
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Artif. Intell. , 28 February 2023
Sec. Medicine and Public Health
Volume 6 - 2023 | https://doi.org/10.3389/frai.2023.985469
 James Andrew Henry1,2,3*
James Andrew Henry1,2,3*Introduction: Technologies abstract intelligence and provide predictor and precision insight in workflows that manage disorders, similar to cardiology and hematological disease. Positive perceptions of Artificial Intelligence (AI) that support Machine Learning (ML) and Deep Learning (DL) manage transformations with a safe system that improves wellbeing. In sections, workflow introduces an eXamination (X = AI) as an end-to-end structure to culture workstreams in a step-by-step design to manage populace health in a governed system.
Method: To better healthcare outcomes, communities and personnel benefit from an explanation and an interpretive that elucidates workflow for citizens or practitioners to comprehend personalized platforms. Therefore, the author undertook structure and practice reviews and appraised perspectives that impact the management of AI in public health and medicine.
Results: Figures for the management of AI workflow illustrate and inform on the model, structure, culture, assurance, process steps, values, and governance required for abstract insights in public health and medicine. The papers' end-to-end structure with explanans in a work culture interprets the step-by-step designs that manage the success of AI. Personalized care graphics offer an explanandum in the management of biological analytic value.
Discussion: Healthcare leadership collaboratives plan population health with an upstream, workplace and workstream format. Secure workflow and safety wellbeing system requirements prove that genomics and AI improve medicine. Therefore, the paper discusses group understanding of current practice, ethics, policy, and legality.
Conclusion: “Culture, intelligent workflow, structure, and steps” improve wellbeing with personalized care and align a percept for national opportunities, regional control, and local needs. Personalized practice cultures support analytic systems to describe, predict, precision, and prescript medicine in population health management eXaminations.
An intro to workflow provides personalized solutions for global health management. Background to the eXamination concept in medical examinations develops AI across all healthcare sector operations in a series of papers that govern through international standard developments. The system prelude and the paper provide an explanation and interpretive of AI while elucidating future insights into Population Health Management for opinions.
AI projects and programs like cardio with coagulum, patient blood management, elderly comorbid care, and newborn screening benefit from Population Health Management. As illustrated throughout the manuscript, workflow delivers upstream data for workplace ML and DL eXaminations that workstream medical solutions (Figure 1). Real-time or batch quality data for insight delivered in practice with healthcare AI governance have ML and DL in the eXamination process and its safety management system. Personalized system practice evolves in a series of papers titled; -
1. Atrial Fibrillation the Genomics Mission
2. Culture Intelligent Workflow, Structure, and Steps
3. Population Health Management Standard eXaminations
4. Personalized System Practice and Group Determinants
5. Personalized System Practice—eXamination Transformation
6. Personalized System Practice—eXamination Improvement
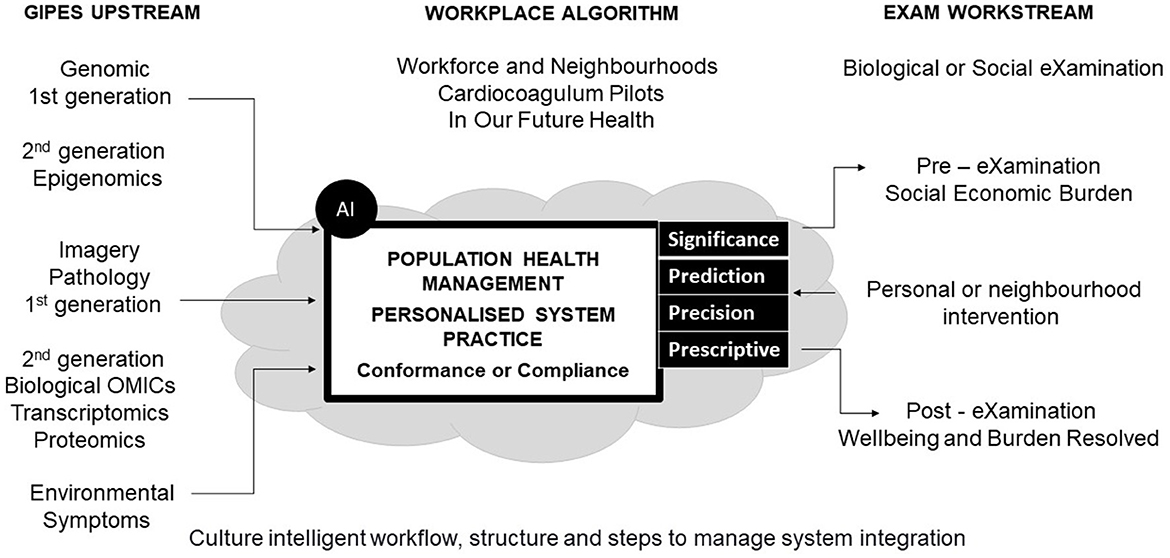
Figure 1. Model workflow.
The World Health Organization supports data-driven services in healthcare for “early detection, diagnosis, and medical decision making,” as the future of Population Health Management (PHM) engages practitioner and citizen users on a global scale (Wiegand et al., 2019). The US introduced the Genomics and Personalized Medicine Act, which called for the study of barriers to implementing personalized medicine, impacting government rethinks on AI (Margetts and Dorobantu, 2019).
A forward-thinking Australian federal state with public funds integrated a flexible and adaptable genomic system-wide approach to medicine. Whilst successful, the lessons learned included budgeting reviews and, most notably, insight on oversight (Vidgen et al., 2021).
The UK Health and Care Bill empowers the secretary of state for health and social care to capitalize on digital and genomic innovations and engage the British Medical Association with digital Life Sciences in PHM (Iacobucci, 2021).
Governments build back better with value and principles to integrate datasets on digital channels, wherein oversight on workflow co-ordinates a central role for diagnostics with informatic core purpose to reduce socio-economic burdens (Minkman, 2016; Boehme et al., 2021).
If not remedy for other countries, the UK resolves variance with a public health approach to workflow with a digital guide to “What Good Looks Like” (Public Health England, 2019). Principles in action seek to enable workflow eXaminations to become the norm to predict health and precision care (Public Health England, 2019).
Globally, responsible genomic data sharing for human health benefits requires not only policy-framing but setting of technical standards (Knoppers, 2014). The UK Multi-Agency Advice Service provides a regulatory collaborative approach for developer or adopter of phenomics to deliver a life sciences vision for clinical research and genomics at scale for wellbeing [International Organization for Standardization (ISO), 2018a]. International workflows organize to sustain system biology success in practice, as digital maturity commences with a standard for self-assessment (NHS, 2022a). PHM at the point of care executes workflow competence through a system standard common to genomics, image, and pathology laboratories [International Organization for Standardization (ISO), 2012]. To build a digital data strategy with intelligence norms integrate upstream, workplace and workstreams to realize personalized biological eXaminations that impact socioeconomic success [International Organization for Standardization (ISO), 2017, Figure 1].
In 2014, the Barnes report recommended that pathology quality systems integrate hospital trust governance to reduce variable adversities (Pathology Quality Assurance Review [Internet], 2014), similar to cardiology or hematology diagnostics that impact clinical decisions. In 2017, the author presented an abstract at a UK national assurance conference for a Patient Blood Management Quality System proposal which summarized the need for life science intercepts (Henry, 2017).
In 2019, the US Society for Advanced Blood Management presented an abstract on an atrial fibrillation (cardio) related coagulation (coagulum) in genomic futures, as the author framed cardiocoagulum champions (Henry, 2019). Further analysis of cardiocoagulum socioeconomic risks, predictive health, and precision care opportune a genomic mission for our industrial lives with workflow for PHM in Future Health (Our Future Health, 2021).
Today, the UK genomic strategy for end-to-end delivery of research, preventative and precision pillars build on data-driven themes (GENOME UK, 2020). Digital AI strategy support regional analytic study designs for long-term citizen needs (GOV.UK, 2021a), with workplace and homeplace delivery proposals for personalized eXaminations.
In moving forward, Integrated Care Systems (ICS) bring medical debate on AI clinical studies that secure data flow for safe PHM (Shelmerdine et al., 2021). Citizens' needs, assessed with genomics, build model ontology foundations in an end-to-end structure that engage and operate for communities as ICS boards precision medicine (Aronson and Rehm, 2015).
Workflow designs shows health provider or communes that populace health can be managed with upstream features for workplace intelligence that workstream eXaminations which intercept biological and socio-economic burdens (Figure 1). Shaping digital futures on Biological Ontology Models across a Model Hospital that includes social care requires workflow comprehension and function to get the best out of AI (Hardie et al., 2021; Maguire et al., 2021). Planning with our communities and presenting algorithm assurance enhance health cultures as alliances bring end-to-end structures with delivery of core eXaminations for accurate support decisions (Department of Health and Social Care Public Health England, 2020; NHS England, 2020a).
Predictive health and precision care reduce the frequency of harm to wellbeing with an upstream of biological data, similar to features for Genomic variations, tissue Images, and Pathology diagnostics [GIP] data. Cardiocoagulum pre-eXamination inputs nucleotide informatics, with or without other informatics, to personalize health with a population health management requirement (Table 1).
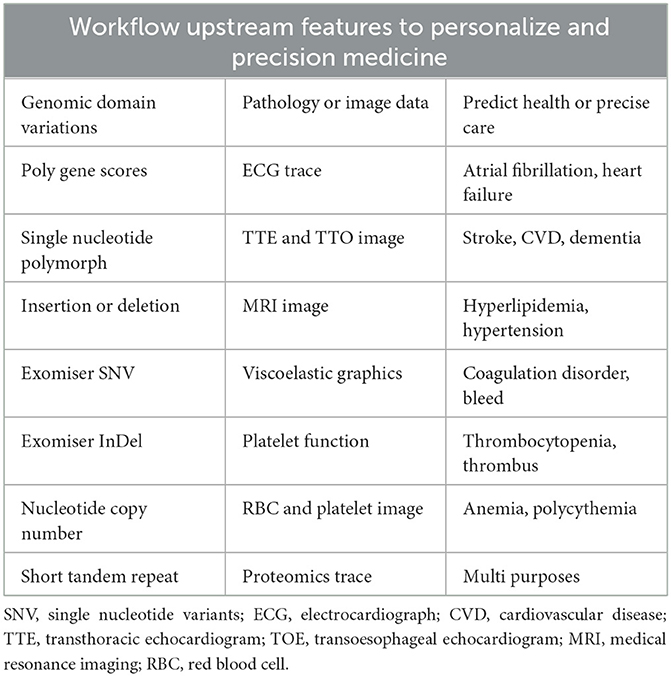
Table 1. Cardiocoagulum table.
The cardiocoagulum table informs on the potential for genomic domains to weight pathology or image data, evaluate the current clinical significance, or report on the predictive health value. The input of cardiocoagulum quality data will improve precision care intercepts for cardiovascular and hematological-related disorders. P of GIPES, input pathology, and phenomics informatics as life science integrates image-proteomics for multiple medical purposes (Table 1).
