 Chané Fourie1
Chané Fourie1 Faheema Mahomed-Asmail1,2
Faheema Mahomed-Asmail1,2 Ilze Oosthuizen1,2
Ilze Oosthuizen1,2 Vinaya Manchaiah1,2,3,4,5
Vinaya Manchaiah1,2,3,4,5 Charlotte Vercammen6,7,8
Charlotte Vercammen6,7,8 De Wet Swanepoel1,2,3*
De Wet Swanepoel1,2,3*- 1Department of Speech-Language Pathology and Audiology, University of Pretoria, Pretoria, South Africa
- 2Virtual Hearing Lab, Collaborative Initiative Between University of Colorado School of Medicine, Aurora, CO, United States
- 3Department of Otolaryngology-Head and Neck Surgery, University of Colorado School of Medicine, Aurora, CO, United States
- 4UCHealth Hearing and Balance, University of Colorado Hospital, Aurora, CO, United States
- 5Department of Speech and Hearing, School of Allied Health Sciences, Manipal Academy of Higher Education, Manipal, India
- 6Sonova AG, Research & Development, Stäfa, Switzerland
- 7Manchester Centre for Audiology and Deafness, School of Health Sciences, Faculty of Biology, Medicine and Health, University of Manchester, Manchester, United Kingdom
- 8Department of Neurosciences, Research Group Experimental Oto-Rhino-Laryngology, KU Leuven-University of Leuven, Leuven, Belgium
Introduction: Understanding hearing aid wearer experiences in real-world settings is important to provide responsive and individualized hearing care. This study aimed to describe real-life benefits of hearing aids (HAs), as reported by hearing aid wearers through Ecological Momentary Assessment (EMA) in various listening environments.
Method: Qualitative content analysis of 1,209 open-text responses, provided through self-initiated EMAs, was conducted. The de-identified data was collected retrospectively via a smartphone app compatible with these HAs. Only text responses reflecting positive hearing aid experiences were analyzed. The 1,209 open-text responses were categorized into 18 pre-determined sub-categories, further organized into five overarching categories: Conversational, Leisure, Device-related aspects, Lifestyle, and Other factors.
Results: Across these categories, 48 self-generated meaning units highlighted the multifaceted benefits of HAs. In particular, participants reported significant improvements in conversational settings, specifically during phone conversations and meetings, attributed to improved sound quality and speech understanding when wearing their HAs. During leisure activities, particularly TV watching and music listening, clearer sound and ease of Bluetooth streaming contributed to experienced benefits. Lifestyle improvements were reported in occupational and social settings, as hearing aid wearers stated enhanced communication and sound awareness. Device-related factors contributing to positive wearer experiences included extended battery life and the convenience of rechargeable batteries. The most prominent sub-category, other factors, underscored overall satisfaction, comfort with the device, and improved auditory experiences across various environments.
Conclusion: This study reveals the diverse benefits of HAs in improving communication, listening experiences, and quality of life across various settings, as captured through EMA. By emphasizing features like direct streaming and rechargeability, the findings highlight the importance of personalized hearing care and the potential of real-time listener feedback to inform device enhancements and support strategies, advancing more tailored and effective hearing rehabilitation.
1 Introduction
Hearing rehabilitation aims to enhance hearing functioning, participation, and quality of life for individuals with hearing loss (Boothroyd, 2007). Providing amplification through hearing aids (HAs) is a primary component of hearing care, as HAs amplify sound and improve the clarity of sounds, with a specific emphasis on speech and communication (Ferguson et al., 2017). However, the effectiveness of HAs depends on wearers being familiar with the correct way to handle the devices, understanding the expected benefits and satisfaction, and the clinicians' ability to create personalized and achievable rehabilitation plans with the HAs (Heselton et al., 2022; Humes, 2003; Wong et al., 2003). A recent study that included former HA wearers revealed that almost half of them attributed non-use to device-related issues such as wearing comfort, not liking to wear the HAs, or limited perceived benefit (Franks and Timmer, 2023; Mothemela et al., 2023). It is therefore important to explore the factors contributing to HA wearers' experiences, in order to enhance understanding of HA benefit and satisfaction from the wearer's perspective, provide person-centered care, and validate the effectiveness of treatment with HAs.
Satisfaction is commonly measured through self-reported measures, often referred to as patient-reported outcome measures (PROMs) (Timmer et al., 2018; Oosthuizen et al., 2022). Self-reported questionnaires can, for instance, gather information about the individual's perspective on how well rehabilitation goals have been achieved in real-world settings (von Gablenz et al., 2021). Some limitations of PROMs include that they necessitate client input based on memory and experiences with specific listening conditions. As memory affects recall, this can introduce recall bias. Also, listening situations posed in PROMs might not apply to all HA wearers (Timmer et al., 2018). Ecological momentary assessment (EMA) has been proposed to address some limitations of PROMs, by asking participants to repeatedly report on their experiences during or close in time to an event of interest (Bolger et al., 2003; Shiffman et al., 2008). EMA, also known as ambulatory assessment or experience sampling (Trull and Ebner-Priemer, 2014), is a real-time data collection method, applied in participants' real-world environments. EMA allows the capturing of individuals' daily experiences and changes in their experiences over time (Holube et al., 2020).
In practical terms, EMA research today commonly employs personal digital devices, utilizing auditory or vibratory alerts to prompt participants to respond to a series of questions throughout the day. This prompted EMA approach involves participants receiving messages on their smartphone-based app at regular intervals to complete surveys (Burke et al., 2017). Patients may not always comply with the EMA data collections, as the highly dense data collection can burden participants. This limitation arises when patients do not provide feedback when prompted, thereby restricting the coverage of the analysis. This could lead to inadequate results, as they might fail to accurately portray the diverse range of experiences people have (Holube et al., 2020; Schinkel-Bielefeld et al., 2020). An alternative approach to prompted EMA is self-initiated EMA. During self-initiated EMA, the individuals decide when something of interest has happened, and subsequently fill in a survey on their initiative, without any prompting (Schinkel-Bielefeld et al., 2020).
In addition to being used in research, EMA is also proposed as a valuable clinical tool, enabling patients to monitor daily challenges systematically and contributing to personalized hearing healthcare (Schinkel-Bielefeld et al., 2020). Data collected through EMA could guide healthcare professionals in tailoring HA settings to meet individual patient needs during fitting, fine-tuning, and acclimation (Holube et al., 2020). Combined with a person-centered care approach, such data can enhance understanding, leading to improved health outcomes. These rich data collection methods could also facilitate improved communication between patients and healthcare professionals, particularly concerning patient-specific needs and residual hearing difficulties experience in real life situations (Wu et al., 2015; Brice and Almond, 2022).
