
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Bioeng. Biotechnol., 22 September 2023
Sec. Tissue Engineering and Regenerative Medicine
Volume 11 - 2023 | https://doi.org/10.3389/fbioe.2023.1089031
 Yeqian Huang1
Yeqian Huang1 Hanxing Zhao1,2
Hanxing Zhao1,2 Yixi Wang1
Yixi Wang1 Siwei Bi1
Siwei Bi1 Kai Zhou2Hairui Li2
Kai Zhou2Hairui Li2 Changchun Zhou3Yudong Wang1Wenqing Wu1Bo Peng1,2Jun Tang1,2
Changchun Zhou3Yudong Wang1Wenqing Wu1Bo Peng1,2Jun Tang1,2 Bo Pan4Baoyun Wang1,2Zhixing Chen1,2Zhengyong Li1,2*
Bo Pan4Baoyun Wang1,2Zhixing Chen1,2Zhengyong Li1,2* Zhenyu Zhang1,2*
Zhenyu Zhang1,2*Microtia is a congenital deformity of the ear with an incidence of about 0.8–4.2 per 10,000 births. Total auricular reconstruction is the preferred treatment of microtia at present, and one of the core technologies is the preparation of cartilage scaffolds. Autologous costal cartilage is recognized as the best material source for constructing scaffold platforms. However, costal cartilage harvest can lead to donor-site injuries such as pneumothorax, postoperative pain, chest wall scar and deformity. Therefore, with the need of alternative to autologous cartilage, in vitro and in vivo studies of biomaterial scaffolds and cartilage tissue engineering have gradually become novel research hot points in auricular reconstruction research. Tissue-engineered cartilage possesses obvious advantages including non-rejection, minimally invasive or non-invasive, the potential of large-scale production to ensure sufficient donors and controllable morphology. Exploration and advancements of tissue-engineered cartilaginous framework are also emerging in aspects including three-dimensional biomaterial scaffolds, acquisition of seed cells and chondrocytes, 3D printing techniques, inducing factors for chondrogenesis and so on, which has greatly promoted the research process of biomaterial substitute. This review discussed the development, current application and research progress of cartilage tissue engineering in auricular reconstruction, particularly the usage and creation of biomaterial scaffolds. The development and selection of various types of seed cells and inducing factors to stimulate chondrogenic differentiation in auricular cartilage were also highlighted. There are still confronted challenges before the clinical application becomes widely available for patients, and its long-term effect remains to be evaluated. We hope to provide guidance for future research directions of biomaterials as an alternative to autologous cartilage in ear reconstruction, and finally benefit the transformation and clinical application of cartilage tissue engineering and biomaterials in microtia treatment.
Microtia is a congenital ear malformation that can develop as an isolated birth abnormality or one of the manifestations of other syndromes, which can be classified based on the severity of the deformity, from mild structural changes to complete absence of the auricle (Luquetti et al., 2012). Patients can present with stenosis of the external auditory canal, partial atresia or total atresia, and are often accompanied by hearing impairment (Siegert, 2003).
Microtia occurs in approximately 0.8–4.2 per 10,000 births (Yetman and Hormann, 2015). Current studies have indicated the association between microtia and certain genetic and environmental factors, but the etiology and cause of the extensive epidemic variability have not been thoroughly understood (Luquetti et al., 2012). The main surgical treatment for microtia is total auricle reconstruction. Current options for reconstructive materials broadly include autologous costal cartilage framework, implanted artificial material and auricular prostheses. The first two approaches can be placed subcutaneously or under a vascularized fascial flap and skin graft, while a prosthetic ear fixed on the skin is only applied in patients with severe injury or burn of the auricle, extensive scar resulting in insufficient skin volume, or those who failed in both former two procedures (Zhang et al., 2019a).
One of the basic factors of auricular reconstruction is the supporting framework under skin to maintain the fine anatomical structure of the ear. At present, the supporting framework/scaffold mainly includes the auricular framework carved from the patient’s autologous costal cartilage, the Medpor prefabricated framework, and the tissue-engineered cartilage auricular framework. Autologous costal cartilage transplantation has been the current gold standard treatment for auricular reconstruction, which has the advantages of easy engraving, no rejection, and low incidence of cartilage exposure (Wilkes et al., 2014). In 1920, Gillies first performed external ear reconstruction by embedding the sculpted autologous costal cartilage into the subcutaneous tissue of the mastoid region, which was the earliest auricular framework procedure for microtia (Berghaus and Toplak, 1986). Tanzer is considered one of the leading practitioners of autologous costochondral grafts in ear reconstruction. In 1959 he described a six-stage auricular reconstruction procedure and changed the initial 6-stage procedure to a 4-stage ear reconstruction method as the clinical practice progressed (Tanzer, 1959; Tanzer, 1967; Tanzer, 1978). In 1980, Brent modified the Tanzer method and simplified the operation into three stages. A series of improvements were proposed such as personalized design of ear scaffold and storage of wedge cartilage to support the auricle in later reconstruction to form a more three-dimensional structure (Brent, 1980; Brent, 1999; Brent, 2002). In 1993, Nagata further reduced the procedure to two stages and emphasized the use of superficial temporal fascia flaps and sectional skin. The Nagata method provides a more reliable covering tissue for the scaffold and the layered and reinforced stents also minimize the deformation, which has become one of the most widely used methods in auricle reconstruction (Nagata, 1994a; Nagata, 1994b; Nagata and Edgerton, 1994). Meanwhile, the three-stage tissue expansion method of auricle reconstruction with autologous costal cartilage has also developed rapidly. The tissue expander provides an additional skin flap to cover the cartilage framework without transplantation of the skin graft, and the scar can be invisible. The thinner skin can ensure a more natural appearance and skin color of the reconstructed auricle, especially in some elaborate subunit structures (Park, 2000).
Generally, the 6th, 7th, and 8th costal cartilages of the contralateral thorax were selected as the donor area for sculpting and reinforcing the main framework of the auricular framework (Bly et al., 2016). However, the procedure may cause variable cosmetic results, and costal cartilage harvest can also lead to donor-site defects such as pneumothorax, chest wall pain and chest wall scar (Humphries et al., 2022). Besides, the ideal timing of operation occurs at least from 6 years old in consideration of the development of costal cartilage for framework carving, while in adulthood, costal cartilage becomes calcified and gradually loses elasticity, which is not desirable for surgery (Zhang et al., 2019a). Medpor (Stryker, United States) is a prefabricated synthetic biocompatible porous polyethylene implant that can be custom shaped intraoperatively by heating or engraving (Ali et al., 2017; Jiang et al., 2021). Porous polyethylene is an inorganic, hydrophobic and non-resorbable material that can be utilized in facial reconstructive treatments. However, the main deficiencies of the Medpor auricular framework lie in the significant risk of implant extrusion, fracture, immunogenicity and infection compared to autologous tissue (Romo et al., 2006; Zhang et al., 2019b), which therefore is not commonly applied in ear reconstruction.
Therefore, with the need of an alternative to autologous cartilage, in vitro and in vivo study of biomaterial scaffolds, bioprinting technologies and cartilage tissue engineering have gradually become novel research hot points in auricular reconstruction research (Bichara et al., 2012). Tissue engineering aims to rebuild tissues and organs that can be surgically implanted by utilizing cells and biomaterials (Melgarejo-Ramírez et al., 2016), and the tissue-engineered cartilage possesses benefits including non-rejection, minimal or no invasiveness, the potential of large-scale production to ensure sufficient donors and controllable morphology (Chen and Liu, 2016). This review will mainly discuss the development, current application and research progress of cartilage tissue engineering in auricular reconstruction. We hope to provide guidance for future research directions of biomaterials and finally benefit the transformation and clinical practice in ear reconstruction treatment in microtia.
Tissue engineering technologies use a combination of cells, engineering, materials techniques, and appropriate biochemical and physicochemical parameters to generate different types of target tissues (Langer and Vacanti, 1993). In clinical practice, successful translation in the repair or replacement of portions or whole tissues has been reported in bone (Bhumiratana et al., 2016), cartilage (Whitney et al., 2017), blood vessels (Olausson et al., 2012), bladder (Atala et al., 2006), skin (Boyce and Lalley, 2018) etc., which provides a novel direction for the auricular reconstruction in microtia. Cartilage tissue mainly consists of chondrocytes, extracellular matrix (ECM) and tissue fluid. The extracellular matrix (ECM) of cartilage is made up of collagen fibers (mostly type II collagen) supporting glycoproteins and proteoglycans with a protein core connected with glycosaminoglycan molecules such as hyaluronic acid (HA) and chondroitin sulfate (Hunziker et al., 2002). Exploration and challenges in generating a tissue-engineered cartilaginous framework mainly lie in the acquisition of optimal chondrogenic cell source and creation of a three-dimensional scaffold that the cells can grow upon, inducing factors for chondrogenesis and so on (Figure 1).
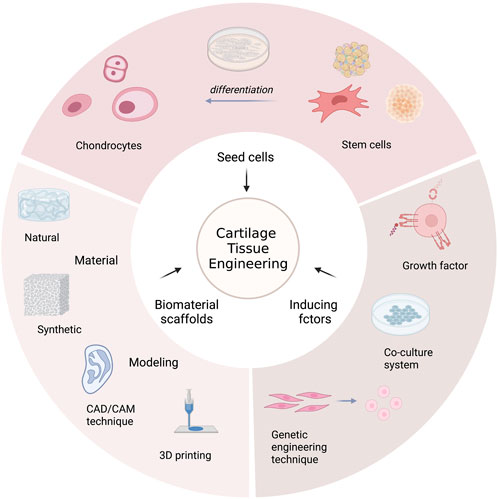
FIGURE 1. The overview of cartilage tissue engineering.
Tissue engineering utilizes progenitor cells that can proliferate and differentiate to obtain biological tissues. Currently, seed cell sources in relation to cartilage regeneration mainly include chondrocytes and stem cells such as bone-marrow-derived mesenchymal stem cells (BMSCs), adipose-derived stem cells (ADSCs), induced pluripotent stem cells (iPSCs), articular cartilage progenitor cells (ACPCs), etc.
Chondrocytes isolated from a biopsy of patients’ autologous cartilage tissues continue to be the principal source of engineered cartilage, for its property of spontaneously secreting cartilage-specific matrix (Xu et al., 2005). Autologous chondrocytes can be obtained from articular hyaline cartilage, auricular elastic cartilage, nasoseptal elastic cartilage and costal hyaline cartilage. The biomechanical and metabolic characteristics of the resulting neocartilage are expected to vary depending on the source of cells employed, and whether the ectopic-derived chondrocytes can regenerate specific types of cartilage and achieve functional reconstruction remains uncertain. For auricular cartilage regeneration, the corresponding type of chondrocytes can be more accessible from the auricle, while it has also been proved that the chondrocytes obtained from nasal septum or auricle sites have higher proliferative activity (Tay et al., 2004; Zhang et al., 2014).
Since the initial attempt at in vitro culturing of the chondrocytes in the 1960s, the optimization of isolation and amplification of chondrocytes has been extensively studied in tissue engineering (Chesterman and Smith, 1968). Studies were mostly focused on the transplantation of isolated chondrocytes into cartilage defects. In 1994, Brittberg et al. (1994) described the autologous chondrocyte implantation (ACI) approach, which has been continuously developed since its first clinical use for articular cartilage repair. During the ACI procedure, chondrocytes were isolated using trypsin and col-lagenase digestion and cultured in vitro in DMEM/F12 with 10% autologous serum supplement. The culturing approach was originally established for the implantation of cells in suspensions, with periosteum or collagen membrane as the mechanical covering. Subsequent studies have improved the technique of cell culturing with a carrier membrane or a 3D scaffold. For instance, hyalograft-C biomaterial scaffold was constructed by network fibers with different-sized interstices, which can be employed as a 3D-scaffold to support cell proliferation, redifferention and extracellular matrix deposition with desirable mechanical properties (Gobbi et al., 2006). Research have also been focused on different phenotypic zones of cartilage tissue. Chondrocytes from the superficial, middle, or deep zones of articular cartilage can be harvested through surface abrasion technique, and then cultured in alginate and seeded on scaffolds to generate cartilaginous tissues. The mechanical and functional properties of cartilaginous tissues formed by different layers of chondrocytes exhibit varied results, but in clinical practice, chondrocytes are often extracted from a full-thickness biopsy (Brittberg et al., 2010).