Both environment and symptomatic datasets [GIPES] will enable a differential diagnosis in nurture vs. nature and evaluate other factors that personally impact that citizen (Bates et al., 2021). Environment inputs scope multiple causations that include virus to CO2 emissions as the centralization of personalized care cross multiple determinants (Luengo-Oroz et al., 2020; Tan et al., 2020).
Genomic systems embed in healthcare as IPES eXaminations seek to resolve wellbeing and stop high stakes decisions with inherent characteristics that manage populace health as phenotype (Rudin, 2019). Models drive scalable, accurate medicine via health records as datasets feature with fast healthcare interoperability resources to abstract informatics and harmonize predictions and precisions with workplace intelligence (Rajkomar et al., 2018).
Workplace machines and deeply learned intelligence use omics features that target each case with supervised or unsupervised algorithms that learn to abstract value, whilst neural networks activate greater biology insight, such as drug discovery (LeCun et al., 2015). For example, a basic machine-learned algorithm illustrated transitions for high dimensional space as teams progress on linear regression, decision tree and support vector analytics (Hastie et al., 2004, Table 2).
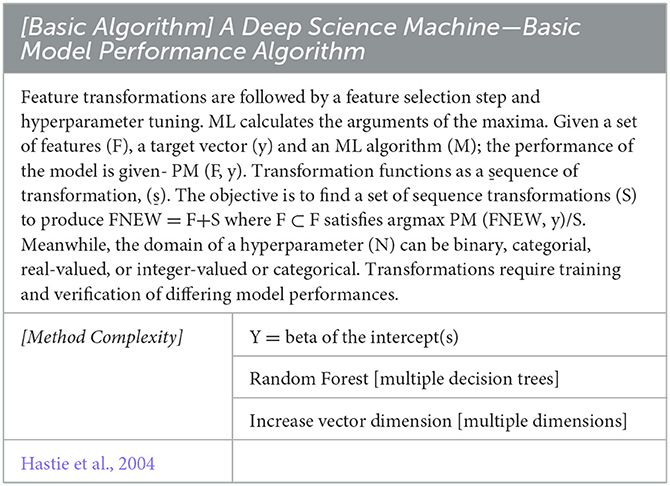
Table 2. Basic algorithm and method complexity.
“Toward automating data science,” algorithm hyperparameter tuning, progressive sampling, and autonomous assembling better learning using data sets to predict wellbeing (Kanter and Veeramachaneni, 2015; Wistuba et al., 2017). Auto-hyperparameter selection and Bayesian neural science probability inference systems improve Genome-Wide Association studies for predictive value (Feurer and Hutter, 2019; Trochet et al., 2019). As abstract training advanced to Neural Architecture Searches (Table 3), the Welcome Trust supports assurances for the right eXaminations to manage population health (Ordish and Hall, 2020).

Table 3. Workplace algorithms.
Open-source access to basic algorithmic coding scripts contrasts the metadata delivery to multiple NAS networks with individuals and their interactions, developing patterns of knowledge in future health (Ciancarini et al., 2020). Today, NAS dives deep into GIPES data, with intercept precision for Atrial Fibrillation induced Venous Thromboembolism and predictive insight on stroke incidences. In addition, back-propagation from pre-and post-eXaminations better the model ontology for hospital model gains and socioeconomic success (Figure 2).
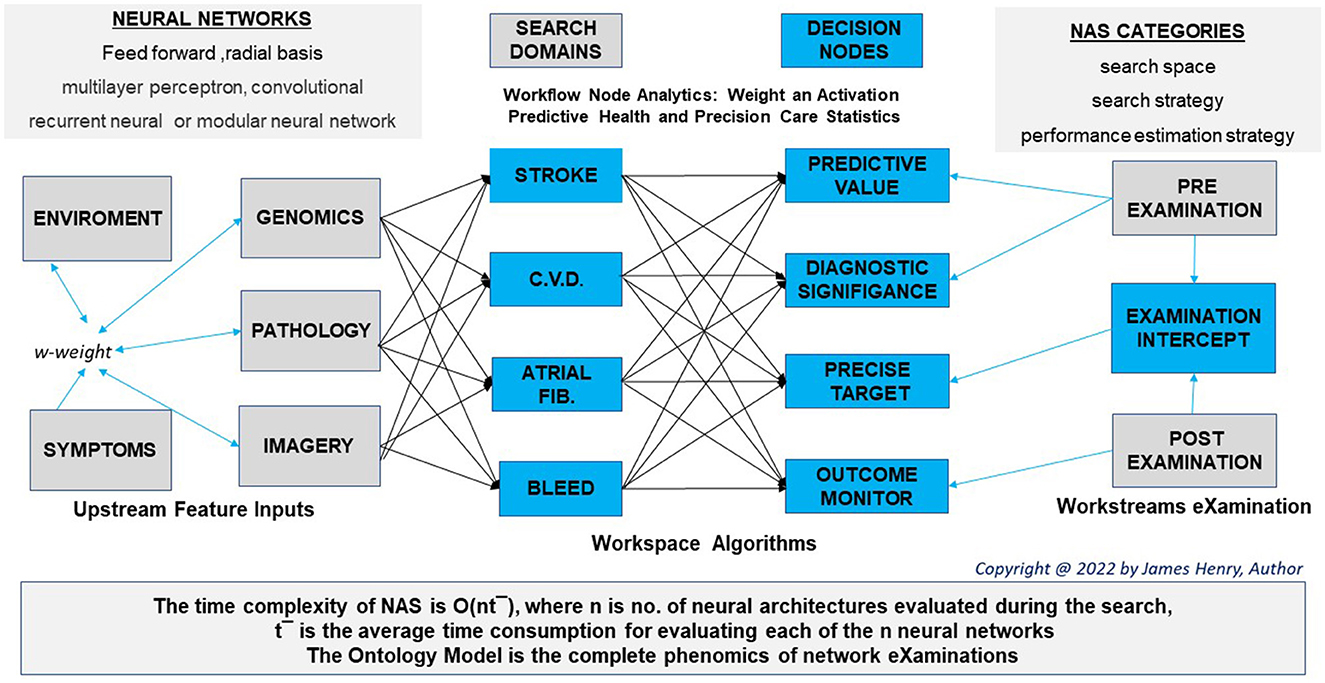
Figure 2. Workflow structure.
NAS requirements for model breadth and depth scope assist with a differential and forewarn on a prognosis as a series of weighted abstractions activate predictive health in chronic cardiovascular disease (Lu and Uddin, 2021). Workplace intelligence has time and dimension in a digital workspace dataset for use cases has “voices of biotech research” forecast greater insight to come (Annabi et al., 2021).
Diagnostics feature in more than 70% of medical interventions but often fail to deliver informed phenotypes or the most appropriate intervention, whilst future workstreams deliver better citizen health as phenomics datasets integrate use cases to personalize eXaminations (Hallworth, 2011).
Consider the following eXaminations workstream evidence on non-manual clinical support within personalized medicine. The workplace streams insight on diagnostic significance, predictive health, and precision care whilst observing the eXamination intercept. A 44 year old male committed his DNA to a genomic screen and presented to A/E with mild chest pain and palpitations. An electrocardiograph and bloods for analysis were scheduled:
1st STREAM: Diagnostic significance included ECG with a short QT interval. Hb 11.1, Platelets 148, White Cell Count 2.9, Chol. 6.1 mmol/l, HDL 0.9 mmol/l, equivocal Trop I. and a viscoelastic raised MCF. A mild angina history scheduled an angiogram.
2nd STREAM: Predictive health included sudden death syndrome, with scores on stroke, cardiovascular disease, and bleed risks [Anti-coagulant requirement]. Variants included LDLR and KCNQ- rs2074238 T-allele, F.V. [GWAS coagulative] and V.W.F. [non-pathogenic]. Genome differential eXaminations confirmed an acquired cytopenia [GWAS normal].
3rd STREAM: Precision care searched for an ablation, rejected on specialist archive outcomes. Amiodarone, Warfarin, Aspirin, and Clopidogrel were unsupported by VKORC1 and CYPC2C19 polymorphs. Pharmacogenomics targeted an Amiodarone and Rivaroxaban [ABCBI stable] therapy, based on using case data on patient outcomes.
4th STREAM: Post eXamination outcome informed on angiogram as non-occlusive with medicinal efficacy monitored by ECG, viscoelasticity, and blood work. Actions where discontinue Amiodarone for Flecainide, while the DOAC dose increased. Mild cytopenia had resolved. All streams presented can develop calculations on uncertainty probabilities with a post eXamination back propagation methodology development.
Theorists, philosophers, and psychologists review the bio of logic to conclude on assured AI that best personalize medicine, wherein society does not demark the abstract from the manual decision in health (Englebretsen, 2019). Culture on AI ethics has government recommend digital evaluations for care solutions (Gov.UK, 2020). The NHS actions a people promise to realize workforce alignment (NHS England, 2020b), while AI interprets PHM within eXaminations.
Partnerships with abstract leverage engage communes or providers in forums as system quality groups manage operations to target population health intervention, similar pandemic responses to personalize an intercept (Syrowatka et al., 2021). To culture on biological interventions, an eXaminations best practice readies data engineer and scientist with mathematics and expert clinical and quality practitioner in a workforce workflow to deliver solutions together (Li et al., 2020).
The author proposes workflow culture and illustrates multiple groups and arguments to amalgam differing intelligence perceptions that explain AI workplaces and elucidate workstreams to enable PHM (Figure 3).
