
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Audiol. Otol., 20 September 2023
Sec. Tinnitus
Volume 1 - 2023 | https://doi.org/10.3389/fauot.2023.1239119
 François Voruz1*
François Voruz1* Aurélie Vuilleumier2
Aurélie Vuilleumier2 Denis Migliorini2,3,4,5
Denis Migliorini2,3,4,5 German Nacher-Soler6
German Nacher-Soler6 Francis Rousset6Thibault De Maesschalck1
Francis Rousset6Thibault De Maesschalck1 Pascal Senn1,6
Pascal Senn1,6Introduction: Robust clinically relevant epidemiological and audiological data are needed to prepare for future clinical trials aiming at preventing cisplatin-induced ototoxicity in this suffering cancer population. We assessed the incidence, severity, and potential risk factors of symptomatic cisplatin-induced hearing loss in a large cohort of adults.
Methods: Retrospective cohort study at a tertiary care university hospital. The study group included consecutive patients over 18 years old treated with cisplatin-based chemotherapy without concomitant inner ear radiotherapy or other ototoxic medication. Every participant underwent baseline pretreatment audiometry and was asked for audiological symptoms (tinnitus or subjective hearing loss) during the treatment. If symptomatic, comparative standard audiometry (0.125 to 8 kHz) was performed. Hearing loss was defined by a threshold shift ≥15 dB HL in at least one of the tested frequencies.
Results: A total of 401 cancer patients (59% males) with a mean age of 56 years (range 18-80) were included. Eighty-one patients (20%) developed symptomatic hearing loss, predominantly affecting the high frequencies from 4 to 8 kHz. Among them, 49 (60%) experienced simultaneous new-onset tinnitus. None of the analyzed potential risk factors (age, sex, smoking, hypertension, diabetes, dyslipidemia, chemotherapeutic regimen, and cumulative cisplatin dose) was statistically correlated with hearing loss.
Discussion: At least 1 out of 5 patients treated with cisplatin developed audiological symptoms associated with audiometric hearing loss within the 0.125 to 8 kHz range, for which new-onset tinnitus is a sensitive symptom. Not all audiological symptoms are accompanied by audiometric change. No predisposing factor could be identified. Standardized audiological monitoring before and during cisplatin-based chemotherapy allows quantitative assessment of early audiometric signs of ototoxicity, offering to optimize anticancer therapy while minimizing morbidity in a multidisciplinary setting.
According to the World Health Organization (WHO), cancer is the leading cause of death worldwide, with 10 million human lives lost in 2020 (WHO, 2022). Nevertheless, ever-improving anticancer therapies and a longer life expectancy lead to more cancer survivors (Miller et al., 2016; Arnold et al., 2019). Therefore, chemotherapy-induced acute adverse effects such as nausea, anorexia, diarrhea, and loss of hair, as well as long-term sequelae such as neurotoxicity, nephrotoxicity, and hearing loss (Di Maio et al., 2015), among others, are becoming more prevalent and essential to palliate to. The inner ear is sensitive to various insults, including iatrogenic insults such as surgery (Simon, 2011), ionizing radiations (Mujica-Mota et al., 2013), and certain drugs (Roland and Rutka, 2004). When side effects of medicines impair hearing (cochlear damage) and balance (vestibular damage), the phenomenon is referred to as ototoxicity. Several drugs (summarized in Table 1) are ototoxic; among them, cisplatin stands out in potency and prevalence. However, vestibulotoxicity is poorly investigated, and the correlation between symptoms and examination should be interpreted cautiously (Prayuenyong, 2018; Prayuenyong et al., 2020). Additionally, measurements of vestibular impairment are expensive and time-consuming and, therefore, not routinely performed in our clinic in the absence of symptoms. For these reasons, this article will focus only on cochleotoxicity.
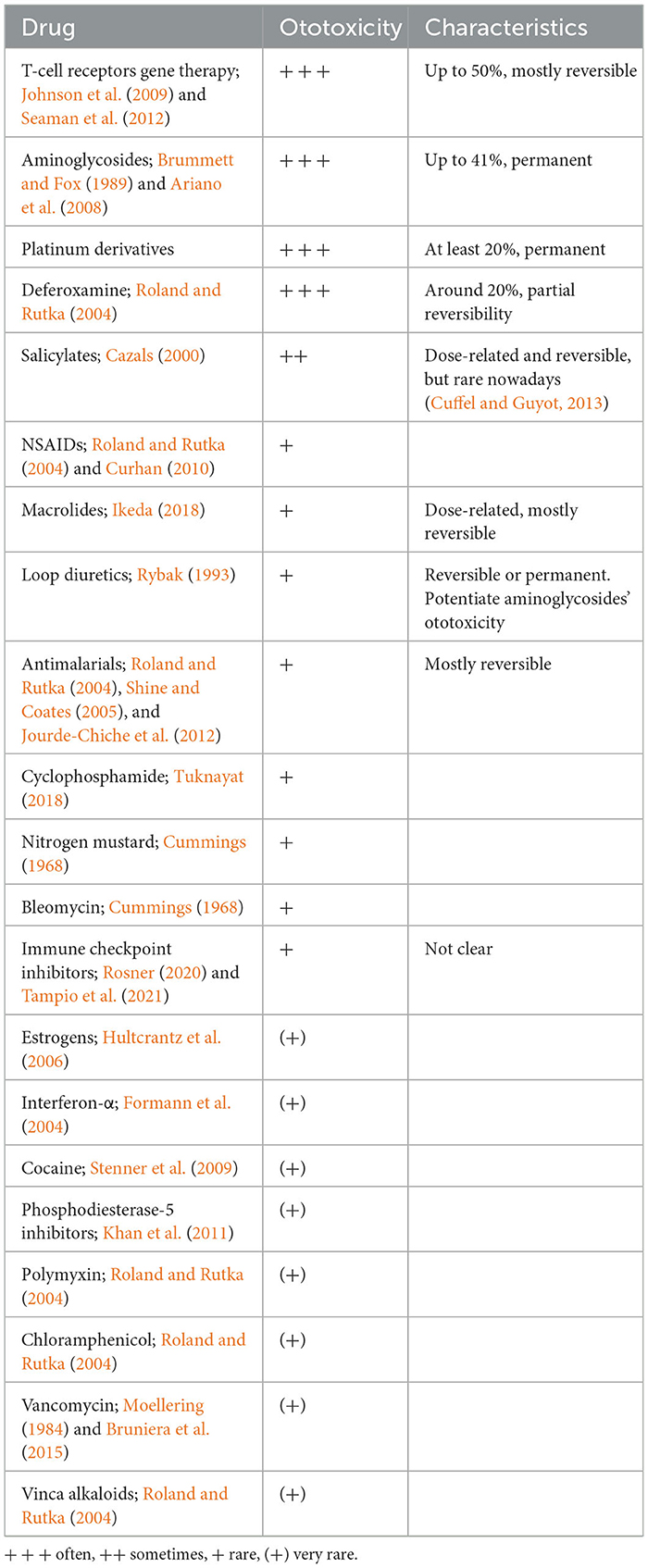
Table 1. Ototoxic drugs are classified according to their potency, with a summary of the main ototoxic characteristics of each compound.
