 Tecla Bonci1*
Tecla Bonci1* Francesca Salis2
Francesca Salis2 Kirsty Scott1
Kirsty Scott1 Lisa Alcock3
Lisa Alcock3 Clemens Becker4Stefano Bertuletti2Ellen Buckley1
Clemens Becker4Stefano Bertuletti2Ellen Buckley1 Marco Caruso5Andrea Cereatti5Silvia Del Din3
Marco Caruso5Andrea Cereatti5Silvia Del Din3 Eran Gazit6
Eran Gazit6 Clint Hansen7
Clint Hansen7 Jeffrey M. Hausdorff6,8,9
Jeffrey M. Hausdorff6,8,9 Walter Maetzler7
Walter Maetzler7 Luca Palmerini10,11Lynn Rochester3,12
Luca Palmerini10,11Lynn Rochester3,12 Lars Schwickert4
Lars Schwickert4 Basil Sharrack13
Basil Sharrack13 Ioannis Vogiatzis14
Ioannis Vogiatzis14 Claudia Mazzà1on behalf of the Mobilise-D consortium
Claudia Mazzà1on behalf of the Mobilise-D consortium- 1Department of Mechanical Engineering, Insigno Institute for In Silico Medicine, The University of Sheffield, Sheffield, United Kingdom
- 2Department of Biomedical Sciences, University of Sassari, Sassari, Italy
- 3Translational and Clinical Research Institute, Faculty of Medical Sciences, Newcastle University, Newcastle Upon Tyne, United Kingdom
- 4Department for Geriatric Rehabilitation, Robert-Bosch-Hospital, Stuttgart, Germany
- 5Department of Electronics and Telecommunications, Politecnico Di Torino, Torino, Italy
- 6Centre for the Study of Movement, Cognition and Mobility, Tel Aviv Sourasky Medical Centre, Tel Aviv, Israel
- 7Department of Neurology, University Hospital Schleswig-Holstein, Campus Kiel, Kiel University, Kiel, Germany
- 8Department of Physical Therapy, Sackler Faculty of Medicine, Sagol School of Neuroscience, Tel Aviv University, Tel Aviv, Israel
- 9Department of Orthopaedic Surgery, Rush Alzheimer’s Disease Center, Rush University Medical Center, Chicago, IL, United States
- 10Department of Electrical, Electronic, and Information Engineering “Guglielmo Marconi”, University of Bologna, Bologna, Italy
- 11Health Sciences and Technologies–Interdepartmental Center for Industrial Research (CIRI-SDV), University of Bologna, Bologna, Italy
- 12The Newcastle Upon Tyne Hospitals NHS Foundation Trust, Newcastle Upon Tyne, United Kingdom
- 13Department of Neuroscience, Sheffield NIHR Translational Neuroscience BRC, Sheffield Teaching Hospitals NHS Foundation Trust, Sheffield, United Kingdom
- 14Department of Sport, Exercise and Rehabilitation, Northumbria University, Newcastle Upon Tyne, United Kingdom
There is growing interest in the quantification of gait as part of complex motor tasks. This requires gait events (GEs) to be detected under conditions different from straight walking. This study aimed to propose and validate a new marker-based GE detection method, which is also suitable for curvilinear walking and step negotiation. The method was first tested against existing algorithms using data from healthy young adults (YA, n = 20) and then assessed in data from 10 individuals from the following five cohorts: older adults, chronic obstructive pulmonary disease, multiple sclerosis, Parkinson’s disease, and proximal femur fracture. The propagation of the errors associated with GE detection on the calculation of stride length, duration, speed, and stance/swing durations was investigated. All participants performed a variety of motor tasks including curvilinear walking and step negotiation, while reference GEs were identified using a validated methodology exploiting pressure insole signals. Sensitivity, positive predictive values (PPV), F1-score, bias, precision, and accuracy were calculated. Absolute agreement [intraclass correlation coefficient (
Introduction
An individual’s ability to walk is usually quantified using spatio-temporal parameters (Perry and Davids, 2010; Preiningerova et al., 2015). Quantifying these parameters depends on the accurate identification of foot-to-ground events, namely, the initial (IC) and final (FC) contacts. Clinical gait analysis is traditionally performed during straight steady-state walking (
Foot-to-ground contacts can be accurately identified in laboratory settings using force platforms, which directly measure the exchanged forces (Bruening and Ridge, 2014; Lempereur et al., 2020), providing gold-standard temporal gait parameters. However, the number of consecutive gait events (GEs) is limited by the number of force platforms, their positioning, and by the correct foot positioning on them. This issue can be overcome when using foot switches or pressure insoles (PIs). When used as a standalone technology, none of the aforementioned tools, however, allow the direct quantification of spatial gait parameters, such as stride length or speed. Instrumented mats (e.g., GAITRite™, ProtoKinetics Zeno™, or Strideway™) can provide both spatial and temporal parameters (Van Uden and Besser, 2004), but only allow the analysis of straight walking and are not readily amenable to the use of walking aids. Moreover, the analysis is still restricted by their dimensions, and combining different mats can be very costly. Therefore, although still limited to a confined capture volume, the most suitable instruments for measurements of unconstrained gait spatio-temporal parameters during complex motor tasks in a laboratory setting are still marker-based stereophotogrammetric (SP) systems.
Optoelectronic stereophotogrammetry allows the tracking of the 3D position of retroreflective markers with high accuracy (<0.1 mm) and at a high sample rate (>100 Hz). GE identification from SP data can be obtained either manually or automatically. Previously proposed automatic GE detection algorithms, either based on peaks (Ghoussayni et al., 2004; Hsue et al., 2007; O’Connor et al., 2007; Zeni et al., 2008; Desailly et al., 2009), zero-crossing detection (Hreljac and Marshall, 2000), or machine learning (Filtjens et al., 2020; Lempereur et al., 2020) approaches, have been extensively tested on straight-line walking. Ulrich et al. (2019) recently tested some marker-based algorithms during turning, but only used a single force platform in different portions of a turn, which prevented the assessment of the complete turning maneuver and constrained turning location. To the authors’ knowledge, none of the marker-based methods have been tested across a variety of mobility tasks including potential confounding factors such as negotiating a step, turning, and sitting on a chair. Therefore, the aim of this study was to propose and validate a method for GE detection in rectilinear and curvilinear walking, and in step negotiation. The method’s performance was initially tested against existing methods using data from young healthy adults (YA). Its generalizability was then demonstrated using data from five cohorts, characterized by different gait patterns: healthy older adults (OA), patients with chronic obstructive pulmonary disease (COPD), multiple sclerosis (MS), Parkinson’s disease (PD), and proximal femur fracture (PFF). Finally, the propagation of temporal inaccuracies in GE detection on the quantification of spatio-temporal stride parameters was assessed.
