
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Bioeng. Biotechnol., 15 September 2022
Sec. Biomaterials
Volume 10 - 2022 | https://doi.org/10.3389/fbioe.2022.1003322
This article is part of the Research TopicBiomaterials in cardiovascular research: models, methods, and therapiesView all 7 articles
 Wansong Hu1
Wansong Hu1 Jun Jiang2*
Jun Jiang2*Coronary heart disease (CHD) is a type of cardiovascular disease with the highest mortality rate worldwide. Percutaneous transluminal coronary intervention (PCI) is the most effective method for treating CHD. However, in-stent restenosis (ISR), a long-term complication after PCI, affects the prognosis of patients with CHD. Previous studies have suggested that hypersensitivity reactions induced by metallic components may be one of the reasons of this complication. With the emergence of first- and second-generation drug-eluting stents (DES), the efficacy and prognosis of patients with CHD have greatly improved, and the incidence of ISR has gradually decreased to less than 10%. Nevertheless, DES components have been reported to induce hypersensitivity reactions, either individually or synergistically, and cause local inflammation and neointima formation, leading to long-term adverse cardiovascular events. In this article, we described the relationship between ISR and hypersensitivity from different perspectives, including its possible pathogenesis, and discussed their potential influencing factors and clinical significance.
Cardiovascular diseases (CVDs) are one of the leading causes of death worldwide. Globally, an estimated 18.6 million people died of CVDs in 2019. Since the 1970s, when the world’s first percutaneous transluminal coronary angioplasty (PTCA) was performed clinically, percutaneous coronary intervention (PCI) has become an important method of treating coronary heart disease (CHD). However, postoperative in-stent restenosis (ISR) and thrombosis are the main factors affecting its efficacy. ISR is defined as the presence of a stenosis greater than 50% of the diameter of the stent segment found on angiography that can clinically manifest as recurrent unstable angina pectoris, and in rare cases, acute myocardial infarction (Dangas et al., 2010). The incidence of ISR can be as high as 20–40%, and is caused by damage to the arterial wall due to various reasons, subsequently resulting in fibroproliferation, inflammatory response, and eventually neointimal hyperplasia (NIH) (Hoffmann et al., 1996). Few studies have shown that local inflammation caused by hypersensitivity to alloy components in metal stents may be one of the reasons for this complication (Table 1). Metal stents, which are foreign bodies, cause vascular remodeling, persistent endothelial dysfunction, and fibrin deposition via local inflammation (Torrado et al., 2018).
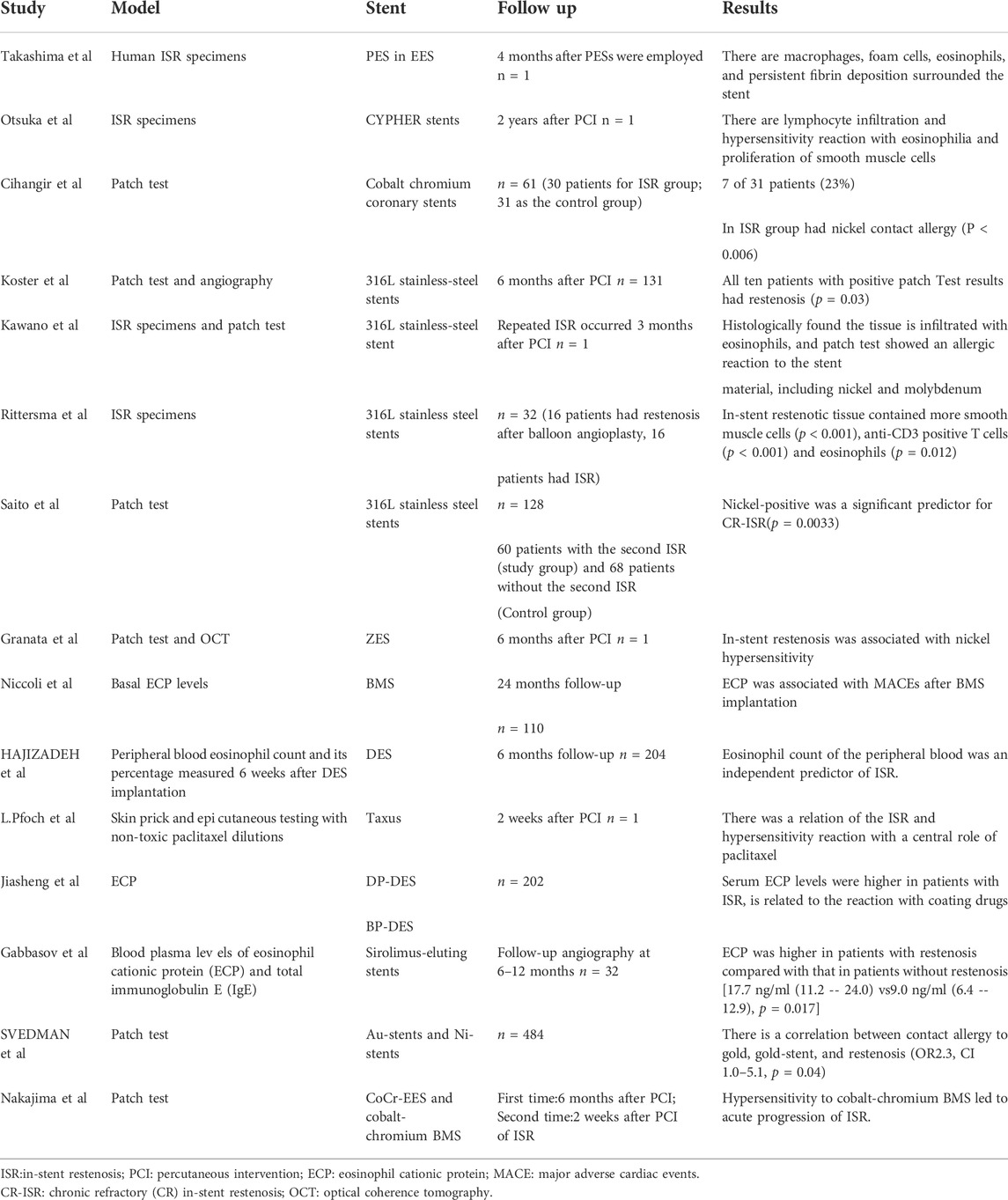
TABLE 1. Human studies and case reports implicating hypersensitivity in the process of restenosis.
Over the past few decades, great strides have been made to reduce the incidence of ISR with the advent of drug-eluting stents (DES). Restenosis rates can be reduced by up to 10–20% in patients treated with first-generation DES. Nevertheless, according to incomplete statistics, the incidence of ISR still requires revascularization is 5 %–10%. The underlying mechanisms of DES restenosis can be considered to result from four factors: mechanical, biological, genetic, and technical factors (Aoki and Tanabe, 2021). In terms of biological factors, in addition to drug resistance, allergic inflammatory responses to polymer and metal scaffold platforms cannot be ignored (Figure 1) (Giustino et al., 2022).
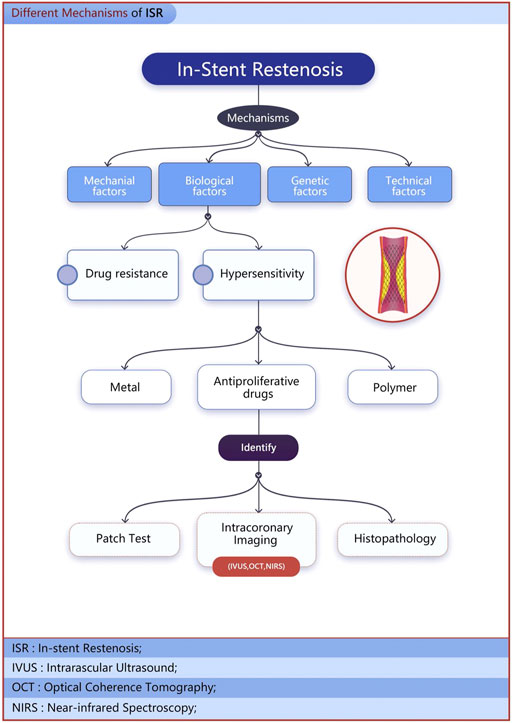
FIGURE 1. The underlying mechanisms of DES restenosis.
In this review, we explored the relationship between hypersensitivity and the different components of different stents, including their potential mechanisms for promoting restenosis and their impact on prognosis. In addition, we summarized the evidence that ISR is associated with allergic reactions and discussed its current diagnosis, treatment strategies, and future prospects.
Inflammatory response is one of the pathogenic mechanisms leading to adverse events after stent implantation, and its role in the occurrence and development of ISR after PCI has been confirmed in several studies (Welt and Rogers, 2002). Balloon expansion and stent implantation can cause vascular endothelial injury to varying degrees, and pro-inflammatory factors, such as tumor necrosis factor (TNF), interleukin-1, and interleukin-6 released at the injury site, mediate the adhesion and aggregation of inflammatory cells. The inflammatory process can stimulate proliferation, differentiation, and extracellular matrix synthesis of vascular smooth muscle, eventually leading to the proliferation of local neointima (Kornowski et al., 1998). In addition, damaged vascular endothelium is prone to platelet and fibrin deposition, which is associated with the formation of mural thrombi (Byrne et al., 2015).
