 Guang Yang
Guang Yang Shangzhe Li
Shangzhe Li Yi Lu
Yi Lu
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Bioeng. Biotechnol. , 01 November 2022
Sec. Biomaterials
Volume 10 - 2022 | https://doi.org/10.3389/fbioe.2022.1041531
This article is part of the Research Topic Biomaterials and Antibacterial Materials for Osseous-ligament System View all 21 articles
Background: Radial head arthroplasty (RHA) is typically performed for non-reconstructible radial head fractures with or without valgus stability. The fixation methods can be divided into cemented rigid fixation, such as screw fixation, and uncemented micromovement fixation, including smooth stem, press-fit, expanded device, in-growth stem, and grit-blasted stem fixations. Different fixation methods may impact long-term clinical outcomes and cause complications. This study aimed to compare the long-term follow-up outcomes of cemented and uncemented radial head prostheses.
Methods: A computerized literature search was performed in the PubMed/MEDLINE, Embase, Cochrane Library, and Web of Science databases for studies on radial head prostheses, replacement, and arthroplasty published from inception to April 2022. The prostheses fixation method was divided into cemented and uncemented fixation groups. The outcomes of interest included the participant characteristics, prostheses types, clinical outcomes, reoperation rates, and complication rates during long-term follow-up.
Results: A total of 57 studies involving 2050 patients who underwent RHA were included in our analysis. Cemented fixation was used in 23 of these studies, uncemented fixation in 35 studies, and both cemented and uncemented fixations in one study. Both fixation groups showed significantly improved clinical outcomes after treatment. In particular, both the reoperation and complication rates were lower in the uncemented fixation group (12% and 22%, respectively) than that in the cemented fixation group (20% and 29%, respectively). Among the studies, uncemented monopolar fixation had the lowest reoperation rate (14%), while cemented monopolar fixation had the highest reoperation rate (36%). Regarding complication rates, uncemented bipolar fixation yielded the lowest rate (12%), while cemented bipolar fixation yielded the highest rate (34%). The range of motion and clinical outcome scores were good in both groups.
Conclusion: Uncemented radial head prostheses had lower reoperation and complication rates than cemented prostheses. In particular, uncemented monopolar prostheses may yield the lowest reoperation rate, while uncemented bipolar prostheses may yield the lowest overall complication rate.
Radial head fractures account for approximately 33% of elbow fractures and 1.7%–5.4% of all fractures (Mason ML, 1954; Kaas L et al., 2010). When dislocation or comminuted radial head fractures (modified Mason types III and IV) occur, it is crucial to restore radial head function because of its essential role in maintaining elbow stabilization (Morrey et al., 1991). Currently, radial head arthroplasty (RHA) is universally accepted for the treatment of comminuted radial head fractures. Sershon et al. reported that approximately 85% of patients achieved good-to-excellent outcomes after primary RHA (Sershon et al., 2018). Li et al. performed a systematic review and meta-analysis and concluded that the application of RHA led to better range of motion (ROM) and lower complication rates (Li and Chen, 2014). However, complications after RHA cannot be avoided, with varying reoperation rates ranging from 0% to 45% (Laumonerie et al., 2017). Among these complications, painful loosening is the primary reason for radial head fixation reoperation (Van Riet et al., 2010; O’Driscoll and Herald, 2012; Duckworth et al., 2014; Delclaux et al., 2015; Neuhaus et al., 2015; Kachooei et al., 2016); its cause is speculated to be related to the manner the prostheses stem is fixed.
Radial head prostheses fixation can be divided according to the stem fixation method: cemented and uncemented. Cemented fixation is defined as firm fixation of a prostheses in the medulla without micromotion. Meanwhile, uncemented fixation is described as fixation of a prostheses in the medullary region with micromotion owing to a 1–2 mm space existing between the prostheses stem and medullary cavity. Previous studies have reported that cemented prostheses can achieve good stability, with a lower loosening rate (Acevedo et al., 2014), while uncemented micromotion prostheses can avoid the oversizing effect, alleviate radial head impingement, and have fewer complications (Chanlalit et al., 2012; Laflamme et al., 2017). Nevertheless, there is still controversy regarding which type of prostheses has better performance.
The purpose of this study was to compare between cemented and uncemented radial head prostheses during long-term follow-up. We hypothesized that uncemented prostheses have lower complication and reoperation rates than cemented prostheses.
The study was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The PubMed/MEDLINE, Embase, Cochrane Library, and Web of Science databases were searched from inception to April 2022 using the following search terms: radial head, radial head arthroplasty, prostheses, unipolar, monopolar, bipolar, cemented, uncemented, and not reviewed. Randomized controlled trials, retrospective cohort studies, and case series were included, and the average follow-up period was >24 months. The prostheses fixation methods were divided into cemented and uncemented fixation groups. Letters, comments, editorials, case reports, proceedings, and personal communications as well as studies in which the characteristics of elbow injury involved active infection, previous treatment failure or bilateral treatment were excluded. The list of potential references was reviewed, and data were extracted by two independent reviewers; a third reviewer was consulted to resolve any uncertainties regarding eligibility.
The following data were extracted from the studies that met the inclusion criteria: name of the first author, year of publication, design of the study, number of participants in each group, age and sex of the participants, implants used for RHA, complications, length of follow-up, and major clinical functional outcomes.
The quality of the included studies was evaluated using the modified 18-item Delphi checklist.
The primary outcomes were the rates of reoperation and overall complications. The secondary outcomes were the average range of clinical functional outcomes, including the mean Mayo Elbow Performance Score (MEPS) and Disabilities of the Arm, Shoulder, and Hand (DASH), visual analog scale (VAS), The American Shoulder and Elbow Surgeons Elbow Questionnaire (ASES), and Broberg–Morrey scores, and the average ROM (flexion minus extension). For subgroup analysis, we would investigate the effect of prostheses polarity on the rates of reoperation and complications.
