 Vera-Genevey Hlayisi
Vera-Genevey Hlayisi Vidya Ramkumar
Vidya Ramkumar Lucretia Petersen
Lucretia Petersen Barnabas Vangerwua2,4
Barnabas Vangerwua2,4
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Audiol. Otol., 09 July 2024
Sec. Tinnitus
Volume 2 - 2024 | https://doi.org/10.3389/fauot.2024.1419219
This article is part of the Research TopicAdvancing Audiology Practice and Knowledge at the World Congress of Audiology 2024: A Comprehensive CollectionView all 12 articles
Historically, modern audiology evolved from the United States of America (USA) after the Second World War, where hearing rehabilitation programs were established across the country. Since then, audiology practice and the profession as a whole has expanded from the west to the far east and global south with considerable contextual variations. Thus, the purpose of this paper is to increase conversation and engagement on definitions and the drawbacks of a single lens approach to the use of best practice guidelines in Audiology. It is important to develop a more expansive lens as influenced by different contexts such as Africa, Asia, and South America that will in turn help facilitate a multidimensional approach to audiology practice and what is considered “best practice.”
Historically, mankind over the past centuries had developed different solutions to hearing and vestibular disorders amongst the different ancient civilizations of the world such as the Egyptians, Babylonians, Greeks, Hindu, Byzantine, etc. Some work was recorded as early as 1500 BC. In one of the earliest classic scientific documents, Eber's Scrolls from Egypt, there are descriptions of battle wounds on temporal bones and how they affected hearing and speech. Similarly, another Egyptian text documented a chapter on “Medications for the hard of hearing ear” where treatment could be found for tinnitus, dizziness and hypacusia (Hawkins, 2004). The Greek philosopher Empedocles of Agrigento in Sicily (504-433 BC), was the first to describe the cochlea, named after a seashell found in the Mediterranean region (Gitter, 1990).
Modern audiology evolved from the United States of America (USA) after the Second World War, where hearing rehabilitation programs were established across the country. From this period audiologists have been collaborating with otologists and researchers in related fields to develop techniques to determine not only the degree of hearing loss but also the site of the patient's lesion in the middle ear, cochlea or retrocochlear structures (Jerger, 2019). These techniques developed over time and expertise have become the bedrock of the key technical skills that laid the foundation for the global professionalization of Audiology.
Professionalization is described as the process of acquiring a professional status (Hoyle and John, 1995) characterized by obtaining scientific knowledge through higher education to develop disciplinary skills and competencies (Abrahams et al., 2019). Among health professions, medicine was the first Western profession to achieve wide professionalization and professional autonomy (Brosnan, 2015). Newer emerging professions, especially rehabilitation occupations such as audiology are said to have galvanized resources, status, and influence of medicine as a platform for their own professional development with an empirical, positivist frame (Abrahams et al., 2019). Professions hold the power to determine ways to think and act in their domain of expertise and that power is realized through the formal education process where students learn how to see and think about the world (Montigny, 1995; Evetts, 2014; Abrahams et al., 2019).
For Audiology, the first university program was offered at Northwestern University in the USA, in 1946 under the guidance of Raymond Carhart (Jerger, 2018). During the 1950–60's, audiology practice started emerging in community speech and hearing centers in America, geared primarily to aural rehabilitation and in medical settings audiologists began conducting hearing assessments in Ear Nose and Throat (ENT) clinics (Jerger, 2019). The 1970 and 80's saw the emergence of subspecialty areas: pediatric audiology, educational audiology, industrial audiology, cochlear implants, and assessment of balance function (University of North Carolina, 2021).
Since the inception of audiology professionalization to date, audiology practice and the profession as a whole has expanded from the west to the far east and global south. With this expansion into different regions in the world and growing number of audiology professionals trained, it can be argued that to date training is heavily influenced by North American and British educational models (Tuomi, 1994; Pillay and Kathard, 2018) with limited considerations of the considerable contextual variations needed in curriculum content and clinical practice. Pre-existing evidence on ancient, diverse, indigenous, and regional contextual approaches to hearing care may be overlooked or obscured by operational training and education models that are predominantly reflective of the foundational audiology program largely from the west and global north.
