 Pauliana Lamounier1,2*
Pauliana Lamounier1,2* Victória Franco Gonçalves1
Victória Franco Gonçalves1 Isabela Carvalho Queiroz2
Isabela Carvalho Queiroz2 Débora Aparecida Gobbo1
Débora Aparecida Gobbo1 Marina Nahas Dafico Bernardes1
Marina Nahas Dafico Bernardes1 Claudiney Cândido Costa1
Claudiney Cândido Costa1 Hugo Valter Lisboa Ramos1
Hugo Valter Lisboa Ramos1 Fayez Bahmad Jr.2
Fayez Bahmad Jr.2- 1Department of Otorhinolaryngology, Rehabilitation and Readaptation Center Dr. Henrique Santillo (CRER), Goiânia, Brazil
- 2Department of Health Science, University of Brasília, Brasília, Brazil
Introduction: Hearing loss affects ~1. 5 billion people worldwide and is the greatest risk factor for tinnitus, a condition that can further worsen people's quality of life, lead to high anxiety and depression, and affect general health and wellbeing.
Objectives: This study aimed to assess the impact of cochlear implants (CIs) on tinnitus perception and quality of life and their relationship with psychological disorders, such as depression and anxiety.
Methods: Thirty adults with profound bilateral hearing loss who were candidates for CI surgery and experienced tinnitus were assessed using the Tinnitus Handicap Inventory (THI), the Visual Analog Scale (VAS), the World Health Organization Quality of Life Instruments–Bref (WHOQOL-BREF), and the Hospital Anxiety and Depression Scale questionnaires at four different time points: preoperatively, 7 days after cochlear implant activation, and 3 and 6 months after cochlear implant surgery. The International Outcome Inventory CI was applied at 3 and 6 months, and the Glasgow Benefit Inventory (GBI) questionnaire was applied at 6 months.
Results: The VAS and THI scores improved; however, significant improvements were only observed in the THI scores 6 months post-surgery. Time spent using hearing aids did not correlate significantly with speech recognition test scores, nor were the changes in the preoperative THI score and VAS scores or the changes in the speech recognition test scores 6 months post-surgery significantly correlated. We observed a decrease in anxiety and depression scores at the 6-month follow-up compared to the preoperative period.
Conclusion: The THI scores significantly increased after CI surgery, suggesting that the tinnitus had improved. Improved anxiety and depression scores after CI surgery were also observed. The WHOQOL-BREF quality-of-life self-evaluation scores, as well as the environment and general domains, significantly improved as well.
Introduction
According to the World Health Organization's 2021 World Report on Hearing, ~1.5 billion people live with some degree of hearing loss worldwide. Moreover, ~430 million people, accounting for 5% of the world's population, utilize hearing rehabilitation services. Untreated hearing loss can have a significant effect on individuals' quality of life, work, cognition, and social interactions (Chadha et al., 2021).
Hearing loss is the greatest risk factor for tinnitus. The association of these two conditions can worsen patients' quality of life, lead to high anxiety and depression levels, and affect patients' wellbeing and global health. Tinnitus can also cause mood changes, sleep disorders, irritability, frustration, difficulty concentrating, and stress (Besteher et al., 2019; Sarac et al., 2020; Opperman et al., 2021).
Tinnitus reflects a complex interplay of peripheral and central auditory mechanisms. Numerous studies have suggested that the hyperexcitability linked to tinnitus is associated with acute GABAergic disinhibition in the ascending auditory pathway. Recent research has suggested that tinnitus involves not only hearing anatomy but also aberrant neural activity and interactions with other regions of the central nervous system, which are associated with emotion, attention, anguish, memory, and motor activity (de Borges et al., 2021; Eggermont and Roberts, 2012; Onishi et al., 2018; Féres and Cairasco, 2001). The amygdala and hippocampus are two large limbic regions that receive direct or indirect neural input from the central auditory nervous system. Tinnitus discomfort was first related to a bilateral increase in the effective connectivity between the amygdala and superior temporal gyrus. This process suggests that the amygdala sends a strong negative emotional signal to the auditory cortex and influences how acoustic information is interpreted (Eggermont and Roberts, 2012). The limbic system can identify an irrelevant signal (such as tinnitus) and stop the undesired signal from reaching the auditory cortex under normal conditions. However, the limbic region fails to recognize and inhibit tinnitus signals under abnormal conditions. This is one of the mechanisms responsible for chronic tinnitus (Onishi et al., 2018; Féres and Cairasco, 2001).
Tinnitus perception is associated with negative emotions, such as anguish, if an unspecific distress network is activated; tinnitus persists when the memory network becomes active. Despite the secondary plasticity generated by cochlear implants and auditory conditioning or training, managing chronic changes caused by limbic system activation must be considered to benefit patients with hearing loss and tinnitus globally (Eggermont and Roberts, 2012).
New auditory input generated by the cochlear implant (CI) can stimulate neural plasticity, which is essential for developing new brain connections that will be key for the appropriate design of auditory skills (Knipper et al., 2020). Several studies have assessed the suppressive effect of CIs on tinnitus (de Borges et al., 2021); however, because tinnitus affects more than auditory structures, further exploration into strategies to improve the quality of life of patients suffering from hearing loss is justified (Eggermont and Roberts, 2012).
Therefore, assessing the impact of CIs on tinnitus, quality of life, anxiety, and depression after surgery based on validated questionnaires was the aim of this study.
Methods
Research design
This prospective cohort study included 30 adult patients older than 18 years who presented with bilateral profound hearing loss, who were candidates for CI surgery, and who reported experiencing tinnitus. Patients signed an informed consent form (ICF) and provided information about demographic data, comorbidities, etiology, and time spent using hearing aids. Questionnaires [the Tinnitus Handicap Inventory (THI), the Visual Analog Scale (VAS), the WHOQOL-BREF, and the Hospital Anxiety and Depression Scale (HADS)] were administered at four time points (preoperative, 7 days post-cochlear implant (CI) activation, and 3 and 6 months post-CICI surgery). The International Outcome Inventory CI (IOI-CI) and Glasgow Benefit Inventory (GBI) questionnaires were administered 3 and 6 months after implant activation. All questionnaires were administered in Portuguese. The speech recognition test was performed 6 months after CI surgery to measure the resulting functional gain.
Procedures
CI surgery
The CI surgery was performed by two surgeons (in the cities of Goiânia and Brasília, Brazil). The CI brand, side, type of inserted electrode, and access route for electrode insertion were recorded for further descriptive analysis.
Functional gain of CIs
The benefit and measurement of functional gain post-CI were evaluated 6 months after CI surgery using the Speech Recognition Percentage Index (IPRF) in an open setting and in silence, testing disyllables and sentences. Correlations between IPRF scores and hearing loss time, hearing aid use time, and tinnitus perception were also evaluated.
Testing was carried out in an acoustic booth treated, calibrated, and illuminated at an intensity of 60/65 dBNA at 0° azimuth. Audiometric calibrations followed the ANSI S3.6–1969/89 S.3.13-1072 calibration standards; ISO 389–1975; IEC 645.
