 David Lluís Garulo1*
David Lluís Garulo1* Maitane Alonso2Judith Rodríguez3Natalia Manent4
Maitane Alonso2Judith Rodríguez3Natalia Manent4 Montse Gomà Gallego3Esther Guerra Fernández5Francesc Xavier Sanjuan Garriga3Paula Gubern Prieto1Anna Penella Prat2Sira Salinas Huertas4David Chivite Guillen6
Montse Gomà Gallego3Esther Guerra Fernández5Francesc Xavier Sanjuan Garriga3Paula Gubern Prieto1Anna Penella Prat2Sira Salinas Huertas4David Chivite Guillen6 Sonia Pernas1
Sonia Pernas1 Catalina Falo1*
Catalina Falo1*- 1Medical Oncology, Catalan Institute of Oncology, Barcelona, Spain
- 2ENT Department, Bellvitge University Hospital, Barcelona, Spain
- 3Pathology Department, Bellvitge University Hospital, Barcelona, Spain
- 4Rehabilitation Department, Bellvitge University Hospital, Barcelona, Spain
- 5Bellvitge University Hospital, Barcelona, Spain
- 6Internal Medicine Department, Bellvitge University Hospital, Barcelona, Spain
Facial nerve (FN) palsy, as a solitary symptom resulting from a metastatic tumor, is uncommon, and metastases to the external auditory canal (EAC) are even more infrequent. In this article, we report a unique case of the de novo stage IV invasive lobular breast carcinoma (LBC) presenting as an EAC metastasis and leading to FN palsy as the first symptom, highlighting the importance of considering a broad differential diagnosis.
Introduction
Idiopathic Bell's palsy is the most common cause of peripheral facial nerve (FN) paralysis, and the diagnosis is one of exclusion. Its setting in the context of metastatic disease is rare but has been described as mostly caused by temporal infiltration leading to compression of the nerve. Otomastoiditis secondary to the external auditory canal (EAC) metastasis is also infrequent (Cumberworth and Friedmann, 1994; Sari et al., 2015). Invasive lobular breast carcinoma (LBC) is a histological subtype of breast cancer with unique clinical and molecular features, including unusual sites of metastatic dissemination (Ashikari et al., 1973; Pestalozzi et al., 2008). We present an uncommon case of a patient in whom all these factors converge: a de novo metastatic lobular breast carcinoma to the EAC that causes otomastoiditis and leads to peripheral FN paralysis. In the era of high-resolution diagnostic tools, this case highlights the importance of a complete medical history, anamnesis, and full physical examination, which are often overlooked.
Case description
A 68-year-old female patient with no previous medical history presented to the general practitioner with a history of progressive left peripheral FN paralysis affecting all levels. There was no pain or evidence of hearing loss, and no other clinical findings were present in the remaining neurological examination, the otoscopy, or the examination of the mastoid process. A steroid taper was recommended.
After 2 weeks, the function of the left facial muscles had not returned, and the patient was remitted to an ear–nose–throat (ENT) specialist. The otolaryngologic examination revealed severe facial palsy: grade VI based on the House Brackmann Facial Nerve Grading System and 0% on the Sunnybrook Facial Grading System. Hearing and vestibular functions were found to be within limits, with mild bilateral presbycusis as the only finding. Over the next months, electromyography revealed greatly deficient motor unit potentials, indicating severe left FN denervation at all levels. High-resolution computerized tomography of the temporal bone was performed, which showed a reduction of the caliber of the left EAC at the expense of the enlargement of its walls, with thickening of the tympanic membrane and total occupation of the mesotympanum and hypotympanum and partial occupation of the epitympanum, with no erosion of the ossicular chain or the tegmen tympani. The presence of otorrhea in the left ear was observed, and a provisional diagnosis of chronic otitis media was made. Empiric topical antibiotic (ciprofloxacin) was prescribed with no immediate improvement.