Event rates with 95% confidence intervals (Cis) were calculated for dichotomous outcomes and means with 95% Cis for continuous outcomes. Heterogeneity among the studies was assessed using Cochran’s Q and I2 statistics. The I2 statistic indicates the percentage of the observed between-study variability caused by heterogeneity. Heterogeneity was evaluated based on the I2 statistic as follows: 0%–24%, no heterogeneity; 25%–49%, moderate heterogeneity; 50%–74%, large heterogeneity; and 75%–100%, extreme heterogeneity. When the I2 statistic (>50%) indicated heterogeneity between the studies, the random-effects model (DerSimonian–Laird method) was used. Otherwise, the fixed-effects model was utilized (Mantel–Haenszel method). Pooled effects were calculated, and a two-sided p value of <0.05 was considered to indicate statistical significance. All statistical analyses were performed using the RevMan software version 5.3 (The Cochrane Collaboration, Oxford, United Kingdom).
Of the 211 studies initially identified, 111 were excluded after preliminary screening of the abstracts and titles because they were not relevant (Figure 1). The remaining 100 articles underwent full-text review, and 42 were excluded for not reporting the outcomes of interest, not applying RHA, and not mentioning whether the periprosthetic fixation method was cemented fixation.
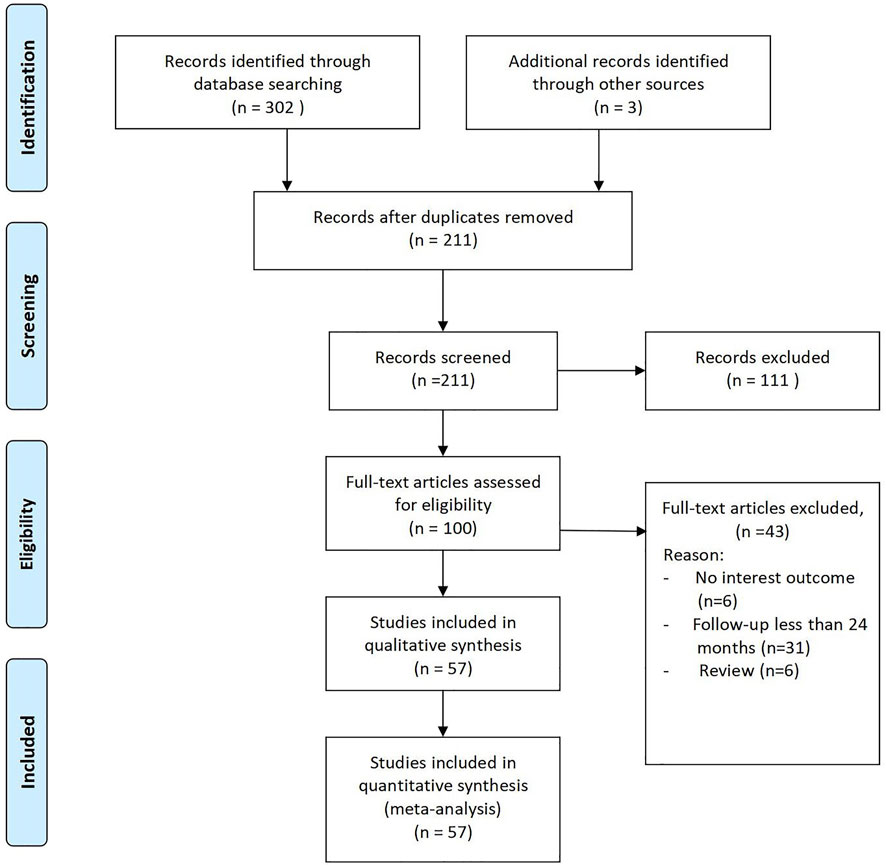
FIGURE. 1. PRISMA 2009 flow diagram.
57 studies were finally included in the analysis, with a total of 2050 patients who received RHA implants: 618 patients received cemented implants, and 1,432 patients received uncemented implants. Two studies were prospective studies; eighteen, retrospective studies; and thirty-seven, case series (Table 1). Across all studies, the mean age in the cemented and uncemented fixation groups was 47.4 and 49.5 years, respectively; the number of the male patients in the cemented and uncemented fixation groups was 320 and 601, respectively, while that of the female patients was 214 and 631 in the studies that mentioned related item, respectively. In general, the average of follow-up in cemented group was 65.6 months, and that in uncemented group was 60.0 months. The detail is shown in Table 1 and 2.