A list of 10 sentences with 50 phonetically balanced characters was presented, developed, and validated by the Center for Audiological Research (CPA, Bauru, Brazil), with each character correction, determined by the evaluation protocol, having a value of 2 points (2%), and a list containing 25 phonetically balanced two-syllable words prepared and validated by the CPA. Each correct word had a value of 4 points (4%), resulting in an achievable total of 100% for each test.
Two examiners (one in Brasília and one in Goiânia, duly trained by the two researchers) carried out the tests. The examiners instructed the patients to repeat the words and sentences according to their listening comprehension (even if they did not understand the sentence completely). After certifying that the patients understood the test, they began the test with the statement “Repeat the statement, please”, preventing the patients from lip reading.
Questionnaires
Tinnitus Handicap Inventory
The THI comprises 25 questions divided into three scales: the functional subscale (F), which measures discomfort caused by tinnitus in mental, social, labor, and physical functions; the emotional subscale (E), which measures affective responses, such as anxiety, anger, and depression; and the catastrophic subscale (C), which quantifies the despair and basic disability of affected people to live with, or eliminate, symptoms. There are three possible answers to each (“yes”, 4 points; “sometimes”, 2 points; and “no”, 0 points), and the questionnaire is scored from 0 to 100 points (Ferreira et al., 2005; Newman et al., 1996). Tinnitus is classified as very light (0–16%), light (18–36%), moderate (38–56%), severe (58–76%), or catastrophic (78–100%). This questionnaire was administered at four time points.
Visual Analog Scale
The VAS for tinnitus load was the second instrument applied. This continuous scale is by patients to evaluate general discomfort caused by tinnitus in the week before its application, and scores range from 0 to 10, with 10 representing intense tinnitus. This questionnaire was administered at four different time points.
WHOQOL-BREF
The WHOQOL-BREF is a 26-item instrument comprising six domains [physical, psychological, social relationships, self-evaluation quality of live (QV), environment, and general domain] and one general domain. The questionnaire was completed using self-evaluations of both quality of life and general health. Each domain was independently evaluated, and each item was rated using a 1–5 scoring system.
Hospital Anxiety and Depression Scale
The HADS is a self-report questionnaire consisting of 14 items, with seven items focussing on anxiety (anxiety subscale) and seven items focussing on depression (depression subscale). Each item's score ranges from 0 to 3 based on symptom frequency; a total score of 8 points, or more, on one or both subscales indicates the presence of depressive or anxiety disorders.
Glasgow Benefit Inventory
The GBI, consisting of 18 questions that use a 5-point Likert scale, is a generic questionnaire used to measure results after otorhinolaryngological procedures. The questionnaire addresses changes in health conditions after any intervention and is based on the total score and the three subscale scores: general health condition, physical health, and social support.
International Outcome Inventory-Cochlear Implant
The IOI-CI consists of seven items based on a 1–5 response scale. Low scores indicate worse outcomes. The questionnaire is divided into two factors: Factor 1 refers to the joint analysis of the domains “daily use of IC,” “benefit,” “satisfaction,” and “quality of life” to indicate the relationship between a user and its CI. Factor 2 refers to the analysis of the domains “limitations and residual activities,” “restriction of residual participation,” and “impact on others,” which, together, indicate a user's relationship with their social medium (Cox and Alexander, 2002). Participants were grouped into happy and unhappy groups based on the questionnaire's factorial scoring: Individuals scoring equal to or lower than 2.5 were considered unhappy, and those scoring higher than 2.5 were considered happy.
Selection criteria
Inclusion criteria
Individuals older than 18 years, of both sexes, with bilateral profound hearing loss who are candidates for cochlear implantation were selected for the study.
Exclusion criteria
Individuals with cerebellopontine angle tumors, middle and external ear diseases, psychiatric and/or cognitive disorders that prevented them from understanding the exams and questionnaires, as well as illicit drug users, were excluded from the study.
Standard protocol approvals, registrations, and patient consent
The study was approved by the Ethics Committee under register n. 36929420.1.0000.5082. All participants were informed about the study aims and methodology; those who agreed to participate signed the ICF. The participants who declined to participate at any stage did not suffer any penalty. No financial incentives were offered to participants who agreed to enroll in the study.
Sample
The convenience sample consisted of 34 individuals with profound bilateral hearing loss who were candidates for CI surgery, according to the criteria of the GM/MS (Gabinete do Ministro/Ministério da Saúde) Ordinance n. 2776 (18 December 2014) and had tinnitus. In total, four patients declined to participate in the follow-up throughout the study, resulting in a final sample of 30 patients. To have 80% power to detect a clinically important difference from the preoperative period in terms of score changes, the sample size calculation indicated that 30 participants were required during the 6-month follow-up period.
Statistical analysis
The statistical analysis, following the methods of Gibbons and Hedeker (2006), is described in the following subsections.
THI and VAS
VAS scores were dichotomized into mild to moderate (VAS < 5) and moderate to intense (VAS ≥ 5); values on the THI scale were dichotomized into moderate (THI < 47) and moderate to catastrophic (THI ≥ 47). Dichotomizing was performed due to the study's sample size. Generalized equation models (GEMs), with binary logit functions, were used to assess the effects of mild and moderate occurrence on both scales over the assessment period when using the perioperative assessment as the reference. Odds ratios (ORs) were estimated and 95% confidence intervals (CIs) were calculated at 7 days, 3 months, and 6 months and compared to the preoperative period. Differences of p < 0.05 were considered statistically significant.
HADS
The HADS scale scores were dichotomized into “anxiety or depression” (HADS ≥ 9) and “without anxiety or depression” (HADS < 9). GEMs with binary logit functions were used to assess the effects of anxiety and depression occurrence over the assessment period. The assessment conducted preoperatively was used as a reference. ORs were estimated and the 95% CIs were calculated at 7 days, 3 months, and 6 months and compared to the preoperative values. Differences of p < 0.05 were considered statistically significant.
WHOQOL-BREF
Longitudinal differences between groups were evaluated by applying linear mixed-effects models with symmetric covariance structures to repeated measurements adjusted for preoperative measurements. The main focus of the analysis was on the longest period observed after the preoperative period in several WHOQOL-BREF domains (physical, psychological, social relationships, environment, quality-of-life self-evaluation, and general elements). Comparisons among the three assessed time points from the preoperative time points were performed when the general p-value recorded for changes over the follow-up time was lower than 0.05. A p-value of < 0.05 was considered statistically significant. SAS 9.4 software was used to complete the statistical analyses.
GBI
General health, physical health, and social support scales, such as the mean, the median, the standard deviation, and the maximum, minimum, and quartile intervals, were calculated for descriptive measurements.
IOI-CI
The mean IOI-CI values measured at 3 and 6 months were compared using paired Student's t-tests. A p-value of.05 was considered statistically significant.
Results
Sample descriptive results
In total, 10 participants were male (33.3%), 20 were female (66.7%), and the mean and the standard deviation value for age was 46.27 ± 14.90 years. Comorbidities are shown in Figure 1, hearing loss features are shown in Figure 2, and etiological diagnosis is shown in Figure 3. The cochlear implant features, laterality, electrodes used, and access pathway to electrode insertion are shown in Table 1.
