related to acquiring accurate information, such as when the doctor needs to know the results of a blood test to decide on an appropriate treatment plan. Therefore, eHomeCaregiving facilitates communication between caregivers to share changes in caregiving and distributes the efforts between caregivers.
Third, the patients themselves face many difficulties, for example, according to the interviews, patients have a difficulty in remembering treatment times and coordinating between medicines and meal times to take the medication on time. Furthermore, according to the interviews, caregivers explain that, the patient may require continuous follow-up with a diet that is appropriate to their health status, and the patient must visit the doctor every three months and undergo medical examinations, such as the dilated eye exam, blood pressure measurement, and kidney function test. Therefore, eHomeCaregiving helps patients with diabetes to address the need for observation and care continuity, reducing the patient waiting time at their doctors’ clinics for routine care management. Finally, there is a lack of solutions in the literature that function in both Arabic and English to support diverse groups of caregivers who speak either language while caring for patients with diabetes. Therefore, eHomeCaregiving supports caregivers who speak both languages by providing them with features in both languages.
Although there are some applications available to support home caregivers, the applications reviewed do not meet caregiving requirements for patients with diabetes in Saudi Arabia. First, some of the available applications are designed to manage specific vital signs or medical problems. An example is the Thermo (Thermo, 2021) application, which synchronizes temperature readings from a thermometer via Wi-Fi or Bluetooth for health care of the whole family. Another example is Sukkari (Sukkari, 2021) which is specifically designed for patients with diabetes. It records blood sugar levels, meals, and sports activities and shares this information with a medical doctor to monitor the patients remotely. Although these applications are suitable for archiving historical medical information, they do not provide sufficient support in home care. Second, other more general applications, such as Medisafe (2021), Fitbit (2021), and Saleem (2021) help patients manage their medications, vital signs, and clinical visits. Medisafe tracks health measurements for diabetes, hypertension, and various medical conditions. Medisafe also shares reports with doctors and allows inviting a person as a friend. Similarly, Fitbit is a wearable device that measures data, such as the number of steps walked, heart rate, quality of sleep, steps climbed, and others. Moreover, it facilitates following a dietitian plan and calorie estimator using a barcode scanner. Saleem enables the measurement of blood sugar and blood pressure by determining the time and date, and all previous records can be viewed. It is primarily designed to connect patients with their medical doctor who can use it at their clinic to monitor vital signs remotely without the patient having to visit the clinic. This reduces the waiting time and optimizes hospital resources. However, none of the three solutions provide support to caregivers. The solutions do not allow the addition or connection of home caregivers. Finally, there are specific solutions for caregiving, such as Carely (2021) and Caring (2021). Carely is a social caregiving application that brings families together around the care of their loved ones. It connects caregivers to improve their caregiving experiences by coordinating care, planning visits, and sharing memories. However, it is a solution focused on social aspects that does not include medical-related features, such as measuring blood sugar or sending an alarm. Moreover, it is available only in the English language. In contrast, Caring is designed to add a person as a caregiver. It allows the addition of notes, sending reminders, and documenting important decisions made by caregivers. This supports caregivers in connecting and maintaining a medication list and medical history. However, it does not support diabetes-specific features (illustrated in Figure 1). For instance, when care is provided to the patient, the doctor must establish treatment plans for the patient, while caregivers must confirm that the patient is following this treatment plan. According to a conducted survey, the need for the measurement of blood sugar for the patient is the most important function. eHomeCaregiving bridges the gap and meets the above needs for patient-centered caregiving. The aim of this solution is to help caregivers by building an ecosystem that coordinates tasks between all caregivers through an mHealth solution, rather than keeping the pressure on one caregiver. Furthermore, the patient is as involved as the caregivers to increase their satisfaction and improve health outcomes.
Methodology
Using a mixture of qualitative research methods, we first identified the requirements of diabetic eHome caregiving in modern healthcare. Second, we studied the implementation of patient-centered home caregiving care. Then, we designed a blockchain that would address these challenges and equip those systems to fully support eHomeCaregiving care. Finally, we validated the proposal by testing user acceptance.
Information Gathering
To identify the requirements and study the current process and needs, we conducted a number of interviews and gathered information using a survey.
Interviews
First, we conducted an interview with a consulting family physician at medical services directorate and medical administration of the Ministry of Defense (Alsalamah et al., 2019). During the interview, the physician described diabetes in general and the differences between the three types of diabetes. He then explained that type 1 diabetes is often developed in childhood and is caused by different factors, such as hereditary and endocrine diseases; type 2 diabetes is the most prevalent type and is usually developed after the age of 40 years; and type 3 diabetes is related to pregnancy. In addition, the consulting family physician and the care team in general face many difficulties in tracking blood glucose tests of patients, since most of the patients have more than one caregiver and there may be a lack of communication among them. This may cause difficulties when the doctor needs to know the results of the latest blood test in a timely manner to determine an appropriate treatment plan. Furthermore, the consulting family physician identified the information the doctors need to check before deciding on a treatment plan: an overall assessment of the patient, such as job, residence, sports engaged in, name, weight, and height. Moreover, they need to keep track of medical records for the patient as well as the history related to the patient’s family and allergies, and their social and medical history. The consulting family physician also discussed the emergencies that require immediate medical intervention for patients with diabetes, and these are centered around two important aspects: the patient’s blood sugar drops, causing unconsciousness, or the blood sugar rises, which causes the patient to be very stressed and may cause problems with vision. In addition, the consulting family physician stated that the treatment plan may change frequently, depending on the changes in the current medical conditions of the patient, in the patient’s diet, injections, medicines, and sports activities. Finally, he concluded that the idea of this project is new in our society and will significantly help in the medical field. Moreover, he suggested investigating the communication between care team members and between the patient and the care team in the future.
