 F. Escribá Alepuz1,2*†
F. Escribá Alepuz1,2*† A. Díaz Ruz1*†J. D. Jiménez Santana1,†
A. Díaz Ruz1*†J. D. Jiménez Santana1,† C. García Cebrián1,2J. Encarnación1M. Hervías Sanz2,3P. Argente Navarro1,4
C. García Cebrián1,2J. Encarnación1M. Hervías Sanz2,3P. Argente Navarro1,4
- 1Department of Anesthesiology and Critical Care, Hospital Universitari I Politècnic La Fe, Valencia, Spain
- 2Paediatric Anaesthesiology Section, Spanish Society of Anesthesiology and Resuscitation (SEDAR), Madrid, Spain
- 3Department of Anesthesiology and Critical Care, Gregorio Marañón General University Hospital, Madrid, Spain
- 4Department of Surgical Specialities, Hospital Universitari I Politècnic La Fe, Valencia, Spain
Predicting fluid responsiveness is a major challenge in the pediatric population as vascular and pulmonary compliance differ from the adults. However it is a crucial thing to avoid the harmful fluid overload. We count on different variables to identify responders being the dynamic parameters the ones with more evidence, specially the Respiratory Variation In Aortic Blood Flow Velocity based on echocardiography. Other variables rely on the arterial waveform, like Pulse Pressure Variation or Stroke Volume Variation seem to have limitations but new tests like VTC are arriving to overcome their drawbacks. We review the actual evidence regarding fluid responsiveness prediction in children and the anatomic and physiologic peculiarities of children that explain why they do not respond like adults and why we should study them in particular.
1 Introduction
Volume expansion is one of the main tools used by anesthesia and intensive care teams in the management of hemodynamic instability (HI) or shock. Fluids increase blood volume and, consequently, preload, so the responsible physician expects, accordingly to the Frank-Starling Law, a raise in stroke volume (SV) and cardiac output (CO) that would ensure adequate tissue perfusion. Patients who increase CO by 10%–15% with fluids are known as fluid responders (1). However, not all patients respond, and furthermore, fluids are not without risks, and fluid overload has demonstrated to increase morbidity and mortality (1, 2). Therefore, volume expansion therapy should be administered when necessary and guided by clinical and hemodynamical criteria, requiring, as a consequence, optimal monitoring and a careful patient selection.
Regarding pediatrics, hemodynamic repercussions during anesthesia are common in these patients due to their susceptibility to potential surgical losses and the consequences of fasting (3). Moreover, as shown on the systematic review of Gan et al., 49%–60% of children do not respond to fluids in an HI scenario, making it crucial to identify those who do to ensure proper therapy (1–3) and minimize consequences of fluid overload. However, it is not an easy thing to identify responders as various hemodynamic variables in pediatrics still need to be validated or re-studied. This happens because of the physiological differences of children at vascular and thoracopulmonary level that indicate that younger ages are expected to have different fluid responsiveness indices and cutoff points even between young and older children.
In the following manuscript we will review variables available for hemodynamic monitoring as well as their use to identify fluid responders. Afterwards we will expose the state of these tests in pediatrics and the main reasons why there might be limitations in their use in children.
2 Static variables for hemodynamic monitoring
Static hemodynamic variables are evaluated at a specific point in time and some of the are clinical outcomes like urinary output, blood pressure (BP), heart rate (HR), or central venous pressure (CVP) (2). In all the studies and revisions included static variables failed to predict fluid responsiveness in children (2, 4).
Traditionally, hypotension has triggered fluid resuscitation; however, BP depends more on vascular tone and peripheral resistance than blood volume, limiting its role in identifying HI, especially patients dependent on fluid therapy. HR is nonspecific, being affected by many other possibly concomitant situations such as pain or anemia, for example (5). Finally, CVP has been dismissed as a good measure of fluid dependency and response to fluids due to low predictive values and its use has also been linked in different studies to longer ICU stays, more mechanical ventilation (MV) time, and excessive fluid administration (5). An important aspect to take into consideration is that already in 2013, it was demonstrated through a systematic review that dynamic variables yielded better results in identifying responders than static variables in pediatric patients (2). This should lead us to study these variables and found the best cutoffs points for children.
3 Dynamic variables for hemodynamic monitoring
Dynamic variables show the continuous change of preload due to mechanical ventilation (MV). During MV inspiration consists on direct lung expansion with positive pressure that directly compresses the heart compromising preload. On the other hand, positive pressure induces cyclic increases in intrathoracic pressure and lung volume. Thus, inspiration causes an increase in systemic venous return resistance, as well as in pulmonary vascular resistance and right ventricular afterload, reducing its systolic volume. Initially, the opposite occurs in the left heart, pulmonary vessels are squeezed along with a decrease in afterload and an increase in systolic volume in early beats, but in subsequent beats, there will be a decrease in systolic volume from the right ventricle, resulting in reduced systolic volume during inspiration (2, 6–10).