With no signs of recovery, the patient was referred to the Facial Paralysis Rehabilitation Unit in a tertiary hospital: Hospital Universitari de Bellvitge. During the first consultation, severe facial hypotonia was noted, and a parotid ultrasound and a skull base, internal auditory canal, and facial tract magnetic resonance imaging (MRI) with contrast were requested. With a persisting Sunnybrook Facial Grading System score of 0, neuromuscular reeducation was initiated because of the lack of improvement. The skull base MRI showed total occupation of the left mastoid cells and middle ear with thickening of the EAC (Figure 1). It also revealed remarkable meningeal thickening in the basal and lateral temporal region, associated with edema predominantly engaging the white matter and extending to the posterior insular region. An unexpected finding revealed that the lesion was also infiltrative, involving the vertebrae bodies of C5 and C6 and the right posterior elements of C5, with partial foraminal narrowing of C4–C5 and C5–C6. Given these results and a diagnosis of complicated otomastoiditis with intracranial involvement, intravenous empiric antibiotics were started, and the patient was admitted for further studies in the ENT department of said hospital.
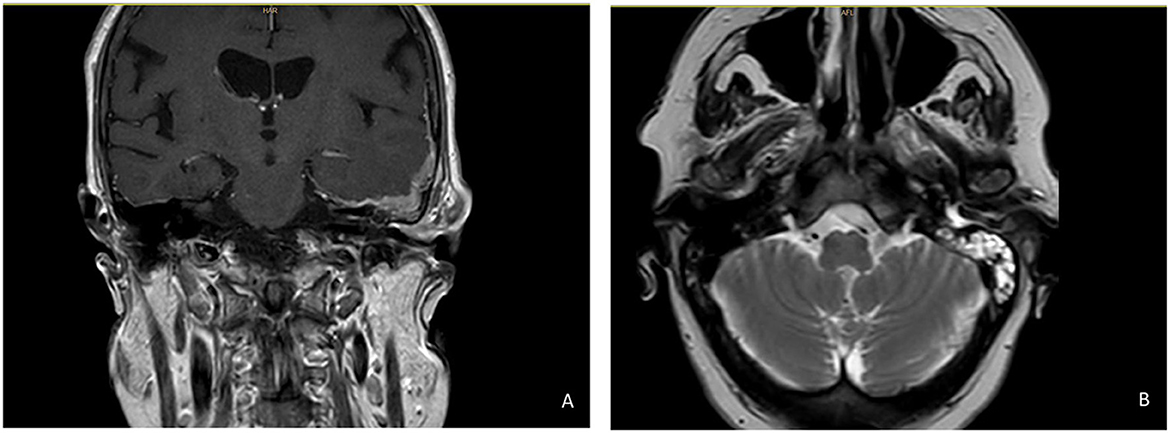
Figure 1. Initial Skull Base MRI showcasing EAC infiltration. (A) Coronal plane, T1 sequence with contrast. (B) Transversal plane, T2 sequenc with contrast.
Upon the patient's admission, the ENT team and the internal medicine consultants performed further evaluations. On interrogation, cephalalgia, left otalgia, hearing loss, and persistence of light purulent ear drainage during the weeks before the MRI were noted. Besides the symptoms related to the otologic disease, the patient also presented with progressive asthenia and left mechanical thigh pain, causing functional motor impairment of the lower limb, which had undergone a parallel, preliminary neurological evaluation as an outpatient with a suspicion of peripheral neuropathy/radiculopathy. Additionally, mild left limb shortening with external rotation plus local pain upon palpation of the right thigh, exacerbated by dynamic flexo-extension of the hip, was reported. The ENT physical examination revealed an edematous left EAC with purulent otorrhea present, a negative tragal sign, a left Rinne test, and a central Webber test. Finally, the thoracic examination disclosed a voluminous, hard, and irregularly shaped right breast mass with skin dimpling, accompanied by at least two ipsilateral axillary lymph nodes, of which the patient was well aware but had been scared to reveal to any of the attending physicians in the preceding months.
With the suspicion of advanced breast cancer with polytopic bone metastases, multiple studies were requested. A simple bone X-ray disclosed lytic lesions in the left femur resulting in a pathological hip neck fracture. A positron electron tomography–computed tomography (PET-CT) imaging scan showed hypermetabolic thickening of heterogeneous density involving the EAC (Figure 2); total occupation of the mastoid cells; a lytic lesion with associated soft-tissue component in the left side of the clivus (Figure 3); multiple lytic bone lesions, including the ones involving C5–C6 and the right femoral head; and abnormal uptake in the right breast and retropectoral, axillary, and mediastinal lymph nodes, among other sites. A medullary MRI revealed radicular compromise at the C6 level and excluded spinal cord compression. Steroid therapy was started, a myringotomy was performed, and a drainage tube was placed, in addition to 3 weeks of intravenous antibiotic therapy with piperacillin/tazobactam being completed while maintaining topical ciprofloxacin. The ear drainage culture showed no bacterial growth.