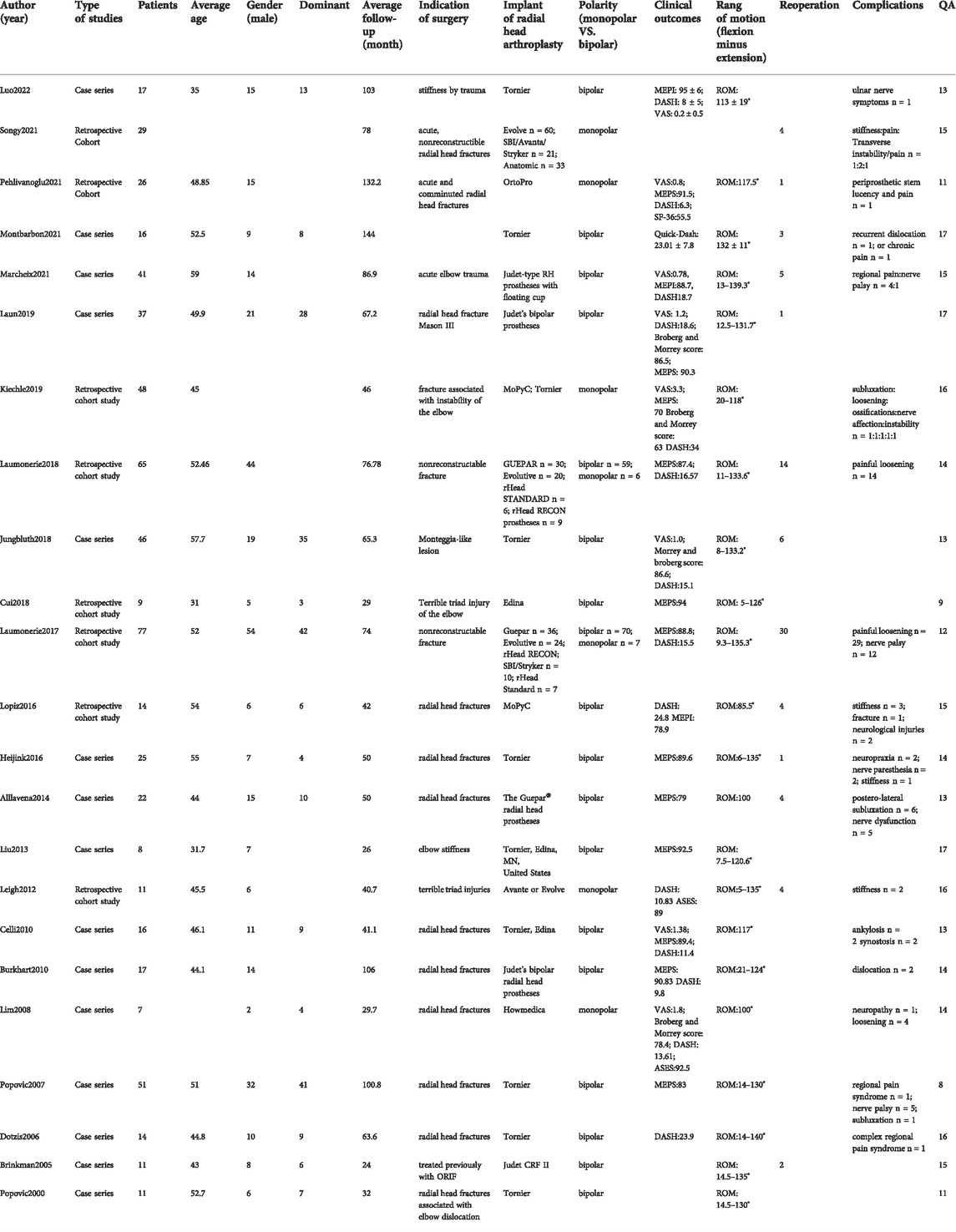
TABLE. 1. Baseline demographics of the selected studies for cemented fixation.
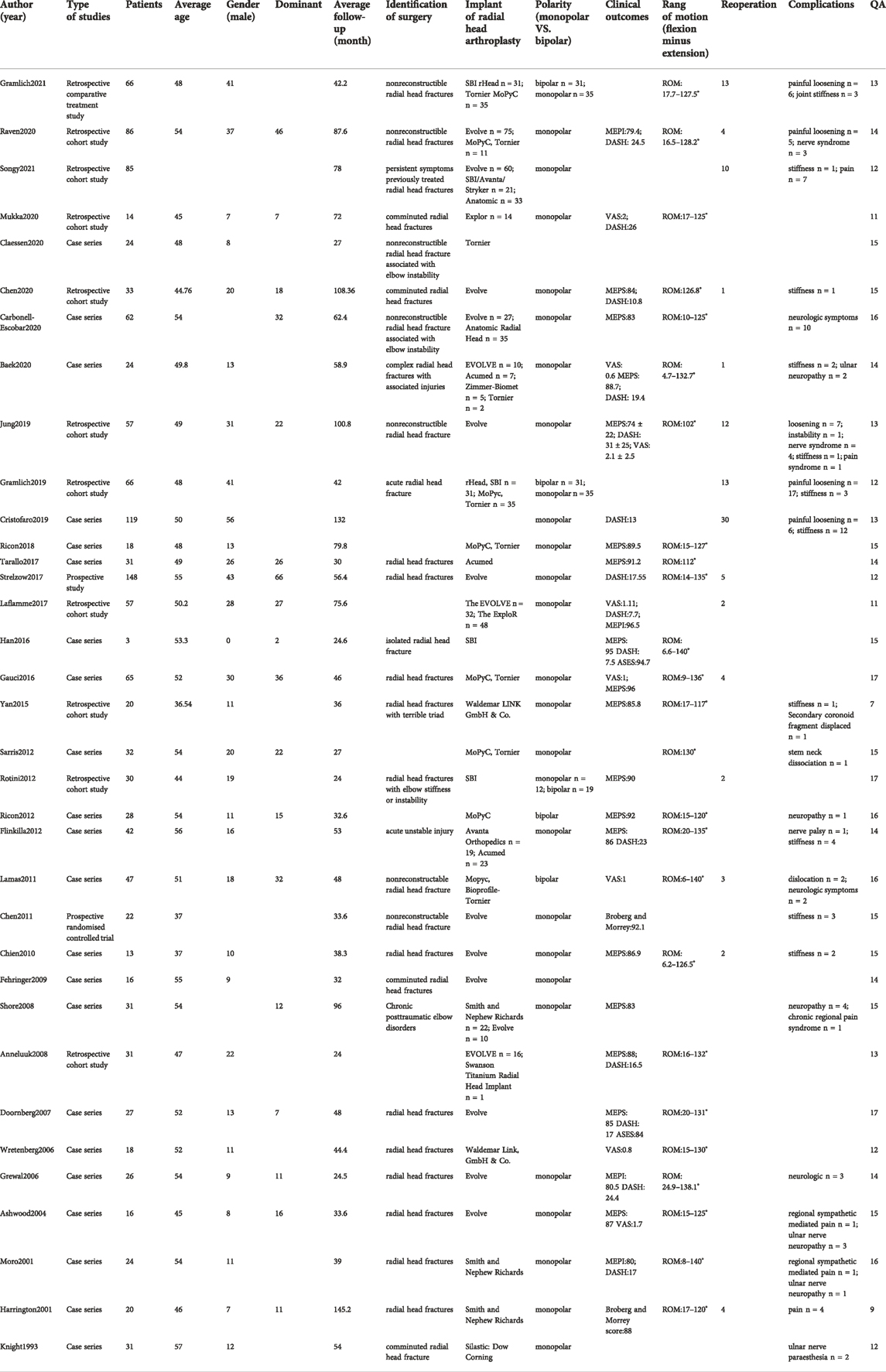
TABLE 2. Baseline demographics of the selected studies for uncemented fixation.