The variation of SV as a consequence of MV is then transmitted to the vascular tree causing changes in aortic blood flow, arterial blood pressure, and plethysmographic waveform amplitude. All these modifications of cardiac and vascular measures are used as indicators of fluid responsiveness. Review of the literature and its findings regarding these indicators can be found on Table 1.
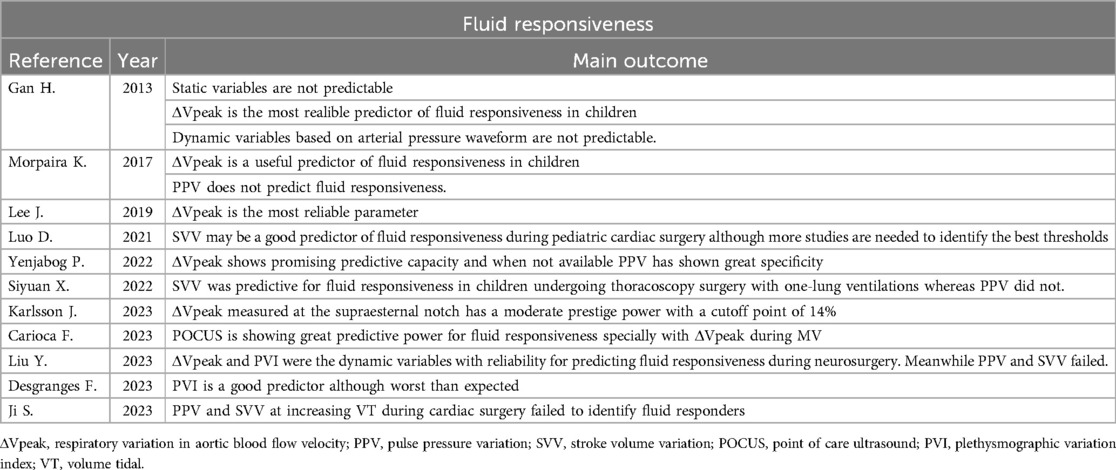
Table 1. Summary of articles in relation to fluid responsiveness prediction in pediatric population.
Derived from arterial pressure waveform we have Pulse Pressure Variation (PPV) that has shown to predict a raise on CO with volume as its value raises on mechanically ventilated patients. Stroke volume variation (SVV) indicates if SV varies significantly with each beat and Leo et al. demonstrated on their meta-analysis a good prediction power of it for children, specially during cardiac surgery (11). Absolute values of PPV or SVV >13% have been associated with low preload and need of intravascular expansion (4), but there are also many studies showing great limitations in children (2, 4, 12). As we explain later, the limitation of these parameters may be a consequence of the increased arterial wall compliance of children that result in a limited distal repercussion of the changes in SV due to MV. Furthermore PPV and SVV have many requirements, even in adults, to be a useful parameter such as VT of at least 8 ml/kg, no spontaneous breathing, no alteration of chest wall or lung compliance or a HR:RR >6 (12).
Nevertheless, one promising aspect regarding PPV and SVV is the Volume Tidal Challenge (VTC), a fluid responsiveness test that relies on the evidence that the predictive value of PPV and SVV increases with higher tidal volumes. In this way VTC consists on studying how much does PPV variate between different tidal volumes (up to 15 ml/kg in some animal studies) (13, 14). Although this test has been already validated in the adult population (13, 14) with great results the investigation is still poor in children. On our research, we only found one study who investigated the role of PPV or SVV variation with increasing tidal volumes in children during cardiac surgery. It concluded however that VTC could not predict fluid responsiveness among pediatric population (15). We do believe that there may be some limitations, specially on the definition of fluid responder, so still VTC may be promising in children, specially investigating the ventilatory parameters that could affect prediction power of PPV/SVV.
Based on the plethysmographic curve we count on other dynamic variables such as plethysmographic waveform amplitude (ΔPOP) or the plethysmographic variation index (PVI). ΔPOP measurement requires specific software and relies on calculating the amplitude of the waveforms which may constantly be resized automatically (4). Meanwhile, PVI relies on the Perfusion Index to be calculated. These parameters are attractive in pediatrics as they are non invasive but there reliability may vary according to the force of the sensor or the use of inotropic (4). However, the evidence for their prediction power is still controversial and although there are some individual studies that showed no capacity of prediction, another meta-analysis concluded PVI was a good predictor of fluid responsiveness (2, 4, 16, 17).