The second interview was with a patient and his caregiver who is also his wife. The aim of the interview was to clarify some points raised while analyzing the requirements. In the first interview, the patient was asked if he had difficulty in remembering treatment times, and from his answer, we discovered that one of the problems facing patients with diabetes was related to taking their medications on time and coordinating between medicines and food. Moreover, the caregiver said that the patient required continuous follow-up with a diet suitable for his health status. Further, the patient must visit the doctor every three months and undergo medical examinations, such as the dilated eye exam, blood pressure measurement, and kidney function test. In addition, the caregiver mentioned the need for observation of patients with diabetes and their care continuity. This includes measuring blood sugar, recording type of food, and providing psychological comfort. This interview enabled us to learn about the needs of patients and caregivers, such as recording changes, confirming treatments, and maintaining contact with the care team.
Questionnaire
To gather more information reflecting the opinions of a large number of caregivers and patients about the proposed solution and to draw some statistical conclusions, a questionnaire was administered. The questionnaires were of two categories: patient and caregiver. The question types included multiple choice, linear scale, true–false, and open-ended questions. The patient questionnaire comprised 15 questions; the first six questions aimed to obtain an overview of the patient and their caregiver. The total number of responses was 68. One of the important questions asked the patients about the type of diabetes (type 1 or 2), and 60.3% of the answers was type 2, whereas 38.2% were type 1. Primarily because of this result, it was decided that the eHomeCaregiving project will target type 2 diabetes.
Another question was a “yes/no” question regarding whether the patients wanted to have a daily blood glucose measurement recorder; 70.1% of the respondents agreed, and 28.4% disagreed (Figure 4). This indicates that there is a need for a recorder with a flowing result.
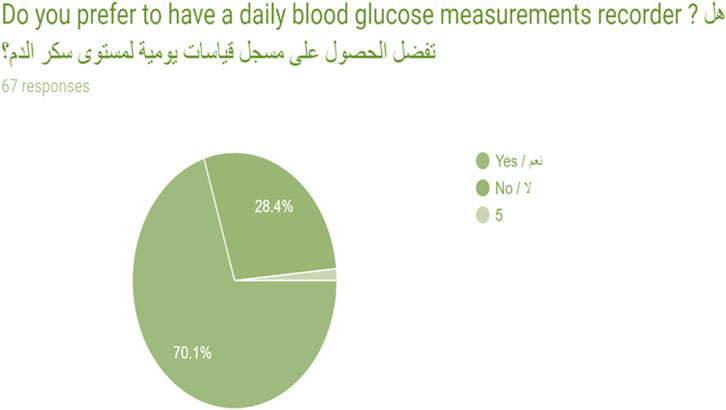
FIGURE 4. Patient’s questionnaire results.
The questionnaire for caregivers consisted of 15 questions. A Likert-type scale question about whether combining all caregivers in one system would save time and effort for communication was included, and the results were that 44.3% of the participants strongly agreed, 17.5% neither agreed nor disagreed, and 9.3% strongly disagreed (Figure 5). These answers validated the need to address the main goals of this project.
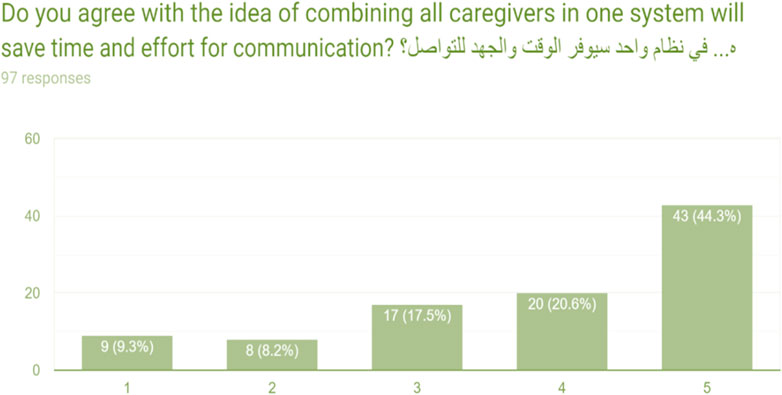
FIGURE 5. Caregiver’s questionnaire results.