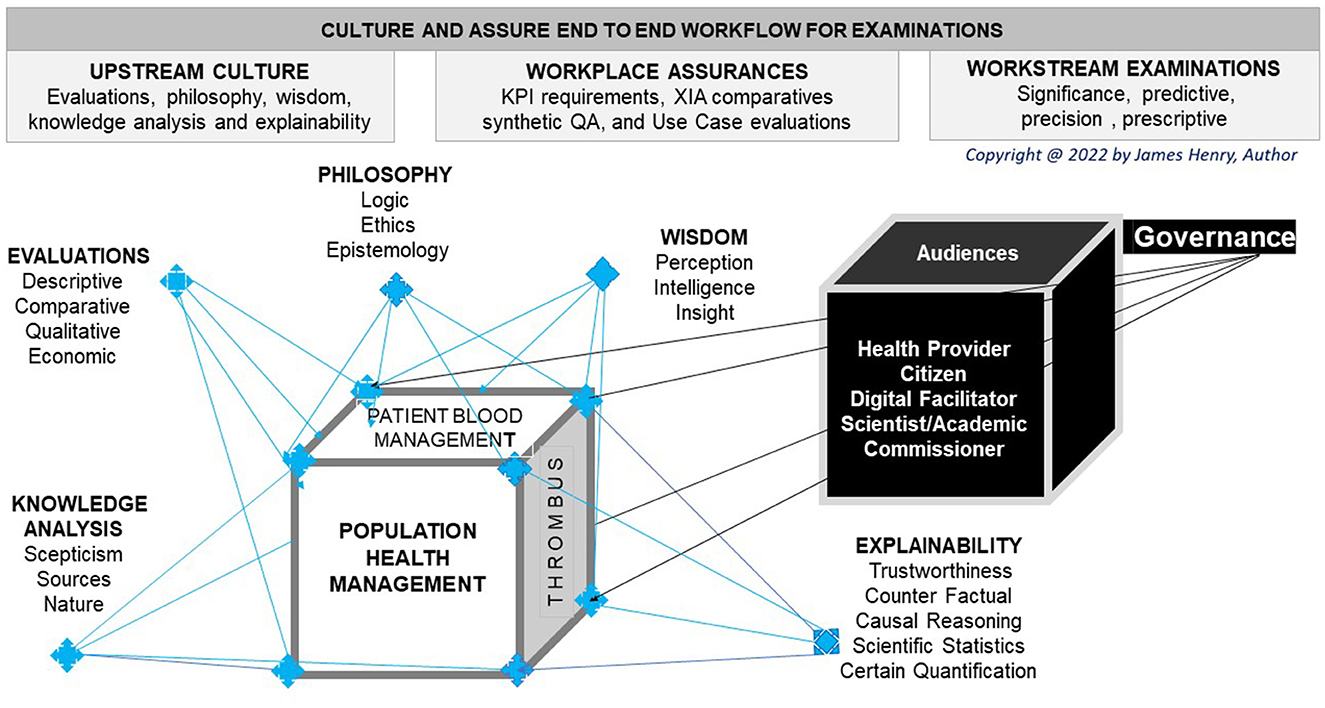
Figure 3. Culture work, assure flow.
Abstract perceptions have academics explain Black Box algorithm incomprehension as beyond a non-scientific analyst's cognitive ability (Nicholson, 2015). Sectors may seek transparency even if an algorithm is not apparent, while observed outcomes inform on lessons to be learned in best practice (Larsson and Heintz, 2020). Positive AI perceptions requires assurances that gain wisdom with a secure digital flow that cultures safe wellbeing in future work to be done (Figure 3).
Like other global efforts, personalized medicine unifies a planet to percept AI benefits (Topol and Lee, 2019). Ownership of data use cases offers many opinions as genomic associations match communities who relate transparency with a concept of knowing (Panch et al., 2019; Larsson and Heintz, 2020). Simplification of transparent intelligence with surrogate learning assists on positive precepts by reason that there are checks on the algorithm to assure the decision (Ferreira and Monteiro, 2020). Transparent integrated care systems align opaqueness with workflow plans for eXamination insight to action change (Table 4).
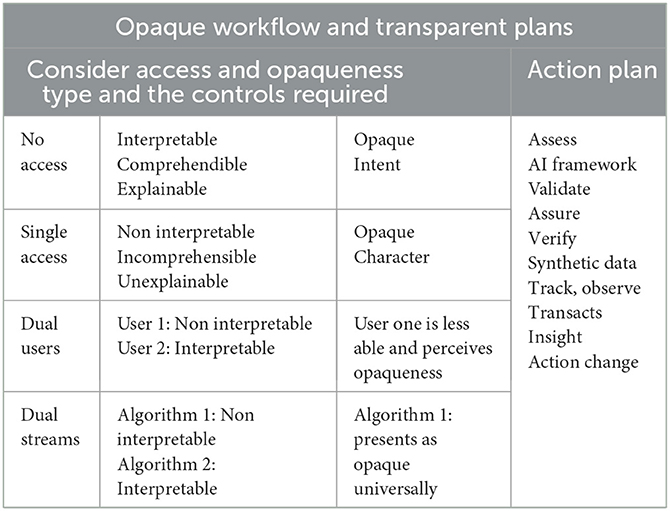
Table 4. Opaque workflow.
As a society, we evaluate biological truth and present evaluations, philosophy, wisdom, knowledge analysis, and explainability (Figure 3). Robust associations in system biology provide research eXaminations for phenomics integration, whence collaborated upon, and governed appropriately (Uffelmann et al., 2021). The explicable workplace advances the approaches and challenges of explainable abstracts to be commissioned for our future health (Xu et al., 2019).
One foresees conventional scientific determinism with abstraction explaining the biological models through PHM (Veatch, 1970). Therein coordinators develop explicable workplaces with interpretable workflow eXaminations that instill trust with operations from cardio epigenomics to coagulum protein modification (de Vries et al., 2020; Schiano et al., 2020). While scientific explanation remains debated, AI surpassed clinical performance over several genomic domains with greater success envisaged in healthcare to improve the citizen lifecycle journey (Veatch, 1970; Fogel and Kvedar, 2018).
Nevertheless, consignment of upstream datasets to format feature use cases brings global ethical queries to workstream eXaminations since they support proportional or definitive prognosis to specify human biology and precision therapy as a decision-making process (Jobin et al., 2019). Responsible, fair and justified ethical principles for genomic informatics foresee the phenotypes while other AI abstracts aim for precision insights to personalize pre ontology intercepts that individualize an eXamination as an implementation plan to improve outcomes (Jobin et al., 2019).
Trust shifts from heuristics to abstracts when monitoring patient outcomes with AI evidence, similar to oncology therapy and their post eXamination follow up with robust scientific support (Kimmelman and Tannock, 2018). A user reasons the counterfactual in assessing needs to speed up requisition of eXaminations that reduce the frequency or severity of harm; therein consider precision medicine without sequence analysis to reason health is not affected by DNA variation, to argue for pharmacogenomic evaluation and safe wellbeing (Prosperi et al., 2020).
Trustworthy claims about algorithms and those made by an algorithm reason an appropriate use case that does not require law, except in claims that AI is trustworthy when not assured, insured, elucidated or agreed upon (Spiegelhalter, 2020).
Explaining an ontology or hospital workstream that reduces mortality rates requires elucidation of the eXaminations with checks on any bias to enable a test interpretation and a valid decision. AI users more readily accept the abstract process for a support decision when performance indicators, surrogate AI, synthetic QA, and commissioned use cases become the norm (Figure 3).
Workstream assurances offer a “judgement, making decisions and prediction,” while mitigating adversity with model-specific or agnostic methods and synthetic data (Ahmed et al., 2020; Chen et al., 2021). Specific tools are intrinsically interpretable, belonging to the essential nature of an algorithm with visibility into how an AI system makes decisions, with the standard deviation founding a “Glass Box (Rai, 2019). Agnostics methods elucidate the black box with AI explanations, with examples for partial dependence and causal interpretation, individual conditional expectation, and accumulated local effects (Renki, 2020).
Neural network practice in medicine futures elucidate data in biotechnology, for a biological or therapeutic specification, as AI presents accurately what the clinician cannot (Sanal et al., 2019). Elucidating work through data mining or in images from place to stream requires assessment and classifiers before extracting knowledge with machine and deep learning (Vidushi Agarwal and Rajoria, 2019; Aggarwal et al., 2021). Communities and health providers engage enhanced computing power and cloud storage to mitigate bias and improve decision accuracy with improvements in workflow that converge the workforce (Topol, 2019). Healthcare models dispel AI apprehension and revolutionize wellbeing with an ICS PHM that brings a norm to organizations and personnel impact (Spatharou et al., 2020).
Consider the term artificial, which invokes a query on machine-made that requires an explanation and elucidation of the stream for positive perception. The word intelligence seeks clarity in a workplace definition as ML and DL use case algorithms abstract upstream data for workstream eXaminations that culture flow and assure work (Figure 3).
The NHS builds on a culture for insight normality by enabling step-by-step processes to realize the digital, data, and technology vision in a long-term NHS plan (Department of Health and Social Care, 2018; GOV.UK, 2019a). Bringing society together with recommendations from the Francis, Carter, and Paterson reports (House of Commons, 2013, 2020; Department of Health, 2016) require key step enablers to mitigate variance or adversity, as shown (Figure 4).
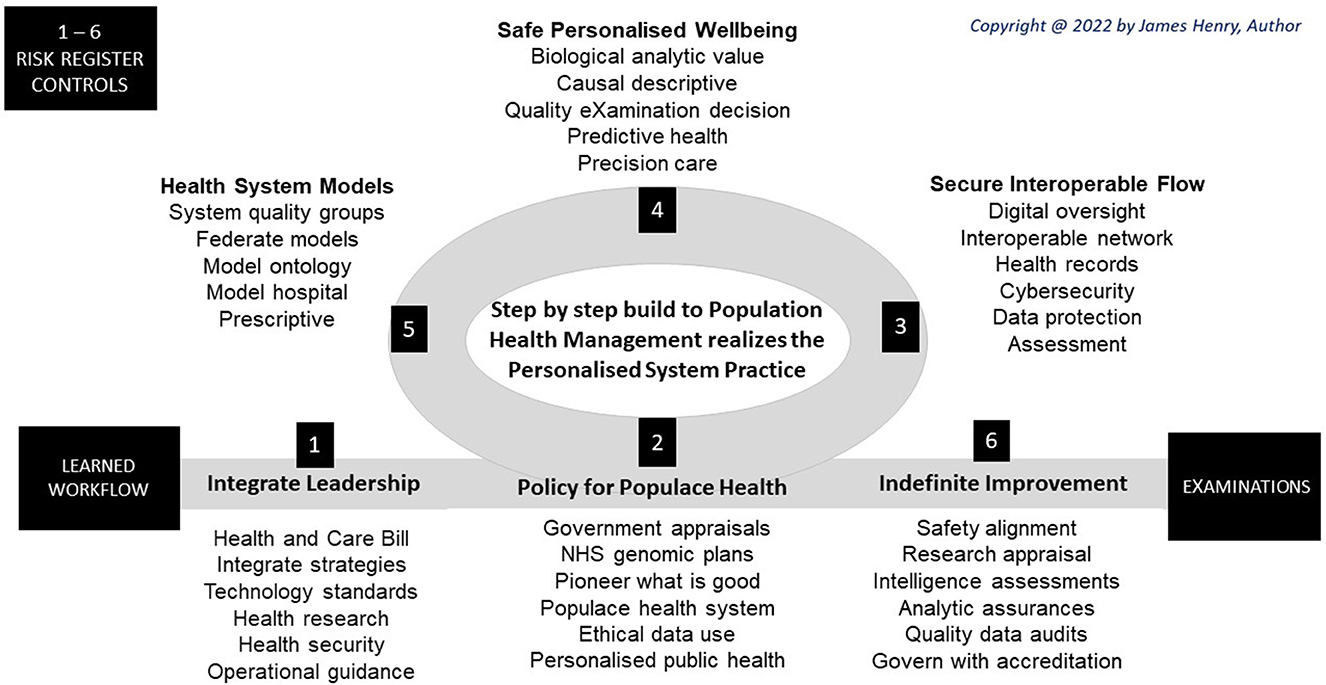
Figure 4. Workflow steps.