Both knowledge and training should be reframed to include all of the vastly different contexts in which hearing care is provided across the various regions, including the far east and global south (Ng, 2012). This reframing is encouraged by the United Nations (UN) report on indigenous peoples' access to health services (United Nations, 2015) on the inclusion of indigenous knowledge, with content that is diverse, context specific, and relevant. These aspects may be relevant in developing curriculum and training for hearing care professionals (Khoza-Shangase and Mophosho, 2018, 2021). As such, literature on contextual relevance in the profession of audiology argues that the professionalization process may be using a single lens that views the western knowledge as the only norm, and inadvertently impact what is considered current best practice (Mignolo, 2009; Ng, 2012; Khoza-Shangase and Mophosho, 2018, 2021).
Currently most healthcare professional bodies use position statements, best practice recommendations and/or clinical practice guidelines to describe how audiology clinical services should be provided. These terminologies are used interchangeably, yet they do not always mean the same. While a clear distinction between position statements, best practice, recommendations and clinical practice guidelines is yet to be made in audiology literature, these descriptions are often used as a blueprint for clinical practice, audiology education, as well as research in audiology practice (see Table 1).
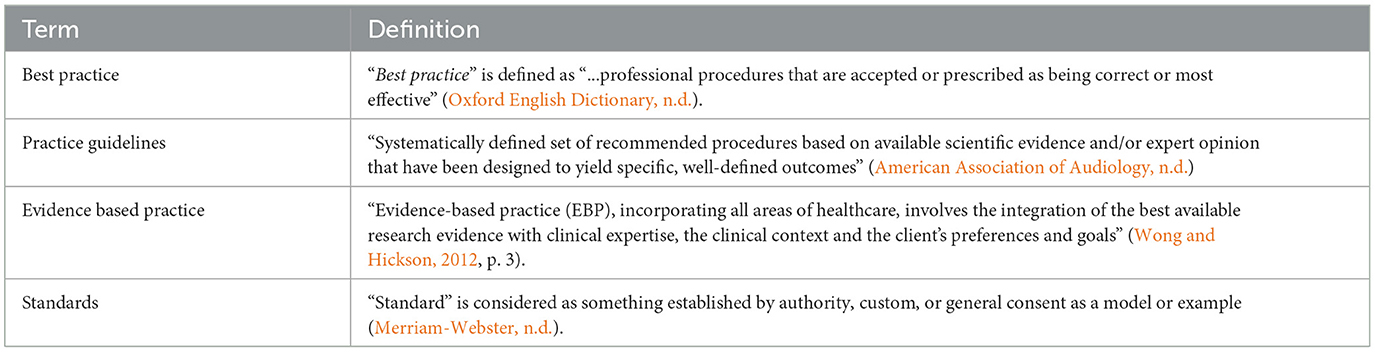
Table 1. Current terminologies and descriptions on “best practice.”
A good practice (method or technique) that has consistently shown results superior to those achieved with other means is often used as a benchmark. The best practices might be used as a kind of checklist against which one can directly evaluate a system's design and code. Lack of adherence to any given best practice, however, does not necessarily imply a lack of quality; they are recommendations that are said to be “best” in most cases and in most contexts, but not all. “A best practice is always subject to improvement as we learn and evolve together” (Mukherji and Albon, 2014). So, this means that guidelines are good, but not always implementable. And best practice is good to get positive results, yet if we do not follow it, it does not mean poor quality. What these definitions do is, they provide the flexibility to factor-in contextual variations such as availability of resources, priorities of different countries, needs of the population, prevailing policies, and power imbalances.
The benchmark descriptions (best practice/guidelines/position statements) are often decided by consensus approach, or evidence-based methods by a group of clinicians/academics/researchers. However, the evidence is often out of context. Therefore, when best practice is viewed from an impact outcome perspective, then contextual variations have to be factored in. “Evidence does not make decisions, people do” (Haynes et al., 2002). Hearing health and illness beliefs differ among populations across the world. For example, South African traditional healers often seek the source of illness (including ear-related diseases) in the supernatural realm (de Andrade and Ross, 2005). Thus, evidence-based practice needs to take into account the heterogeneity of the nature and needs of the context in order to be relevant and implementable (Scheppers et al., 2006; Narayansamy et al., 2014).