One of the open questions asked about the beginning of the experience in caregiving, and one of the answers was: “The continuity of patient care is very hard because of the job environment,” and this indicated the need for help to live a normal life while ensuring the provision of the required care. Another open question was related to whether they had ever experienced an emergency in which they needed immediate assistance and to describe that experience. There was an important answer that shows it is a difficult experience for the person because, owing to shock and lack of knowledge of first aid instructions, they are not able to do anything. This highlights the need for an alarm system, instructions, and guidance when an emergency occurs. The authors elaborated on the data collection in (Alsalamah et al., 2019), which this paper builds on while focusing on design and implementation.
eHomeCaregiving: A Proof-of Concept Prototype
In developing the proof of concept, the waterfall development methodology (Synopsys Editorial Team, 2017) was used. Waterfall features one-direction progress flow with no iteration, which is appropriate for the development of this system. The linear nature of the waterfall method makes the project easier to understand and manage. eHomeCaregiving has three actors: a care team, caregiver, and patient. These users have been utilized for data gathering and system testing. The care team includes medical doctors/healthcare practitioners, who specialize in managing patients with diabetes and also use medical technology. The doctor could be a primary care or family doctor or an internist. Furthermore, an ophthalmologist should check the retina annually and when complications occur, and the patient may need kidney and gangrene doctors. Other specialists, such as those creating a dietitian plan at the beginning of the disease, are also involved. Furthermore, there is a diabetes or health educator who monitors the status of the patient at frequent intervals, measuring the glucose and giving instructions and advice when the results are not optimal. The nurse should be aware of the conditions of the patient throughout the program, and so should the paramedic who takes care of these patients in an emergency.
The caregiver creates an account and logs in. The patient is asked about the disease, registers, and logs into the system. The registration adds the caregiver to the system and creates information about them. The patient can send an alert so that caregivers can see an emergency status. The registered care team determines a specific treatment plan for a specific disease for each patient and then records it on the patient’s timeline. Caregivers, who include family, friends, or neighbors, are included in taking care of their patients. The caregiver views the timeline and its changes, makes changes, and adds comments. Furthermore, a caregiver can send an alarm in emergency situations, give the patient medication, and record it. Some of the key activity diagrams are illustrated in Figure 6 (Alsalamah et al., 2019). Table 1 summarizes eHomeCaregiving key functional requirements for the main stakeholders.
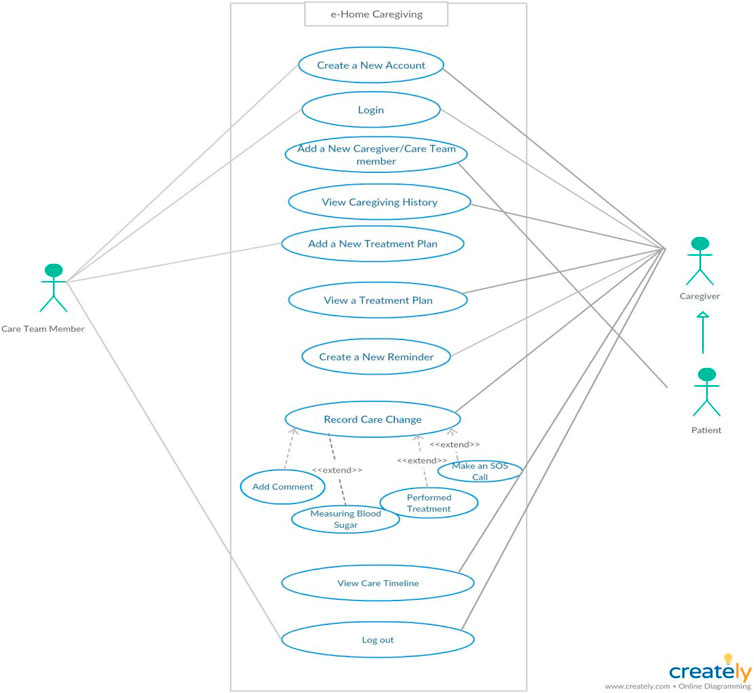
FIGURE 6. eHomeCaregiving use case.
