
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Big Data, 06 February 2023
Sec. Medicine and Public Health
Volume 6 - 2023 | https://doi.org/10.3389/fdata.2023.1095119
This article is part of the Research TopicPerspectives in Digital Health and Big Data in Medicine: Current Trends, Professional Challenges, and Ethical, Legal, and Social ImplicationsView all 24 articles
 Christi J. Guerrini1*†
Christi J. Guerrini1*† Mary A. Majumder1†
Mary A. Majumder1† Jill O. Robinson1
Jill O. Robinson1 Robert Cook-Deegan2
Robert Cook-Deegan2 Matthew Blank1
Matthew Blank1 Juli Bollinger1
Juli Bollinger1 Janis Geary2
Janis Geary2 Amanda M. Gutierrez1
Amanda M. Gutierrez1 Maya Shrikant1
Maya Shrikant1 Amy L. McGuire1
Amy L. McGuire1As entities around the world invest in repositories and other infrastructure to facilitate health data sharing, scalable solutions to data sharing challenges are needed. We conducted semi-structured interviews with 24 experts to explore views on potential issues and policy options related to health data sharing. In this Perspective, we describe and contextualize unconventional insights shared by our interviewees relevant to issues in five domains: data quality, privacy, equity, incentives, and sustainability. These insights question a focus on granular quality metrics for gatekeeping; challenge enthusiasm for maximalist risk disclosure practices; call attention to power dynamics that potentially compromise the patient's voice; encourage faith in the sharing proclivities of new generations of scientists; and endorse accounting for personal disposition in the selection of long-term partners. We consider the merits of each insight with the broad goal of encouraging creative thinking to address data sharing challenges.
It is widely agreed that sharing health data will translate to benefits for patients and populations and is critical to the advancement of science (Institute of Medicine of the National Academies, 2013; Editorial, 2020; Whicher et al., 2021). The widely cited and endorsed FAIR Guiding Principles provide an invaluable foundation for data management and stewardship (Wilkinson et al., 2016). However, technical, motivational, and policy barriers to sharing health data for secondary research persist [National Academies of Sciences, Engineering, and Medicine (NASEM), 2018]. As public and private entities increase investments in repositories and other infrastructure to facilitate health data sharing, scalable approaches to overcoming these barriers are urgently needed (Institute of Medicine of the National Academies, 2013; Whicher et al., 2021).
Addressing this need, we conducted a modified policy Delphi process to identify and prioritize issues and policy options related to sharing cancer-gene variant data (Majumder et al., 2021). Cancer genomics was the focus of our research given the field's significant efforts to make large-scale data sets available for secondary research with the objective of, among other things, resolving problems concerning variants of uncertain significance (The Clinical Cancer Genome Task Team of the Global Alliance for Genomics and Health, 2017). In the first three Delphi rounds, panelists prioritized issues and generated potential options that we categorized into five domains: data quality, privacy and security, equity, incentives, and sustainability. To broaden the range of perspectives considered by panelists in the final Delphi round, we conducted semi-structured interviews with 24 experts who did not participate in the Delphi process (Table 1). Methods for recruiting interviewees, conducting interviews, and analyzing interview data are described in Supplementary material.