In 2001, the concept of chondrocyte quality control was presented, with the idea that an enhanced stable population of chondrocytes could be employed to provide more consistent results from the transplantation of autologous chondrocytes. According to current research, approximately 100–150 million chondrogenic cells are required to generate an adult human auricular-shaped cartilage based on the type and porosity of the scaffold material (Bichara et al., 2012; Zhang et al., 2014). In addition, chondrocytes from the original pathologic auricle of patients can be extracted via enzymatic digestion, which suggested a possible treatment for microtia based on autologous auricular chondrocyte harvest. For example, He et al. (2020) cultured dedifferentiated microtia chondrocytes in a three-dimensional chondrogenic culture system and generated redifferentiated microtia chondrocytes, with the potential to regenerate mature cartilage.
However, major challenges can lie in the in vitro expansion process in which chondrocytes are prone to dedifferentiation, the determination of chondrocyte type and quantity, and the rapid loss of cartilage regeneration ability. To enhance the quality of engineered cartilage structures, several chemical stimuli, including collagen cross-linking boosters, growth factors, and catabolic enzymes have been used in regenerative medicine for cartilage-related abnormalities (Phull et al., 2016).
Stem cells are also important cells with multilineage differentiation potential, which may be employed as a cell source for cartilage tissue engineering. For tissue-engineered articular cartilage, it is mainly implanted into the articular cavity that is rich in chondrogenic inducing factors such as cytokines and mechanical stimulation, which helps the implanted seed cells to fabricate mature chondroid tissue as well as retain the cartilage phenotype. Therefore, a variety of candidate seed cell sources have been accessible for further exploration. While for auricular cartilage reconstruction, there is a lack of chondrogenic inducing signal in subcutaneous transplantation area, which can be adverse to the phenotype stability of the cartilage generated by stem cells, resulting in fibrosis or ossification of chondrocytes (Liu et al., 2008). The current progress of stem cells in articular cartilage tissue engineering may provide reference value, and the co-culturing of chondrocytes and MSCs may also provide a more feasible scheme for seed cells to produce stable regenerated cartilage, which will be described in following section.
Mesenchymal stem cells (MSCs) can be isolated from adipose tissue, synovium, bone marrow and umbilical cord matrix, among which bone marrow-derived MSCs (BMSCs) are especially characterized with high proliferation rate and the potential for chondrogenic differentiation under proper tissue conditions (Moretti et al., 2010) and certain chondrogenic inducing factors such as insulin growth factor 1 (IGF-1), transforming growth factor β1 (TGF-β1) and platelet-rich plasma (PRP) (Mara et al., 2010; Xie et al., 2012; Maldonado and Nam, 2013). Moreover, the multilineage differentiation potential could be maintained after multiple amplification, which has made BMSCs a conductive choice to achieve tissue-specific repair of articular cartilage defects (Zhou et al., 2004; Zhou et al., 2006). Studies have also demonstrated the therapeutic potential of these cells in osteoarthritis (Cho et al., 2020; Anil et al., 2021). Although promising results have indicated the potential as a novel cell source for cartilage repair procedures, the main drawbacks of employing BMSCs are the invasive approach for harvesting cells and the possible complications (Urlić and Ivković, 2021). In addition, it has been shown that the frequency of BMSCs is relatively low (0.001%–0.01%) and that their differentiation capability decreases with age, which may impair the effectiveness of BMSCs in stem cell treatment (Zaim et al., 2012). Moreover, the engineered cartilage regenerated from MSCs was found to present more significant genetic differences from natural cartilage compared to that from primary culture chondrocytes, which may limit the clinical application of MSCs (Bomer et al., 2016).
Adipose-derived stem cells (ADSCs) can differentiate into adipocytes, osteocytes, chondrocytes, and nerve cells under different conditions. These cells have the advantages of abundant tissue sources, easily accessible sampling, low immunogenicity, rapid proliferation and multi-directional differentiation potential, which has become a research hotspot as seed cells in cartilage tissue engineering (Fahy et al., 2018). TGF-β has been proven to induce chondrogenic differentiation of ADSCs (Cicione et al., 2015). IGF-1 was also reported to have the potential alone or act with TGF-β1 to induce chondrogenic differentiation of ADSCs in vitro and in vivo (Lee et al., 2013). Griffin et al. (2019) utilized an argon plasma to modify the nanocomposite polyurethane scaffolds, which were found to facilitate the osteogenic and chondrogenic differentiation of ADSCs.
Induced pluripotent stem cells (iPSCs) can be obtained from somatic cells through reprograming procedures, which were firstly derived from retrovirus-mediated transcription factors into fibroblasts and eventually achieve embryonic-like multilineage differentiation potential (Diederichs et al., 2019) (Takahashi and Yamanaka, 2006). Independent studies considering chondrogenic differentiation application have been focused on osteoarthritis (OA) models. iPSCs were proved to differentiate into chondroid cells in vitro under induced directional induction and successfully generate articular matrix cartilage to repair defects after transplantation (Zhang et al., 2016; Zhu et al., 2016; Rim et al., 2018). A study utilized 3D bio-printing Kenzan approach to fabricate a scaffold-free engineered cartilage construct based on iPSCs. Anatomically shaped cartilage constructs were produced with improved mechanical strength, which may provide a clinically translatable strategy for chondral resurfacing in articular cartilage damages (Nakamura et al., 2021). However, uncertainties of the genetic modification remain to be evaluated, including the target gene overexpression, tissue malformations and impact on pathogenicity and safety of the host, which may be future challenges for iPSC-based cartilage reconstruction application (Yamashita et al., 2018).
Although articular cartilage tissue is not intrinsic reparative, it has demonstrated the existence of progenitor cells that promote the appositional growth of the tissue. Articular cartilage stem cells/progenitor cell (ACPC) was first identified and isolated by Gary P (Dowthwaite et al., 2004). from the surface zone of articular which possesses multilineage differentiation potential, with chondrogenic predisposition in particular. Subsequent research and phenotypic analyses illustrated that ACPCs may serve comparable functions to other tissue-specific stem cells (Fickert et al., 2004; Hiraoka et al., 2006; Seol et al., 2012; Bernstein et al., 2013; Jiang and Tuan, 2015). Jiang et al. (Jiang et al., 2016) group have identified a group of endogenous stem/progenitor cells derived from mature human chondrocytes by tracking the specific molecular markers, which were defined as chondrocyte-derived progenitor cells (CDPCs). CDPCs showed similar phenotypes as BMSCs, while exhibiting greater chondrogenic potential. Furthermore, CDPCs were used to treat large-scale cartilage tissue defects in clinical practice. All fifteen patients who received tissue-engineered cartilage tissue transplantation based on CDPCs achieved satisfactory recovery. The discovery of CDPCs may provide a promising prospect for clinical application. A study involving ACPCs, MSCs and chondrocytes reported that based on platelet-rich plasma (PRP) gel scaffold, ACPCs showed superiority in migration, proliferative and chondrogenesis capacities over the other cell types, which indicated a new strategy for cartilage regeneration (Wang et al., 2019). Meanwhile, ACPCs have also been discovered in both healthy and microtia ear remnants. Evaluation of the repair capabilities via in vitro culture revealed that these cells possess a robust ability to proliferate without losing their multipotent differentiation capacity and to create cartilage-like matrix in the culture framework (Otto et al., 2022), which may suggest a feasible candidate cell type for ear reconstruction.
The biological scaffold serves as a temporary substitute that mimics the cartilage extracellular matrix, on which the isolated seed cells can be planted after in vitro expansion. Subsequently, after in vitro culture, they are transplanted back into the body to achieve the purpose of tissue repair or replacement (Huang et al., 2018). The ideal scaffold should preserve a structurally stable three-dimensional projection, satisfactory biocompatibility and degradability, and be easy to manipulate into a certain form. It should be able to provide a favorable physiological environment for the cells while also maintaining the temporary mechanical integrity that is necessary to generate an elaborately structured framework throughout the process of chondrogenesis. Meanwhile, to sustain the form of the construct, the degradation rate of the scaffold must be commensurate with the tissue regeneration rate. In addition, it should be sturdy while providing flexible structural support to complement the neocartilage (Hoshi et al., 2018; Yang et al., 2019). Over the past few decades, varied types of natural, synthetic and hybrid materials have been explored in vitro and in vivo as biological scaffolds (Pearson et al., 2017).
For auricular tissue engineering, natural materials are mainly hydrogel polymers, among which alginate, pluronic, hyaluronic acid, chitosan, and collagen derivatives have been investigated as potential candidates to produce bioactive scaffolds (Yue et al., 2015; Rastogi and Kandasubramanian, 2019). The capacity to be injected and shaped into three-dimensional structures is an evident benefit of these materials. Besides, no apparent cytotoxicity has been found and the inflammatory reaction can be mild. However, inadequate mechanical strength, fast deterioration rate in vivo, and difficulties in morphological maintenance are their main drawbacks (Catoira et al., 2019; Yang et al., 2019; Salehi et al., 2020).
Alginate is derived from seaweed and forms hydrogels when in contact with calcium ions. The physical characteristics can be modified by adjusting the concentrations of alginate and calcium, which has been utilized to preserve chondrogenesis in animal and human and produce neocartilage (Ponticiello et al., 2000; Chang et al., 2001; Chang et al., 2003). Leslie et al. (2013); Leslie et al. (2018) developed a method to obtain degradable alginate saline gel by adding alginate lyase which can deliver stem cells through injection. The controlled release of ADSCs was achieved through alginate microbeads, which were then confirmed to form the chondroid tissue in rabbit ear defect model. Gelatin can be obtained through partial hydrolysis of collagen. When added with β-fibroblast growth factors (β-FGFs), the gelatin sponge scaffold can promote a slow release of β-FGF to facilitate the formation of auricle cartilage (Otani et al., 2015). The interaction of thrombin and fibrinogen yields fibrin gel which can be extracted from autologous plasma, and it can also be employed as a vehicle for cell transport (Silverman et al., 1999). Yue et al. (2021) developed a chondrocytes/chondrocyte-microtissues laden fibrin gel ear-shape scaffold, which has regenerated a stable anatomical structure in a rabbit model. Pluronic F-127 (consisting of 70% polyethylene oxide and 30% polypropylene oxide) is a synthetic thermosensitive hydrogel that has been illustrated to sustain engineered neocartilage (Cao et al., 1998; Saim et al., 2000; Kamil et al., 2004). Research directions have also focused on the modification of natural polymers via cross-linking and surface functionalization to enhance the mechanical and degradation properties (García-López et al., 2015; Xu et al., 2020). Collagen gel sponges were believed to increase the adhesion and proliferation of chondrocytes and the production of fibrocartilage-like ECM (Houck et al., 2018). More recently, studies based on collagen gel were carried out which focus on the mixture of seed cell types with different ratios (Cohen et al., 2018) and appropriate times of the seed cell passage (Bernstein et al., 2018), indicating that the tissue engineering ear reconstruction technology is developing towards a more precise and optimized strategy.
Synthetic polymers, notably aliphatic polyesters with fine biodegradability and biocompatibility such as polyglycolic acid (PGA), polylactic acid (PLA), and poly-caprolactone (PCL) and are widely used as medical biodegradable materials, controlled drug delivery systems and tissue engineering scaffolds (Arif et al., 2019; Wu et al., 2021). The advantage that synthetic polymers own over biological polymers is that they are custom-made materials whose biological and material features may be modified chemically and physically, and thus ensures strong plasticity, fine mechanical properties, and accurate control of morphology maintenance after implantation (Chen et al., 2020a). However, foreign body response and the lack of surface morphology that promotes cellular adhesion and development are the main limitations. The substance and its degradation products can trigger the foreign body inflammatory response and inhibit cartilage regeneration after implantation (Coenen et al., 2018). In addition, the lack of physiological qualities of flexible materials, material exposure, infection, and other complications might also be potential concerns.