Materials and Methods
Gait Event Detection Methods
Ten methods for marker-based GE identification were evaluated in this study (Table 1). Among these, six methods, using either marker-trajectory positions (M1 and M2), velocities (M3 and M4), or accelerations (M8 and M9), were implemented as described in the literature (Hreljac and Marshall, 2000; Ghoussayni et al., 2004; Hsue et al., 2007; O’Connor et al., 2007; Zeni et al., 2008; Desailly et al., 2009). The main features of these methods, all using heel and toe markers (Figure 1), are summarized in Table 1. All methods except for M3 (O’Connor et al., 2007) used the anterior–posterior (AP) components of displacements, velocities, or accelerations. To this purpose, a reference system was identified in each frame (Cappozzo et al., 2005) using markers from a rigid cluster attached to the pelvis (Figure 1) and foot marker displacements, velocities, or accelerations were calculated along the three identified directions (anterior–posterior, AP; medio–lateral, ML; and vertical, V; Figure 1). Marker trajectories were filtered using a zero-lag fourth order Butterworth filter (cut-off frequency 7 Hz).
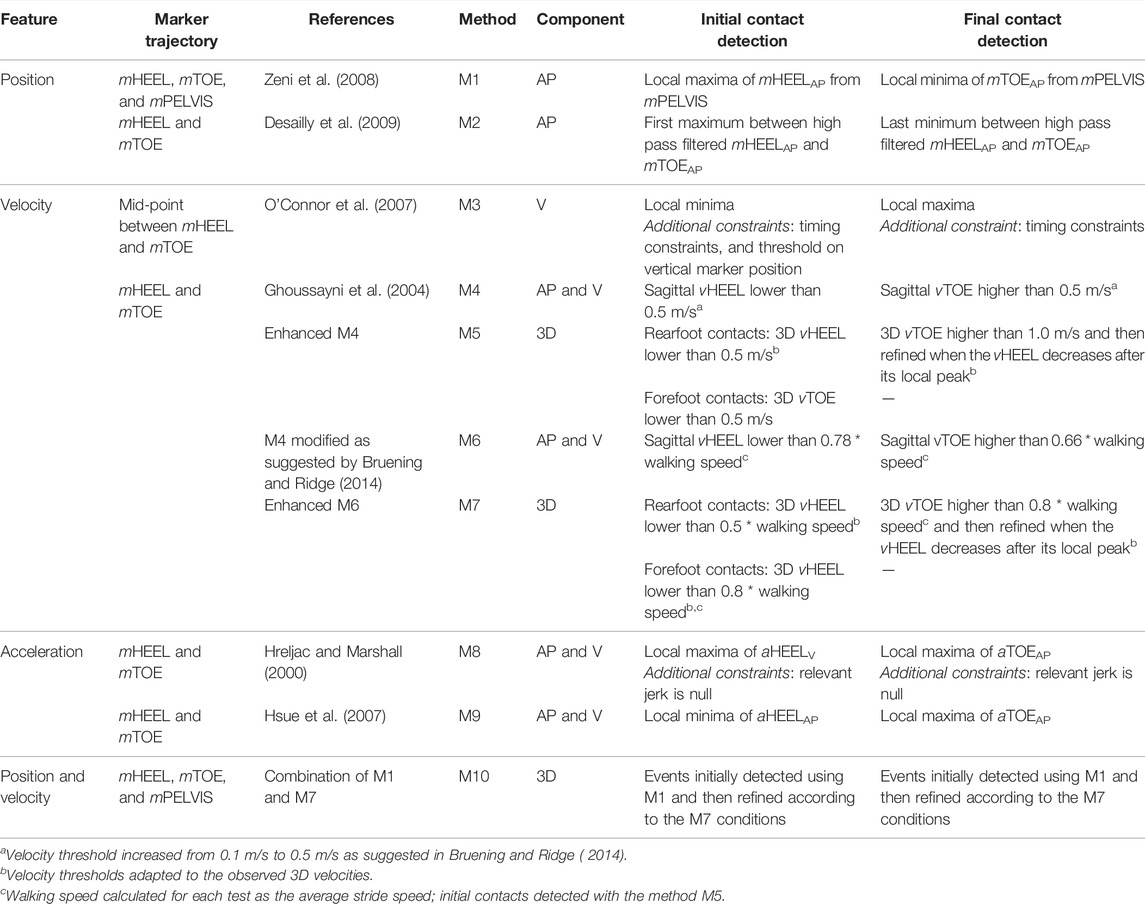
TABLE 1. Outline of the gait event identification methods adopted in this study.
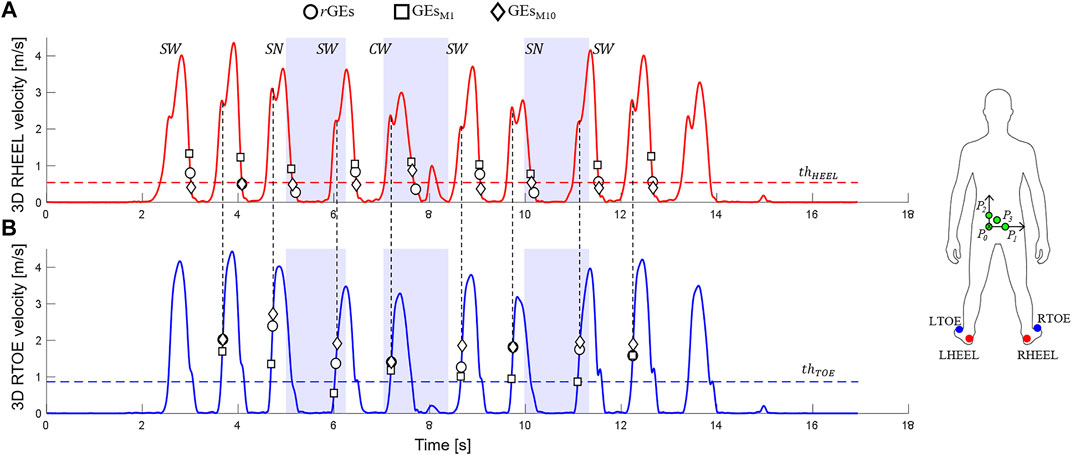
FIGURE 1. 3D heel [in red, (A)] and toe [in blue, (B)] marker velocities (data from one participant performing a Hallway test, 2.3 section) are shown. Relevant ground-truth (circles, rGEs) and marker-based GEs (squares for the M1 method, GEsM1; diamonds for the M10 method, GEsM10) are indicated together with the adopted thresholds (
A modified version of M4, M6, was also implemented using an adaptive velocity threshold (Bruening and Ridge, 2014). The use of 3D rather than the marker velocity in the sagittal plane (AP-V plane) was also explored. In particular, candidate IC instances of time (
1) If
2) If
For the FC detection (Figure 1), a threshold [fixed = 1.0 m/s (M5) or adaptive = 0.8*walking speed (M7)] was initially set on the 3D toe velocity. The instant (
A further new method, M10, was defined: estimations of both IC and FC were initially provided by M1, to reduce potential false positives exploiting the existence of markers on the pelvis, and then refined using the relevant events detected using M7. If the pelvic markers were occluded, the events were directly detected using M7.
