
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Behav. Neurosci. , 09 February 2023
Sec. Emotion Regulation and Processing
Volume 17 - 2023 | https://doi.org/10.3389/fnbeh.2023.1111349
This article is part of the Research Topic Gut-Microbiota-Brain Axis in Depression: Mechanisms and Possible Therapies View all 5 articles
 Evan Forth1,2,3*
Evan Forth1,2,3* Benjamin Buehner2
Benjamin Buehner2 Ana Storer2
Ana Storer2 Cassandra Sgarbossa1,2,3
Cassandra Sgarbossa1,2,3 Roumen Milev1,2,3,4
Roumen Milev1,2,3,4 Arthi Chinna Meyyappan1,2,3
Arthi Chinna Meyyappan1,2,3Introduction: Many psychiatric illnesses have been linked to the gut microbiome, with supplements such as probiotics showing some efficacy in alleviating the symptoms of some psychiatric illnesses. The aim of this review is to evaluate the current literature investigating the effects of adjuvant probiotic or synbiotic administration in combination with first-line treatments for psychiatric illnesses.
Method: A systematic search of four databases was conducted using key terms related to treatments for psychiatric illnesses, the gut microbiome, and probiotics. All results were then evaluated based on specific eligibility criteria.
Results: Eight studies met eligibility criteria and were analyzed for reported changes in outcome measures used to assess the symptoms of psychiatric illness and the tolerability of treatment. All Major Depressive Disorder (MDD) (n = 5) and Generalized Anxiety Disorder (GAD) (n = 1) studies found adjuvant probiotic or synbiotic treatment to be more efficacious in improving the symptoms of psychiatric illness than the first-line treatment alone or with placebo. The schizophrenia studies (n = 2) found adjuvant probiotic treatment to have no significant difference in clinical outcomes, but it was found to improve the tolerability of first-line antipsychotics.
Discussion and conclusion: The findings of the studies included in this review suggest the use of adjuvant probiotic treatment with selective serotonin reuptake inhibitors (SSRIs) for MDD and GAD to be superior to SSRI treatment alone. Probiotic adjuvant treatment with antipsychotics could be beneficial for improving the tolerability of the antipsychotics, but these findings do not suggest that adjuvant probiotic treatment would result in improved clinical outcomes for symptoms of schizophrenia.
The human gastrointestinal (GI) tract houses trillions of microorganisms, which have co-evolved with their host and collectively contain over 100 times as many genes as the human genome (Bermon et al., 2015). Colonization of the gut begins at birth, being influenced by the mode of delivery and breastfeeding (Martin et al., 2016) and through the gut’s microbial composition somewhat stabilizes throughout adulthood, factors such as the environment, diet, medication, genetics, and age continue to shape microbiota composition and function throughout one’s life (Li et al., 2014; Heiman and Greenway, 2016; Odamaki et al., 2016; Cussotto et al., 2019). There is a well-established, bidirectional connection between the gut microbiome and the brain, known as the gut-brain-axis (GBA). This communication includes portions of the sympathetic and the parasympathetic nervous system, the enteric nervous system, as well as both neuroimmune and neuroendocrine signaling (Cryan et al., 2019; Morais et al., 2021; Liu et al., 2022). Research suggests that the GBA may influence a variety of neurological functions, including the pathology of psychiatric disorders.
Major Depressive Disorder (MDD), Generalized Anxiety Disorder (GAD) and Schizophrenia (SZ) are widely known and severe psychiatric disorders. MDD is characterized by pervasive depressed mood and/or loss of interest or pleasure, along with an array of other possible psychiatric and physiological symptoms, and is the leading cause of disability worldwide (Evans-Lacko et al., 2018). GAD has a similarly significant impairment in daily functioning (American Psychiatric Association [APA], 2013), and is characterized by a persistent, exaggerated worry about everyday events. MDD and GAD are also somewhat gendered illnesses, with the prevalence in women being reported as 1.5 to 3 times that of men (Vesga-López et al., 2008; Sabic et al., 2021). Antidepressant medications such as selective serotonin reuptake inhibitors (SSRIs) are considered a first-line therapy for MDD and GAD (Gelenberg et al., 2010; Baldwin et al., 2011). SZ is a highly heterogenous psychotic disorder, characterized by continuous or relapsing episodes of positive symptoms like delusions, hallucinations and irrational thoughts or actions, and negative symptoms like lethargy, apathy, and social withdrawal. Second-generation antipsychotics are considered the first-line treatment for SZ (Patel et al., 2014). Gender differences found in schizophrenia are less consistent, with some reports of equal prevalence between men and women, and some reports of increased prevalence among men (Ochoa et al., 2012).
Various studies have found the microbiota composition of patients with these psychiatric disorders to be significantly different from those of healthy controls (Zhu et al., 2020; Nikolova et al., 2021). Interestingly, fecal microbiota transplants from psychiatric patients to germ-free rodents have been shown to induce symptoms similar to those associated with the disorders of the donors (Bercik et al., 2011; Neufeld et al., 2011). Certain probiotics or fecal microbiota transplants from healthy patients have also helped alleviate symptoms and induced positive outcomes in patients with psychiatric disorders (Meyyappan et al., 2020; Johnson et al., 2021). As such, there is emerging evidence to suggest that the gut microbiome and the GBA play a crucial role in inducing and modulating psychiatric disorders.
A significant subset of patients affected by these disorders are treatment-resistant or experience adverse effects when taking antidepressants or antipsychotics. Antipsychotic usage is commonly associated with adverse metabolic and endocrine effects such as weight gain and insulin resistance (De Hert et al., 2011), while SSRIs frequently induce unpleasant side effects such as nausea, insomnia, drowsiness and agitation (Hirsch and Birnbaum, 2017). Such adverse effects contribute to low treatment compliance and tolerability. Low compliance and inconsistent efficacy indicate that there is a need to explore alternative treatments, or approaches to counteract these unwanted side effects.
Interestingly, both antipsychotics and antidepressants have been found to have antimicrobial properties (Munoz-Bellido et al., 2000; Maier et al., 2018). It is thought that such psychotropic medications can modulate the gut microbiome, and consequently influence the GBA. Whether the therapeutic benefits or the adverse effects of these medications are influenced, in part, by their impact on the GBA remains to be determined, however, several recent studies have indicated that the gut microbiome composition could be used as a biomarker to predict pharmacological treatment outcomes (responders versus treatment resistance) in MDD and SZ (Fontana et al., 2020; Ciocan et al., 2021; Yuan et al., 2021). This suggests that the GBA could play a significant role in the efficacy and tolerability of psychotropic medication. This evidence, combined with the aforementioned therapeutic benefits of microbiome modulation on psychiatric disorders, and the proven ability of probiotics to normalize metabolic issues (Le Barz et al., 2015), suggest that combining psychotropic medication with gut microbiome targeting treatments could have beneficial results. The aim of this systematic review is to evaluate the current literature investigating the effect of adjuvant probiotic or synbiotic (a combination of probiotics and prebiotics) treatment on clinical outcomes and tolerability of first-line psychotropic treatments. We conducted this systematic review as a means to gather scientific evidence and provide a comprehensive and current overview of this topic.