In 1997, Cao et al. (1997) reported the generation of human ear-shaped engineered cartilage in a nude mouse model which consisted of a PGA/PLA scaffold seeded with bovine chondrocytes. After removing the supporting stent, the constructs demonstrated instability and deformation, but the picture vividly demonstrated the enormous clinical translation potential of tissue engineering. Shieh et al. (2004) assessed PGA scaffolds covered with poly-L-lactic acid (PLLA), PCL, and poly-4 hydroxybutyrate for engineered cartilage formation and structure maintenance in nude mouse and rabbit models for 10 months. Cartilage formation was observed in scaffolds of all types with the PCL obtained with the optimal structure of human auricular, while constructions showed significant deformation in rabbit models. A number of follow-up studies utilizing different types of cells and combinations of synthetic polymers have been published since then. Nakao et al. (2017) constructed nanoscale-diameter PGA scaffolds with the microtia remnant chondrocytes seeded on and found the regenerative cartilage in histological similarity to normal auricular chondrocyte, which maintained over 40 weeks. Zhang et al. (2014) cultured microtia chondrocytes and BMSCs with pressed PGA fiber mesh coated with PLA scaffold. The ear-shaped construction showed a complex structure with 100% chondrocytes formed. In 2018, Zhou et al. (2018) conducted the regeneration of patient-specific auricular and the first clinical translation in the field of tissue engineering in total ear reconstruction. In this study of five unilateral microtia patients, a three-dimensional (3D) printed resin model was employed to fabricate a scaffold comprising PCL as the kernel and PGA/PLA for the outer layer. The scaffold was trimmed according to the resin ear model, implanted with ear chondrocytes and cultured in vitro. The first patient presented a satisfactory reconstructed auricular morphology after the 2.5-year follow-up, and the histological examination also showed typical cartilage formation which resembles natural cartilage. Meanwhile, they also preliminarily coped with the inflammatory reaction of stent material by extending the induction time in vitro. This research provided a new strategy to improve the mechanical strength of engineered cartilage and maintain the morphology after implantation. However, the residual polymer materials are prone to cause aseptic inflammation, and the formation and distribution of chondrocytes and ECM also affect the mechanical stability, which remains the major problems to be solved in the application of synthetic material scaffolds.
During the last decade, hybrid materials consisting of natural and artificial synthetic materials have gradually become a research hotspot on account of the shortcomings of single materials. Experiments have been carried out to obtain composites with good histocompatibility, controllable morphology, and appropriate mechanical properties with the fabrication of hybrid implants. There are also studies emphasizing the combination of degradable and nondegradable materials in an attempt to help maintain the framework of the complex auricular contours.
Studies have reported the usage of fibrin gel where auricular chondrocytes are suspended to cover the Medpor framework with oxidizing solution utilized to alter the implant’s surface by adding hydrophilic properties (Lee et al., 2011; Hwang et al., 2014). There was a significant reduction of skin necrosis, implant exposure and extrusion with engineered cartilage-covered implants compared to the bare Medpor scaffold, which suggested a promising prospect of this combined implant with structural and functional stability for total ear reconstruction. Bichara et al. (2010) described cartilage engineering with alginate hydrogel and porous poly (vinyl alcohol). Improved surface chemistry and cartilage development on porous polyethylene may contribute to alleviating the constraints of scaffold extrusion and skin erosion. Alginate/PCL composite scaffolds were constructed with a 3D-printed PCL outer model and an injected alginate hydrogel, providing suitable mechanical and biomimetic properties for chondrocyte formation. With a pore size of 300 μm, the PCL model can be convenient for assembly, degradation and absorption (Visscher et al., 2019). A co-culturing of ADSCs and chondrocytes based on an alginate/PCL framework also depicted an enhanced tendency of chondrogenic differentiation (Jang et al., 2020). Similar results were seen in the co-culture of ADSCs and auricular chondrocytes by replacing the internal hydrogel with hyaluronic acid-collagen (Zopf et al., 2018). Hybrid materials composed of synthetic and natural biological materials in different forms or proportions can achieve comprehensive properties by improving the biocompatibility while also maintaining the mechanical properties, which may become preferable scaffold sources in future research and application of auricular tissue engineering.
Diverse biomaterial scaffold fabrication techniques have been established for processing different microstructures with controlled characteristics such as pore size, porosity, and pore interconnectivity, such that they are suited for chondrocyte growth, adhesion, and rapid nutrient transport (Kuberka et al., 2002). The most common methods include solvent casting/salt leaching, 3D fiber deposition, electrospinning, hydrogels and so on.
Solvent casting and particulate leaching (SC/PL) approach requires the construction of a salt/polymer suspension that is cast using a specific solvent. Upon solidification, as a result of solvent evaporation, the salt may be dissolved out of the scaffold and exit the pores. The pore spaces involved in such scaffolds may improve the proliferation and extracellular matrix production and benefit the growth of chondrocytes. However, this SC/PL technique was reported to achieve well effect mainly in small templates (Lee et al., 2003; Gong et al., 2008). Jing et al. (2006), (Wu et al., 2005) conducted a fabrication of 3D porous scaffolds based on a specially designed rigid-flexible mold using a particle leaching approach combined with compression molding. Scaffold shrinkage was tolerable under normal fabrication conditions with high salt contents, however, it requires precise control of the processing temperature and comparatively high loading of the compressing machine. Electrospinning can produce nanoscale fibers in an electrostatic field, resulting in high cell attachment-specific surface areas. These fibers resemble the collagen fibrils present in ECM, giving a highly porous, mechanical, and structural support. The usage of such scaffold architectures in cartilage tissue creation has shown encouraging results (Min et al., 2004; Li et al., 2005). Three-dimensional fiber deposition employs thermoplastic polymers that are delivered from a computer-controlled syringe onto a template so that the fibers can solidify in a predetermined manner, which is reproducible and revisable. As the layers of fibers accumulate, a structure of consistent pore size and 100% porosity can be formed (Woodfield et al., 2004).
Injection modeling has been extensively studied based on natural material scaffolds such as alginate (Chang et al., 2001; Chang et al., 2003; Dobratz et al., 2009), fibrin gel (Silverman et al., 1999) and pluronic F-127 (Saim et al., 2000). The engineered gel-chondrocytes construct can be molded by previously prepared silastic molds and injected into the subcutaneous tissue of animal molds (Yang et al., 2000) or used as a direct minimally invasive implant material for further exploration. However, the individual construction of such molds is time-consuming, and the quality cannot be precisely controlled and adjusted. The initial stage to construct an engineered auricle is the exact design and sculpting of the 3D distinctive contralateral auricle. Therefore, the development of computer-assisted processing methodology has become increasingly essential.
Computer aided design and manufacturing (CAD/CAM) has been reported in the preoperative planning and the creation of patient-specific ear prostheses (Nishimoto et al., 2014; Bos et al., 2015), and has also been utilized to assist in the fabrication of bioscaffolds in tissue engineering. Liu et al. (2010a) have developed an approach to precisely fabricate the auricular cartilage in vitro with the same structure which is mirror-symmetrical to the normal ear. The CAD/CAM method was applied to produce a negative cast of a half-sized human ear in a mirror image. Based on this mold, it was capable to form the PGA fibers into a scaffold in the shape of a typical ear in half size. Furthermore, they enhanced the mechanical strength of the PGA scaffold by coating it with an optimized amount of PLA, which as well maintained the biocompatibility of the framework. This technique has also been actively employed subsequently in the field of auricular tissue engineering (Zhou et al., 2018; Visscher et al., 2019; Jia et al., 2022).
Three-dimensional (3D) printing based on CAD/CAM enables rapid production of patient-specific anatomically attainable 3D models (Chae et al., 2015). Specifically, the CAD/CAM technique accurately carries out intricate 3D data transformations like scaling, mirroring, and Boolean operations. Printing methods can include extrusion, inkjet, laser-assisted, etc (Derakhshanfar et al., 2018). Spatial resolution and mechanical qualities may also be precisely controlled during 3D printing in addition to scaffold form (Gu et al., 2016; Mouser et al., 2020). The structures were constructed by layering biocompatible materials, known as cell-based “bio-ink,” from the bottom up (Zopf et al., 2015), and the expected tissues or organs can be obtained through in vitro culture. Bio-inks are cross-linked or stabilized during or immediately after printing to fabricate the desired structure (Kačarević Ž et al., 2018). An ideal bio-ink should provide tissue constructs with adequate mechanical strength and robustness while retaining tissue-matching mechanics and supporting chemical modifications in a specific tissue. It also requires fine biocompatibility, biodegradability, adjustable gelation and stabilization of the biomaterial (Loo et al., 2015).
Different natural and synthetic biomaterials with specific features have been identified as cell-laden bio-inks in different bioprinting applications (Lee et al., 2016a). Currently, there are two major types of 3D-printed auricle scaffolds, including hydrogels which auricle shape is printed directly, and biomaterials as support framework covered by a cell-containing hydrogel using 3D printing or immersing the scaffold into the hydrogel (Jang et al., 2020). Hydrogels have unique cell-binding sites that are advantageous for cell attachment, spreading, growth, and differentiation. In addition, several of these biomaterials may be readily photocross-linked in their modified forms (Wang et al., 2022). Silk fibroin (Rosadi et al., 2019), alginate (Unagolla and Jayasuriya, 2020), gelatin (Duan et al., 2013; Unagolla and Jayasuriya, 2020), and chitosan are often utilized as printing materials or used as part of a cartilage scaffold. Such hydrogels can act as a cell matrix to support cell growth (Unagolla and Jayasuriya, 2020). The use of high molecular weight polymers in 3D printing of irregularly shaped cartilage has also been reported in several studies, including poly (lactic-co-glycolic acid) (PLGA) (Wei et al., 2020), PLA (Rosenzweig et al., 2015), PCL (Xu et al., 2019; Li et al., 2021a), and polyurethane (Kim et al., 2019), to print cartilage scaffolds that are stable due to their optimal mechanical properties. Although natural bio-ink has good biocompatibility, its stability and mechanical properties are less satisfactory, and it is inclined to represent more rapid degradation, while synthetic bio-ink has excellent mechanical properties, but the lack of biological activity remains to be a major drawback (Wang et al., 2021).
Zopf et al. (2015) developed a 3D-printed PCL scaffold seeded with swine chondrocytes, which was then injected with a hydrogel-based construct involving growth and differentiation factors, which increased chondroinductivity in animal models after transplantation. Lee et al. (2014) constructed an auricular-shaped 3D scaffold comprised of cell-laden alginate hydrogel supported by a PCL-based biocompatible polymeric framework. This study utilized a method known as the Multi-head tissue/organ building system (MtoBS), in which two cytotypes were added to a three-dimensional construct independently. Chondrocytes and adipocytes derived from ADSCs were employed to generate auricular cartilage and the earlobe respectively and the chondrogenesis and adipogenesis were demonstrated by in vitro immunostaining (Lv et al., 2012). A unique 3D scaffold based on a chondrocyte-laden alginate construction with an integrated circular coil antenna attached to cochlear-shaped electrodes was designed by Mannoor et al. (2013). A study has designed a section of the polymeric framework with added silver nanoparticles, which were served as a conductive substance to embed the antenna. This attempt aimed to treat not only the cosmetic aspect of microtia but also the hearing impairment that results from it.
Gelatin methacrylate (GelMA) is a photosensitive semi-synthetic hydrogel that when combined with a photoinitiator, it can be quickly cross-linked and solidified to produce a three-dimensional structure of particular strength. The structure contains cell adhesion sites and matrix metalloproteinase hydrolysis sites, which enables cell growth and migration (Yue et al., 2015). The mechanical properties of the cross-linked hydrogel can be adjusted by changing the degree of substitution and the concentration of GelMA material. GelMA is mostly utilized for tissue engineering and 2D/3D cell culture due to its high biocompatibility. It can also be configured into mixed ink for 3D bioprinting based on the characteristics of printed tissue (Pepelanova et al., 2018).
In the field of auricular reconstruction, research has focused on the combination of PCL and GelMA as scaffolds, which depicts compressive properties similar to native auricular cartilage with satisfactory shape preservation, on which abundant cartilage-like matrix was produced based on progenitor cells (Otto et al., 2021). In another study, 3D-printed ear-shaped PLA scaffolds were prepared initially, and chondrocytes were fastened to the scaffolds via GelMA hydrogels, which showed good proliferative properties and stabilized structure after implantation (Tang et al., 2021). Novel bio-ink designs based on GelMA have also been actively conducted. A biomimetic microporous methacrylate-modified acellular cartilage matrix (ACMMA) was fabricated which then supported the generation of mature auricular cartilage-like tissues with satisfactory realistic form, elasticity and cartilage-specific ECM deposition in vivo (Jia et al., 2022). In combination with GelMa, bio-inks based on microtissues comprising microtia chondrocytes and cartilage acellular matrix (CAM) microparticles were printed by digital light processing with high printing accuracy. Mature cartilage regeneration was demonstrated in the mice model after transplantation (Xie et al., 2022).