Cisplatin (Cis-diamminedichloroplatinum(II), [Pt(NH3)2Cl2]) is an active platinum-based complex authorized for human use since 1978 (Kelland, 2007). Today, it is one of the most efficient anticancer agents against solid tumors (Dasari and Tchounwou, 2014) in adults and children and has been included in the WHO's list of “essential medicines” (WHO, 2021). Synergistic effects with different molecules have been described (Dasari and Tchounwou, 2014) together with a radio-sensitization effect potentializing radiotherapy (Yanfang Dong et al., 2017). Cisplatin-containing regimens are given with curative intent in various clinical settings, such as cervical, head and neck, lung, bladder, and testicular cancers. Among many chemical analogs with different toxicity and efficacy profiles, only carboplatin and oxaliplatin have brought an advantage over cisplatin regarding the adverse event profile, particularly ototoxicity (Kelland, 2007; Dasari and Tchounwou, 2014), and are also considered by the WHO as essential medicines (WHO, 2021). Because of the intrinsic and unspecific cytotoxic mechanisms (DNA alkylation, DNA repair, and replication inhibition), cisplatin is widely associated with toxic adverse effects, such as nausea, nephrotoxicity, neurotoxicity, cardiotoxicity, hepatotoxicity, gastrotoxicity, myelosuppression, allergic reactions and prevalent ototoxicity (Dasari and Tchounwou, 2014).
Some adverse events such as nephrotoxicity can be partly palliated (Bajorin et al., 1986), but no preventive drug or measure has been validated against ototoxicity (Chattaraj et al., 2023). Cisplatin-induced ototoxicity typically induces bilateral, symmetrical, irreversible sensorineural hearing loss, affecting primarily high frequencies, commonly in combination with tinnitus (Mujica-Mota et al., 2013), which can occur transiently or permanently and even without hearing loss. The cumulative dose, number of cycles, method of administration (bolus, continuous), and impaired renal function influence the occurrence and severity of cisplatin ototoxicity (Paken et al., 2016; van As et al., 2016). In addition, noise exposure, concomitant chemicals, and other ototoxic drugs can potentiate hearing loss (Paken et al., 2016). Genetic susceptibility may be an essential factor (Tserga et al., 2019). In the oncological context, it is important to note that cranial radiotherapy—another free-radical inducing therapy—is, per se, a significant risk factor, with a sensorineural hearing loss occurrence of up to 33% (Jereczek-Fossa et al., 2003). At the cellular level, the most reported cisplatin-related ototoxic mechanism involves reactive oxygen species (ROS) upregulation, leading to cochlear inflammation, stria vascularis degeneration, and apoptosis of outer hair cells, inner hair cells, and spiral ganglion neurons (Sheth et al., 2017).
Ototoxicity (including hearing loss, tinnitus and vestibular disorders) durably impact the quality of life of patients (Phillips et al., 2023; Sanchez et al., 2023a). The occurrence of cisplatin ototoxicity reported in clinical studies ranges from 26 to 100%, although the clinical relevance of these numbers is questionable (a selection of the literature including pretreatment audiogram is listed in Table 2). The wide variation of occurrence and severity across different studies mainly results from differences in methodologies, outcome measurements (especially hearing loss criteria), patient characteristics, and grading scales used, the latter having limitations (Waissbluth et al., 2017). Furthermore, the baseline pretreatment audiometry is often missing, limiting adequate interpretation of later exams during or after chemotherapy; this limitation is especially relevant in elderly cancer patients often suffering from concomitant age-related hearing loss (Nagy et al., 1999). Finally, despite the methodological differences, a significantly higher occurrence and severity of ototoxic hearing loss has been observed in young children (Landier, 2016).

Table 2. Representative literature from the beginning of cisplatin FDA approval, reporting ototoxicity in adults with baseline pretreatment audiometry, is listed.
At the dawn of a new age of otology, where promising treatment strategies aiming at otoprotection and regeneration are being tested in preclinical trials and await translation into clinical trials (Rousset et al., 2015; Isherwood et al., 2022), there is an increasing need for high-quality pragmatic data regarding cisplatin ototoxicity. The present study aims to establish solid clinically relevant epidemiological and audiological bases for the oncologists and otolaryngologists, besides helping institutions interested in preparing for future clinical trials aiming at preventing cisplatin-induced ototoxicity and offering to this suffering patient population adequate and timely translation of innovative treatment modalities to minimize morbidity. This study retrospectively assessed the incidence, severity, and potential risk factors of symptomatic cisplatin-induced ototoxicity in a large cohort of adults with various cancer types who were treated with cisplatin without concurrent other ototoxic drugs or head radiotherapy.
Single-center (tertiary care) retrospective study in a cohort of consecutive patients, after obtaining authorization from the Geneva's Cantonal Ethics Commission for Research on Human Beings (protocol no. 2018-02065). All the analyses were performed anonymously in accordance with the Declaration of Helsinki, thus no consent was needed in agreement with the Ethics Committee. The comprehensive literature review on cisplatin-induced ototoxicity (Table 1) was conducted in MEDLINE, with the keywords ototoxicity, cisplatin, platinum, and hearing loss, until May 2023. We selected representative prospective and retrospective studies in adults treated with cisplatin-based regimens that incorporated baseline audiometry before the treatment, in English language.
Patients above 18 years of age, with baseline audiometric examination and treated with at least one dose of cisplatin-based chemotherapy between January 2015 and January 2019 at the Geneva University Hospitals, were included. Exclusion criteria included pre-existing bilateral cophosis, bilateral ear pathology not compatible with accurate hearing measurement, disease of the central auditory pathways, concomitant ototoxic drug therapy (such as aminoglycosides, deferoxamine, carboplatin, cyclophosphamide), concomitant inner ear radiotherapy, and chronic renal insufficiency. The medical files were analyzed for disease and treatment-specific data, pre-existing and concurrent risk factors including age, sex, smoking, hypertension, diabetes, dyslipidemia, and cumulative cisplatin dose. Cisplatin was either administrated alone or in combination with etoposide phosphate, gemcitabine, bleomycin, pemetrexed, docetaxel, cetuximab, fluorouracil, vinorelbine, ifosfamide, paclitaxel, cytarabine, mitomycin, rituximab, bevacizumab, methotrexate, vinblastine, doxorubicin, dacarbazine, and interferon-α (the most prevalent regimens are presented in Table 3). Cisplatin chemotherapy was flanked in every case with intravenous administration of dexamethasone (mostly 12 mg) for anti-emetic purposes.
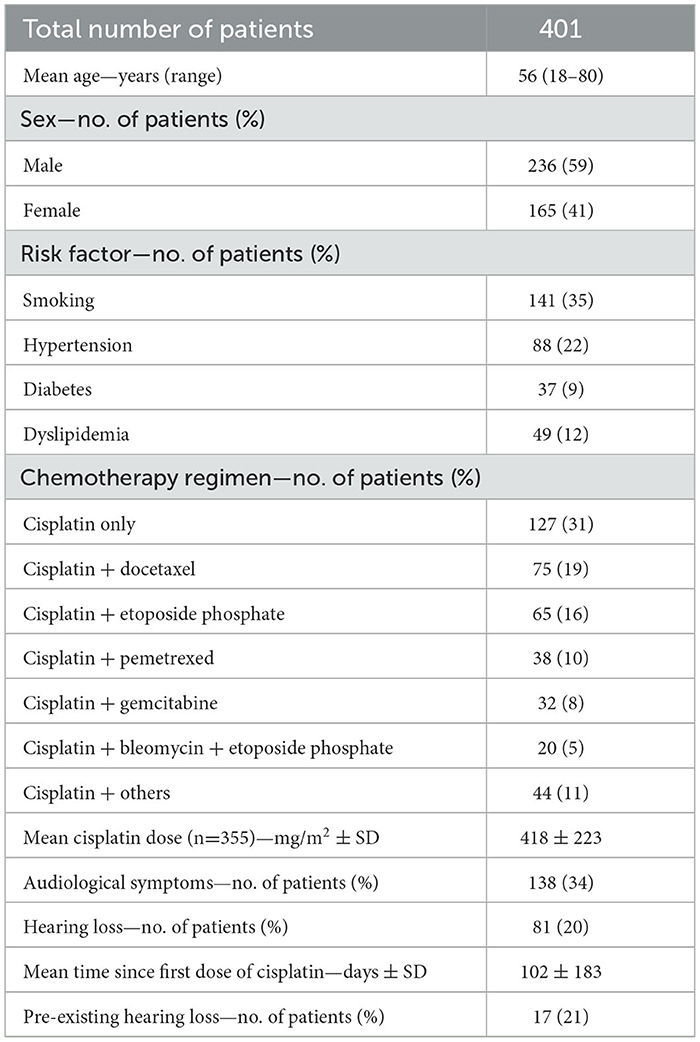
Table 3. Demographic and clinical characteristics of the patients.