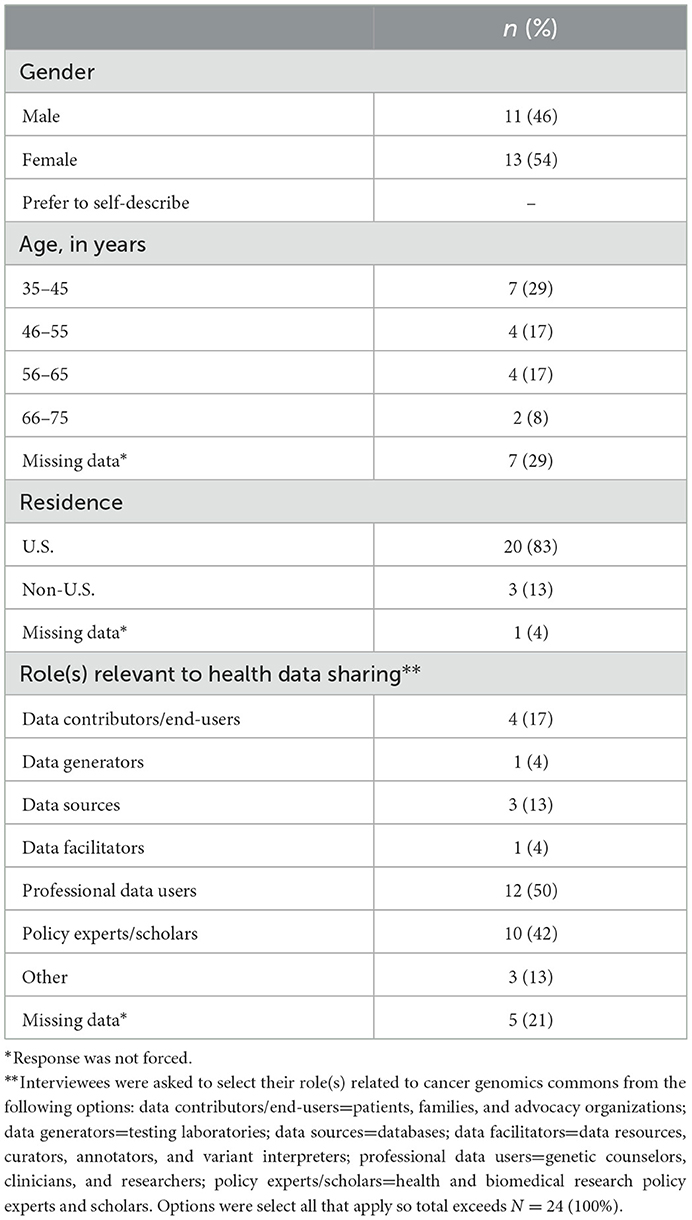
Table 1. Characteristics of interview participants (N = 24).
In this Perspective, we describe and contextualize select insights of interviewees on data sharing that we found intriguing and generated rich discussion among our research team (Table 2). Importantly, these insights are not limited to cancer genomics but are relevant to any efforts to share health data. We do not claim that these perspectives have never before been aired, but because they depart (in some cases significantly) from conventional thinking, we refer to them as “fresh takes.” Although some might be controversial, we believe each has sufficient merit to justify exploration. More generally, by airing these fresh takes, we aim to encourage consideration of novel approaches to sharing health data.
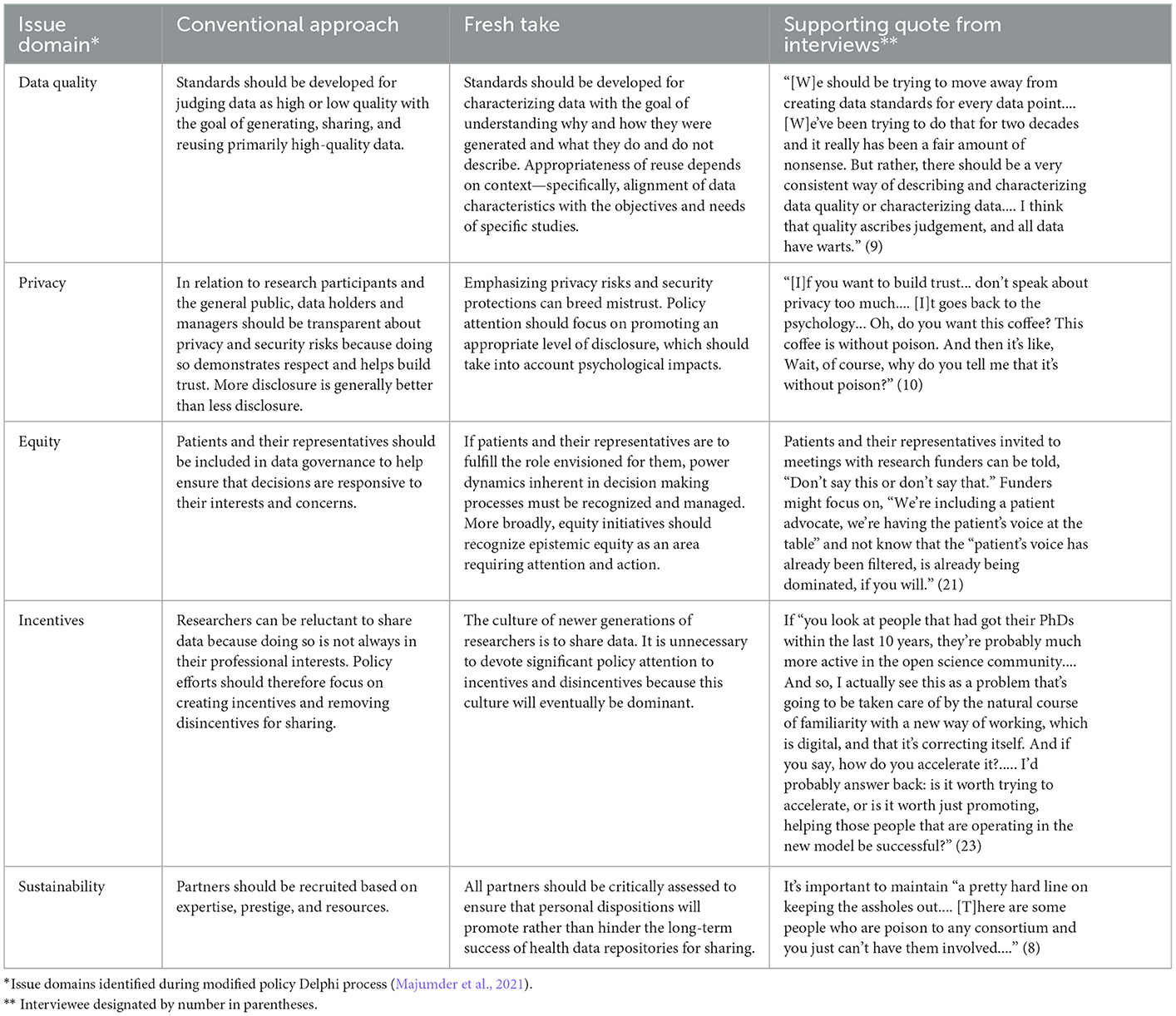
Table 2. Insights on health data sharing issues shared by interviewees (N = 24).
The first fresh take focuses on the consequences of sharing data judged to be low quality. The conventional approach is to develop standards by which to designate data as high or low quality with the goal of generating, sharing, and reusing primarily high-quality data. One interviewee, however, worried about generalized use of metrics to expunge or block data from repositories, based on a judgment that they are low-quality according to those metrics, because “all data have warts.” Depending on the specific objectives and needs of studies that might reuse data, the interviewee suggested, a data set's particular blemishes might not be significant or even relevant. To help researchers make decisions about reusing data, standards should therefore be developed for characterizing why and how the data were generated, and what they do and do not describe, to promote understanding of their strengths and limitations for specific secondary use contexts.