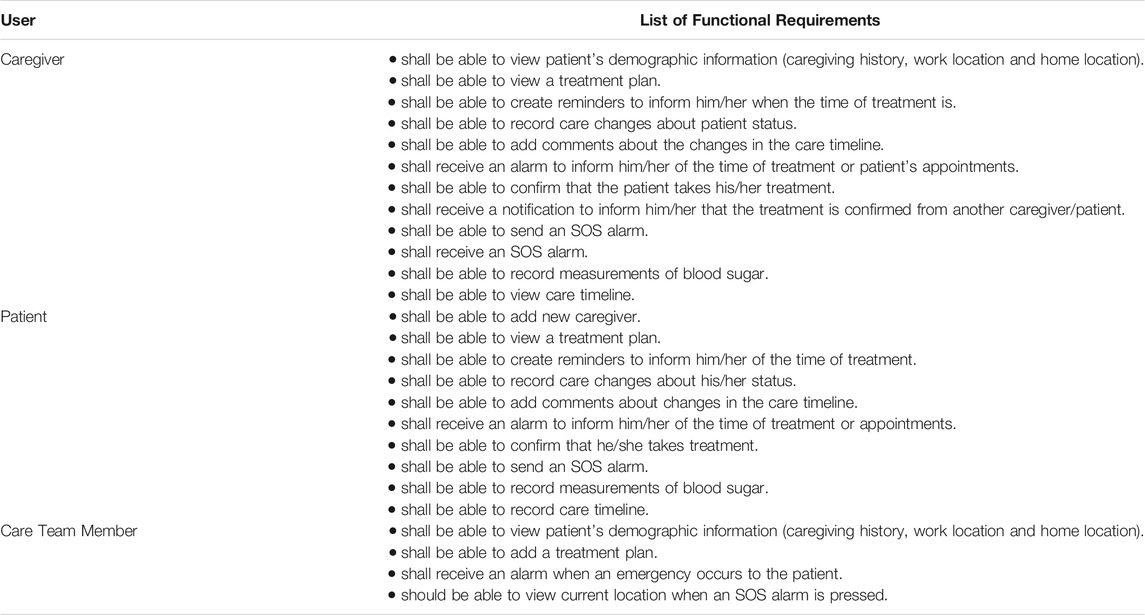
TABLE 1. eHomeCaregiving Functional Requirements
eHomeCaregiving Architecture Design
The eHomeCaregiving architecture is illustrated in Figure 7. Using a layered architecture pattern provides a high level of security and enhances the scalability. The eHomeCaregiving layered architecture consists of five layers: the user interface layer with three different interfaces, for the patient, caregiver, and care team member. The application layer contains the functional business logic, and the authorization layer is used to authorize users by directly accessing the local off-chain database to check their privileges to allow them to make changes in addition to authentication. The blockchain layer stores the part of the data that must remain immutable, known generator, and time sequence. The blockchain layer is connected directly to the database, and the physical layer consists of two different databases: hospital electronic medical records for patient treatment plans and local off-chain database, which is suitable for blockchain platforms, stores the other parts of the data.
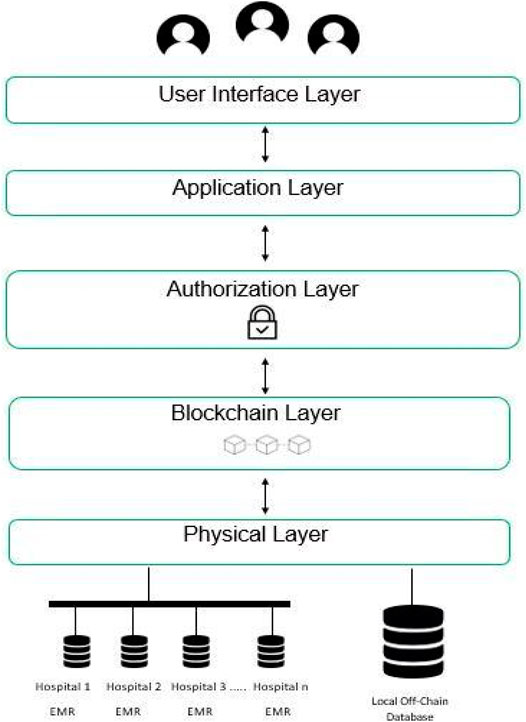
FIGURE 7. eHomeCaregiving architecture design.
eHomeCaregiving System Implementation
At the beginning of the implementation phase, it was important to decide which data should be stored in the database (i.e., off-chain data) and which should be stored in the solution’s blockchain ledger (i.e., on-chain data). The off-chain data were fully implemented using Firebase, and we decided to store the data related to the record care change use case consisting of four sub-use cases in the blockchain to be recorded in the shared ledger. Every patient has one ledger connected to their caregivers, and this contains all the data related to the use cases: Add Comment, Measuring Blood Sugar, Performed Treatment, and SOS Call. Figure 8 illustrates the off-chain and on-chain data components (explained below) along with the remaining system components.

FIGURE 8. Off-chain and on-chain components.
However, the storing of the on-chain data proved to be challenging. Therefore, a separate Web Dapp and IOS app were developed, as shown in Figure 9. The information is stored only on the blockchain. We then tried to store this information in both the database (off-chain) and the developed Dapp (on-Chain). Dapp was the only way to store information related to record care change.
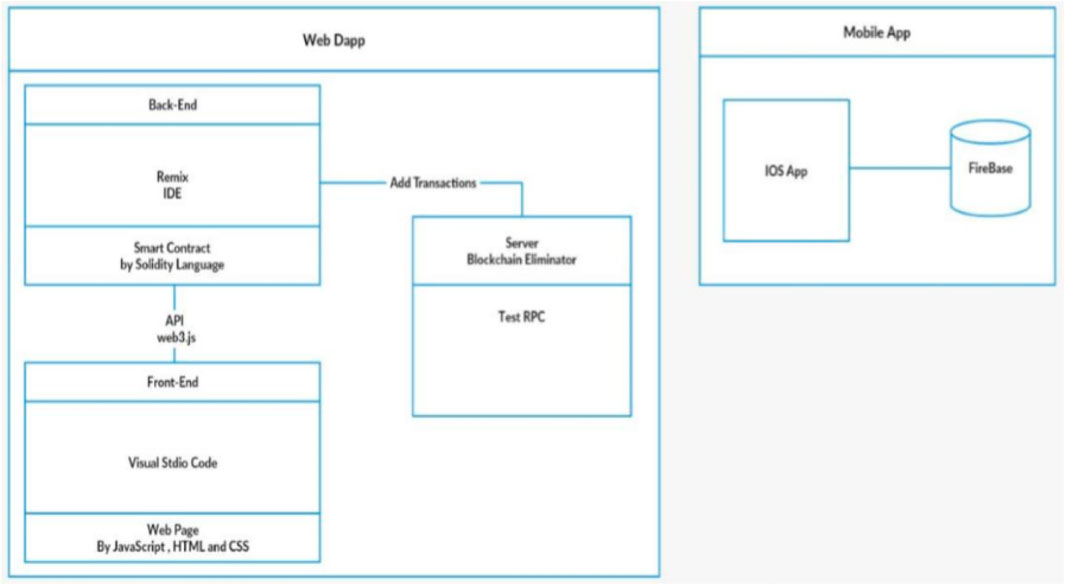
FIGURE 9. Structure of eHomeCaregiving.