This review was carried out according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Figure 1; Moher et al., 2009). A systematic search was conducted using 4 databases (MEDLINE, EMBASE, PsycINFO, and Web of Science) to identify relevant studies using the following search terms:(antidepressant OR selective serotonin reuptake inhibitors, SSRI OR SNRI OR TCA OR MAOI OR anti-anxiety drugs OR anxiolytics OR benzodiazepines OR beta-blockers OR antipsychotic medication OR mood stabilizer) AND (microbiome OR microbiota OR gut bacteria OR intestinal bacteria OR dysbiosis OR bacteriostatic OR bactericidal OR antibiotic OR bacterial therapy OR bacteriotherapy OR psychobiotic OR microbial therapy OR fecal microbiota transplant OR probiotic) AND (depression OR depressive disorder OR major depression OR bipolar OR mood disorders OR affective disorders OR stress, psychological OR anxiety OR anxiety disorder OR generalized anxiety disorder OR social anxiety disorder OR PTSD OR OCD OR mania OR panic OR phobia OR psychiatric illness). The database searches were supplemented by retrieval of any additional papers meeting eligibility criteria that were cited in reference lists of relevant review articles yielding 820 additional articles. Searches were conducted in January and February 2022 and yielded 3957 studies after duplicates were removed. Studies that were excluded during full-text screening were rejected due to wrong study design, including the article being a review article or abstract only, and wrong study outcomes. Articles rejected due to “wrong study outcome” did not measure changes in psychiatric symptoms in response to the use of a microbiome-targeted therapeutic as an adjuvant to medication for psychiatric illness.

Figure 1. Flow chart showing literature search and screening process using PRISMA guidelines.
Eligible articles were restricted to those that were published in peer-reviewed journals and were written in English. Studies eligible for inclusion involved clinical samples that assessed changes in psychiatric wellbeing after standard treatment indicated for psychiatric illness and an adjuvant therapeutic targeting the microbiome.
Two authors (BB and AS) completed the initial search of the databases, adhering to the search strategy as described above. Two authors (EF and one of BB or AS) independently assessed the titles and abstracts of records retrieved from a systematic search according to the identified inclusion and exclusion criteria. Two authors (BB and EF) completed the full-text review. Any disagreements were resolved by a fourth author (AC). Quality assessment of eligible articles was completed by a fifth author (CS).
Quality assessment of articles was completed using Covidence’s built-in, Cochrane Handbook for Systematic Reviews of Interventions, Risk of Bias (RoB) template. The Cochrane RoB tool assesses the risk of bias for the following domains: sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, and “other” sources of bias. Most studies presented with a low level of bias. Studies where there was no mention of blinding to participants, personnel, outcome assessors, or allocation of treatment, were assigned a “high” judgment in risk of bias. In studies where there was no given description or details regarding one of the RoB domains (i.e., sequence generation), the risk of bias was assigned as “unsure.” A detailed summary of the quality assessment can be found in Table 1.
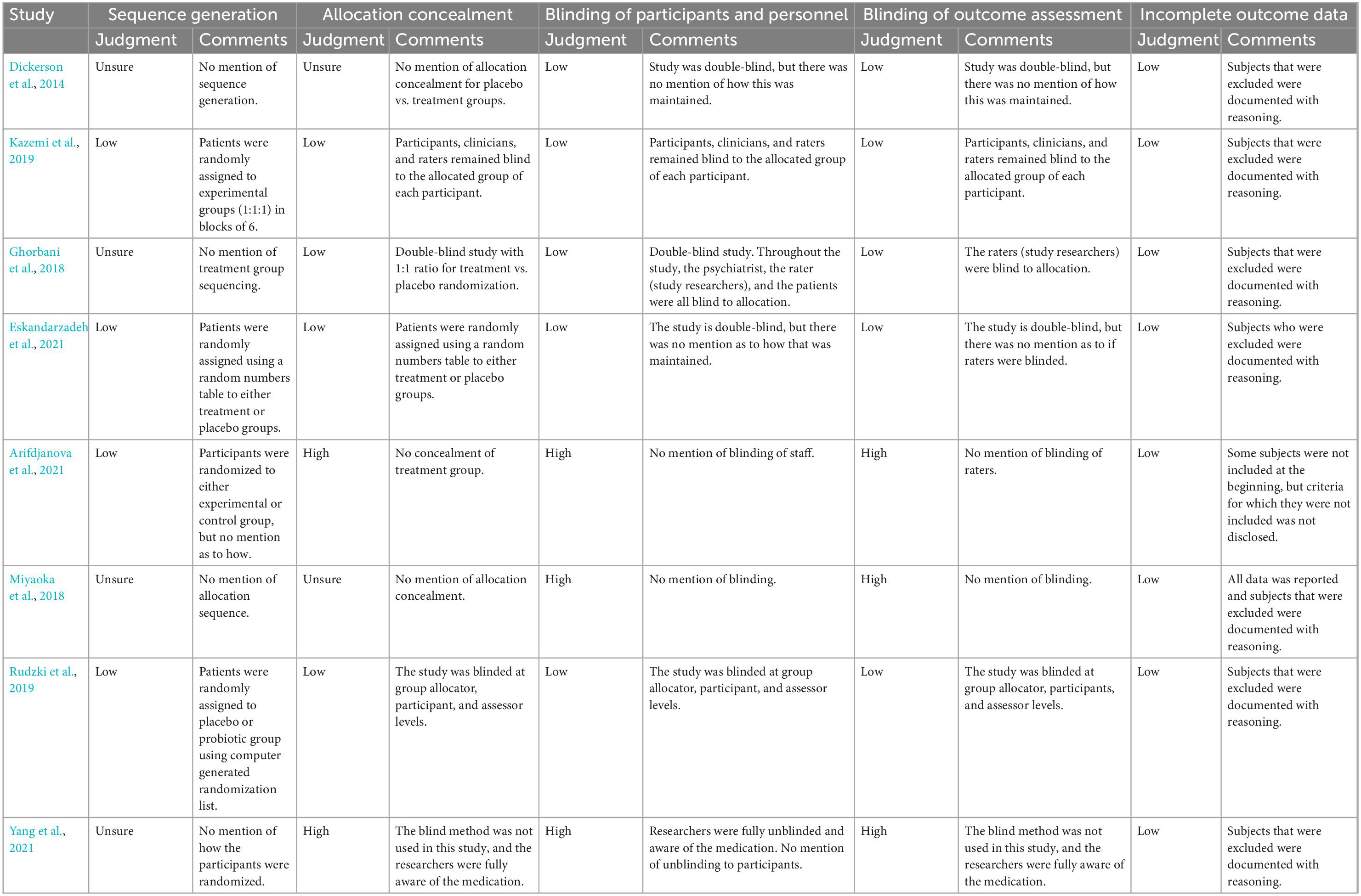
Table 1. Summary of quality assessment details and judgment for risk of bias of each study.