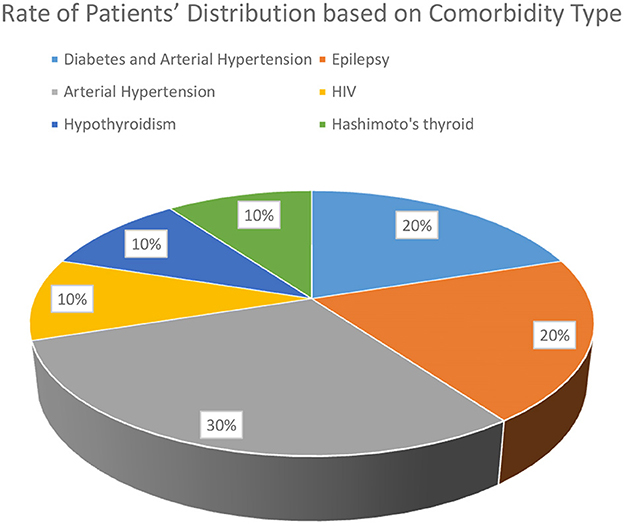
Figure 1. Percentage distribution of patients by type of comorbidity.
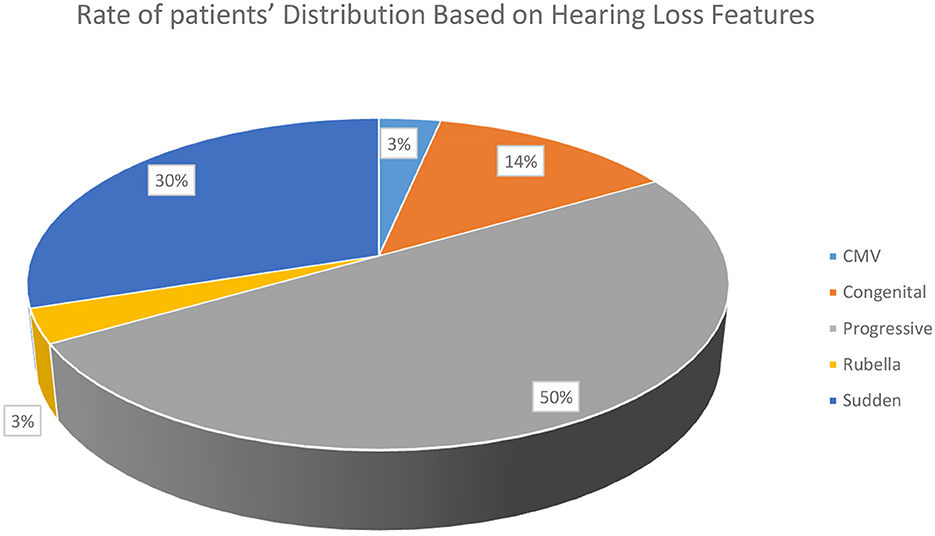
Figure 2. Percentage distribution of patients by hearing loss characteristic.
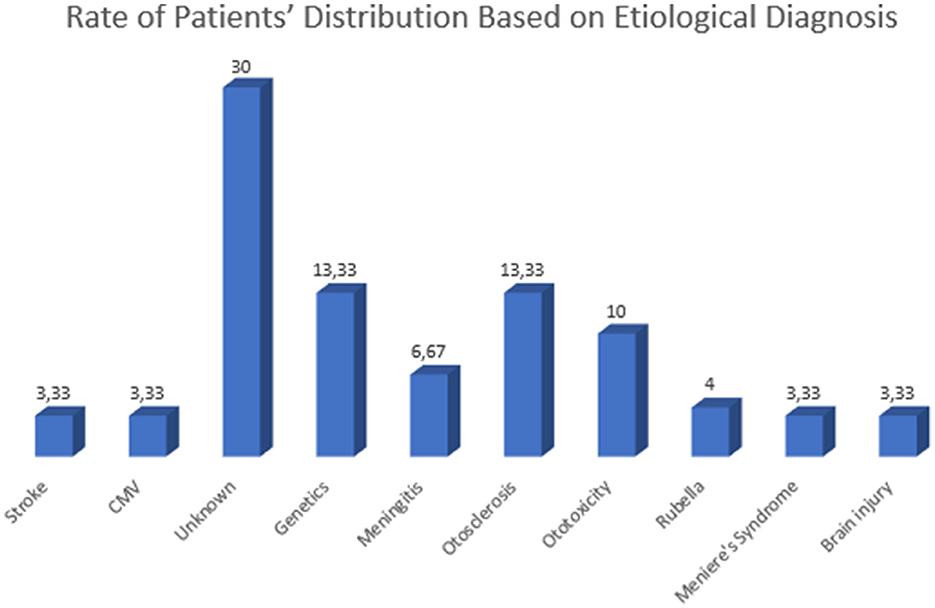
Figure 3. Percentage distribution of patients by etiological diagnosis.
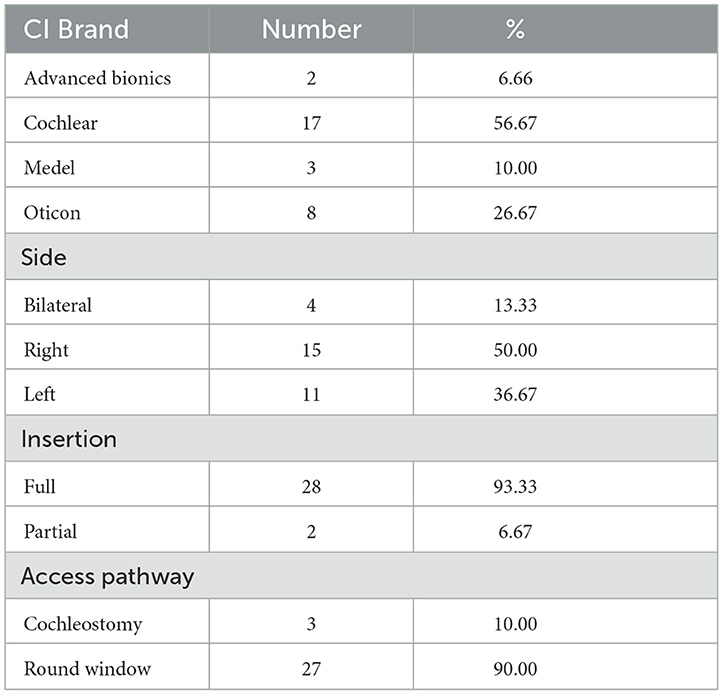
Table 1. Distribution of cochlear implant (CI) surgical features adopted for patients in the sample.
Featuring the performed procedures
Functional gain of CIs
Functional gain was analyzed 6 months after CI surgery through a speech recognition test for sentences and disyllables.
The mean speech recognition test value at 6 months for sentences was 86 ± 20%, ranging from 36 to 100%. The mean value of the speech recognition test at 6 months recorded for disyllables was 69 ± 22%, ranging from 28 to 96% (Table 2).