First, off-chain data was constructed (Figure 10) using Firebase and connected it with an XCode project using Swift programming language; then, the designed interfaces were connected with related classes. In each class, the stored information of each function was saved in a database and retrieved. In addition, other functionalities of Firebase related to authentication were used, so that every time the user logs in after creating an account, it checks if they already exist in the authentication list.
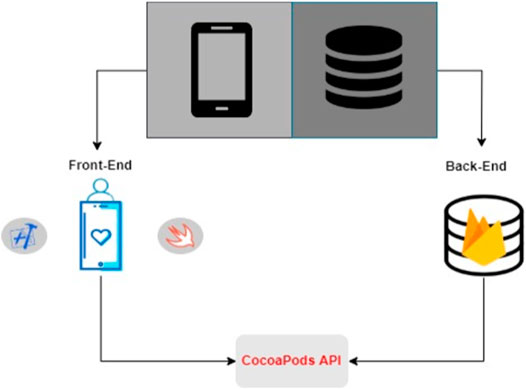
FIGURE 10. Off-chain components.
Second, as shown in Figure 11, the Web Dapp for Ethereum Blockchain is built separately from the IOS app. The Web Dapp consists of a front end, back end, and server. More specifically, the back end uses Remix to write, compile, and deploy a smart contract. Solidity programming language was used to write the smart contract. In addition, the Web3 provider was chosen as the execution environment connected to the Ethereum client node at the local host, as shown in Figure 12.
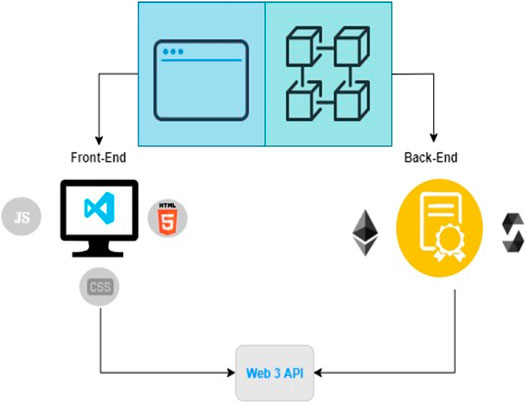
FIGURE 11. On-chain system components.
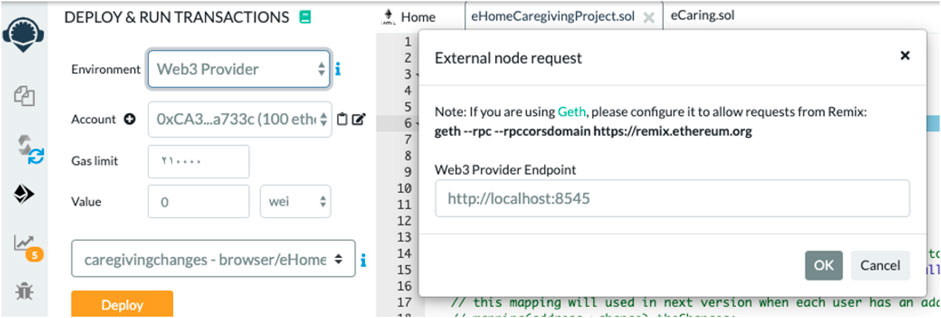
FIGURE 12. Screen shot of Web3 provider as execution environment.
The front end was developed using vscode to build a web page with HTML, JavaScript, and CSS. The connection of the back end with the front end uses Web3 to interact with the smart contract with the HTML page. The linking between them was achieved by obtaining the ContractABI and ContractAddress from Remix to the HTML page. Web3 was written on the HTML page using JavaScript. The back end and front end interacting with the TestRPC server is the Ethereum Blockchain emulator for running the transactions (Figure 13). When the TestRPC server is activated, it provides 10 fake Ethereum accounts with 100 Ethers for each account illustrated in Figure 14, which allows making calls to the blockchain.