Curvilinear walking (
Participants
A cohort of 20 YAs (Table 2) was recruited across two centers (University of Sheffield and University of Sassari) for the concurrent evaluation of the ten GE identification methods. All participants signed a consent form before taking part in the investigation (University of Sheffield Research Ethics Committee, Application number 029143).
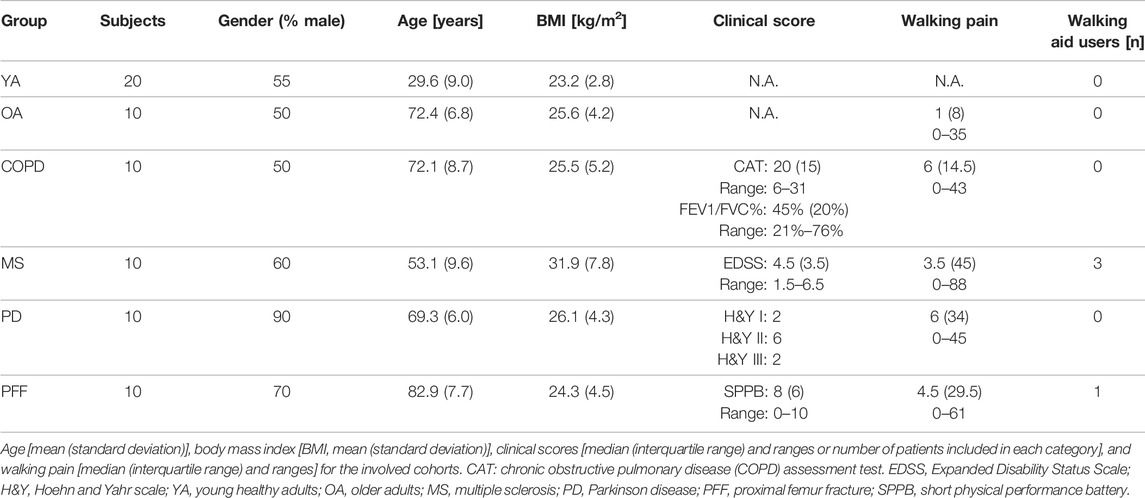
TABLE 2. Demographic and clinical characteristics of the study participants.
The generalizability of the results was then evaluated using a subset of the data from a multicentric study (Mobilise-D Technical Validation Study, Mazzà et al. [2021]), including 10 OAs, and 10 participants from the following four cohorts: COPD, MS, PD, and PFF. Participants (demographic and clinical characteristics shown in Table 2) were recruited from five centers and included in the study after providing written informed consent (Ethics approvals: Tel Aviv Sourasky Medical Center: the Helsinki Committee, 0551-19TLV; Robert Bosch Foundation for Medical Research: Medical Faculty of the University of Tübingen, 647/2019BO2; University of Kiel: Medical Faculty of Kiel University, D540/19; The Newcastle upon Tyne Hospitals NHS Foundation Trust and Sheffield Teaching Hospitals NHS Foundation Trust: London–Bloomsbury Research Ethics committee, 19/LO/1507). The adopted inclusion and exclusion criteria are detailed in Mazzà et al. (2021).
Experimental Protocol
Reflective markers were attached bilaterally to participants’ shoes, in correspondence of the posterior side of calcaneus (HEEL) and of the second metatarsal head (TOE). Four markers were attached on the pelvis using a rigid cluster (Figure 1). The marker trajectories were acquired using different SP systems (8-camera Vicon T10, 10-camera Vicon T160, 12-camera Qualisys Miqus, 12-camera Vicon Vero, and 14-camera Vicon Bonita). Before data collection, a spot-check was performed to quantify the accuracy of the different SP systems, following the works of Scott et al. (2021). Pre-processing procedures were standardized with an ad-hoc pipeline, where foot trajectories were gap-filled only for gaps lower than 0.5 s (10.15131/shef.data.19115450). Participants were also equipped with a multi-sensing wearable system including two PIs, synchronized with the SP using a hardware-based solution (sampling frequency 100 Hz, Salis et al. [2021]).
Participants were asked to perform five structured mobility tasks (Mazzà et al., 2021):
• Straight-line walking: walk for 5 m at three self-selected speeds (slow, comfortable, and fast, twice each)
• Timed Up and Go: stand-up from a chair, walk for 3 m, turn around (U-turn, ∼ 180°), walk back to the chair, and sit down
• L-Test: stand-up from a chair, walk for 4 m, turn 90° to the left, walk for 2 m, U-turn to the left (∼180°), walk back, turn 90° to the right, walk 2 m back to the chair, and sit down
• Surface test: walk twice in a loop (∼4 m rectilinear, and four ∼180° U-turns), with different surfaces along the path
• Hallway test: walk 6 m, stepping up and down a step, turn 180° turn, and walk back (again negotiating the step)
Data Processing and Statistical Analysis
The PI signals were used to isolate the different walking bouts [defined as comprising of at least two right and two left strides (Kluge et al., 2021)] and all reference GEs (rGEs) were identified according to the methodology proposed and validated by Salis et al. (2021).
The ten GE methods were compared using the YA data and the following performance criteria:
• Sensitivity (S), positive predictive values (PPV), and F1 values: for each rGE, a marker-based GE was classified as a true positive (TP), false negative (FN), or false positive (FP) using a tolerance window (TW) of 0.5 s centered on rGE.
where
• Accuracy, bias, and precision: for each identified TP, the relevant time error of a method
Reference stride, stance, and swing phase durations were quantified using the rGEs, and foot marker trajectories were used to calculate the reference length and speed during these time intervals. The impact of the GE detection inaccuracies on all other parameters was then assessed for each method and condition. The errors were computed only for the strides identified by TP ICs, with the remaining strides counted as missing. TP strides were further labeled as curvilinear or step negotiation strides if they had at least one IC belonging to either
The aforementioned analyses allowed the method that best satisfied the GE performance criteria to be chosen. Its generalizability was then established by applying it to the data from the five different cohorts and repeating all the aforementioned analyses, both at the event level and stride level.