Finally, other dynamic variables depend on echocardiography such as velocity time integral (VTI) or the respiratory variation in aortic blood flow velocity (ΔVpeak) (1, 2). This last variable have shown the best results in determining fluid responsiveness in children, specially on congenital cardiac pathologies, and with a cutoff point between 12% and 14% (15, 17, 18). However it is highly operator dependent (1, 4). This parameter can be obtained from transthoracic (5 chamber apical view or supraesternal notch) or transesophageal echocardiography.
4 The challenge of directing fluid therapy in pediatric patients
Children present an immature myocardium and complex ventricular-arterial coupling with a reduced ventricular compliance and a less steep Frank-Starling curve (2). Furthermore, both peripheral and proximal arterial wall elastance in children decrease after birth, with increased stiffness as children grow (4, 10, 19). This translates in a deterioration of the relationship between SV and changes in the arterial wall and therefore a limitation for the arterial pressure waveform variables. This explains why PPV o SVV alone are limited parameters when studying fluid responsiveness in children. At the same time it may explain why ΔVpeak is more reliable, as it measures at a central level and does not depend on the peripheral effect of SV variation. It also helps to understand why children with congenital heart conditions undergoing cardiac surgery may present with better prediction power of PPV or SVV as their vascular compliance and ventricular-arterial coupling is altered and varies from children without these pathologies (1, 20).
On the other hand, lung distensibility and the elastic properties of the thoracic wall also change with age, resulting in improved distensibility of the lung parenchyma and modification of the thoracic wall structure. Until the 2nd-3rd year, the thoracic wall is three times more compliant than the lungs and this contributes to the attenuation of pleural and transpulmonary pressure transmission with respiratory cycles. If in healthy adults, with similar compliance of the thoracic wall and lung, intratorathic pressure increases by about half of the total airway pressures, in children, where there is lower pulmonary compliance, (relative to thoracic wall compliance), there will be less pressure transmission and thus less hemodynamic repercussion (10). In conclusion, respiratory system pressures will not be transmitted equally to intrathoracic vascular structures, meaning that there may be less impact on preload and CO when intrathoracic pressure increases. This is undoubtedly another reason why patient age can affect the ability of dynamic indices to predict fluid responsiveness (9). From two years onwards, they have similar proportions to adults and the indices are likely to have a more straightforward interpretation.
5 Conclussion
With everything exposed above it results crucial to determine optimal ways of identifying fluid responders among pediatric patients in order to improve our therapies and the medical care of our patients. As already proven static variables are not useful to guide volume expansion therapy and may lead us to major errors. Regarding dynamic parameters there are several promising variables. ΔVpeak, with the major evidence till now and the most studied one stands out as the most promising parameter.
Arterial waveform based variables seem to not be reliable but from our point of view, VTC challenge as it may overcome the PPV or SVV alone limitations while being an easy and accesible test for clinicians should be considered to study and validation among pediatric population.
We believe major efforts on identifying the best tests and parameters to identify fluid responsive children must be made in order to optime our use of volume expansion therapy and furthermore a study according to different ages may be useful as physiology varies so much.
Author contributions
FE: Conceptualization, Investigation, Methodology, Supervision, Writing – review & editing. AD: Conceptualization, Investigation, Methodology, Writing – review & editing, Writing – original draft. JJ: Conceptualization, Methodology, Writing – review & editing. CG: Supervision, Writing – review & editing. JE: Supervision, Visualization, Writing – review & editing. MH: Supervision, Validation, Visualization, Writing – review & editing. PA: Supervision, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Yenjabog P, Kanchongkittiphon W, Chutipongtanate S, Lertbunrian R, Ungprasert P. Dynamic parameters for fluid responsiveness in mechanically ventilated children: a systematic review. Front Pediatr. (2022) 10:1010600. doi: 10.3389/fped.2022.1010600
2. Gan H, Cannesson M, Chandler JR, Ansermino JM. Predicting fluid responsiveness in children: a systematic review. Anesth Analg. (2013) 117(6):1380–92. doi: 10.1213/ANE.0b013e3182a9557e
3. Coté CJ, Lerman J, Anderson B. A Practice of Anesthesia for Infants and Children. 6 edn Philadelphia, PA: Elsevier (2019). p. 1256.