Most recently, a first-in-human clinical trial of a 3D-bioprinted living tissue ear implant (AuriNovo™, United States) was conducted led by a regenerative medicine company (3DBio, United States) for ear reconstruction in patients with unilateral microtia (NCT04399239). The printed collagen hydrogel scaffold was made to encase the patient’s auricular chondrocytes after 3D scanning of the opposite ear which precisely matches the patient’s auricular shape. Exclusive 3D-bioprinter, bio-ink, cell culture system and implanted protective technology were designed systematically in the therapeutic production. This procedure may make breakthrough progress in the 3D bioprinting field in auricular reconstruction in the future, and the 3D-bioprinted implants may provide beneficial effects for microtia patients. Moreover, it also suggests the great significance of 3D bioprinting technique in a broader field of regenerative medicine, such as the realization of organ printing.
It is estimated that approximately 100–150 million chondrogenic cells are required to generate an adult human ear-shaped cartilage (Bichara et al., 2012), but cells that have undergone different cultures may dedifferentiate and lead to the gradual loss of the original cartilage phenotype. Therefore, a variety of growth factors are required as crucial inducing elements which they can be incorporated into culture media directly or by other biological techniques to promote chondrocyte growth, morphology maintenance and cartilage formation. Currently, growth factors promoting cartilage regeneration in articular cartilage defects have been extensively studied, which also provides reference value and guidance for auricular cartilage reconstruction.
Transforming growth factor β (TGF-β) family act as multifunctional components mostly produced in cartilage and bone. TGF-β1, TGF-β2 and TGF-β3 are correlated with the processes of differentiation and de-differentiation of chondrocytes as a prelude to cartilage synthesis, stimulation of type II collagen and proteoglycans as well as differentiation of MSCs (Patil et al., 2011). TGF-β1 has been reported to facilitate inducing undifferentiated MSCs into a chondrogenic pathway, integrating chondrocytes into endogenous tissues and enhancing cartilage repair (Fan et al., 2006). The research of auricular reconstruction considering chondrocyte culturing has proved the vital role of TGF in improving redifferentiation and matrix formation of auricular chondrocytes, as well as proliferation and chondrogenesis of MSCs (Shieh et al., 2004). Bone morphogenetic proteins (BMPs) regulate the proliferation and differentiation of osteoblasts and chondrocytes (Katagiri and Watabe, 2016). Different types of BMPs have shown promising effectiveness in inducing chondrogenesis and auricular cartilage defect repair in animal models (Kuo et al., 2006; Vinatier et al., 2009; Li et al., 2021b). A study based on remnant auricular cartilage of microtia patients also illustrated that BMP-2 in the atelocollagen with the addition of insulin and T3 in the media could generate greater glycosaminoglycan (GAG) matrix in a shorter period but also sustain cell viability with lower mortality (Ko et al., 2012). BMP-7 and BMP-2 were also reported to help increase matrix production in nasal chondrocytes in vitro (Hicks et al., 2007). Insulin-like growth factor-1 (IGF-1) is considered a significant mediator mainly expressed in mature and developing cartilage which is involved in the maintenance of cartilage homeostasis (Davies et al., 2008). Studies have indicated that IGF-1 can serve as a stimulation factor for proteoglycan synthesis, chondrocyte proliferation, and cell homing in osteochondral defect repair (Pabbruwe et al., 2009; Cho et al., 2020). Combination of insulin and IGF-1 has shown additional benefits in formation and properties of engineered auricular cartilage with the thickness of native auricular cartilage (Rosa et al., 2014). Fibroblast growth factors (FGFs) are involved in chondrocyte proliferation, cell division and osteogenic processes (Itoh, 2014). FGF-2 was proven to increase GAG and type II collagen biosynthesis and proliferation and differentiation in costal chondrocytes and articular chondrocytes (Kato and Gospodarowicz, 1985; Veilleux and Spector, 2005), while FGF-18 was found to stimulate hyaline-cartilage production (Gigout et al., 2017; Sennett et al., 2018). Studies have also indicated that sustained release of b-FGF augments can enhance neovascularization and chondrogenesis in a tissue-engineered auricular cartilage construct (Isogai et al., 2005).
Despite the stable proliferation of auricular chondrocytes, dedifferentiation with rapid loss of chondrocyte phenotype and competence is unavoidable during repeated passages (Kang et al., 2012). The co-culturing system allows different cell types to be cultured together, which can help to investigate the effects and the molecules involved in cell-to-cell interactions such as cellular stimulation, gene pathways and cellular differentiation (Carter et al., 2015). Chondrocytes and MSCs were concurrently seeded onto an engineered scaffold in a co-culture experiment. It has shown that chondrocytes can stimulate BMSCs to differentiate into chondroblasts by producing exogenous growth factors, which can lessen the demand for exogenous growth factor supply (Fischer et al., 2010; Xue et al., 2012). Additionally, chondrocytes can act as a matrix for MSC migration and prevent MSC-derived chondrocytes from ossifying (Mo et al., 2009; Liu et al., 2010b). It has been proved that the biological induction co-culture mode of ADSCs and chondrocytes can induce the differentiation of ADSCs into osteoblasts and chondroblasts (Shi et al., 2017; Chen et al., 2020b). A study of a co-culture model of ADSCs and chondrocytes achieved successful production of cartilage based on 3D-printed bioresorbable scaffolds without the use of exogenous growth factors (Morrison et al., 2018). At present, research on co-culture of stem cells and articular chondrocytes has made significant progress in the field of biological engineering, which also provides guidance for auricular cartilage reconstruction. Co-culturing technique may develop a new solution for limited quantity and dedifferentiation of seed cells in cartilage tissue engineering and promote clinical translation of auricular cartilage engineering with lower cost and more stable tissue formation.
Genetic engineering technique intends to transfer cartilage growth factor genes into target cells through a carrier (such as adeno-associated virus) or attach the carrier to a biological scaffold so that the growth factor can achieve a stable and sustained expression to promote cartilage regeneration. Studies considering gene transfer of growth factors such as IGF-1, BMP-2, TGF-β and FGF-2 have been reported to lead to an enhancement in chondrogenic differentiation of MCSs (Cucchiarini et al., 2011; Lee et al., 2016b; Ikeda et al., 2017; Munsell et al., 2018). Genetic transfer technique has also become a research hotspot of cartilage, while more experimental evidence is still needed to evaluate the safety and effectiveness of this technology.
At present, surgical procedure based on autologous costal cartilage carving and transplantation remains the major treatment of total ear reconstruction. During the past decades, a variety of research and progress has been made in the field of auricular cartilage tissue engineering. The application of 3D printing and tissue engineering in medicine holds great promise for future innovation and more consistent results for microtia patients. The 3D printing approach can shorten operation time, avoid morbidity at the donor region, produce repeatable outcomes and reduce rejection rates compared to autologous costal cartilage transplantation. However, the prohibitive cost, limited application of printers and clinical translation obstacles are still confronted challenges before these potentially revolutionary choices become available to patients.
Clinical trials in human have also achieved preliminary results, but the safety and long-term effectiveness have not been fully confirmed. Before large-scale clinical application, a number of scientific and technical challenges need to be solved. The complex interrelation between cellular biochemistry, immunoreaction, and biomechanics of natural and synthetic material requires further investigation to design and fabricate the optimal individual-characterized auricular cartilage. The exploration and development of hybrid materials may be a favorable direction to obtain an ideal cartilage scaffold. The pathogenesis and molecular biomechanism of chondrogenic process in congenital microtia need to be further studied, which may contribute to the optimization of cartilage regeneration system.
The research progress of tissue-engineered cartilage in ear reconstruction requires mutual promotion of multiple research fields, and further to develop a systematic and standardized model of scaffold fabrication, cell extraction and culturing, and construct implantation to realize the clinical transformation and application of tissue-engineered auricular reconstruction in microtia.
YH: conceptualization, data curation, writing—original draft and submission. HZ: conceptualization, data curation, writing—reviewing and editing. YIW: data curation, writing—reviewing and editing. SB: data curation, writing—reviewing and editing. KZ: data curation, writing—reviewing and editing. HL: writing—reviewing and editing. CZ: writing—reviewing and editing. YDW: data curation. WW: data curation. BPE: data curation. JT: data curation. BPA: data curation. BW: data curation. ZC: data curation, writing—reviewing and editing. ZL: conceptualization, writing—reviewing and editing and supervision. ZZ: conceptualization, writing—reviewing and editing and supervision. All authors revised and approved the article, then agreed to be accountable for all aspects of the work.
This work was funded by Sichuan Science and Technology Program (2022YFS0197, 2022NSFSC0717, and 2022NSFSC1579), and the 1·3·5 Project for Disciplines of Excellence, West China Hospital, Sichuan University (ZYPY20003 and ZYPY20004).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Ali, K., Trost, J., Truong, T., and Harshbarger, R. (2017). Total ear reconstruction using porous polyethylene. Semin. Plast. Surg. 31 (3), 161–172. doi:10.1055/s-0037-1604261
Anil, U., Markus, D. H., Hurley, E. T., Manjunath, A. K., Alaia, M. J., Campbell, K. A., et al. (2021). The efficacy of intra-articular injections in the treatment of knee osteoarthritis: A network meta-analysis of randomized controlled trials. Knee 32, 173–182. doi:10.1016/j.knee.2021.08.008
Arif, U., Haider, S., Haider, A., Khan, N., Alghyamah, A. A., Jamila, N., et al. (2019). Biocompatible polymers and their potential biomedical applications: A review. Curr. Pharm. Des. 25 (34), 3608–3619. doi:10.2174/1381612825999191011105148
Atala, A., Bauer, S. B., Soker, S., Yoo, J. J., and Retik, A. B. (2006). Tissue-engineered autologous bladders for patients needing cystoplasty. Lancet (London, Engl. 367 (9518), 1241–1246. doi:10.1016/s0140-6736(06)68438-9
Berghaus, A., and Toplak, F. (1986). Surgical concepts for reconstruction of the auricle. History and current state of the art. Archives otolaryngology--head neck Surg. 112 (4), 388–397. doi:10.1001/archotol.1986.03780040028007
Bernstein, J. L., Cohen, B. P., Lin, A., Harper, A., Bonassar, L. J., and Spector, J. A. (2018). Tissue engineering auricular cartilage using late passage human auricular chondrocytes. Ann. Plast. Surg. 80 (4), S168–s173. doi:10.1097/sap.0000000000001400
Bernstein, P., Sperling, I., Corbeil, D., Hempel, U., and Fickert, S. (2013). Progenitor cells from cartilage--no osteoarthritis-grade-specific differences in stem cell marker expression. Biotechnol. Prog. 29 (1), 206–212. doi:10.1002/btpr.1668
Bhumiratana, S., Bernhard, J. C., Alfi, D. M., Yeager, K., Eton, R. E., Bova, J., et al. (2016). Tissue-engineered autologous grafts for facial bone reconstruction. Sci. Transl. Med. 8 (343), 343ra83. doi:10.1126/scitranslmed.aad5904
Bichara, D. A., O'Sullivan, N. A., Pomerantseva, I., Zhao, X., Sundback, C. A., Vacanti, J. P., et al. (2012). The tissue-engineered auricle: Past, present, and future. Tissue Eng. Part B Rev. 18 (1), 51–61. doi:10.1089/ten.teb.2011.0326
Bichara, D. A., Zhao, X., Hwang, N. S., Bodugoz-Senturk, H., Yaremchuk, M. J., Randolph, M. A., et al. (2010). Porous poly(vinyl alcohol)-alginate gel hybrid construct for neocartilage formation using human nasoseptal cells. J. Surg. Res. 163 (2), 331–336. doi:10.1016/j.jss.2010.03.070
Bly, R., Bhrany, A. D., Murakami, C. S., and Sie, K. C. (2016). Microtia reconstruction. Facial plastic Surg. Clin. N. Am. 24 (4), 577–591. doi:10.1016/j.fsc.2016.06.011
Bomer, N., den Hollander, W., Suchiman, H., Houtman, E., Slieker, R., Heijmans, B., et al. (2016). Neo-cartilage engineered from primary chondrocytes is epigenetically similar to autologous cartilage, in contrast to using mesenchymal stem cells. Osteoarthr. Cartil. 24 (8), 1423–1430. doi:10.1016/j.joca.2016.03.009
Bos, E. J., Scholten, T., Song, Y., Verlinden, J., Wolff, J., Forouzanfar, T., et al. (2015). Developing a parametric ear model for auricular reconstruction: A new step towards patient-specific implants. J. Craniomaxillofac Surg. 43 (3), 390–395. doi:10.1016/j.jcms.2014.12.016
Boyce, S. T., and Lalley, A. L. (2018). Tissue engineering of skin and regenerative medicine for wound care. Burns Trauma 6, 4. doi:10.1186/s41038-017-0103-y
Brent, B. (2002). Microtia repair with rib cartilage grafts: A review of personal experience with 1000 cases. Clin. plastic Surg. 29 (2), 257–271.
