
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Behav. Neurosci., 06 October 2022
Sec. Emotion Regulation and Processing
Volume 16 - 2022 | https://doi.org/10.3389/fnbeh.2022.977600
This article is part of the Research TopicCredition - An Interdisciplinary Approach to the Nature of Beliefs and BelievingView all 42 articles
 Irene Cristofori1,2*
Irene Cristofori1,2* Shira Cohen-Zimerman3,4
Shira Cohen-Zimerman3,4 Joseph Bulbulia5,6
Joseph Bulbulia5,6 Barry Gordon7,8
Barry Gordon7,8 Frank Krueger9,10
Frank Krueger9,10 Jordan Grafman3,4,11,12
Jordan Grafman3,4,11,12Religious beliefs emerged in conjunction with moral beliefs, political, and legal beliefs (Cristofori and Grafman, 2017). As pointed out by Oviedo and Szocik (Oviedo and Szocik, 2020) recent debates attempted to determine whether compared to other beliefs, religious beliefs have a specific (Van Leeuwen, 2014) or shared cognitive structure (Boudry and Coyne, 2016). Empirical evidence supports both positions (Levy, 2017; Van Leeuwen, 2018), while neuroscientific findings support a shared neural network between religious and other beliefs [e.g., political beliefs (Cristofori et al., 2015)]. Religious beliefs shape a person's character and influence daily decision-making and social interactions (Cristofori and Grafman, 2017). Religious beliefs are often concerned with the existence of supernatural agents and are often entangled with moral, political, economic, and legal beliefs that have collectively had a profound influence throughout known human history. Their pervasiveness and power have suggested they have a special status in the human brain. However, despite being much in need of investigation, studying the neurobiological basis of religious beliefs has proved difficult. Here, we focus on the contribution of a set of brain-lesions studies that shed light on the neurocognitive underpinnings of religious beliefs. We then compare the findings of these brain-lesions studies with results from neuroimaging studies.
Lesion studies were among the first approaches to investigating how neural-anatomy relates to brain-function (Harlow, 1848). Since the 1990 s, however, functional neuroimaging studies have come to dominate functional-anatomic brain research [e.g., (Fox and Raichle, 2007; Raichle, 2009)]. Despite their popularity, functional neuroimages studies have two limitations. First, while such studies can reveal correlations between brain activation and behavior (e.g., area X is active when behavior y is present), they are limited in their scope for providing causal understanding about the relationship (Siddiqi et al., 2021). The extent to which randomized controlled experiments may manipulate brain anatomy is clearly limited. Second, even where interventions may in principle yield causal inferential knowledge, in practice, most neuroimaging studies are underpowered [e.g., (Marek et al., 2022)]. On the other hand, the distribution of brain lesions across a population is typically a matter of chance. For this reason, by comparing religious cognition in a population with focal lesions and without lesions, causal identification if functional neuroanatomical relationships may be possible. Another virtue of functional neuroanatomical lesion studies of religious cognition, as we shall next describe, is that they are not underpowered. It is important to acknowledge that even whether brain lesions mapping is a model for studying structure/function relationship, lesions emerging from a traumatic brain injury can involve adjacent brain areas that, may accommodate different neurological and/or cognitive functions. For instance, see Rorden et al. recommendations (Rorden et al., 2009) for performing lesion behavior mapping. We do note, however, that we have studied penetrating traumatic brain injuries and, in that case, identification of the lesion parameters like volume loss and areas affected are made somewhat easier by the relative focality of the lesion (Raymont et al., 2011). In addition, we must highlight the studies presented here involve a slightly different cohort number, depending if the participant performed the test or not. As a reminder, our participants were tested over a 1-week period, with extensive neuropsychological and experimental assessments (for more details see Raymont et al., 2011).
The Vietnam Head Injury Study [VHIS (Raymont et al., 2011)] is a longitudinal follow-up of American male combat veterans who served in the Vietnam War, most of whom suffered from focal penetrating traumatic brain injury (pTBI). This dataset provide data on participants who are similar in age, and education level, and is unique in that it includes pre-injury intelligence. The study has followed the veterans (those with, and those without, focal brain lesions) for about 50 years post injury. Particularly, in the final phase of the VHIS (2008–2012), 169 participants (134 with pTBI, 35 with no injury) were assessed for executive functions, social cognition, personality, as well as large battery of tests dedicated to religious beliefs, including fundamentalism, God-Image, and mystical experiences. Individuals studied here are from a monotheistic culture with one God (or no God) rather than many Gods.