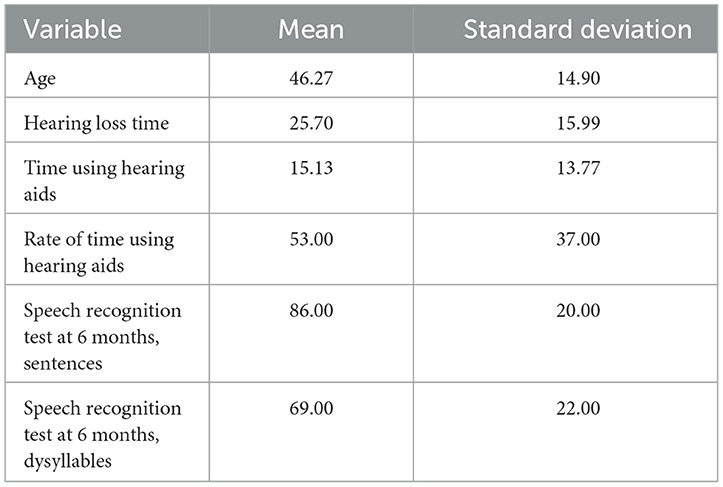
Table 2. Descriptive measurements recorded for variables “hearing loss time,” “time using hearing aids,” and “speech recognition test applied to sentences and disyllables.”
The mean hearing loss duration was 25.7 years. The correlations between hearing loss time and the results of the speech recognition test at 6 months for sentences and disyllables were not statistically significant [r = −0.27, 95% CI (−0.58, 0.11), p = 0.1487, and r = −0.14, 95% CI (−0.48, 0.24), p = 0.4570, respectively].
The mean hearing aid use time was 15.12 years. The correlations between the time spent using hearing aids and the results of the speech recognition test at 6 months for sentences and disyllables were not statistically significant [r = 0.01, 95% CI (−0.36, 0.37), p = 0.9706 and r = −0.07, 95% CI (−0.43, 0.30), p = 0.6971, respectively].
Questionnaire results
THI and VAS
The mean VAS score recorded preoperatively was 4.47 ± 2.92, with a minimum of 1 and a maximum of 10 at 6 months; the mean score decreased to 2.30 ± 2.31, with a minimum of 0 and a maximum of 7. The improvement reached 2.17 ± 3.71, and the values ranged from 6 to 10.
The number of patients classified as mild to moderate in terms of the VAS score and THI increased over the follow-up period (Table 3).

Table 3. Number of cases classified as mild to moderate based on VAS and THI.
The mild-to-moderate ORs associated with the VAS scores did not significantly differ over the follow-up period compared to the preoperative period (p-values ranged from 0.1054 to 0.7386). The mild-to-moderate THI scores were not significantly different at 7 days or 3 months compared to the preoperative values (p = 1.0000 and p = 0.1502, respectively). However, patients at 6 months presented 5.21 times greater chances of having mild-to-moderate responses in THI than at the preoperative time (p = 0.0107; Table 4).
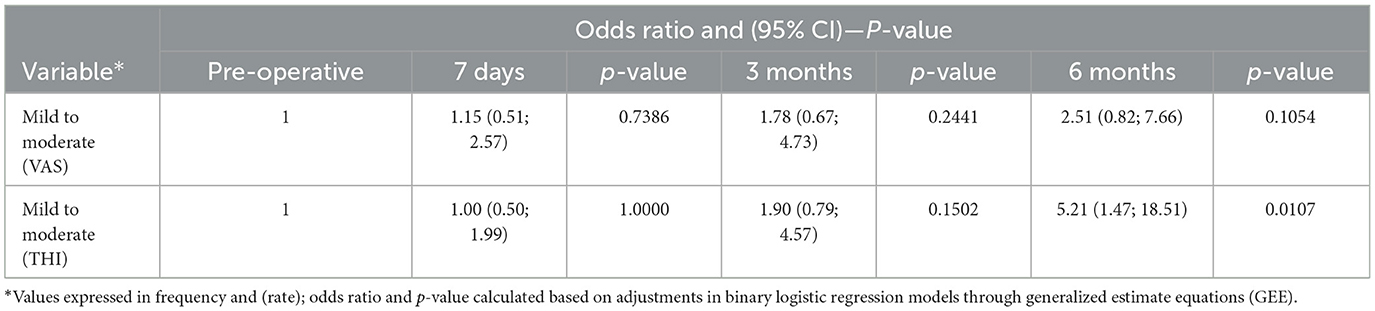
Table 4. Odds ratio and (95% CI)—p-value set for mild-to-moderate classification, based on VAS and THI.
Significant correlations between the THI score and the speech recognition test score at 6 months for sentences and disyllables were not significant [r = −0.14, 95% CI (−0.48, 0.24), p = 0.4543, and r = −0.08, 95% CI (−0.43, 0.30), p = 0.6879, respectively].
The correlation between the VAS score and the speech recognition test score at 6 months for sentences and disyllables was also not statistically significant [r = −0.02, 95% CI (−0.38, 0.35), p = 0.9229, and r = −0.06, 95% CI (−0.41, 0.32), p = 0.7648, respectively].
In total, five patients (16.67%) in our sample presented with worsened tinnitus according to the THI when we compared their results from the postoperative questionnaires at 6 months to the preoperative data. In total, the VAS score worsened in four of these five patients. In terms of etiology, two patients had sudden deafness, one of whom was diagnosed with deafness because of meningitis; the other patient had deafness due to unknown causes. Three patients had a diagnosis of congenital and progressive hearing loss, two because of unknown causes and one because of rubella. However, worsening only presented changes in the tinnitus category, based on the THI and VAS classifications, in three patients (10% of the sample).
WHOQOL-BREF
The mean values recorded for the physical domains did not significantly change over the follow-up time compared to the preoperative values (p = 0.1961). The mean values observed for the psychological domain did not significantly change over the follow-up time compared to the preoperative values (p = 0.2180). The mean values recorded for the social relationships domain did not significantly change over the follow-up period compared to the preoperative values (p = 0.1748). The mean values recorded for the environment domain presented significant changes over the follow-up time compared to the preoperative time in at least one follow-up time point (p = 0.0189). The mean value recorded at 6 months was significantly greater (0.67) than the preoperative value (p = 0.0411; Table 5).
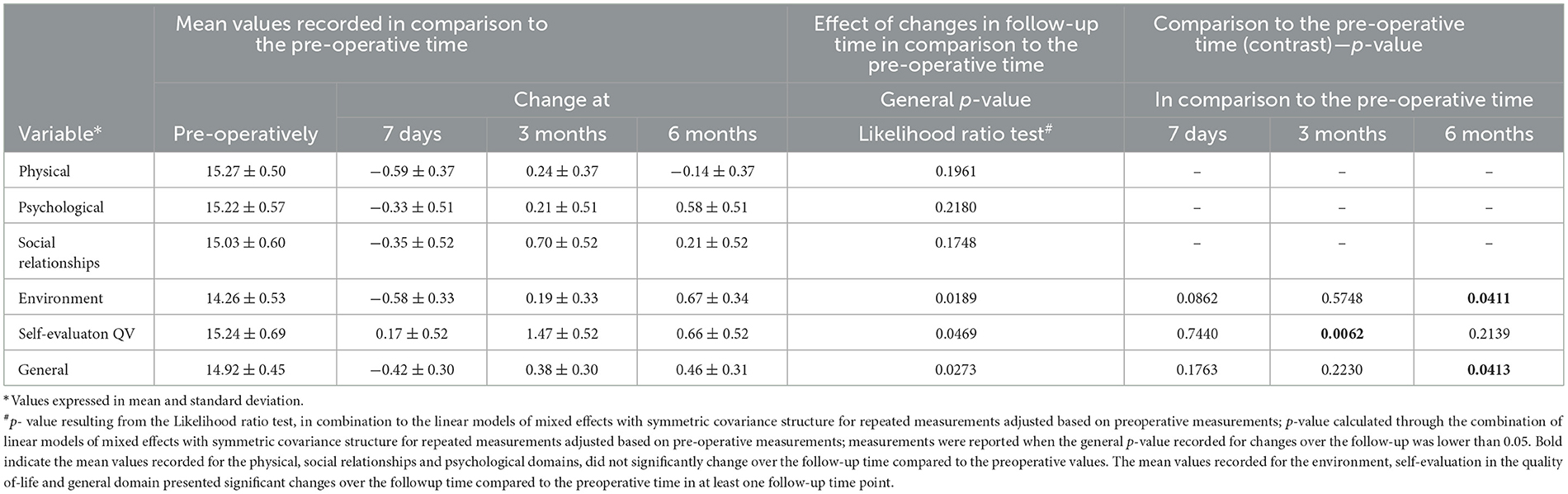
Table 5. Effect of changes over the follow-up time on the WHOQOL-BREF domains.