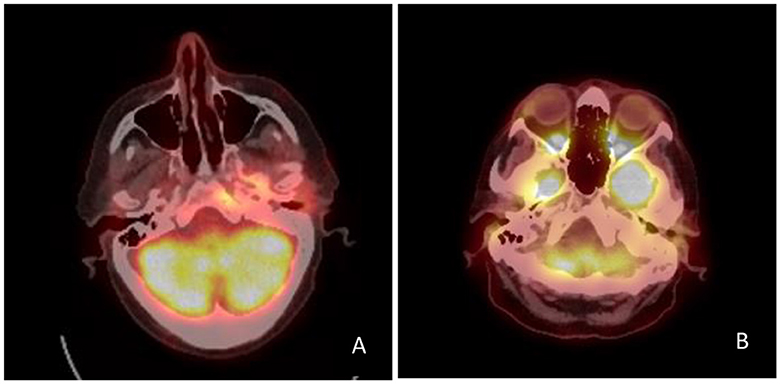
Figure 2. PET-CT scans showcasing EAC infiltration. (A) Initial scan: hypermetabolic thickening of heterogeneous density involving de EAC, with a SUVmax of 6.5. (B) Follow-up scan after 6 months: absence of metabolic intake the EAC.
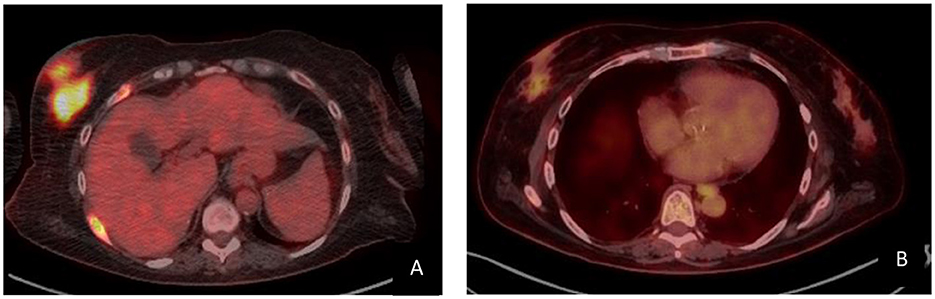
Figure 3. PET-CT scans showcasing the breast mass. (A) Initial scan: hypermetabolic mass of 52 × 58 mm involving the inferior quadrants of the right breast with a SUVmax of 11.17. (B) Follow-up scan after 6 months: hypermetabolic mass of 16 × 27 mm with a SUVmax of 2.94.
Concomitant biopsies were performed. The core breast biopsy showed an ILC with a Nottingham histologic grade 2, and no evidence of vascular invasion, tumor-infiltrating lymphocytes (TILs), or tumoral necrosis. Immunohistochemically, the cells were positive for estrogen and progesterone receptors, with 100% and 90% nuclear positivity, respectively. The proliferative index was 16%. It conveyed an equivocal HER2++, with a negative gene status evaluation by FISH. E-cadherin expression was negative (Figure 4). However, a surgical exploration of the ear was performed with myringotomy, and a transtympanic drainage tube was placed to solve the middle ear effusion. An incision biopsy of the EAC also revealed infiltration by carcinoma compatible with a mammary origin (Figure 5).