Classical and allergic inflammation are the two main inflammatory response mechanisms. The activation pathway of the former involves monocytes, macrophages, neutrophils, and T lymphocytes, whereas, the latter is mainly caused by eosinophils and mast cells (Montone et al., 2013).
In the classical inflammatory response, C-reactive protein (CRP) is a common inflammatory marker. Few studies have found that plasma CRP levels are significantly increased in patients with restenosis. Clinically, it can be used as an independent predictor of major adverse cardiac events (MACE) and restenosis after stent implantation (Buffon et al., 1999). Other inflammatory markers, such as plasminogen activator inhibitor (PAI-1) and matrix metalloproteinases (MMPs), are also considered to be associated with first-generation DES restenosis (Katsaros et al., 2008; Katsaros et al., 2010).
Eosinophils and mast cells are effector cells involved in allergic inflammatory responses (Costa et al., 1997). Eosinophils can secrete growth factors, chemokines, and interleukin-1 (Fulkerson and Rothenberg, 2013). Mast cells are involved in the release of histamine, tryptase, chymase, a series of cytokines and chemokines, platelet activating factors, and arachidonic acid products (Shi et al., 2015). Cellular mediators of allergic inflammation also play roles in the formation and development of coronary plaques. Among them, histamine and leukotrienes are effective vasoactive inflammatory molecules that can increase the vascular permeability and activate endothelial cells (Kunder et al., 2011). Tryptase and chymase may be involved in the degradation of high-density lipoprotein (HDL) (Lee et al., 2002), which may be related to plaque rupture in patients with acute coronary syndrome (Lee-Rueckert and Kovanen, 2006). Additionally, mast cells promote the activation of T cells and macrophages, leading to endothelial cell proliferation and fibrosis. In fact, both the types of cells are functionally capable of regulating each other, forming the so-called “allergic effector units” (Gangwar et al., 2016).
Most coronary stents, especially bare metal stents (BMS) and first-generation DES, are made of 316 L stainless steel, which contains metal elements such as nickel, chromium, and molybdenum. These metal ions are eluted from the stent by the blood, saline, proteins, and mechanical stress. It is estimated that up to 17% of the population is allergic to nickel and another 1–2% of the population is allergic to other elements, such as cobalt and chromium, to varying degrees (Basko-Plluska et al., 2011). Allergies related to metal implants are well documented in orthopedics, dentistry, and other fields (Honari et al., 2008). Metal ions eluted from the device may bind to endogenous proteins in complexes or directly activate T cell receptors in a super-antigen fashion. Additionally, they may lead to macrophage activation and cause delayed allergic reactions. The allergic reactions may be localized as local dermatitis, systemic as eczema, or may induce a syndrome similar to systemic lupus erythematosus. Hypersensitivity to related metal components has been found in patients with late adverse cardiovascular events (Granata et al., 2015) such as ISR and late stent thrombosis (LST) (Kataoka et al., 2012).
Köster et al. were the first to demonstrate that patients with delayed hypersensitivity reactions to metals, especially nickel, have a higher incidence of ISR(Köster et al., 2000). However, due to the limitations of retrospective studies, only 8% of patients in the study had positive results. Compared with the high incidence in the population, this finding is not surprising. In addition, investigators have pointed out that patients without suspected restenosis were not investigated in this study; hence, it is difficult to rule out possible metal allergy, which is an important missing control group (Keane et al., 2001). Some follow-up studies of ISR in patients treated with stainless steel stents did not confirm Köster’s original observations. Furthermore, Saito et al. found that tissue response to nickel is a major factor in chronic refractory ISR (Saito et al., 2009). New-generation DES use metal alloys, such as cobalt-chromium (CoCr) or platinum-chromium (PTCR), which, in contrast, have thinner struts and lower nickel content than stainless steel stents (Gori et al., 2019). However, nickel allergy remained significantly associated with ISR in CoCr stent-treated patients (Aliagaoglu et al., 2012). Additionally, a study reported local hypersensitivity and restenosis at the site of stent fracture after CoCr stent implantation, suggesting a potential role of the accelerated release of metal ions (Mori et al., 2017).
Previous case reports have demonstrated repeated incidence of ISR after receiving CoCr stents in patients with proven nickel allergy. After switching to bio-absorbable vascular stents (Jurado-Roman et al., 2017) and prednisolone anti-allergic treatment (Nakajima et al., 2016) after PCI, the patients’ prognosis significantly improved. In 2016, Nakajima also reported a case of recurrent ISR and overt metal allergy after implantation of CoCr everolimus-eluting stents (CoCr—EES), in which recurrent restenosis was terminated with prednisolone and tranilast treatment (Nakajima et al., 2016).
Studies have shown that nickel salts such as nickel chloride can directly activate vascular endothelial cells and upregulate the expression of intercellular adhesion molecule 1 (ICAM-1) (Messer et al., 2005). As a cell surface glycoprotein and adhesion receptor (Hubbard and Rothlein, 2000), ICAM-1 plays a role in leukocyte transendothelial migration (TEM). In response to inflammatory stimuli, ICAM-1 is involved in the regulation of leukocyte rolling and adhesion interactions with the vessel wall in the vascular endothelium and guides leukocytes across the endothelial layer (Yang et al., 2005), thereby promoting the occurrence of local in-stent restenosis. Additionally, ICAM-1 is involved in many other physiological processes, including immune cell effector functions, clearance of pathogens and dead cells, and activation of T cells. Related studies have also been conducted on the development, metastasis, and prognosis of tumors. Furthermore, studies have demonstrated that ICAM-1 expression can be induced in conjunctival epithelial cells (ECs) of allergic patients, revealing its role as a marker of allergic inflammation (Bui et al., 2020).
However, there have always been a controversy regarding the allergy and restenosis associated with stainless steel stents. Few studies do not report a link between these factors (Thyssen et al., 2011; Slodownik et al., 2018). In a prospective study, Norgaz et al. did not find an association between nickel allergy and the development of ISR in patients with stainless steel stents (Norgaz et al., 2005). Similarly, Iijima et al. prospectively assessed the differential relationship between metal allergy in initial ISR and after restenosis treatment and found that metal allergy was not associated with restenosis after the initial stent implantation but was associated with recurrent restenosis (Iijima et al., 2005). It is worth noting that unlike the patch test method in previous studies, Santiago et al. only included patients with a history of metal allergy before coronary stent placement by querying personal history. The possibility of sensitization directly caused by the stent placement was ruled out. The findings showed that a history of metal allergy was not associated with adverse outcomes in patients undergoing PCI (Romero-Brufau et al., 2012). Furthermore, in a retrospective study, Svedman et al. found that gold-plated stents were significantly associated with gold allergy and restenosis. Conversely, this behavior was not observed for nickel in this study. These findings suggest that gold is a stronger sensitizer than nickel and may elicit a stronger immune response leading to endothelial cell proliferation (Svedman et al., 2009). Nevertheless, larger prospective studies and randomized controlled trials are needed to confirm the association between this metal allergy and ISR.
The allergic reaction resulting from the use of DES is not solely from the non-drug components of the stent. Compared with BMS, DES incorporate antiproliferative agents to prevent restenosis. There are two main classes of impregnated drugs in first-generation DES: inhibitors of the mammalian target of rapamycin (mTOR) (e.g., sirolimus and its analogs) and paclitaxel and its derivatives. The first drug used in the Cypher stents was sirolimus. Sirolimus (rapamycin) is a macrolide antibiotic extracted from S. hygroscopicus (Aminian et al., 2009). It is a multifunctional serine-threonine kinase that acts on IL-2-mediated signal transduction pathways, and is a central regulator of cell growth, proliferation, and apoptosis. Therefore, it is used in immunosuppressive therapy for cancer and as an anti-rejection agent after transplantation. Moreover, it is used in coronary stents to reduce the neointimal formation and restenosis (Kawano et al., 2004; Steffel and Tanner, 2007). Although sirolimus is mostly considered to be an unlikely cause of allergy as it generally reduces eosinophil infiltration and histamine release, clinical adverse reactions to sirolimus such as bone marrow suppression, hyperlipidemia, and hypercholesterolemia, are still visible (Brara et al., 2003). In addition, life-threatening coronary spasms have been reported, which may be related to severe endothelial dysfunction (Wheatcroft et al., 2006). This is similar to the clinical complications of the type I variant of Kounis syndrome. At the same time, rapamycin was also found to increase the expression and activity of thrombin and tumor necrosis factor-α-induced endothelial tissue factor (Steffel et al., 2005).
In an animal study, histopathological examination of the heart of laboratory rats administered with sirolimus revealed a focal myocardial infarction (Walpoth and Hess, 2004). The incidence was positively correlated with the drug dose. In addition, animal experiments have shown that a rat model of synthetic vascular grafts treated with systemic or topical rapamycin has a propensity for thrombosis (Walpoth et al., 2001). Previous human studies have also reported that allergic vasculitis after DES implantation may be associated with late and very late stent thrombosis, and occurs almost exclusively with first-generation sirolimus-eluting stents (SES, Cypher) (Cook et al., 2009). In addition, Nakazawa et al. evaluated patients’ coronary stent histomorphology and found that although SES can better inhibit NIH, the allergic inflammation mediated by cells including eosinophils and lymphocytes is more serious and is the main cause of LST compared with paclitaxel-eluting stents (PES) (Nakazawa et al., 2008). In contrast, LST in PES is mostly secondary to the malpositioning caused by excessive fibrin deposition.