Consistent with the notion of quality as fitness for use, information systems professionals have described quality dimensions from the perspective of data users that include extrinsic indicators of contextual appropriateness, such as relevance to the task at hand and completeness, in addition to intrinsic indicators, such as accuracy (Wang and Strong, 1996). Medical researchers also recognize that annotation of data facilitates reuse, but data quality frameworks generally focus on development of and compliance with quality standards or metrics. In a systematic review of frameworks for data sharing within consortium-wide platforms for international health research, for example, principles and norms for data sharing included development and implementation of quality standards or threshold metrics (Kalkman et al., 2019). Our interviewee's unconventional insight is that the “play books” of primary researchers—e.g., the rich, narrative descriptions of how the data were originally generated, coded, and interrogated (Bauchner et al., 2016)—are as or even more useful to secondary researchers than granular quality metrics, especially those focused on identifying and quantifying quality “defects” as a basis for exclusion from the data commons. More broadly, it is worth considering whether use of the term “quality” promotes simplistic judgements about data that discourage appropriate reuse.
The second fresh take concerns research participants' privacy and challenges with keeping their data confidential once shared. Because it is usually impossible to guarantee that data will never come into the possession of unauthorized persons or be used for unauthorized purposes, including reidentification, the conventional wisdom is that disclosing more information about privacy risks is generally better than less. Transparency is also believed to promote trust. One of our interviewees, however, argued that privacy-related disclosures can have the opposite effect by arousing suspicion. By analogy, the interviewee described a neighborhood coffee shop that assures customers its coffee is poison-free. Because customers do not normally wonder whether their coffee is laced with arsenic, the assurance causes customers to worry and ask, “Wait... why do you tell me that it's without poison?” The interviewee therefore advised, “if you want to build trust... don't speak about privacy too much.”