In 2022, the UK Health and Care Bill enactment brings rigidity to steps designed for NHS recovery with cohesive and safer services to tackle long-term waiting lists, chronic conditions, and health inequalities1 A global genomic lead has national strategies for innovation, AI, data, and commission of a core purposes to improve outcomes, tackle inequalities, and enable productivity with socioeconomic development (GOV.UK, 2019b, 2021a,b; Global Alliance for Genomics and Health, 2021; NICE, 2021; NHS, 2022b). Thereby future wellbeing has integrated system governance of steps for an eXamination norm (NHS, 2022b, Figure 4).
To unite eXaminations, a UK code of practice assists the government in the design and build of technology to deliver secure and ethical workflow functions (GOV.UK, 2021c). At the same time, an NHS standard reinforces best practices (NHS, 2021a). Our future health programme underpins public health eXaminations in developing new ways to prevent, detect and treat disease (NHS, 2020). The Health Research Authority and the Biomedical Catalyst Program assist researchers and businesses develop projects that personalize an efficacious pre- to post-eXamination process that also assures the intercept (UK Bioindustry Programme, 2020; NHS Health Research Authority, 2021).
ICS leadership focus on the patient's perspectives with accountability for safe digital delivery as clinical and life science experts with technology partners assess citizen and health provider needs for the commission of the workflow eXamination (NHS, 2022b). After that, the UK Health Security Agency and the Healthcare Safety Investigation Branch can protect the community from the impact of health threats and provide intellectual, scientific, and operational leadership for secure wellbeing that can review an eXamination process and its system management (GOV.UK, 2021d; Healthcare Safety Investigation Branch, 2021).
Integrated care with a system for the management of populace health requires “approved thinking models” with personalized practices to underpin advice that clarifies socioeconomic, NHS and public benefits in the delivery of policy aims (NHS, 2021b). NHS England plan with Genome UK on implementation commitments that action pillars to predict health and precision care (GOV.UK, 2006).
Digital electrical and electronic engineers pioneered autonomous models for human-centric aims, ethics, and value, with mitigation of privacy and security risk (IEEE Advancing Technology for Humanity, 2017). Work for what good looks like frame digital principles to describe how ICS arrangements support success as maturity assessments level up and deliver population management via health records (NHS, 2021c).
Principal steps transition to analytic norms in populace health as digital genomics develop health care system eXams built on secure interoperable flow for safe personalized wellbeing (Figure 4). Model ontology and model hospitals develop with plans for Microsoft Healthcare and Genomic Laboratory Information Systems (Microsoft Industry, 2015; Digital Health, 2021a).
Personalized public health requires the integration of research innovations with ethics for “appropriate and responsible data use in government and the wider public sector” (Government Digital Service, 2020). Appropriate public policy projects foresee the genomic revolution and plan digital health for data research with respect for the person, genetic solidarity, and altruism (Public Policy Projects Public Policy Institute, 2021).
The NHSE transformation directorate oversee digital strategy and policy with project commissions for secure technologies and open standards to meet populace needs on public health platforms (Digital Health, 2021b; NHS Digital, 2022a). Systems support framework support populace health to integrate care with networks to analytic suppliers with scope limited to non-clinical services (NHS England, 2022).
NHSE digital aims accelerate partner working to make effective resource use, with scope for virtual wards, digitization, and skills (NHS England, 2022). Interoperable access to secure flow in personalized health has API and FHIR enabling populace wellbeing (Alterovitz et al., 2020), as mobile app evaluation, education, and awareness of digital formularies better health (Lagan et al., 2020).
A nationwide e-health record enables populace health management with system links to data from multiple settings which enable biological ontology workflow (Wood et al., 2021). Data mining records enables better research for applications in clinical care, as cardiocoagulum learning on genetic data to phenotype depend on secure interoperable flow (Jensen et al., 2012; Zhao et al., 2019).
NHSE Transformation Directorate oversees security with the “WannaCry” crisis, a wake up for a cyber-service essential framework for process review and response to alerts in toolkits (Hoeksma, 2017; NHS Digital, 2022b). DCB standards issued by NHSE Transformation Directorate require IT system manufacturers and healthcare organizations to carry out a product risk assessment to determine acceptance (NHS Digital, 2022c).
Digital Technology Assessment Criteria for secure interoperable flow instills provider and community confidence that access, usability, interoperability, and technical security meet assurances (NHSE Transformation Directorate, 2021). Both data protection and clinical safety processes require a sign off evaluation process in transition to safe populace wellbeing, as itemized (Table 5).
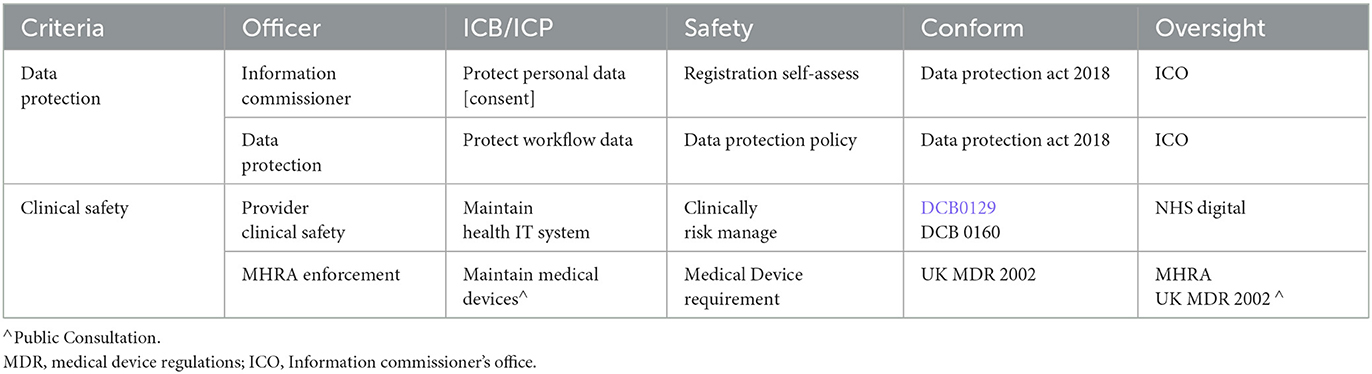
Table 5. Data protection and clinical safety.
Society seeks explanation to present significance and describe incidence as clinically relevant at reviews to integrate GIPES insight to manage populace health. Big data analytic challenges offer biological value for safe populace wellbeing, social behaviors, and economics with descriptive, predictive, precision, and prescriptive points of interest, so mapped (Figure 5).
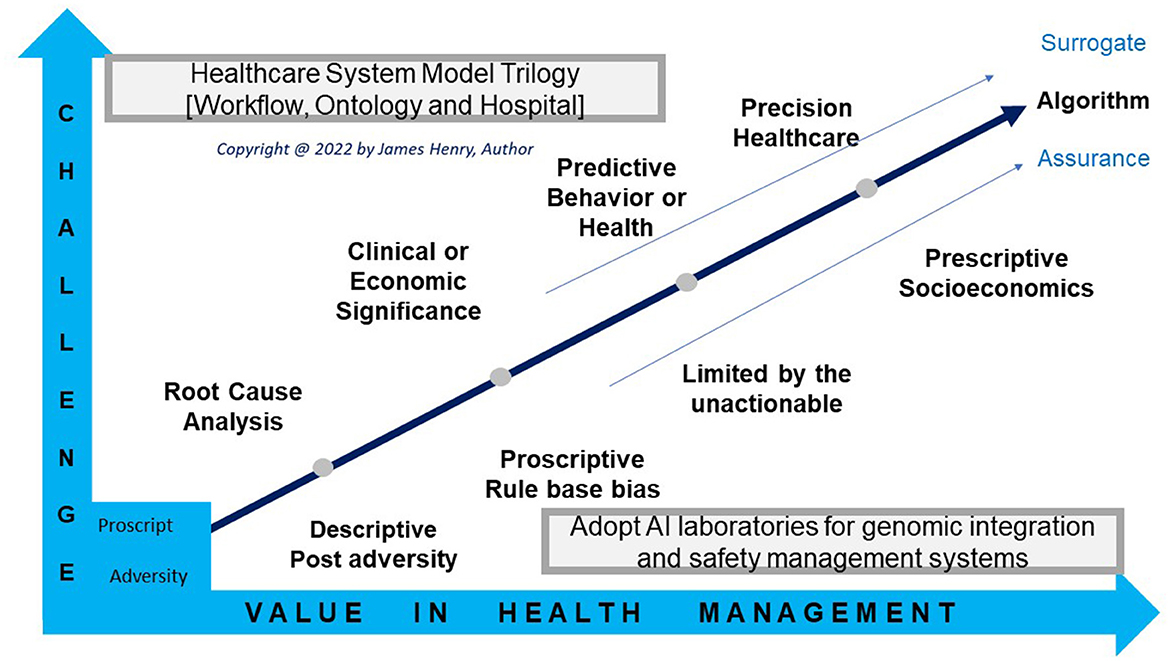
Figure 5. Workflow values.
Critical realists of the causal descriptive use eXaminations to present a pathology or explain adverse outcomes which inform on a phenotype variation or a decision bias (Fox and Aranko, 2017). Building eXaminations from GIPES descriptive data to foresee the clinical significance, morbidity, or mortality can resource predictors before the event which requires data mining of electronic health records (Tomašev et al., 2021).
Quality decisions from pathology results, input clean “examination” data as a norm to manage diagnosis, while GIPES feature in AI use cases for biological “eXaminations” that personalize health [International Organization for Standardization (ISO), 2017; Get It Right First Time, 2021; ISO/DI 15189 [Internet], 2022]. AI builds across places after experts simulate health efficacy or hospital efficiency, wherein data scientists validate eXaminations to commission and accredit excellence for health providers to adopt the integrated system [ISO/DI 15189 [Internet], 2022; NHS, 2022b].
AI laboratory eXaminations predict pathology to personalize intercepts in models when assessed on the validity of the process in the future of healthcare (Barker, 2017; de Hond et al., 2022). Advances in predictive health are restricted in the volume and veracity of GIPES data as analytics trial patterns in associations of predictors in VTE outcomes, like A-Fib polygenic risk scores with; monogenic variables (Abraham et al., 2021), clinical risks (O'Sullivan et al., 2021), and lifestyle choice (Ye et al., 2021).
Precision terms offer Pre-eXamination value to intercept as the data mining of GIPES informatics embrace more than genomic alone to define or insight phenotype with predictor searches to exact an interventional choice (Abraham et al., 2021; O'Sullivan et al., 2021; Ye et al., 2021), as an eXamination norm. For instance, VTE predictive power can precision intercepts similar pharmaceuticals, lifestyle choices and invasive procedures, such as A-Fib ablation (Burstein et al., 2017; Mai et al., 2019; Kolin et al., 2021; Yuan et al., 2021).
Models manage disease predictor or business opportunity and develop genomic systems with operations for cloud computing and AI laboratories [graph A]. As people live longer with co-morbidities society address health system fragmentation with strategies to execute models (GOV.UK, 2019b, 2021a,b; Global Alliance for Genomics and Health, 2021; NICE, 2021; NHS, 2022b). Thereby a system quality group and a local needs quality group terms of reference abstract decision-making for ontology and hospital gains with partners sharing system insights that predict health and precision care (National Quality Board, 2022a).