Paclitaxel was isolated from the bark of Taxus japonica and was later used as an anti-restenosis drug for the TAXUS stent. Unlike mTOR inhibitors, paclitaxel is a cytotoxic agent that binds to β-tubulin and causes cell cycle arrest in the second growth phase by inhibiting the microtubule assembly (M phase of the cell cycle), leading to the dissolution of mitotic spindle structures (G2) and mitosis (M) (Blagosklonny et al., 2004)and inhibiting the proliferation of human endothelial cells. Allergic reactions such as neutropenia, thrombocytopenia, gastrointestinal symptoms, and peripheral neuropathy are common in patients with various cancers treated with paclitaxel (Picard, 2017). Although it is an effective antirestenosis drug, its safety has been questioned. A previous study found that paclitaxel may be an important cause of the excessive deposition of intravascular fibrin, which is related to LST (Nakazawa et al., 2011). Pfoch also reported a case of anaphylaxis 2 weeks after PES stent placement in a patient who was desensitized after antihistamine therapy (Pfoch et al., 2009). Owing to the timely detection and treatment, the patient did not develop ISR during the follow-up period of more than 1 year. However, it is worth noting that it is often easy to ignore the follow-up data in patients whose early allergic reactions are not obvious in the whole body and could possibly turn fatal. Although DES have been shown to reduce restenosis rates, allergic reactions to stent components have the opposite effect.
Compared with first-generation DES, second-generation DES use derivatives of sirolimus, such as Evorolimus and Zotarolimus, as carrier drugs. Compared with sirolimus, they can be used at lower drug concentrations and have reduced toxicity compared. However, Otsuka et al. reported a case of ZES and EES implantation. The patient had three ZES and one EES implanted for severe LAD lesions and died 238 days later. Histological examination of the scaffold revealed persistent inflammation and fibrin deposition with marked infiltration of eosinophils, T-lymphocytes, and multinucleated giant cells (Otsuka et al., 2015). Moreover, hypersensitivity pneumonitis has been previously reported in kidney transplant patients treated with sirolimus (Shin et al., 2013). Although ZES-related allergic events are rare, the biological toxicity of zotarolimus cannot be ruled out (Takashima et al., 2015).
Polymers, an important part of DES, can control the release of anti-proliferative drugs to ensure the anti-restenosis efficacy. As carriers for topical administration, polymers in first-generation DES such as polystyrene-b-isobutylene-b-styrene of the Taxus Express PES, Cipher sirolimus polyethylene vinyl acetate (PEV-A), and polybutyl methacrylate (PBMA) of SES-eluting stents can effectively control drug release and significantly reduce the rate of restenosis (Byrne et al., 2017). However, data suggest that polymers used in first-generation DES have poor biocompatibility and are associated with late clinical adverse events. Allergic reactions have been reported with the use of polymers, such as those in latex and vinyl gloves. These allergic reactions are usually type IV hypersensitivity reactions caused by low-molecular-weight compounds called haptens. In 2004, a case of a local allergic reaction to Cipher SES was reported, possibly triggered by its polymers (Virmani et al., 2004b). Notably, the local inflammatory response was found to be more pronounced after 90 days, when the antiproliferative drugs were released. In addition, an animal experiment found localized extensive inflammation with abundant eosinophils at 28 and 90 days in Cipher stents implanted in porcine coronary arteries (Virmani et al., 2004a). However, in polymer-free metal stents, the inflammation was less pronounced at 90 days than at 28 days, and the inflammatory response was found to be polymer-related at longer durations. Similar reports have been reported in other clinical trials. These results suggest that polymers are associated with excessive inflammation and stent thrombosis (ST). In addition, it has been reported that the polyethylene-vinyl acetate compound of Cipher copolymer can cause an inflammatory response in 25% of rabbits when used as an antigen delivery matrix (Niemi et al., 1985). Both PES and SES elicited distinct inflammatory responses in animal models for over 90 days. The second-generation DES can reduce the inflammatory or allergic reaction caused by polymers by improving the biocompatibility of the stent polymer coating or by applying a degradable polymer coating. Second-generation DES use highly fluorinated polymers or amphiphilic polymers (i.e., PVDF-HFP and BioLinx) (Strohbach and Busch, 2015), which reduce the platelet adhesion and activation compared to non-fluoropolymer-coated metal stents and have better resistance than previous polymers (Torii et al., 2020). However, a case report found persistent fibrin deposition and extensive periarthritis in stent segments at autopsy 8 months after implantation of the CoCr-EES and Resolute zotarolimus-eluting stent (R-ZES), caused by palisade macrophage cells, T lymphocytes, eosinophils, and multinucleated giant cells, suggesting the occurrence of allergic reactions (Otsuka et al., 2015). This can be attributed to either of the two components of DES: the drug and the polymer. The coexistence of PBMA as a component of the polymer in both the scaffolds should be suspected. In addition, many new durable and biodegradable polymers (Gong et al., 2010) have been studied. Most biodegradable polymers are synthetic polyesters of the polylactic acid-hydroxy acid family. Studies have found that they decrease MACE within 24 months and show a certain advantage (Han et al., 2008). However, more clinical studies are needed to determine their long-term prognosis. Furthermore, it has been suggested that neither the polymer nor the drug could be an allergen, since allergic ISR still occurs 8 and 12 months after stent implantation in the absence of both biodegradable polymer and sirolimus (Jimba et al., 2020).
The prognosis of patients with acute coronary lesions undergoing PCI is confirmed to be related to the activation of various inflammatory cells and the production and release of several mediators (Niccoli et al., 2010b).
Previously, researchers defined an allergy-related acute coronary syndrome as “Kounis Syndrome” (KS). The pathophysiology of KS is characterized by a localized allergic response leading to mast cell activation and release of inflammatory mediators. When this process exceeds a certain threshold, coronary spasm and plaque erosion or rupture can occur (Kounis et al., 2007). There are three variants of KS. The type I variant is the most common, accounting for approximately 72.6% of the cases, with a clinical manifestation in the form of coronary artery spasm with or without an increase in myocardial enzyme and troponin levels. The type II variant (22.3%) is accompanied by plaque erosion or rupture, manifesting as acute myocardial infarction. Type III variant (5.1%) involves coronary stent thrombosis due to allergic reactions (Kounis et al., 2012; Abdelghany et al., 2017). KS, a possible manifestation of hypersensitivity to stent components, may play a key role in the development of acute or late thrombus formation in DES (Chen et al., 2009).
ISR is a multifactorial and complex process, and studies have suggested that inflammation and immune imbalance play important roles. Eosinophils are important effector cells associated with allergy and play an important role in promoting allergic inflammation by releasing pro-inflammatory mediators (histamine and leukotriene C4) (Bochner, 2000). Eosinophils have been demonstrated to be reliable predictors of ISR after DES implantation (Hajizadeh et al., 2017). Histopathological studies have shown that eosinophils are associated with ISR with BMS. Numerous pathological studies have also shown inflammatory responses such as macrophages, foam cells, eosinophils, and persistent fibrin deposition around the scaffold in patients with ISR. In particular, the infiltration of a large number of eosinophils suggests hypersensitivity (Rittersma et al., 2006). Similarly, some case reports have revealed histopathological findings of lymphocytic and eosinophilic infiltration following Cipher stent implantation. Eosinophils may accumulate late and secrete inflammatory factors, initiate inflammatory and hypersensitivity reactions, and exacerbate tissue damage, thereby promoting smooth muscle cell migration and proliferation, leading to lumen narrowing and the occurrence and development of ISR (Gabbasov et al., 2009). Notably, eosinophils are equally important in the promotion of thrombosis (Sakai et al., 2009). Eosinophils also synthesize and release many other pro-angiogenic cytokines such as IL-8, IL-6, transforming growth factor-beta, and granulocyte-macrophage colony-stimulating factor (GM-CSF), both of which play a role in promoting wound healing and maintaining allergic inflammation (Munitz and Levi-Schaffer, 2004). Nevertheless, most related studies are single case reports or small sample clinical observations. There is a lack of clinical studies with larger samples for verification.
The eosinophil cationic protein (ECP) is a sensitive marker of eosinophil activation (Niccoli et al., 2010a; Niccoli et al., 2014a), and a variety of biological activities that interact with other immune cells and plasma proteins. Elevated eosinophil activation plays an important role in the pathogenesis of restenosis in DES (Gabbasov et al., 2011). ECP also upregulates the ICAM-1 expression in endothelial cells, allowing monocytes to adhere to endothelial cells, which is thought to be an essential step in atherogenesis. In addition to its pronounced cytotoxic activity, ECP has several regulatory activities in vitro, including the inhibition of proliferating T lymphocyte responses to antigens and inhibition of B lymphocyte synthesis of immunoglobulins. In a prospective study, baseline serum ECP levels were used to predict the risk of MACEs after BMS and first-generation DES implantation (Niccoli et al., 2009; Niccoli et al., 2011). In addition, Niccoli et al. found that unlike CRP, ECP is associated with the severity of coronary atherosclerosis (Niccoli et al., 2014b). Moreover, this study found that serum ECP levels were significantly elevated in patients with advanced ISR and were an independent risk factor for ISR.