The mean values recorded for self-assessment in the quality-of-life domain presented significant changes over the follow-up time compared to the preoperative time in at least one follow-up time point (p = 0.0469). The mean value observed at 3 months was significantly greater (1.47) than the preoperative value (p = 0.0062). The mean values recorded for the general domain presented significant changes over the follow-up time compared to the preoperative time in at least one follow-up (p = 0.0273). The mean value recorded at 6 months was significantly greater (0.46) than the preoperative value (p = 0.0413; Figure 4).
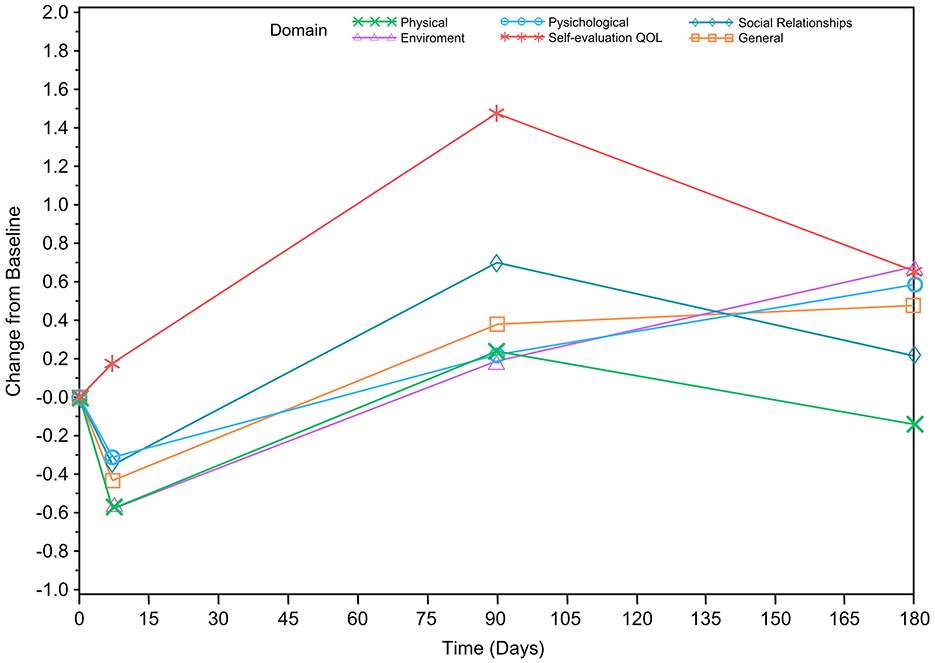
Figure 4. Effect of change over the follow-up period in relation to the preoperative period for the different WHOQOL domains.
HADS
Individuals with scores higher than, or equal to, 8 on the HADS questionnaire were considered anxiety and depression carriers (Table 6). There was a decrease in the incidence of anxiety and depression, according to the analysis carried out at 3 and 6 months after surgery, but the ORs for anxiety or depression were not statistically significant over the follow-up period in comparison to the preoperative time (p-values ranged from 0.857 to 0.6542; Table 7).

Table 6. Number of anxiety and depression cases according to the HADS scale.

Table 7. Odds ratio and (95 % CI)—p-value# recorded for anxiety and depression according to the HADS scale.
GBI
Positive values on the GBI (higher than 0) indicated satisfaction with the CI. The general health scale recorded the best performance, with a mean value of 63.61 ± 28.36 and a value ranging from −4.17 to 100.00. By comparison, the physical health scale presented the lowest performance, with a mean value of 23.89 ± 40.28 and a value ranging from −66.67 to 100.00. The measurements recorded for the three scales were positive, indicating an increase in quality of life after the CI procedure (Figure 5).
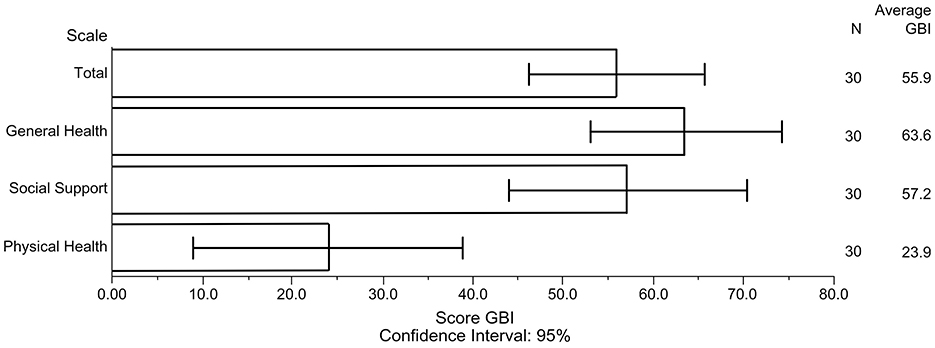
Figure 5. Confidence interval recorded for Glasgow Benefit Inventory's subscales.
IOI-CI
The mean IOI-CI value recorded at 3 and 6 months was >2.5; therefore, patients in our sample were happy with the CI surgery.
The seven items in the questionnaire were based on a 1–5 response scale, with the lowest scores indicating worse outcomes. Initial mean values recorded for the IOI-CI and values recorded at 6 months were compared using the non-parametric Wilcoxon signed-rank test. Differences of p < 0.05 were considered statistically significant.
The mean value recorded for the IOI-CI at 6 months did not significantly differ from that recorded at 3 months (p = 0.39963).
Discussion
Our cohort study included 30 patients and mainly aimed to assess the impact of CIs on tinnitus perception and determine whether the degree of auditory improvement in the speech recognition tests after cochlear implantation followed the improvement in tinnitus. We also aimed to analyze the correlations among hearing loss duration, duration of hearing aid use, and speech recognition test results. We assessed the impact of hearing loss and tinnitus before and after CI surgery on psychological disorders, such as depression and anxiety, and quality of life.