The study quality was assessed using the modified 18-item Delphi checklist (maximal [i.e., best] score: 18). In general, the studies were of good quality, with most (55/59) studies having a score of >10. Two studies had a score of nine and other two studies had scores of 7 and 8, respectively.
Twenty-three and thirty-five studies were included in the analysis of cemented and uncemented fixations, respectively. No significant heterogeneity was found in the rate of cemented and uncemented reoperations (cemented: Q = 7.9, I2 = 0%; uncemented: Q = 7.47, I2 = 0%); therefore, the fixed-effects model was used. The rate of cemented reoperation ranged from 3% to 39%, while that of uncemented reoperation ranged from 2% to 25%, with pooled estimates of 20% and 12%, respectively (cemented: 95% CI: 0.12–0.29, uncemented: 95% CI: 0.06–0.19) (Figures 2, 3). Heterogeneity was observed in the overall complication rate (cemented: Q = 41; I2 = 61%, uncemented: Q = 61.67; I2 = 68%). Therefore, the random-effects model was used. The pooled estimate of overall complications in the cemented and uncemented fixation groups was 29% and 22%, respectively (cemented: 95% CI: 0.16–0.41, uncemented: 95% CI: 0.11–0.34) (Figures 4, 5). Moreover, the mean MEPS and DASH, VAS, ASES, and Broberg–Morrey scores were 70–95, 6.5–34, 0–3.3, 86–92.5, and 63–90.1 in the cemented fixation group and 74–96, 6.17–31, 0.6–2.9, 70–94.7, and 85.5–94.2 in the uncemented fixation group, respectively. The mean ranges of flexion, extension, pronation, and supination between the cemented and uncemented fixation groups were 118–140 vs 124–145, 5–21 vs 4.7–34, 43–87.5 vs. 47.9–85, and 57–88 vs. 35–85, respectively. Seventeen and twenty-two studies reported complications in the cemented and uncemented fixation groups, respectively. The following complications were found in the cemented fixation group: painful loosening (10.1%), nerve symptoms (6.5%), elbow stiffness (2%), dislocation (2%), and regional pain syndrome (1%). Meanwhile, the following complications were reported in the uncemented fixation group: painful loosening (4.3%), nerve symptoms (3.7%), elbow stiffness (3.5%), regional pain syndrome (1.6%), and dislocation (0.5%).
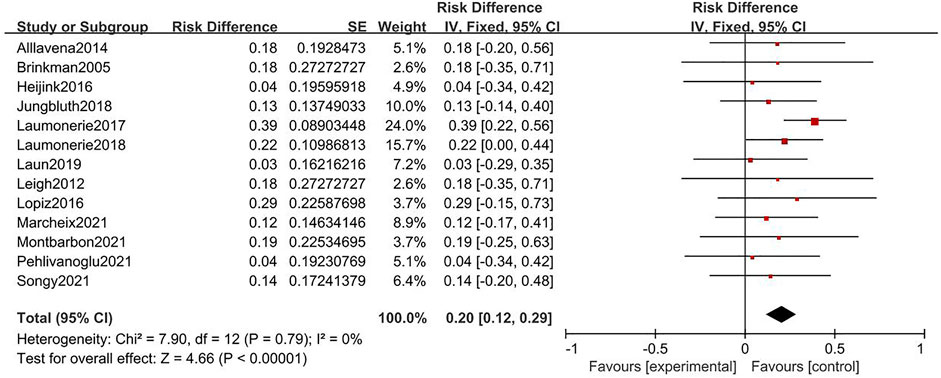
FIGURE. 2. Forest plot for rate of reoperation of cemented fixation.
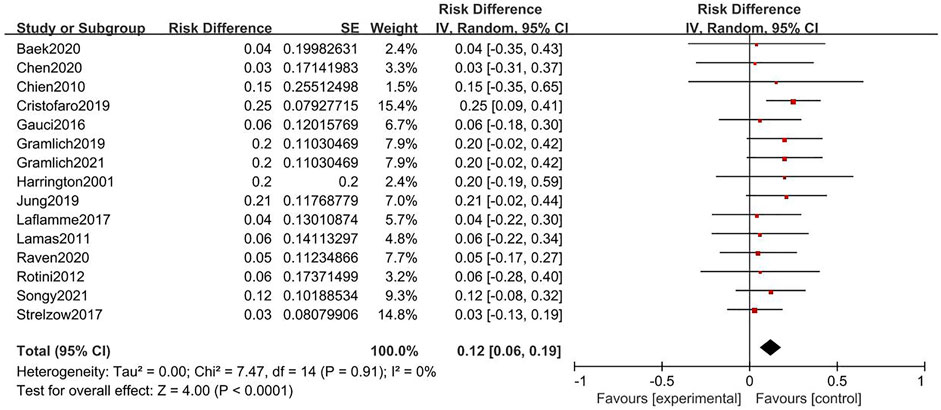
FIGURE. 3. Forest plot for rate of reoperation of uncemented fixation.