The limitedness of context specificity in the existing models of professionalization and clinical practice in Audiology may largely be creating a single lens view to what is best practice, or evidence-based practice. Similar to other rehabilitation professions, the hearing care profession is filled with conventions especially about what is objective and/or subjective evidence (Pillay and Kathard, 2018). Some anecdotal examples of a one size fits all/single lens approach that are some of the basis for this discussion paper are described in Table 2.
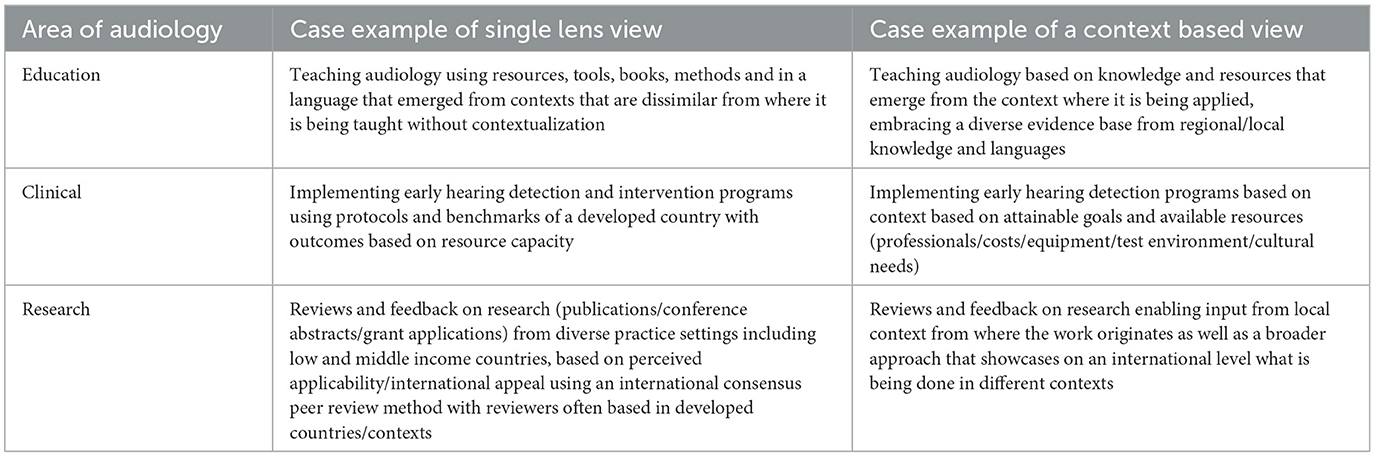
Table 2. Examples of a single lens view vs. a context based view.
If the specific example of Early Hearing Detection and Intervention Programs is considered, the guidelines given by The Joint Committee on Infant Hearing (2019) for screening, diagnosis and intervention is an aspirational guideline that many countries have adopted. However, in reality, implementing this evidence-based guideline, for example, in a country like India has been challenging. This is because India serves a population that is predominantly rural, where births are largely at primary health care clinics that are at far distances from tertiary care centers having infrastructure for hearing screening or diagnosis. Further, a significant proportion of births still occur at home (Ou et al., 2021). Also, resources (equipment, professional, and infrastructure) are allocated to the more prevalent or lifesaving conditions. Additionally, the recommended screening and diagnostic tools such as OAE and AABR have not been affordable (one time purchase cost, plus annual servicing/maintenance multiplied by the number of birthing centers).
Therefore, low-cost behavioral measures that are sensitive tools to screen more severe hearing losses (Ramesh et al., 2012) is an alternative to be considered until such time that the country can afford to detect/identify mild hearing loss. Similarly, check list based high-risk screening and behavioral observation audiometry at remote birthing centers followed by referral to tertiary care centers was found to improve screening coverage (Rajpoot et al., 2023) in a developing country setting.