Following the removal of 1072 duplicates, the search yielded 3,957 results. Subsequent abstract screening and full-text screening, according to the search criteria highlighted earlier (shown in Figure 1) resulted in 8 papers with direct relevance to the research question.
Our findings can be grouped into studies examining three major categories of psychological disorders. For one, 370 patients across 5 trials were categorized and treated as patients with MDD (Ghorbani et al., 2018; Miyaoka et al., 2018; Kazemi et al., 2019; Rudzki et al., 2019; Arifdjanova et al., 2021). A significant majority of these patients received traditional antidepressant medication in the form of SSRIs. The sole trial examining 48 patients with GAD (Eskandarzadeh et al., 2021) assessed the use of sertraline, a common SSRI, as its psychotropic agent. The remaining two trials examined 132 patients with SZ or schizoaffective disorder (SZA) (Dickerson et al., 2014; Yang et al., 2021), one in which participants received the atypical antipsychotic Olanzapine, and the other in which participants continued taking whichever antipsychotic they were prescribed prior to enrolling in the study. As can be seen in Table 2, the studies were conducted across 6 different countries and on predominantly female populations. Furthermore, while the majority of studies used an SSRI or atypical antipsychotic, the makeup and the quantity of probiotic administered varied greatly across trials, reducing the generalizability of conclusions.
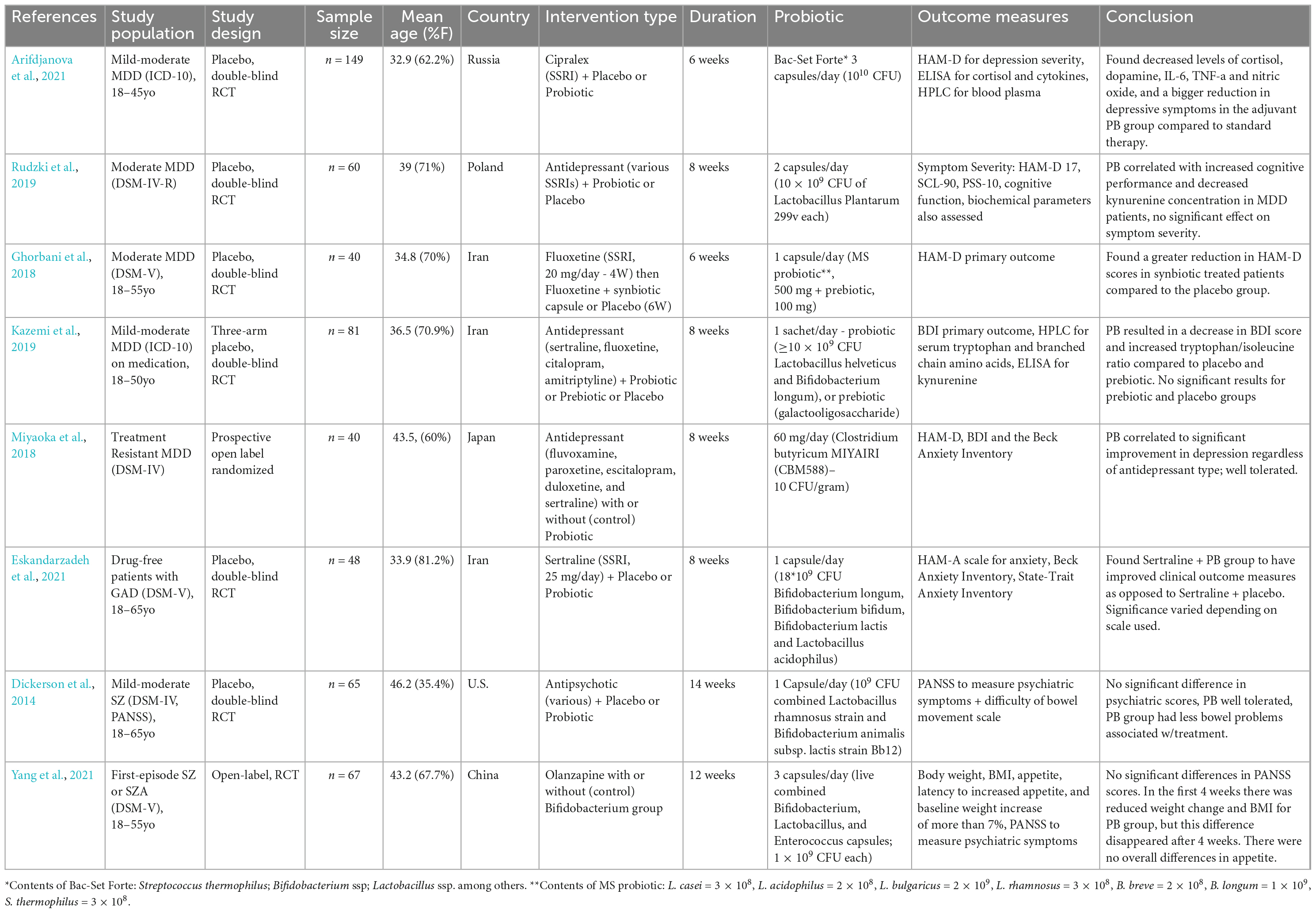
Table 2. Summary of key study characteristics and outcomes.
In all studies, a subset of patients received their psychotropic medication in conjunction with a type of probiotic supplementation. Most of these studies were conducted in the form of a double-blinded, randomized clinical trial. Two studies, however, (Miyaoka et al., 2018; Yang et al., 2021) lacked a placebo arm, following an open-label randomized format.