Kolmogorov–Smirnov tests were used to assess the normality of the error distributions for the
For all cohorts, Bland–Altman (BA) plots (Martin Bland and Altman, 1986) were used to visually compare the marker-based parameters and check for nonlinear or heteroscedastic distributions of the differences between them. Absolute agreements were tested using intraclass correlation coefficients (
Results
Selection of the Best Gait Event Detection Method
Overall, 4,476 GEs (2,427 ICs) were detected with the PIs for the YA cohort, of which 2,876 were in
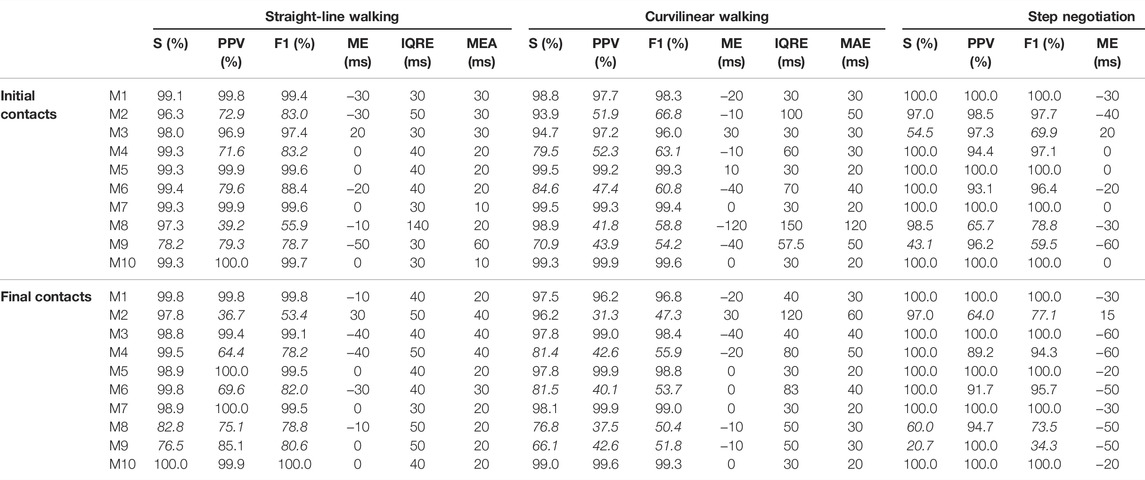
TABLE 3. Performances of the 10 methods (M1 … M10) in detecting both initial and final contacts in the young healthy adult cohort in straight-line walking (
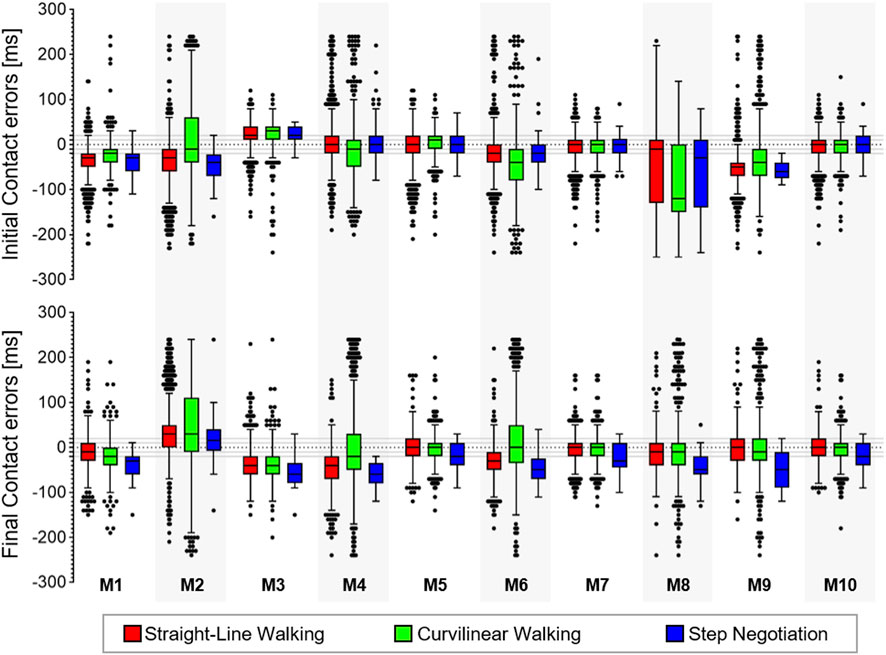
FIGURE 2. Box-plots (minimum, lower quartile, median, upper quartile, and maximum) of the error (ms) for the true positive (TP) initial and final contacts from the 10 methods (M1, … , M10) in the young healthy adult cohort in the three walking conditions. Outliers are also shown.
For each walking condition
Propagation of Gait Event Inaccuracies on the Estimate of the Stride Level Parameters
Overall, 1,000, 981, and 89 strides were detected for the YA cohort in
Accuracy of M10 in Pathological Gait
Overall, 2,514 (1,337 ICs) gait events were detected for the OA cohort, 3,172 (1,681 ICs) for the COPD, 3,548 (1,879 ICs) for the MS, 2,766 (1,468 ICs) for the PD, and 3,042 (1,609 ICs) for the PFF cohorts. Figure 3 shows the sensitivity, PPV, F1 scores, and performance metrics for M10 in the three walking conditions. The IC events identified within four frames (40 ms) ranged between 65% (
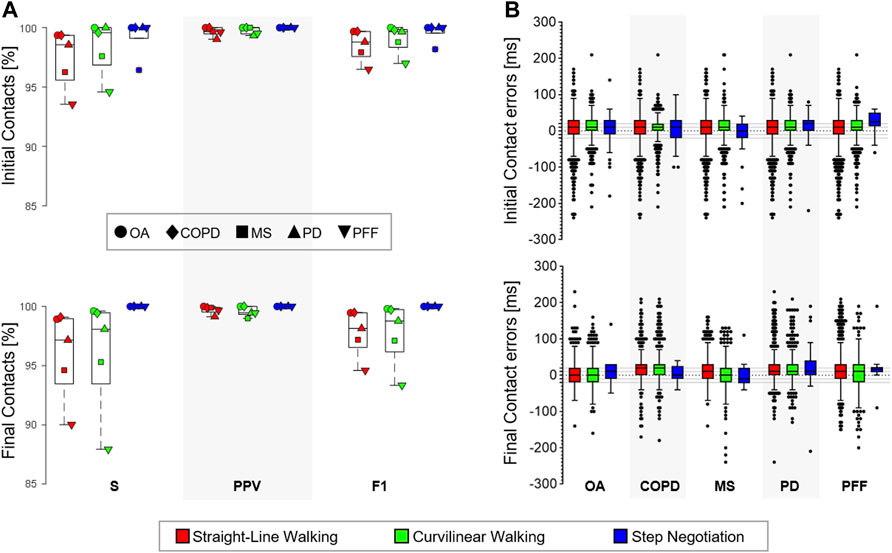
FIGURE 3. (A) Sensitivity (
The overall detected strides were 1,174 in the OA (39% in
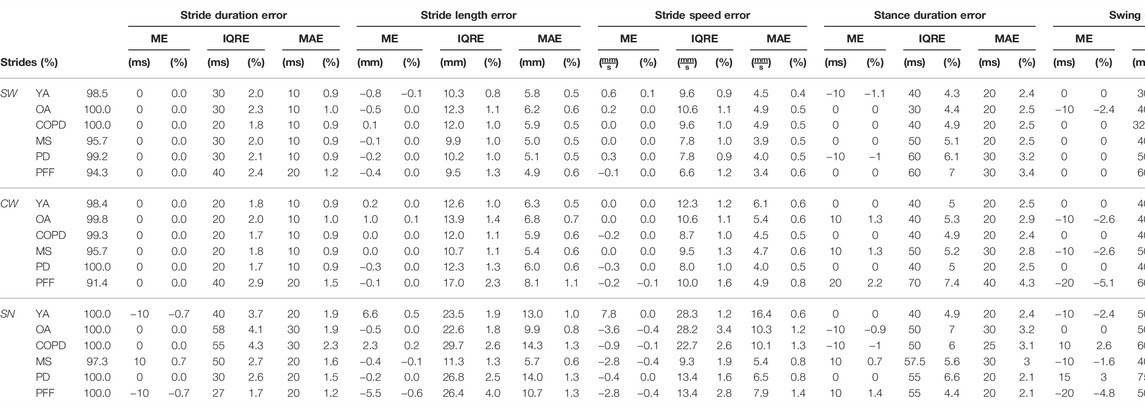