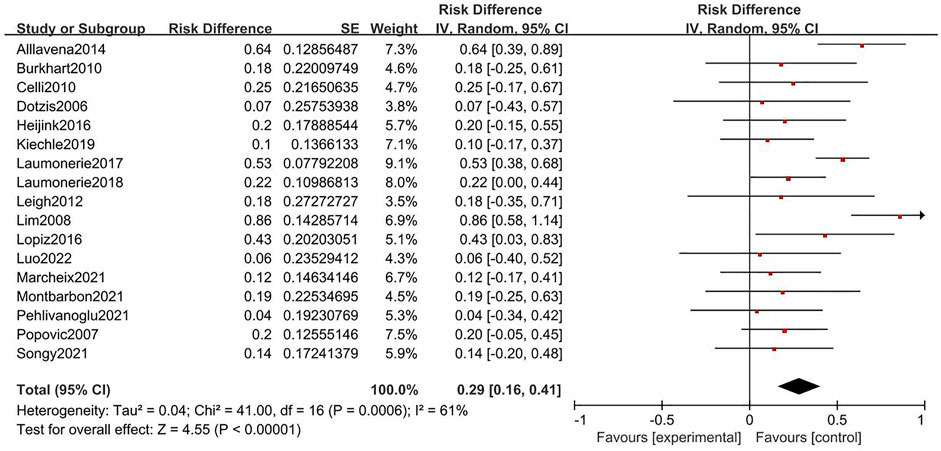
FIGURE. 4. Forest plot for rate of complication of cemented fixation.
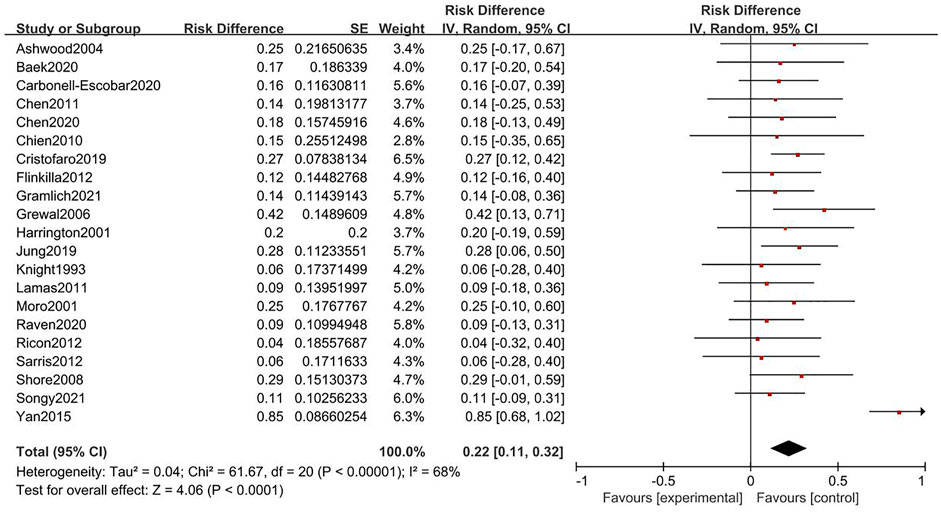
FIGURE. 5. Forest plot for rate of complication of uncemented fixation.
Eighteen studies used cemented bipolar prostheses; six, cemented monopolar prostheses; five, uncemented bipolar prostheses; and twenty-five, uncemented monopolar prostheses. In the meta-analysis, the lowest rate of reoperation was reported for uncemented monopolar fixation (14%, 95% CI: 0.08–0.20) and the lowest rate of complications for uncemented bipolar fixation (12%, 95% CI: 0.05–0.30). The highest rate of reoperation was reported for cemented monopolar fixation (36%, 95% CI: 0.15–0.56) and the highest rate of complications for cemented bipolar fixation (34%, 95% CI: 0.26–0.42) (Table 3). The range of clinical outcomes in cemented bipolar and monopolar was MEPS: 78.9–95 and 70–91.5, DASH: 8–23.9 and 6.3–34, VAS: 0.2–1.38 and 0.8–3.39, Broberg and Morrey: 86.5–86.6 and 63–78.4, while ASES score was only mentioned in two studies using cemented monopolar prostheses, it ranged from 89 to 92.5. And the range of that uncemented bipolar and monopolar was MEPS: 90–92 and 74–96.5, VAS: one and 0.6–2.1, while DASH and Broberg and Morrey reported in studies using uncemented monopolar were 7.7–31 and 88–92.1, respectively. For some of the more concerned complications, distribution of complications in cemented bipolar: nerve symptoms 0.05%, painful loosening 8%, elbow stiffness 2%, dislocation 2.9%, regional pain syndrome 2%, while that in studies using cemented monopolar: nerve symptoms 3.3%, painful loosening 33%, elbow stiffness 5%, dislocation 1.7%, regional pain syndrome 3.3%. Distribution of complications in uncemented bipolar: nerve symptoms 2%, painful loosening 17.5%, elbow stiffness 6%, dislocation 2%, while that in studies using uncemented monopolar: nerve symptoms 3.9%, painful loosening 3%, elbow stiffness 3.2%, dislocation 0.2%, regional pain syndrome 1.7%.