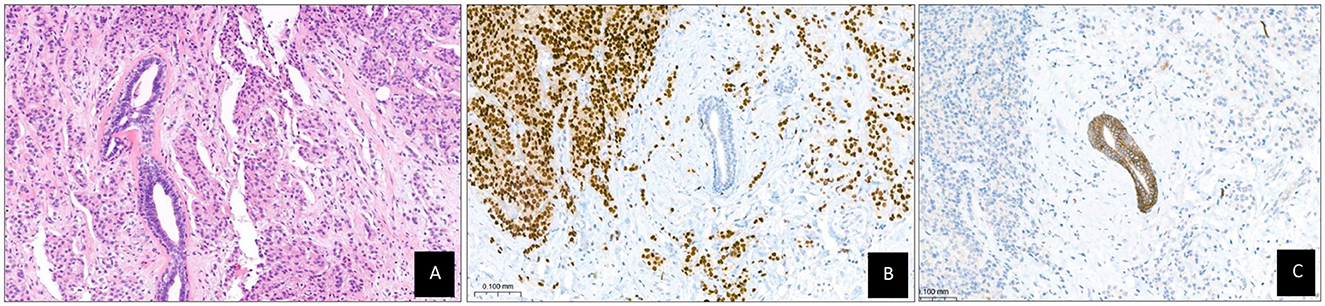
Figure 4. Breast biopsy. (A) Invasive lobular carcinoma surrounding a benign DUCT (HE). (B) Estrogen receptors: positive. (C) E-cahderin: negative in invasive tumor and positive in benign duct.

Figure 5. External auditory biopsy. (A) Connective tissue showing artefacted cords and nests of epithelial cells (arrow mark). (B) Estrogen receptors: positive. (C) Cytoqueratin 19: positive.
With the clinical diagnosis of hormone receptor (HR) positive, HER2 negative de novo stage IV ILC of the breast, the patient was referred to the medical oncology department. While the patient was still hospitalized, systemic therapy with aromatase inhibitor and endovenous bisphosphonates was initiated. The patient underwent a hemiarthroplasty for the femoral neck fracture without major complications, and the bone tissue histopathological examination confirmed the presence of invasive LBC. A hard cervical collar was placed, and the patient received palliative radiation therapy over two of the affected areas: the C5–6–7 and D1 vertebral somas and the L1 vertebral soma, 20Gy over 4 sessions each. The patient was then discharged.
At the oncology clinic 1 month after the femoral surgery, the patient presented an excellent recovery, and therapy with cyclin-dependent kinase inhibitors (CDK 4/6i) was added. At a follow-up after 6 months of therapy, the disease presented an excellent response, with a morpho-metabolic decrease in both breast and bones according to PET-CT scans (Figures 2, 3). Ear pain and otorrhea have resolved completely, but the peripheral FN paralysis remains. A left and predominantly sensorineural, with an auditory threshold of 70 decibels hearing loss, persists. Hearing rehabilitation with hearing aids was proposed, but the patient rejected it due to acceptable contralateral hearing. A lateral tarsal strip surgery was performed successfully to avoid eye damage. In the latest follow-up, the patient fortunately had regained autonomy, was able to walk without support, and conveyed a good quality of life, maintaining a Karnofsky Index of 90%.
Discussion
Invasive LBC is the second-most common histological type of invasive cancer, representing 5%−15% of all breast cancers (Ashikari et al., 1973). Compared to invasive ductal carcinoma (IDC) of the breast, invasive LBC is characterized by unique features, including a more challenging radiographic detection by mammography and ultrasound due to its distinctive growth pattern that prevents the cells from forming any distinct masses (Arpino et al., 2004). Even PET imaging might be a suboptimal diagnostic tool, due to the low histological grade and high HR positivity associated with most invasive LBCs (Gilardi et al., 2023). Other more controversial features between invasive LBC and IDC might be its relationship with hormone dependence (Pestalozzi et al., 2008) and the differences in recurrence and overall prognosis (Pestalozzi et al., 2008; Garcia-Fernandez et al., 2015). Multiple studies have compared its metastatic patterns; for instance, Inoue et al. (2017) reported a higher incidence of spreading to the bone, gastrointestinal, or gynecologic tracts of the invasive LBC compared to the IDC, which most commonly spreads to the lung and pleura (Pestalozzi et al., 2008). Other studies, such as those by Lamovec and Bracko (1991) and Ferlicot et al. (2004), displayed similar findings (Pestalozzi et al., 2008). The causes of these distinct traits are unclear, although the loss of expression of the cell–cell adhesion molecule E-cadherin in invasive LBC might be responsible (Gruel et al., 2010) as an association between mutations in the cadherin (CDH1) gene and invasive LBC development has been reported (Keller et al., 1999).