An examination by an otolaryngologist followed by a tonal audiometry with a frequency range from 0.125 to 8 kHz (Equinox 2.0, Interacoustics, in a soundproof booth) by a trained audiometrist were performed in every case before the onset of the chemotherapy. Speech audiometry was not routinely performed. The oncologist routinely asked patients about any audiological symptoms during the chemotherapy, meaning tinnitus and new-onset hearing loss. If the patient reported one of these two symptoms during or after the treatment, a new consultation with tonal audiometry was performed. The otolaryngologist compared the baseline and follow-up audiometric curves. For this study, the most recent audiogram was analyzed for each symptomatic patient. Significant hearing loss was defined as a threshold shift of ≥15 dB HL in any of the tested frequencies, keeping in mind that there is an experimental error of ±5 dB HL across audiograms (Flamme et al., 2014) and, as a consequence, a 10 dB HL threshold shift in any isolated tested frequencies would still be considered non-significant. We did not use previously used ototoxic hearing loss criteria because of their limitations, such as lack of objectivity and precision (Waissbluth et al., 2017).
The incidence of hearing loss and tinnitus were described as percentages. The severity of hearing loss (i.e. hearing threshold shift) was described in mean. The association between the occurrence of ototoxicity and other variables (age, mean cumulative cisplatin dose, sex, smoking habits, diabetes, hypertension, dyslipidemia, cisplatin-based chemotherapeutics regimen) was assessed with multivariate logistic regression and the association between the severity of the hearing loss and age and mean cumulative cisplatin dose was evaluated with multivariate linear regression. All employed statistical tests included two-sided analysis, and the significance level was set as α = 0.05. The data analysis for this study was generated using Stata Statistical Software: Release 17, StataCorp. 2021. College Station, TX: StataCorp LLC.
A total of 401 patients were included in the study. The cisplatin dose was available in 355 patients, and every other variable analyzed was available in 401 patients. Table 3 summarizes the pertinent patient-related data. Cisplatin was administered for 30 different types of cancers in the patient collective.
138 patients (34%) reported audiological symptoms, among them, audiometric hearing loss was found in 81 patients (20%). No difference was found regarding hearing loss occurrence and severity between the right and left ears (overlapping of 95% confidence interval). Therefore, the average of both ears for each patient was used in this analysis. In patients exhibiting hearing loss, the average threshold shift over the entire frequency spectrum was 9.5 dB HL ± 6.5, with greater involvement of the 4, 6, and 8 kHz frequencies (threshold shift 18 dB HL ± 12), as shown in Figures 1, 2. Of the 81 patients with hearing loss, their most recent audiometry available was performed after a mean of 102 days ± 183 after the first dose of cisplatin, and 17 patients (21%) had preexisting hearing impairment detected at baseline audiometry according to the WHO's definition (average hearing threshold >25 dB HL at the frequencies of 0.5, 1, 2, and 4 kHz in the better ear) (WHO, 1991). When the information was available (n = 37), hearing loss was reported to occur after the first cycle of chemotherapy in 54% of the cases and in 29% after the second cycle. Of the 81 patients with symptomatic hearing loss, 49 (60%) reported the occurrence of simultaneous tinnitus.
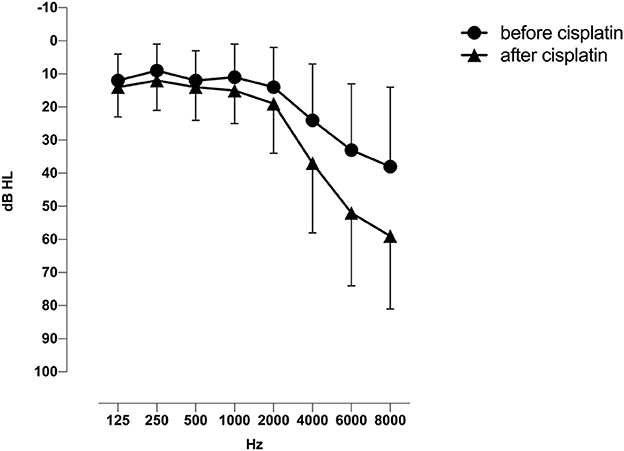
Figure 1. Mean sensorineural hearing thresholds (±1 SD) averaged for both ears, before and after cisplatin in 81 patients with symptomatic hearing loss.
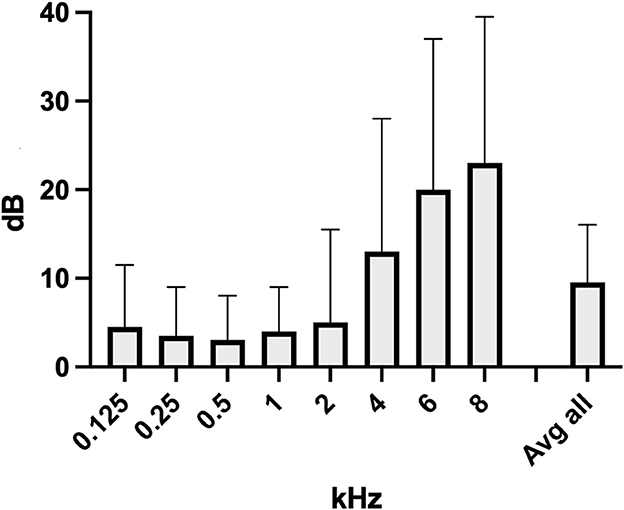
Figure 2. Mean threshold shifts (+1 SD) across frequencies, averaged for both ears, in the same 81 patients with symptomatic ototoxic hearing loss.
None of the potential risk factors was associated with a significant change in the occurrence of hearing loss. Including or removing the mean cisplatin cumulative dose variable from the multivariate logistic regression did not significantly change the odds ratios of developing hearing loss. Although there is a trend of developing more hearing loss in males than females, it did not reach statistical significance. There was no significant difference in ototoxicity occurrence in the most prevalent cisplatin-based chemotherapeutic regimens compared to cisplatin only. Details are provided in Table 4. The average hearing threshold shift in 81 patients with hearing loss was not correlated with the cumulative dose of cisplatin (adjusted r2 = 0, p = 0.18) nor the age (adjusted r2 = 0, p = 0.9).