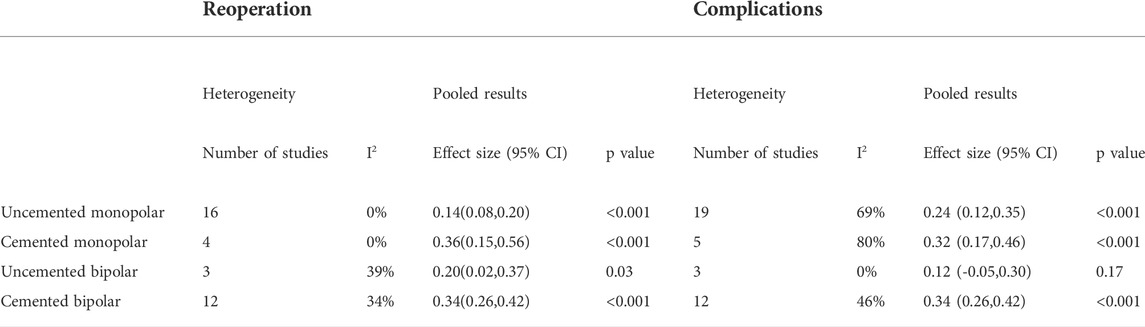
TABLE 3. Meta-analysis for secondary outcomes.
The main finding of this study is that uncemented radial head prostheses had lower reoperation and overall complication rates than cemented radial head protheses. In particular, uncemented monopolar prostheses yielded the lowest reoperation rate and uncemented bipolar prostheses, the lowest overall complication rate.
Multiple radial head prostheses fixation can be classified according to the stem fixation method: uncemented or cemented. For uncemented fixation, there is often a gap of 1–2 mm between the prosthetic stem and medullary cavity, allowing micromotion, which can lead to excessive stress that is appropriately dispersed. Muhm et al. conducted a survey on the outcome of uncemented prostheses during mid-term follow-up; they found a mean Broberg–Morrey score of 85.5 ± 12.2, indicating good results observed in the group (Muhm et al., 2011). For cemented stem fixation, the prostheses was rigidly fixed to the medulla using bone cement. Cement fixation, including firm fixation, may reduce early prostheses loosening, and smaller-diameter stems avoid iatrogenic fracture during surgery. Agyeman et al. performed a systematic review and meta-analysis and found no significant outcome between the cemented prostheses group and the loose smooth stem group, although the cemented prostheses group had a higher risk of complications and reoperation than the other group (Agyeman et al., 2019). Laumonerie et al. conducted a survey of prostheses implanted via cemented fixation and found a relatively high rate of painful loosening (approximately 21.5%), osteolysis (53.8%), and overstuffing (46.2%) (Laumonerie et al., 2018). Szmit et al. performed a biomechanical study and found that using cemented fixation would make the radial head prostheses less effective in distributing high contact stress and easier to get abraded (Szmit et al., 2019). Although Kachooei et al. observed the lowest rate of revision with cemented fixation in their systematic review and meta-analysis, they thought that the rate may be related to difficulties in removing the implant design (Kachooei et al., 2018). Regarding radiographic evaluation, Popovic et al. observed progressive radiographic loosening lines in 16 of 51 patients, and further 16 patients had loss of proximal bone support at the neck of the radius (Popovic et al., 2007). Similarly, Marcheix et al. found that 24% of elbows had radiographic loosening, and 54% of elbows developed lateral condyle demineralization (Marcheix et al., 2021). The results of the present study are comparable with those of previous studies. Herein, higher rates of reoperation and overall complications were found with cemented fixation than with uncemented fixation; in particular, the painful loosening rate was higher with cemented fixation than with uncemented fixation (10% vs 5.5%).
In addition, radial head prostheses were divided into monopolar and bipolar prostheses. Most monopolar prostheses are one-piece unipolar metallic devices with a closely connected junction between the radial head and the stem. Strelzow et al. conducted a survey on monopolar prostheses and found that the final mean PREE and Quick-DASH scores were 17 ± 3 and 14 ± 3, respectively, with a complication rate of 26% (Strelzow et al., 2017). Baek et al. reported satisfactory results of monopolar prostheses for complex radial head fractures, with a mean MEPS of 88.7 ± 11.5 and a mean DASH score of 19.4 ± 7.8 (Baek et al., 2020). In the present study, the rates of complications and reoperation with uncemented monopolar protheses were 24% and 14%, respectively; the rates with cemented monopolar prostheses were 32% and 36%, respectively. The mean VAS score, MEPS, DASH score, and Broberg–Morrey score were 0.8–3.3, 70–91.5, 6.3–34, and 63–78.4, respectively. Bipolar radial head implants were invented to improve the junction and ROM of the elbow, and some experts suggest that their use leads to better elbow kinematics after surgery. Laun et al. reported good-to-excellent results of bipolar arthroplasty for radial head fractures at an average of 5.6 years of follow-up (Laun et al., 2019). Patients showed a mean DASH score of 18.6 and a mean MEPS of 90.3. Burkhart et al. also reported promising mid-to-long-term results with bipolar radial head prostheses. The mean MEPS reached approximately 90.8, and the mean DASH score reached approximately 9.8. However, Burkhart et al. reported degenerative changes in 71% and periarticular ossification after surgery in 76%, which were confirmed in the present study (Burkhart et al., 2010). Herein, the rates of complications and reoperation with uncemented bipolar protheses were 24% and 14%, respectively; the rates with cemented bipolar protheses were 32% and 36%, respectively. The mean VAS score, MEPS, DASH score, and Broberg–Morrey score were 0.2–1.4, 78.9–95, 8–23.9, and 86.5–86.6, respectively.