Most studies on hearing-related EMA have predominantly utilized quantitative methodologies to capture experiences with HAs and their features (Galvez et al., 2012; Hasan et al., 2014; Timmer et al., 2017; Wu et al., 2018). However, there remains a notable scarcity in the application of EMA for gathering qualitative data, such as personal experiences with HAs in real-life scenarios. Notably, Galvez et al. (2012) undertook a qualitative analysis of prompted EMA data to explore hearing difficulties among HA wearers, providing valuable insights for evaluating HA parameters and enhancing patient care. Similarly, Vercammen et al. (2023) identified key themes in feedback from HA wearers using automated text analysis of self-initiated EMA data, revealing a predominance of positive experiences related to communication and sound quality, in contrast to challenges in HA management.
While recent technological advancements, such as real-time speech-to-text transcription and advanced natural language processing (NLP) techniques, provide unprecedented opportunities for capturing and analyzing qualitative wearer feedback (Manchaiah et al., 2021a,b), their full potential has yet to be explored. To complement insights from such computational methods, this study employs a manual qualitative analysis to delve into a portion of the dataset previously investigated by Vercammen et al. (2023) using NLP techniques. This methodological decision is intentional, addressing the constraints of computational methods, which may lack the depth and nuanced understanding inherent in direct human analysis (Jiang et al., 2021; Baden et al., 2022). Employing this approach, our study seeks to gain a more thorough understanding of the qualitative EMA data, with a particular emphasis on identifying psychosocial elements of satisfaction with HA usage (Oosthuizen et al., 2022; Knoetze et al., 2023). To this end, we focused on a subset of the original dataset, focusing on positive HA experiences only. Thereby providing a unique perspective, as opposed to the commonly reported challenges with HAs.
2 Materials and methods
2.1 Study design
The study considered a retrospective subset of the data presented in Vercammen et al. (2023) i.e., 1,209 positive open-text statements provided by real-world HA wearers as part of their hearing care. Due to size of the dataset, this manuscript focused on positive responses only, with negative responses being analyzed as part of an upcoming manuscript. Prior to participation, participants were informed of de-identified data analysis for clinical and research purposes per the mobile application's data privacy notice. In addition, no personal identifying information was logged to ensure participant privacy. Institutional Review Board clearance was granted (HUM023/0922) prior to data analysis.
2.2 Study participants, material, and apparatus
The de-identified data was collected through a smartphone mobile application compatible with commercially available HAs, fitted to real-world HA wearers from English-speaking countries, i.e., Australia, Canada, England, Ireland, New Zealand, and the United States. Clinicians activated the EMA application feature within the fitting software during consultations. Clinicians could activate the feature to use as a real-time feedback system whenever they deemed it advantageous for the HA wearer and their hearing care (Vercammen et al., 2023). Participants initiated the mobile application on their own when they had a listening experience that they wanted to report (i.e., self-initiated EMA) and navigated through the windows (see Supplementary material 1) (a) indicate the listening experience as positive or negative; (b) select the listening situation from the list, closest to the experienced situation (i.e., activities, battery or charging, entertainment, hearing children, in meeting, in restaurant, in vehicle, listening music, other, phone conversations, playing games, quiet conversations, shopping, social activities, social event, streaming media, worship, and watching TV); (c) provide description of the listening experience (open text field).
2.3 Data extraction and data cleaning
Between May 2018 and June 2021, an initial sample of 30,127 self-initiated EMAs on real-world HA experiences were collected worldwide and extracted from cloud-based data logging of the smartphone mobile application. Text statements shorter than 20 characters were removed for content quality, and a manual data cleaning process was conducted to correct spelling mistakes, remove nonsense text, and exclude non-English entries. Following data extraction and cleaning, a dataset of 5,331 negative and 3,462 positive EMAs (a total of 8,793 responses) was extracted. Only the 3,462 positive EMA's were considered for further analysis in this study (see Figure 1). During data familiarization, it was found that some of the comments under each pre-determined sub-category (which were derived from the listening situation self-selected by the user—see Supplementary material 1, panel B) were unrelated to the specific situation the participant had chosen (i.e., they were more applicable to another pre-determined sub-category). In addition, some of the comments were negative despite the participant's choice of a positive experience. After a discussion with the research team (IO, FMA, VM, CV, and DWS) a consensus was reached, and 799 open text statements were reclassified (i.e., moved to a more applicable sub-category), and 2,150 comments were moved from positive experiences to negative experiences. Furthermore, 103 comments could not be coded as they were irrelevant to any pre-determined sub-category. A final sample of 1,209 positive self-initiated EMAs was considered for further analysis (see Figure 1).
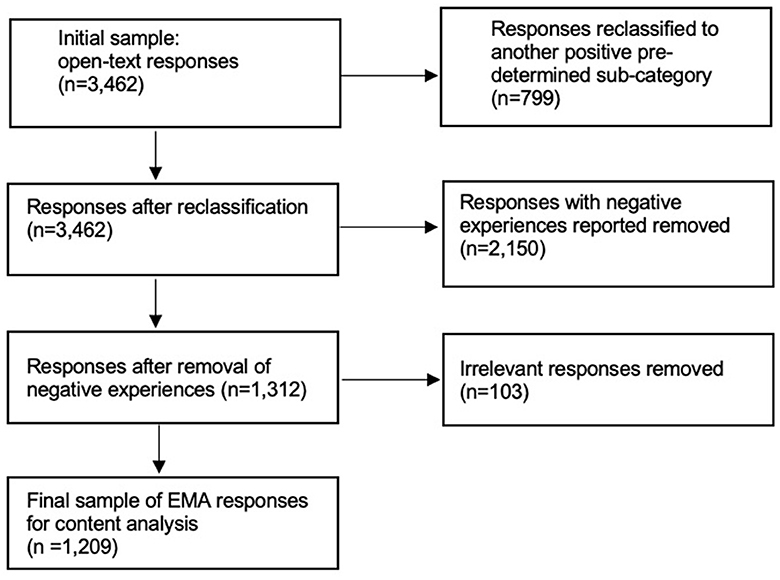
Figure 1. Illustration of the manual data cleaning process, leading to the final cample of 1,209 EMA responses that were considered for manual qualitative analysis.
2.4 Data analysis
The final 1,209 positive self-initiated EMAs were analyzed using qualitative content analysis (Graneheim and Lundman, 2004; Knudsen et al., 2012). This approach was deemed suitable due to the diverse range of responses obtained from the open-ended question, which varied significantly in depth and detail. Qualitative content analysis involves an iterative process of revisiting and refining coding and categorization, facilitating a nuanced and comprehensive understanding of the data. Initially, responses within each of the 18 pre-determined subcategories, derived from the users' selected listening situations in the app (e.g., phone conversations, watching TV etc.), were reviewed, coded and condensed into meaning units, capturing the essence of each participant's experience (Graneheim and Lundman, 2004). These condensed meaning units were further examined and the sub-categories were grouped into broader categories, resulting in five main categories: Conversational, leisure, device-related, lifestyle, and other factors. To ensure clarity, we have detailed the hierarchical classification process used in our data analysis. Seemingly similar responses were placed in distinct categories based on their contextual relevance and the nuances of participant comments. This approach aimed to capture the multifaceted nature of hearing aid experiences. However, we acknowledge the potential overlap of similar responses in different categories and have included this consideration in Section 4.1.