In the eight studies examined (shown in Table 2), the medications to treat psychiatric illness were either antidepressants (n = 6), or antipsychotics (n = 2). All studies included measures for clinical outcomes and symptom severity. In the depression studies, the majority used the Hamilton Depression Rating Scale (Hamilton, 1960) (HAM-D) (n = 4) or the Beck Depression Inventory (Beck et al., 1996) (BDI) (n = 2) to measure symptoms of mood, anhedonia, sleep, anxiety, appetite, and other symptoms associated with depression. The anxiety study used the Hamilton Anxiety Rating Scale (Hamilton, 1959) (HAM-A) (n = 1) to assess symptoms of anxiety such as mood, tension, insomnia, physiological symptoms. The schizophrenia studies used the Positive and Negative Syndrome Scale (Kay et al., 1987) (PANSS) (n = 2) to assess positive and negative symptoms associated with schizophrenia such as delusions, hallucinations, blunted affect, and social withdrawal. Higher scores on these scales correspond to an increased severity of the illness.
When examining the effects on symptom severity in patients with MDD or GAD, five of the six studies found that patients who received adjuvant probiotic treatment had significant reductions in symptom severity on the majority of the scales used. One study (Rudzki et al., 2019) did not find any significant effects on symptom severity in patients with MDD receiving adjuvant probiotic therapy using the HAM-D, Symptom Checklist-90 (Derogatis and Savitz, 1999) (SCL-90), and Perceived Stress Scale-10 (Cohen et al., 1983) (PSS-10), but did find that adjuvant probiotic treatment was correlated with increased cognitive performance. Neither of the two studies using patients with schizophrenia or schizoaffective disorder taking antipsychotics found adjuvant probiotic treatment to have any effect on the psychiatric symptoms. That being said, both studies found adjuvant probiotic treatment to reduce the adverse events and side effects associated with antipsychotic treatment, with Dickerson et al. finding fewer reports of bowel difficulties, and Yang et al. finding a reduced weight gain in the first 4 weeks in the adjuvant probiotic groups. Though the reduced weight gain in the study conducted by Yang et al. was transient, with no differences between the adjuvant and monotherapy groups by weeks 8 and 12, adjuvant probiotic therapy was found to eliminate the observed sex-based differences in weight gain seen in the olanzapine monotherapy group. There was no significant difference in body weight change between men and women in the adjuvant probiotic group, whereas there were significantly higher increases in the body weight of women compared to men in the olanzapine monotherapy group.
The clinical outcome findings from the studies included in this review suggest probiotic and synbiotic adjuvant treatment with SSRIs for MDD and GAD to be more effective in decreasing depressive and anxious symptomology, respectively, than SSRI treatment alone. In the one study included in this review that used included a prebiotic group, prebiotics alone were not found to have a significant effect on clinical symptoms. The improved clinical outcomes of probiotic adjuvant treatment for MDD and GAD were found to be persistent throughout the course of the treatment, but further long-term follow-up assessments would be needed to investigate the persistence of this effect when treatment is discontinued. For individuals with schizophrenia, adjuvant probiotic treatment was not found to be more effective in reducing clinical symptom severity than standard antipsychotic treatment alone. Some potential limitations that could explain this lack of effect on clinical symptoms and outcomes are discussed in the conclusion. Though there was no significance in clinical findings for the schizophrenia groups, adjuvant probiotic treatment was associated with a decrease in treatment associated adverse events and side effects. The findings of these studies suggest adjuvant probiotic treatment to have an alleviative effect on some of the gastrointestinal adverse events associated with antipsychotic treatment, such as weight gain and bowel problems. Some of these beneficial effects were found to be fairly long lasting, as is the case in the trial by Dickerson et al. (2014), but some effects were found to be transient, with Yang et al. finding a reduced weight gain for only the first 4 weeks of adjuvant probiotic treatment (Yang et al., 2021).
As mentioned in the introduction, some antipsychotics and antidepressants have been found to have antibacterial properties, as such, it is important to consider the specific medications used in each study. All MDD and GAD studies used participants taking SSRIs, with Miyoaka et al. including participants taking the SNRIs duloxetine (n = 9) and milnacipran (n = 3) and Kazemi et al. including participants taking the tricyclic antidepressant amitriptyline (n not reported). The SSRIs involved in the studies included escitalopram, citalopram, fluoxetine, fluvoxamine, paroxetine, and sertraline. It has been found SSRIs vary in the degree to which the inhibit bacterial growth, with sertraline and fluoxetine having the strongest antimicrobial activity, followed by paroxetine and fluvoxamine, and then escitalopram and citalopram (McGovern et al., 2019). Amitriptyline has also been found to have antimicrobial effects to around the same degree as paroxetine (Mandal et al., 2010). The antimicrobial effect of SNRIs is less clear, with studies finding venlafaxine to have no effect (Ait Chait et al., 2020), and others finding the clinical effects of duloxetine to be reduced by the bacteria Ruminococcus flavefaciens (Lukić et al., 2019), suggesting an interaction between duloxetine and the bacteria. Despite the differences in medications used and their degree of antimicrobial activity, all the MDD and GAD studies found results suggesting probiotics combined with antidepressants improved clinical outcomes when compared to antidepressants alone.
For the schizophrenia studies, all participants in the study conducted by Yang et al. took olanzapine, whereas participants in the Dickerson et al. study took a variety of antipsychotics. The antipsychotics used in the Dickerson et al. study were clozapine (n = 17), olanzapine (n = 15), risperidone (n = 15), aripiprazole (n = 11), quetiapine (n = 9), haloperidol (n = 7), ziprasidone (n = 5), and asenapine (n = 1), including some participants that took more than one antipsychotic. Though a variety of antipsychotics were used in the Dickerson et al. study, all fall under the category of atypical antipsychotics except for haloperidol which is a butyrophenone derivative. Olanzapine has been found to shift the fecal microbiota in mice toward an “obesogenic” profile (Morgan et al., 2014), and all of the atypical antipsychotics used in the Dickerson et al. study have been found to be associated with significant changes in the gut microbiome and a decrease in species diversity in females (Flowers et al., 2017). Haloperidol has also been found to have some bacteria inhibiting effects (Korbee et al., 2018). Taking that into consideration, though the two studies used different antipsychotics, they both used primarily atypical antipsychotics, but the exact degree in which each individual antipsychotic effects the gut microbiome is not certain. As such, it is possible that the use of differing antipsychotics could have contributed to the difference in longevity of the observed beneficial effects.