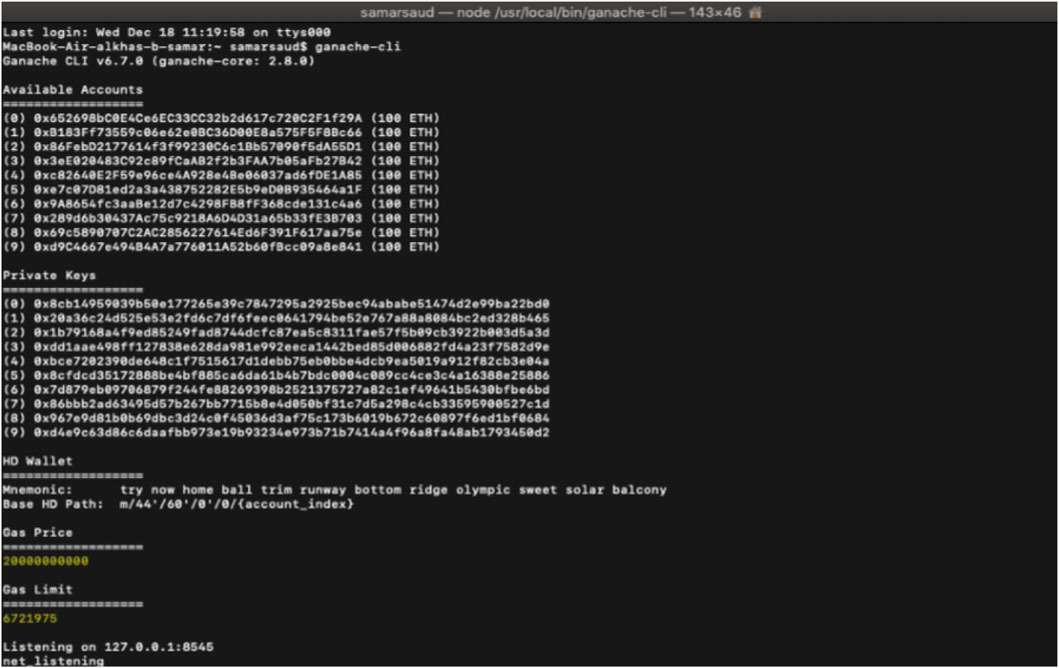
FIGURE 13. TestRPC (ganache-cli) and 10 accounts.
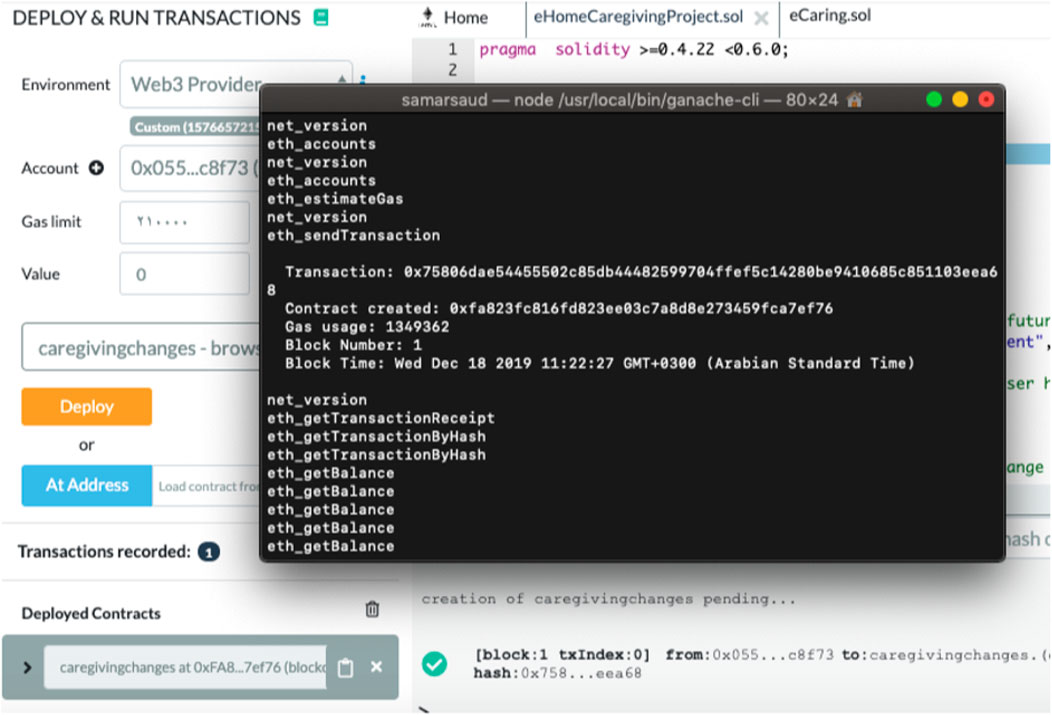
FIGURE 14. First transaction in blockchain when smart contract created.
The transactions were made by calling smart contract functions, as shown in Figure 14. The smart contract is called from web3 on the HTML page by using an account address. The transactions were performed in the TestRPC server.