The efficacy of bipolar or monopolar prostheses is still controversial. Theoretically, bipolar designs reduce abrasion of the capitellar cartilage and stress at the implant-to-cement and cement-to-bone interfaces because of the free rotation between the stem and articular components. The radiocapitellar contact pressure may also decrease with bipolar designs compared with that with monopolar designs owing to the better alignment of the articular component onto the capitellum. Antoni et al. reported similar clinical and radiological results and complication and revision rates (Antoni et al., 2020). Hejink et al. reviewed 30 studies involving 727 patients and found that there was no significant difference in the ROM or clinical outcomes between bipolar and monopolar prostheses (Heijink et al., 2016). Mukka et al. conducted a mean follow-up of 6 years between two kinds of prostheses and found no significant difference in the QuickDASH score and ROM (Mukka et al., 2020). Van Riet et al. reviewed radial head prostheses revisions and observed a lower incidence of loosening with fixed-stem bipolar prostheses than with monopolar prostheses (Van Riet et al., 2010). In the survey by Antoni et al., the rate of ectopic ossification was higher in monopolar prostheses, which may be attributed to the longer follow-up in the monopolar prostheses group.
In our study, cemented monopolar prostheses yielded the highest reoperation rate, while uncemented monopolar prostheses yielded the lowest reoperation rate. Similarly, cemented bipolar prostheses had the highest complication rate, while uncemented bipolar prostheses had the lowest complication rate. Thus, the effect of cemented or uncemented fixation may be dominant in the outcome of RHA, with a minimal effect of bipolar or monopolar fixation. However, further biomechanical and clinical studies are required.
As with any systematic review or meta-analysis, our study has several limitations. First, because data interpretation depends on the quality of the information gathered, the validity of our study may be limited by the respective levels of evidence. Second, different prostheses differ in morphological design, which may have an impact on the results. Third, in the subgroup analysis, only three studies mentioned the rate of periprosthetic loosening in uncemented bipolar prostheses, while three studies mentioned the rate of overall complications in monopolar cemented prostheses, which would create a significant bias. Finally, we included only English literature; studies in other languages were not included, and the results may be affected by the fact that the prostheses used worldwide vary.
Uncemented radial head prostheses have lower rates of reoperation and overall complications than cemented radial head prostheses. In particular, uncemented monopolar prostheses may yield the lowest rate of reoperation, while uncemented bipolar prostheses may yield the lowest rate of overall complications.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
SL, HZ, and YL designed the study and collected the data. SL and GY analyzed and interpreted the patient data. GY was a major contributor in writing the manuscript. All authors read and approved the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer, JC, declared a shared parent affiliation with the authors to the handling editor at the time of review.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acevedo, D. C., Paxton, E. S., Kukelyansky, I., Abboud, J., and Ramsey, M. (2014). Radial head arthroplasty: State of the art. J. Am. Acad. Orthop. Surg. 22 (10), 633–642. doi:10.5435/JAAOS-22-10-633
Agyeman, K. D., Damodar, D., Watkins, I., and Dodds, S. D. (2019). Does radial head implant fixation affect functional outcomes? A systematic review and meta-analysis. J. shoulder Elb. Surg. 28 (1), 126–130. doi:10.1016/j.jse.2018.07.032
Antoni, M., Kempf, J. F., and Clavert, P. (2020). Comparison of bipolar and monopolar radial head prostheses in elbow fracture-dislocation. Orthop. Traumatology Surg. Res. 106 (2), 311–317. doi:10.1016/j.otsr.2019.10.027
Baek, C. S., Kim, B. S., Kim, D. H., and Cho, C. H. (2020). Short- to mid-term outcomes of radial head replacement for complex radial head fractures. Clin. Shoulder Elb. 23 (4), 183–189. doi:10.5397/cise.2020.00325
Burkhart, K. J., Mattyasovszky, S. G., Runkel, M., Schwarz, C., Küchle, R., Hessmann, M. H., et al. (2010). Mid- to long-term results after bipolar radial head arthroplasty. J. shoulder Elb. Surg. 19 (7), 965–972. doi:10.1016/j.jse.2010.05.022
Chanlalit, C., Shukla, D. R., Fitzsimmons, J. S., An, K. N., and O’Driscoll, S. W. (2012). Effect of hoop stress fracture on micromotion of textured ingrowth stems for radial head replacement. J. shoulder Elb. Surg. 21 (7), 949–954. doi:10.1016/j.jse.2011.05.001
Delclaux, S., Lebon, J., Faraud, A., Toulemonde, J., Bonnevialle, N., Coulet, B., et al. (2015). Complications of radial head prostheses. Int. Orthop. 39 (5), 907–913. doi:10.1007/s00264-015-2689-7
Duckworth, A. D., Wickramasinghe, N. R., Clement, N. D., Court-Brown, C. M., and McQueen, M. M. (2014). Radial head replacement for acute complex fractures: What are the rate and risks factors for revision or removal? Clin. Orthop. Relat. Res. 472 (7), 2136–2143. doi:10.1007/s11999-014-3516-y
Heijink, A., Kodde, I. F., Mulder, P., Van Dijk, C. N., and Eygendaal, D. (2016). Cemented bipolar radial head arthroplasty: Midterm follow-up results. J. shoulder Elb. Surg. 25 (11), 1829–1838. doi:10.1016/j.jse.2016.05.017