Brent, B. (1999). Technical advances in ear reconstruction with autogenous rib cartilage grafts: Personal experience with 1200 cases. Plastic Reconstr. Surg. 104 (2), 335–338. doi:10.1097/00006534-199908000-00002
Brent, B. (1980). The correction of mi-rotia with autogenous cartilage grafts: I. The classic deformity.? Plastic Reconstr. Surg. 66 (1), 1–12. doi:10.1097/00006534-198007000-00001
Brittberg, M.U.o.G., Sweden (2010). Cartilage tissue repair: Autologous chondrocyte implantation. Regen. Med. Biomaterials Repair Connect. Tissues 19 (4), 227–250.
Brittberg, M., Lindahl, A., Nilsson, A., Ohlsson, C., Isaksson, O., and Peterson, L. (1994). Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. N. Engl. J. Med. 331 (14), 889–895. doi:10.1056/nejm199410063311401
Cao, Y., Rodriguez, A., Vacanti, M., Ibarra, C., Arevalo, C., and Vacanti, C. A. (1998). Comparative study of the use of poly(glycolic acid), calcium alginate and pluronics in the engineering of autologous porcine cartilage. J. Biomater. Sci. Polym. Ed. 9 (5), 475–487. doi:10.1163/156856298x00578
Cao, Y., Vacanti, J. P., Paige, K. T., Upton, J., and Vacanti, C. A. (1997). Transplantation of chondrocytes utilizing a polymer-cell construct to produce tissue-engineered cartilage in the shape of a human ear. Plast. Reconstr. Surg. 100 (2), 297–302. doi:10.1097/00006534-199708000-00001
Carter, M., and Shieh, J. (2015). “Chapter 14 - cell culture techniques,” in Guide to research techniques in neuroscience. Editors M. Carter, and J. Shieh Second Edition (San Diego: Academic Press), 295–310.
Catoira, M. C., Fusaro, L., Di Francesco, D., Ramella, M., and Boccafoschi, F. (2019). Overview of natural hydrogels for regenerative medicine applications. J. Mater Sci. Mater Med. 30 (10), 115. doi:10.1007/s10856-019-6318-7
Chae, M. P., Rozen, W. M., McMenamin, P. G., Findlay, M. W., Spychal, R. T., and Hunter-Smith, D. J. (2015). Emerging applications of bedside 3D printing in plastic surgery. Front. Surg. 2, 25. doi:10.3389/fsurg.2015.00025
Chang, S. C., Rowley, J. A., Tobias, G., Genes, N. G., Roy, A. K., Mooney, D. J., et al. (2001). Injection molding of chondrocyte/alginate constructs in the shape of facial implants. J. Biomed. Mater Res. 55 (4), 503–511. doi:10.1002/1097-4636(20010615)55:4<503::aid-jbm1043>3.0.co;2-s
Chang, S. C., Tobias, G., Roy, A. K., Vacanti, C. A., and Bonassar, L. J. (2003). Tissue engineering of autologous cartilage for craniofacial reconstruction by injection molding. Plast. Reconstr. Surg. 112 (3), 793–799. doi:10.1097/01.prs.0000069711.31021.94
Chen, F., and Liu, X. (2016). Advancing biomaterials of human origin for tissue engineering. Prog. Polym. Sci. 53, 86–168. doi:10.1016/j.progpolymsci.2015.02.004
Chen, L., Liu, J., Guan, M., Zhou, T., Duan, X., and Xiang, Z. (2020). <p>Growth factor and its polymer scaffold-based delivery system for cartilage tissue engineering</p>. Int. J. Nanomedicine 15, 6097–6111. doi:10.2147/ijn.s249829
Chen, Y., Wang, G., Ouyang, X., Wu, Y., and Guo, S. (2020). Co-Culture and mechanical stimulation on mesenchymal stem cells and chondrocytes for cartilage tissue engineering. Curr. Stem Cell Res. Ther. 15 (1), 54–60. doi:10.2174/1574888x14666191029104249
Chesterman, P. J., and Smith, A. U. (1968). Homotransplantation of articular cartilage and isolated chondrocytes. An experimental study in rabbits. J. Bone Jt. Surg. Br. 50 (1), 184–197. doi:10.1302/0301-620x.50b1.184
Cho, H., Kim, J., Kim, S., Jung, Y. C., Wang, Y., Kang, B. J., et al. (2020). Dual delivery of stem cells and insulin-like growth factor-1 in coacervate-embedded composite hydrogels for enhanced cartilage regeneration in osteochondral defects. J. Control Release 327, 284–295. doi:10.1016/j.jconrel.2020.08.002
Cicione, C., Muiños-López, E., Hermida-Gómez, T., Fuentes-Boquete, I., Díaz-Prado, S., and Blanco, F. J. (2015). Alternative protocols to induce chondrogenic differentiation: Transforming growth factor-β superfamily. Cell Tissue Bank. 16 (2), 195–207. doi:10.1007/s10561-014-9472-7
Coenen, A. M. J., Bernaerts, K. V., Harings, J. A., Jockenhoevel, S., and Ghazanfari, S. (2018). Elastic materials for tissue engineering applications: Natural, synthetic, and hybrid polymers. Acta Biomater. 79, 60–82. doi:10.1016/j.actbio.2018.08.027
Cohen, B. P., Bernstein, J. L., Morrison, K. A., Spector, J. A., and Bonassar, L. J. (2018). Tissue engineering the human auricle by auricular chondrocyte-mesenchymal stem cell co-implantation. PLoS One 13 (10), e0202356. doi:10.1371/journal.pone.0202356
Cucchiarini, M., Ekici, M., Schetting, S., Kohn, D., and Madry, H. (2011). Metabolic activities and chondrogenic differentiation of human mesenchymal stem cells following recombinant adeno-associated virus-mediated gene transfer and overexpression of fibroblast growth factor 2. Tissue Eng. Part A 17 (15-16), 1921–1933. doi:10.1089/ten.tea.2011.0018
Davies, L. C., Blain, E. J., Gilbert, S. J., Caterson, B., and Duance, V. C. (2008). The potential of IGF-1 and TGFβ1 for promoting “adult” articular cartilage repair: AnIn VitroStudy. Tissue Eng. Part A 14 (7), 1251–1261. doi:10.1089/ten.tea.2007.0211
Derakhshanfar, S., Mbeleck, R., Xu, K., Zhang, X., Zhong, W., and Xing, M. (2018). 3D bioprinting for biomedical devices and tissue engineering: A review of recent trends and advances. Bioact. Mater 3 (2), 144–156. doi:10.1016/j.bioactmat.2017.11.008
Diederichs, S., Klampfleuthner, F. A. M., Moradi, B., and Richter, W. (2019). Chondral differentiation of induced pluripotent stem cells without progression into the endochondral pathway. Front. Cell Dev. Biol. 7, 270. doi:10.3389/fcell.2019.00270
Dobratz, E. J., Kim, S. W., Voglewede, A., and Park, S. S. (2009). Injectable cartilage: Using alginate and human chondrocytes. Arch. Facial Plast. Surg. 11 (1), 40–47. doi:10.1001/archfacial.2008.509
Dowthwaite, G., Bishop, J. C., Redman, S. N., Khan, I. M., Rooney, P., Evans, D. J. R., et al. (2004). The surface of articular cartilage contains a progenitor cell population. J. cell Sci. 117, 889–897. doi:10.1242/jcs.00912
Duan, B., Hockaday, L. A., Kang, K. H., and Butcher, J. T. (2013). 3D bioprinting of heterogeneous aortic valve conduits with alginate/gelatin hydrogels. J. Biomed. Mater Res. A 101 (5), 1255–1264. doi:10.1002/jbm.a.34420
Fahy, N., Alini, M., and Stoddart, M. J. (2018). Mechanical stimulation of mesenchymal stem cells: Implications for cartilage tissue engineering. J. Orthop. Res. 36 (1), 52–63. doi:10.1002/jor.23670
Fan, H., Hu, Y., Qin, L., Li, X., Wu, H., and Lv, R. (2006). Porous gelatin–chondroitin–hyaluronate tri-copolymer scaffold containing microspheres loaded with TGF-β1 induces differentiation of mesenchymal stem cellsin vivo for enhancing cartilage repair. J. Biomed. Mater Res. A 77 (4), 785–794. doi:10.1002/jbm.a.30647
Fickert, S., Fiedler, J., and Brenner, R. E. (2004). Identification of subpopulations with characteristics of mesenchymal progenitor cells from human osteoarthritic cartilage using triple staining for cell surface markers. Arthritis Res. Ther. 6 (5), R422–R432. doi:10.1186/ar1210
Fischer, J., Dickhut, A., Rickert, M., and Richter, W. (2010). Human articular chondrocytes secrete parathyroid hormone-related protein and inhibit hypertrophy of mesenchymal stem cells in coculture during chondrogenesis. Arthritis Rheum. 62 (9), 2696–2706. doi:10.1002/art.27565
García-López, J., Garciadiego-Cázares, D., Melgarejo-Ramírez, Y., Sánchez-Sánchez, R., Solís-Arrieta, L., García-Carvajal, Z., et al. (2015). Chondrocyte differentiation for auricular cartilage reconstruction using a chitosan based hydrogel. Histol. Histopathol. 30 (12), 1477–1485. doi:10.14670/HH-11-642
Gigout, A., Guehring, H., Froemel, D., Meurer, A., Ladel, C., Reker, D., et al. (2017). Sprifermin (rhFGF18) enables proliferation of chondrocytes producing a hyaline cartilage matrix. Osteoarthr. Cartil. 25 (11), 1858–1867. doi:10.1016/j.joca.2017.08.004
Gobbi, A., Kon, E., Berruto, M., Francisco, R., Filardo, G., and Marcacci, M. (2006). Patellofemoral full-thickness chondral defects treated with hyalograft-C: A clinical, arthroscopic, and histologic review. Am. J. Sports Med. 34 (11), 1763–1773. doi:10.1177/0363546506288853
Gong, Y., Ma, Z., Zhou, Q., Li, J., Gao, C., and Shen, J. (2008). Poly(lactic acid) scaffold fabricated by gelatin particle leaching has good biocompatibility for chondrogenesis. J. Biomater. Sci. Polym. Ed. 19 (2), 207–221. doi:10.1163/156856208783432453
Griffin, M. F., Ibrahim, A., Seifalian, A. M., Butler, P. E., Kalaskar, D. M., and Ferretti, P. (2019). Argon plasma modification promotes adipose derived stem cells osteogenic and chondrogenic differentiation on nanocomposite polyurethane scaffolds; implications for skeletal tissue engineering. Mater Sci. Eng. C Mater Biol. Appl. 105, 110085. doi:10.1016/j.msec.2019.110085
Gu, B. K., Choi, D. J., Park, S. J., Kim, M. S., Kang, C. M., and Kim, C. H. (2016). 3-dimensional bioprinting for tissue engineering applications. Biomater. Res. 20, 12. doi:10.1186/s40824-016-0058-2
He, A., Ye, A., Song, N., Liu, N., Zhou, G., Liu, Y., et al. (2020). Phenotypic redifferentiation of dedifferentiated microtia chondrocytes through a three-dimensional chondrogenic culture system. Am. J. Transl. Res. 12 (6), 2903–2915.
Hicks, D. L., Sage, A. B., Shelton, E., Schumacher, B. L., Sah, R. L., and Watson, D. (2007). Effect of bone morphogenetic proteins 2 and 7 on septal chondrocytes in alginate. Otolaryngol. Head. Neck Surg. 136 (3), 373–379. doi:10.1016/j.otohns.2006.10.040
Hiraoka, K., Grogan, S., Olee, T., and Lotz, M. (2006). Mesenchymal progenitor cells in adult human articular cartilage. Biorheology 43 (3), 447–454.