To ensure consistency and reliability, an experienced qualitative researcher cross-checked 50% of the coding, and any discrepancies were resolved through team discussions. This iterative review process allowed for refining the categories, ensuring they accurately represented the data. The final categorization facilitated the identification of 48 self-generated meaning units, providing a comprehensive understanding of the diverse benefits of hearing aids as experienced by participants in their daily lives. This detailed categorization process ensured that the diverse and nuanced experiences of hearing aid users were systematically captured and analyzed, yielding robust insights into the real-world benefits of HAs.
3 Results
The 18 pre-determined sub-categories were categorized into five categories as part of the manual qualitative content analysis: (1) Conversational, representing diverse settings where participants engaged in conversations; (2) Leisure settings, representing various recreational pursuits for enjoyment and relaxation; (3) Device-related aspects, encompassing different facets of HA functionality; (4) Lifestyle factors, covering settings that contribute to an individual's way of life and daily routines; and (5) Other factors, including settings not falling within the aforementioned domains. From these categories, a total of 48 meaning units were self-generated (see Tables 1–5).
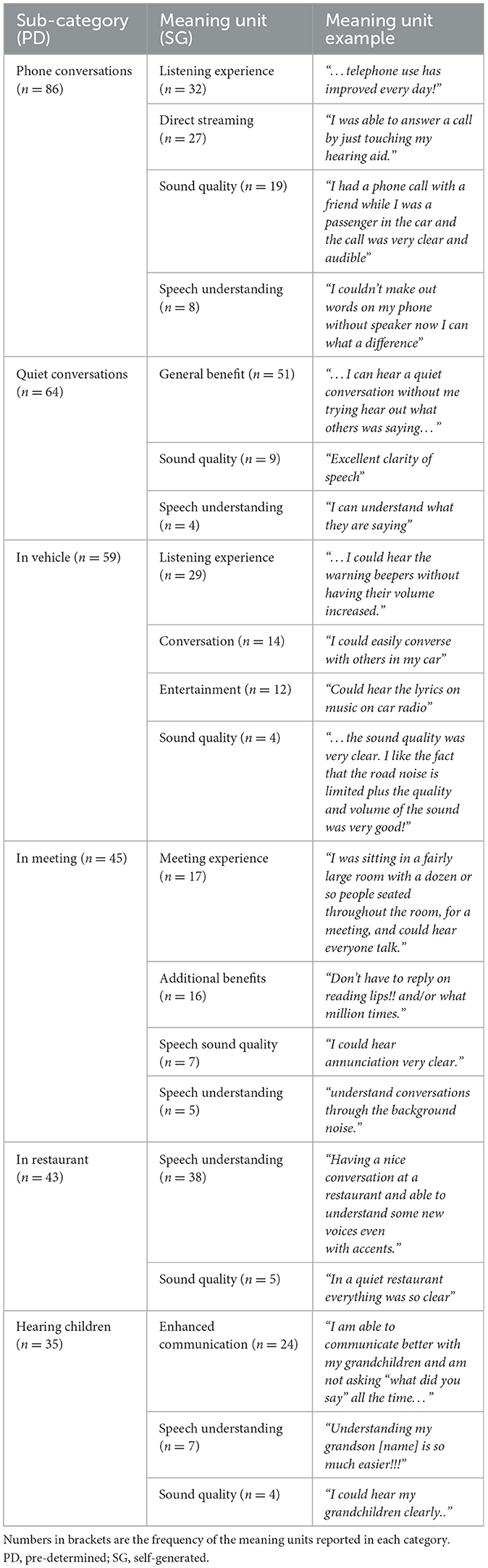
Table 1. Positive experiences in conversational settings (n = 332 meaning units).
Category 1: Conversational setting benefits of HAs
Six pre-determined sub-categories i.e., phone conversations (n = 86), quiet conversations (n = 64), in vehicle (n = 59), in meeting (n = 45), in restaurant (n = 43), and hearing children (n = 35) were combined into the overarching category “conversational settings” (see Figure 2). Twenty self-generated meaning units were identified (see Table 1 and Supplementary material 2 for elaboration on meaning units). Within phone conversations, the largest identified meaning unit of listening experience (n = 32) focused on aspects such as volume and general satisfaction. The direct streaming capability facilitated seamless call handling, introducing a private and hands-free dimension to phone conversations. In quieter settings, participants enjoyed their ability to engage in one-on-one conversations, emphasizing the significance of both sound quality and improved speech understanding. In vehicle settings, improved sound quality, ease of conversing with passengers, and greater enjoyment of music and audio contributed to enhanced listening experiences. Participants also experienced increased participation and improved speech understanding during group conversations such as meetings and in noisy restaurant environments. Furthermore, participants reported improved communication with children, highlighting enhanced speech understanding and sound quality.
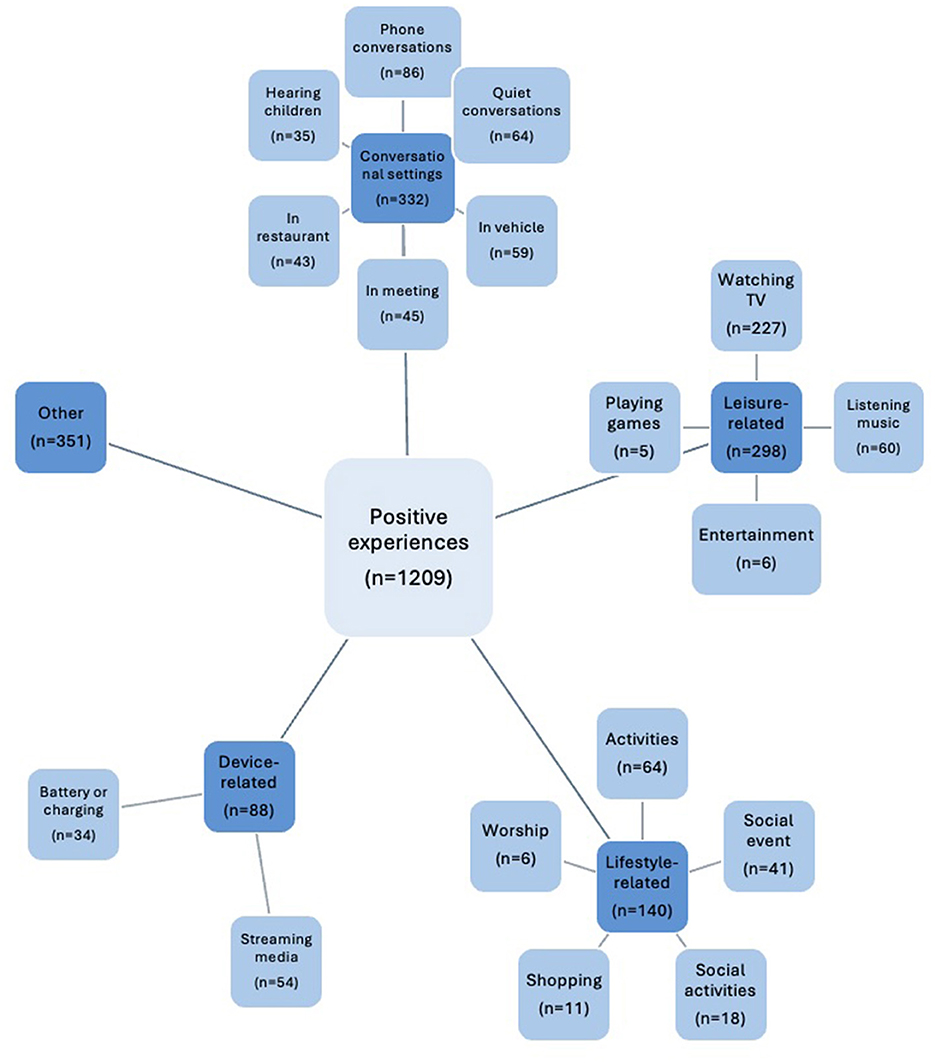
Figure 2. Overview of 18 pre-determined sub-categories that were derived from the listening situation self-selected by the users in the app (light blue boxes), organized into five overarching categories (dark blue boxes) as part of the qualitative content analysis.