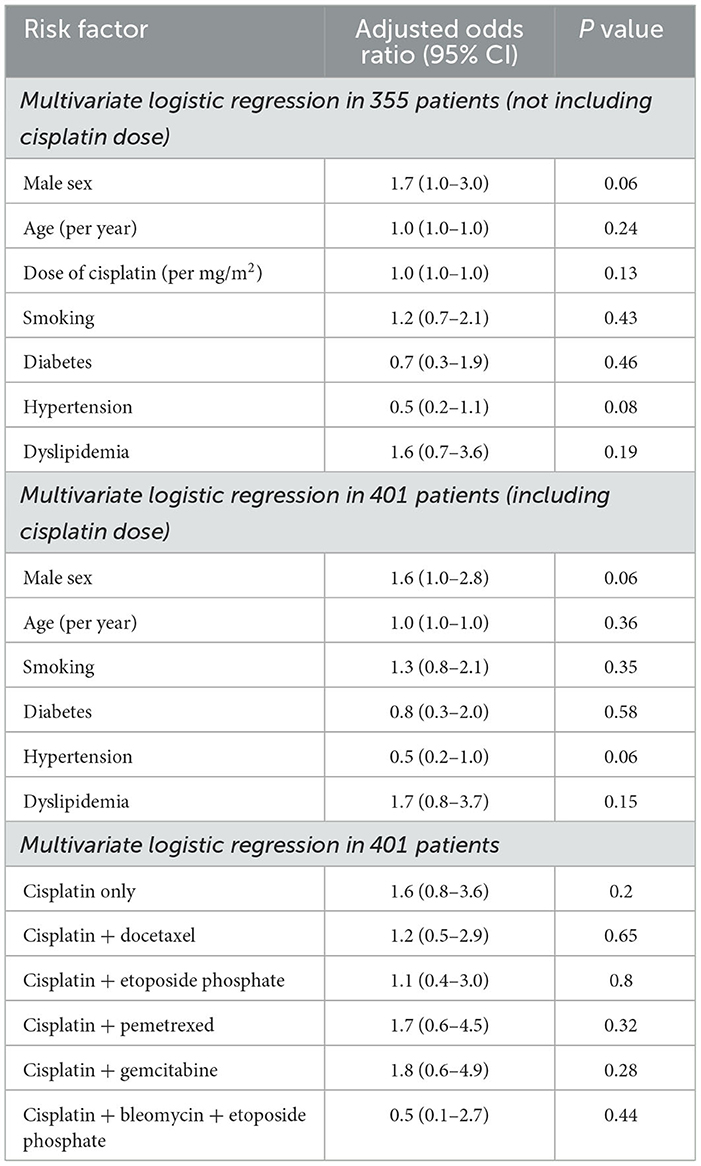
Table 4. Association of different possible risk factors and different cisplatin-based chemotherapeutic regimens with the occurrence of hearing loss.
In this cohort of 401 consecutive adult patients treated with cisplatin-based therapy flanked by intravenous application of dexamethasone, a total of 20% developed a symptomatic and audiometric hearing loss in at least one of the tested frequencies between the pretreatment baseline and the follow-up audiometry during or after the chemotherapy. A recent prospective study of 100 adults treated with cisplatin found a similar rate of symptomatic patients (20%), with a slightly higher hearing loss occurrence (28%), possibly due to the prospective nature of the analysis compared to ours (Flamme et al., 2014). Similar to the global literature, hearing loss was sensorineural, affecting both ears symmetrically and predominantly the high frequencies beyond 4 kHz (shown in Figures 1, 2) with an average threshold shift of 18 dB HL ± 12. None of the patients developed cophosis. Other large studies including baseline audiometry and no other concomitant ototoxic insults reported an occurrence of ototoxicity around 50% (Whitehorn et al., 2014; Fernandez et al., 2021). Still, their use of ototoxicity criteria with acknowledged limitations (Waissbluth et al., 2017) makes comparative analysis difficult. This is because the assessment is conducted by various means and there is no standardized criterion or accepted definition of cisplatin-induced ototoxicity in adults (Waissbluth et al., 2017). We therefore used conservative criteria of any audiometrical threshold shift ≥15 dB HL in any of the tested frequencies comparing to baseline testing. In our experience, clinical cisplatin-induced hearing loss occurrence is far from some extreme numbers reported in the literature, close to 100% (see Table 2). These numbers can be falsely alarming for the patient and the oncologist during their informative pretreatment consultation, and quantitative occurrence should be communicated with caution. We feel that the patient and the oncologist will benefit much more from clinically relevant information on symptomatic ototoxicity, rather than descriptive numbers without a clinical correlate.
Following our analysis, hearing loss primarily occurred after the first cisplatin cycle and to a lesser extent after the second, suggesting as a hypothesis a cisplatin exponential ototoxicity with a fast saturation of the ototoxic effect following the first dose. Interestingly, platinum has been found in plasma even 20 years after treatment (Gietema et al., 2000) and is indefinitely retained in cochleae of humans and mice, suggesting that cisplatin accumulation, rather than hypersensitivity, can drive the progressive hearing loss observed in a high percentage of patients (Breglio et al., 2017).
The reported hearing loss occurrence and severity were not associated with the cumulative dose. However, several articles reported a correlation between hearing loss and the cumulative cisplatin dose, commonly accepted in daily practice (Dutta et al., 2005; Arora et al., 2009; Frisina et al., 2016; Monfared et al., 2017; Okada and Kitagawa, 2023). We can hypothesize that by adapting the dose or changing the molecule (e.g., carboplatin instead of cisplatin) at the first occurrence of hearing loss, one's may diminish the occurrence and severity of ototoxicity in our cohort, compared to others in alternative care centers. At least, in our tertiary hospital, the multidisciplinary approach foresees discussing the treatment regimen at first sight of ototoxic hearing loss for every patient.
The different cisplatin-based regimens did not influence the occurrence of ototoxicity, suggesting that cisplatin is the principal accountant of toxicity, without potentiation. Each treatment was accompanied by the adjuvant administration of dexamethasone, which, besides its anti-emetic properties against chemotherapy-induced nausea and vomiting (Hesketh et al., 2020), possesses an anti-inflammatory effect, with no ototoxicity. None of the analyzed medical cofactors was associated with the occurrence of hearing loss. Cardiovascular comorbidities did not seem to precipitate cochlear damage, as could have been expected (Madhan et al., 2023; Saba et al., 2023; Sanchez et al., 2023b), considering that the inner ear is a sensitive organ with terminal vascularity and, therefore, vulnerable to ischemia (Tabuchi et al., 2002; Mom et al., 2005; Gyo, 2013). This may be due to a too small side-effect. Albeit there is a tendency for increased hearing loss occurrence in males, it did not reach statistical significance. The literature about comorbidities predisposing to ototoxicity remains non-conclusive today.
Another essential finding was the high prevalence of tinnitus (60%) in patients with symptomatic audiometric hearing loss. Tinnitus may be an indicator of hidden hearing loss (Song et al., 2021), and other studies reported an association with cisplatin ototoxicity at various rates (Piel et al., 1974; Frisina et al., 2016; Niemensivu et al., 2016; Monfared et al., 2017; Okada and Kitagawa, 2023; Sanchez et al., 2023a). Therefore, when new-onset tinnitus develops during the course of the chemotherapy, it may be an early sign of hearing damage and a complete audiometric evaluation should follow. If mild and oligosymptomatic hearing loss, the treatment should be thoroughly discussed between the patient, the otolaryngologist, and the oncologist. Either the therapy is continued with an equivalent or lower dose, or modified with a lesser ototoxic compound (e.g., carboplatin). If severe hearing loss is acknowledged, this discussion needs to be held similarly, but strongly highlighting the eventual modification or even cessation of the chemotherapy, if the oncological evolution and overall medical context allow it.
Hearing rehabilitation must be discussed with the patient if symptomatic hearing loss persists beyond the oncological phase. In Switzerland, hearing aids are proposed if the total hearing loss is calculated ≥20% using the classification of Council on Physical Therapy, American Medical Association (CPT-AMA) (Council on Physical Therapy, 1972). Should hearing aids be insufficient—especially for speech recognition—cochlear implants can be proposed, particularly in the cases of partial deafness with preserved hearing in the low frequencies and complete deafness in the frequencies >2 kHz (Roland et al., 2018). In our cohort, none of the patients developed severe or profound hearing loss (e.g., previous moderate hearing loss precipitated by ototoxicity), and none required cochlear implantation. This is reassuring regarding the maximal severity expected in cisplatin-induced hearing loss.