Tinnitus perception improved in our patients over the 6-month follow-up, but the associated improvement in VAS scores was not statistically significant. The THI score improved at 3 months, but only improvement at 6 months was statistically significant. Patients presented with a 5.21 times greater likelihood of being classified as mild to moderate than as moderate to catastrophic in comparison with the preoperative time.
Much is known about the auditory deprivation time and audiological outcomes after cochlear implantation (Lin et al., 2014; McKay, 2018; Pichora-Fuller, 2015). The more the auditory pathway is stimulated by early hearing loss treatment, the more likely satisfactory speech recognition test outcomes and functional gain due to CI are able to be obtained (Carasek et al., 2022). We observed a mean hearing loss time of 25.7 years and a mean hearing aid use time of 15.12 years; these numbers corresponded to a mean hearing loss duration of 53%. However, the small sample size of the current study precluded a statistically significant correlation between hearing aid use time and optimal speech recognition test scores from being observed. That said, we found satisfactory means values for sentences (78%) and disyllables (77%). We also did not find a correlation between changes in the THI and VAS scores from before surgery to 6 months after surgery, with speech recognition test modifications.
We observed that five patients presented worsened tinnitus (16.67% of the sample), but this worsening created a shift only in the tinnitus category, based on the THI classification, in three patients (10%). Therefore, the results recorded in our study agree with those reported in the literature, just as those reported by Ramakers et al. (2015), who reported tinnitus worsening ranging from 0 to 25% in assessed patients. Only three of these patients presented satisfactory speech recognition tests 6 months after surgery; presumably, they improved, even more so, after a longer follow-up, after longer therapy times, and after auditory training. This is because these factors can consequently improve tinnitus. Some etiologies, especially those capable of causing neural damage, need more time to achieve the same audiological outcomes (Ramakers et al., 2015). The results from our research group demonstrated that patients with meningitis, for example, take longer to achieve speech recognition than patients with otosclerosis. Improvements in tinnitus, in many cases, are accompanied by improvements in speech recognition, which is compatible with the reorganization of the auditory pathway, which requires more time for hearing loss of neural origin (Lamounier et al., 2024).
Some studies report that for patients who have recorded a significant increase in tinnitus sensation, this may coincide with different electrode-insertion depths or the conditions in which patients only had such a perception during the first months after CI surgery and may improve with a longer follow-up (de Borges et al., 2021; Kloostra et al., 2021). Most of the samples were administered with CI electrode array insertion through a round window (27 patients); this access pathway is ideal for auditory preservation because it accounts for less cochlear damage. Therefore, we could not correlate tinnitus worsening in these patients to the insertion pathway or depth because all five patients whose tinnitus worsened had their electrodes fully inserted; four of these patients were administered round window insertion, and one patient was subjected to insertion through cochleostomy.
In a retrospective longitudinal study, Opperman et al. (2021) assessed the effect of tinnitus discomfort on quality of life in adult CI users using a sample of 210 adults. The author reported a significant reduction in tinnitus discomfort up to 2 years after the implant surgery. The secondary plasticity generated by auditory training (speech therapy) and conditioning is part of the cortical reorganization that accounts for improvements in tinnitus, which can often demand a longer duration (Opperman et al., 2021).
A meta-analysis carried out by de Borges et al. (2021) revealed that tinnitus perception scores improved by more than 50% after cochlear implantation based on the applied questionnaires. Ramakers et al. (2015) reported that the THI was the questionnaire most often used in publications included in his systematic review. All six studies that used the THI to measure the CI effect on tinnitus reported significant reductions in scores. This review revealed a decrease in the mean score after unilateral CI in the 18 assessed studies. The total suppression rate recorded for tinnitus ranged from 8 to 45%, and the reduction ranged from 25 to 72%; the scores were stable and ranged from 0 to 36%. Previously, tinnitus development after surgery has been reported to range from 0 to 10% in patients without preoperative tinnitus (Ramakers et al., 2015).
Compared to the preoperative scores, anxiety and depression scores recorded through the HADS questionnaire dropped over the 6-month follow-up. This finding demonstrates that improvement in psychological disorders can occur after CI surgery; however, these findings were not statistically significant. Although questionnaires are subjective tools and the small size of this study may have influenced the conclusions drawn in the current study, our data corroborate several studies on this topic. This improvement in scores aligns with the general improvement observed by patients after auditory skill restoration and their slow return to daily activities. Further improvement may be evident with longer follow-up periods.
Regarding quality of life, assessed using the WHOQOL-BREF, the mean values recorded for the physical, psychological, and social relationship domains did not significantly change over the follow-up period. Mean values recorded for the environment domain at 6 months were significantly different from the preoperative values. This finding reflects improvements in perceptions of financial resources, opportunities to acquire new skills and knowledge, and leisure and transportation. The mean value recorded for quality-of-life self-assessment at 3 months represented a significant increase from the preoperative period. Mean general health evaluation values significantly increased over the follow-up period.
However, based on the graphics, all domains (except for self-assessment) presented a worse quality of life within the first 7 days after CI activation (37 days after surgery). The recorded values suggest a greater need to adjust the expectations of patients about rehabilitation time. Importantly, auditory outcomes and recognition do not emerge immediately after implant activation, but after speech therapy, auditory training, and hours of conversation over the days after implantation are needed; these requirements are fundamental for stimulating auditory pathway reorganization.
Therefore, the relevance of multidisciplinary follow-up is clear; it must be carried out by a team of speech therapists and psychologists, among other professionals, to best adjust this process.
The IOI-CI scores in our sample revealed that most patients were happy with CI surgery, even at the 3-month follow-up. This finding is important for understanding how to address patients' expectations of the rehabilitation process to which they are subjected. Values for all three GBI scale domains—general health status, social support, and physical health—were positive, indicating a better quality of life after cochlear implantation. The general health scale presented the best performance and reflected the general perceptions of social and psychological wellbeing.
The reintegration of individuals into their family life and labor activities returns independence to them, which may be linked to improvements in their perceptions of wellbeing (Olze et al., 2011; Andries et al., 2021; Hallberg et al., 2005; Blazer and Tucci, 2019). In a recent study, de Angelo et al. (2016) compared a set of individuals with CIs to a group of individuals without hearing loss and reported that each group's quality-of-life analysis results were similar to the other.
Tretbar et al. (2019) reported that, in addition to effective auditory rehabilitation, healthcare professionals must monitor psychosocial treatment because of the worsened quality of life caused by disabling hearing loss. Developing a specific psychotherapeutic treatment for patients with auditory disability requires additional research focused on vulnerability factors that can influence the rise of psychological disorders in this population (Tretbar et al., 2019). Our study provides important data concerning the worsening of WHOQOL-BREF scores 7 days after CI activation. Although this finding was not significant, it suggests that measures to prevent patients from declining follow-up can be taken. We recommend a follow-up protocol based on psychotherapy sessions to improve the support provided to these patients 7 days after activation and 3 and 6 months after surgery given the challenges patients face during these periods when adapting to CIs.
Depressive symptoms are important parameters for rehabilitation outcomes in CI patients. The support team and CI users must become oriented and sensitized to the close association between depressive symptoms and the progressive development of speech recognition after the implant, as shown by Heinze-Köhler et al. (2021).