Category 2: Leisure activity benefits of HAs
Four pre-determined sub-categories i.e., watching TV (n = 227), listening music (n = 60), entertainment (n = 6), and playing games (n = 5) were combined into the overarching category “leisure settings” (see Figure 2). Nine self-generated meaning units were identified (see Table 2 and Supplementary material 3 for elaboration on meaning units). Watching TV was the most frequently selected predetermined subcategory with listening experience identified as the largest meaning unit (n = 143) followed by sound quality (n = 46), speech understanding (n = 20), and direct screening (n = 18). These indicate the primary perceived benefits for the HA wearers in this specific leisure activity. Some participants also reported enhanced music listening experiences, noting improved recognition of lyrics, and vibrant sound quality. Greater enjoyment of other media, such as improved listening to radio, gaming, and podcast streaming, was also mentioned.
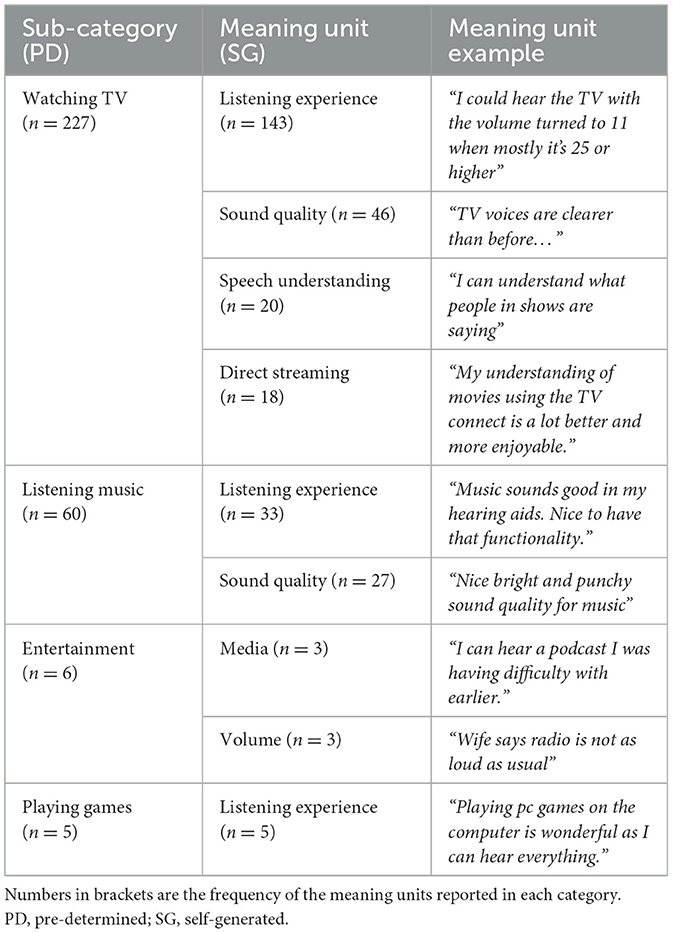
Table 2. Leisure related experiences (n = 298 meaning units).
Category 3: Lifestyle-related benefits of HAs
Five pre-determined sub-categories i.e., activities (n = 64), social event (n = 41), social activities (n = 18), shopping (n = 11), and worship (n = 6) were combined into the overarching category “lifestyle” (see Figure 2). Ten self-generated meaning units were identified (see Table 3 and Supplementary material 4 for elaboration on meaning units). Within Activities, the largest identified meaning unit was occupational settings (n = 26), in which HAs facilitated effective communication, even with face masks on, and heightened awareness of work-related sounds. HAs were valuable in various situations, including recreation, education, travel, social events, shopping, and worship. Participants reported clearer speech, improved hearing, and enhanced satisfaction across these diverse settings.
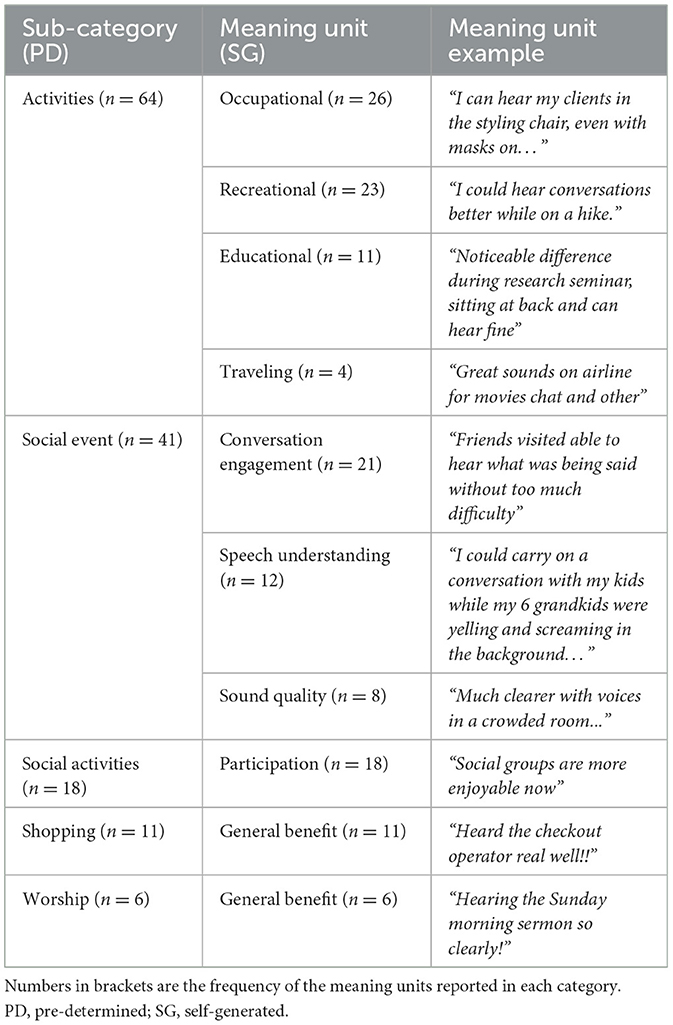
Table 3. Lifestyle related experiences (n = 140 meaning units).