Federating datasets enables digital solutions to abstract outcome with accurate and robust statistical health system models (Rieke et al., 2020). Population health management improve quality of care and reduce cost growth with model ontology and hospital (Berwick et al., 2018). The Systematized Nomenclature of MEDicine -clinical terms provides a vocabulary norm for e-informatics exchanges wherein ontology prediction and precision care are realized. Model hospitals plan with social care to lower burdens with business intelligence supported by SNOMED (NHS Digital, 2018).
Learning communities expand on biomedical space to GIPES dimensions to improve wellbeing and social system challenges as federated models provide a rational on ontology and hospital eXamination solutions for socioeconomic success (Hill, 1984; Xu et al., 2020). Descriptive to predictive repositories add post eXamination intercept data to enable neural network to back propagate on models and prescript control by cognitive analysis (Hennessy et al., 2015; Whittington and Bogacz, 2019).
Data administrators, engineers, and analysts ingest, process, and visualize better health and social care whilst digital improvement becomes a legal requirement of ICS organizations for a license to operate (Carding, 2022). To govern personalized care, then six A's, align, appraise, assess, assure, audit, and accredit healthcare eXaminations. Workforce healthcare management imputes a workflow bot for national improvements executed regionally for safe health and social care delivered locally (Figure 6).
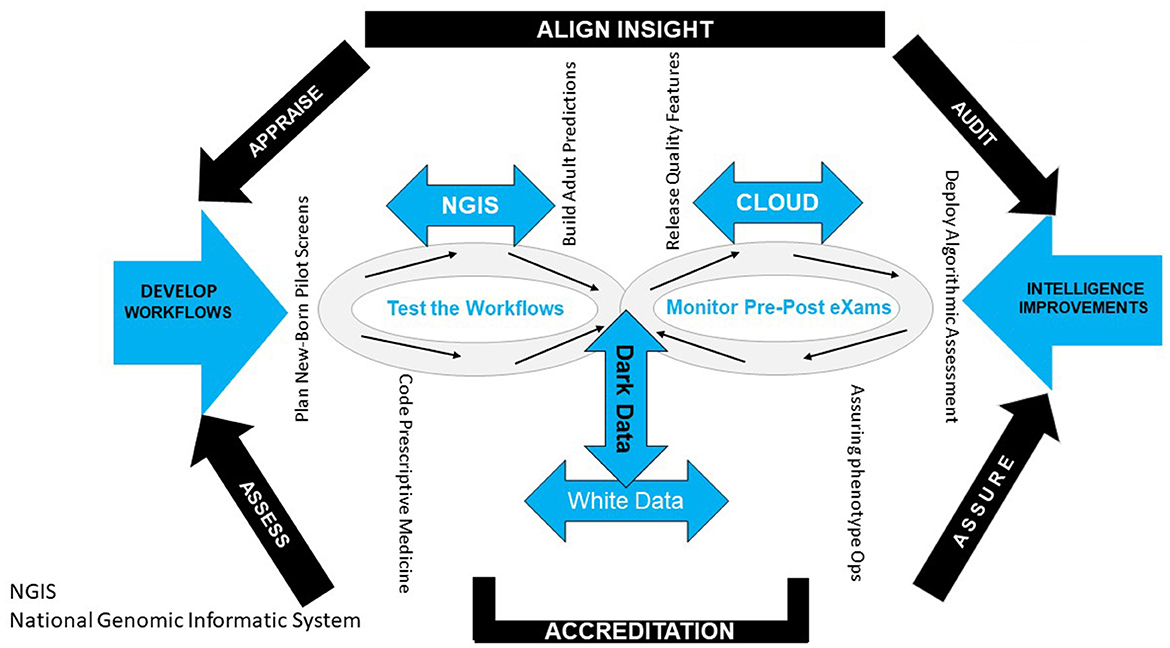
Figure 6. Workflow governance.
The Health Research Authority action health and social care with portfolio appraisals to put people first for indefinite improvement as workflows with GIPES databases (NHS Health Research Authority, 2021; NHS, 2022c). The Academic Health and Science Networks assess community and health provider needs for AI laboratory developments, similar A-Fib projects, and community pharmacies to support cardiocoagulum proposals (The AHS Network, 2020; Turner et al., 2020).
Recommendations in the Francis, Paterson and Carter reports explaining, in part, the approximation of 11 K deaths from patient safety incidents each year (House of Commons, 2013, 2020; Hogan et al., 2015; Department of Health, 2016). To assure our future health and reduce elective waiting lists, the ontology and hospital eXaminations accumulate descriptive to predictive data to precision and prescript wellbeing near to patients (Our Future Health, 2021; Get It Right First Time, 2022).
The Medical Healthcare and products Regulatory Authority audits clinical trial conduct whilst the Care Quality Commission re-focus on auditing information and fewer on-site inspections (Khin et al., 2021; Care Quality Commission, 2022). The Data Alliance Partnership Board enable data collections whilst a Records Management Code of Practice audits contracted organizations, adult social care, and public health on standard data migration (NHS, 2021d; NHS Digital, 2022d).
Accrediting workflow workstream eXaminations originates in a quality report from 2014 (Henry, 2017). A shared national quality policy actions internal and external, qualitative, and quantitative functions (Burstein et al., 2017; National Quality Board, 2022b). The National Institute of Health and Clinical Excellence and Health Education England develop standards and AI programme training (NICE, 2021; NHS Health Education England, 2022). International standards enable governance of data use cases with an eXamination process control and a safe AI risk management system that personalizes practice [International Organization for Standardization (ISO), 2017, 2018b; ISO, 2022; UKAS, 2022].
Taken collectively the 6 A's—align, appraise, assess, assure, audit, and accredit- personalized care as an evidence unit as the system workforce demonstrates a citizen centric impact. By sharing decision making between clinicians and the public whilst utilizing intelligent abstracts in future health provides greater value with predictive health and precision care with realistic expectation and a therapy choice that offers more appropriate interventions on wellbeing2.
Integrating hospital with social care require a personalized end-to-end structure for intelligence eXaminations that support decisions. Oversight by system quality groups embeds a positive culture for abstract explanation and elucidation with context to transparent workflow. Such support to workforces brings confidence to plan and perform data functions upstream that place personal use cases in the workstream.
Digital health laboratories work for communities with stakeholders and partner co-operations to accelerate Population Health Management to personalize care. Senior Programme Management's commitment to public safety develops effective plans for healthcare systems that expedite digital eXaminations for wellbeing, regardless of the place of access.
Personalized care groups with integrated organizational-wide functions require technology to scale populace health with knowledge accumulation and best-practice analytics for agile service. Health service governance aims for a program to benefit personalization, working with teams on long-term plans to execute innovation, digital, data, and excellence pillars as genomic commitments better future health.
Getting personalized care right the first time requires informatic resilience and coding scripts that place the citizen centric. In future health, population health management enhances public outcomes and impacts productivity. Corporate programme managers plan model ontology with model hospital and action workflow functions to enable practitioner reviews that confirm effectiveness and efficiencies nationally, regionally, and locally.
Strategy development with analytics operates business intelligence into our future health. It links hospitals with social care to identify socioeconomic burdens and deliver personalized care group oversight on personalized health and care programme solutions. Change control readies with NHSE Directorates, personalized care groups, and stakeholder support of health industry controls that evidence cases.
Global apportioning of health-related informatics readies for predictive health and precision care. National challenges raised by partner and provider to integrate genomic care requires deep understanding of intelligent workflow for the management of populace health. Digital data-driven non-manual outputs support personalized medicine decisions regarding a bleed or thrombus event. Workflow delivers citizen system biology to general practice, Hospital Trust, and community as digital AI develop phenotype eXaminations.
Upstream, workplace and workstream end-to-end solutions feature genomics, images and pathology data, where AI abstracts develop better admin and clinical operative decisions that increase productivity and enhance health outcomes. Culturing abstract algorithms has workforce share perceptions with system quality groups joint, working committees and communes by engagements that elucidate workstreams in a personalized practice proposal.
Workflow steps integrate leadership to plan health management policies with insights from transformation and improvement actions of an eXamination process. Steps secure the digital flow of data for safe wellbeing and observe health service practice with safety insight for an NHS recovery. Culture intelligent workflow, structure, culture, and steps proposes leading groups and improving personalized practice for national opportunities, regional priorities, and local needs. Aligning organization, practitioner, genomic and social variations by overseeing descriptive, predictive, precision, and prescriptive analytics commences by culturing the step-by-step design for population health management.
The author confirms being the sole contributor of this work and has approved it for publication.
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. ^Health and Care Bill—Parliamentary Bills—UK Parliament [Internet]. Available online at: https://bills.parliament.uk/bills/3022.
2. ^14:00-17:00. International Organization for Standardisation (2020).
Abraham, G., Rutten-Jacobs, L., and Inouye, M. (2021). Risk prediction using polygenic risk scores for prevention of stroke and other cardiovascular diseases. Stroke 52, 2983–2991. doi: 10.1161/STROKEAHA.120.032619
Aggarwal, R., Sounderajah, V., Martin, G., Ting, D. S. W., Karthikesalingam, A., King, D., et al. (2021). Diagnostic accuracy of deep learning in medical imaging: a systematic review and meta-analysis. NPJ Digit. Med. 4:65. doi: 10.1038/s41746-021-00438-z
Ahmed, M. U., Barua, S., and Begum, S. (2020). “Artificial intelligence, machine learning and reasoning in health informatics—an overview,” in Intelligent Systems Reference Library, 171–92. Available online at: https://link.springer.com/chapter/10.1007/978-3-030-54932-9_7 (cited April 29, 2022).
Alterovitz, G., Heale, B., Jones, J., Kreda, D., Lin, F., Liu, L., et al. (2020). FHIR Genomics: enabling standardization for precision medicine use cases. NPJ Genom. Med. 5:13. doi: 10.1038/s41525-020-0115-6
Annabi, N., Baker, M., Boettiger, A., Chakraborty, D., Chen, Y., Corbett, K. S., et al. (2021). Voices of biotech research. Nat. Biotechnol. 39, 281–286. doi: 10.1038/s41587-021-00847-1
Aronson, S. J., and Rehm, H. L. (2015). Building the foundation for genomics in precision medicine. Nature 526, 336–342. doi: 10.1038/nature15816
Barker, R. W. (2017). Is precision medicine the future of healthcare? Pers. Med. 14, 459–461. doi: 10.2217/pme-2017-0060
Bates, D. W., Levine, D., Syrowatka, A., Kuznetsova, M., Craig, K. J. T., Rui, A., et al. (2021). The potential of artificial intelligence to improve patient safety: a scoping review. NPJ Digit. Med. 4:54. doi: 10.1038/s41746-021-00423-6
Berwick, D. M., Nolan, T. W., and Whittington, J. (2018). The triple aim: care, health, and cost. Health Affairs 27, 759–769. doi: 10.1377/hlthaff.27.3.759
Boehme, C., Hannay, E., and Pai, M. (2021). Promoting diagnostics as a global good. Nat. Med. 27, 367–368. doi: 10.1038/s41591-020-01215-3
Burstein, B., Barbosa, R. S., Kalfon, E., Joza, J., Bernier, M., and Essebag, V. (2017). Venous thrombosis after electrophysiology procedures. Chest 152, 574–586. doi: 10.1016/j.chest.2017.05.040
Carding, N. (2022). Government Plans New “Regulatory Levers” to Force Pace of NHS's Digital Uptake [Internet]. Health Service Journal. Available online at: https://www.hsj.co.uk/technology-and-innovation/government-plans-new-regulatory-levers-to-force-pace-of-nhss-digital-uptake/7032714.article (cited July 1, 2022).