Outcomes of implementation in settings where health care services are self-financed will differ considerably from publicly-funded services (Olusanya, 2012). Therefore, it is prudent for countries to develop guidelines based on existing context, with consensus among all relevant stakeholders such that it is currently feasible to improve the situation of EHDI within that setting. The impact outcomes of such implementation has the potential to eventually guide improvements in resource allocations that are closer to the evidence-base.
Using South Africa as an example where there are several cultures, ethnicities and belief systems, research has continued to argue for cultural contextualization for the adaptation of knowledge, methods and approach in the teaching and training of audiologists (Khoza-Shangase and Mophosho, 2018, 2021). South African researchers, Pillay and Serooe (2019) highlight the prominence and use of traditional healing as a source of hearing healthcare for many South Africans of varying spiritual, religious and cultural beliefs. However, there seems to be no acknowledgment and or openness to explore the value of traditional care models for audiology within curriculum and or research (De Andrade, 2011; Pillay and Serooe, 2019). Thus, graduates produced for practice in South African audiology through the current global north influenced curriculum are often found completely dismissing the option to even ask in case history if clients consult with traditional or cultural healers (Pillay and Serooe, 2019).
Health beliefs as a whole are not often acknowledged in guidelines used for training. If the example of South Africa is used once more, another area in audiology where contextualization would be culturally responsive is with the South African guidelines on audiological management of ototoxicity (Health Professionals Council of South Africa, 2018) that are used widely in training. Particularly, within the guidelines, there is the inclusion of the term all in the ototoxicity monitoring recommendation: “All patients on ototoxic medication presenting with these risk factors must be monitored …” This here is an example of how this recommendation does not consider or allow for the autonomy of patients with health—and/or illness beliefs different to the guidelines' authors.
Context can be described as the broad circumstances and environmental characteristics or settings (Damschroder et al., 2009) in which health care services are implemented. Therefore, apart from the training, competence, and professional influences of the audiologists, the delivery of services is influenced by a number of additional contextual factors. Local infrastructure (including test environment), social fabric, financial resources, legal and socio-political climate, are some examples of these factors that have an impact (Watson et al., 2018).
Often capability, opportunity, and motivation of professionals have been attributed to lack of compliance to professional guidelines in audiology (Goulios and Patuzzi, 2008; Watson et al., 2018; Marques et al., 2022). While guidelines are driven by knowledge, “Knowledge to Action” is not spontaneous and requires one to “Adapt knowledge to local context” (Moodie et al., 2011). While exploring why audiologists do not adhere to best practice, the lack of understanding of internal conditions for the individual hearing healthcare practitioner [and their] social and physical work environment was speculated as a possible reason (Shaw, 2012).
In low and middle income countries, hearing care services are provided by various cadres of service providers including community volunteers, school teachers, special educators, audiometrists, other allied professionals, audiologists, and even otolaryngologists. These are often based on the level of capacity of individual countries to have a specialized workforce to provide hearing care services. Therefore, a vast difference exists in audiology practices based on the local context and setting prevailing in that region. To account for some of these, many local professional bodies have developed their own guidelines (Indian Speech and Hearing Association, 2017; HPCSA, 2021; SACIG, 2022). While such practices may not meet “benchmarks,” they may still cater to the ear and hearing care needs plus fill service gaps that exist in that region.
This paper would like to propose that practice context should be factored into audiology best practice engagements and guidelines. We propose a process of contextualization which according to Ernstzen et al. (2019) is based on the premise that clinical practice guidelines produced in one place, timeline and context may not be appropriate for implementation across varying contexts due to differences in the healthcare systems, socio-cultural, societal, policy and economic contexts. Therefore, contextualization requires identification of practice context to which existing practice guidelines must be tailored to (Siegfried et al., 2018). In the schematic (Figure 1) we propose some of the contextual factors that can influence audiological practices and have broadly classified them into (i) environment (related to the physical environment and end-users) and (ii) circumstances (related to other variables that directly influence service provision; Watson et al., 2018).