Category 4: Device-related benefits of HAs
Two pre-determined sub-categories streaming media (n = 54) and battery or charging (n = 34) were combined into the overarching category “device-related benefits” (see Figure 2). Five self-generated meaning units, namely listening experience, sound quality, duration, rechargeability, and battery replacement (see Table 4 and Supplementary material 5 for elaboration on meaning units). Battery and charging experiences were characterized by descriptions of extended battery life with some participants maintaining Bluetooth connectivity throughout the day. Rechargeable HAs offered convenience and eliminated the need for disposable batteries. Participants using disposable batteries reported no hindrance, and the process of replacing batteries was deemed straightforward.

Table 4. Device related experiences (n = 88 meaning units).
Category 5: Other benefits of HAs
This pre-determined sub-category was the most frequently selected (n = 351) (see Figure 2). Four categories were self-generated by the researcher from the responses, encompassing general advantages, device-related aspects, environmental sound considerations, and enhanced speech understanding (see Table 5 and Supplementary material 6 for elaboration on meaning units). Participants reported noticeable improvements in their overall hearing abilities, leading to reduced instances of asking for repetitions and enhancing daily interactions. The comfort and inconspicuous nature of the devices were particularly noteworthy. A richer auditory experience emerged as wearers appreciated sounds not heard as well-before using HAs, such as the melodic songs of springtime birds to the sizzling of bacon.
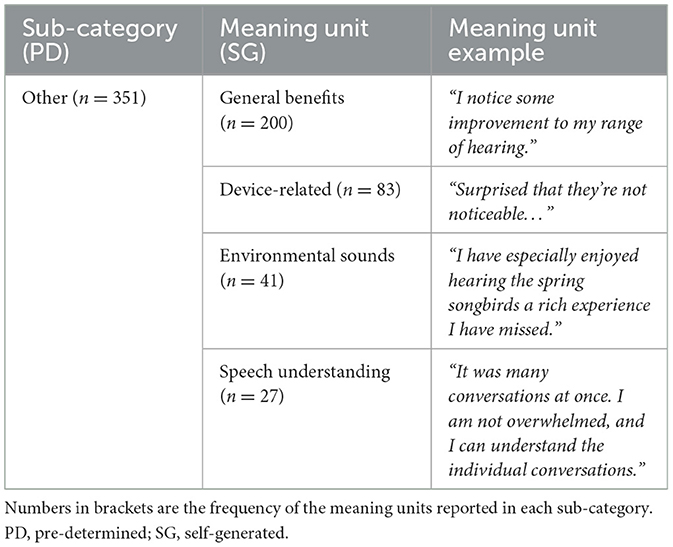
Table 5. Positive experiences for the pre-determined sub-category, Other (n = 351 meaning units).
4 Discussion
This study employed a qualitative content analysis to explore positive real-world HA use experiences of a large sample of HA wearers, who provided self-initiated EMAs through a smartphone application. The pre-determined sub-categories that resulted from the users in-app responses were grouped into categories, as part of the manual qualitative content analysis, and consisted of (1) conversational settings, (2) leisure-related, (3) lifestyle-related, and (4) device-related aspects, and (5) other listening situations (see Supplementary materials 2–6 for more detailed examples of the sub-categories and meaning units).
The cornerstone of hearing rehabilitation is using HAs to improve access to sounds and speech, thereby enhancing communication—a fundamental aspect of daily life (Ferguson et al., 2017). This study particularly highlighted the significant benefits in conversational settings, with a notable emphasis on the advantages of smartphone-connected HAs in facilitating effective telephone communication. The rise in smartphone ownership among adults in the United States and the United Kingdom since 2015 has paralleled an increase in research into smartphone-connected HAs, underscoring improvements in phone conversation quality, speech intelligibility, and reduced listening effort thanks to direct streaming capabilities (Maidment et al., 2019; Gomez et al., 2022; Pew Research Center, 2022). Moreover, the capacity for wearers to self-manage their HAs via a smartphone app has not only contributed to enhanced wearer satisfaction and integration into daily routines but has also empowered wearers through improved autonomy and ownership over their hearing experience (Chasin, 2017). Direct streaming, particularly for media and communication via videotelephony platforms, has been identified as a pivotal feature, aligning with the trend toward greater technological integration within HA design. This trend underscores the importance of connectivity in augmenting the wearers experience, fostering enhanced engagement with modern communication platforms (Chasin, 2017), and thereby enriching both listening experiences and social connections. Enhanced speech understanding was consistently reported, particularly in intimate settings such as conversations with spouses, further demonstrating the value of real-time EMA in providing detailed insights into everyday listening environments outside typical scenarios. Across various settings—from quiet conversations to dynamic social events—improvements in sound quality have been central to the wearer's enhanced ability to engage in meaningful interactions (Cox et al., 2014), reinforcing the critical role of sound quality in effective communication (Kaplan-Neeman et al., 2012).
In occupational settings, HAs significantly enhanced communication and sound awareness, aligning with prior research emphasizing the critical role of hearing in professional environments and the heavy reliance of wearers on their devices in such settings (Granberg and Gustafsson, 2021; Timmer et al., 2023). This study extends these insights by demonstrating positive experiences even in traditionally challenging situations such as group meetings and noisy environments (Picou, 2020; Oosthuizen et al., 2022), where HAs facilitated effective communication and sound source localization in the workplace. These findings, consistent with earlier studies, underscore the efficacy of HAs in improving occupational performance and highlight the unique value of self-initiated EMA data in capturing real-life, wearer-specific experiences, thus advocating for improved person-centered care. The positive feedback from self-initiated EMAs not only highlights the functional benefits of hearing technology in challenging situations but also underscores its impact on social engagements and interactions with close companions. This enhancement of communication and social involvement echoes previous findings on the significance of audiological interventions for improving the quality of life among individuals with hearing impairments (Holman et al., 2021).
It is widely recognized that, in addition to speech clarity, effective communication, and sound quality (Picou, 2020; Oosthuizen et al., 2022), HA wearers value device usage during leisure activities such as watching television (Strelcyk and Singh, 2018), enjoying music, and gaming (Greasley et al., 2020). The same was found in this study's analysis of leisure-related experiences, where watching TV and listening to music were the two most self-selected leisure-related sub-categories. Specifically, the enhanced appreciation of listening to and performing music when using HAs reported in our study, supported the survey results by Greasley et al. (2020). Participants also reported improved speech clarity during several recreational activities, contributing to enhanced participation and enjoyment e.g., while playing netball, hiking, and taking guitar lessons. Improved listening experiences while playing computer games were also mentioned.