The exact mechanisms of action for these beneficial effects of probiotic adjuvant treatment are not fully understood. Though the exact pathway and importance of the various pathways by which probiotic adjuvant treatment may exert its effect is not known, multiple pathways have been described for ways in which the microbiome affects the brain and central nervous system. Biomarker data collected in the MDD studies suggests that the probiotic adjuvant treatment exerts its therapeutic effect through effects on the immune system, the hypothalamic pituitary adrenal axis (HPA-axis), and the tryptophan system. Decreased concentrations of immune markers such as interleukin-6, tumor necrosis factor-a, and nitric oxide suggests a decrease in the activity of the immune system in response to probiotic adjuvant treatment. The immune system has long been known to be intimately linked to MDD and depressive symptomology, with an over-active immune system often being observed in individuals with MDD (Leonard, 2010). One proposed mechanism of action for microbiome targeting treatment for MDD is a reduction in immune system activity through a decrease in gut permeability. It is thought that individuals with MDD and/or other illnesses have increased gastrointestinal permeability, allowing for microorganisms and other potentially harmful toxins from the gut to pass into the body, resulting in an increase in inflammation and immune system activity. Repopulation of the gut microbiome and/or the introduction of beneficial bacteria through probiotic treatment is thought to alleviate this increased gut permeability, and thus reduce inflammation and immune system activity, leading to a decrease in depressive symptomology. Biomarker data from the study conducted by Arifdjanova et al. (2021) also found cortisol levels to be decreased in the probiotic adjuvant treatment group. Cortisol is often associated with stress and is a major indicator HPA-axis activity. Individuals with MDD and/or GAD often are found to have an overactive HPA-axis and increased levels of cortisol. Probiotic and other gut microbiome targeting treatments have been frequently found to have an inhibitory effect on HPA-axis activity and has been associated with decreased cortisol levels. Influencing the HPA-axis and cortisol production and availability seems to be another pathway by which probiotic adjuvant treatment results in improved clinical outcomes. Another potential mechanism for the improved clinical outcome observed in the probiotic adjuvant treatment groups is through effects on the tryptophan system. Kazemi et al. (2019) and Rudzki et al. (2019) found an increased tryptophan/isoleucine ratio and decreased kynurenine (a tryptophan metabolite) concentration in the probiotic treatment groups of their respective studies. Tryptophan is a precursor to serotonin, a neurotransmitter that has long been associated with MDD and GAD. SSRIs exert their therapeutic action by inhibiting serotonin reuptake transporter proteins, leading to an increase in the relative abundance and concentration of serotonin in the brain. Though serotonin is often associated with the brain and psychiatric illnesses, up to 90% of the body’s serotonin is produced in the gut. The mechanism by which the gut microbiome affects serotonin production and availability is thought to be through interactions with microbiome metabolites and enterochromaffin cells (EC cells) in the gut. The microbiome produces long and short chain fatty acids (SCFA) through the fermentation of non-digestible carbohydrates. Long chain fatty acids influence serotonin production indirectly through interactions with glucagon-like protein-1 (GLP-1) cells leading to increased GLP-1 which interacts with EC cells to increase serotonin production and availability. Short chain fatty acids interact directly with EC cells to increase serotonin production and availability. In addition to these interactions with EC cells, short chain fatty acids have the ability to cross the gut-blood and blood-brain barriers, and are thought to have an anti-inflammatory effect, thus further influencing the immune system. The exact bacteria involved in these processes are not fully characterized, but some species Lactobacillus and Bifidobacterium have been found to produce neurotransmitters such as acetylcholine and gamma-aminobutyric acid, and Streptococcus, Enterococcus, and Escherichia have been found to produce serotonin, dopamine, and epinephrine (Galland, 2014). These biomarker findings suggest that the beneficial clinical outcomes in the adjuvant probiotic groups with MDD and GAD are a result of the adjuvant probiotic treatment affecting multiple if not all of the pathways by which the microbiome and brain are connected.
As for the observed effect of a decrease in gastrointestinal adverse events in the adjuvant probiotic group of the schizophrenia studies, the mechanism of action is largely unclear. The alleviation of gastrointestinal issues, such as constipation, most likely acted through interactions with the serotonin pathway. As described above, probiotic administration may have resulted in an increase in SCFAs produced by the microbiome, which in turn increases serotonin synthesis through EC cells. Serotonin has been found to activate enteric neural circuitry to initiate peristalsis and reduce constipation (Crowell, 2004). The transient effect of decreasing weight gain for the first 4 weeks could be from a variety of factors. Bifidobacterium administration has been linked to both weight gain and weight loss depending on the strain (Yin et al., 2010). The exact strain used by Yang et al. was not reported (Miyaoka et al., 2018), but increased bacteria with bile salt hydrolase has been found to prevent weight gain through the deconjugation of bile acids (Joyce et al., 2014). This may have been the case for the Yang et al. study, but the general negative impact on energy by olanzapine as well as its own mechanism of action for weight gain may have outweighed the preventative action of the probiotic over time. Although it is thought that probiotics may improve clinical outcomes and symptom severity in populations with schizophrenia through interaction with the immune system (Fond et al., 2020), neither of the studies included a robust collection of immune system related biomarkers, and thus the effect of adjuvant probiotic treatment on the immune system of the patients in these studies is unknown.
Although the studies included in this review were generally found to be of high quality with low risk of bias, there were still some limitations to these studies that impact the generalizability and conclusions that could be drawn from their findings. A major limitation is the small number of studies for each psychiatric illness and the lack of studies investigating other psychiatric illnesses. With only eight studies in total, five of which used a population with MDD, it is difficult to draw strong generalizable conclusions about the effect of adjuvant probiotic treatment on GAD and schizophrenia. Additionally, though the studies included had relatively large sample sizes, further larger scale, double blind, randomized controlled trials are required in the future to make any definitive conclusions. Many of the studies included in this review also did not have comprehensive biomarker collection. To be able to elucidate the mechanisms of action of probiotic supplementation as an adjuvant treatment, as well as to evaluate the colonization of the gut by the probiotics administered and changes in key features of the gut such as intestinal permeability, robust and consistent biomarker collection is necessary. This collection would include biomarkers for the immune system, HPA-axis, serotonin system, and the gut microbiome. Another limitation of the studies was the fact that many used a variety of first-line antidepressant or antipsychotic treatments in combination with the probiotics, which is helpful for evaluating adjunctive probiotic treatment in general but does not give strong insight into the effectiveness of adjunctive probiotic administration with specific antidepressants and antipsychotics. As different psychiatric treatments can have differing effects on the gut microbiome, studies or analyses focusing on one specific intervention could allow for more detail in determining what combination of treatment would be most effective for an individual. These studies are also limited by their length, with the majority being unable to have significant long-term follow-ups to investigate the longevity of the observed effects. Another limitation in this field is the lack of consensus on dosages for probiotics as well as the treatments they are given in combination with. Dose finding studies in the future are needed, in addition to studies investigating the efficacy of adjuvant probiotic treatment at different stages and severity of the illnesses. This is especially relevant for the schizophrenia studies, which included populations with relatively severe clinical symptoms and later stages of the illness. It is possible that in a population with milder symptoms and a more recent onset, adjuvant probiotic therapy could effectively impact clinical outcomes.