Ototoxic inner ear damage may occur simultaneously or sequentially with other progressive hearing loss etiologies such as presbycusis or genetic preconditions (Joo et al., 2019). In our cohort, 21% of the patients with ototoxic hearing loss had preexisting hearing impairment to some degree, according to the WHO's definition (WHO, 1991). This highlights the need for a thorough audiological baseline examination in every patient before the onset of cisplatin or any other ototoxic chemotherapy, a practice that is still not ubiquitously adopted today (Weiss et al., 2018; Chattaraj et al., 2023).
This study has limitations. First, although baseline audiological examination is performed in our institution, the present analysis will likely underestimate the true incidence and severity of cisplatin-induced hearing loss. Partly because of its retrospective nature, but also because auditory follow-up examinations were conducted only in patients reporting tinnitus or hearing loss spontaneously or after being asked explicitly by their oncologist. For this reason, patients without auto-reported hearing-related symptoms—often not a priority on health agenda compared to other cancer-related morbidities—may not have been included in the analysis, and their hearing loss remained undetected. In a similar fashion, a deterioration of hearing in the high-frequency range could probably not be self-recognized by many patients. Other studies with a prospective enrollment of cancer patients following strict audiological workup protocols corroborate this hypothesis. Those studies reported a much higher ototoxicity occurrence, reaching up to 64%, depending on the hearing loss criteria (Helson et al., 1978; Aguilar-Markulis et al., 1981; Reddel et al., 1982; Schultz et al., 2009). Furthermore, centers performing additional extended high-frequency audiometry (up to 20 kHz) reported a higher occurrence of cisplatin ototoxicity than centers with the standard audiometric testing (up to 8 kHz), as used in the present study (Zuur et al., 2008; Arora et al., 2009). Additionally, once ototoxicity or some other side effects developed, some patients benefited from a change of regimen for carboplatin instead of the ongoing cisplatin. This study did not include audiometric analyses starting from this point to avoid bias. Therefore, the severity of the cisplatin-induced hearing loss may have been underestimated.
On the other hand, the patients may benefit from being informed about the risk of potential symptoms, rather than purely descriptive subclinical damages, like neuropathy and renal insufficiency. The present study has the advantage of providing pragmatic risk quantification of developing hearing loss based on a rather large cohort of patients. Moreover, the chosen hearing loss criteria were conservative and objective (compared to baseline), applied to symptomatic patients only, making the occurrence and severity reported clinically relevant. Additionally, one out of ten patients developed audiological symptoms (such as tinnitus or subjective hearing loss) during the treatment without audiometric change. This information can help reassure the patient and the oncologist during the treatment phase if no threshold change is found in the audiogram. However, a patient complaining of hearing difficulties in noisy environments, although with a normal audiogram, may have developed hidden hearing loss. The latter is a subtle sign of early damage to the hearing, especially in high frequencies (Song et al., 2021), reflecting cochlear synaptopathy or neuropathy, for which diagnostic tools are yet to be validated (Kohrman et al., 2020; Valderrama et al., 2022). Nevertheless, speech audiometry (in silence and in noise) and extended high-frequency tonal audiometry (up to 20 kHz) may reveal hearing damage in symptomatic patients with normal standard audiometry (Frisina and Frisina, 1997; Song et al., 2021). Similarly to the early loss of ribbon synapses (the highly specialized inner hair cells' tonic synapses) in age-, noise-, and aminoglycoside-induced hearing loss in animal models (Liu et al., 2013; Kujawa and Liberman, 2015; Xiong et al., 2020), cisplatin-induced synaptopathy may occur in humans as well. Indeed, the auditory synapse has been found to be the most vulnerable part of the cochlea regarding cisplatin ototoxicity in mice (Nacher-Soler et al., 2022).
This extensive retrospective analysis of consecutive cancer patients treated with cisplatin-based chemotherapy showed symptomatic hearing loss in 20% of the cases, adding morbidity to this already suffering population (Phillips et al., 2023). Therefore, preventing ototoxic hearing loss through molecular or pharmacological intervention would interest thousands of patients worldwide. To this end, our and many other institutions currently undertake translational research projects aiming at otoprotection by different methods (Rousset et al., 2015; Waissbluth et al., 2017; Nacher-Soler et al., 2022). We believe that a strong collaboration between clinicians and basic scientists will significantly increase the chances of developing an effective preventive therapy against cisplatin ototoxicity in the future, tailored to the patient's need and with a meaningful mode of application for otologists.
At least 1 out of 5 patients treated with cisplatin developed audiological symptoms correlated with audiometric hearing loss within the 0.125–8 kHz range, for which new-onset tinnitus is a sensitive symptom. Not all audiological symptoms are accompanied by audiometric change. No predisposing factor could be identified. To improve early detection, the systematic application of a thorough audiological examination before, during, and after the completion of cisplatin chemotherapy is mandatory. Early detection of ototoxic hearing loss is a prerequisite for a multidisciplinary discussion and a potential modification of the treatment regimen to maximize anticancer action while minimizing morbidity for each patient. In addition, pragmatic clinical data lays a sound base for imminent clinical trials aiming to prevent cisplatin-induced ototoxicity.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The study involving humans was approved by Geneva's Cantonal Ethics Commission for Research on Human Beings. The study was conducted in accordance with the local legislation and institutional requirements. The Ethics Committee/Institutional Review Board waived the requirement of written informed consent for participation from the participants or the participants' legal guardians/next of kin because all the analyses were performed anonymously in a retrospective manner, in accordance with the Declaration of Helsinki, thus no consent was needed in agreement with the Ethics Committee.
FV contributed to conception and design of the study, collection of data, statistical analyses, and original draft preparation. AV, DM, GN-S, FR, and TD contributed to writing sections of the manuscript. PS contributed to conception and design of the study and writing and editing. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Aguilar-Markulis, N. V., Beckley, S., Priore, R., and Mettlin, C. (1981). Auditory toxicity effects of long-term cis-dichlorodiammineplatinum II therapy in genitourinary cancer patients. J. Surg. Oncol. 16, 111–123. doi: 10.1002/jso.2930160203
Ariano, R. E., Zelenitsky, S. A., and Kassum, D. A. (2008). Aminoglycoside-induced vestibular injury: maintaining a sense of balance. Ann. Pharmacother. 42, 1282–1289. doi: 10.1345/aph.1L001
Arnold, M., Rutherford, M. J., Bardot, A., Ferlay, J., Andersson, T. M-L., Myklebust, T. Å., et al. (2019). Progress in cancer survival, mortality, and incidence in seven high-income countries 1995-2014 (ICBP SURVMARK-2): a population-based study. Lancet Oncol. 20, 1493–1505. doi: 10.1016/S1470-2045(19)30456-5
Arora, R., Thakur, J. S., Azad, R. K., Mohindroo, N. K., Sharma, D. R., and Seam, R. K. (2009). Cisplatin-based chemotherapy: add high-frequency audiometry in the regimen. Indian J. Cancer 46, 311–317. doi: 10.4103/0019-509X.55551
ASHA (1994). Guidelines for the audiologic management of individuals receiving cochleotoxic drug therapy. ASHA 36 (Suppl. 12), 11–19.
Bajorin, D. F., Bosl, G. J., Alcock, N. W., Niedzwiecki, D., Gallina, E., and Shurgot, B. (1986). Pharmacokinetics of cis-diamminedichloroplatinum(II) after administration in hypertonic saline. Cancer Res. 46, 5969–5972.