A recent study suggests that members of the public who are open to donating their health data for research believe that transparency about how their data are used would help them trust the data-sharing enterprise (Milne et al., 2021). However, people's views and behaviors around privacy and related trade-offs are more uncertain, malleable, and context-dependent than is often recognized (Acquisti et al., 2015). Indeed, limited attention, “motivated attention” away from unpleasant information, and biased assessments of probability can diminish or even reverse intended effects of privacy-related disclosures (Loewenstein et al., 2014). Further, groups can have different levels of pre-existing concern about privacy that influence how disclosures affect trust. Still, some advocates for disclosure may appeal to considerations such as respect as justification for transparency regardless of any effects on trust (McGuire et al., 2019). In sum, many factors complicate the relationship between disclosures and their impact on trust and accountability (Loewenstein et al., 2014). The nugget of wisdom here is to be curious about and account for human psychology when obtaining consent for sharing health data and beware of unreflective disclosure maximalism.
The third fresh take is in the domain of equity. Increasing diversity and sensitivity to the needs and concerns of patients and communities have recently been articulated as priorities in biomedical research (Aguilar-Gaxiola et al., 2022). Consistent with these priorities, some have championed biobank and data repository systems and processes that engage the general public, patients, and patient representatives in data governance (O'Doherty et al., 2011; Kaye et al., 2018; McGuire et al., 2019). But one of our interviewees cautioned that “having the patient's voice at the table” is not in itself sufficient to achieve equity. This is due to inherent power differences between patients and researchers—who may also be treating physicians. We might expect those desperate for help to avoid doing anything that might alienate those researchers. Thus, the interviewee observed, patients might not use their authentic voices—and might even simply parrot what researchers tell them to say—when invited to the table.
The interviewee's concerns are relevant to what Miranda Fricker calls epistemic injustice (Fricker, 2003). Epistemic injustice can occur when a hearer (e.g., physician or researcher) assigns lower credibility to a speaker (e.g., patient or caregiver) as a result of a prejudice stemming from differences of social identity, especially where the differences are characterized by unequal power between the hearer and the speaker (Fricker, 2003). It can also occur preemptively when the speaker remains silent out of fear of not being believed (Lee, 2021). Our interviewee's novel insight is that such silencing can occur out of fear of disrupting existing relationships as a result of being believed. Therefore, to protect against the (sometimes unintentional) filtering or dominance of the patient's voice, upstream solutions are needed to better identify and manage relevant power dynamics. For example, data governance can be structured to require the input of many patients and caregivers, rather than just a few.
The fourth fresh take addresses the misalignment of data sharing with researchers' professional incentives. The conventional approach to this well-known problem is to reward data sharing, reduce professional incentives for data hoarding, and enshrine data sharing as an institutional and cultural norm. There are many examples of efforts that have adopted this approach, including the use of sharing badges by journals and data advertising by consortia to enhance the visibility of data sets and reputational credit of their creators (Devriendt et al., 2021). One of our interviewees, however, wondered whether these approaches are necessary given the popularity of open science norms among scientists who have pursued advanced degrees “within the last 10 years.” They explained: “I actually see this as a problem that's going to be taken care of by the natural course of familiarity with a new way of working, which is digital, and that it's correcting itself.” To those asking how to accelerate this change, the interviewee continued, “I'd probably answer back: is it worth trying to accelerate, or is it worth just promoting, helping those people that are operating in the new model be successful?”
Because incentive-related barriers to health data sharing have proven especially tricky to overcome, the wait-it-out approach endorsed by this interviewee has undeniable appeal. It is also true that there is broad enthusiasm for open science, as evidenced by global initiatives to facilitate access to research data, methods, and products [National Academies of Sciences, Engineering, and Medicine (NASEM), 2018]. Yet, one survey of over 1,300 scientists found that, compared to their older colleagues, younger scientists were less willing to share their research data without restriction, although they were more likely to agree that lack of access to data is a major impediment to progress in science and has restricted their ability to answer scientific questions (Tenopir et al., 2011). Other scholars attribute this finding to competitive pressures that are likely experienced more intensely by non-tenured scientists compared to their tenured colleagues (Fecher et al., 2015). More generally, the literature suggests that incentives and norms should move in the same direction to sustain behavior (Nicholas et al., 2019), and so it does not seem wise to disinvest in incentives for data sharing. Still, the interviewee's insight is useful in thinking about how to maximize the impact of those investments: instead of working to change the behaviors of a resistant old guard, focus on supporting new generations of scientists who might be more receptive to sharing.