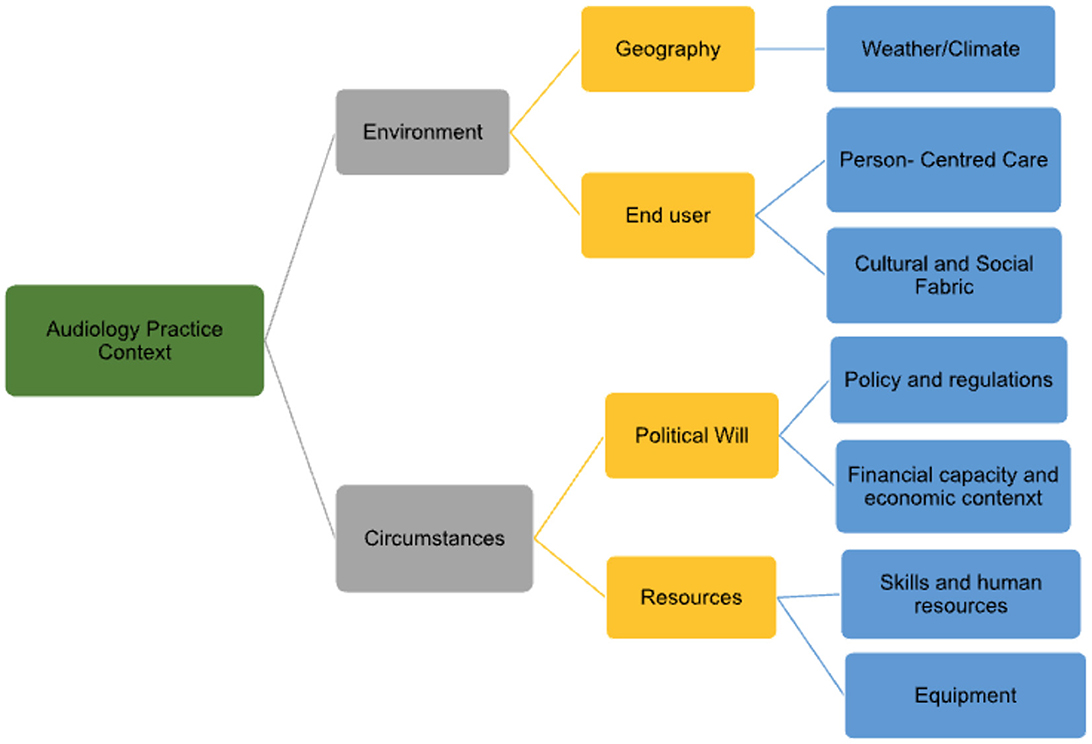
Figure 1. Contextual factors influencing audiology practices.
These are described with some case examples below:
• Environment:
° Geography:
▪ Weather/climate—influences travel access (e.g., snowy mountains of Bhutan, deserts of Afghanistan), working hours (which in turn alters service availability), allowable/feasible testing time and protocol (e.g., in the mountains of Bhutan having test sessions across multiple days is challenging and there will be non-compliance due to difficulty in returning as a result of long distances). Therefore, conclusive time efficient test batteries may have to be conducted in single sessions.
° End users:
▪ Person-centered care/Patient care practices—Is it participatory culture or top-down (medical model) or advocacy-rights based culture that prevails in the context where audiology services are provided? The dominant culture will dictate the choice of services (e.g., Deaf vs. deaf).
▪ Cultural and social fabric—stigma around disability, language (influences test tool choices), belief systems, and local practices.
• Circumstances:
° Political will:
▪ Policy and regulations—will decide what benefits are provided (free hearing aids, cochlear implants, travel concessions, or educational concessions, etc.), who will receive benefits (children and adults).
▪ Financial capacity and allocation/economic context—Resources- types of schools, type of rehabilitation.
• Equipment (e.g., otoscopy vs. tympanometry to rule out middle ear pathology).
• Human Resources (e.g., community worker vs. audiologist performing basic hearing testing).