Breglio, A. M., Rusheen, A. E., Shide, E. D., Fernandez, K. A., Spielbauer, K. K., McLachlin, K. M., et al. (2017). Cisplatin is retained in the cochlea indefinitely following chemotherapy. Nat. Commun. 8, 1654. doi: 10.1038/s41467-017-01837-1
Brock, P. R., Bellman, S. C., Yeomans, E. C., Pinkerton, C., and Pritchard, J. (1991). Cisplatin ototoxicity in children: a practical grading system. Med. Pediatr. Oncol. 19, 295–300. doi: 10.1002/mpo.2950190415
Brummett, R. E., and Fox, K. E. (1989). Aminoglycoside-induced hearing loss in humans. Antimicrob. Agents Chemother. 33, 797–800. doi: 10.1128/AAC.33.6.797
Bruniera, F. R., Ferreira, F. M., Saviolli, L. R. M., Bacci, M. R., Feder, D., Pedreira, M., et al. (2015). The use of vancomycin with its therapeutic and adverse effects: a review. Eur. Rev. Med. Pharmacol. Sci. 19, 694–700.
Cazals, Y. (2000). Auditory sensori-neural alterations induced by salicylate. Prog. Neurobiol. 62, 583–631. doi: 10.1016/S0301-0082(00)00027-7
Chattaraj, A., Syed, M. P., Low, C. A., and Owonikoko, T. K. (2023). Cisplatin-induced ototoxicity: a concise review of the burden, prevention, interception strategies. JCO Oncol Pract 19, 278–283. doi: 10.1200/OP.22.00710
Cuffel, C., and Guyot, J. P. (2013). Aspirin ototoxicity: a rare situation today. Rev. Med. Suisse 9, 1785–1788.
Cummings, C. W. (1968). Experimental observations on the ototoxicity of nitrogen mustard. Laryngoscope 78, 530–538. doi: 10.1288/00005537-196804000-00004
Curhan, S. G, Eavey, R, Shargorodsky, J, Curhan, G. C. (2010). Analgesic use and the risk of hearing loss in men. Am. J. Med. 123, 231–237. doi: 10.1016/j.amjmed.2009.08.006
Dasari, S., and Tchounwou, P. B. (2014). Cisplatin in cancer therapy: molecular mechanisms of action. Eur. J. Pharmacol. 740, 364–378. doi: 10.1016/j.ejphar.2014.07.025
Dell'Aringa, A. H. B., Isaac, M. L., Arruda, G. V., Esteves, M. C. B. N., Dell'aringa, A. R., Júnior, J. L. S., et al. (2009). Audiological findings in patients treated with radio- and concomitant chemotherapy for head and neck tumors. Radiat. Oncol. 4, 53. doi: 10.1186/1748-717X-4-53
Di Maio, M., Gallo, C., Leighl, N. B., Piccirillo, M. C., Daniele, G., Nuzzo, F., et al. (2015). Symptomatic toxicities experienced during anticancer treatment: agreement between patient and physician reporting in three randomized trials. J. Clin. Oncol. 33, 910–915. doi: 10.1200/JCO.2014.57.9334
Dutta, A., Venkatesh, M. D., and Kashyap, R. C. (2005). Study of the effects of chemotherapy on auditory function. Indian J. Otolaryngol. Head Neck Surg. 57, 226–228. doi: 10.1007/BF03008019
Fernandez, K. A., Allen, P., Campbell, M., Page, B., Townes, T., Li, C-M., et al. (2021). Atorvastatin is associated with reduced cisplatin-induced hearing loss. J. Clin. Invest. 131, JCI142616. doi: 10.1172/JCI142616
Flamme, G. A., Stephenson, M. R., Deiters, K. K., Hessenauer, A., VanGessel, D. K., Geda, K., et al. (2014). Short-term variability of pure-tone thresholds obtained with TDH-39P earphones. Int. J. Audiol. 53 Suppl 2, S5–15. doi: 10.3109/14992027.2013.857435
Formann, E., Stauber, R., Denk, D-M., Jessner, W., Zollner, G., Munda-Steindl, P., et al. (2004). Sudden hearing loss in patients with chronic hepatitis C treated with pegylated interferon/ribavirin. Am. J. Gastroenterol. 99, 873–877. doi: 10.1111/j.1572-0241.2004.30372.x
Frisina, D. R., and Frisina, R. D. (1997). Speech recognition in noise and presbycusis: relations to possible neural mechanisms. Hear. Res. 106, 95–104. doi: 10.1016/S0378-5955(97)00006-3
Frisina, R. D., Wheeler, H. E., Fossa, S. D., Kerns, S. L., Fung, C., Sesso, H. D., et al. (2016). Comprehensive audiometric analysis of hearing impairment and tinnitus after cisplatin-based chemotherapy in survivors of adult-onset cancer. J. Clin. Oncol. 34, 2712–2720. doi: 10.1200/JCO.2016.66.8822
Gietema, J. A., Meinardi, M. T., Messerschmidt, J., Gelevert, T., Alt, F., Uges, D. R., et al. (2000). Circulating plasma platinum more than 10 years after cisplatin treatment for testicular cancer. Lancet 355, 1075–1076. doi: 10.1016/S0140-6736(00)02044-4
Greene, J. B., Standring, R., Siddiqui, F., and Ahsan, S. (2015). Incidence of cisplatin induced ototoxicity in adults with head and neck cancer. Adv. Otolaryngol. 2015, 4. doi: 10.1155/2015/245613
Gyo, K. (2013). Experimental study of transient cochlear ischemia as a cause of sudden deafness. World J. Otorhinolaryngol. 3, 1–15. doi: 10.5319/wjo.v3.i1.1
Helson, L., Okonkwo, E., Anton, L., and Cvitkovic, E. (1978). cis-Platinum ototoxicity. Clin. Toxicol. 13, 469–478. doi: 10.3109/15563657808988252
Hesketh, P. J., Kris, M. G., Basch, E., Bohlke, K., Barbour, S. Y., Clark-Snow, R. A., et al. (2020). Antiemetics: ASCO guideline update. J. Clin. Oncol. 38, 2782–2797. doi: 10.1200/JCO.20.01296
Hultcrantz, M., Simonoska, R., and Stenberg, A. E. (2006). Estrogen and hearing: a summary of recent investigations. Acta Otolaryngol. 126, 10–14. doi: 10.1080/00016480510038617
Ikeda, A. K, Prince, A. A, Chen, J. X, Lieu, J. E. C, and Shin, J. J. (2018). Macrolide-associated sensorineural hearing loss: a systematic review. Laryngoscope 128, 228–236. doi: 10.1002/lary.26799
Institute NC (2017). Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0. Available online at: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf
Isherwood, B., Goncalves, A. C., Cousins, R., and Holme, F. (2022). The global hearing therapeutic pipeline. Drug Discov. Today 27, 912–922. doi: 10.1016/j.drudis.2021.11.009
Jereczek-Fossa, B. A., Zarowski, A., Milani, F., and Orecchia, R. (2003). Radiotherapy-induced ear toxicity. Cancer Treat. Rev. 29, 417–430. doi: 10.1016/S0305-7372(03)00066-5