After completing the previous stage, the Dapp was developed and improved by building a private Ethereum blockchain. A private Ethereum blockchain was built by, first, preparing the computer’s environment, and installing a dependency. Second, a smart contract was written using Solidity programming language and compiled it to the private Ethereum network using Truffle. Finally, to run the private Ethereum blockchain, the Geth Server was used.
eHomeCaregiving User Acceptance Testing
The purpose of acceptance testing is to confirm that the system is ready for operational use. During the acceptance test, end users (customers) of the system compare the system to its initial requirements. User acceptance testing was conducted at the College of Computer and Information Sciences (CCIS) and College of Nursing, King Saud University. A brief description of the system, its purpose, and functionalities were provided, and then the end users used an iPhone to evaluate the functionalities of the system. Six end users tested and evaluated the functionalities of the solution: one patient tested the functionalities associated with the patient, two caregivers tested the functionalities associated with the caregiver, and three care team members tested the functionalities associated with care team members. Furthermore, they were asked to answer survey questions. The feedback we received on the eHomeCaregiving proof-of-concept prototype exceeded our expectations regarding the role of caregiving. This system would adapt to more than one caregiver, which is helpful for full communication, and this property impressed the end users. Moreover, 75% of users who were caregivers and patients strongly agreed that all functionality provided in eHomeCaregiving was highly beneficial. All care team members agreed that the process of adding a treatment plan was smooth and easy. Finally, all participants recommend installing eHomeCaregiving; their opinions were that the system would help patients with diabetes receive optimal care. In addition, some highlighted that they would prefer to have a profile page for all users. The feedback can be explored further as a focus of future research.
Discussion and Conclusion
Caregiving is most commonly used to address impairments of people who are aging or have disabilities, diseases, conditions, injuries, or mental disorders. Supporting caregivers is one of the most important issues that has been neglected around the world, although there is a growing demand for their help, especially amidst the COVID-19 pandemic. Moreover, patients with diabetes require home caregiving since there are no hospitals or nursing homes that can accommodate their high and rising numbers. In addition, most of these patients are aged over 45 years, which means that these patients have type 2 diabetes and require special care. eHomeCaregiving aims to address the key challenges home caregivers face in supporting their loved ones, and the development of the application was motivated by the increasing number of patients with diabetes. There are many difficulties related to communication between caregivers and between caregivers and the care team in terms of communicating the accurate timestamped information regarding patients with diabetes. Meanwhile, the patients themselves face significant difficulties, such as waiting times and needing to see more than one doctor on the same day to receive full treatment, which may be stressful for them. In addition, there is a lack of Arabic speaking platforms that facilitate caregivers’ connectedness with patients with diabetes. eHomeCaregiving aims to build a blockchain-based social network ecosystem for patient-centered family caregiving. It empowers and connects the patients’ families, friends, and neighbors to share patient-centered information and informed decision making about care. eHomeCaregiving achieves this by allowing caregivers to track and record their patients’ care management changes, health status, and psychological status on an ongoing basis. It also provides caregivers with a treatment plan for diabetes and other comorbidities, as determined by the care team members. eHomeCaregiving would facilitate the process of caregivers’ connectedness to provide professional, timestamped care continuity to patients with type 2 diabetes in Saudi Arabia.
Nowadays, technology and human life cannot be separated; technology makes our lives much easier. It impacts education, communication, health, business, commerce, and more. Saudi society is a caring one, and eHomeCaregiving would have a profound influence on the caregiving process for patients with diabetes by allowing the patient’s family to receive continuous, patient-centered information to help them provide the best care while reducing the burden of caregiving. Furthermore, eHomeCaregiving has a significant impact on the field of computer science by allowing analysts, developers, and engineers to interact with healthcare professionals to provide a solution that serves patients with type 2 diabetes along with their caregivers. This study aimed to provide a system with full treatment plan for patients with diabetes who have different types of diseases and conditions associated with diabetes. Finally, this solution has an ethical and legal impact on society, as it provides transparency among all caregivers. eHomeCaregiving supports caregivers of patients with diabetes and improves the quality of their lives while maintaining care continuity. However, we noted a limitation in eHomeCaregiving. First, it is restricted to a specific sample of patients with type 2 diabetes who are the primary targets; it is focused specifically on the needs of the Saudi Arabian community, and it is restricted to iOS mobile phone users. Scalability is considered for future work on the application to include more languages, to involve communities from Arab countries as well as from the rest of the world, to cover other chronic diseases, including type 1 and 3 diabetes, to include Internet of Things (IoT) devices and wearables to connect eHomeCaregiving with caregivers’ and patients’ smart devices, and to include users of other operating systems, such as Android users.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author Contributions
HA wrote the article and contributed to the overall development from a subject-matter expertise perspective to validate the problem statement, design, and technical solution. SA (9th author) conceptualized the article, supervised and reviewed the concepts, design, development of the overall solution, and the article. GA, FR, SA (4th author), SA (5th author), RA, SA (7th author), implemented the solution, reviewed the literature, conducted the surveys and interviews for data gathering, and wrote relevant sections in this article. SA (9th author) contributed to the special needs of COVID-19 diabetes guidelines and article writing.