TABLE 4. Correctly detected strides (%) for each cohort (young adults (YA), older adults (OA), multiple sclerosis (MS), Parkinson disease (PD), chronic obstructive pulmonary disease (COPD); and proximal femur fracture (PFF) and walking conditions (straight-line walking,
In light of the spatial resolutions assessed for each cohort, virtually null errors in the stride length were observed in 14.7%, 10.5%, 25.4%, 23.5%, and 12.8% of the cases for the OA (<1.5 mm), COPD (<0.6 mm), MS (<2.0 mm), PD (<1.3 mm), and PFF (<0.8 mm) cohorts, respectively. Similarly, the percentage of strides in which the errors in the stride duration were equal to or lower than the temporal resolution (
For the TP strides, the relevant errors for each cohort are shown using Bland–Altman plots; errors for the YA group are also provided in (Figure 4). Excellent absolute (
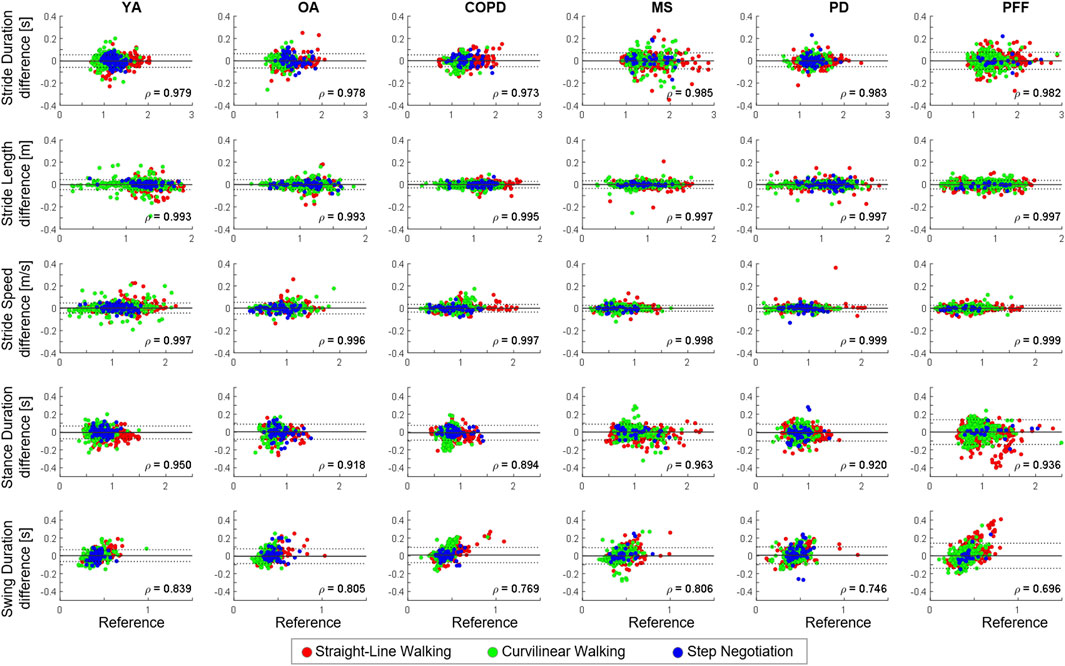
FIGURE 4. Bland–Altman (BA) plots of the different stride-level parameters [stride length (m), stride duration (s), stride speed (m/s), and stance/swing duration (s)] in the young healthy adults (YA), older adults (OA), chronic obstructive pulmonary disease (COPD), multiple sclerosis (MS), Parkinson disease (PD), and proximal femur fracture (PFF) cohorts. Strides detected during straight-line walking, curvilinear walking, and step negotiation are reported in green, red, and blue, respectively. In each BA plot, bias (mean value, gray line) and limits of agreements (bias ±1.96 standard deviations; black with dotted lines) are represented. Spearman correlation coefficients (
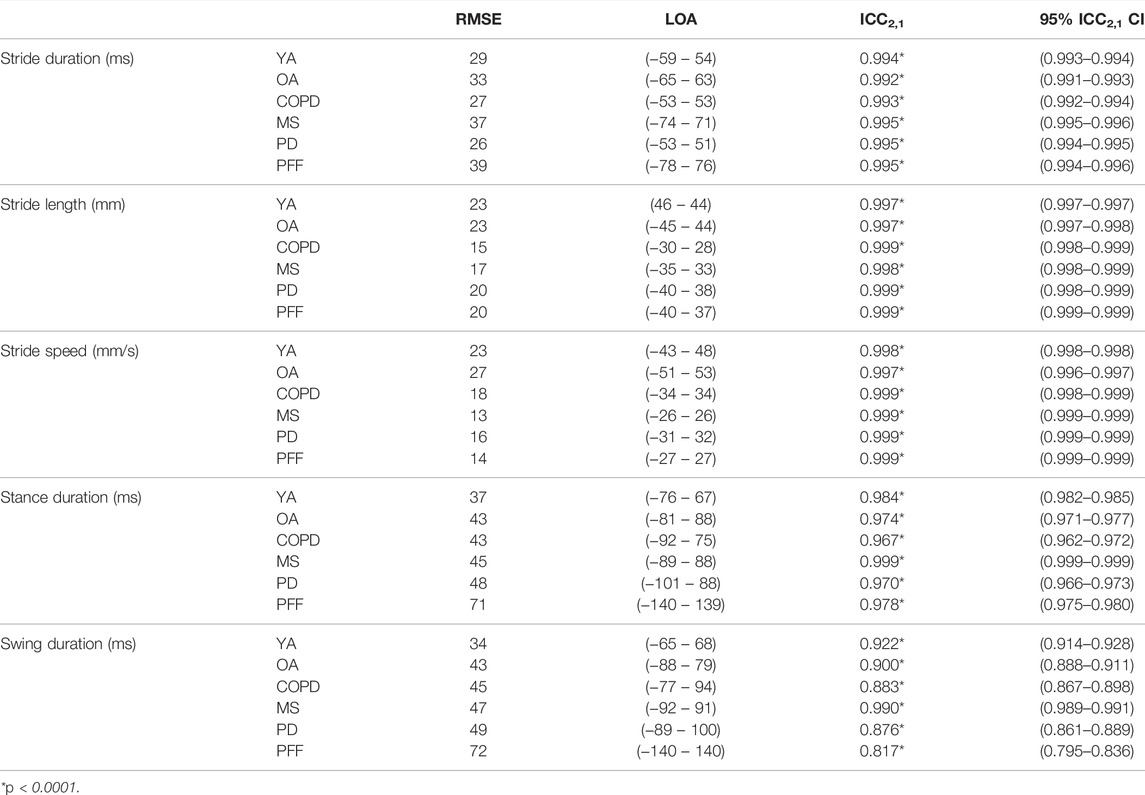
TABLE 5. For each stride parameter (stride duration, length, speed, and stance/swing duration) and cohort (young healthy adults (YA), older adults (OA), chronic obstructive pulmonary disease (COPD), multiple sclerosis (MS), Parkinson disease (PD), and proximal femur fracture (PFF), root mean square error (RMSE) values, limits of agreement (LOA), ICC2,1 with its 95% confidence interval (CI) are shown.