The final fresh take concerns the financial and human resource challenges associated with maintaining data repositories and sharing programs. A standard approach to promoting sustainability is to partner with individuals and institutions based on their access to resources, as well as their expertise and prestige, which can help attract external funding. But one of our interviewees recommended including an additional screen for personal disposition. Specifically, they explained, it is important to maintain “a pretty hard line on keeping the assholes out.” The interviewee elaborated: “[T]here are some people who are poison to any consortium and you just can't have them involved.”
Following publication of Sutton's (2004, 2007) landmark Harvard Business Review essay in 2004 and follow-on book in 2007, the “no asshole rule” has become well-known in management circles. This rule is intended to protect organizational culture by denying entry (usually in the form of employment) to even high-achieving individuals if they are known to exhibit abusive or other difficult behavior. The interviewee's novel insight was recognizing its relevance beyond business hiring contexts and applying it to decisions about partners in long-term and large-scale scientific collaborations. The move provokes a broader question: what other lessons about long-term operational success might data sharing efforts glean from the business management literature?
Given the intractability of issues associated with developing and sustaining repositories and other infrastructure to facilitate health data sharing, we believe it is worth paying attention to these and other unconventional perspectives. They have the potential to generate new and better solutions by drawing from literature in different fields, highlighting edge and hidden cases, and even reframing the problems. While not every fresh take will ultimately be useful to efforts to promote health data sharing, soliciting and airing them can help ensure that this work is conducted in ways that are open-minded and creative.
The data presented in this article are not readily available due to the confidential nature of interviewees' participation and consistent with the IRB-approved protocol for this study. Requests to access the data should be directed to Z3VlcnJpbmlAYmNtLmVkdQ==.
The studies involving human participants were reviewed and approved by Baylor College of Medicine Institutional Review Board. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
AM, CG, MM, and JR conceived of and designed this study. CG, MM, RC-D, JB, JG, and AG participated in data collection with support provided by JR and MB. CG, MM, JR, MB, and MS analyzed the data. CG, MM, and JR led the drafting of this manuscript. Funding for this research was obtained by RC-D and AM. All authors contributed to the article and approved the submitted version.
This research was supported by the National Cancer Institute of the National Institutes of Health under Award Number R01 CA237118.
The authors would like to thank Amira Daoud for their work supporting preparation of the manuscript and the interviewees for sharing their insights and opinions with us.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The content is solely the responsibility of the authors and does not represent the views of the National Institutes of Health, the authors' employers, or any institutions with which they are or have been affiliated.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fdata.2023.1095119/full#supplementary-material
Acquisti, A., Brandimarte, L., and Loewenstein, G. (2015). Privacy and human behavior in the age of information. Science 347, 509–514. doi: 10.1126/science.aaa1465
Aguilar-Gaxiola, S., Ahmed, S. M., Anise, A., Azzahir, A., Baker, K. E., Cupito, A., et al. (2022). Assessing meaningful community engagement: a conceptual model to advance health equity through transformed systems for health. NAM Perspect. doi: 10.31478/202202c
Bauchner, H., Golub, R. M., and Fontanarosa, P. B. (2016). Data sharing: an ethical and scientific imperative. JAMA 315, 1237–1239. doi: 10.1001/jama.2016.2420
Devriendt, T., Shabani, M., and Borry, P. (2021). Data sharing in biomedical sciences: a systematic review of incentives. Biopreserv. Biobank. 19, 219–227. doi: 10.1089/bio.2020.0037
Fecher, B., Friesike, S., and Hebing, M. (2015). What drives academic data sharing? PLoS ONE. 10, e0118053. doi: 10.1371/journal.pone.0118053
Fricker, M. (2003). Epistemic justice and a role for virtue in the politics of knowing. Metaphil. 34, 154–173. doi: 10.1111/1467-9973.00266
Institute of Medicine of the National Academies. (2013). Sharing Clinical Research Data: Workshop Summary. Washington, D.C.: National Academies Press.