Metastatic tumors of the breast in the EAC are exceptionally rare. So far, only two cases have been reported in the literature with otalgia, hearing loss, and bleeding presenting as the initial symptoms. In both cases, the patients had a prior history of breast cancer, and the metastases appeared as a disease recurrence (Cumberworth and Friedmann, 1994; Sari et al., 2015). In our case, the initial CT scan showed an enlargement of the EAC that suggested infiltration, confirmed by a biopsy showing a microscopic focus on carcinoma. The possibility that other parts of the temporal bone may be infiltrated by carcinoma cannot be ruled out either by extension or because of a differentiated metastatic focus. Given the extended bone involvement, knowing exactly which segment of the nerve was compromised is difficult. Although ear drainage cultures showed no bacterial growth, an infectious component is likely, even if it was only present during the weeks before admission as otorrhea and earache improved after antimicrobial therapy was established.
Peripheral FN paralysis as the first manifestation of metastatic breast disease is also fairly rare, although several cases have been reported either due to compression by temporal bone involvement (Breadon et al., 1977) or, less frequently, due to intraneural infiltration (Makuszewska et al., 2021). Other common symptoms include hearing loss, pain, and vertigo (Hadjigeorgiou et al., 2020). In the presented case, the diagnosis was driven by the prolonged symptoms of facial paralysis, followed by hearing loss, earache, and otorrhea, which led to additional imaging and the findings that suggested a metastatic neoplastic disease. The absence of a prior cancer history, in addition to the patient's concealment of the breast mass, partially explains the delay in diagnosis.
In terms of treatment, given the uniqueness of the case, there is no specific treatment. During admission, high-dose corticoid therapy and intravenous antibiotic therapy were administered, and with the final diagnosis of invasive LBC, targeted treatment for first-line HR+/HER2-negative metastatic breast cancer with endocrine therapy plus CDK 4/6i was promptly initiated. Most otolaryngological symptoms resolved, except for the facial palsy, which might be due to a permanently damaged nerve.
Conclusion
Deep anamnesis and complete physical examination should always be carried out, as a solitary symptom may be underlying systemic involvement. Despite the rarity, metastatic disease should be included in the differential diagnosis in any patient who develops otomastoiditis and peripheral FN paralysis, especially when it presents with challenging management, as it may be masquerading as other conditions. Further investigation is needed to better understand the characteristic attributes of invasive LBC that lead to atypical presentations.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
Ethics statement
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
DL: Writing – original draft, Writing – review & editing. MA: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. JR: Writing – original draft, Writing – review & editing. NM: Writing – original draft, Writing – review & editing. MG: Writing – original draft, Writing – review & editing. EG: Writing – original draft, Writing – review & editing. FS: Writing – original draft, Writing – review & editing. PG: Writing – original draft, Writing – review & editing. AP: Writing – original draft, Writing – review & editing. SS: Writing – original draft, Writing – review & editing. DC: Writing – original draft, Writing – review & editing. SP: Writing – original draft, Writing – review & editing. CF: Writing – original draft, Writing – review & editing, Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Arpino, G., Bardou, V. J., Clark, G. M., and Elledge, R. M. (2004). Infiltrating lobular carcinoma of the breast: tumor characteristics and clinical out- come. Breast Cancer Res. 6, R149–R156. doi: 10.1186/bcr767
Ashikari, R., Huvos, A. G., Urban, J. A., and Robbins, G. F. (1973). Infiltrating lobular carcinoma of the breast. Cancer. 31, 110–116. doi: 10.1002/1097-0142(197301)31:1<110::AID-CNCR2820310115>3.0.CO;2-V