In contrast to general situations included in typical self-report questionnaires (Timmer et al., 2018), the findings of this study offer deeper insights into the nuanced benefits and satisfaction derived from hearing aid use in specific lifestyle-related activities, such as airline travel—a context scarcely documented in existing literature. The unique capacity of EMA to capture real-time feedback across diverse life situations not only enriches our understanding of hearing aid utility but also provides a rich dataset for informing device design and clinician support strategies. This granular insight, especially from unique contexts like airline travel, can serve as valuable data, guiding the development of HAs optimized for both common and complex environments. Moreover, the documented psychosocial benefits, including enhanced engagement in social settings and increased self-assurance in communication, underscore the comprehensive impact of HAs on wearers' wellbeing (Holman et al., 2019, 2021; Vercammen et al., 2021; Gomez et al., 2022; Oosthuizen et al., 2022). These findings highlight the transformative potential of hearing rehabilitation, affirming its role in improving not just hearing but the overall quality of life. Thus, by leveraging EMA data, clinicians are empowered to make nuanced adjustments that address the full spectrum of wearers' needs, fostering improved hearing care that is as dynamic as the lives of the individuals it aims to support.
HA wearers also attributed positive experiences to the battery life and convenience of rechargeable HAs in terms of device-related experiences. Similarly, participants in a previous study reported that rechargeable technology is reliable and offers consistent performance (Taneja, 2020). Rechargeable HAs, noted for their reliability and consistent performance (Taneja, 2020), offer an eco-friendly alternative to disposables, simplifying daily routines and reducing costs (Sun, 2019). Despite the ease of recharging, the straightforward replacement of disposable batteries was also appreciated since it can avoid downtime due to batteries needing to be recharged. This emphasizes the importance of person-centered care that supports wearers to make informed choices based on differentiated advantages related to rechargeable and replaceable battery devices and considers proficiency in HA management skills (Campos et al., 2014).
Participants reported a range of benefits from using HAs, including enhanced hearing optimization, the ability to adjust volume for improved hearing range, and fewer needs to ask for repetitions, classified under the “Other” sub-category. Wearers reported wearing HAs comfortably throughout various daily activities, even during sleep, and valued the discreetness of their devices. This inconspicuousness plays a crucial role in diminishing the stigma often associated with HAs, fostering a more positive wearer attitude and enhancing overall device satisfaction (Maidment et al., 2019). Additionally, the enriched perception of environmental sounds—ranging from the natural ambiance of birds and waves to the everyday sounds of home appliances—further underscores the comprehensive benefits of HAs. These improvements contribute to a more engaging and emotionally positive auditory experience, underlining the significant role HAs play in facilitating wearers' active participation in life's diverse scenarios and mitigating communication challenges.
4.1 Limitations
To our knowledge, this study is the first to perform a manual qualitative content analysis on self-initiated EMA data. However, several limitations should be acknowledged. Primarily, the data was collected as part of clinical practice and intended to support HA wearers and clinicians, and thus not initially collected for research (Friedman et al., 2015). This secondary use of the data, while insightful, introduces challenges related to data quality and generalizability, as also acknowledged in studies by Verheij et al. (2018) and Dillard et al. (2020).
The exclusive use of a specific brand of smartphone-connected HAs, including the functionality that had to be activated by the clinician, limited participation, potentially introducing a selection bias toward a more technologically adept and motivated subgroup. Also, we included responses from individuals who provided feedback in English only. The absence of detailed demographic and audiological profiles of participants further restricts the findings' applicability across a broader HA wearers' population.
Additionally, the use of the mobile application's pre-determined sub-categories (i.e., pre-determined listening situations presented in-app for the user to respond to and select) to guide the categorization and grouping of responses may have constrained the coding process. While this classification ensured consistency, it might have limited the exploration of emergent themes not predefined in the app. We acknowledge the potential overlap of similar responses in different categories as a methodological limitation, as the predefined sub-categories imposed a structure not necessarily shared by all participants. Furthermore, the reliance on self-initiated EMAs introduces potential biases related to participant self-selection and memory recall, as users may selectively report experiences they perceive as significant. The voluntary nature of feedback and the potential for retrospective reporting introduces risks regarding compliamce and recall bias, respectively (Shiffman et al., 2008). In addition, this study focuses exclusively on positive self-initiated EMA responses, presenting a partial view of the overall hearing aid experience. The exclusion of negative responses means that while the study highlights significant benefits, it does not document the full range of user experiences, including potential challenges and negative aspects. Additionally, a follow-up paper is underway to analyze the negative EMA feedback, which will complement this work and provide a more balanced understanding of hearing aid experiences. Furthermore, the free-text EMA method, while rich in detail, can be time-consuming for participants, which may influence engagement and data comprehensiveness.
Future studies could benefit from enhanced app instructions and prompts, alongside efforts to capture a more diverse participant demographic to broaden the research's relevance. Addressing these limitations in future research would help in obtaining more generalized and comprehensive insights into the real-world benefits of hearing aids.
5 Conclusions
Qualitative self-initiated EMA with positive sentiment has demonstrated its potential to uncover the diverse benefits of HAs, offering unique insights into the wearer's experience in real-world settings. The effort participants invest in free-text EMAs yields significant insights, particularly when analyzing positive EMA statements. This study confirms the substantial role of HAs in enhancing listening experiences, sound quality, and communication, even in less documented contexts such as air travel. Features like direct streaming, extended battery life, and rechargeability were particularly valued, bolstering satisfaction and supporting audiologists in delivering personalized auditory solutions. An innovative use of EMA through smartphone apps could enable wearers to contribute feedback spontaneously, allowing for example the immediate analysis of voice notes via NLP strategies. This could extract meaningful themes in real-time, informing clinicians or activating support mechanisms (i.e., specialized chatbots) to assist individuals in those exact moments of need. Employing this technology could lead to more dynamic, responsive, and person-centered hearing care, leveraging personal narratives to address the intricacies of daily life for HA wearers and enhance hearing rehabilitation strategies.
Data availability statement
The datasets presented in this article are not readily available because of the mobile application's data privacy notice. Requests to access the datasets should be directed to Q2hhcmxvdHRlLlZlcmNhbW1lbiYjeDAwMDQwO3Nvbm92YS5jb20=.
Ethics statement
The studies involving humans were approved by Research Ethics Committee of the Faculty of Humanities, University of Pretoria, South Africa (HUM023/0922). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
CF: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. FM-A: Supervision, Writing – review & editing. IO: Supervision, Writing – review & editing. VM: Supervision, Writing – review & editing. CV: Supervision, Writing – review & editing. DS: Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. CV was supported by the NIHR Manchester Biomedical Research Centre. IO is a post-doctoral fellow at the University of Pretoria supported by a grant from Sonova, AG.