Kalkman, S., Mostert, M., Gerlinger, C., van Delden, J. J. M., and van Thiel, G. J. M. W. (2019). Responsible data sharing in international health research: a systematic review of principles and norms. BMC Med. Ethics. 20, 21. doi: 10.1186/s12910-019-0359-9
Kaye, J., Terry, S. F., Juengst, E., Coy, S., Harris, J. R., Chalmers, D., et al. (2018). Including all voices in international data-sharing governance. Hum. Genomics. 12, 13. doi: 10.1186/s40246-018-0143-9
Lee, J. Y. (2021). Anticipatory epistemic injustice. Soc. Epistemol. 35, 564–576. doi: 10.1080/02691728.2021.1924306
Loewenstein, G., Sunstein, C. R., and Golman, R. (2014). Disclosure: psychology changes everything. Annu. Rev. Econ. 6, 391–419. doi: 10.1146/annurev-economics-080213-041341
Majumder, M. A., Blank, M. L., Geary, J., Bollinger, J. M., Guerrini, C. J., Robinson, J. O., et al. (2021). Challenges to building a gene variant commons to assess hereditary cancer risk: results of a modified policy Delphi panel deliberation. J. Pers. Med. 11, 646. doi: 10.3390/jpm11070646
McGuire, A. L., Majumder, M. A., Villanueva, A. G., Bardill, J., Bollinger, J. M., Boerwinkle, E., et al. (2019). Importance of participant-centricity and trust for a sustainable medical information commons. J. Law Med. Ethics. 47, 12–20. doi: 10.1177/1073110519840480
Milne, R., Morley, K. I., Almarri, M. A., Anwer, S., Atutornu, J., Baranova, E. E., et al. (2021). Demonstrating trustworthiness when collecting and sharing genomic data: public views across 22 countries. Genome Med. 13, 92. doi: 10.1186/s13073-021-00903-0
National Academies of Sciences Engineering, and Medicine (NASEM). (2018). Open Science by Design: Realizing a Vision for 21st Century Research. Washington, D.C.: National Academies Press.
Nicholas, D., Boukacem-Zeghmouri, C., Abrizah, A., Rodriquez-Bravo, B., Xu, J., Swigon, M., et al. (2019). Open science from the standpoint of the new wave of researchers: views from the scholarly frontline. Inf. Serv. Use. 39, 369–374. doi: 10.3233/ISU-190069
O'Doherty, K. C., Burgess, M. M., Edwards, K., Gallagher, R. P., Hawkins, A. K., Kaye, J., et al. (2011). From consent to institutions: designing adaptive governance for genomic biobanks. Soc. Sci. Med. 73, 367–374. doi: 10.1016/j.socscimed.2011.05.046
Sutton, R. (2004). More trouble than they're worth. Harv. Bus. Rev. 82, 19–20. doi: 10.1109/EMR.2004.25045
Sutton, R. (2007). The No Asshole Rule: Building a Civilized Workplace and Surviving One That Isn't. New York: Warner Business Books.
Tenopir, C., Allard, S., Douglass, K., Aydinoglu, A. U., Wu, L., Read, E., et al. (2011). Data sharing by scientists: practices and perceptions. PLoS ONE. 6, e21101. doi: 10.1371/journal.pone.0021101
The Clinical Cancer Genome Task Team of the Global Alliance for Genomics and Health. (2017). Sharing clinical and genomic data on cancer—the need for global solutions. N. Engl. J. Med. 376, 2006–2009. doi: 10.1056/NEJMp1612254
Wang, R. Y., and Strong, D. M. (1996). Beyond accuracy: what data quality means to data consumers. J. Manag. Inf. Syst. 12, 5–33. doi: 10.1080/07421222.1996.11518099
Whicher, D., Ahmed, M., Siddiqi, S., Adams, I., Zirkle, M., Grossmann, C., et al. (2021). Health Data Sharing to Support Better Outcomes: Building a Foundation of Stakeholder Trust. Washington, D.C.: National Academy of Medicine.
Keywords: data sharing, data quality, ethics, data privacy, data archives
Citation: Guerrini CJ, Majumder MA, Robinson JO, Cook-Deegan R, Blank M, Bollinger J, Geary J, Gutierrez AM, Shrikant M and McGuire AL (2023) Fresh takes on five health data sharing domains: Quality, privacy, equity, incentives, and sustainability. Front. Big Data 6:1095119. doi: 10.3389/fdata.2023.1095119
Received: 10 November 2022; Accepted: 16 January 2023;
Published: 06 February 2023.
Edited by:
João Valente Cordeiro, New University of Lisbon, PortugalReviewed by:
Rob Hooft, Dutch Techcentre for Life Sciences, NetherlandsCopyright © 2023 Guerrini, Majumder, Robinson, Cook-Deegan, Blank, Bollinger, Geary, Gutierrez, Shrikant and McGuire. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christi J. Guerrini,  Z3VlcnJpbmlAYmNtLmVkdQ==
Z3VlcnJpbmlAYmNtLmVkdQ==
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.