Audiology practice and the profession as a whole has grown since the main inception era and the footprint of audiologists has expanded to reach each continent. This paper seeks to increase engagement on development of context influenced best practice definitions, evidence gathering and evaluation methods as well as a multifaceted regional approach to the implementation of practice guidelines. We believe that it is crucial to expand audiology and the practice thereof in each region based on the milieu such as those in Africa, Asia and South America. This expanded lens can begin with a relook at how the profession defines best practice and we propose that the audiology practice context be used as a multifactorial and multifaceted lens to contextualize existing best practice guidelines.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
V-GH: Conceptualization, Visualization, Writing – original draft, Writing – review & editing. VR: Conceptualization, Project administration, Visualization, Writing – original draft, Writing – review & editing. LP: Conceptualization, Visualization, Writing – original draft, Writing – review & editing. BV: Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Africa Asia South America Audiology Coalition (AASAAC): This work is a result of collaborative discussions and conceptualization from a collective of audiologists from Brazil, Tunisia, South Africa, Nigeria, India, Bhutan, Thailand, Malaysia, Sri Lanka, and Nepal. This collective is known as the Africa Asia South America Audiology Coalition.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abrahams, K., Kathard, H., Harty, M., and Pillay, M. (2019). Inequity and the professionalisation of speech-language pathology. Professions Professionalism 9:3285. doi: 10.7577/pp.3285
American Association of Audiology (n.d.). Practice Guidelines and Standards. The American Academy of Audiology. Available online at: https://www.audiology.org/practice-resources/practice-guidelines-and-standards/ (Retrieved April 27 2024)
Brosnan, C. (2015). “Quackery” in the academy? Professional knowledge, autonomy and the debate over complementary medicine degrees. Sociology 49, 1047–1064. doi: 10.1177/0038038514557912
Damschroder, L. J., Aron, D. C., Keith, R. E., Kirsh, S. R., Alexander, J. A., and Lowery, J. C. (2009). Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement. Sci. 4:50. doi: 10.1186/1748-5908-4-50
De Andrade, V. (2011). “Traditional healers and modern doctors do not understand each other because they learn different things”: South African traditional health practitioners' training with regards to hearing impairment. Int. J. Health Promot. Educ. 49, 120–127. doi: 10.1080/14635240.2011.10708218
de Andrade, V., and Ross, E. (2005). Beliefs and practices of Black South African traditional healers regarding hearing impairment. Int. J. Audiol. 44, 489–499. doi: 10.1080/14992020500188999
Ernstzen, D.V, Hillier, S.A, and Louw, Q.A. (2019). An innovative method for clinical practice guideline contextualisation for chronic musculoskeletal pain in the South African context. BMC Med. Res. Methodol. 19:134. doi: 10.1186/s12874-019-0771-3
Evetts, J. (2014). “The concept of professionalism: professional work, professional practice and learning,” in International Handbook of Research in Professional and Practice-Based Learning, eds. S. Billet, C. Harteis, and H. Gruber (Dordrecht: Springer), 29–56.
Gitter, A. H. (1990). Eine kurze Geschichte der Hörforschung. I. Antike [A short history of hearing research. I. Antiquity]. Laryngo- rhino- otologie 69, 442–445. doi: 10.1055/s-2007-998226
Goulios, H., and Patuzzi, R. B. (2008). Audiology education and practice from an international perspective. Int. J. Audiol. 47, 647–664. doi: 10.1080/14992020802203322
Hawkins, J. E. (2004). Sketches of otohistory. Part 1: otoprehistory: how it all began. Audiol. Neurotol. 9, 66–71. doi: 10.1159/000075997
Haynes, R. B., Devereaux, P. J., and Guyatt, G. H. (2002). Physicians' and patients' choices in evidence based practice. Br. Med. J. 324:1350. doi: 10.1136/bmj.324.7350.1350
Health Professionals Council of South Africa (2018). Guidelines for the Audiological Management of Patients on Treatment That Includes Ototoxic Medications. Available online at: https://www.hpcsa.co.za/Uploads/SLH/Guidelines%20for%20Audiological%20Management%20of%20Patients%20on%20Treatment%20that%20includes%20Ototoxic%20Medications.pdf
HPCSA (2021). Guidelines for Good Practice in the Healthcare Professions. Available online at: https://cdn.ymaws.com/saslha.co.za/resource/collection/3DBDE116-0E29-401E-BC6F-488950C17A0D/Booklet_1_Guidelines_for_Good_Practice_Dec_2021.pdf (Retrieved March 14, 2024).