Religious beliefs can reflect the particular relationship an individual has with God. A strong personal relationship with God is theoretically (Fiori et al., 2006) and empirically (Newton and McIntosh, 2010) associated with an enhanced sense of control. A recent study by Cohen-Zimerman et al. (2020) aimed at understanding whether damage to the vmPFC—a region associated with emotionally meaningful religious experiences and with a sense of control—could modulate self-reports of a personal relationship with God and a sense of control. Voxel-based lesion-symptom mapping found that damage to the right vmPFC caused a stronger personal relationship with God, and patients with damage to this region reported a greater sense of control compared to patients with damage to the posterior cortex as well as matched healthy patients. Moreover, the association between the vmPFC damage and a greater sense of control was associated with a stronger personal relationship with God. Taken together, these results suggest that a strong personal relationship with God can serve a crucial psychological function by affecting a sense of personal control, with both enhanced after right vmPFC lesions.
More recently, Cristofori et al. (2021) investigated the neural interplay between empathy and personal relationship with God. Extending previous observations that theory of mind networks is recruited during prayer (Boyer, 2003, 2008), the authors found that people with vmPFC damage reported higher scores on the personal relationship with God inventory (Lawrence, 1997) even when they were not praying. The results showed that vmPFC and posterior superior temporal sulcus/temporoparietal junction (pSTS/TPJ) lesions, associated with the strength of the personal relationship with God, affected empathetic responses. The authors suggested that the neurological networks underpinning God representations amplify human empathetic responses. The cultural evolutionary study of religion has argued that supernatural beliefs evoke pro-social responses because people fear the wrath of Gods (Atran and Norenzayan, 2004). In accordance with other studies e.g., (Norenzayan et al., 2012), our findings imply that, in contrast to the focus of the evolutionary literature on punishment, greater attention should be addressed to investigating the mechanisms by which the religious belief system modulates empathetic responses to others. It may seem that a stronger relationship with God, based on the lesioned right vmPFC, is counterintuitive. However, a stronger relationship with God post-injury might be due to the crucial role of the vmPFC in scaling and evaluating social behavior (Moretti et al., 2009; Cristofori et al., 2015). Counterintuitive behavior changes provided by lesion-free contralateral homotopic areas are documented in the neuroscientific literature. However, recovery from severe and complex neural deficits may be more dependent upon extended neural networks rather than on a confined neural structure.
Religious beliefs can be influenced by certain experiences, such as mystical experiences, i.e., subjectively believed encounters with a supernatural world. Mystical experiences diverge from religious beliefs, in the sense that someone can experience a mystical phenomenon even without prior religious beliefs. Cristofori and collaborators (Cristofori et al., 2016) investigated pTBI patients and healthy volunteers. Mystical experiences were assessed using the Mystical scale [M-Scale (Hood, 1975)]. The M-scale refers to mystical experiences that the people may have previously experienced (e.g., “I have had an experience that was both timeless and spaceless”). Voxel-based lesion-symptom mapping analysis showed that lesions to frontal and temporal brain regions were linked with greater mystical experiences. Such regions included the dlPFC and middle/superior temporal cortex (TC). Performing a confirmatory group analysis, the researchers found that the dlPFC lesion group reported experiencing increased mysticism. Notably, longitudinal analysis of pre-injury data (correlating with general intelligence and executive functions task performance) excludes explanations from individual differences. These findings support previous speculation linking executive functions to mystical experiences and reveal that executive functions (particularly those aspects of executive functions that depend upon dlPFC) causally contribute to the down-regulation of mystical experiences. This study provided evidence in favor of the executive inhibition hypothesis, for the emergence of mystical experiences. This hypothesis was based on previous studies where the authors observed decreased activity in the dlPFC during mystical exercises in practitioners of glossolalia [i.e., religious prayer group experiences in which individuals speak an incomprehensible language (Newberg et al., 2006)] or a reduction of cognitive resources invested in error monitoring during religious rituals (Schjoedt et al., 2013). Another neuroimaging study has shown that participants down-regulated regions in the dlPFC during prayers performed by charismatic speakers (Schjoedt et al., 2011).