Despite these limitations, the findings of these studies suggest the use of adjuvant probiotic treatment with SSRI treatment for MDD and GAD to be superior to SSRI treatment alone. Probiotic adjuvant treatment with antipsychotics could be beneficial for improving the GI issues associated with antipsychotics, but these findings do not suggest that adjuvant probiotic treatment would result in improved clinical outcomes for symptoms of schizophrenia. Though progress in psychiatric research is challenging, these studies have shown that combining probiotic treatment with first line pharmaceutical treatments is promising, and their findings certainly justify continued research in this area. The gut microbiome and the brain are clearly linked, and these studies show that combining treatments that target both areas, respectively, is a viable and efficacious way to combat the symptoms and treat psychiatric illnesses.
The original contributions presented in this study are included in this article/supplementary material, further inquiries can be directed to the corresponding author.
BB and AS completed the initial search of the databases, adhering to the search strategy. EF and one of BB or AS independently assessed the titles and abstracts of records retrieved from a systematic search according to the identified inclusion and exclusion criteria. BB and EF completed the full-text review. AC resolved any disagreements. CS completed quality assessment of eligible articles. All authors contributed to the article and approved the submitted version.
RM has received consulting and speaking honoraria from AbbVie, Allergan, Eisai, Janssen, KYE, Lallemand, Lundbeck, Neonmind, Otsuka, and Sunovion, and research grants from CAN-BIND, CIHR, Janssen, Lallemand, Lundbeck, Nubiyota, OBI, and OMHF. AC has received CIHR Doctoral Funding.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
BDI, Beck Depression Inventory; BMI, body mass index; CFU, colony forming units; DSM, Diagnostic and Statistical Manual of Mental Disorders; EC, enterochromaffin cells; GAD, Generalized Anxiety Disorder; GBA, gut brain axis; GI, gastrointestinal; GLP-1, glucagon-like Protein 1; HAM-A, Hamilton Anxiety Rating Scale; HAM-D, Hamilton Depression Rating Scale 17-item; HPA, hypothalamic pituitary adrenal axis; ICD, International Classification of Diseases; MDD, Major Depressive Disorder; MS, multi-strain probiotic; PANSS, Positive and Negative Syndrome Scale; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; PSS-10, Perceived Stress Scale 10; RCT, randomized controlled trial; RoB, risk of bias; SZA, schizoaffective disorder; SCL-90, Symptom Checklist-90; SSRI, selective serotonin reuptake inhibitors; SZ, schizophrenia.
Ait Chait, Y., Mottawea, W., Tompkins, T., and Hammami, R. (2020). Unravelling the antimicrobial action of antidepressants on gut commensal microbes. Sci. Rep. 10:17878. doi: 10.1038/s41598-020-74934-9
American Psychiatric Association [APA] (2013). Diagnostic and statistical manual of mental disorders: DSM-5. Washington, DC: American psychiatric association. doi: 10.1176/appi.books.9780890425596
Arifdjanova, S., Abrurakhmanova, Z., Bizulya, E., Gumenyuk, L., Sorokina, L., and Gerbali, O. (2021). The role of probiotics in combination therapy of depressive disorders. Russ. Open Med. J. 10:e0109. doi: 10.15275/rusomj.2021.0109
Baldwin, D., Woods, R., Lawson, R., and Taylor, D. (2011). Efficacy of drug treatments for generalised anxiety disorder: Systematic review and meta-analysis. BMJ 342:d1199. doi: 10.1136/bmj.d1199
Beck, A. T., Steer, R. A., and Brown, G. K. (1996). Manual for the beck depression inventory-II. San Antonio, TX: Psychological Corporation. doi: 10.1037/t00742-000
Bercik, P., Denou, E., Collins, J., Jackson, W., Lu, J., Jury, J., et al. (2011). The intestinal microbiota affect central levels of brain-derived neurotropic factor and behavior in mice. Gastroenterology 141, 599–609, 609e.1–609e.3. doi: 10.1053/j.gastro.2011.04.052
Bermon, S., Petriz, B., Kajeniene, A., Prestes, J., Castell, L., and Franco, O. (2015). The microbiota: An exercise immunology perspective. Exerc. Immunol. Rev. 21, 70–79.
Ciocan, D., Cassard, A., Becquemont, L., Verstuyft, C., Voican, C., El Asmar, K., et al. (2021). Blood microbiota and metabolomic signature of major depression before and after antidepressant treatment: A prospective case–control study. J. Psychiatry Neurosci. 46, E358–E368. doi: 10.1503/jpn.200159
Cohen, S., Kamarck, T., and Mermelstein, R. (1983). A global measure of perceived stress. J. Health Soc. Behav. 24, 385–396. doi: 10.2307/2136404
Crowell, M. (2004). Role of serotonin in the pathophysiology of the irritable bowel syndrome. Br. J. Pharmacol. 141, 1285–1293. doi: 10.1038/sj.bjp.0705762
Cryan, J., O’Riordan, K., Cowan, C., Sandhu, K., Bastiaanssen, T., Boehme, M., et al. (2019). The microbiota-gut-brain axis. Physiol. Rev. 99, 1877–2013. doi: 10.1152/physrev.00018.2018
Cussotto, S., Clarke, G., Dinan, T., and Cryan, J. (2019). Psychotropics and the microbiome: A chamber of secrets. Psychopharmacology 236, 1411–1432. doi: 10.1007/s00213-019-5185-8
De Hert, M., Dobbelaere, M., Sheridan, E., Cohen, D., and Correll, C. (2011). Metabolic and endocrine adverse effects of second-generation antipsychotics in children and adolescents: A systematic review of randomized, placebo controlled trials and guidelines for clinical practice. Eur. Psychiatry 26, 144–158. doi: 10.1016/j.eurpsy.2010.09.011
Derogatis, L. R., and Savitz, K. L. (1999). “The SCL-90-R, brief symptom inventory, and matching clinical rating scales,” in The use of psychological testing for treatment planning and outcomes assessment, ed. M. E. Maruish (Mahwah, NJ: Lawrence Erlbaum Associates Publishers), 679–724.