Breadon, G. E., Cody, D. T., and Weilandz, L. H. (1977). Facial palsy: unusual etiology. Laryngoscope 87, 26–34. doi: 10.1288/00005537-197701000-00004
Cumberworth, V. L., and Friedmann, I. (1994). Late metastasis of breast carcinoma to the external auditory canal. J. Laryngol. Otol. 108, 808–810. doi: 10.1017/S0022215100128208
Ferlicot, S., Vincent-Salomon, A., Medioni, J., Genin, P., Rosty, C., Sigal-Zafrani, B., et al. (2004). Wide metastatic spreading in infiltrating lobular carcinoma of the breast. Eur. J. Cancer 40, 336–341. doi: 10.1016/j.ejca.2003.08.007
Garcia-Fernandez, A., Lain, J. M., Chabrera, C., Garcia Font, M., Fraile, M., Barco, I., et al. (2015). Comparative longterm study of a large series of patients with invasive ductal carcinoma and invasive lobular carcinoma. Loco regional recurrence, metastasis, and survival. Breast J. 21, 533–537. doi: 10.1111/tbj.12455
Gilardi, L., Airò Farulla, L. S., Curigliano, G., Corso, G., Leonardi, M. C., Ceci, F. F. D. G., et al. (2023). FDG and non FDG radiopharmaceuticals for PET imaging in invasive lobular breast carcinoma. Biomedicines 11:1350. doi: 10.3390/biomedicines11051350
Gruel, N., Lucchesi, C., Raynal, V., Rodrigues, M. J., Pierron, G., Goudefroye, R., et al. (2010). Lobular invasive carcinoma of the breast is a molecular entity distinct from luminal invasive ductal carcinoma. Eur. J Cancer. 46, 2399–2407. doi: 10.1016/j.ejca.2010.05.013
Hadjigeorgiou, G. F., Michalinos, A., Shiakallis, L., Fountas, K. F., and Johnson, E. O. (2020). Facial palsy caused by an intrameatal metastatic disease - Reconstruction with an autologous sural nerve graft. Injury 51, S93–S95. doi: 10.1016/j.injury.2020.03.048
Inoue, M., Nakagomi, H., Nakada, H., Furuya, K., Ikegame, K., Watanabe, H., et al. (2017). Specific sites of metastases in invasive lobular carcinoma: a retrospective cohort study of metastatic breast cancer. Breast Cancer 24, 667–672. doi: 10.1007/s12282-017-0753-4
Keller, G., Vogelsang, H., Becker, I., Hutter, J., Ott, K., Candidus, S., et al. (1999). Diffuse type gastric and lobular breast carcinoma in a familial gastric cancer patient with an E-cadherin germline mutation. Am. J. Pathol. 155, 337–342. doi: 10.1016/S0002-9440(10)65129-2
Lamovec, J., and Bracko, M. (1991). Metastatic pattern of infiltrating lobular carcinoma of the breast: an autopsy study. J. Surg. Oncol. 48, 28–33. doi: 10.1002/jso.2930480106
Makuszewska, M., Fus, Ł., and Bartoszewicz, R. (2021). Solitary breast cancer metastasis to the facial nerve. Breast J. 27, 838–840. doi: 10.1111/tbj.14279
Pestalozzi, B. C., Zahrieh, D., Mallon, E., Gusterson, B. A., Price, K. N., Gelber, R. D., et al. (2008). Distinct clinical and prognostic features of infiltrating lobular carcinoma of the breast: combined results of 15 International Breast Cancer Study Group clinical trials. J. Clin. Oncol. 26, 3006–3014. doi: 10.1200/JCO.2007.14.9336
Keywords: peripheral facial nerve palsy, metastatic breast adenocarcinoma, external auditory canal, lobular breast carcinoma, temporal bone abnormalities, case report
Citation: Lluís Garulo D, Alonso M, Rodríguez J, Manent N, Gomà Gallego M, Guerra Fernández E, Sanjuan Garriga FX, Gubern Prieto P, Penella Prat A, Salinas Huertas S, Chivite Guillen D, Pernas S and Falo C (2024) External auditory canal metastasis leading to peripheral facial paralysis as first manifestation of de novo stage IV invasive lobular carcinoma of the breast: a rare case report. Front. Audiol. Otol. 2:1391998. doi: 10.3389/fauot.2024.1391998
Received: 26 February 2024; Accepted: 30 July 2024;
Published: 20 August 2024.
Edited by:
David R. Friedmann, New York University, United StatesReviewed by:
Gianluca Piras, Gruppo Otologico, ItalyBrian Richard Earl, University of Cincinnati, United States
Copyright © 2024 Lluís Garulo, Alonso, Rodríguez, Manent, Gomà Gallego, Guerra Fernández, Sanjuan Garriga, Gubern Prieto, Penella Prat, Salinas Huertas, Chivite Guillen, Pernas and Falo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: David Lluís Garulo, ZGF2aWRsbHVpc2dAZ21haWwuY29t; Catalina Falo, Y2ZhbG9AaWNvbmNvbG9naWEubmV0