Among the different aspects that characterize religious beliefs, a crucial one is the strength of the beliefs, i.e., the fundamentalism aspect. Previous research has identified the vmPFC as critical to representing fundamentalism (Asp et al., 2012). However, the means by which vmPFC regulates fundamentalism was still less certain. Zhong and collaborators hypothesized that the vmPFC represents diverse religious beliefs and that a vmPFC lesion would be associated with religious fundamentalism or the narrowing of religious beliefs (Zhong et al., 2017). To test this prediction, the authors assessed religious adherence with a widely-used religious fundamentalism scale (Altemeyer and Hunsberger, 1992). The results showed that participants with dlPFC lesions had fundamentalism beliefs similar to patients with vmPFC lesions, however, the effect of a dlPFC lesion on fundamentalism was associated with decreased cognitive flexibility and openness. These findings indicated that cognitive flexibility and openness are necessary for flexible and adaptive religious commitment and that such diversity of religious thought is dependent on the functionality of the dlPFC.
The increase of fundamentalism and diminished flexibility and openness might be related to hemisphere dominance laterality. There is evidence that the left hemisphere is focused on facts whereas the right hemisphere represents contextual information and, therefore more adapted to specific situations (McGilchrist, 2012). Moreover, in mental tasks, like meditation, left-brain dominance is effective in top-down regulation, while interhemispheric integration of facts and context takes place in anterior brain areas (Raffone et al., 2019). In addition, other psychological factors such as emotional support and self-efficacy (Zahodne et al., 2014) may influence diminished cognitive resources and induce increased fundamentalism to control new experiences and daily life.
In summary, the lesion studies we describe above identify a network of neural substrates involved in the production of religious cognition, and clarify the functional relationship between religious beliefs, mystical experience, executive control, emotional regulation, rigidity of ideological commitments, and other features of social cognition. The following Table 1 summarizes the main results.
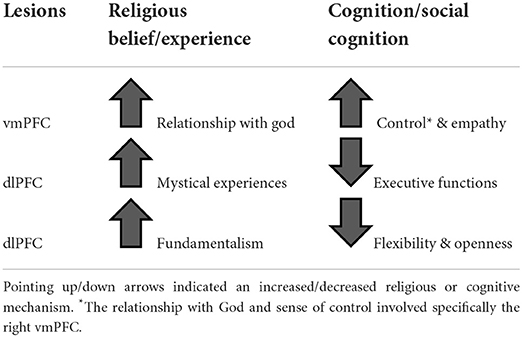
Table 1. Represents a summary of how damage to a brain region affects religious beliefs/experience, cognition/social cognition.
We have delineated a network of lesioned areas within the prefrontal cortex including dlPFC and vmPFC, and more posterior regions such as superior temporal cortex (STC), and pSTS/TPJ (default mode network). More importantly, the network involved included areas damaged in both hemispheres, i.e., vmPFC on the right (belonging functionally to the default mode network) and dlPFC on both sides (belonging functionally to the fronto-parietal control network). In addition, spared areas of the left hemisphere might have driven recovery, e.g., left vmPFC homotopic to its damaged right counterpart.
To sum up, the studies reviewed here complement functional neuroimaging [e.g., (Schjoedt et al., 2011)] and non-invasive brain stimulation [e.g., (Holbrook et al., 2016)] in contributing to our understanding of the religious belief system.
Our results support the belief system model proposed by Seitz and collaborators (see Seitz et al., 2018). According to the credition model, beliefs are the result of neural processes involving the perception and evaluation of external information, and they drive individuals' decisions. Beliefs are unique representations with imaginative and emotional content, using linguistic and memory functions by which beliefs can be expressed, stored, and recalled (Seitz, 2022). Beliefs are fundamental cognitive constructs connecting people's prior experiences with their future behaviors (Krueger and Grafman, 2017).
Questions concerning the Vietnam Head Injury Study can be directed to JG, amdyYWZtYW5Abm9ydGh3ZXN0ZXJuLmVkdQ==.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
This research was supported by the Therapeutic Cognitive Neuroscience Fund (BG). The funder played no role in the design of this study or the interpretation of its results.
The authors thank all the Vietnam veterans, without their long-term commitment to improving the health care of veterans, these studies could not have been completed.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Altemeyer, B., and Hunsberger, B. (1992). Authoritarianism, religious fundamentalism, quest, and prejudice. Int. J. Psychol. Relig. 2, 113–133.