Care Quality Commission (2022). Responding to Our Consultation: Changes for More Flexible and Responsive Regulation [Internet]. Care Quality Commission. Available online at: https://apo.org.au/node/313644 (cited July 1, 2022).
Chen, R. J., Lu, M. Y., Chen, T. Y., Williamson, D. F. K., and Mahmood, F. (2021). Synthetic data in machine learning for medicine and healthcare. Nat. Biomed. Eng. 5, 493–497. doi: 10.1038/s41551-021-00751-8
Ciancarini, P., Missiroli, M., Poggi, F., and Russo, D. (2020). An Open Source Environment for an Agile Development Model. IFIP Advances in Information and Communication Technology [Internet], 148–62. Available online at: https://link.springer.com/chapter/10.1007/978-3-030-47240-5_15#citeas
de Hond, A. A. H., Leeuwenberg, A. M., Hooft, L., Kant, I. M. J., Nijman, S. W. J., van Os, H. J. A., et al. (2022). Guidelines and quality criteria for artificial intelligence-based prediction models in healthcare: a scoping review. NPJ Digit. Med. 5, 1–13. doi: 10.1038/s41746-021-00549-7
de Vries, J. J., Snoek, C. J. M., Rijken, D. C., and de Maat, M. P. M. (2020). Effects of post-translational modifications of fibrinogen on clot formation, clot structure, and fibrinolysis. Arterioscl. Thromb. Vasc. Biol. 40, 554–569. doi: 10.1161/ATVBAHA.119.313626
Department of Health (2016). Operational Productivity and Performance in English NHS Acute Hospitals: Unwarranted Variations [Internet]. Department of Health. Available online at: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/499229/Operational_productivity_A.pdf (cited May 26, 2022).
Department of Health Social Care (2018). The Future of Healthcare: Our Vision for Digital, Data and Technology in Health and Care [Internet]. GOV.UK. Available online at: https://www.gov.uk/government/publications/the-future-of-healthcare-our-vision-for-digital-data-and-technology-in-health-and-care/the-future-of-healthcare-our-vision-for-digital-data-and-technology-in-health-and-care
Department of Health Social Care Public Health England (2020). VCSE Health and Wellbeing Alliance 2021-24 Information Pack for VCSE Organisations [Internet]. Department of Health and Social Care Public Health England. Available online at: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/921737/HW_Alliance_pack_final_CLEAN_FINAL.pdf (cited April 24, 2022).
Digital Health (2021a). CliniSys Launches System for Genomic Laboratories in the UK. Digital Health Available online at: https://www.digitalhealth.net/2021/01/clinisys-launches-system-for-genomic-laboratories-in-the-uk/ (cited June 26, 2022).
Digital Health (2021b). NHS Digital and NHSX to Merge With NHS England [Internet]. Digital Health. Available online at: https://www.digitalhealth.net/2021/11/nhs-digital-nhsx-merge-nhs-england/ (cited June 26, 2022).
Englebretsen, G. (2019). The logician and the biologist. Acta Baltic Hist. Philos. Sci. 7, 39–52. doi: 10.11590/abhps.2019.1.03
Ferreira, J. J., and Monteiro, M. S. (2020). “What are people doing about XAI user experience? A survey on ai explainability research and practice,” in Design, User Experience, and Usability Design for Contemporary Interactive Environments. HCII 2020 (Lecture Notes in Computer Science), Vol. 12201, eds A. Marcus and E. Rosenzweig (Cham: Springer), 56–73. doi: 10.1007/978-3-030-49760-6_4
Feurer, M., and Hutter, F. (2019). Hyperparameter optimization. Autom. Mach. Learn. 3–33. doi: 10.1007/978-3-030-05318-5_1
Fogel, A. L., and Kvedar, J. C. (2018). Artificial intelligence powers digital medicine. NPJ Digit. Med. 1:5. doi: 10.1038/s41746-017-0012-2
Fox, S., and Aranko, O. (2017). Healthcare framing: critical realist framing for causal interdependencies and uncertainties within healthcare. Technol. Soc. 50, 66–72. doi: 10.1016/j.techsoc.2017.05.001
GENOME UK (2020). The Future of Healthcare [Internet]. Available online at: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/920378/Genome_UK_-_the_future_of_healthcare.pdf
Get It Right First Time (2021). Pathology GIRFT Programme National Specialty Report [Internet]. Available online at: https://www.rcpath.org/uploads/assets/171f0ed0-ec20-4c93-b399d8518ee55641/Pathology-GIRFT-Programme-National-Specialty-Report-Sept-2021.pdf (cited May 19, 2022).
Get It Right First Time (2022). High Volume Low Complexity (HVLC) Programme [Internet]. Getting It Right First Time - GIRFT. Available online at: https://www.gettingitrightfirsttime.co.uk/hvlc/ (cited May 19, 2022).
Global Alliance for Genomics Health (2021). Global Alliance for Genomics and Health: 2021 Policy on Clinically Actionable Genomic Research Results [Internet]. Available online at: https://www.ga4gh.org/wp-content/uploads/2021-Policy-on-Clinically-Actionable-Genomic-Research-Results.pdf (cited May 16, 2022).
GOV.UK (2006). The Green Book (2022) [Internet]. GOV.UK. Available oniline at: https://www.gov.uk/government/publications/the-green-book-appraisal-and-evaluation-in-central-governent/the-green-book-2020#a2-place-based-analysis (cited May 13, 2022).
GOV.UK (2019a). NHS Long Term Plan launched [Internet]. News Story. Available online at: https://www.gov.uk/government/news/nhs-long-term-plan-launched (cited June 7, 2022).
GOV.UK (2019b). National Data Strategy [Internet]. GOV.UK. Available online at: https://www.gov.uk/guidance/national-data-strategy (cited September 16, 2021).
Gov.UK (2020). Choose Evaluation Methods: Evaluating Digital Health Products [Internet]. GOV.UK. Available online at: https://www.gov.uk/guidance/choose-evaluation-methods-evaluating-digital-health-products#approaches-that-cut-across-categories (cited April 25, 2022).
GOV.UK (2021a). National AI Strategy - HTML Version [Internet]. GOV.UK. Available online at: https://www.gov.uk/government/publications/national-ai-strategy/national-ai-strategy-html-version
GOV.UK (2021b). UK Innovation Strategy Leading the Future by Creating It [Internet]. Available online at: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1009577/uk-innovation-strategy.pdf (cited May 13, 2022).
GOV.UK (2021c). Technology Code of Practice [Internet]. Available online at: https://www.gov.uk/guidance/the-technology-code-of-practice#define-your-purchasingstrategy (cited May 17, 2022).
GOV.UK (2021d). New UK Health Security Agency to Lead Response to Future Health Threats [Internet]. GOV.UK. Available online at: https://www.gov.uk/government/news/new-uk-health-security-agency-to-lead-response-to-future-health-threats (cited April 7, 2021).
Government Digital Service (2020). Data Ethics Framework [Internet]. Available online at: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/923108/Data_Ethics_Framework_2020.pdf#:~:text=The%20Data%20Ethics%20Framework%20guides%20appropriate%20and%20responsible,and%20encourages%20responsible%20innovation.%20Who%20is%20it%20for%3F (cited June 26, 2022).
Hallworth, M. J. (2011). The '70% claim': what is the evidence base? Ann. Clin. Biochem. 48, 487–488. doi: 10.1258/acb.2011.011177
Hardie, T., Horton, T., and Warburton, W. (2021). Switched On: How Do We Get the Best Out of Automation and AI in Health Care? Available online at: https://www.health.org.uk/sites/default/files/upload/publications/2021/SwitchedOn_WEB.pdf (cited March 31, 2022).
Hastie, T., Tibshirani, R., and Friedman, J. H. (2004). The Elements of Statistical Learning: Data Mining, Inference, and Prediction: With 200 Full-Color Illustrations. New York, NY: Springer.
Healthcare Safety Investigation Branch (2021). Healthcare Safety Investigation Branch. Available online at: https://www.hsib.org.uk/
Hennessy, D. A., Flanagan, W. M., Tanuseputro, P., Bennett, C., Tuna, M., Kopec, J., et al. (2015). The Population Health Model (POHEM): an overview of rationale, methods and applications. Popul. Health Metrics. 13:24. doi: 10.1186/s12963-015-0057-x
Henry, J. A. (2017). Viscoelastometric Point of Care Testing – Patient Blood Management Quality System [Abstract]. Abstract Book CLH 2017 UK NEQAS for Blood Coagulation.
Henry, J. A. (2019). Personalised and regeneration medicine require a Coagulum-OMICs model [Abstract]. Anesth. Analg. doi: 10.21767/2471-8084-C1-023
Hill, P. (1984). The Rationale for Learning Communities and Learning Community Models [Internet]. Available online at: https://files.eric.ed.gov/fulltext/ED309818.pdf (cited June 29, 2022).
Hoeksma, J. (2017). NHS cyberattack may prove to be a valuable wake up call. BMJ 357:j2818. doi: 10.1136/bmj.j2818
Hogan, H., Zipfel, R., Neuburger, J., Hutchings, A., Darzi, A., and Black, N. (2015). Avoidability of hospital deaths and association with hospital-wide mortality ratios: retrospective case record review and regression analysis. BMJ 351:h3239. doi: 10.1136/bmj.h3239
House of Commons (2013). Report of the Mid Staffordshire NHS Foundation Trust Public Inquiry [Internet]. Available online at: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/279124/0947.pdf
House of Commons (2020). Report of the Independent Inquiry Into the Issues Raised by Paterson [Internet]. Available online at: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/863211/issues-raised-by-paterson-independent-inquiry-report-web-accessible.pdf (cited May 26, 2022).