Kaas, L., van Riet, R. P., Vroemen, J. P., and Eygendaal, D. (2010). The epidemiology of radial head fractures. J. shoulder Elb. Surg. 19 (4), 520–523. doi:10.1016/j.jse.2009.10.015
Kachooei, A. R., Baradaran, A., Ebrahimzadeh, M. H., van Dijk, C. N., and Chen, N. (2018). The rate of radial head prosthesis removal or revision: A systematic review and meta-analysis. J. hand Surg. 43 (1), 39–53.e1. e1. doi:10.1016/j.jhsa.2017.08.031
Kachooei, A. R., Claessen, F. M., Chase, S. M., Verheij, K. K., van Dijk, C. N., and Ring, D. (2016). Factors associated with removal of a radial head prosthesis placed for acute trauma. Injury 47 (6), 1253–1257. doi:10.1016/j.injury.2016.02.023
Laflamme, M., Grenier-Gauthier, P. P., Leclerc, A., Antoniades, S., and Bédard, A. M. (2017). Retrospective cohort study on radial head replacements comparing results between smooth and porous stem designs. J. shoulder Elb. Surg. 26 (8), 1316–1324. doi:10.1016/j.jse.2017.04.008
Laumonerie, P., Reina, N., Gutierrez, C., Delclaux, S., Tibbo, M. E., Bonnevialle, N., et al. (2018). Tight-fitting radial head prosthesis: Does stem size help prevent painful loosening? Int. Orthop. 42 (1), 161–167. doi:10.1007/s00264-017-3644-6
Laumonerie, P., Reina, N., Kerezoudis, P., Declaux, S., Tibbo, M. E., Bonnevialle, N., et al. (2017). The minimum follow-up required for radial head arthroplasty: A meta-analysis. bone & Jt. J. 99-B (12), 1561–1570. doi:10.1302/0301-620X.99B12.BJJ-2017-0543.R2
Laun, R., Tanner, S., Grassmann, J. P., Schneppendahl, J., Wild, M., Hakimi, M., et al. (2019). Primary cemented bipolar radial head prostheses for acute elbow injuries with comminuted radial head fractures: Mid-term results of 37 patients. Musculoskelet. Surg. 103 (1), 91–97. doi:10.1007/s12306-018-0576-2
Li, N., and Chen, S. (2014). Open reduction and internal-fixation versus radial head replacement in treatment of Mason type III radial head fractures. Eur. J. Orthop. Surg. Traumatol. 24 (6), 851–855. doi:10.1007/s00590-013-1367-y
Marcheix, P. S., Cuenca, C., Vergnenegre, G., Mabit, C., Hardy, J., and Charissoux, J. L. (2021). Factors influencing the mid-term radiological and functional outcomes of 41 post-fracture bipolar radial head arthroplasty cases at a mean follow-up of 87 months. Orthop. Traumatology Surg. Res. 107 (2), 102818. doi:10.1016/j.otsr.2021.102818
Mason, M. L. (1954). Some observations on fractures of the head of the radius with a review of one hundred cases. Br. J. Surg. 42 (172), 123–132. doi:10.1002/bjs.18004217203
Morrey, B. F., Tanaka, S., and An, K. N. (1991). Valgus stability of the elbow. A definition of primary and secondary constraints. Clin. Orthop. Relat. Res. 265 (265), 187–195. doi:10.1097/00003086-199104000-00021
Muhm, M., de Castro, R., and Winkler, H. (2011). Radial head arthroplasty with an uncemented modular metallic radial head prosthesis: Short- and mid-term results. Eur. J. trauma Emerg. Surg. 37. St. Pölten, Austria: official publication of the European Trauma Society, 85–95. doi:10.1007/s00068-010-0051-8
Mukka, S., Sjöholm, P., Perisynakis, N., Wahlström, P., Rahme, H., and Kadum, B. (2020). Radial head arthroplasty for radial head fractures: A clinical and radiological comparison of monopolar and bipolar radial head arthroplasty at a mean follow-up of 6 years. Eur. J. trauma Emerg. Surg., 46. St. Pölten, Austria: official publication of the European Trauma Society, 565–572. doi:10.1007/s00068-018-1042-4
Neuhaus, V., Christoforou, D. C., Kachooei, A. R., Jupiter, J. B., Ring, D. C., and Mudgal, C. S. (2015). Radial head prosthesis removal: A retrospective case series of 14 patients. Arch. Bone Jt. Surg. 3 (2), 88–93.
O’Driscoll, S. W., and Herald, J. A. (2012). Forearm pain associated with loose radial head prostheses. J. shoulder Elb. Surg. 21 (1), 92–97. doi:10.1016/j.jse.2011.05.008
Popovic, N., Lemaire, R., Georis, P., and Gillet, P. (2007). Midterm results with a bipolar radial head prosthesis: Radiographic evidence of loosening at the bone-cement interface. J. Bone Jt. Surg. 89 (11), 2469–2476. doi:10.2106/JBJS.F.00723
Sershon, R. A., Luchetti, T. J., Cohen, M. S., and Wysocki, R. W. (2018). Radial head replacement with a bipolar system: An average 10-year follow-up. J. shoulder Elb. Surg. 27 (2), e38–e44. doi:10.1016/j.jse.2017.09.015
Strelzow, J. A., Athwal, G. S., MacDermid, J. C., Grewal, R., Faber, K. J., Drosdowech, D., et al. (2017). Effect of concomitant elbow injuries on the outcomes of radial head arthroplasty: A cohort comparison. J. Orthop. Trauma 31 (10), e327–e333. doi:10.1097/BOT.0000000000000921
Szmit, J., King, G., Johnson, J. A., and Langohr, G. (2019). The effect of stem fit on the radiocapitellar contact mechanics of a metallic axisymmetric radial head hemiarthroplasty: Is loose fit better than rigidly fixed? J. shoulder Elb. Surg. 28 (12), 2394–2399. doi:10.1016/j.jse.2019.05.019
Keywords: radial head, arthroplasty, replacement, prostheses, fixation
Citation: Yang G, Li S, Zhang H and Lu Y (2022) A systematic review and meta-analysis on different stem fixation methods of radial head prostheses during long-term follow-up. Front. Bioeng. Biotechnol. 10:1041531. doi: 10.3389/fbioe.2022.1041531
Received: 11 September 2022; Accepted: 21 October 2022;
Published: 01 November 2022.
Edited by:
Yansong Qi, Inner Mongolia People’s Hospital, ChinaReviewed by:
Jianhai Chen, Peking University People’s Hospital, ChinaCopyright © 2022 Yang, Li, Zhang and Lu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yi Lu, bHV5aV9zcG9ydHNAMTI2LmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.