Discussion
This study aimed to propose a method for marker-based gait event detections from motion capture data in complex motor tasks and demonstrate its applicability to gait assessment in different conditions. Using reference gait events detected with pressure insoles, several methods were initially compared with data collected from young healthy adults and the best results were achieved by combining a method based on the AP trajectories (Zeni et al., 2008), largely used in the literature and already tested on different populations (Zeni et al., 2008; Bruening and Ridge, 2014; Hendershot et al., 2016; Filtjens et al., 2020; Gonçalves et al., 2020; Lempereur et al., 2020; Visscher et al., 2021), with an innovative solution exploiting 3D foot velocities, which overcame previously reported issues associated with gait event anticipation. This method (M10) provided estimations with a virtually null bias for both initial and final contacts for all investigated variables, except for a 20 ms bias (2 frame anticipation) for the final contact detection during step negotiation. Very few GEs were missed and extra events were introduced, as shown by the very high values of both sensitivity and PPV (>99% overall). Additionally, F1 scores higher than 99% were recorded in all the three walking conditions, confirming the method is able to correctly identify GEs.
From a methodological perspective, the fact that M10 was the best method is supported by the previous literature using feet marker velocity features (Bruening and Ridge, 2014; Gonçalves et al., 2020; Visscher et al., 2021). When using only the sagittal velocity as per previous literature (M4/M6), a very high sensitivity was observed in the absence of changes of direction (straight-line walking or step negotiation). However, the performance of M4/M6 clearly deteriorated when investigating turning, as previously reported in both young and older participants (Ulrich et al., 2019). This was true also when accounting for changes of direction using the pelvis reference system, likely due to the turn initiation of the foot being delayed with respect to that of the pelvis (Akram et al., 2010). Using 3D velocity overcame this issue, justifying the better results obtained for both M7 and M10.
Having demonstrated superior performance in terms of higher sensitivity and positive predicted values, the generalizability of M10 was then tested on data from five other cohorts, including older adults and patients suffering from conditions regularly associated with distinct gait impairment. High F1 scores (>95%) were still observed for all walking conditions and cohorts, with the only exception of the GEs in the PFF cohort, where for patients with the highest disability (SPPB score ≤4) some GEs were missed in both straight-line and curvilinear walking. Generally, extra and missing GEs were observed in patients using walking aids, reporting severe walking pain, or having the highest disability scores, suggesting that a visual check of the data should always be performed in patients with severely affected gait for data veracity. A null bias was observed in 20% of the observed cases (cohorts and walking conditions) for IC and FC and a residual bias ≤20 ms in all others. Considering previous literature indicates an accuracy of 21 ms for the pressure insoles (Salis et al., 2021), these residual biases can be considered entirely negligible for the ICs. However, they might still need to be accounted for when investigating FCs, where the insoles have an average error of 3 ms (Salis et al., 2021); it is unlikely that such a small difference has a practical relevance. Overall, reported results clearly show that the newly proposed M10 method can be used to accurately extract GEs under different walking conditions and in the presence of a variety of gait impairments.
Visscher et al. (2021) recently quantified how the temporal inaccuracies associated with the detection of gait events propagate to other spatio-temporal parameters, reporting relevant effects only on step width and single limb support. These results were confirmed here in
This study has some limitations. First, the cohorts were too small to include approaches based on machine learning [e.g., Filtjens et al. (2020) and Lempereur et al. (2020)] in the comparison. Nonetheless, the very satisfactory results obtained with M10 seem to leave little room for improvement. Second, the number of events and strides investigated in
In conclusion, the proposed strategy can be combined with motion capture data to automatically extract accurate gait events during complex motor tasks in both young and older healthy individuals and in patients with PD, MS, COPD, and PFF. As an example of a possible application, the method is currently being used as part of a multi-centric study where different stereophotogrammetric systems are used as the gold standard for the validation of digital mobility outcomes obtained from a single inertial sensor device attached to the pelvis (Mazzà et al., 2021). To foster its adoption, the methodology implemented in the present study has been made available via Figshare (https://doi.org/10.15131/shef.data.19102619.v1).
Data Availability Statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found at: https://doi.org/10.15131/shef.data.19102619.v1.
Ethics Statement
The studies involving human participants were reviewed and approved by the University of Sheffield Research Ethics Committee, Tel Aviv Sourasky Medical Center: the Helsinki Committee, Robert Bosch Foundation for Medical Research: Medical Faculty of the University of Tübingen University of Kiel: Medical Faculty of Kiel University, The Newcastle upon Tyne Hospitals NHS Foundation Trust, and Sheffield Teaching Hospitals NHS Foundation Trust: London—Bloomsbury Research Ethics committee. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
TB, CM, and AC designed the study. TB, FS, KS, LA, SB, EB, MC, EG, CH, and LS conducted the experiments, acquiring and pre-processing the data. TB analyzed the experimental data. TB and CM interpreted the results and drafted the article. AC, SD, JH, WM, LP, LR, BS, IV, and CB made important intellectual contributions during revision. All authors have reviewed the manuscript and approved the submitted version.