Coronary angiography remains the clinical standard for diagnosing ISR and assessing its severity. Different morphologies indicated by angiographic results are of great significance for the classification, treatment, and prognostic evaluation of ISR. However, coronary angiography has certain limitations, especially in assessing the lumen size and plaque characteristics. Intracoronary imaging techniques allow for a detailed, objective assessment of the extent and morphology of lesions by changing the imaging modality. Furthermore, it has become an important tool for understanding the pathophysiology associated with ST and ISR(Koskinas et al., 2016; Mintz and Guagliumi, 2017).
Current commonly used intracoronary imaging tools include intravascular ultrasound (IVUS) and optical coherence tomography (OCT). IVUS has the ability to visualize the coronary lumen and vessel wall and can help delineate the outer elastic lamina behind stents, thereby revealing the actual vessel size, assessing the post-stent under-expansion, and distribution of NIH. A classification system for DES-ISR was proposed based on the inspection findings under IVUS (Kang et al., 2011). In contrast, OCT provides higher-resolution imaging that can better characterize the tissue, delineate the lumen-intima interface, and determine the distribution of stent struts. Additionally, it can visualize the macrophage clumps and vascular components and distinguish the white thrombi from the red thrombi. It is important to measure the fibrous caps and identify unstable plaques (Kashiwagi et al., 2013; Taruya et al., 2015). The ISRs of BMS and DES exhibit different characteristics in OCT. The BMS-ISR typically shows a homogeneous hyperintense tissue band on OCT, reflecting its NIH richness in smooth muscle cells. In contrast, DES-ISR is seen as unevenly distributed on OCT, suggesting that the neointima contains more proteoglycans or fibrin, and fewer cells. In addition, OCT is helpful for the assessment of neoatherosclerosis. A new classification scheme was recently proposed to describe the mechanism of ISR by using OCT to guide the associated treatment (Gonzalo et al., 2009). Near-infrared spectroscopy is another less-used imaging technique capable of localizing and quantifying lipid core load (Roleder et al., 2017); however, its clinical benefit is currently limited to relevant case reports.
Intracoronary imaging can be helpful in the detection of NIH in the context of allergic reactions; however, the clinical diagnosis of allergic reactions is mostly derived from the histopathology of restenotic stents or autopsy pathology. In addition, serum eosinophil level is a sensitive marker of allergic reactions. The detection of allergy to metal components mostly adopts a unified patch test, and the standard of positive reaction is an inflammatory reaction after 48 h or 72 h, accompanied by erythema, edema, papules, or other infiltrative changes (Johansen et al., 2015).
Repeated DES implantation is the most effective treatment for ISR (Giacoppo et al., 2015; Siontis et al., 2015); however, interventional procedures are subject to complications such as perioperative myocardial injury (PMI) (Nano et al., 2022). In addition to the reopening of diseased blood vessels, drug therapy for allergic inflammation is worthy of further study. Related drugs mainly inhibit the activation and local recruitment of allergic inflammatory effector cells and release of allergic response mediators.
Statins are widely used in the treatment of CVDs and have anti-inflammatory, antioxidant, and anti-atherosclerotic functions. In addition, statins exhibit immunomodulatory effects. Fluvastatin is a potent inhibitor of IgE-mediated activation and degranulation of basophils and mast cells (Kolawole et al., 2016).
Leukotrienes mediate various inflammatory and allergic responses and are produced by the metabolism of arachidonic acid via the 5-lipoxygenase pathway. Leukotriene B4, produced by enzymatic hydrolysis, can induce chemotaxis and adhesion of inflammatory cells such as neutrophils and macrophages to vascular endothelial cells (De Caterina and Zampolli, 2004). Leukotriene receptor antagonists are widely used as anti-inflammatory and anti-allergic drugs. In a study of the low-density lipoprotein (LDL) receptor mouse model, it was found that the degree of arterial injury in mice with 5-lipoxygenase gene deficiency was significantly reduced, suggesting that 5-lipoxygenase may play an important role in atherosclerosis (De Caterina and Zampolli, 2004). Similarly, a clinical study of patients with acute coronary syndromes found significant reductions in the volume of noncalcified coronary plaques in patients treated with inhibitors of 5-lipoxygenase activity (Tardif et al., 2010).
Moreover, the traditional mast cell stabilizer, sodium cromoglycate, has a good therapeutic effect on allergic reactions as it inhibits the release of allergic response mediators such as histamine and serotonin by stabilizing the mast cell membranes and preventing degranulation. The mas-related G protein-coupled receptor-X2 (MRGPRX2) receptor is thought to be one of the possible links between cardiovascular events and allergies (Azimi and Lerner, 2017). Novel mast cell stabilizers such as QWF (Boc-Gln-D-Trp [Formyl]-Phe benzyl ester tri-fluoroacetate) inhibit the substance P-induced mast cell degranulation and inflammatory responses by antagonizing MRGPRX2. The study also found that in LDL receptor-deficient (Ldlr−/−) mice, mast cell stabilization may have played an important role in delaying the progression of coronary atherosclerosis, reducing inflammation, and improving lipid metabolism (Wang et al., 2013).
The main mechanism for the occurrence of adverse reactions after DES implantation is the activation of both the classical and allergic inflammatory pathways. All DES components, including metal and polymer coatings, can induce hypersensitivity reactions individually or synergistically. In addition to acute or late ST, the IRS due to hypersensitivity-induced NIH also significantly affects patient prognosis. Regarding metal allergy, some researchers have proposed the use of nickel-free stainless steel materials and degradable metal stents. Recently, a study has considered the use of new titanium-alloy stents. Titanium alloy as a drug storage layer can replace the original polymer coating to overcome the possible existing polymer sensitization by forming a nanotube-like oxide layer on the anodized surface (Soliman et al., 2019). The study showed that in patients with acute coronary syndromes, CoCr-titanium-coated stents were non-inferior to the platinum-chromium biodegradable polymer, EES, in inducing major cardiac events at 12 months (Tonino et al., 2020). Despite the biocompatibility of the target moiety and improved tissue specificity and cellular uptake (Yin et al., 2014), nanoparticles, as a new generation of smart drug delivery materials, still require extensive research to evaluate their safety issues (Cherian et al., 2021). In addition, clinical evaluation of polymer-free DES is also underway. In a clinical follow-up trial of up to 3 years, polymer-free amphilimus-eluting stents were compared with the new-generation permanent-polymer zotarolimus-eluting stents in 1–3 years of TLF (in terms of target lesion failure) (van Hemert et al., 2021). No significant differences were observed in studies with longer follow-up periods (Kufner et al., 2020). Among the many factors that contribute to ISR, implantation is usually the most important and relatively controllable factor (Farooq et al., 2011).
With the gradual deepening of the concept of “intervention without implantation,” fully bioabsorbable stents should have gradually entered the clinic. The advantages of bioresorbable coronary scaffolds (BRS) can be divided into the following aspects: 1) The absence of permanent stent implants can restore the response of blood vessels to normal physiological stimuli, which is helpful for the dilatative remodeling of blood vessels at the late stage; 2) Without metal stents, continuous stimulation of the material can reduce the occurrence of local chronic inflammatory reactions, thereby reducing intimal hyperplasia and thrombotic events; 3) BRS will not affect revascularization after complete absorption, nor will it affect the noninvasive imaging. Related absorbable magnesium alloy stents have been studied and have been shown to demonstrate better antithrombotic properties in clinical trials (Sakamoto et al., 2018). However, long-term follow-up data are required to verify its safety and efficacy.
Stent coverings for nitric oxide donors and stents embedded with anti-inflammatory and anti-allergic drugs are gradually being developed (Kural et al., 2019). However, whether these can address this worrying complication remains a question worthy of further clinical research. Scientists are actively seeking new interventions to reduce the inflammation after stent implantation. Microribonucleic acids are a class of small non-coding RNAs that play important roles in the initiation and resolution of inflammation after vascular injury. The MiR-21 stem loop plays an important role in the activation of smooth muscle cells (SMCs) and macrophages after vascular injury. Animal studies have shown that the genetic ablation of the miR-21 stem loop reduces neointimal formation following stent implantation in mice (McDonald et al., 2015).
ISR remains a challenging problem in the cardiovascular field and its occurrence is often multifactorial, where local inflammation leading to aggressive neointimal proliferation and advanced neoatherosclerosis is common. Stratification according to the etiology and pathogenesis of ISR may be necessary to guide the individualized treatment (Shlofmitz et al., 2019). Stent-related allergic reactions are commonly reported with the use of BMS and first-generation DES. Although the use of second-generation DES has improved in-stent platform design and antiproliferative drugs, polymer coatings and allergic reactions related to stent components have been previously reported. In addition, DES-related hypersensitivity is associated with ST (Yokouchi et al., 2010) and late-acquired stent dislocation. Hypersensitivity-related mediators are involved in platelet activation, and endothelial dysfunction caused by inflammatory responses that may induce neoatherosclerosis, thereby promoting ST (Chioncel et al., 2021). Compared with BMS, late lumen loss in DES occurred more than 9 months later and increased gradually, a phenomenon known as late catch-up. A meta-analysis showed that allergy to stent materials significantly increased the risk of ISR (Gong et al., 2013). However, the limitations of the meta-analysis are that the included studies were case-control studies and not a single prospective study was included.