Iacobucci, G. (2021). Health and care bill: what changes do healthcare leaders want to see? BMJ 374:n1806. doi: 10.1136/bmj.n1806
IEEE Advancing Technology for Humanity (2017). A Vision for Prioritizing Human Well-being with Autonomous and Intelligent Systems [Internet]. Dec [cited 2022 Jun 26]. Available from: https://www.bing.com/search?q=when+was+the+A+Vision+for+Prioritizing+Human+Well-being+with+Autonomous+and+Intelligent+Systems+publishedandform=ANNTH1andrefig=2ad67d961f2448418b7f629279d4b32d
International Organization for Standardisation (2020). ISO 22367:2020 Medical laboratories – Application of risk management to medical laboratories. ISO. Available online at: https://www.iso.org/standard/71254.html
International Organization for Standardization (ISO) (2012). Medical laboratories — Requirements for quality and competence [Internet]. [cited 2022 May 17]. Available from: https://www.iso.org/standard/56115.html
International Organization for Standardization (ISO) (2017). ISO/IEC JTC 1/SC 42 - Artificial intelligence [Internet]. ISO. [cited 2022 May 23]. Available from: https://www.iso.org/committee/6794475.html
International Organization for Standardization (ISO) (2018a). ISO 9004:2018. ISO. [cited 2022 Apr 24]. Available from: https://www.iso.org/standard/70397.html
International Organization for Standardization (ISO) (2018b). ISO 13485:2016 [Internet]. ISO. 2018 [cited 2022 Apr 16]. Available from: https://www.iso.org/standard/59752.html
ISO (2022). ISO 9001:2015 [Internet]. ISO. Available online at: https://www.iso.org/standard/62085.html (cited August 13, 2022).
ISO/DI 15189 [Internet] (2022). genorma.com. Available online at: https://genorma.com/en/project/show/iso:proj:76677#:~:text=ISO%2FDIS%2015189%20Medical%20laboratories%20%E2%80%94%20Requirements%20for%20quality (cited June 28, 2022).
Jensen, P. B., Jensen, L. J., and Brunak, S. (2012). Mining electronic health records: towards better research applications and clinical care. Nat. Rev. Genet. 13, 395–405. doi: 10.1038/nrg3208
Jobin, A., Ienca, M., and Vayena, E. (2019). The global landscape of AI ethics guidelines. Nat. Mach. Intell. 1, 389–399. doi: 10.1038/s42256-019-0088-2
Kanter, J. M., and Veeramachaneni, K. (2015). “Deep feature synthesis: towards automating data science endeavors,” in IEEE International Conference on Data Science and Advanced Analytics (DSAA) [Internet] (Paris). doi: 10.1109/DSAA.2015.7344858
Khin, N. A., Grandinetti, C., Dixey, H., Yu, B., Skeete, R., Ayalew, K., et al. (2021). Tackling challenging data integrity topics in 2020: update on good clinical practice perspectives from the US FDA and MHRA UK. Clin. Pharmacol. Therap. 112, 31–43. doi: 10.1002/cpt.2386
Kimmelman, J., and Tannock, I. (2018). The paradox of precision medicine. Nat. Rev. Clin. Oncol. 15, 341–342. doi: 10.1038/s41571-018-0016-0
Knoppers, B. M. (2014). Framework for responsible sharing of genomic and health-related data. HUGO J. 8:3. doi: 10.1186/s11568-014-0003-1
Kolin, D. A., Kulm, S., and Elemento, O. (2021). Prediction of primary venous thromboembolism based on clinical and genetic factors within the U.K. Biobank. Sci. Rep. 11:21340. doi: 10.1038/s41598-021-00796-4
Lagan, S., Aquino, P., Emerson, M. R., Fortuna, K., Walker, R., and Torous, J. (2020). Actionable health app evaluation: translating expert frameworks into objective metrics. NPJ Digit. Med. 3:100. doi: 10.1038/s41746-020-00312-4
Larsson, S., and Heintz, F. (2020). Transparency in artificial intelligence. Intern. Policy Rev. 9. doi: 10.14763/2020.2.1469
LeCun, Y., Bengio, Y., and Hinton, G. (2015). Deep learning. Nature 521, 436–444. doi: 10.1038/nature14539
Li, R. C., Asch, S. M., and Shah, N. H. (2020). Developing a delivery science for artificial intelligence in healthcare. NPJ Digit. Med. 3:107. doi: 10.1038/s41746-020-00318-y
Lu, H., and Uddin, S. (2021). A weighted patient network-based framework for predicting chronic diseases using graph neural networks. Sci. Rep. 11:22607. doi: 10.1038/s41598-021-01964-2
Luengo-Oroz, M., Hoffmann Pham, K., Bullock, J., Kirkpatrick, R., Luccioni, A., Rubel, S., et al. (2020). Artificial intelligence cooperation to support the global response to COVID-19. Nat. Mach. Intell. 2, 295–297. doi: 10.1038/s42256-020-0184-3
Maguire, D., Honeyman, M., Fenney, D., and Jabbal, J. (2021). Shaping the Future of Digital Technology in Health and Social Care [Internet]. Available online at: https://www.kingsfund.org.uk/sites/default/files/2021-04/Shaping%20the%20future%20of%20digital%20technology%20in%20health%20and%20social%20care.pdf (citedApril 24, 2022).
Mai, V., Guay C-, Perreault, L., Bonnet, S., Bertoletti, L., Lacasse, Y., et al. (2019). Extended Anticoagulation for VTE. Chest 155, 1199–1216. doi: 10.1016/j.chest.2019.02.402
Margetts, H., and Dorobantu, C. (2019). Rethink government with AI. Nature 568, 163–165. doi: 10.1038/d41586-019-01099-5
Microsoft Industry (2015). Innovation in the NHS: Moving to the Cloud [Internet]. Microsoft Industry. Available online at: https://cloudblogs.microsoft.com/industry-blog/en-gb/government/2016/08/05/innovation-nhs/#:~:text=NHS%20Choices%20chose%20Microsoft%20Azure%20to%20provide%20the,possible%20without%20the%20elastic%20scale%20of%20cloud%20services (cited June 26, 2022).
Minkman, M. M. N. (2016). Values and principles of integrated care. Int. J. Integr. Care 16, 1–3. doi: 10.5334/ijic.2458
National Quality Board (2022a). National Guidance on System Quality Groups. Available online at: https://www.england.nhs.uk/wp-content/uploads/2022/01/B0894-nqb-guidance-on-system-quality-groups.pdf (cited July 1, 2022).
National Quality Board (2022b). National Quality Board Position Statement: Managing Risks and Improving Quality Through Integrated Care Systems High Quality, Personalised and Equitable Care for all WELL-LED EXPERIENCE (RESPONSIVE AND CARING) [Internet]. National Quality Board. Available online at: https://www.england.nhs.uk/wp-content/uploads/2021/04/nqb-position-statement.pdf (cited May 23, 2022).
NHS (2021a). NHS Service Standard [Internet]. NHS. Available online at: https://service-manual.nhs.uk/standards-and-technology/service-standard (cited June 26, 2022).
NHS (2021b). 2022/23 Priorities and Operational Planning Guidance [Internet]. NHS. Available online at: https://www.england.nhs.uk/wp-content/uploads/2022/02/20211223-B1160-2022-23-priorities-and-operational-planning-guidance-v3.2.pdf (cited May 16, 2022).
NHS (2021c). What Good Looks Like Framework [Internet]. NHS. Available online at: https://www.nhsx.nhs.uk/digitise-connect-transform/what-good-looks-like/what-good-looks-like-publication/ (cited May 16, 2022).
NHS (2021d). Records Management Code of Practice 2021 [Internet]. NHS. Available online at: https://www.nhsx.nhs.uk/information-governance/guidance/records-management-code/records-management-code-of-practice-2021/#:~:text=The%20Records%20Management%20Code%20of%20Practice%20for%20Health,or%20under%20contract%20to%2C%20the%20NHS%20in%20England (cited May 29, 2022).
NHS (2022a). The Multi-Agency Advice Service (MAAS) [Internet]. NHS Transformation Directorate. Available online at: https://transform.england.nhs.uk/ai-lab/ai-lab-programmes/regulating-the-ai-ecosystem/the-multi-agency-advice-service-maas/ (cited November 4, 2022).
NHS (2022b). Classification: Official Publications Approval Reference: PAR642 Integrated Care Systems: Design Framework [Internet]. NHS. Available online at: https://www.england.nhs.uk/wp-content/uploads/2021/06/B0642-ics-design-framework-june-2021.pdf
NHS (2022c). Homepage, Putting People First [Internet]. Health Research Authority. Available online at: https://www.hra.nhs.uk/ (cited May 14, 2022).
NHS Digital (2018). SNOMED CT - NHS Digital [Internet]. NHS Digital. Available online at: https://digital.nhs.uk/services/terminology-and-classifications/snomed-ct (cited May 15, 2022).
NHS Digital (2022a). Spine Futures [Internet]. NHS Digital. Available online at: https://digital.nhs.uk/services/spine/spine-futures (cited June 26, 2022).
NHS Digital (2022b). News [Internet]. Available online at: https://www.dsptoolkit.nhs.uk/News/2021-2022-standard
NHS Digital (2022c). Applicability of DCB 0129 and DCB 0160 [Internet]. NHS Digital. Available online at: https://digital.nhs.uk/services/clinical-safety/applicability-of-dcb-0129-and-dcb-0160?key= (cited June 26, 2022).
NHS Digital (2022d). Data Alliance Partnership Board [Internet]. Available online at: https://digital.nhs.uk/data-and-information/information-standards/information-standards-and-data-collections-including-extractions/data-alliance-partnership-board (cited May 17, 2022).
NHS England (2020a). WE ARE THE NHS: People Plan 2020/21 - action for us all [Internet]. NHS England. Available online at: https://www.england.nhs.uk/wp-content/uploads/2020/07/We-Are-The-NHS-Action-For-All-Of-Us-FINAL-March-21.pdf
NHS England (2020b). The Promise [Internet]. NHS England. Available online at: https://www.england.nhs.uk/ournhspeople/online-version/lfaop/our-nhs-people-promise/the-promise/ (cited April 25, 2022).
NHS England (2022). About the Health Systems Support Framework [Internet]. NHS England. Available online at: https://www.england.nhs.uk/hssf/background/ (cited June 26, 2022).
NHS Health Education England (2022). Digital, Artificial Intelligence and Robotics Technologies in Education (DART-Ed) [Internet]. NHS Health Education England. Available online at: https://digital-transformation.hee.nhs.uk/building-a-digital-workforce/dart-ed (cited May 17, 2022).
NHS Health Research Authority (2021). Business plan 2021 - 2022 [Internet]. Health Research Authority. Available online at: https://www.hra.nhs.uk/about-us/what-we-do/business-plan/business-plan-2021-2022/#businessplan
NHS (2020). Our Future Health [Internet]. Available online at: https://ourfuturehealth.org.uk/
NHSE Transformation Directorate (2021). Digital Technology Assessment Criteria (DTAC) [Internet]. NHSX. Available online at: https://www.nhsx.nhs.uk/key-tools-and-info/digital-technology-assessment-criteria-dtac/ (cited June 26, 2022).
NICE (2021). The NICE Strategy 2021 to 2026 | Corporate Publications | Who We Are | About [Internet]. NICE. Available online at: https://www.nice.org.uk/about/who-we-are/corporate-publications/the-nice-strategy-2021-to-2026 (cited May 13, 2022).