Hoshi, K., Fujihara, Y., Yamawaki, T., Harai, M., Asawa, Y., and Hikita, A. (2018). Biological aspects of tissue-engineered cartilage. Histochem Cell Biol. 149 (4), 375–381. doi:10.1007/s00418-018-1652-2
Houck, D. A., Kraeutler, M. J., Belk, J. W., McCarty, E. C., and Bravman, J. T. (2018). Similar clinical outcomes following collagen or polyurethane meniscal scaffold implantation: A systematic review. Knee Surg. Sports Traumatol. Arthrosc. 26 (8), 2259–2269. doi:10.1007/s00167-018-4838-1
Huang, K., Li, Q., Li, Y., Yao, Z., Luo, D., Rao, P., et al. (2018). Cartilage tissue regeneration: The roles of cells, stimulating factors and scaffolds. Curr. Stem Cell Res. Ther. 13 (7), 547–567. doi:10.2174/1574888x12666170608080722
Humphries, S., Joshi, A., Webb, W. R., and Kanegaonkar, R. (2022). Auricular reconstruction: Where are we now? A critical literature review. Eur. Arch. Otorhinolaryngol. 279 (2), 541–556. doi:10.1007/s00405-021-06903-5
Hunziker, E. B., Quinn, T. M., and Häuselmann, H. J. (2002). Quantitative structural organization of normal adult human articular cartilage. Osteoarthr. Cartil. 10 (7), 564–572. doi:10.1053/joca.2002.0814
Hwang, C. M., Lee, B. K., Green, D., Jeong, S. Y., Khang, G., Jackson, J. D., et al. (2014). Auricular reconstruction using tissue-engineered alloplastic implants for improved clinical outcomes. Plast. Reconstr. Surg. 133 (3), 360e–369e. doi:10.1097/01.prs.0000438460.68098.4b
Ikeda, Y., Sakaue, M., Chijimatsu, R., Hart, D. A., Otsubo, H., Shimomura, K., et al. (2017). IGF-1 gene transfer to human synovial MSCs promotes their chondrogenic differentiation potential without induction of the hypertrophic phenotype. Stem Cells Int. 2017, 1–10. doi:10.1155/2017/5804147
Isogai, N., Morotomi, T., Hayakawa, S., Munakata, H., Tabata, Y., Ikada, Y., et al. (2005). Combined chondrocyte-copolymer implantation with slow release of basic fibroblast growth factor for tissue engineering an auricular cartilage construct. J. Biomed. Mater Res. A 74 (3), 408–418. doi:10.1002/jbm.a.30343
Itoh, N. (2014). “Fibroblast growth factor (FGF)☆,” in Reference module in biomedical sciences (Amsterdam, Netherlands: Elsevier).
Jang, C. H., Koo, Y., and Kim, G. (2020). ASC/chondrocyte-laden alginate hydrogel/PCL hybrid scaffold fabricated using 3D printing for auricle regeneration. Carbohydr. Polym. 248, 116776. doi:10.1016/j.carbpol.2020.116776
Jia, L., Hua, Y., Zeng, J., Liu, W., Wang, D., Zhou, G., et al. (2022). Bioprinting and regeneration of auricular cartilage using a bioactive bioink based on microporous photocrosslinkable acellular cartilage matrix. Bioact. Mater 16, 66–81. doi:10.1016/j.bioactmat.2022.02.032
Jiang, C., Zhao, C., Chen, B., Lu, L., Sun, Y., Yan, X., et al. (2021). Auricular reconstruction using Medpor combined with different hearing rehabilitation approaches for microtia. Acta Otolaryngol. 141 (6), 572–578. doi:10.1080/00016489.2021.1900601
Jiang, Y., Cai, Y., Zhang, W., Yin, Z., Hu, C., Tong, T., et al. (2016). Human cartilage-derived progenitor cells from committed chondrocytes for efficient cartilage repair and regeneration. Stem Cells Transl. Med. 5 (6), 733–744. doi:10.5966/sctm.2015-0192
Jiang, Y., and Tuan, R. S. (2015). Origin and function of cartilage stem/progenitor cells in osteoarthritis. Nat. Rev. Rheumatol. 11 (4), 206–212. doi:10.1038/nrrheum.2014.200
Jing, D., Wu, L., and Ding, J. (2006). Solvent-assisted room-temperature compression molding approach to fabricate porous scaffolds for tissue engineering. Macromol. Biosci. 6 (9), 747–757. doi:10.1002/mabi.200600079
Kačarević Ž, P., Rider, P., Alkildani, S., Retnasingh, S., Smeets, R., Jung, O., et al. (2018). An introduction to 3D bioprinting: Possibilities, challenges and future aspects. Mater. (Basel) 11 (11), 2199. doi:10.3390/ma11112199
Kamil, S. H., Vacanti, M. P., Vacanti, C. A., and Eavey, R. D. (2004). Microtia chondrocytes as a donor source for tissue-engineered cartilage. Laryngoscope 114 (12), 2187–2190. doi:10.1097/01.mlg.0000149455.68135.de
Kang, N., Liu, X., Guan, Y., Wang, J., Gong, F., Yang, X., et al. (2012). Effects of co-culturing BMSCs and auricular chondrocytes on the elastic modulus and hypertrophy of tissue engineered cartilage. Biomaterials 33 (18), 4535–4544. doi:10.1016/j.biomaterials.2012.03.019
Katagiri, T., and Watabe, T. (2016). Bone morphogenetic proteins. Cold Spring Harb. Perspect. Biol. 8 (6), a021899. doi:10.1101/cshperspect.a021899
Kato, Y., and Gospodarowicz, D. (1985). Sulfated proteoglycan synthesis by confluent cultures of rabbit costal chondrocytes grown in the presence of fibroblast growth factor. J. Cell Biol. 100 (2), 477–485. doi:10.1083/jcb.100.2.477
Kim, H. Y., Jung, S. Y., Lee, S. J., Lee, H. J., and Truong, M. D. (2019). Fabrication and characterization of 3D-printed elastic auricular scaffolds: A pilot study. Laryngoscope 129 (2), 351–357. doi:10.1002/lary.27344
Ko, E., Fujihara, Y., Ogasawara, T., Asawa, Y., Nishizawa, S., Nagata, S., et al. (2012). BMP-2 embedded atelocollagen scaffold for tissue-engineered cartilage cultured in the medium containing insulin and triiodothyronine—a new protocol for three-dimensional in vitro culture of human chondrocytes. Part C. Methods 18 (5), 374–386. doi:10.1089/ten.tec.2011.0217
Kuberka, M., Von Heimburg, D., Schoof, H., Heschel, I., and Rau, G. (2002). Magnification of the pore size in biodegradable collagen sponges. Int. J. Artif. Organs 25 (1), 67–73. doi:10.1177/039139880202500111
Kuo, A. C., Rodrigo, J., Reddi, A., Curtiss, S., Grotkopp, E., and Chiu, M. (2006). Microfracture and bone morphogenetic protein 7 (BMP-7) synergistically stimulate articular cartilage repair. Osteoarthr. Cartil. 14 (11), 1126–1135. doi:10.1016/j.joca.2006.04.004
Langer, R., and Vacanti, J. P. (1993). Tissue engineering. Science 260 (5110), 920–926. doi:10.1126/science.8493529
Lee, C. S., Watkins, E., Burnsed, O. A., Schwartz, Z., and Boyan, B. D. (2013). Tailoring adipose stem cell trophic factor production with differentiation medium components to regenerate chondral defects. Tissue Eng. Part A 19 (11-12), 1451–1464. doi:10.1089/ten.tea.2012.0233
Lee, D. Y., Lee, H., Kim, Y., Yoo, S. Y., Chung, W. J., and Kim, G. (2016). Phage as versatile nanoink for printing 3-D cell-laden scaffolds. Acta Biomater. 29, 112–124. doi:10.1016/j.actbio.2015.10.004
Lee, H. L., Yu, B., Deng, P., Wang, C. Y., and Hong, C. (2016). Transforming growth factor-β-induced KDM4B promotes chondrogenic differentiation of human mesenchymal stem cells. Stem Cells 34 (3), 711–719. doi:10.1002/stem.2231
Lee, J. S., Hong, J. M., Jung, J. W., Shim, J. H., Oh, J. H., and Cho, D. W. (2014). 3D printing of composite tissue with complex shape applied to ear regeneration. Biofabrication 6 (2), 024103. doi:10.1088/1758-5082/6/2/024103
Lee, S. J., Broda, C., Atala, A., and Yoo, J. J. (2011). Engineered cartilage covered ear implants for auricular cartilage reconstruction. Biomacromolecules 12 (2), 306–313. doi:10.1021/bm100856g
Lee, W. K., Ichi, T., Ooya, T., Yamamoto, T., Katoh, M., and Yui, N. (2003). Novel poly(ethylene glycol) scaffolds crosslinked by hydrolyzable polyrotaxane for cartilage tissue engineering. J. Biomed. Mater Res. A 67 (4), 1087–1092. doi:10.1002/jbm.a.10570
Leslie, S. K., Cohen, D. J., Hyzy, S. L., Dosier, C. R., Nicolini, A., Sedlaczek, J., et al. (2018). Microencapsulated rabbit adipose stem cells initiate tissue regeneration in a rabbit ear defect model. J. Tissue Eng. Regen. Med. 12 (7), 1742–1753. doi:10.1002/term.2702
Leslie, S. K., Cohen, D. J., Sedlaczek, J., Pinsker, E. J., Boyan, B. D., and Schwartz, Z. (2013). Controlled release of rat adipose-derived stem cells from alginate microbeads. Biomaterials 34 (33), 8172–8184. doi:10.1016/j.biomaterials.2013.07.017
Li, H., Liao, Z., Yang, Z., Gao, C., Li, P., Zhao, T., et al. (2021). 3D printed poly(ε-caprolactone)/meniscus extracellular matrix composite scaffold functionalized with kartogenin-releasing PLGA microspheres for meniscus tissue engineering. Front. Bioeng. Biotechnol. 9, 662381. doi:10.3389/fbioe.2021.662381
Li, W. J., Tuli, R., Okafor, C., Derfoul, A., Danielson, K. G., Hall, D. J., et al. (2005). A three-dimensional nanofibrous scaffold for cartilage tissue engineering using human mesenchymal stem cells. Biomaterials 26 (6), 599–609. doi:10.1016/j.biomaterials.2004.03.005
Li, Y., Liu, Y., and Guo, Q. (2021). Silk fibroin hydrogel scaffolds incorporated with chitosan nanoparticles repair articular cartilage defects by regulating TGF-β1 and BMP-2. Arthritis Res. Ther. 23 (1), 50. doi:10.1186/s13075-020-02382-x
Liu, K., Zhou, G. D., Liu, W., Zhang, W. J., Cui, L., Liu, X., et al. (2008). The dependence of in vivo stable ectopic chondrogenesis by human mesenchymal stem cells on chondrogenic differentiation in vitro. Biomaterials 29 (14), 2183–2192. doi:10.1016/j.biomaterials.2008.01.021
Liu, X., Sun, H., Yan, D., Zhang, L., Lv, X., Liu, T., et al. (2010). In vivo ectopic chondrogenesis of BMSCs directed by mature chondrocytes. Biomaterials 31 (36), 9406–9414. doi:10.1016/j.biomaterials.2010.08.052
Liu, Y., Zhang, L., Zhou, G., Li, Q., Liu, W., Yu, Z., et al. (2010). In vitro engineering of human ear-shaped cartilage assisted with CAD/CAM technology. Biomaterials 31 (8), 2176–2183. doi:10.1016/j.biomaterials.2009.11.080
Loo, Y., Lakshmanan, A., Ni, M., Toh, L. L., Wang, S., and Hauser, C. A. E. (2015). Peptide bioink: Self-assembling nanofibrous scaffolds for three-dimensional organotypic cultures. Nano Lett. 15 (10), 6919–6925. doi:10.1021/acs.nanolett.5b02859
Luquetti, D. V., Heike, C. L., Hing, A. V., Cunningham, M. L., and Cox, T. C. (2012). Microtia: Epidemiology and genetics. Am. J. Med. Genet. A 158A (1), 124–139. doi:10.1002/ajmg.a.34352
Lv, X., Zhou, G., Liu, X., Liu, H., Chen, J., Liu, K., et al. (2012). Chondrogenesis by co-culture of adipose-derived stromal cells and chondrocytes in vitro. Connect. Tissue Res. 53 (6), 492–497. doi:10.3109/03008207.2012.694926
Maldonado, M., and Nam, J. (2013). The role of changes in extracellular matrix of cartilage in the presence of inflammation on the pathology of osteoarthritis. Biomed. Res. Int. 2013, 1–10. doi:10.1155/2013/284873
Mannoor, M. S., Jiang, Z., James, T., Kong, Y. L., Malatesta, K. A., Soboyejo, W. O., et al. (2013). 3D printed bionic ears. Nano Lett. 13 (6), 2634–2639. doi:10.1021/nl4007744