Nevertheless, physicians should be aware of the occurrence of allergic reactions associated with stent placement. Further research is required to improve the biocompatibility of coronary stents. Clinically, high-risk individuals with potential allergic reactions to stent components after DES implantation can be identified based on the evaluation of markers, such as eosinophil count and ECP. In addition, there is a need to develop new and reliable diagnostic methods for identifying the potential allergens. The predictive value of related indicators for poor prognosis, such as ISR, can also help optimize the clinical management of patients. In patients with potential allergic reactions, patch testing before and after stent placement and subsequent risk stratification for allergic predisposition may be necessary, while few patients may require combined anti-allergic therapy. Furthermore, given the development of anaphylaxis and poor prognosis of ISR, more research is needed to understand the specific pathways involved in the recruitment and activation of allergic inflammatory effector cells associated with coronary artery disease, which may reveal new important therapeutic targets (Niccoli et al., 2018) for de novo or refractory ISR, thereby reducing the occurrence of this clinical event and the associated risk of long-term cardiovascular events.
All authors contributed to the study conception and design. Literature review and analysis were performed by WH. JJ participated in the analysis and discussion of the results of the article. The first draft of the manuscript was written by WH and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
This work was supported by National Natural Science Foundation of China (No. 81570322 and 82170332), Zhejiang Provincial Key Research and Development Plan (No. 2020C03016).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abdelghany, M., Subedi, R., Shah, S., and Kozman, H. (2017). Kounis syndrome: A review article on epidemiology, diagnostic findings, management and complications of allergic acute coronary syndrome. Int. J. Cardiol. 232, 1–4. doi:10.1016/j.ijcard.2017.01.124
Aliagaoglu, C., Turan, H., Erden, I., Albayrak, H., Ozhan, H., Basar, C., et al. (2012). Relation of nickel allergy with in-stent restenosis in patients treated with cobalt chromium stents. Ann. Dermatol. 24 (4), 426–429. doi:10.5021/ad.2012.24.4.426
Aminian, A., Kabir, T., and Eeckhout, E. (2009). Treatment of drug-eluting stent restenosis: An emerging challenge. Catheter. Cardiovasc. Interv. 74 (1), 108–116. doi:10.1002/ccd.21938
Aoki, J., and Tanabe, K. (2021). Mechanisms of drug-eluting stent restenosis. Cardiovasc. Interv. Ther. 36 (1), 23–29. doi:10.1007/s12928-020-00734-7
Azimi, E., and Lerner, E. A. (2017). Implications of MRGPRX2 in human and experimental cardiometabolic diseases. Nat. Rev. Cardiol. 14 (2), 124. doi:10.1038/nrcardio.2016.212
Basko-Plluska, J. L., Thyssen, J. P., and Schalock, P. C. (2011). Cutaneous and systemic hypersensitivity reactions to metallic implants. Dermatitis 22 (2), 65–79. doi:10.2310/6620.2011.10055
Blagosklonny, M. V., Darzynkiewicz, Z., Halicka, H. D., Pozarowski, P., Demidenko, Z. N., Barry, J. J., et al. (2004). Paclitaxel induces primary and postmitotic G1 arrest in human arterial smooth muscle cells. Cell CycleGeorget. Tex.) 3 (8), 1048–1054. doi:10.4161/cc.3.8.986
Bochner, B. S. (2000). Systemic activation of basophils and eosinophils: Markers and consequences. J. Allergy Clin. Immunol. 106 (5), S292–S302. doi:10.1067/mai.2000.110164
Brara, P. S., Moussavian, M., Grise, M. A., Reilly, J. P., Fernandez, M., Schatz, R. A., et al. (2003). Pilot trial of oral rapamycin for recalcitrant restenosis. Circulation 107 (13), 1722–1724. doi:10.1161/01.cir.0000066282.05411.17
Buffon, A., Liuzzo, G., Biasucci, L. M., Pasqualetti, P., Ramazzotti, V., Rebuzzi, A. G., et al. (1999). Preprocedural serum levels of C-reactive protein predict early complications and late restenosis after coronary angioplasty. J. Am. Coll. Cardiol. 34 (5), 1512–1521. doi:10.1016/s0735-1097(99)00348-4
Bui, T. M., Wiesolek, H. L., and Sumagin, R. (2020). ICAM-1: A master regulator of cellular responses in inflammation, injury resolution, and tumorigenesis. J. Leukoc. Biol. 108 (3), 787–799. doi:10.1002/JLB.2MR0220-549R
Byrne, R. A., Joner, M., and Kastrati, A. (2015). Stent thrombosis and restenosis: What have we learned and where are we going? The andreas grüntzig lecture ESC 2014. Eur. Heart J. 36 (47), 3320–3331. doi:10.1093/eurheartj/ehv511
Byrne, R. A., Stone, G. W., Ormiston, J., and Kastrati, A. (2017). Coronary balloon angioplasty, stents, and scaffolds. Lancet 390 (10096), 781–792. doi:10.1016/s0140-6736(17)31927-x
Chen, J. P., Hou, D., Pendyala, L., Goudevenos, J. A., and Kounis, N. G. (2009). Drug-eluting stent thrombosis: The Kounis hypersensitivity-associated acute coronary syndrome revisited. JACC Cardiovasc. Interv. 2 (7), 583–593. doi:10.1016/j.jcin.2009.04.017
Cherian, A. M., Nair, S. V., Maniyal, V., and Menon, D. (2021). Surface engineering at the nanoscale: A way forward to improve coronary stent efficacy. Apl. Bioeng. 5 (2), 021508. doi:10.1063/5.0037298
Chioncel, V., Andrei, C. L., Brezeanu, R., Sinescu, C., Avram, A., and Tatu, A. L. (2021). Some perspectives on hypersensitivity to coronary stents. Int. J. Gen. Med. 14, 4327–4336. doi:10.2147/IJGM.S326679
Cook, S., Ladich, E., Nakazawa, G., Eshtehardi, P., Neidhart, M., Vogel, R., et al. (2009). Correlation of intravascular ultrasound findings with histopathological analysis of thrombus aspirates in patients with very late drug-eluting stent thrombosis. Circulation 120 (5), 391–399. doi:10.1161/CIRCULATIONAHA.109.854398
Costa, J. J., Weller, P. F., and Galli, S. J. (1997). The cells of the allergic response: Mast cells, basophils, and eosinophils. JAMA 278 (22), 1815–1822. doi:10.1001/jama.1997.03550220021005
Dangas, G. D., Claessen, B. E., Caixeta, A., Sanidas, E. A., Mintz, G. S., and Mehran, R. (2010). In-stent restenosis in the drug-eluting stent era. J. Am. Coll. Cardiol. 56 (23), 1897–1907. doi:10.1016/j.jacc.2010.07.028
De Caterina, R., and Zampolli, A. (2004). From asthma to atherosclerosis--5-lipoxygenase, leukotrienes, and inflammation. N. Engl. J. Med. Overseas. Ed. 350 (1), 4–7. doi:10.1056/nejmp038190
Farooq, V., Gogas, B. D., and Serruys, P. W. (2011). Restenosis: Delineating the numerous causes of drug-eluting stent restenosis. Circ. Cardiovasc. Interv. 4 (2), 195–205. doi:10.1161/CIRCINTERVENTIONS.110.959882
Fulkerson, P. C., and Rothenberg, M. E. (2013). Targeting eosinophils in allergy, inflammation and beyond. Nat. Rev. Drug Discov. 12 (2), 117–129. doi:10.1038/nrd3838
Gabbasov, Z. A., Kozlov, S. G., Imaeva, A. E., Saburova, O. S., Zykov, K. A., Masenko, V. P., et al. (2011). In-stent restenosis after revascularization of myocardium with drug-eluting stents is accompanied by elevated level of blood plasma eosinophil cationic protein. Can. J. Physiol. Pharmacol. 89 (6), 413–418. doi:10.1139/y11-038
Gabbasov, Z. A., Kozlov, S. G., Lyakishev, A. A., Saburova, O. S., Smirnov, V. A., and Smirnov, V. N. (2009). Polymorphonuclear blood leukocytes and restenosis after intracoronary implantation of drug-eluting stentsThis article is one of a selection of papers from the NATO Advanced Research Workshop on Translational Knowledge for Heart Health (published in part 1 of a 2-part Special Issue). Can. J. Physiol. Pharmacol. 87 (2), 130–136. doi:10.1139/Y08-107
Gangwar, R. S., Friedman, S., Seaf, M., and Levi-Schaffer, F. (2016). Mast cells and eosinophils in allergy: Close friends or just neighbors. Eur. J. Pharmacol. 778, 77–83. doi:10.1016/j.ejphar.2015.10.036