Conflict of interest
CV is professionally employed by Sonova AG. VM serves as the scientific advisor for hearX SA Pty Ltd.
The remaining authors state that the study was done without any commercial or financial links that could be interpreted as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fauot.2024.1397822/full#supplementary-material
References
Baden, C., Pipal, C., Schoonvelde, M., and van der Velden, M. A. C. G. (2022). Three gaps in computational text analysis methods for social sciences: a research agenda. Commun. Methods Meas. 16, 1–18. doi: 10.1080/19312458.2021.2015574
Bolger, N., Davis, A., and Rafaeli, E. (2003). Diary methods: capturing life as it is lived. Annu. Rev. Psychol. 54, 579–616. doi: 10.1146/annurev.psych.54.101601.145030
Boothroyd, A. (2007). Adult aural rehabilitation: what is it and does it work? Trends Amplif. 11, 63–71. doi: 10.1177/1084713807301073
Brice, S., and Almond, H. (2022). Is teleaudiology achieving person-centered care: a review. Int. J. Environ. Res. Public Health 19:7436. doi: 10.3390/ijerph19127436
Burke, L. E., Shiffman, S., Music, E., Styn, M. A., Kriska, A., Smailagic, A., et al. (2017). Ecological momentary assessment in behavioral research: addressing technological and human participant challenges. J. Med. Int. Res. 19:77. doi: 10.2196/jmir.7138
Campos, P. D., Bozza, A., and Ferrari, D. V. (2014). Hearing aid handling skills: relationship with satisfaction and benefit. CoDAS 26, 10–16. doi: 10.1590/s2317-17822014.001-0003
Chasin, M. (2017). Overview of Smartphone Control of Hearing Aids. Canadian Audiologist. Available at: https://canadianaudiologist.ca/smartphone-overview-feature/ (accessed November 3, 2023).
Cox, R. M., Johnson, J. A., and Xu, J. (2014). Impact of advanced hearing aid technology on speech understanding for older listeners with mild to moderate, adult-onset, sensorineural hearing loss. J. Gerontol. 60, 557–568. doi: 10.1159/000362547
Dillard, L. K., Saunders, G. H., Zobay, O., and Naylor, G. (2020). Insights into conducting audiological research with clinical databases. Am. J. Audiol. 29, 676–681. doi: 10.1044/2020_AJA-19-00067
Ferguson, M. A., Kitterick, P. T., Chong, L. Y., Edmondson-Jones, M., Barker, F., and Hoare, D. J. (2017). Hearing aids for mild to moderate hearing loss in adults. Cochr. Database Syst. Rev. 9:CD012023. doi: 10.1002/14651858.CD012023.pub2
Franks, I., and Timmer, B. H. B. (2023). Reasons for the non-use of hearing aids: perspectives of non-users, past users, and family members. Int. J. Audiol. 1–8. doi: 10.1080/14992027.2023.2270703
Friedman, C., Rubin, J., Brown, J., Buntin, M., Corn, M., Etheredge, L., et al. (2015). Toward a science of learning systems: a research agenda for the high-functioning Learning Health System. J. Am. Med. Inform. Assoc. 22, 43–50. doi: 10.1136/amiajnl-2014-002977
Galvez, G., Turbin, M. B., Thielman, E. J., Istvan, J. J., Andrews, J. A., and Henry, J. A. (2012). Feasibility to ecological momentary assessment of hearing difficulties encountered by hearing aid users. Ear Hear. 33, 497–507. doi: 10.1097/AUD.0b013e3182498c41
Gomez, R., Habib, A., Maidment, D. W., and Ferguson, M. A. (2022). Smartphone-connected hearing aids enable and empower self-management of hearing loss: a qualitative interview study underpinned by the behavior change wheel. Ear Hear. 43, 921–932. doi: 10.1097/AUD.0000000000001143
Granberg, S., and Gustafsson, J. (2021). Key findings about hearing loss in the working-life: a scoping review from a well-being perspective. Int. J. Audiol. 60, 60–70. doi: 10.1080/14992027.2021.1881628
Graneheim, U. H., and Lundman, B. (2004). Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ. Today 24, 105–112. doi: 10.1016/j.nedt.2003.10.001
Greasley, A., Crook, H., and Fulford, R. (2020). Music listening and hearing aids: perspectives from audiologists and their patients. Int. J. Audiol. 59, 694–706. doi: 10.1080/14992027.2020.1762126
Hasan, S. S., Chipara, O., Wu, Y. H., and Aksan, N. (2014). “Evaluating auditory contexts and their impacts on hearing aid outcomes with mobile phones,” in Proceedings - PERVASIVEHEALTH 2014: 8th International Conference on Pervasive Computing Technologies for Healthcare, 126–133. doi: 10.4108/icst.pervasivehealth.2014.254952
Heselton, T., Bennett, R. J., Manchaiah, V., and Swanepoel, W. (2022). Online reviews of hearing aid acquisition and use: a qualitative thematic analysis. Am. J. Audiol. 31, 284–298. doi: 10.1044/2021_AJA-21-00172
Holman, J. A., Drummond, A., Hughes, S. E., and Naylor, G. (2019). Hearing impairment and daily-life fatigue: a qualitative study. Int. J. Audiol. 58, 408–416. doi: 10.1080/14992027.2019.1597284
Holman, J. A., Drummond, A., and Naylor, G. (2021). Hearing aids reduce daily-life fatigue and increase social activity: a longitudinal study. Trends hear. 25:23312165211052786. doi: 10.1177/23312165211052786
Holube, I., von Gablenz, P., and Bitzer, J. (2020). Ecological momentary assessment in hearing research: current state, challenges, and future directions. Ear Hear. 41, 79–90. doi: 10.1097/AUD.0000000000000934
Humes, L. E. (2003). Modeling and predicting hearing aid outcome. Trends Amplif. 7, 41–75. doi: 10.1177/108471380300700202
Jiang, J. A., Wade, K., Fiesler, C., and Brubaker, J. R. (2021). Supporting serendipity: opportunities and challenges for human-ai collaboration in qualitative analysis. Proc. ACM Hum. Comput. Interact. 5, 1–23. doi: 10.1145/3449168
Kaplan-Neeman, R., Muchnik, C., Hildesheimer, M., and Henkin, Y. (2012). Hearing aid satisfaction and use in the advanced digital era. Laryngosc. Investig. Otolaryngol. 122, 2029–2036. doi: 10.1002/lary.23404
Knoetze, M., Manchaiah, V., Mothemela, B., and Swanepoel, W. (2023). Factors influencing hearing help-seeking and hearing aid uptake in adults: a systematic review of the past decade. Trends Hear. 27:23312165231157255. doi: 10.1177/23312165231157255
Knudsen, L. V., Laplante-Lévesque, A., Jones, L., Preminger, J. E., Nielsen, C., Lunner, T., et al. (2012). Conducting qualitative research in audiology: a tutorial. Int. J. Audiol. 51, 83–92. doi: 10.3109/14992027.2011.606283
Maidment, D. W., Ali, Y. H. K., and Ferguson, M. A. (2019). Applying the COM-B model to assess the usability of smartphone-connected listening devices in adults with hearing Loss. J. Am. Acad. Audiol. 30, 417–430. doi: 10.3766/jaaa.18061
Manchaiah, V., Swanepoel, D. W., Bailey, A., Pennebaker, J. W., and Bennett, R. J. (2021a). Hearing aid consumer reviews: a linguistic analysis in relation to benefit and satisfaction ratings. Am. J. Audiol. 30, 761–768. doi: 10.1044/2021_AJA-21-00061
Manchaiah, V., Swanepoel, D. W., and Bennett, R. J. (2021b). Online consumer reviews on hearing health care services: a textual analysis approach to examine psychologically meaningful language dimensions. Am. J. Audiol. 30, 669–675. doi: 10.1044/2021_AJA-20-00223
Mothemela, B., Manchaiah, V., Mahomed-Asmail, F., Knoetze, M., and Swanepoel, W. (2023). Factors influencing hearing aid use, benefit and satisfaction in adults: a systematic review of the past decade. Int. J. Audiol. 63, 661–674. doi: 10.1080/14992027.2023.2272562
Oosthuizen, I., Manchaiah, V., Launer, S., and Swanepoel, W. (2022). Hearing aid experiences of adult hearing aid owners during and after fitting: a systematic review of qualitative studies. Trends Hear. 26:23312165221130584. doi: 10.1177/23312165221130584
Pew Research Center (2022). Social Media Seen as Mostly Good for Democracy Across Many Nations, But U.S. Is a Major Outlier. Available at: https://www.pewresearch.org/global/2022/12/06/internet-smartphone-and-social-media-use-in-advanced-economies-2022/ (accessed December 11, 2023).