Funding
This work was supported by the Mobilise-D project that has received funding from the Innovative Medicines Initiative 2 Joint Undertaking (JU) under grant agreement No. 820820. This JU receives support from the European Union’s Horizon 2020 research and innovation program and the European Federation of Pharmaceutical Industries and Associations (EFPIA). This study was also supported by the National Institute for Health Research (NIHR) through the Sheffield Biomedical Research Centre (BRC, Grant Number IS-BRC-1215–20017) and the United Kingdom Engineering and Physical Sciences Research Council (Multisim and MultiSim2 projects, Grant Numbers EP/K03877X/1 and EP/S032940/1, respectively). Subsequent to this work, SD was also supported by the Innovative Medicines Initiative 2 Joint Undertaking (IMI2 JU) project IDEA-FAST - Grant Agreement 853981. LA, LR, and SD were also supported by the National Institute for Health Research (NIHR) Newcastle Biomedical Research Centre (BRC) based at Newcastle upon Tyne Hospital NHS Foundation Trust and Newcastle University. LA, LR, and SD were also supported by the NIHR/Wellcome Trust Clinical Research Facility (CRF) infrastructure at Newcastle upon Tyne Hospitals NHS Foundation Trust. All opinions are those of the authors and not the funders. The content in this publication reflects the authors’ view, and neither IMI nor the European Union, EFPIA, NHS, NIHR, DHSC, or any associated partners are responsible for any use that may be made of the information contained herein.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors would like to acknowledge all the members of the Mobilise-D WP2 work-package for continuous discussion and critical input. They are particularly grateful to the participants in the study for their time and enthusiastic contribution, especially during the pandemic.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fbioe.2022.868928/full#supplementary-material
References
Akram, S. B., Frank, J. S., and Fraser, J. (2010). Coordination of Segments Reorientation during On-The-Spot Turns in Healthy Older Adults in Eyes-Open and Eyes-Closed Conditions. Gait Posture 32 (4), 632–636. doi:10.1016/j.gaitpost.2010.09.006
Bovonsunthonchai, S., Hiengkaew, V., Vachalathiti, R., Said, C. M., and Batchelor, F. (2015). Temporospatial Analysis: Gait Characteristics of Young Adults and the Elderly in Turning while Walking. Int. J. Ther. Rehabilitation 22 (3), 129–134. doi:10.12968/ijtr.2015.22.3.129
Bruening, D. A., and Ridge, S. T. (2014). Automated Event Detection Algorithms in Pathological Gait. Gait Posture 39 (1), 472–477. doi:10.1016/j.gaitpost.2013.08.023
Butland, R. J., Pang, J., Gross, E. R., Woodcock, A. A., and Geddes, D. M. (1982). Two-, Six-, and 12-minute Walking Tests in Respiratory Disease. Bmj 284 (6329), 1607–1608. doi:10.1136/bmj.284.6329.1607
Camomilla, V., Bonci, T., and Cappozzo, A. (2017). Soft Tissue Displacement over Pelvic Anatomical Landmarks during 3-D Hip Movements. J. Biomechanics 62, 14–20. doi:10.1016/j.jbiomech.2017.01.013
Cappozzo, A., Della Croce, U., Leardini, A., and Chiari, L. (2005). Human Movement Analysis Using Stereophotogrammetry. Part 1: Theoretical Background. Gait Posture 21 (2), 186–196. doi:10.1016/j.gaitpost.2004.01.010
Carpinella, I., Gervasoni, E., Anastasi, D., Lencioni, T., Cattaneo, D., and Ferrarin, M. (2018). Instrumental Assessment of Stair Ascent in People with Multiple Sclerosis, Stroke, and Parkinson's Disease: A Wearable-Sensor-Based Approach. IEEE Trans. Neural Syst. Rehabil. Eng. 26 (12), 2324–2332. doi:10.1109/TNSRE.2018.2881324
Crenna, P., Carpinella, I., Rabuffetti, M., Calabrese, E., Mazzoleni, P., Nemni, R., et al. (2007). The Association between Impaired Turning and Normal Straight Walking in Parkinson's Disease. Gait Posture 26 (2), 172–178. doi:10.1016/j.gaitpost.2007.04.010
Curtze, C., Nutt, J. G., Carlson-Kuhta, P., Mancini, M., and Horak, F. B. (2016). Objective Gait and Balance Impairments Relate to Balance Confidence and Perceived Mobility in People with Parkinson Disease. Phys. Ther. 96 (11), 1734–1743. doi:10.2522/ptj.20150662
Deathe, A. B., and Miller, W. C. (2005). The L Test of Functional Mobility: Measurement Properties of a Modified Version of the Timed "Up & Go" Test Designed for People with Lower-Limb Amputations. Phys. Ther. 85 (7), 626–635. doi:10.1093/ptj/85.7.626
Desailly, E., Daniel, Y., Sardain, P., and Lacouture, P. (2009). Foot Contact Event Detection Using Kinematic Data in Cerebral Palsy Children and Normal Adults Gait. Gait Posture 29 (1), 76–80. doi:10.1016/j.gaitpost.2008.06.009
El-Gohary, M., Pearson, S., McNames, J., Mancini, M., Horak, F., Mellone, S., et al. (2014). Continuous Monitoring of Turning in Patients with Movement Disability. Sensors 14 (1), 356–369. doi:10.3390/s140100356
Filtjens, B., Nieuwboer, A., D’cruz, N., Spildooren, J., Slaets, P., and Vanrumste, B. (2020). A Data-Driven Approach for Detecting Gait Events during Turning in People with Parkinson's Disease and Freezing of Gait. Gait Posture 80, 130–136. doi:10.1016/j.gaitpost.2020.05.026
Ghoussayni, S., Stevens, C., Durham, S., and Ewins, D. (2004). Assessment and Validation of a Simple Automated Method for the Detection of Gait Events and Intervals. Gait Posture 20 (3), 266–272. doi:10.1016/j.gaitpost.2003.10.001
Gonçalves, R. V., Fonseca, S. T., Araújo, P. A., Araújo, V. L., Barboza, T. M., Martins, G. A., et al. (2020). Identification of Gait Events in Children with Spastic Cerebral Palsy: Comparison between the Force Plate and Algorithms. Braz. J. Phys. Ther. 24 (5), 392–398. doi:10.1016/j.bjpt.2019.05.007
Hendershot, B. D., Mahon, C. E., and Pruziner, A. L. (2016). A Comparison of Kinematic-Based Gait Event Detection Methods in a Self-Paced Treadmill Application. J. Biomechanics 49 (16), 4146–4149. doi:10.1016/j.jbiomech.2016.10.046