Nicholson, W. (2015). Black-box medicine. Harvard J. Law Technol. 28, 420–467. Available online at: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=2499885
Ordish, J., and Hall, A. (2020). Black Box Medicine and Transparency Interpretable Machine Learning A PHG Foundation Report for the Wellcome Trust [Internet]. Available online at: https://phgfoundation.org/media/154/download/black-box-interpretable-machine-learning.pdf?v=1andinline=1 (cited April 24, 2022).
O'Sullivan, J. W., Shcherbina, A., Justesen, J. M., Turakhia, M., Perez, M., Wand, H., et al. (2021). Combining clinical and polygenic risk improves stroke prediction among individuals with atrial fibrillation. Circulation 14:e003168. doi: 10.1161/CIRCGEN.120.003168
Our Future Health (2021). Our Future Health[Internet]. Our Future Health. Available online at: https://ourfuturehealth.org.uk/
Panch, T., Mattie, H., and Celi, L. A. (2019). The “inconvenient truth” about AI in healthcare. NPJ Digit. Med. 2:77. doi: 10.1038/s41746-019-0155-4
Pathology Quality Assurance Review [Internet] (2014). Available online at: https://www.england.nhs.uk/wp-content/uploads/2014/01/path-qa-review.pdf
Prosperi, M., Guo, Y., Sperrin, M., Koopman, J. S., Min, J. S., He, X., et al. (2020). Causal inference and counterfactual prediction in machine learning for actionable healthcare. Nat. Mach. Intell. 2, 369–375. doi: 10.1038/s42256-020-0197-y
Public Health England (2019). What Good Looks Like. Public Health England. Available online at: https://www.adph.org.uk/wp-content/uploads/2019/06/What-Good-Looks-Like-Programme-Summary.pdf (cited April 24, 2022).
Public Policy Projects Public Policy Institute (2021). Genomics Revolution [Internet]. Available online at: https://publicpolicyprojects.com/wp-content/uploads/sites/6/2021/10/PPP-Genomics-Revolution-Report-FINAL.pdf (cited May 16, 2022).
Rai, A. (2019). Explainable AI: from black box to glass box. J. Acad. Market. Sci. 48, 137–141. doi: 10.1007/s11747-019-00710-5
Rajkomar, A., Oren, E., Chen, K., Dai, A. M., Hajaj, N., Hardt, M., et al. (2018). Scalable and accurate deep learning with electronic health records. NPJ Digit. Med. 1:18. doi: 10.1038/s41746-018-0029-1
Renki, E. (2020). Chapter 1: Introduction | Limitations of Interpretable Machine Learning Methods [Internet]. Available online at: https://slds-lmu.github.io/iml_methods_limitations/introduction.html (cited June 26, 2022).
Rieke, N., Hancox, J., Li, W., Milletarì, F., Roth, H. R., Albarqouni, S., et al. (2020). The future of digital health with federated learning. NPJ Digit. Med. 3, 1–7. doi: 10.1038/s41746-020-00323-1
Rudin, C. (2019). Stop explaining black box machine learning models for high stakes decisions and use interpretable models instead. Nat. Mach. Intell. 1, 206–215. doi: 10.1038/s42256-019-0048-x
Sanal, M. G., Paul, K., Kumar, S., and Ganguly, N. K. (2019). Artificial intelligence and deep learning: the future of medicine and medical practice. J. Assoc. Phys. India 67, 71–73.
Schiano, C., Benincasa, G., Franzese, M., Della Mura, N., Pane, K., Salvatore, M., et al. (2020). Epigenetic-sensitive pathways in personalized therapy of major cardiovascular diseases. Pharmacol. Therap. 2020:107514. doi: 10.1016/j.pharmthera.2020.107514
Shelmerdine, S. C., Arthurs, O. J., Denniston, A., and Sebire, N. J. (2021). Review of study reporting guidelines for clinical studies using artificial intelligence in healthcare. BMJ Health Care Inform. 28:e100385. doi: 10.1136/bmjhci-2021-100385
Spatharou, A., Hieronimus, S., and Jenkins, J. (2020). Transforming Healthcare With AI: The Impact on the Workforce and Organizations | McKinsey [Internet]. Available online at: https://www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/transforming-healthcare-with-ai (cited June 26, 2022).
Syrowatka, A., Kuznetsova, M., Alsubai, A., Beckman, A. L., Bain, P. A., Craig, K. J. T., et al. (2021). Leveraging artificial intelligence for pandemic preparedness and response: a scoping review to identify key use cases. NPJ Digit. Med. 4, 1–14. doi: 10.1038/s41746-021-00459-8
Tan, L., Guo, J., Mohanarajah, S., and Zhou, K. (2020). Can we detect trends in natural disaster management with artificial intelligence? A review of modeling practices. Nat. Hazards 107, 2389–2417. doi: 10.1007/s11069-020-04429-3
The AHS Network (2020). National Programmes and Priorities [Internet]. AHSN Network. Available online at: https://www.ahsnnetwork.com/about-academic-health-science-networks/national-programmes-priorities (cited July 1, 2022).
Tomašev, N., Harris, N., Baur, S., Mottram, A., Glorot, X., Rae, J. W., et al. (2021). Use of deep learning to develop continuous-risk models for adverse event prediction from electronic health records. Nature Protocols. 16, 2765–2787. doi: 10.1038/s41596-021-00513-5
Topol, E., and Lee, K.-F. (2019). It takes a planet. Nat. Biotechnol. 37, 858–861. doi: 10.1038/s41587-019-0214-z
Topol, E. J. (2019). High-performance medicine: the convergence of human and artificial intelligence. Nature Medicine. 25, 44–56. doi: 10.1038/s41591-018-0300-7
Trochet, H., Pirinen, M., Band, G., Jostins, L., McVean, G., and Spencer, C. C. A. (2019). Bayesian meta-analysis across genome-wide association studies of diverse phenotypes. Genet. Epidemiol. 43, 532–547. doi: 10.1002/gepi.22202
Turner, R. M., Newman, W. G., Bramon, E., McNamee, C. J., Wong, W. L., Misbah, S., et al. (2020). Pharmacogenomics in the UK National Health Service: opportunities and challenges. Pharmacogenomics 21, 1237–1246. doi: 10.2217/pgs-2020-0091
Uffelmann, E., Huang, Q. Q., Munung, N. S., de Vries, J., Okada, Y., Martin, A. R., et al. (2021). Genome-wide association studies. Nat. Rev. Methods Primers 1:59. doi: 10.1038/s43586-021-00056-9
UK Bioindustry Programme (2020). £30 Million Biomedical Catalyst to Launch Following Successful BIA Campaign [Internet]. Available online at: https://www.bioindustry.org/news-listing/30-million-biomedical-catalyst-to-launch-following-successful-bia-campaign.html#:~:text=The%20Biomedical%20Catalyst%20has%20been%20a%20leading%20campaign,companies%20to%20build%20world-leading%20British%20life%20science%20companies (cited June 26, 2022).
UKAS (2022). Update of UKAS Certificates for ISO 15189 – Medical Laboratories [Internet]. Available online at: https://www.ukas.com/resources/latest-news/update-of-ukas-certificates-for-iso-15189-medical-laboratories/ (cited June 7, 2022).
Veatch, H. (1970). Aspects of scientific explanation and other essays in the philosophy of science. Philos. Sci. 37, 312–314. doi: 10.1086/288305
Vidgen, M. E., Williamson, D., Cutler, K., McCafferty, C., Ward, R. L., McNeil, K., et al. (2021). Queensland Genomics: an adaptive approach for integrating genomics into a public healthcare system. NPJ Genom. Med. 6:71. doi: 10.1038/s41525-021-00234-4
Vidushi Agarwal, M., and Rajoria, R. (2019). “Analysis of various classification methods,” in International Conference on Issues and Challenges in Intelligent Computing Techniques (ICICT) [Internet]. doi: 10.1109/ICICT46931.2019.8977688
Whittington, J. C. R., and Bogacz, R. (2019). Theories of error back-propagation in the brain. Trends Cogn. Sci. 23, 235–250. doi: 10.1016/j.tics.2018.12.005
Wiegand, T., Krishnamurthy, R., Kuglitsch, M., Lee, N., Pujari, S., Salath,é, M., et al. (2019). WHO and ITU establish benchmarking process for artificial intelligence in health. Lancet 394, 9–11. doi: 10.1016/S0140-6736(19)30762-7
Wistuba, M., Schilling, N., and Schmidt-Thieme, L. (2017). “Automatic frankensteining: creating complex ensembles autonomously,” in Proceedings of the 2017 SIAM International Conference on Data Mining [Internet], 741–749. Available online at: https://www.researchgate.net/publication/317486108_Automatic_Frankensteining_Creating_Complex_Ensembles_Autonomously
Wood, A., Denholm, R., Hollings, S., Cooper, J., Ip, S., Walker, V., et al. (2021). Linked electronic health records for research on a nationwide cohort of more than 54 million people in England: data resource. BMJ 373:n826. doi: 10.1136/bmj.n826
Xu, F., Uszkoreit, H., Du, Y., Fan, W., Zhao, D., and Zhu, J. (2019). “Explainable AI: a brief survey on history, research areas, approaches and challenges,” in Natural Language Processing and Chinese Computing (NLPCC) 2019 (Lecture Notes in Computer Science), Vol. 11839, eds J. Tang, M. Y. Kan, D. Zhao, S. Li, and H. Zan (Cham: Springer), 563–574. doi: 10.1007/978-3-030-32236-6_51
Xu, J., Glicksberg, B. S., Su, C., Walker, P., Bian, J., and Wang, F. (2020). Federated learning for healthcare informatics. J. Healthc. Inform. Res. 5, 1–19. doi: 10.1007/s41666-020-00082-4
Ye, Y., Chen, X., Han, J., Jiang, W., Natarajan, P., and Zhao, H. (2021). Interactions between enhanced polygenic risk scores and lifestyle for cardiovascular disease, diabetes, and lipid levels. Circulation 14:e003128. doi: 10.1161/CIRCGEN.120.003128
Yuan, S., Bruzelius, M., Håkansson, N., Åkesson, A., and Larsson, S. C. (2021). Lifestyle factors and venous thromboembolism in two cohort studies. Thrombos. Res. 202, 119–124. doi: 10.1016/j.thromres.2021.03.024
Keywords: population, health, management, artificial, intelligence
Citation: Henry JA (2023) Culture intelligent workflow, structure, and steps. Front. Artif. Intell. 6:985469. doi: 10.3389/frai.2023.985469
Received: 03 July 2022; Accepted: 06 February 2023;
Published: 28 February 2023.
Edited by:
Thomas Hartung, Bloomberg School of Public Health, Johns Hopkins University, United StatesReviewed by:
Alberto Ochoa Zezzatti, Universidad Autónoma de Ciudad Juárez, MexicoCopyright © 2023 Henry. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: James Andrew Henry,  amFtZXMuaGVucnkxOUBvdXRsb29rLmNvbQ==
amFtZXMuaGVucnkxOUBvdXRsb29rLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.