Giacoppo, D., Gargiulo, G., Aruta, P., Capranzano, P., Tamburino, C., and Capodanno, D. (2015). Treatment strategies for coronary in-stent restenosis: Systematic review and hierarchical bayesian network meta-analysis of 24 randomised trials and 4880 patients. BMJ Clin. Res. ed.) 351, h5392. doi:10.1136/bmj.h5392
Giustino, G., Colombo, A., Camaj, A., Yasumura, K., Mehran, R., Stone, G. W., et al. (2022). Coronary in-stent restenosis: JACC state-of-the-art review. J. Am. Coll. Cardiol. 80 (4), 348–372. doi:10.1016/j.jacc.2022.05.017
Gong, F., Cheng, X., Wang, S., Zhao, Y., Gao, Y., and Cai, H. (2010). Heparin-immobilized polymers as non-inflammatory and non-thrombogenic coating materials for arsenic trioxide eluting stents. Acta Biomater. 6 (2), 534–546. doi:10.1016/j.actbio.2009.07.013
Gong, Z., Li, M., Guo, X., Ma, Z., and Shi, J. (2013). Stent implantation in patients with metal allergy: A systemic review and meta-analysis. Coron. Artery Dis. 24 (8), 684–689. doi:10.1097/MCA.0b013e3283647ad1
Gonzalo, N., Serruys, P. W., Okamura, T., van Beusekom, H. M., Garcia-Garcia, H. M., van Soest, G., et al. (2009). Optical coherence tomography patterns of stent restenosis. Am. Heart J. 158 (2), 284–293. doi:10.1016/j.ahj.2009.06.004
Gori, T., Polimeni, A., Indolfi, C., Raber, L., Adriaenssens, T., and Munzel, T. (2019). Predictors of stent thrombosis and their implications for clinical practice. Nat. Rev. Cardiol. 16 (4), 243–256. doi:10.1038/s41569-018-0118-5
Granata, F., Moscarella, E., and Varricchio, A. (2015). In-stent restenosis because of nickel hypersensitivity: A bioresorbable solution? Coron. Artery Dis. 26 (5), 461–462. doi:10.1097/MCA.0000000000000233
Hajizadeh, R., Ghaffari, S., Separham, A., Shokouhi, B., Kavandi, H., Pourafkari, L., et al. (2017). The value of peripheral blood eosinophil count in predicting in-stent restenosis in patients with stable angina pectoris undergoing drug eluting stenting. Rom. J. Intern Med. 55 (4), 229–236. doi:10.1515/rjim-2017-0024
Han, Y., Jing, Q., Chen, X., Wang, S., Ma, Y., Liu, H., et al. (2008). Long-term clinical, angiographic, and intravascular ultrasound outcomes of biodegradable polymer-coated sirolimus-eluting stents. Catheter. Cardiovasc. Interv. 72 (2), 177–183. doi:10.1002/ccd.21600
Hoffmann, R., Mintz, G. S., Dussaillant, G. R., Popma, J. J., Pichard, A. D., Satler, L. F., et al. (1996). Patterns and mechanisms of in-stent restenosis. A serial intravascular ultrasound study. Circulation 94 (6), 1247–1254. doi:10.1161/01.cir.94.6.1247
Honari, G., Ellis, S. G., Wilkoff, B. L., Aronica, M. A., Svensson, L. G., and Taylor, J. S. (2008). Hypersensitivity reactions associated with endovascular devices. Contact Dermat. 59 (1), 7–22. doi:10.1111/j.1600-0536.2008.01351.x
Hubbard, A. K., and Rothlein, R. (2000). Intercellular adhesion molecule-1 (ICAM-1) expression and cell signaling cascades. Free Radic. Biol. Med. 28 (9), 1379–1386. doi:10.1016/s0891-5849(00)00223-9
Iijima, R., Ikari, Y., Amiya, E., Tanimoto, S., Nakazawa, G., Kyono, H., et al. (2005). The impact of metallic allergy on stent implantation: Metal allergy and recurrence of in-stent restenosis. Int. J. Cardiol. 104 (3), 319–325. doi:10.1016/j.ijcard.2004.12.034
Jimba, T., Hashikata, T., Matsushita, M., and Yamasaki, M. (2020). Repetitive restenosis in a biodegradable polymer sirolimus-eluting stent with hypersensitivity reaction: A case report. Eur. Heart J. Case Rep. 4 (1), 1–5. doi:10.1093/ehjcr/ytaa001
Johansen, J. D., Aalto-Korte, K., Agner, T., Andersen, K. E., Bircher, A., Bruze, M., et al. (2015). European Society of Contact Dermatitis guideline for diagnostic patch testing - recommendations on best practice. Contact Dermat. 73 (4), 195–221. doi:10.1111/cod.12432
Jurado-Roman, A., Lopez-Lluva, M. T., Sanchez-Perez, I., Piqueras-Flores, J., Maseda, R., and Lozano-Ruiz-Poveda, F. (2017). Bioresorbable vascular scaffold to treat malignant in-stent restenosis in a patient with nickel allergy. Cardiovasc. Revasc. Med. 18 (6S1), 38–40. doi:10.1016/j.carrev.2016.12.020
Kang, S.-J., Mintz, G. S., Park, D.-W., Lee, S.-W., Kim, Y.-H., Whan Lee, C., et al. (2011). Mechanisms of in-stent restenosis after drug-eluting stent implantation: Intravascular ultrasound analysis. Circ. Cardiovasc. Interv. 4 (1), 9–14. doi:10.1161/CIRCINTERVENTIONS.110.940320
Kashiwagi, M., Kitabata, H., Ozaki, Y., Imanishi, T., and Akasaka, T. (2013). Fatty streak assessed by optical coherence tomography: Early atherosclerosis detection. Eur. Heart J. - Cardiovasc. Imaging 14 (2), 109. doi:10.1093/ehjci/jes182
Kataoka, Y., Kapadia, S. R., Puri, R., Harvey, J. E., Martin, J., Nicholls, S. J., et al. (2012). Suspected hypersensitivity reaction following drug-eluting stent implantation. JACC Cardiovasc. Interv. 5 (7), e21–23. doi:10.1016/j.jcin.2011.12.019
Katsaros, K. M., Kastl, S. P., Zorn, G., Maurer, G., Wojta, J., Huber, K., et al. (2010). Increased restenosis rate after implantation of drug-eluting stents in patients with elevated serum activity of matrix metalloproteinase-2 and -9. JACC Cardiovasc. Interv. 3 (1), 90–97. doi:10.1016/j.jcin.2009.10.023
Katsaros, K. M., Speidl, W. S., Kastl, S. P., Zorn, G., Huber, K., Maurer, G., et al. (2008). Plasminogen activator inhibitor-1 predicts coronary in-stent restenosis of drug-eluting stents. J. Thromb. Haemost. 6 (3), 508–513. doi:10.1111/j.1538-7836.2007.02884.x
Kawano, H., Koide, Y., Baba, T., Nakamizo, R., Toda, G., Takenaka, M., et al. (2004). Granulation tissue with eosinophil infiltration in the restenotic lesion after coronary stent implantation-A case report-. Circ. J. 68 (7), 722–723. doi:10.1253/circj.68.722
Keane, F. M., Morris, S. D., Smith, H. R., and Rycroft, R. J. G. (2001). Allergy in coronary in-stent restenosis. Lancet 357 (9263), 1205–1206. doi:10.1016/s0140-6736(00)04350-6
Kolawole, E. M., McLeod, J. J., Ndaw, V., Abebayehu, D., Barnstein, B. O., Faber, T., et al. (2016). Fluvastatin suppresses mast cell and basophil IgE responses: Genotype-dependent effects. J. Immunol. 196 (4), 1461–1470. doi:10.4049/jimmunol.1501932
Kornowski, R., Hong, M. K., Tio, F. O., Bramwell, O., Wu, H., and Leon, M. B. (1998). In-stent restenosis: Contributions of inflammatory responses and arterial injury to neointimal hyperplasia. J. Am. Coll. Cardiol. 31 (1), 224–230. doi:10.1016/s0735-1097(97)00450-6
Koskinas, K. C., Ughi, G. J., Windecker, S., Tearney, G. J., and Räber, L. (2016). Intracoronary imaging of coronary atherosclerosis: Validation for diagnosis, prognosis and treatment. Eur. Heart J. 37 (6), 524–535a. doi:10.1093/eurheartj/ehv642
Köster, R., Vieluf, D., Kiehn, M., Sommerauer, M., Kähler, J., Baldus, S., et al. (2000). Nickel and molybdenum contact allergies in patients with coronary in-stent restenosis. Lancet 356 (9245), 1895–1897. doi:10.1016/s0140-6736(00)03262-1
Kounis, N. G., Giannopoulos, S., Tsigkas, G. G., and Goudevenos, J. (2012). Eosinophilic responses to stent implantation and the risk of Kounis hypersensitivity associated coronary syndrome. Int. J. Cardiol. 156 (2), 125–132. doi:10.1016/j.ijcard.2011.05.052
Kounis, N. G., Hahalis, G., and Theoharides, T. C. (2007). Coronary stents, hypersensitivity reactions, and the Kounis syndrome. J. Interv. Cardiol. 20 (5), 314–323. doi:10.1111/j.1540-8183.2007.00283.x
Kufner, S., Ernst, M., Cassese, S., Joner, M., Mayer, K., Colleran, R., et al. (2020). 10-Year outcomes from a randomized trial of polymer-free versus durable polymer drug-eluting coronary stents. J. Am. Coll. Cardiol. 76 (2), 146–158. doi:10.1016/j.jacc.2020.05.026
Kunder, C. A., St John, A. L., and Abraham, S. N. (2011). Mast cell modulation of the vascular and lymphatic endothelium. Blood 118 (20), 5383–5393. doi:10.1182/blood-2011-07-358432