Johnson, L. A., Morgan, R. A., Dudley, M. E., Cassard, L., Yang, J. C., Hughes, M. S., et al. (2009). Gene therapy with human and mouse T-cell receptors mediates cancer regression and targets normal tissues expressing cognate antigen. Blood 114, 535–546. doi: 10.1182/blood-2009-03-211714
Joo, Y., Cruickshanks, K. J., Klein, B. E. K., Klein, R., Hong, O., and Wallhagen, M. I. (2019). The contribution of ototoxic medications to hearing loss among older adults. J. Gerontol. A. Biol. Sci. Med. Sci. 75, 561–566. doi: 10.1093/gerona/glz166
Jourde-Chiche, N., Mancini, J., Dagher, N., Taugourdeau, S., Thomas, G., Brunet, C., et al. (2012). Antimalarial ototoxicity: an underdiagnosed complication? A study of spontaneous reports to the French Pharmacovigilance Network. Ann Rheum. Dis. 71, 1586. doi: 10.1136/annrheumdis-2011-201265
Kelland, L. (2007). The resurgence of platinum-based cancer chemotherapy. Nat. Rev. Cancer 7, 573–584. doi: 10.1038/nrc2167
Khan, A. S., Sheikh, Z., Khan, S., Dwivedi, R., and Benjamin, E. (2011). Viagra deafness–sensorineural hearing loss and phosphodiesterase-5 inhibitors. Laryngoscope 121, 1049–1054. doi: 10.1002/lary.21450
Kohrman, D. C., Wan, G., Cassinotti, L., and Corfas, G. (2020). Hidden hearing loss: a disorder with multiple etiologies and mechanisms. Cold Spring Harb. Perspect. Med. 10, a035493. doi: 10.1101/cshperspect.a035493
Kujawa, S. G., and Liberman, M. C. (2015). Synaptopathy in the noise-exposed and aging cochlea: Primary neural degeneration in acquired sensorineural hearing loss. Hear Res. 330, 191–9. doi: 10.1016/j.heares.2015.02.009
Liu, K., Jiang, X., Shi, C., Shi, L., Yang, B., Shi, L., et al. (2013). Cochlear inner hair cell ribbon synapse is the primary target of ototoxic aminoglycoside stimuli. Mol. Neurobiol. 48, 647–654. doi: 10.1007/s12035-013-8454-2
Low, W. K., Toh, S. T., Wee, J., Fook-Chong, S. M. C., and Wang, D. Y. (2006). Sensorineural hearing loss after radiotherapy and chemoradiotherapy: a single, blinded, randomized study. J. Clin. Oncol. 24, 1904–1909. doi: 10.1200/JCO.2005.05.0096
Madhan, S., Rao, R. B. S., Parameshwarappa, A., Basavaraj, B. M., Ganesh, P. B., Shetty, S., et al. (2023). Evaluation of the effects of dyslipidemia on hearing in patients with type 2 diabetes mellitus. Indian J. Otolaryngol. Head Neck Surg. 75, 541–547. doi: 10.1007/s12070-023-03626-3
Malgonde, M. S., Nagpure, P. S., and Kumar, M. (2015). Audiometric patterns in ototoxicity after radiotherapy and chemotherapy in patients of head and neck cancers. Indian J. Palliat. Care 21, 164–167. doi: 10.4103/0973-1075.156479
Miller, K. D., Siegel, R. L., Lin, C. C., Mariatto, A. B., Yaborff, K. R., Jemal, A., et al. (2016). Cancer treatment and survivorship statistics. CA Cancer J. Clin. 66, 271–289. doi: 10.3322/caac.21349
Moellering, R. C. (1984). Pharmacokinetics of vancomycin. J. Antimicrob. Chemother. 14, 43–52. doi: 10.1093/jac/14.suppl_D.43
Mom, T., Chazal, J., Gabrillargues, J., Gillain, L., and Avan, P. (2005). Cochlear blood supply: an update on anatomy and function. Fr ORL 81, 88.
Monfared, Z. E., Khosravi, A., Naini, A. S., Radmand, G., and Khodadad, K. (2017). Analysis of cisplatin-induced ototoxicity risk factors in iranian patients with solid tumors: a cohort, prospective and single institute study. Asian Pac. J. Cancer Prev. 18, 753–758.
Mujica-Mota, M., Waissbluth, S., and Daniel, S. J. (2013). Characteristics of radiation-induced sensorineural hearing loss in head and neck cancer: a systematic review. Head Neck 35, 1662–1668. doi: 10.1002/hed.23201
Nacher-Soler, G., Marteyn, A., Barenzung, N., Sgroi, S., Krause, K-H., Senn, P., et al. (2022). Development and in vivo validation of small interfering RNAs targeting NOX3 to prevent sensorineural hearing loss. Front. Neurol. 13, 993017. doi: 10.3389/fneur.2022.993017
Nagy, J. L., Adelstein, D. J., Newman, C. W., Rybicki, L. A., Rice, T. W., and Lavertu, P. (1999). Cisplatin ototoxicity: the importance of baseline audiometry. Am. J. Clin. Oncol. 22, 305–308. doi: 10.1097/00000421-199906000-00020
Niemensivu, R., Saarilahti, K., Ylikoski, J., Aarnisalo, A., and Mäkitie, A. A. (2016). Hearing and tinnitus in head and neck cancer patients after chemoradiotherapy. Eur. Arch. Otorhinolaryngol. 273, 2509–2514. doi: 10.1007/s00405-015-3857-5
Okada, H., and Kitagawa, K. (2023). Risk factors associated with cisplatin-induced ototoxicity in Japanese patients with solid tumors. Cancer Med. 12, 7904–7910. doi: 10.1002/cam4.5565
Paken, J., Govender, C. D., Pillay, M., and Sewram, V. (2016). Cisplatin-associated ototoxicity: a review for the health professional. J. Toxicol. 2016, 1809394. doi: 10.1155/2016/1809394
Phillips, O. R., Baguley, D. M., Pearson, S. E., and Akeroyd, M. A. (2023). The long-term impacts of hearing loss, tinnitus and poor balance on the quality of life of people living with and beyond cancer after platinum-based chemotherapy: a literature review. J. Cancer Surviv. 17, 40–58. doi: 10.1007/s11764-022-01314-9
Piel, I. J., Meyer, D., Perlia, C. P., and Wolfe, V. I. (1974). Effects of cis-diamminedichloroplatinum (NSC-119875) on hearing function in man. Cancer Chemother. Rep. 58, 871–875.
Prayuenyong, P, Taylor, J. A, Pearson, S. E, Gomez, R, Patel, P. M, Hall, D. A, et al. (2018). Vestibulotoxicity associated with platinum-based chemotherapy in survivors of cancer: a scoping review. Front. Oncol. 8, 363. doi: 10.3389/fonc.2018.00363
Prayuenyong, P., Kasbekar, A. V., Hall, D. A., and Baguley, D. M. (2020). Audiovestibular clinician experiences and opinions about cisplatin vestibulotoxicity. Eur. Arch. Otorhinolaryngol. 277, 3283–3293. doi: 10.1007/s00405-020-06033-4
Reddel, R. R., Kefford, R. F., Grant, J. M., Coates, A. S., Fox, R. M., and Tattersall, M. H. (1982). Ototoxicity in patients receiving cisplatin: importance of dose and method of drug administration. Cancer Treat. Rep. 66, 19–23.