Castiglione et al. (2016) reported improvements in depression levels and cognitive performance in older adults after cochlear implantation and proposed six hypotheses for such an improvement: (a) improvement in social distancing; (b) electrical stimuli to preserve the function and tridimensional dimension of peripheral and central synapses; (c) auditory rehabilitation to neutralize the neuroplasticity negative process; (d) auditory training and speech effects that can positively influence labor memory and learning skills; (e) improvements in motivation, self-esteem, and self-confidence; and (f) the placebo effect.
Sarac et al. (2020) also reported a statistically significant decrease in depression after cochlear implantation. We also observed improvements in anxiety and depression scores; however, these findings were not statistically significant, likely due to the sample size of our study. A longer follow-up time may yield better outcomes given the adaptation time required by CIs and the progressive improvement in speech recognition (Sarac et al., 2020).
Given the relevant connections between the auditory and limbic systems, carrying out a joint analysis of quality of life, anxiety, depression, and audiological outcomes after CI surgery is essential. The amygdala and hippocampus are two large limbic regions that receive direct and indirect neural input from the central auditory system. These projections can affect neural activity and plasticity (Besteher et al., 2019; de Fleck et al., 1999; Pais-Ribeiro et al., 2007; Robinson et al., 1996). After tinnitus is triggered, it can influence emotional and cognitive functions; thus, these patients need a broad approach to manage such a prevailing comorbidity, which can strongly impact the daily life of an individual.
de Sousa et al. (2018) reported that although several studies have shown that adult CI users with postlingual auditory disability report significant improvements in quality of life after implantation, great variability in these data exists. These authors hypothesize that the term quality of life encompasses different life conditions and circumstances preventing a reference score from being established for a given population (Raj-Koziak et al., 2018). Accordingly, in addition to using generic questionnaires about quality of life, such as the WHOQOL-BREF, we also adopted more specific questionnaires, such as the HADS, to assess anxiety and depression and the IOI-CI and GBI to assess the degree of satisfaction with the CI.
One strength of our study was the follow-up period, which involved monitoring the evolution of tinnitus together with quality of life, anxiety, and depression using internationally validated tools. A major limitation of the study was that it was conducted during the COVID-19 pandemic when performing elective surgeries was difficult, which made it difficult to increase the sample size, perhaps influencing the statistical significance of the findings. Another limitation is the different etiologies of hearing loss among the study patients; however, the fact that all patients included had profound bilateral hearing loss reduced the heterogeneity of the sample in relation to the etiology of hearing loss.
Although questionnaires are subjective, those used in our study are internationally well-known and validated tools. Our sample size calculation demonstrated that our study has 80% power to detect a clinically important difference, reassuring the relevance of our data. However, studies based on larger samples and longer follow-up times should be conducted, given the relevance of psychological aspects for patients with hearing loss. This approach is part of hearing-loss recovery and may aid individuals in returning to their full activities. Managing symptoms, such as anxiety and depression, and understanding patient satisfaction with the procedure may substantially contribute to auditory rehabilitation.
The secondary effects of CI surgery must be assessed and reported to patients. Prospective studies allow the assessment of important aspects of auditory rehabilitation in these individuals. Obviously, emotional aspects are more complex and broader, but the reintegration into daily activities leads to greater perceptions of quality of life.
All the cited data demonstrate the possibility of treating tinnitus through CIs under different circumstances. An unorganized auditory pathway caused by hearing loss or tinnitus (as a consequence) can indeed be treated through auditory system reorganization based on a new input, such as a CI.
Conclusion
Changes in the VAS and THI scores revealed that tinnitus improved after CI surgery, with statistically significant findings observed for THI scores. There was no significant correlation between the time spent using hearing aids and the results of the speech recognition test. Moreover, there was no correlation between the THI score and the VAS score preoperatively or at 6 months after surgery, with speech recognition test modifications. Based on the IOI-CI and GBI questionnaires, patients were happy with the CI surgery. Anxiety and depression rates improved after CI surgery, although this improvement Was not statistically significant. The quality-of-life self-assessment, based on the WHOQOL-BREF, and the environment and general domains improved significantly.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Comitê de Ética Leide das Neves Ferreira. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
PL: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Visualization, Writing – original draft. VG: Formal analysis, Writing – review & editing, Data curation, Methodology, Project administration. IQ: Project administration, Writing – review & editing, Resources, Software. DG: Visualization, Formal analysis, Project administration, Resources, Writing – review & editing. MB: Software, Formal analysis, Visualization, Writing – review & editing. CC: Conceptualization, Supervision, Validation, Visualization, Writing – review & editing. HR: Visualization, Validation, Writing – review & editing. FB: Supervision, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Andries, E., Gilles, A., Topsakal, V., Vanderveken, O. M., Van de Heyning, P., Van Rompaey, V., et al. (2021). Systematic review of quality of life assessments after cochlear implantation in older adults. Audiol. Neurootol. 26, 61–75. doi: 10.1159/000508433
Besteher, B., Gaser, C., Ivanšić, D., Guntinas-Lichius, O., Dobel, C., Nenadić, I., et al. (2019). Chronic tinnitus and the limbic system: reappraising brain structural effects of distress and affective symptoms. Neuroimage Clin. 24:101976. doi: 10.1016/j.nicl.2019.101976
Blazer, D. G., and Tucci, D. L. (2019). Hearing loss and psychiatric disorders: a review. Psychol. Med. 49, 891–897. doi: 10.1017/S0033291718003409
Carasek, N., Lamounier, P., Maldi, I. G., Bernardes, M. N. D., Ramos, H. V. L., Costa, C. C., et al. (2022). Is there benefit from the use of cochlear implants and hearing aids in cognition for older adults? A systematic review. Front. Epidemiol. 2:934750. doi: 10.3389/fepid.2022.934750
Castiglione, A., Benatti, A., Velardita, C., Favaro, D., Padoan, E., Severi, D., et al. (2016). Aging, cognitive decline and hearing loss: effects of auditory rehabilitation and training with hearing aids and cochlear implants on cognitive function and depression among older adults. Audiol. Neurotol. 21(Suppl. 1), 21–28. doi: 10.1159/000448350
Chadha, S., Kamenov, K., and Cieza, A. (2021). The world report on hearing. Bull. World Health Organ. 99, 242–242A. doi: 10.2471/BLT.21.285643
Cox, R. M., and Alexander, G. C. (2002). The International Outcome Inventory for Hearing Aids (IOI-HA): psychometric properties of the English version. Int. J. Audiol. 41, 30–35. doi: 10.3109/14992020209101309
de Angelo, T. C. S., Moret, A. L. M., da Costa, O. A., Nascimento, L. T., and sw Alvarenga, K. F. (2016). Qualidade de vida em adultos usuários de implante coclear. Codas 28, 106–112. doi: 10.1590/2317-1782/20162015097
de Borges, A. L. F., Duarte, P. L. E. S., de Almeida, R. B. S., Ledesma, A. L. L., de Azevedo, Y. J., Pereira, L. V., et al. (2021). Cochlear implant and tinnitus-a meta-analysis. Braz. J. Otorhinolaryngol. 87, 353–365. doi: 10.1016/j.bjorl.2020.11.006
de Fleck, M. P. A., Leal, O. F., Louzada, S., Xavier, M., Chachamovich, E., Vieira, G., et al. (1999). Desenvolvimento da versão em português do instrumento de avaliação de qualidade de vida da OMS (WHOQOL-100). Rev. Bras. Psiquiatr. 21, 19–28. doi: 10.1590/S1516-44461999000100006
de Sousa, A. F., Couto, M. I. V., and Martinho-Carvalho, A. C. (2018). Quality of life and cochlear implant: results in adults with postlingual hearing loss. Braz. J. Otorhinolaryngol. 84, 494–499. doi: 10.1016/j.bjorl.2017.06.005
Eggermont, J. J., and Roberts, L. E. (2012). The neuroscience of tinnitus: understanding abnormal and normal auditory perception. Front. Syst. Neurosci. 6:53. doi: 10.3389/fnsys.2012.00053
Féres, M. C. L., and Cairasco, N. G. (2001). Plasticidade do sistema auditivo. Rev. Bras. Otorrinolaringol. 67, 716–720. doi: 10.1590/S0034-72992001000500018
Ferreira, P. É. A., Cunha, F., Onishi, E. T., Branco-Barreiro, F. C. A., and Ganança, F. F. (2005). Tinnitus handicap inventory: adaptação cultural para o Português brasileiro. Pro Fono. 17, 303–310. doi: 10.1590/S0104-56872005000300004
Gibbons, R. D., and Hedeker, D. (2006). Longitudinal Data Analysis. Chicago: John Wiley & Sons; University of Illinois.