Mara, C. S., Duarte, A. S., Sartori, A., Luzo, A. C., Saad, S. T., and Coimbra, I. B. (2010). Regulation of chondrogenesis by transforming growth factor-ß3 and insulin-like growth factor-1 from human mesenchymal umbilical cord blood cells. J. Rheumatol. 37 (7), 1519–1526. doi:10.3899/jrheum.091169
Melgarejo-Ramírez, Y., Sánchez-Sánchez, R., García-López, J., Brena-Molina, A. M., Gutiérrez-Gómez, C., Ibarra, C., et al. (2016). Characterization of pediatric microtia cartilage: A reservoir of chondrocytes for auricular reconstruction using tissue engineering strategies. Cell tissue Bank. 17 (3), 481–489. doi:10.1007/s10561-016-9574-5
Min, B. M., Lee, G., Kim, S. H., Nam, Y. S., Lee, T. S., and Park, W. H. (2004). Electrospinning of silk fibroin nanofibers and its effect on the adhesion and spreading of normal human keratinocytes and fibroblasts in vitro. Biomaterials 25 (7-8), 1289–1297. doi:10.1016/j.biomaterials.2003.08.045
Mo, X. T., Guo, S. c., Xie, H. q., Deng, L., Zhi, W., Xiang, Z., et al. (2009). Variations in the ratios of co-cultured mesenchymal stem cells and chondrocytes regulate the expression of cartilaginous and osseous phenotype in alginate constructs. Bone 45 (1), 42–51. doi:10.1016/j.bone.2008.07.240
Moretti, P., Hatlapatka, T., Marten, D., Lavrentieva, A., Majore, I., Hass, R., et al. (2010). Mesenchymal stromal cells derived from human umbilical cord tissues: Primitive cells with potential for clinical and tissue engineering applications. Adv. Biochem. Eng. Biotechnol. 123, 29–54. doi:10.1007/10_2009_15
Morrison, R. J., Nasser, H. B., Kashlan, K. N., Zopf, D. A., Milner, D. J., Flanangan, C. L., et al. (2018). Co-culture of adipose-derived stem cells and chondrocytes on three-dimensionally printed bioscaffolds for craniofacial cartilage engineering. Laryngoscope 128 (7), E251–e257. doi:10.1002/lary.27200
Mouser, V. H. M., Levato, R., Mensinga, A., Dhert, W. J. A., Gawlitta, D., and Malda, J. (2020). Bio-ink development for three-dimensional bioprinting of hetero-cellular cartilage constructs. Connect. Tissue Res. 61 (2), 137–151. doi:10.1080/03008207.2018.1553960
Munsell, E. V., Kurpad, D. S., Freeman, T. A., and Sullivan, M. O. (2018). Histone-targeted gene transfer of bone morphogenetic protein-2 enhances mesenchymal stem cell chondrogenic differentiation. Acta Biomater. 71, 156–167. doi:10.1016/j.actbio.2018.02.021
Nagata, S., and Edgerton, M. T. (1994). Secondary reconstruction for unfavorable microtia results utilizing temporoparietal and innominate fascia flaps. Plast. Reconstr. Surg. 94 (2), 266–267. doi:10.1097/00006534-199408000-00007
Nagata, S. (1994). Modification of the stages in total reconstruction of the auricle: Part I. Grafting the three-dimensional costal cartilage framework for lobule-type microtia. Plast. Reconstr. Surg. 93 (2), 221–230. doi:10.1097/00006534-199402000-00001
Nagata, S. (1994). Modification of the stages in total reconstruction of the auricle: Part II. Grafting the three-dimensional costal cartilage framework for concha-type microtia. Plast. Reconstr. Surg. 93 (2), 231–242. doi:10.1097/00006534-199402000-00002
Nakamura, A., Murata, D., Fujimoto, R., Tamaki, S., Nagata, S., Ikeya, M., et al. (2021). Bio-3D printing iPSC-derived human chondrocytes for articular cartilage regeneration. Biofabrication 13 (4), 044103. doi:10.1088/1758-5090/ac1c99
Nakao, H., Jacquet, R. D., Shasti, M., Isogai, N., Murthy, A. S., and Landis, W. J. (2017). Long-term comparison between human normal conchal and microtia chondrocytes regenerated by tissue engineering on nanofiber polyglycolic acid scaffolds. Plast. Reconstr. Surg. 139 (4), 911e–921e. doi:10.1097/prs.0000000000003201
Nishimoto, S., Sotsuka, Y., Kawai, K., Fujita, K., and Kakibuchi, M. (2014). Three-dimensional mock-up model for chondral framework in auricular reconstruction, built with a personal three-dimensional printer. Plastic Reconstr. Surg. 134 (1), 180e–181e. doi:10.1097/prs.0000000000000263
Olausson, M., Patil, P. B., Kuna, V. K., Chougule, P., Hernandez, N., Methe, K., et al. (2012). Transplantation of an allogeneic vein bioengineered with autologous stem cells: A proof-of-concept study. Lancet 380 (9838), 230–237. doi:10.1016/s0140-6736(12)60633-3
Otani, Y., Komura, M., Komura, H., Ishimaru, T., Konishi, K., Komuro, H., et al. (2015). Optimal amount of basic fibroblast growth factor in gelatin sponges incorporating β-tricalcium phosphate with chondrocytes. Tissue Eng. Part A 21 (3-4), 627–636. doi:10.1089/ten.tea.2013.0655
Otto, I. A., Bernal, P. N., Rikkers, M., van Rijen, M. H., Mensinga, A., Kon, M., et al. (2022). Human adult, pediatric and microtia auricular cartilage harbor fibronectin-adhering progenitor cells with regenerative ear reconstruction potential. iScience 25 (9), 104979. doi:10.1016/j.isci.2022.104979
Otto, I. A., Capendale, P., Garcia, J., de Ruijter, M., van Doremalen, R., Castilho, M., et al. (2021). Biofabrication of a shape-stable auricular structure for the reconstruction of ear deformities. Mater Today Bio 9, 100094. doi:10.1016/j.mtbio.2021.100094
Pabbruwe, M. B., Esfandiari, E., Kafienah, W., Tarlton, J. F., and Hollander, A. P. (2009). Induction of cartilage integration by a chondrocyte/collagen-scaffold implant. Biomaterials 30 (26), 4277–4286. doi:10.1016/j.biomaterials.2009.02.052
Park, C. (2000). Subfascial expansion and expanded two-flap method for microtia reconstruction. Plast. Reconstr. Surg. 106 (7), 1473–1487. doi:10.1097/00006534-200012000-00005
Patil, A. S., Sable, R. B., and Kothari, R. M. (2011). An update on transforming growth factor-β (TGF-β): Sources, types, functions and clinical applicability for cartilage/bone healing. J. Cell Physiol. 226 (12), 3094–3103. doi:10.1002/jcp.22698
Pearson, R. G., Bhandari, R., Quirk, R. A., and Shakesheff, K. M. (2017). Recent advances in tissue engineering. J. Long. Term. Eff. Med. Implants 27 (2-4), 199–231. doi:10.1615/jlongtermeffmedimplants.v27.i2-4.70
Pepelanova, I., Kruppa, K., Scheper, T., and Lavrentieva, A. (2018). Gelatin-Methacryloyl (GelMA) hydrogels with defined degree of functionalization as a versatile toolkit for 3D cell culture and extrusion bioprinting. Bioeng. (Basel) 5 (3), 55. doi:10.3390/bioengineering5030055
Phull, A. R., Eo, S. H., Abbas, Q., Ahmed, M., and Kim, S. J. (2016). Applications of chondrocyte-based cartilage engineering: An overview. Biomed. Res. Int. 2016, 1–17. doi:10.1155/2016/1879837
Ponticiello, M. S., Schinagl, R. M., Kadiyala, S., and Barry, F. P. (2000). Gelatin-based resorbable sponge as a carrier matrix for human mesenchymal stem cells in cartilage regeneration therapy. J. Biomed. Mater Res. 52 (2), 246–255. doi:10.1002/1097-4636(200011)52:2<246::aid-jbm2>3.0.co;2-w
Rastogi, P., and Kandasubramanian, B. (2019). Review of alginate-based hydrogel bioprinting for application in tissue engineering. Biofabrication 11 (4), 042001. doi:10.1088/1758-5090/ab331e
Rim, Y. A., Nam, Y., Park, N., Lee, J., Park, S. h., and Ju, J. H. (2018). Repair potential of nonsurgically delivered induced pluripotent stem cell-derived chondrocytes in a rat osteochondral defect model. J. Tissue Eng. Regen. Med. 12 (8), 1843–1855. doi:10.1002/term.2705
Romo, T., Presti, P. M., and Yalamanchili, H. R. (2006). Medpor alternative for microtia repair. Facial Plast. Surg. Clin. North Am. 14 (2), 129–136. doi:10.1016/j.fsc.2006.01.006
Rosa, R. G., Joazeiro, P. P., Bianco, J., Kunz, M., Weber, J. F., and Waldman, S. D. (2014). Growth factor stimulation improves the structure and properties of scaffold-free engineered auricular cartilage constructs. PLoS One 9 (8), e105170. doi:10.1371/journal.pone.0105170
Rosadi, I., Karina, K., Rosliana, I., Sobariah, S., Afini, I., Widyastuti, T., et al. (2019). In vitro study of cartilage tissue engineering using human adipose-derived stem cells induced by platelet-rich plasma and cultured on silk fibroin scaffold. Stem cell Res. Ther. 10 (1), 369. doi:10.1186/s13287-019-1443-2
Rosenzweig, D. H., Carelli, E., Steffen, T., Jarzem, P., and Haglund, L. (2015). 3D-Printed ABS and PLA scaffolds for cartilage and nucleus pulposus tissue regeneration. Int. J. Mol. Sci. 16 (7), 15118–15135. doi:10.3390/ijms160715118
Saim, A. B., Cao, Y., Weng, Y., Chang, C. N., Vacanti, M. A., Vacanti, C. A., et al. (2000). Engineering autogenous cartilage in the shape of a helix using an injectable hydrogel scaffold. Laryngoscope 110 (10), 1694–1697. doi:10.1097/00005537-200010000-00023
Salehi, S., Koeck, K., and Scheibel, T. (2020). Spider silk for tissue engineering applications. Molecules 25 (3), 737. doi:10.3390/molecules25030737
Sennett, M. L., Meloni, G. R., Farran, A. J. E., Guehring, H., Mauck, R. L., and Dodge, G. R. (2018). Sprifermin treatment enhances cartilage integration in an in vitro repair model. J. Orthop. Res. 36 (10), 2648–2656. doi:10.1002/jor.24048
Seol, D., McCabe, D. J., Choe, H., Zheng, H., Yu, Y., Jang, K., et al. (2012). Chondrogenic progenitor cells respond to cartilage injury. Arthritis Rheum. 64 (11), 3626–3637. doi:10.1002/art.34613
Shi, J., Liang, J., Guo, B., Zhang, Y., Hui, Q., Chang, P., et al. (2017). Adipose-derived stem cells cocultured with chondrocytes promote the proliferation of chondrocytes. Stem Cells Int. 2017, 1–17. doi:10.1155/2017/1709582
Shieh, S., Terada, S., and Vacanti, J. (2004). Tissue engineering auricular reconstruction: In vitro and in vivo studies. Biomaterials 25 (9), 1545–1557. doi:10.1016/s0142-9612(03)00501-5
Siegert, R. (2003). Combined reconstruction of congenital auricular atresia and severe microtia. Laryngoscope 113 (11), 2021–2027. ; discussion 2028-9. doi:10.1097/00005537-200311000-00031
Silverman, R. P., Passaretti, D., Huang, W., Randolph, M. A., and Yaremchuk, M. J. (1999). Injectable tissue-engineered cartilage using a fibrin glue polymer. Plast. Reconstr. Surg. 103 (7), 1809–1818. doi:10.1097/00006534-199906000-00001
Takahashi, K., and Yamanaka, S. (2006). Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell 126 (4), 663–676. doi:10.1016/j.cell.2006.07.024
Tang, P., Song, P., Peng, Z., Zhang, B., Gui, X., Wang, Y., et al. (2021). Chondrocyte-laden GelMA hydrogel combined with 3D printed PLA scaffolds for auricle regeneration. Mater Sci. Eng. C Mater Biol. Appl. 130, 112423. doi:10.1016/j.msec.2021.112423