Indian Speech and Hearing Association (2017). Protocol for Hearing Aid Trial and Assessment of Benefit in Adults. Available online at: https://www.ishaindia.org.in/pdf/Protocol-for-Hearing-Aid-Trial-and-Assessment-of-Benefit-inAdults.pdf (Retrieved February 22, 2024).
Jerger, J. (2018). Lessons from the Past: Two Influential Articles in the Early History of Audiology. Available online at: https://hearingreview.com/hearing-loss/hearing-loss-prevention/industrial-military/lessons-past-two-influential-articles-early-history-audiology (accessed January 10, 2023).
Jerger, J. (2019). Ten highlights from the history of audiology. Hear. Rev. 26, 10–14. Available online at: https://hearingreview.com/practice-building/practice-management/continuing-education/ten-highlights-history-audiology
Khoza-Shangase, K., and Mophosho, M. (2018). Language and culture in speech-language and hearing professions in South Africa: the dangers of a single story. South Afri. J. Commun. Disord. 65:7. doi: 10.4102/sajcd.v65i1.594
Khoza-Shangase, K., and Mophosho, M. (2021). Language and culture in speech-language and hearing professions in South Africa: re-imagining practice. South Afri. J. Commun. Disord. 68:a793. doi: 10.4102/sajcd.v68i1.793
Marques T. Silvestre M. Rosa B. S. Miguéis A. (2022). Audiologist's perspective in auditory rehabilitation: implications for ethical conduct and decision-making in Portugal. Audiol. Res. 12, 171–181. doi: 10.3390/audiolres12020020
Merriam-Webster (n.d.). Standard. Merriam-Webster.com dictionary. Available online at: https://www.merriam-webster.com/dictionary/standard (accessed February 22 2023).
Mignolo, W. D. (2009). Epistemic disobedience, independent thought and de-colonial freedom. Theory Cult. Soc. 26, 1–23. doi: 10.1177/0263276409349275
Montigny, G. A. J. (1995). “The power of being professional,” in Knowledge, Experience, and Ruling Relations: Studies in the Social Organisation of Knowledge, eds. M. Campbell and A. Manicom (Toronto, ON: University of Toronto Press), 211–220.
Moodie, S. T., Kothari, A., Bagatto, M. P., Seewald, R., Miller, L. T., and Scollie, S. D. (2011). Knowledge translation in audiology: promoting the clinical application of best evidence. Trends Amplificat. 15, 5–22. doi: 10.1177/1084713811420740
Mukherji, P., and Albon, D. (2014). Research Methods in Early Childhood: An Introductory Guide, 2nd Edn. Newcastle upon Tyne: Sage.
Narayansamy, M., Ramkumar, V., and Nagarajan, R. (2014). Knowledge and beliefs about ear and hearing health among mothers of young children in a rural community in South India. Disabil. CBR Incl. Dev. 25, 119–135. doi: 10.5463/dcid.v25i4.328
Ng, S. (2012). Reflection and reflective practice: creating knowledge through experience. Semin. Hear. 33, 117–134. doi: 10.1055/s-0032-1311673
Olusanya, B. O. (2012). Neonatal hearing screening and intervention in resource-limited settings: an overview. Archiv. Dis. Childh. 97, 654–659. doi: 10.1136/archdischild-2012-301786
Ou, C. Y., Yasmin, M., Ussatayeva, G., Lee, M. S., and Dalal, K. (2021). Maternal delivery at home: issues in India. Adv. Ther. 38, 386–398. doi: 10.1007/s12325-020-01551-3
Oxford English Dictionary (n.d.). Entry. Available online at: https://www.oed.com/view/Entry/18180?redirectedFrom=best+practice#eid22233502 (Retrieved March 18 2024).