Funding
This work was funded by the Deanship of Scientific Research at the King Saud University.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Al-Hazzaa, H. M., Abahussain, N. A., Al-Sobayel, H. I., Qahwaji, D. M., and Musaiger, A. O. (2011). Physical Activity, Sedentary Behaviors and Dietary Habits Among Saudi Adolescents Relative to Age, Gender and Region. Int. J. Behav. Nutr. Phys. Activ. 8, 140. doi:10.1186/1479-5868-8-140
Al-Megren, S., Alsalamah, S., Altoaimy, L., Alsalamah, H., and Soltanisehat, L. (2018). Blockchain Use Cases in Digital Sectors: A Review of the Literature 2018 IEEE Confs on Internet of Things, Green Computing and Communications, Cyber, Physical and Social Computing, Smart Data, Blockchain, Computer and Information Technology, Congress on Cybermatics. 1417–1424. Halifax, Canada: IEEE. doi:10.1109/cybermatics2018.2018.00242
Alhowaish, A. (2013). Economic Costs of Diabetes in Saudi Arabia. J. Fam. Community Med. 20 (1), 1–7. doi:10.4103/2230-8229.108174
Alsalamah, S., Alsuwailem, G., Alrajeh, F., Aharbi, S., AlQahtani, S., AlArifi1, R., et al. (2019). HEALTHINFO 2019 : Building a Patient-Centered Blockchain Ecosystem for Caregivers: Diabetes Type II Case Study, The Fourth International Conference on Informatics and Assistive Technologies for Health-Care, Medical Support and Wellbeing.
Alsalamah, S., and Nuzzolese, E. (2020). Promising Blockchain Technology Applications and Use Case Designs for the Identification of Multinational Victims of Mass Disasters. Frontiers in Blockchain 3, 34. doi:10.3389/fbloc.2020.00034
Carely (2021). Available at: https://www.care.ly/ (Accessed April 17, 2021).
Caring (2021). Available at: https://www.thecaring.app/ (Accessed April 17, 2021).
Fitbit (2021). Available at: https://www.fitbit.com/global/us/home (Accessed April 17, 2021).
Florenica, A., (2013). IDF Diabetes Atlas. sixth edition. Basel: Switzerland: International Diabetes Federation.
Hunt, C. K. (2003). Concepts in Caregiver Research. J. Nurs. Scholarsh. 35, 1. doi:10.1111/j.1547-5069.2003.00027.x
International Diabetes Federation (2020). COVID-19 and Diabetes. Brussel, Belgium: International Diabetes Federation, 2020.
International Medical Travel Journal: News (2018). Saudi Arabia Lunches Healthcare Provision Program. International Medical Travel Journal. Available at: https://www.imtj.com/news/saudi-arabia-l:aunches-healthcare-privatisation-programme/(Accessed January 16, 2021).
Kronfol, N. M. (2012). Health Services to Group with Special Needs in the Arab World. East. Mediterr. Health J. 18, 12. doi:10.26719/2012.18.12.1247
Medisafe (2021). Medisafe App. Available at: https://www.medisafe.com/ (Accessed April 17, 2021).
pHealth (2017). Available at: http://www.phealth2017.eu/ (Accessed January 16, 2021).
Rouse, M. (2018). mHealth (Mobile Health). TechTarget Available at: https://searchhealthit.techtarget.com/definition/mHealth (Accessed January 16, 2021).
Saleem (2021). Available at: http://saleem.life/privacy.html (Accessed April 17, 2021). doi:10.7759/cureus.12091
Swan, M. (2015). Blockchain: Blueprint for New Economy. 1stedition. Sebastopol, CA, United States: O’Reilly Media Inc.
Sokary (2021). Available at: https://play.google.com/store/apps/details?id=com.sokry&hl=ar&gl=US. (Accessed April 17, 2021).
Synopsys Editorial team (2017). Top 4 Software Development Methodologies. Available at: https://www.synopsys.com/blogs/software-security/top-4-software-development-methodologies/. (Accessed January 16, 2021).
Thermo (2021). Apple Withings Thermo. Available at: https://apps.apple.com/us/app/withings-thermo/id1108420798 (Accessed April 17, 2021).
United Nations Population Fund (2020). World Population Dashboard, United Nations Population Fund. Available at: https://www.unfpa.org/data/world-population-dashboard (Accessed January 16, 2021).
Keywords: blockchain technology, caregiving, diabetes, eHealth, pHealth, patient-centered care, mHealth
Citation: Alsalamah HA, Alsuwailem G, Bin Rajeh F, Alharbi S, AlQahtani S, AlArifi R, AlShargi S, Alsalamah SA and Alsalamah S (2021) eHomeCaregiving: A Diabetes Patient-Centered Blockchain Ecosystem for COVID-19 Caregiving. Front. Blockchain 4:477012. doi: 10.3389/fbloc.2021.477012
Received: 16 January 2021; Accepted: 30 April 2021;
Published: 30 June 2021.
Edited by:
Jonathan Passerat-Palmbach, Imperial College London, United KingdomReviewed by:
Alexander Vladimirovich Bogdanov, Saint Petersburg State University, RussiaSoulla Louca, University of Nicosia, Cyprus
Copyright © 2021 Alsalamah, Alsuwailem, Bin Rajeh, Alharbi, AlQahtani, AlArifi, AlShargi, Alsalamah and Alsalamah. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hessah A. Alsalamah, aGFsc2FsYW1haEBrc3UuZWR1LnNh