Dickerson, F., Stallings, C., Origoni, A., Katsafanas, E., Savage, C., Schweinfurth, L., et al. (2014). Effect of probiotic supplementation on schizophrenia symptoms and association with gastrointestinal functioning: A randomized, placebo-controlled trial. Prim. Care Companion CNS Disord. 16:26294. doi: 10.4088/PCC.13m01579
Eskandarzadeh, S., Effatpanah, M., Khosravi-Darani, K., Askari, R., Hosseini, A., Reisian, M., et al. (2021). Efficacy of a multispecies probiotic as adjunctive therapy in generalized anxiety disorder: A double blind, randomized, placebo-controlled trial. Nutr. Neurosci. 24, 102–108. doi: 10.1080/1028415X.2019.1598669
Evans-Lacko, S., Aguilar-Gaxiola, S., Al-Hamzawi, A., Alonso, J., Benjet, C., Bruffaerts, R., et al. (2018). Socio-economic variations in the mental health treatment gap for people with anxiety, mood, and substance use disorders: Results from the WHO world mental health (WMH) surveys. Psychol. Med. 48, 1560–1571. doi: 10.1017/S0033291717003336
Flowers, S., Evans, S., Ward, K., McInnis, M., and Ellingrod, V. (2017). Interaction between atypical antipsychotics and the gut microbiome in a bipolar disease cohort. Pharmacotherapy 37, 261–267. doi: 10.1002/phar.1890
Fond, G., Lançon, C., Korchia, T., Auquier, P., and Boyer, L. (2020). The role of inflammation in the treatment of schizophrenia. Front. Psychiatry 11:160. doi: 10.3389/fpsyt.2020.00160
Fontana, A., Manchia, M., Panebianco, C., Paribello, P., Arzedi, C., Cossu, E., et al. (2020). Exploring the role of gut microbiota in major depressive disorder and in treatment resistance to antidepressants. Biomedicines 8:311. doi: 10.3390/biomedicines8090311
Galland, L. (2014). The gut microbiome and the brain. J. Med. Food 17, 1261–1272. doi: 10.1089/jmf.2014.7000
Gelenberg, A., Freeman, M., Markowitz, J., Rosenbaum, J., Thase, M., Trivedi, M., et al. (2010). American psychiatric association practice guidelines for the treatment of patients with major depressive disorder. Am. J. Psychiatry 167, (Suppl. 10), 9–118.
Ghorbani, Z., Nazari, S., Etesam, F., Nourimajd, S., Ahmadpanah, M., and Jahromi, S. (2018). The effect of synbiotic as an adjuvant therapy to fluoxetine in moderate depression: A randomized multicenter trial. Arch. Neurosci. 5:e60507. doi: 10.5812/archneurosci.60507
Hamilton, M. (1959). The assessment of anxiety states by rating. Br. J. Med. Psychol. 32, 50–55. doi: 10.1111/j.2044-8341.1959.tb00467.x
Hamilton, M. (1960). A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 23, 56–62. doi: 10.1136/jnnp.23.1.56
Heiman, M., and Greenway, F. L. (2016). A healthy gastrointestinal microbiome is dependent on dietary diversity. Mol. Metab. 5, 317–320. doi: 10.1016/j.molmet.2016.02.005
Hirsch, M., and Birnbaum, R. (2017). Selective serotonin reuptake inhibitors: Pharmacology, administration, and side effects, eds P. Roy-Byrne and D. Solomon (Waltham, MA: UpToDate).
Johnson, D., Thurairajasingam, S., Letchumanan, V., Chan, K., and Lee, L. (2021). Exploring the role and potential of probiotics in the field of mental health: Major depressive disorder. Nutrients 13:1728. doi: 10.3390/nu13051728
Joyce, S., MacSharry, J., Casey, P., Kinsella, M., Murphy, E., Shanahan, F., et al. (2014). Regulation of host weight gain and lipid metabolism by bacterial bile acid modification in the gut. Proc. Natl. Acad. Sci. U.S.A. 111, 7421–7426. doi: 10.1073/pnas.1323599111
Kay, S., Fiszbein, A., and Opler, L. (1987). The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr. Bull. 13, 261–276. doi: 10.1093/schbul/13.2.261
Kazemi, A., Noorbala, A., Azam, K., Eskandari, M., and Djafarian, K. (2019). Effect of probiotic and prebiotic vs placebo on psychological outcomes in patients with major depressive disorder: A randomized clinical trial. Clin. Nutr. 38, 522–528. doi: 10.1016/j.clnu.2018.04.010
Korbee, C., Heemskerk, M., Kocev, D., van Strijen, E., Rabiee, O., Franken, K., et al. (2018). Combined chemical genetics and data-driven bioinformatics approach identifies receptor tyrosine kinase inhibitors as host-directed antimicrobials. Nat. Commun. 9:358. doi: 10.1038/s41467-017-02777-6
Le Barz, M., Anhê, F., Varin, T., Desjardins, Y., Levy, E., Roy, D., et al. (2015). Probiotics as complementary treatment for metabolic disorders. Diabetes Metab. J. 39, 291–303. doi: 10.4093/dmj.2015.39.4.291
Leonard, B. (2010). “The concept of depression as a dysfunction of the immune system,” in Depression: From psychopathology to pharmacotherapy, Vol. 27, ed. J. F. Cryan (Basel: Karger Publishers), 53–71. doi: 10.1159/000319504
Li, J., Jia, H., Cai, X., Zhong, H., Feng, Q., Sunagawa, S., et al. (2014). An integrated catalog of reference genes in the human gut microbiome. Nat. Biotechnol. 32, 834–841. doi: 10.1038/nbt.2942
Liu, L., Huh, J., and Shah, K. (2022). Microbiota and the gut-brain-axis: Implications for new therapeutic design in the CNS. EBioMedicine 77:103908. doi: 10.1016/j.ebiom.2022.103908
Lukić, I., Getselter, D., Ziv, O., Oron, O., Reuveni, E., Koren, O., et al. (2019). Antidepressants affect gut microbiota and Ruminococcus flavefaciens is able to abolish their effects on depressive-like behavior. Transl. Psychiatry 9:133. doi: 10.1038/s41398-019-0466-x
Maier, L., Pruteanu, M., Kuhn, M., Zeller, G., Telzerow, A., Anderson, E., et al. (2018). Extensive impact of non-antibiotic drugs on human gut bacteria. Nature 555, 623–628. doi: 10.1038/nature25979