Kural, M. H., Wang, J., Gui, L., Yuan, Y., Li, G., Leiby, K. L., et al. (2019). Fas ligand and nitric oxide combination to control smooth muscle growth while sparing endothelium. Biomaterials 212, 28–38. doi:10.1016/j.biomaterials.2019.05.011
Lee, M., Sommerhoff, C. P., von Eckardstein, A., Zettl, F., Fritz, H., and Kovanen, P. T. (2002). Mast cell tryptase degrades HDL and blocks its function as an acceptor of cellular cholesterol. Arterioscler. Thromb. Vasc. Biol. 22 (12), 2086–2091. doi:10.1161/01.atv.0000041405.07367.b5
Lee-Rueckert, M., and Kovanen, P. T. (2006). Mast cell proteases: Physiological tools to study functional significance of high density lipoproteins in the initiation of reverse cholesterol transport. Atherosclerosis 189 (1), 8–18. doi:10.1016/j.atherosclerosis.2006.02.014
McDonald, R. A., Halliday, C. A., Miller, A. M., Diver, L. A., Dakin, R. S., Montgomery, J., et al. (2015). Reducing in-stent restenosis: Therapeutic manipulation of miRNA in vascular remodeling and inflammation. J. Am. Coll. Cardiol. 65 (21), 2314–2327. doi:10.1016/j.jacc.2015.03.549
Messer, R. L. W., Wataha, J. C., Lewis, J. B., Lockwood, P. E., Caughman, G. B., and Tseng, W.-Y. (2005). Effect of vascular stent alloys on expression of cellular adhesion molecules by endothelial cells. J. Long. Term. Eff. Med. Implants 15 (1), 39–48. doi:10.1615/jlongtermeffmedimplants.v15.i1.50
Mintz, G. S., and Guagliumi, G. (2017). Intravascular imaging in coronary artery disease. Lancet 390 (10096), 793–809. doi:10.1016/S0140-6736(17)31957-8
Montone, R. A., Sabato, V., Sgueglia, G. A., and Niccoli, G. (2013). Inflammatory mechanisms of adverse reactions to drug-eluting stents. Curr. Vasc. Pharmacol. 11 (4), 392–398. doi:10.2174/1570161111311040003
Mori, H., Kutys, R., Romero, M., Virmani, R., and Finn, A. V. (2017). Metallic coronary stents: Is there a relationship between stent fracture and hypersensitivity? JACC Cardiovasc. Interv. 10 (11), 1175–1177. doi:10.1016/j.jcin.2017.03.014
Munitz, A., and Levi-Schaffer, F. (2004). Eosinophils: 'new' roles for 'old' cells. Allergy 59 (3), 268–275. doi:10.1111/j.1398-9995.2003.00442.x
Nakajima, Y., Itoh, T., and Morino, Y. (2016). Metal allergy to everolimus-eluting cobalt chromium stents confirmed by positive skin testing as a cause of recurrent multivessel in-stent restenosis. Catheter. Cardiovasc. Interv. 87 (4), E137–E142. doi:10.1002/ccd.26017
Nakazawa, G., Finn, A. V., Vorpahl, M., Ladich, E. R., Kolodgie, F. D., and Virmani, R. (2011). Coronary responses and differential mechanisms of late stent thrombosis attributed to first-generation sirolimus- and paclitaxel-eluting stents. J. Am. Coll. Cardiol. 57 (4), 390–398. doi:10.1016/j.jacc.2010.05.066
Nakazawa, G., Tanabe, K., Aoki, J., Onuma, Y., Higashikuni, Y., Yamamoto, H., et al. (2008). Sirolimus-eluting stents suppress neointimal formation irrespective of metallic allergy. Circ. J. 72 (6), 893–896. doi:10.1253/circj.72.893
Nano, N., Aytekin, A., Ndrepepa, G., Seguchi, M., Bresha, J., Alvarez Covarrubias, H. A., et al. (2022). Periprocedural myocardial injury according to optical characteristics of neointima and treatment modality of in-stent restenosis. Clin. Res. Cardiol. 111 (7), 827–837. doi:10.1007/s00392-022-02024-z
Niccoli, G., Calvieri, C., Minelli, S., Copponi, G., Montone, R. A., Imaeva, A., et al. (2014a). Permanent polymer of drug eluting stents increases eosinophil cationic protein levels following percutaneous coronary intervention independently of C-reactive protein. Atherosclerosis 237 (2), 816–820. doi:10.1016/j.atherosclerosis.2014.11.002
Niccoli, G., Dato, I., Imaeva, A. E., Antonazzo Panico, R., Roberto, M., Burzotta, F., et al. (2014b). Association between inflammatory biomarkers and in-stent restenosis tissue features: An optical coherence tomography study. Eur. Heart J. - Cardiovasc. Imaging 15 (8), 917–925. doi:10.1093/ehjci/jeu035
Niccoli, G., Ferrante, G., Cosentino, N., Conte, M., Belloni, F., Marino, M., et al. (2010a). Eosinophil cationic protein: A new biomarker of coronary atherosclerosis. Atherosclerosis 211 (2), 606–611. doi:10.1016/j.atherosclerosis.2010.02.038
Niccoli, G., Montone, R. A., Ferrante, G., and Crea, F. (2010b). The evolving role of inflammatory biomarkers in risk assessment after stent implantation. J. Am. Coll. Cardiol. 56 (22), 1783–1793. doi:10.1016/j.jacc.2010.06.045
Niccoli, G., Montone, R. A., Sabato, V., and Crea, F. (2018). Role of allergic inflammatory cells in coronary artery disease. Circulation 138 (16), 1736–1748. doi:10.1161/CIRCULATIONAHA.118.035400
Niccoli, G., Schiavino, D., Belloni, F., Ferrante, G., La Torre, G., Conte, M., et al. (2009). Pre-intervention eosinophil cationic protein serum levels predict clinical outcomes following implantation of drug-eluting stents. Eur. Heart J. 30 (11), 1340–1347. doi:10.1093/eurheartj/ehp120
Niccoli, G., Sgueglia, G. A., Conte, M., Cosentino, N., Minelli, S., Belloni, F., et al. (2011). Eosinophil cationic protein and clinical outcome after bare metal stent implantation. Atherosclerosis 215 (1), 166–169. doi:10.1016/j.atherosclerosis.2010.11.044
Niemi, S. M., Fox, J. G., Brown, L. R., and Langer, R. (1985). Evaluation of ethylene-vinyl acetate copolymer as a non-inflammatory alternative to Freund's complete adjuvant in rabbits. Lab. Anim. Sci. 35 (6), 609–612.
Norgaz, T., Hobikoglu, G., Serdar, Z. A., Aksu, H., Alper, A. T., Ozer, O., et al. (2005). Is there a link between nickel allergy and coronary stent restenosis? Tohoku J. Exp. Med. 206 (3), 243–246. doi:10.1620/tjem.206.243
Otsuka, F., Yahagi, K., Ladich, E., Kutys, R., Alexander, R., Fowler, D., et al. (2015). Hypersensitivity reaction in the US food and drug administration-approved second-generation drug-eluting stents: Histopathological assessment with ex vivo optical coherence tomography. Circulation 131 (3), 322–324. doi:10.1161/CIRCULATIONAHA.114.012658
Pfoch, L., Mahler, V., and Sticherling, M. (2009). Drug-eluting coronary stents: Hypersensitivity reactions to paclitaxel. Dermatology 218 (1), 52–55. doi:10.1159/000171817
Picard, M. (2017). Management of hypersensitivity reactions to taxanes. Immunol. Allergy Clin. N. Am. 37 (4), 679–693. doi:10.1016/j.iac.2017.07.004
Rittersma, S. Z., Meuwissen, M., van der Loos, C. M., Koch, K. T., de Winter, R. J., Piek, J. J., et al. (2006). Eosinophilic infiltration in restenotic tissue following coronary stent implantation. Atherosclerosis 184 (1), 157–162. doi:10.1016/j.atherosclerosis.2005.03.049
Roleder, T., Karimi Galougahi, K., Chin, C. Y., Bhatti, N. K., Brilakis, E., Nazif, T. M., et al. (2017). Utility of near-infrared spectroscopy for detection of thin-cap neoatherosclerosis. Eur. Heart J. Cardiovasc. Imaging 18 (6), 663–669. doi:10.1093/ehjci/jew198
Romero-Brufau, S., Best, P. J., Holmes, D. R., Mathew, V., Davis, M. D., Sandhu, G. S., et al. (2012). Outcomes after coronary stent implantation in patients with metal allergy. Circ. Cardiovasc. Interv. 5 (2), 220–226. doi:10.1161/CIRCINTERVENTIONS.111.966614
Saito, T., Hokimoto, S., Oshima, S., Noda, K., Kojyo, Y., and Matsunaga, K. (2009). Metal allergic reaction in chronic refractory in-stent restenosis. Cardiovasc. Revasc. Med. 10 (1), 17–22. doi:10.1016/j.carrev.2008.01.004
Sakai, T., Inoue, S., Matsuyama, T.-A., Takei, M., Ota, H., Katagiri, T., et al. (2009). Eosinophils may Be involved in thrombus growth in acute coronary syndrome histologic examination of aspiration samples. Int. Heart J. 50 (3), 267–277. doi:10.1536/ihj.50.267
Sakamoto, A., Jinnouchi, H., Torii, S., Virmani, R., and Finn, A. V. (2018). Understanding the impact of stent and scaffold material and strut design on coronary artery thrombosis from the basic and clinical points of view. Bioeng. (Basel) 5 (3), 71. doi:10.3390/bioengineering5030071