Asp, E., Ramchandran, K., and Tranel, D. (2012). Authoritarianism, religious fundamentalism, and the human prefrontal cortex. Neuropsychology 26, 414–421. doi: 10.1037/a0028526
Atran, S., and Norenzayan, A. (2004). Religion's evolutionary landscape: counterintuition, commitment, compassion, communion. Behav. Brain Sci. 27, 713–730. doi: 10.1017/S0140525X04000172
Boudry, M., and Coyne, J. (2016). Disbelief in belief: on the cognitive status of supernatural beliefs. Philosoph. Psychol. 29, 601–615. doi: 10.1080/09515089.2015.1110852
Boyer, P. (2003). Religious thought and behaviour as by-products of brain function. Trends Cogn. Sci. 7, 119–124. doi: 10.1016/s1364-6613(03)00031-7
Cohen-Zimerman, S., Cristofori, I., Zhong, W., Bulbulia, J., Krueger, F., Gordon, B., et al. (2020). Neural underpinning of a personal relationship with God and sense of control: A lesion-mapping study. Cogn. Affect. Behav. Neurosci. 20, 575–587. doi: 10.3758/s13415-020-00787-4
Cristofori, I., Bulbulia, J., Shaver, J. H., Wilson, M., Krueger, F., and Grafman, J. (2016). Neural correlates of mystical experience. Neuropsychologia 80, 212–220. doi: 10.1016/j.neuropsychologia.2015.11.021
Cristofori, I., and Grafman, J. (2017). “Neural underpinnings of the human belief system,” in Processes of Believing: The Acquisition, Maintenance, and Change in Creditions New Approaches to the Scientific Study of Religion, eds. H.-F. Angel, L. Oviedo, R. F. Paloutzian, A. L. C. Runehov, and R. J. Seitz (Cham: Springer International Publishing), 111–123.
Cristofori, I., Viola, V., Chau, A., Zhong, W., Krueger, F., Zamboni, G., et al. (2015). The neural bases for devaluing radical political statements revealed by penetrating traumatic brain injury. Soc. Cogn. Affect. Neurosci. 10, 1038–1044. doi: 10.1093/scan/nsu155
Cristofori, I., Zhong, W., Cohen-Zimerman, S., Bulbulia, J., Gordon, B., Krueger, F., et al. (2021). Brain networks involved in the influence of religion on empathy in male Vietnam War veterans. Sci. Rep. 11:11047. doi: 10.1038/s41598-021-90481-3
Fiori, K. L., Brown, E. E., Cortina, K. S., and Antonucci, T. C. (2006). Locus of control as a mediator of the relationship between religiosity and life satisfaction: age, race, and gender differences. Mental Health Rel. Culture 9, 239–263. doi: 10.1080/13694670600615482
Fox, M. D., and Raichle, M. E. (2007). Spontaneous fluctuations in brain activity observed with functional magnetic resonance imaging. Nat. Rev. Neurosci. 8, 700–711. doi: 10.1038/nrn2201
Harlow, J. M. (1848). Passage of an Iron rod through the head. Boston Med. Surg. J. 39, 389–393. doi: 10.1056/NEJM184812130392001
Holbrook, C., Izuma, K., Deblieck, C., Fessler, D. M. T., and Iacoboni, M. (2016). Neuromodulation of group prejudice and religious belief. Soc. Cogn. Affect. Neurosci. 11, 387–394. doi: 10.1093/scan/nsv107
Hood, R. W. (1975). The construction and preliminary validation of a measure of reported mystical experience. J. Sci. Study Rel. 14, 29–41. doi: 10.2307/1384454
Krueger, F., and Grafman, J. (2017). The Neural Basis of Human Belief Systems. Available online at: https://www.routledge.com/The-Neural-Basis-of-Human-Belief-Systems/Krueger-Grafman/p/book/9781138109896 (accessed August 28, 2022).
Lawrence, R. T. (1997). Measuring the image of god: the god image inventory and the god image scales. J. Psychol. Theol. 25, 214–226.
Levy, N. (2017). Religious beliefs are factual beliefs: content does not correlate with context sensitivity. Cognition 161, 109–116. doi: 10.1016/j.cognition.2017.01.012
Marek, S., Tervo-Clemmens, B., Calabro, F. J., Montez, D. F., Kay, B. P., Hatoum, A. S., et al. (2022). Reproducible brain-wide association studies require thousands of individuals. Nature 603, 654–660. doi: 10.1038/s41586-022-04492-9
McGilchrist, I. (2012). The Master and His Emissary: The Divided Brain and the Making of the Western World. Loondon: Yale University Press.