Mandal, A., Sinha, C., Kumar Jena, A., Ghosh, S., and Samanta, A. (2010). An Investigation on in vitro and in vivo antimicrobial properties of the antidepressant: Amitriptyline hydrochloride. Braz. J. Microbiol. 41, 635–645. doi: 10.1590/S1517-83822010000300014
Martin, R., Makino, H., Cetinyurek Yavuz, A., Ben-Amor, K., Roelofs, M., Ishikawa, E., et al. (2016). Early-life events, including mode of delivery and type of feeding, siblings and gender, shape the developing gut microbiota. PLoS One 11:e0158498. doi: 10.1371/journal.pone.0158498
McGovern, A., Hamlin, A., and Winter, G. (2019). A review of the antimicrobial side of antidepressants and its putative implications on the gut microbiome. Aust. N. Z. J. Psychiatry 53, 1151–1166. doi: 10.1177/0004867419877954
Meyyappan, A., Forth, E., Wallace, C., and Milev, R. (2020). Effect of fecal microbiota transplant on symptoms of psychiatric disorders: A systematic review. BMC Psychiatry 20:299. doi: 10.1186/s12888-020-02654-5
Miyaoka, T., Kanayama, M., Wake, R., Hashioka, S., Hayashida, M., Nagahama, M., et al. (2018). Clostridium butyricum MIYAIRI 588 as adjunctive therapy for treatment-resistant major depressive disorder: A prospective open-label trial. Clin. Neuropharmacol. 41, 151–155. doi: 10.1097/WNF.0000000000000299
Moher, D., Liberati, A., Tetzlaff, J., and Altman, D., and Prisma Group. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 151, 264–269. doi: 10.7326/0003-4819-151-4-200908180-00135
Morais, L., Schreiber, H., and Mazmanian, S. (2021). The gut microbiota–brain axis in behaviour and brain disorders. Nat. Rev. Microbiol. 19, 241–255. doi: 10.1038/s41579-020-00460-0
Morgan, A., Crowley, J., Nonneman, R., Quackenbush, C., Miller, C., Ryan, A., et al. (2014). The antipsychotic olanzapine interacts with the gut microbiome to cause weight gain in mouse. PLoS One 9:e115225. doi: 10.1371/journal.pone.0115225
Munoz-Bellido, J., Munoz-Criado, S., and Garcıa-Rodrıguez, J. (2000). Antimicrobial activity of psychotropic drugs: Selective serotonin reuptake inhibitors. Int. J. Antimicrob. Agents 14, 177–180. doi: 10.1016/S0924-8579(99)00154-5
Neufeld, K., Kang, N., Bienenstock, J., and Foster, J. (2011). Reduced anxiety-like behavior and central neurochemical change in germ-free mice. Neurogastroenterol. Motil. 23, 255–264, e119. doi: 10.1111/j.1365-2982.2010.01620.x
Nikolova, V., Hall, M., Hall, L., Cleare, A., Stone, J., and Young, A. (2021). Perturbations in gut microbiota composition in psychiatric disorders: A review and meta-analysis. JAMA Psychiatry 78, 1343–1354. doi: 10.1001/jamapsychiatry.2021.2573
Ochoa, S., Usall, J., Cobo, J., Labad, X., and Kulkarni, J. (2012). Gender differences in schizophrenia and first-episode psychosis: A comprehensive literature review. Schizophr. Res. Treatment 2012:916198. doi: 10.1155/2012/916198
Odamaki, T., Kato, K., Sugahara, H., Hashikura, N., Takahashi, S., Xiao, J., et al. (2016). Age-related changes in gut microbiota composition from newborn to centenarian: A cross-sectional study. BMC Microbiol. 16:90. doi: 10.1186/s12866-016-0708-5
Patel, K., Cherian, J., Gohil, K., and Atkinson, D. (2014). Schizophrenia: Overview and treatment options. Pharm. Ther. 39, 638–645.
Rudzki, L., Ostrowska, L., Pawlak, D., Małus, A., Pawlak, K., Waszkiewicz, N., et al. (2019). Probiotic Lactobacillus plantarum 299v decreases kynurenine concentration and improves cognitive functions in patients with major depression: A double-blind, randomized, placebo controlled study. Psychoneuroendocrinology 100, 213–222. doi: 10.1016/j.psyneuen.2018.10.010
Sabic, D., Sabic, A., and Bacic-Becirovic, A. (2021). Major depressive disorder and difference between genders. Mater. Sociomed. 33, 105–108. doi: 10.5455/msm.2021.33.105-108
Vesga-López, O., Schneier, F., Wang, S., Heimberg, R., Liu, S., Hasin, D., et al. (2008). Gender differences in generalized anxiety disorder: Results from the national epidemiologic survey on alcohol and related conditions (NESARC). J. Clin. Psychiatry 69, 1606–1616. doi: 10.4088/JCP.v69n1011
Yang, Y., Long, Y., Kang, D., Liu, C., Xiao, J., Wu, R., et al. (2021). Effect of Bifidobacterium on olanzapine-induced body weight and appetite changes in patients with psychosis. Psychopharmacology 238, 2449–2457. doi: 10.1007/s00213-021-05866-z
Yin, Y., Yu, Q., Fu, N., Liu, X., and Lu, F. (2010). Effects of four Bifidobacteria on obesity in high-fat diet induced rats. World J. Gastroenterol. 16, 3394–3401. doi: 10.3748/wjg.v16.i27.3394
Yuan, X., Wang, Y., Li, X., Jiang, J., Kang, Y., Pang, L., et al. (2021). Gut microbial biomarkers for the treatment response in first-episode, drug-naïve schizophrenia: A 24-week follow-up study. Transl. Psychiatry 11:422. doi: 10.1038/s41398-021-01531-3
Keywords: probiotics, psychiatric illness, psychotropics, adjuvant therapy, gut-brain-axis probiotics, gut-brain-axis, Major Depressive Disorder
Citation: Forth E, Buehner B, Storer A, Sgarbossa C, Milev R and Chinna Meyyappan A (2023) Systematic review of probiotics as an adjuvant treatment for psychiatric disorders. Front. Behav. Neurosci. 17:1111349. doi: 10.3389/fnbeh.2023.1111349
Received: 29 November 2022; Accepted: 20 January 2023;
Published: 09 February 2023.
Edited by:
Angelica Thomaz Vieira, Federal University of Minas Gerais, BrazilReviewed by:
Alessandra Riva, University of Vienna, AustriaCopyright © 2023 Forth, Buehner, Storer, Sgarbossa, Milev and Chinna Meyyappan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Evan Forth,  MTRlZjE5QHF1ZWVuc3UuY2E=
MTRlZjE5QHF1ZWVuc3UuY2E=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.