Picou, E. M. (2020). MarkeTrak 10 (MT10) Survey results demonstrate high satisfaction with and benefits from hearing aids. Semin. Hear. 41, 21–36. doi: 10.1055/s-0040-1701243
Schinkel-Bielefeld, N., Kunz, P., Zutz, A., and Buder, B. (2020). Evaluation of hearing aids in everyday life using Ecological Momentary Assessment: what situations are we missing? Am. J. Audiol. 29, 591–609. doi: 10.1044/2020_AJA-19-00075
Shiffman, S., Stone, A. A., and Hufford, M. R. (2008). Ecological momentary assessment. Annu. Rev. Clin. Psychol. 4, 1–32. doi: 10.1146/annurev.clinpsy.3.022806.091415
Strelcyk, O., and Singh, G. (2018). TV listening and hearing aids. PLoS ONE 13:e0200083. doi: 10.1371/journal.pone.0200083
Sun, B. M. (2019). The Counseling Advantages of Rechargeable Hearing Aid Batteries. CUNY Academic Works. Available at: https://academicworks.cuny.edu/gc_etds/3188
Taneja, N. (2020). Rechargeable battery slutions for digital hearing aids: a mini review. Int. J. Otolaryngol. 5, 14–17. Available at: https://openventio.org/wp-content/uploads/Rechargeable-Battery-Solutions-for-Digital-Hearing-Aids-A-Mini-Review-OTLOJ-SE-5-104.pdf
Timmer, B. H. B., Bennett, R. J., Montano, J., Hickson, L., Weinstein, B., Wild, J., et al. (2023). Social-emotional well-being and adult hearing loss: clinical recommendations. Int. J. Audiol. 63, 381–392. doi: 10.1080/14992027.2023.2190864
Timmer, B. H. B., Hickson, L., and Launer, S. (2017). Ecological momentary assessment: feasibility, construct validity, and future applications. Am. J. Audiol. 26, 436–442. doi: 10.1044/2017_AJA-16-0126
Timmer, B. H. B., Hickson, L., and Launer, S. (2018). The use of ecological momentary assessment in hearing research and future clinical applications. Hear. Res. 369:24228. doi: 10.1016/j.heares.2018.06.012
Trull, T. J., and Ebner-Priemer, U. (2014). The role of ambulatory assessment in psychological science. Curr. Dir. Psychol. Sci. 23, 466–470. doi: 10.1177/0963721414550706
Vercammen, C., Bott, A., and Saunders, G. H. (2021). Hearing health in the broader context of healthy living and well-being: changing the narrative. Int. J. Audiol. 60, 86–91. doi: 10.1080/14992027.2021.1905893
Vercammen, C., Oosthuizen, I., Manchaiah, V., Ratinaud, P., Launer, S., and Swanepoel, D. W. (2023). Real-life and real-time hearing aid experiences: Insights from self-initiated ecological momentary assessments and natural language analysis. Front. Digit. Health. 5:1104308. doi: 10.3389/fdgth.2023.1104308
Verheij, R. A., Curcin, V., Delaney, B. C., and McGilchrist, M. M. (2018). Possible sources of bias in primary care electronic health record data use and reuse. J. Med. Int. Res. 20:e185. doi: 10.2196/jmir.9134
von Gablenz, P., Kowalk, U., Bitzer, J., Meis, M., and Holube, I. (2021). Individual hearing aid benefit in real life evaluated using Ecological Momentary Assessment. Trends Hear. 25:2331216521990288. doi: 10.1177/2331216521990288
Wong, L. L., Hickson, L., and McPherson, B. (2003). Hearing aid satisfaction: what does research from the past 20 years say? Trends Amplif. 7, 117–161. doi: 10.1177/108471380300700402
Wu, Y., Stangl, E., Chipara, O., Hasan, S. S., Wellhaven, A., and Oleson, J. (2018). Characteristics of real-world signal-to-noise ratios and speech listening situations of older adults with mild-to-moderate hearing loss. Ear Hear. 39, 293–304. doi: 10.1097/AUD.0000000000000486
Keywords: hearing aids, hearing aid outcome, Ecological Momentary Assessment (EMA), everyday situations, real-life data
Citation: Fourie C, Mahomed-Asmail F, Oosthuizen I, Manchaiah V, Vercammen C and Swanepoel DW (2024) Hearing aid benefit in daily life: a qualitative ecological momentary assessment study. Front. Audiol. Otol. 2:1397822. doi: 10.3389/fauot.2024.1397822
Received: 08 March 2024; Accepted: 16 September 2024;
Published: 09 October 2024.
Edited by:
Norbert Dillier, University of Zurich, SwitzerlandReviewed by:
Niels Henrik Pontoppidan, Eriksholm Research Centre, DenmarkRazan Alfakir, Auburn University, United States
Copyright © 2024 Fourie, Mahomed-Asmail, Oosthuizen, Manchaiah, Vercammen and Swanepoel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: De Wet Swanepoel, ZGV3ZXQuc3dhbmVwb2VsJiN4MDAwNDA7dXAuYWMuemE=