Pillay, D., and Serooe, T. (2019). Shifting and transforming the practice of audiology: the inclusion of traditional healing. South Afri. J. Commun. Disord. 66, 1–9. doi: 10.4102/sajcd.v66i1.635
Pillay, M., and Kathard, H. (2018). Renewing our cultural borderlands. Top. Lang. Disord. 38, 143–160. doi: 10.1097/TLD.0000000000000151
Rajpoot, A., Mishra, A., Verma, V., and Raza, I. F. (2023). Modified universal new-born hearing screening: practical approach for developing world (Georgean experience). Int. J. Pediatr. Otorhinolaryngol. 173:111717. doi: 10.1016/j.ijporl.2023.111717
Ramesh, A., Jagdish, C., Nagapoorinima, M., Rao, P. S., Ramakrishnan, A. G., Thomas, G. C., et al. (2012). Low cost calibrated mechanical noisemaker for hearing screening of neonates in resource constrained settings. Ind. J. Med. Res. 135, 170–176. Available online at: https://api.semanticscholar.org/CorpusID:8636374
SACIG (2022). Quality Standards Cochlear Implant Services for Adults and Children in South Africa. Available online at: http://www.sacig.org.za/guidelines/ (Retrieved February 10, 2024).
Scheppers, E., van Dongen, E., Dekker, J., Geertzen, J., and Dekker, J. (2006). Potential barriers to the use of health services among ethnic minorities: a review. Fam. Pract. 23, 325–348. doi: 10.1093/fampra/cmi113
Shaw, G. (2012). Preventing medical errors, how to proceed with caution. Hear. J. 67, 14–16. doi: 10.1097/01.HJ.0000418983.13114.f3
Siegfried, N., Draper, B., Draper, G., Porter, M., Bonaconsa, C., Hunter, J., et al. (2018). A contextualisation approach to health promotion guideline development in South Africa. South Afri. Med. J. 108, 1036–1041. doi: 10.7196/SAMJ.2018.v108i12.13129
The Joint Committee on Infant Hearing (2019). Year 2019 position statement: principles and and guidelines for early hearing detection and intervention programs. J. Early Hear. Detect. Intervent. 4, 1–44. doi: 10.15142/fptk-b748
Tuomi, S. K. (1994). Speech-language pathology in South Africa: a profession in Transition. Am. J. Speech-Lang. Pathol. 3, 5–8. doi: 10.1044/1058-0360.0302.05
United Nations (2015). State of the World's Indigenous Peoples, 2nd vol. Indigenous Peoples' Access to Health Services. New York, NY: United NationsDepartment of Economic and Social Affairs. Available online at: http://www.un.org/esa/socdev/unpfii/documents/2015/sowip2volume-ac.pdf (accessed December 9, 2022).
University of North Carolina (2021). History of the Professions: A Brief History of Audiology. Available online at: https://hsl.lib.unc.edu/speechandhearing/professionshistory (accessed January 6, 2023).
Watson, D. P., Adams, E. L., Shue, S., Coates, H., McGuire, A., Chesher, J., et al. (2018). Defining the external implementation context: an integrative systematic literature review. BMC Health Serv. Res. 18:209. doi: 10.1186/s12913-018-3046-5
Keywords: best-practice, contextualization, evidence, guidelines, global-audiology, multidimensional approach
Citation: Hlayisi V-G, Ramkumar V, Petersen L and Vangerwua B (2024) Best practice in audiology: context matters. Front. Audiol. Otol. 2:1419219. doi: 10.3389/fauot.2024.1419219
Received: 17 April 2024; Accepted: 14 June 2024;
Published: 09 July 2024.
Edited by:
Claus-Peter Richter, Northwestern University, United StatesReviewed by:
Kristi Oeding, Minnesota State University, Mankato, United StatesCopyright © 2024 Hlayisi, Ramkumar, Petersen and Vangerwua. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vera-Genevey Hlayisi, dmVyYS5obGF5aXNpQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.