Hallberg, L. R. M., Ringdahl, A., Holmes, A., and Carver, C. (2005). Psychological general well-being (quality of life) in patients with cochlear implants: importance of social environment and age. Int. J. Audiol. 44, 706–711. doi: 10.1080/14992020500266852
Heinze-Köhler, K., Lehmann, E. K., and Hoppe, U. (2021). Depressive symptoms affect short- and long-term speech recognition outcome in cochlear implant users. Eur. Arch. Otorhinolaryngol. 278, 345–351. doi: 10.1007/s00405-020-06096-3
Kloostra, F. J. J., de Kleine, E., Free, R. H., Hofman, R., and Van Dijk, P. (2021). Changes in tinnitus by cochlear implantation: a parametric study of the effect of single-electrode stimulation. Audiol. Neurootol. 26, 140–148. doi: 10.1159/000509202
Knipper, M., van Dijk, P., Schulze, H., Mazurek, B., Krauss, P., Scheper, V., et al. (2020). The neural bases of tinnitus: lessons from deafness and cochlear implants. J. Neurosci. 40, 7190–7202. doi: 10.1523/JNEUROSCI.1314-19.2020
Lamounier, P., Carasek, N., Daher, V. B., Costa, C. C., Ramos, H. V. L., de Martins, S. C., et al. (2024). Cochlear implants after meningitis and otosclerosis: a comparison between cochlear ossification and speech perception tests. J. Pers. Med. 14:428. doi: 10.3390/jpm14040428
Lin, F. R., Ferrucci, L., An, Y., Goh, J. O., Doshi, J., Metter, E. J., et al. (2014). Association of hearing impairment with brain volume changes in older adults. Neuroimage 90, 84–92. doi: 10.1016/j.neuroimage.2013.12.059
McKay, C. M. (2018). Brain plasticity and rehabilitation with a cochlear implant. Adv. Otorhinolaryngol. 81, 57–65. doi: 10.1159/000485586
Newman, C. W., Jacobson, G. P., and Spitzer, J. B. (1996). Development of the tinnitus handicap inventory. Arch. Otolaryngol. Head Neck Surg. 122, 143–148. doi: 10.1001/archotol.1996.01890140029007
Olze, H., Szczepek, A. J., Haupt, H., Förster, U., Zirke, N., Gräbel, S., et al. (2011). Cochlear implantation has a positive influence on quality of life, tinnitus, and psychological comorbidity. Laryngoscope 121, 2220–2227. doi: 10.1002/lary.22145
Onishi, E. T., de Coelho, C. C., Oiticica, J., Figueiredo, R. R., de Guimarães, R. C. C., Sanchez, T. G., et al. (2018). Tinnitus and sound intolerance: evidence and experience of a Brazilian group. Braz. J. Otorhinolaryngol. 84, 135–149. doi: 10.1016/j.bjorl.2017.12.002
Opperman, E., le Roux, T., Masenge, A., and Eikelboom, R. H. (2021). The effect of tinnitus on hearing-related quality of life outcomes in adult cochlear implant recipients. Int. J. Audiol. 60, 246–254. doi: 10.1080/14992027.2020.1828633
Pais-Ribeiro, J., Silva, I., Ferreira, T., Martins, A., Meneses, R., Baltar, M., et al. (2007). Validation study of a Portuguese version of the Hospital Anxiety and Depression Scale. Psychol. Health Med. 12, 225–235. quiz 235–237. doi: 10.1080/13548500500524088
Pichora-Fuller, M. K. (2015). Forum on the brain and hearing aids. Am. J. Audiol. 24, 112–112. doi: 10.1044/2015_AJA-14-0067
Raj-Koziak, D., Gos, E., Swierniak, W., Rajchel, J. J., Karpiesz, L., Niedzialek, I., et al. (2018). Visual analogue scales as a tool for initial assessment of tinnitus severity: psychometric evaluation in a clinical population. Audiol. Neurootol. 23, 229–237. doi: 10.1159/000494021
Ramakers, G. G. J., van Zon, A., Stegeman, I., and Grolman, W. (2015). The effect of cochlear implantation on tinnitus in patients with bilateral hearing loss: a systematic review. Laryngoscope 125, 2584–2592. doi: 10.1002/lary.25370
Robinson, K., Gatehouse, S., and Browning, G. G. (1996). Measuring patient benefit from otorhinolaryngological surgery and therapy. Ann. Otol. Rhinol. Laryngol. 105, 415–422. doi: 10.1177/000348949610500601
Sarac, E. T., Ozbal Batuk, M., Batuk, I. T., and Okuyucu, S. (2020). Effects of cochlear implantation on tinnitus and depression. ORL J. Otorhinolaryngol. Relat. Spec. 82, 209–215. doi: 10.1159/000508137
Keywords: hearing loss, tinnitus, cochlear implant, quality of life, anxiety, depression
Citation: Lamounier P, Gonçalves VF, Queiroz IC, Gobbo DA, Bernardes MND, Costa CC, Ramos HVL and Bahmad F Jr (2024) Improvement of tinnitus, anxiety, and depression following cochlear implant surgery: a prospective cohort study. Front. Audiol. Otol. 2:1436372. doi: 10.3389/fauot.2024.1436372
Received: 22 May 2024; Accepted: 21 October 2024;
Published: 16 December 2024.
Edited by:
Grant Searchfield, The University of Auckland, New ZealandReviewed by:
Maria Nicastri, Sapienza University of Rome, ItalyBrian Richard Earl, University of Cincinnati, United States
Emma Stapleton, The University of Manchester, United Kingdom
Copyright © 2024 Lamounier, Gonçalves, Queiroz, Gobbo, Bernardes, Costa, Ramos and Bahmad. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pauliana Lamounier, cGF1bGlhbmFsYW1vdW5pZXJvcmxAZ21haWwuY29t