Shi, G.-P., Bot, I., and Kovanen, P. T. (2015). Mast cells in human and experimental cardiometabolic diseases. Nat. Rev. Cardiol. 12 (11), 643–658. doi:10.1038/nrcardio.2015.117
Shin, H. W., Nam, C. W., Kim, H., Hur, S. H., Kim, Y. N., Kim, K. B., et al. (2013). Zotarolimus-eluting stent-induced hypersensitivity pneumonitis. Korean J. Intern. Med. 28 (1), 108–111. doi:10.3904/kjim.2013.28.1.108
Shlofmitz, E., Iantorno, M., and Waksman, R. (2019). Restenosis of drug-eluting stents: A new classification system based on disease mechanism to guide treatment and state-of-the-art review. Circ. Cardiovasc. Interv. 12 (8), e007023. doi:10.1161/CIRCINTERVENTIONS.118.007023
Siontis, G. C. M., Stefanini, G. G., Mavridis, D., Siontis, K. C., Alfonso, F., Pérez-Vizcayno, M. J., et al. (2015). Percutaneous coronary interventional strategies for treatment of in-stent restenosis: A network meta-analysis. Lancet 386 (9994), 655–664. doi:10.1016/S0140-6736(15)60657-2
Slodownik, D., Danenberg, C., Merkin, D., Swaid, F., Moshe, S., Ingber, A., et al. (2018). Coronary stent restenosis and the association with allergy to metal content of 316L stainless steel. Cardiovasc. J. Afr. 29 (1), 43–45. doi:10.5830/CVJA-2017-036
Soliman, A. M., Tolba, S. A., Sharafeldin, I. M., Gepreel, M. A., and Allam, N. K. (2019). Ni-free, built-in nanotubular drug eluting stents: Experimental and theoretical insights. Mater. Sci. Eng. C 103, 109750. doi:10.1016/j.msec.2019.109750
Steffel, J., Latini, R. A., Akhmedov, A., Zimmermann, D., Zimmerling, P., Lüscher, T. F., et al. (2005). Rapamycin, but not FK-506, increases endothelial tissue factor expression: Implications for drug-eluting stent design. Circulation 112 (13), 2002–2011. doi:10.1161/circulationaha.105.569129
Steffel, J., and Tanner, F. C. (2007). Biological effects of drug-eluting stents in the coronary circulation. Herz 32 (4), 268–273. doi:10.1007/s00059-007-3000-5
Strohbach, A., and Busch, R. (2015). Polymers for cardiovascular stent coatings. Int. J. Polym. Sci. 2015, 1–11. doi:10.1155/2015/782653
Svedman, C., Ekqvist, S., Möller, H., Björk, J., Pripp, C.-M., Gruvberger, B., et al. (2009). A correlation found between contact allergy to stent material and restenosis of the coronary arteries. Contact Dermat. 60 (3), 158–164. doi:10.1111/j.1600-0536.2008.01502.x
Takashima, A., Shimabukuro, M., Tabata, M., Fukuda, D., Uematsu, E., Ishibashi-Ueda, H., et al. (2015). Histopathological heterogeneity of in-stent restenosis in four coronary endarterectomy specimens. Cardiovasc. Pathol. 24 (3), 194–197. doi:10.1016/j.carpath.2014.11.002
Tardif, J.-C., L'Allier, P. L., Ibrahim, R., Grégoire, J. C., Nozza, A., Cossette, M., et al. (2010). Treatment with 5-lipoxygenase inhibitor VIA-2291 (Atreleuton) in patients with recent acute coronary syndrome. Circ. Cardiovasc. Imaging 3 (3), 298–307. doi:10.1161/CIRCIMAGING.110.937169
Taruya, A., Tanaka, A., Nishiguchi, T., Matsuo, Y., Ozaki, Y., Kashiwagi, M., et al. (2015). Vasa vasorum restructuring in human atherosclerotic plaque vulnerability: A clinical optical coherence tomography study. J. Am. Coll. Cardiol. 65 (23), 2469–2477. doi:10.1016/j.jacc.2015.04.020
Thyssen, J. P., Engkilde, K., Menne, T., Johansen, J. D., Hansen, P. R., and Gislason, G. H. (2011). No association between metal allergy and cardiac in-stent restenosis in patients with dermatitis-results from a linkage study. Contact Dermat. 64 (3), 138–141. doi:10.1111/j.1600-0536.2010.01857.x
Tonino, P. A. L., Pijls, N. H. J., Collet, C., Nammas, W., Van der Heyden, J., Romppanen, H., et al. (2020). Titanium-nitride-oxide-coated versus everolimus-eluting stents in acute coronary syndrome: The randomized TIDES-ACS trial. JACC Cardiovasc. Interv. 13 (14), 1697–1705. doi:10.1016/j.jcin.2020.04.021
Torii, S., Jinnouchi, H., Sakamoto, A., Kutyna, M., Cornelissen, A., Kuntz, S., et al. (2020). Drug-eluting coronary stents: Insights from preclinical and pathology studies. Nat. Rev. Cardiol. 17 (1), 37–51. doi:10.1038/s41569-019-0234-x
Torrado, J., Buckley, L., Duran, A., Trujillo, P., Toldo, S., Valle Raleigh, J., et al. (2018). Restenosis, stent thrombosis, and bleeding complications: Navigating between Scylla and charybdis. J. Am. Coll. Cardiol. 71 (15), 1676–1695. doi:10.1016/j.jacc.2018.02.023
van Hemert, N. D., Voskuil, M., Rozemeijer, R., Stein, M., Frambach, P., Pereira, B., et al. (2021). 3-Year clinical outcomes after implantation of permanent-polymer versus polymer-free stent: ReCre8 landmark analysis. JACC Cardiovasc. Interv. 14 (22), 2477–2486. doi:10.1016/j.jcin.2021.08.078
Virmani, R., Farb, A., Guagliumi, G., and Kolodgie, F. D. (2004a). Drug-eluting stents: Caution and concerns for long-term outcome. Coron. Artery Dis. 15 (6), 313–318. doi:10.1097/00019501-200409000-00003
Virmani, R., Guagliumi, G., Farb, A., Musumeci, G., Grieco, N., Motta, T., et al. (2004b). Localized hypersensitivity and late coronary thrombosis secondary to a sirolimus-eluting stent: Should we be cautious? Circulation 109 (6), 701–705. doi:10.1161/01.CIR.0000116202.41966.D4
Walpoth, B. H., and Hess, O. M. (2004). Late coronary thrombosis secondary to a sirolimus-eluting stent. Circulation 110 (11), e309. doi:10.1161/01.cir.0000141422.05934.dc
Walpoth, B. H., Pavlicek, M., Celik, B., Nicolaus, B., Schaffner, T., Althaus, U., et al. (2001). Prevention of neointimal proliferation by immunosuppression in synthetic vascular grafts. Eur. J. Cardio-Thoracic Surg. 19 (4), 487–492. doi:10.1016/s1010-7940(01)00582-6
Wang, J., Sjöberg, S., Tia, V., Secco, B., Chen, H., Yang, M., et al. (2013). Pharmaceutical stabilization of mast cells attenuates experimental atherogenesis in low-density lipoprotein receptor-deficient mice. Atherosclerosis 229 (2), 304–309. doi:10.1016/j.atherosclerosis.2013.05.025
Welt, F. G. P., and Rogers, C. (2002). Inflammation and restenosis in the stent era. Arterioscler. Thromb. Vasc. Biol. 22 (11), 1769–1776. doi:10.1161/01.atv.0000037100.44766.5b
Wheatcroft, S., Byrne, J., Thomas, M., and MacCarthy, P. (2006). Life-threatening coronary artery spasm following sirolimus-eluting stent deployment. J. Am. Coll. Cardiol. 47 (9), 1911–1912. doi:10.1016/j.jacc.2006.02.017
Yang, L., Froio, R. M., Sciuto, T. E., Dvorak, A. M., Alon, R., and Luscinskas, F. W. (2005). ICAM-1 regulates neutrophil adhesion and transcellular migration of TNF-alpha-activated vascular endothelium under flow. Blood 106 (2), 584–592. doi:10.1182/blood-2004-12-4942
Yin, R. X., Yang, D. Z., and Wu, J. Z. (2014). Nanoparticle drug- and gene-eluting stents for the prevention and treatment of coronary restenosis. Theranostics 4 (2), 175–200. doi:10.7150/thno.7210
Yokouchi, Y., Oharaseki, T., Ihara, F., Naoe, S., Sugawara, S., and Takahashi, K. (2010). Repeated stent thrombosis after DES implantation and localized hypersensitivity to a stent implanted in the distal portion of a coronary aneurysm thought to be a sequela of kawasaki disease: Autopsy report. Pathol. Int. 60 (2), 112–118. doi:10.1111/j.1440-1827.2009.02484.x
Keywords: in-stent restenosis, hypersensitivity, drug-eluting stent, eosinophils, stainless steel
Citation: Hu W and Jiang J (2022) Hypersensitivity and in-stent restenosis in coronary stent materials. Front. Bioeng. Biotechnol. 10:1003322. doi: 10.3389/fbioe.2022.1003322
Received: 26 July 2022; Accepted: 16 August 2022;
Published: 15 September 2022.
Edited by:
Yingfei Xue, Columbia University, United StatesReviewed by:
Prashanth Ravishankar, Namida Lab, Inc., United StatesCopyright © 2022 Hu and Jiang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jun Jiang, amlhbmctanVuQHpqdS5lZHUuY24=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.