Roland, J. T., Gantz, B. J., Waltzman, S. B., and Parkinson, A. J. (2018). Long-term outcomes of cochlear implantation in patients with high-frequency hearing loss. Laryngoscope 128, 1939–1945. doi: 10.1002/lary.27073
Rosner, S, Agrawal, Y, Sun, D. Q, Aygun, N, Schollenberger, M. D, and Lipson, E, et al. (2020). Immune-mediated ototoxicity associated with immune checkpoint inhibitors in patients with melanoma. J. Immunother. Cancer 8, 1675. doi: 10.1136/jitc-2020-001675
Rousset, F., Carnesecchi, S., Senn, P., and Krause, K-H. (2015). Nox3-targeted therapies for inner ear pathologies. Curr. Pharm. Des. 21, 5977–5987. doi: 10.2174/1381612821666151029112421
Rybak, L. P. (1993). Ototoxicity of loop diuretics. Otolaryngol. Clin. North Am. 26, 829–844. doi: 10.1016/S0030-6665(20)30770-2
Saba, E. S., Swisher, A. R., Ansari, G. N., and Rivero, A. (2023). Cardiovascular risk factors in patients with sudden sensorineural hearing loss: a systematic review and meta-analysis. Otolaryngol. Head Neck Surg. 168, 907–921. doi: 10.1002/ohn.163
Sanchez, V. A., Dinh, P. C., Rooker, J., Monahan, P. O., Althouse, S. K., Fung, C., et al. (2023b). Prevalence and risk factors for ototoxicity after cisplatin-based chemotherapy. J. Cancer Surviv. 17, 27–39. doi: 10.1007/s11764-022-01313-w
Sanchez, V. A., Shuey, M. M., Dinh, P. C., Monahan, P. O., Fosså, S. D., Sesso, H. D., et al. (2023a). Patient-reported functional impairment due to hearing loss and tinnitus after cisplatin-based chemotherapy. J. Clin. Oncol. 41, 2211–2226. doi: 10.1200/JCO.22.01456
Schultz, C., Goffi-Gomez, M. V. S., Liberman, P. H. P., and Carvalho, A. L. (2009). Report on hearing loss in oncology. Braz. J. Otorhinolaryngol. 75, 634–641. doi: 10.1590/S1808-86942009000500004
Seaman, B. J., Guardiani, E. A., Brewer, C. C., Zalewski, C. K., King, K. A., Rudy, S., et al. (2012). Audiovestibular dysfunction associated with adoptive cell immunotherapy for melanoma. Otolaryngol. Head Neck Surg. 147, 744–749. doi: 10.1177/0194599812448356
Sheth, S., Mukherjea, D., Rybak, L. P., and Ramkumar, V. (2017). Mechanisms of cisplatin-induced ototoxicity and otoprotection. Front. Cell. Neurosci. 11, 338. doi: 10.3389/fncel.2017.00338
Shine, N. P., and Coates, H. (2005). Systemic ototoxicity: a review. East Afr. Med. J. 82, 536–539. doi: 10.4314/eamj.v82i10.9353
Simon, M. V. (2011). Neurophysiologic intraoperative monitoring of the vestibulocochlear nerve. J. Clin. Neurophysiol. 28, 566–581. doi: 10.1097/WNP.0b013e31823da494
Song, Z., Wu, Y., Tang, D., Lu, X., Qiao, L., Wang, J., et al. (2021). Tinnitus is associated with extended high-frequency hearing loss and hidden high-frequency damage in young patients. Otol. Neurotol. 42, 377–383. doi: 10.1097/MAO.0000000000002983
Stenner, M., Stürmer, K., Beutner, D., and Klussmann, J. P. (2009). Sudden bilateral sensorineural hearing loss after intravenous cocaine injection: a case report and review of the literature. Laryngoscope 119, 2441–2443. doi: 10.1002/lary.20711
Tabuchi, K., Tsuji, S., Fujihira, K., Oikawa, K., Hara, A., and Kusakari, J. (2002). Outer hair cells functionally and structurally deteriorate during reperfusion. Hear. Res. 173, 153–163. doi: 10.1016/S0378-5955(02)00349-0
Tampio, A. J. F., Dhanireddy, S., Sivapiragasam, A., and Nicholas, B. D. (2021). Bilateral sensorineural hearing loss associated with nivolumab therapy for stage IV malignant melanoma. Ear Nose Throat. J. 100, 286S–291S. doi: 10.1177/0145561320940847
Tserga, E., Nandwani, T., Edvall, N. K., Bulla, J., Patel, P., Canlon, B., et al. (2019). The genetic vulnerability to cisplatin ototoxicity: a systematic review. Sci. Rep. 9, 3455. doi: 10.1038/s41598-019-40138-z
Tuknayat, A, Thami, G. P, Gogia, P, Bhutani, M. (2018). Cyclophosphamide-induced hearing loss: reversibility and preventive strategies. Am. J. Ther. 25, e692–e695. doi: 10.1097/MJT.0000000000000701
Valderrama, J. T., de la Torre, A., and McAlpine, D. (2022). The hunt for hidden hearing loss in humans: From preclinical studies to effective interventions. Front. Neurosci. 16, 1000304. doi: 10.3389/fnins.2022.1000304
van As, J. W., van den Berg, H., and van Dalen, E. C. (2016). Platinum-induced hearing loss after treatment for childhood cancer. Cochrane Database Syst. Rev. 2016, CD010181. doi: 10.1002/14651858.CD010181.pub2
Waissbluth, S., Peleva, E., and Daniel, S. J. (2017). Platinum-induced ototoxicity: a review of prevailing ototoxicity criteria. Eur. Arch. Otorhinolaryngol. 274, 1187–1196. doi: 10.1007/s00405-016-4117-z
Waters, G. S., Ahmad, M., Katsarkas, A., Stanimir, G., and McKay, J. (1991). Ototoxicity due to cis-diamminedichloroplatinum in the treatment of ovarian cancer: influence of dosage and schedule of administration. Ear Hear. 12, 91–102. doi: 10.1097/00003446-199104000-00003
Weiss, A., Kuonen, R., Brockmeier, H., Grotzer, M., Candreia, C., Maire, R., et al. (2018). Audiological monitoring in Swiss childhood cancer patients. Pediatr. Blood Cancer 65 doi: 10.1002/pbc.26877
Whitehorn, H., Sibanda, M., Lacerda, M., Spracklen, T., Ramma, L., Dalvie, S., et al. (2014). High prevalence of cisplatin-induced ototoxicity in Cape Town, South Africa. S. Afr. Med. J. 104, 288–291. doi: 10.7196/SAMJ.7389
WHO (1991). WHO and Report of the Informal Working Group On Prevention Of Deafness And Hearing Impairment Programme Planning. WHO: Geneva.
WHO (2021). WHO Model List of Essential Medicines, 22nd List (2021). Available online at: https://www.who.int/groups/expert-committee-on-selection-and-use-of-essential-medicines/essential-medicines-lists
WHO (2022). WHO Fact Sheets–Cancer. Available online at: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed 9 June, 2023.
Xiong, W., Yu, S., Liu, K., and Gong, S. (2020). Loss of cochlear ribbon synapses in the early stage of aging causes initial hearing impairment. Am. J. Transl. Res. 12, 7354–7366.
Yanfang Dong, L. Z., Tian, Q., Zheng, Y., and Sanche, L. (2017). Chemoradiation cancer therapy: molecular mechanisms of cisplatin radiosensitization. J. Phys. Chem. C. 121, 17505–17513. doi: 10.1021/acs.jpcc.7b05271
Keywords: cisplatin, platinum, ototoxicity, hearing loss, tinnitus, cancer, sensorineural hearing loss, chemotherapy
Citation: Voruz F, Vuilleumier A, Migliorini D, Nacher-Soler G, Rousset F, De Maesschalck T and Senn P (2023) Incidence of cisplatin-induced ototoxicity in adult cancer patients based on audiometric confirmation of patient self-report. Front. Audiol. Otol. 1:1239119. doi: 10.3389/fauot.2023.1239119
Received: 12 June 2023; Accepted: 23 August 2023;
Published: 20 September 2023.
Edited by:
Tobias Kleinjung, University of Zurich, SwitzerlandReviewed by:
Agnieszka J. Szczepek, Charité University Medicine Berlin, GermanyCopyright © 2023 Voruz, Vuilleumier, Migliorini, Nacher-Soler, Rousset, De Maesschalck and Senn. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: François Voruz, ZnJhbmNvaXMudm9ydXpAaGlzcGVlZC5jaA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.