Tanzer, R. C. (1978). Microtia--a long-term follow-up of 44 reconstructed auricles. Plast. Reconstr. Surg. 61 (2), 161–166. doi:10.1097/00006534-197802000-00001
Tanzer, R. C. (1967). Total reconstruction of the auricle: A 10-year report. Plast. Reconstr. Surg. 40 (6), 547–550. doi:10.1097/00006534-196740060-00006
Tanzer, R. C. (1959). Total reconstruction of the external ear. Plast. Reconstr. Surg. Transpl. Bull. 23 (1), 1–15. doi:10.1097/00006534-195901000-00001
Tay, A., Farhadi, J., Suetterlin, R., Pierer, G., Heberer, M., and Martin, I. (2004). Cell yield, proliferation, and postexpansion differentiation capacity of human ear, nasal, and rib chondrocytes. Tissue Eng. 10, 762–770. doi:10.1089/1076327041348572
Unagolla, J. M., and Jayasuriya, A. C. (2020). Hydrogel-based 3D bioprinting: A comprehensive review on cell-laden hydrogels, bioink formulations, and future perspectives. Appl. Mater Today 18, 100479. doi:10.1016/j.apmt.2019.100479
Urlić, I., and Ivković, A. (2021). Cell sources for cartilage repair-biological and clinical perspective. Cells 10 (9), 2496. doi:10.3390/cells10092496
Veilleux, N., and Spector, M. (2005). Effects of FGF-2 and IGF-1 on adult canine articular chondrocytes in type II collagen-glycosaminoglycan scaffolds in vitro. Osteoarthr. Cartil. 13 (4), 278–286. doi:10.1016/j.joca.2004.12.013
Vinatier, C., Mrugala, D., Jorgensen, C., Guicheux, J., and Noël, D. (2009). Cartilage engineering: A crucial combination of cells, biomaterials and biofactors. Trends Biotechnol. 27 (5), 307–314. doi:10.1016/j.tibtech.2009.02.005
Visscher, D. O., Gleadall, A., Buskermolen, J. K., Burla, F., Segal, J., Koenderink, G. H., et al. (2019). Design and fabrication of a hybrid alginate hydrogel/poly(ε-caprolactone) mold for auricular cartilage reconstruction. J. Biomed. Mater Res. B Appl. Biomater. 107 (5), 1711–1721. doi:10.1002/jbm.b.34264
Wang, H., Wang, Z., Liu, H., Liu, J., Li, R., Zhu, X., et al. (2021). Three-dimensional printing strategies for irregularly shaped cartilage tissue engineering: Current state and challenges. Front. Bioeng. Biotechnol. 9, 777039. doi:10.3389/fbioe.2021.777039
Wang, H., Yu, H., Zhou, X., Zhang, J., Zhou, H., Hao, H., et al. (2022). An overview of extracellular matrix-based bioinks for 3D bioprinting. Front. Bioeng. Biotechnol. 10, 905438. doi:10.3389/fbioe.2022.905438
Wang, K., Li, J., Li, Z., Wang, B., Qin, Y., Zhang, N., et al. (2019). Chondrogenic progenitor cells exhibit superiority over mesenchymal stem cells and chondrocytes in platelet-rich plasma scaffold-based cartilage regeneration. Am. J. Sports Med. 47 (9), 2200–2215. doi:10.1177/0363546519854219
Wei, P., Xu, Y., Gu, Y., Yao, Q., Li, J., and Wang, L. (2020). IGF-1-releasing PLGA nanoparticles modified 3D printed PCL scaffolds for cartilage tissue engineering. Drug Deliv. 27 (1), 1106–1114. doi:10.1080/10717544.2020.1797239
Whitney, G., Jayaraman, K., Dennis, J. E., and Mansour, J. M. (2017). Scaffold-free cartilage subjected to frictional shear stress demonstrates damage by cracking and surface peeling. J. tissue Eng. Regen. Med. 11 (2), 412–424. doi:10.1002/term.1925
Wilkes, G. H., Wong, J., and Guilfoyle, R. (2014). Microtia reconstruction. Plast. Reconstr. Surg. 134 (3), 464e–479e. doi:10.1097/prs.0000000000000526
Woodfield, T. B., Malda, J., de Wijn, J., Péters, F., Riesle, J., and van Blitterswijk, C. (2004). Design of porous scaffolds for cartilage tissue engineering using a three-dimensional fiber-deposition technique. Biomaterials 25 (18), 4149–4161. doi:10.1016/j.biomaterials.2003.10.056
Wu, D., Munguia-Lopez, J. G., Cho, Y. W., Ma, X., Song, V., Zhu, Z., et al. (2021). Polymeric scaffolds for dental, oral, and craniofacial regenerative medicine. Mol. (Basel, Switz. 26 (22), 7043. doi:10.3390/molecules26227043
Wu, L., Zhang, H., Zhang, J., and Ding, J. (2005). Fabrication of three-dimensional porous scaffolds of complicated shape for tissue engineering. I. Compression molding based on flexible-rigid combined mold. Tissue Eng. 11 (7-8), 1105–1114. doi:10.1089/ten.2005.11.1105
Xie, X., Wang, Y., Zhao, C., Guo, S., Liu, S., Jia, W., et al. (2012). Comparative evaluation of MSCs from bone marrow and adipose tissue seeded in PRP-derived scaffold for cartilage regeneration. Biomaterials 33 (29), 7008–7018. doi:10.1016/j.biomaterials.2012.06.058
Xie, X., Wu, S., Mou, S., Guo, N., Wang, Z., and Sun, J. (2022). Microtissue-based bioink as a chondrocyte microshelter for DLP bioprinting. Adv. Healthc. Mater 11, e2201877. doi:10.1002/adhm.202201877
Xu, J. W., Johnson, T. S., Motarjem, P. M., Peretti, G. M., Randolph, M. A., and Yaremchuk, M. J. (2005). Tissue-engineered flexible ear-shaped cartilage. Plast. Reconstr. Surg. 115 (6), 1633–1641. doi:10.1097/01.prs.0000161465.21513.5d
Xu, Y., Peng, J., Richards, G., Lu, S., and Eglin, D. (2019). Optimization of electrospray fabrication of stem cell-embedded alginate-gelatin microspheres and their assembly in 3D-printed poly(ε-caprolactone) scaffold for cartilage tissue engineering. J. Orthop. Transl. 18, 128–141. doi:10.1016/j.jot.2019.05.003
Xu, Y., Xu, Y., Bi, B., Hou, M., Yao, L., Du, Q., et al. (2020). A moldable thermosensitive hydroxypropyl chitin hydrogel for 3D cartilage regeneration in vitro and in vivo. Acta Biomater. 108, 87–96. doi:10.1016/j.actbio.2020.03.039
Xue, K., Zhu, Y., Zhang, Y., Chiang, C., Zhou, G., and Liu, K. (2012). Xenogeneic chondrocytes promote stable subcutaneous chondrogenesis of bone marrow-derived stromal cells. Int. J. Mol. Med. 29 (2), 146–152. doi:10.3892/ijmm.2011.830
Yamashita, A., Tamamura, Y., Morioka, M., Karagiannis, P., Shima, N., and Tsumaki, N. (2018). Considerations in hiPSC-derived cartilage for articular cartilage repair. Inflamm. Regen. 38, 17. doi:10.1186/s41232-018-0075-8
Yang, D., Xiao, J., Wang, B., Li, L., Kong, X., and Liao, J. (2019). The immune reaction and degradation fate of scaffold in cartilage/bone tissue engineering. Mater Sci. Eng. C Mater Biol. Appl. 104, 109927. doi:10.1016/j.msec.2019.109927
Yang, W. D., Chen, S. J., Mao, T. Q., Chen, F. L., Lei, D. L., Tao, K., et al. (2000). A study of injectable tissue-engineered autologous cartilage. Chin. J. Dent. Res. 3 (4), 10–15.
Yetman, R., and Hormann, M. (2015). Pediatrics PreTest self-assessment and review. Thirteenth Edition. New York, NY: McGraw hill book company.
Yue, H., Pathak, J. L., Zou, R., Qin, L., Liao, T., Hu, Y., et al. (2021). Fabrication of chondrocytes/chondrocyte-microtissues laden fibrin gel auricular scaffold for microtia reconstruction. J. Biomater. Appl. 35 (7), 838–848. doi:10.1177/0885328220954415
Yue, K., Trujillo-de Santiago, G., Alvarez, M. M., Tamayol, A., Annabi, N., and Khademhosseini, A. (2015). Synthesis, properties, and biomedical applications of gelatin methacryloyl (GelMA) hydrogels. Biomaterials 73, 254–271. doi:10.1016/j.biomaterials.2015.08.045
Zaim, M., Karaman, S., Cetin, G., and Isik, S. (2012). Donor age and long-term culture affect differentiation and proliferation of human bone marrow mesenchymal stem cells. Ann. Hematol. 91 (8), 1175–1186. doi:10.1007/s00277-012-1438-x
Zhang, B., Zeng, X., and Yang, X. (2019). Clinical applications of ear reconstruction with Medpor. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 44 (5), 562–570. doi:10.11817/j.issn.1672-7347.2019.05.014
Zhang, L., He, A., Yin, Z., Yu, Z., Luo, X., Liu, W., et al. (2014). Regeneration of human-ear-shaped cartilage by co-culturing human microtia chondrocytes with BMSCs. Biomaterials 35 (18), 4878–4887. doi:10.1016/j.biomaterials.2014.02.043
Zhang, T. Y., Bulstrode, N., Chang, K. W., Cho, Y. S., Frenzel, H., Jiang, D., et al. (2019). International consensus recommendations on microtia, aural atresia and functional ear reconstruction. J. Int. Adv. Otol. 15 (2), 204–208. doi:10.5152/iao.2019.7383
Zhang, W., Ouyang, H., Dass, C. R., and Xu, J. (2016). Current research on pharmacologic and regenerative therapies for osteoarthritis. Bone Res. 4, 15040. doi:10.1038/boneres.2015.40
Zhou, G. D., Wang, X. Y., Miao, C. L., Liu, T. Y., Zhu, L., Liu, D. L., et al. (2004). Repairing porcine knee joint osteochondral defects at non-weight bearing area by autologous BMSC. Zhonghua Yi Xue Za Zhi 84 (11), 925–931.
Zhou, G., Jiang, H., Yin, Z., Liu, Y., Zhang, Q., Zhang, C., et al. (2018). In vitro regeneration of patient-specific ear-shaped cartilage and its first clinical application for auricular reconstruction. EBioMedicine 28, 287–302. doi:10.1016/j.ebiom.2018.01.011
Zhou, G., Liu, W., Cui, L., Wang, X., Liu, T., and Cao, Y. (2006). Repair of porcine articular osteochondral defects in non-weightbearing areas with autologous bone marrow stromal cells. Tissue Eng. 12 (11), 061017080728006–061017080728021. doi:10.1089/ten.2006.12.ft-256
Zhu, Y., Wu, X., Liang, Y., Gu, H., Song, K., Zou, X., et al. (2016). Repair of cartilage defects in osteoarthritis rats with induced pluripotent stem cell derived chondrocytes. BMC Biotechnol. 16 (1), 78. doi:10.1186/s12896-016-0306-5
Zopf, D. A., Flanagan, C. L., Mitsak, A. G., Brennan, J. R., and Hollister, S. J. (2018). Pore architecture effects on chondrogenic potential of patient-specific 3-dimensionally printed porous tissue bioscaffolds for auricular tissue engineering. Int. J. Pediatr. Otorhinolaryngol. 114, 170–174. doi:10.1016/j.ijporl.2018.07.033
Keywords: microtia, auricular reconstruction, tissue engineering, biomaterial scaffold, 3D printing
Citation: Huang Y, Zhao H, Wang Y, Bi S, Zhou K, Li H, Zhou C, Wang Y, Wu W, Peng B, Tang J, Pan B, Wang B, Chen Z, Li Z and Zhang Z (2023) The application and progress of tissue engineering and biomaterial scaffolds for total auricular reconstruction in microtia. Front. Bioeng. Biotechnol. 11:1089031. doi: 10.3389/fbioe.2023.1089031
Received: 04 November 2022; Accepted: 21 April 2023;
Published: 22 September 2023.
Edited by:
Pablo Taboada, University of Santiago de Compostela, SpainReviewed by:
Cristina Velasquillo, National Institute of Rehabilitation Luis Guillermo Ibarra, Ibarra, MexicoCopyright © 2023 Huang, Zhao, Wang, Bi, Zhou, Li, Zhou, Wang, Wu, Peng, Tang, Pan, Wang, Chen, Li and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhengyong Li, bGl6eWRkQHNpbmEuY29t; Zhenyu Zhang, emhhbmd6aGVueXVAc2N1LmVkdS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.