Hreljac, A., and Marshall, R. N. (2000). Algorithms to Determine Event Timing during Normal Walking Using Kinematic Data. J. Biomechanics 33 (6), 783–786. doi:10.1016/S0021-9290(00)00014-2
Hsue, B.-J., Miller, F., Su, F.-C., Henley, J., and Church, C. (2007). Gait Timing Event Determination Using Kinematic Data for the Toe Walking Children with Cerebreal Palsy. J. Biomechanics 40 (2), S529. doi:10.1016/s0021-9290(07)70519-5
Kluge, F., Del Din, S., Cereatti, A., Gaßner, H., Hansen, C., Helbostad, J. L., et al. (2021). Consensus Based Framework for Digital Mobility Monitoring. PLOS ONE 16 (8), e0256541. doi:10.1371/journal.pone.0256541
Koo, T. K., and Li, M. Y. (2016). A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 15 (2), 155–163. doi:10.1016/j.jcm.2016.02.012
Lempereur, M., Rousseau, F., Rémy-Néris, O., Pons, C., Houx, L., Quellec, G., et al. (2020). A New Deep Learning-Based Method for the Detection of Gait Events in Children with Gait Disorders: Proof-Of-Concept and Concurrent Validity. J. Biomechanics 98, 109490. doi:10.1016/j.jbiomech.2019.109490
Lizrova Preiningerova, J., Novotna, K., Rusz, J., Sucha, L., Ruzicka, E., and Havrdova, E. (2015). Spatial and Temporal Characteristics of Gait as Outcome Measures in Multiple Sclerosis (EDSS 0 to 6.5). J. NeuroEngineering Rehabilitation 12 (1), 14–17. doi:10.1186/s12984-015-0001-0
Martin Bland, J., and Altman, D. (1986). Statistical Methods for Assessing Agreement between Two Methods of Clinical Measurement. Lancet 327 (8476), 307–310. doi:10.1016/S0140-6736(86)90837-8
Mazzà, C., Alcock, L., Aminian, K., Becker, C., Bertuletti, S., Bonci, T., et al. (2021). Technical Validation of Real-World Monitoring of Gait: a Multicentric Observational Study. BMJ Open 11 (12), e050785. doi:10.1136/bmjopen-2021-050785
Nightingale, C. J., Mitchell, S. N., and Butterfield, S. A. (2019). Validation of the Timed up and Go Test for Assessing Balance Variables in Adults Aged 65 and Older. J. Aging Phys. Activity 27 (2), 230–233. doi:10.1123/japa.2018-0049
O’Connor, C. M., Thorpe, S. K., O’Malley, M. J., and Vaughan, C. L. (2007). Automatic Detection of Gait Events Using Kinematic Data. Gait Posture 25 (3), 469–474. doi:10.1016/j.gaitpost.2006.05.016
Perry, J., and Davids, J. R. (2010). Gait Analysis. Normal and Pathological Function. 2nd ed. California: Slack.
Rehman, R. Z. U., Klocke, P., Hryniv, S., Galna, B., Rochester, L., Del Din, S., et al. (2020). Turning Detection during Gait: Algorithm Validation and Influence of Sensor Location and Turning Characteristics in the Classification of Parkinson's Disease. Sensors 20 (18), 5377. doi:10.3390/s20185377
Salis, F., Bertuletti, S., Bonci, T., Della Croce, U., Mazzà, C., and Cereatti, A. (2021). A Method for Gait Events Detection Based on Low Spatial Resolution Pressure Insoles Data. J. Biomechanics 127, 110687. doi:10.1016/j.jbiomech.2021.110687
Scott, K., Bonci, T., Alcock, L., Buckley, E., Hansen, C., Gazit, E., et al. (2021). A Quality Control Check to Ensure Comparability of Stereophotogrammetric Data between Sessions and Systems. Sensors 21 (24), 8223. doi:10.3390/s21248223
Shah, V. V., McNames, J., Mancini, M., Carlson-Kuhta, P., Spain, R. I., Nutt, J. G., et al. (2020). Quantity and Quality of Gait and Turning in People with Multiple Sclerosis, Parkinson's Disease and Matched Controls during Daily Living. J. Neurol. 267, 1188–1196. doi:10.1007/s00415-020-09696-5
Ulrich, B., Santos, A. N., Jolles, B. M., Benninger, D. H., and Favre, J. (2019). Gait Events during Turning Can Be Detected Using Kinematic Features Originally Proposed for the Analysis of Straight-Line Walking. J. Biomechanics 91, 69–78. doi:10.1016/j.jbiomech.2019.05.006
Van Uden, C. J., and Besser, M. P. (2004). Test-retest Reliability of Temporal and Spatial Gait Characteristics Measured with an Instrumented Walkway System (GAITRite). BMC Musculoskelet. Disord. 5 (1), 13–14. doi:10.1186/1471-2474-5-13
Visscher, R. M. S., Sansgiri, S., Freslier, M., Harlaar, J., Brunner, R., Taylor, W. R., et al. (2021). Towards Validation and Standardization of Automatic Gait Event Identification Algorithms for Use in Paediatric Pathological Populations. Gait Posture 86, 64–69. doi:10.1016/j.gaitpost.2021.02.031
Walther, B. A., and Moore, J. L. (2005). The Concepts of Bias, Precision and Accuracy, and Their Use in Testing the Performance of Species Richness Estimators, with a Literature Review of Estimator Performance. Ecography 28 (6), 815–829. doi:10.1111/j.2005.0906-7590.04112.x
Keywords: gait analysis, spatio-temporal gait parameters, gait cycle, stride length, stride duration, stride speed, stereophotogrammetry
Citation: Bonci T, Salis F, Scott K, Alcock L, Becker C, Bertuletti S, Buckley E, Caruso M, Cereatti A, Del Din S, Gazit E, Hansen C, Hausdorff JM, Maetzler W, Palmerini L, Rochester L, Schwickert L, Sharrack B, Vogiatzis I and Mazzà C (2022) An Algorithm for Accurate Marker-Based Gait Event Detection in Healthy and Pathological Populations During Complex Motor Tasks. Front. Bioeng. Biotechnol. 10:868928. doi: 10.3389/fbioe.2022.868928
Received: 03 February 2022; Accepted: 20 April 2022;
Published: 02 June 2022.
Edited by:
Rezaul Begg, Victoria University, AustraliaReviewed by:
David Cornelius Kingston, University of Nebraska Omaha, United StatesTony Sparrow, Victoria University, Australia
Copyright © 2022 Bonci, Salis, Scott, Alcock, Becker, Bertuletti, Buckley, Caruso, Cereatti, Del Din, Gazit, Hansen, Hausdorff, Maetzler, Palmerini, Rochester, Schwickert, Sharrack, Vogiatzis and Mazzà. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tecla Bonci, dC5ib25jaUBzaGVmZmllbGQuYWMudWs=