4. Lee JH, Kim EH, Jang YE, Kim HS, Kim JT. Fluid responsiveness in the pediatric population. Korean J Anesthesiol. (2019) 72(5):429–40. doi: 10.4097/kja.19305
5. Karlsson J, Peters E, Denault A, Beaubien-Souligny W, Karsli C, Roter E. Assessment of fluid responsiveness in children using respiratory variations in descending aortic flow. Acta Anaesthesiol Scand. (2023) 67(8):1045–53. doi: 10.1111/aas.14265
6. Pinsky MR. Cardiopulmonary interactions: physiologic basis and clinical applications. Ann Am Thorac Soc. (2018) 15(Supplement_1):S45–8. doi: 10.1513/AnnalsATS.201704-339FR
7. Pinsky MR. Heart-lung interactions during mechanical ventilation. Curr Opin Crit Care. (2012) 18(3):256–60. doi: 10.1097/MCC.0b013e3283532b73
9. Papastamelos C, Panitch HB, England SE, Allen JL. Developmental changes in chest wall compliance in infancy and early childhood. J Appl Physiol Bethesda Md 1985. (1995) 78(1):179–84. doi: 10.1152/jappl.1995.78.1.179
10. Senzaki H, Akagi M, Hishi T, Ishizawa A, Yanagisawa M, Masutani S, et al. Age-associated changes in arterial elastic properties in children. Eur J Pediatr. (2002) 161(10):547–51. doi: 10.1007/s00431-002-1025-6
11. Luo D, Liu F, Dai W, Zhang J, Shao Q, Tao W, et al. Diagnostic accuracy of stroke volume variation for predicting fluid responsiveness in children undergoing cardiac surgery: a systematic review and meta-analysis. Paediatr Anaesth. (2021) 31(7):755–62. doi: 10.1111/pan.14195
12. Morparia KG, Reddy SK, Olivieri LJ, Spaeder MC, Schuette JJ. Respiratory variation in peak aortic velocity accurately predicts fluid responsiveness in children undergoing neurosurgery under general anesthesia. J Clin Monit Comput. (2018) 32(2):221–6. doi: 10.1007/s10877-017-0013-3
13. Messina A, Montagnini C, Cammarota G, Giuliani F, Muratore L, Baggiani M, et al. Assessment of fluid responsiveness in prone neurosurgical patients undergoing protective ventilation: role of dynamic indices, tidal volume challenge, and End-expiratory occlusion test. Anesth Analg. (2020) 130(3):752–61. doi: 10.1213/ANE.0000000000004494
14. Myatra SN, Prabu NR, Divatia JV, Monnet X, Kulkarni AP, Teboul JL. The changes in pulse pressure variation or stroke volume variation after a “tidal volume challenge” reliably predict fluid responsiveness during low tidal volume ventilation. Crit Care Med. (2017) 45(3):415–21. doi: 10.1097/CCM.0000000000002183
15. Ji SH, Jang YE, Park JB, Kang P, Cho SA, Kim EH, et al. Effect of tidal volume change on pressure-based prediction of fluid responsiveness in children. Paediatr Anaesth. (2023) 33(11):930–7. doi: 10.1111/pan.14751
16. Desgranges FP, Bouvet L, Pereira de Souza Neto E, Evain JN, Terrisse H, Joosten A, et al. Non-invasive measurement of digital plethysmographic variability index to predict fluid responsiveness in mechanically ventilated children: a systematic review and meta-analysis of diagnostic test accuracy studies. Anaesth Crit Care Pain Med. (2023) 42(3):101194. doi: 10.1016/j.accpm.2023.101194
17. Liu YF, Song LL, Ma W, Wang DX. Dynamic variables to predict fluid responsiveness in young children. Pediatr Int. (2023) 65(1):e15477. doi: 10.1111/ped.15477
18. Carioca FL, de Souza FM, de Souza TB, Rubio AJ, Brandão MB, Nogueira RJN, et al. Point-of-care ultrasonography to predict fluid responsiveness in children: a systematic review and meta-analysis. Paediatr Anaesth. (2023) 33(1):24–37. doi: 10.1111/pan.14574
19. Rowland DG, Gutgesell HP. Noninvasive assessment of myocardial contractility, preload, and afterload in healthy newborn infants. Am J Cardiol. (1995) 75(12):818–21. doi: 10.1016/S0002-9149(99)80419-6
Keywords: fluid therapy, children, responsiveness, pediatrics, PPV, SVV, ecocardiography, PVI
Citation: Escribá Alepuz F, Díaz Ruz A, Jiménez Santana JD, García Cebrián C, Encarnación J, Hervías Sanz M and Argente Navarro P (2024) Fluid responsiveness in pediatrics: an unsolved challenge. Front. Anesthesiol. 3:1430430. doi: 10.3389/fanes.2024.1430430
Received: 9 May 2024; Accepted: 21 October 2024;
Published: 6 November 2024.
Edited by:
Thomas Schricker, McGill University, CanadaReviewed by:
Geremia Zito Marinosci, AORN Santobono-Pausilipon, ItalyWasineenart Mongkolpun, Mahidol University, Thailand
Copyright: © 2024 Escribá Alepuz, Díaz Ruz, Jiménez Santana, García Cebrián, Encarnación, Hervías Sanz and Argente Navarro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: F. Escribá Alepuz, ZXNjcmliYTE5ODJAZ21haWwuY29t; A. Díaz Ruz, ZHJhZGlhenJ1ekBnbWFpbC5jb20=
†These authors have contributed equally to this work and share first authorship