Moretti, L., Dragone, D., and di Pellegrino, G. (2009). Reward and social valuation deficits following ventromedial prefrontal damage. J. Cogn. Neurosci. 21, 128–140. doi: 10.1162/jocn.2009.21011
Newberg, A. B., Wintering, N. A., Morgan, D., and Waldman, M. R. (2006). The measurement of regional cerebral blood flow during glossolalia: a preliminary SPECT study. Psychiatry Res. Neuroimag. 148, 67–71. doi: 10.1016/j.pscychresns.2006.07.001
Newton, A. T., and McIntosh, D. N. (2010). Specific religious beliefs in a cognitive appraisal model of stress and coping. Int. J. Psychol. Rel. 20, 39–58. doi: 10.1080/10508610903418129
Norenzayan, A., Gervais, W. M., and Trzesniewski, K. H. (2012). Mentalizing deficits constrain belief in a personal god. PLoS ONE 7, e36880. doi: 10.1371/journal.pone.0036880
Oviedo, L., and Szocik, K. (2020). Religious—and other beliefs: how much specificity? Sage Open 10:2158244019898849. doi: 10.1177/2158244019898849
Raffone, A., Marzetti, L., Del Gratta, C., Perrucci, M. G., Romani, G. L., and Pizzella, V. (2019). Toward a brain theory of meditation. Prog. Brain Res. 244, 207–232. doi: 10.1016/bs.pbr.2018.10.028
Raichle, M. E. (2009). A brief history of human brain mapping. Trends Neurosci. 32, 118–126. doi: 10.1016/j.tins.2008.11.001
Raymont, V., Salazar, A. M., Krueger, F., and Grafman, J. (2011). “Studying injured minds” – the vietnam head injury study and 40 years of brain injury research. Front. Neurol. 2:15. doi: 10.3389/fneur.2011.00015
Rorden, C., Fridriksson, J., and Karnath, H-O. (2009). An evaluation of traditional and novel tools for lesion behavior mapping. Neuroimage 44, 1355–1362. doi: 10.1016/j.neuroimage.2008.09.031
Schjoedt, U., Sørensena, J., Nielboa, K. L., Xygalatasa, D., Mitkidisa, M., and Bulbulia, J. (2013). Cognitive resource depletion in religious interactions. Religion Brain Behav. 3, 39–86. doi: 10.1080/2153599X.2012.736714
Schjoedt, U., Stodkilde-Jorgensen, H., Geertz, A. W., Lund, T. E., and Roepstorff, A. (2011). The power of charisma–perceived charisma inhibits the frontal executive network of believers in intercessory prayer. Soc. Cogn. Affect. Neurosci. 6, 119–127. doi: 10.1093/scan/nsq023
Seitz, R. J. (2022). Beliefs: a challenge in neuropsychological disorders. J Neuropsychol 16, 21–37. doi: 10.1111/jnp.12249
Seitz, R. J., Paloutzian, R. F., and Angel, H.-F. (2018). From believing to belief: a general theoretical model. J. Cogn. Neurosci. 30, 1254–1264. doi: 10.1162/jocn_a_01292
Siddiqi, S. H., Schaper, F. L. W. V. J., Horn, A., Hsu, J., Padmanabhan, J. L., Brodtmann, A., et al. (2021). Brain stimulation and brain lesions converge on common causal circuits in neuropsychiatric disease. Nat. Human Behav. 5, 1707–1716. doi: 10.1038/s41562-021-01161-1
Van Leeuwen, N. (2014). Religious credence is not factual belief. Cognition 133, 698–715. doi: 10.1016/j.cognition.2014.08.015
Van Leeuwen, N. (2018). The factual belief fallacy. Contem. Prag. 15, 319–343. doi: 10.1163/18758185-01503004
Zahodne, L. B., Nowinski, C. J., Gershon, R. C., and Manly, J. J. (2014). Which psychosocial factors best predict cognitive performance in older adults? J. Int. Neuropsychol. Soc. 20, 487–495. doi: 10.1017/S1355617714000186
Keywords: religious belief, cognition, social cognition, lesions mapping, dorsolateral prefrontal cortex, ventromedial prefrontal cortex
Citation: Cristofori I, Cohen-Zimerman S, Bulbulia J, Gordon B, Krueger F and Grafman J (2022) The neural underpinning of religious beliefs: Evidence from brain lesions. Front. Behav. Neurosci. 16:977600. doi: 10.3389/fnbeh.2022.977600
Received: 30 June 2022; Accepted: 20 September 2022;
Published: 06 October 2022.
Edited by:
Rüdiger J. Seitz, Heinrich Heine University of Düsseldorf, GermanyReviewed by:
Bruno J. Weder, University of Bern, SwitzerlandCopyright © 2022 Cristofori, Cohen-Zimerman, Bulbulia, Gordon, Krueger and Grafman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Irene Cristofori, aWNyaXN0b2ZvcmlAaXNjLmNucnMuZnI=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.