 Miguel A. Valbuena-Bueno1*
Miguel A. Valbuena-Bueno1* Javier Ripollés-Melchor2,3*
Javier Ripollés-Melchor2,3* Alicia Ruiz-Escobar2,3
Alicia Ruiz-Escobar2,3 Paula Fernández-Valdes-Bango2,3
Paula Fernández-Valdes-Bango2,3 Juan V. Lorente4,5
Juan V. Lorente4,5 Alfredo Abad-Gurumeta2,3
Alfredo Abad-Gurumeta2,3 M. Ignacio Monge-García4,6
M. Ignacio Monge-García4,6
- 1Universidad Politécnica de Madrid, Madrid, Spain
- 2Department of Anesthesia, Infanta Leonor University Hospital, Madrid, Spain
- 3Department of Pharmacology and Toxicology, Universidad Complutense de Madrid, Spain
- 4Fluid Therapy and Hemodynamic Monitoring Group of the Spanish Society of Anesthesiology and Critical Care, Huelva, Spain
- 5Department of Anesthesia, Juan Ramón Jiménez University Hospital, Huelva, Spain
- 6Department of Critical Care, Jerez de la Frontera University Hospital, Spain
Intraoperative hypotension (IOH) poses significant risks during surgeries, necessitating effective management to ensure patient safety and successful outcomes. The Hypotension Prediction Index (HPI) software was developed as a decision support model to assist anesthesiologists in monitoring and addressing hypotensive episodes during non-cardiac surgeries. We have utilized the predictive capabilities of HPI and the physiological variables provided by the Hemosphere monitor to create a Decision Support System (HPI-DSS) for hemodynamic management. This article presents a comprehensive overview of the HPI-DSS, detailing its model for hemodynamic decision support. The system's performance and its ability to enhance intraoperative management are discussed. The article explores the methodology, results, and limitations of the HPI-DSS. It also covers potential applications of the system and offers suggestions for further research to improve and refine its capabilities.
Introduction
Hemodynamic optimization in perioperative care involves two main priorities: volume optimization and maintaining arterial blood pressure within acceptable physiological ranges. To prevent excessive or insufficient fluid intake, a hemodynamic optimization strategy guided by advanced cardiac output (CO) monitoring has been recommended for high-risk surgical patients (1). This approach aims to tailor treatments by prescribing fluids and vasopressor/inotropic medications based on hemodynamic indexes such as stroke volume (SV) and CO (2). Several studies have shown that implementing this strategy can reduce postoperative complications (3). The association between low hypotension and postoperative complications, particularly renal and cardiovascular complications, has been extensively observed. Large-scale observational prospective studies have suggested a possible causal link between perioperative hypotension and postoperative morbidity (4). As a result, a tailored hemodynamic approach that simultaneously optimizes flow and mean arterial pressure (MAP) has been proposed for high-risk patients to reduce postoperative complications (5).
The Hypotension Prediction Index (HPI) software (Edwards Lifesciences) is a valuable tool in the management of intraoperative hypotension (IOH). The HPI software utilizes advanced algorithms and machine learning (ML) techniques to analyze real-time hemodynamic data and generate predictive indicators of impending hypotensive events (6). The HPI software can identify patterns and trends that may indicate an increased risk of hypotension. This early warning system allows anesthesiologists to intervene before complications arise, and allows for proactive interventions, such as fluid administration, vasopressor use, or adjustments in anesthesia management, to maintain stable blood pressure, potentially preventing adverse outcomes (7).
To enhance adherence to hemodynamic optimization protocols, interactive tools such as decision-making support systems and automated devices are being developed (8, 9). These advancements have the potential to facilitate the widespread implementation of hemodynamic optimization practices and improve patient outcomes. Based on the predictive capabilities of HPI, as well as the physiological variables offered by the Hemosphere monitor (Edwards Lifesciences), we have created a Decision support system (HPI-DSS) for hemodynamic management, which through dedicated software and by obtaining real-time data from the Hemosphere platform, allows for comprehensive hemodynamic management guidance.
Methods
The aim of this study was to develop an assisted Decision support system (HPI-DSS) based on a hemodynamic algorithm (Figure 1) that has been shown to reduce IOH practically to zero when used in centers with expertise in the management of HPI (10). While the Predict-H study laid the foundation for using HPI in hemodynamic management (10), our study introduces significant enhancements by integrating additional hemodynamic parameters and a comprehensive HPI-DSS. This integration aims to provide a more nuanced and precise approach to managing intraoperative hypotension, thereby expanding upon the groundwork established by Predict-H.

Figure 1. Hemodynamic therapeutic algorithm.
This HPI-DSS utilized the hemodynamic parameters provided by the Edwards Hemosphere monitoring system with the HPI software during surgical interventions (Table 1). The goal was to improve the management of arterial hypotension and intraoperative hemodynamics. The study followed a retrospective observational design, collecting data from eligible patients undergoing elective surgery. After create the software, new data were collected and analyzed in real-time using the developed application.
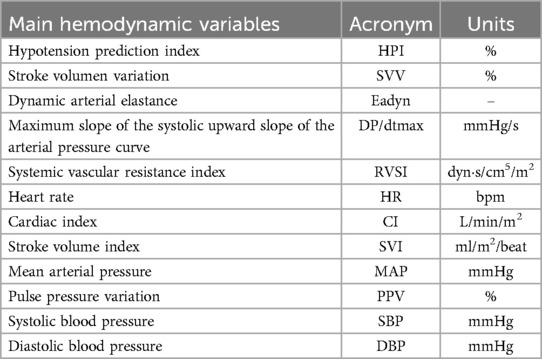
Table 1. Hemodynamic parameters provided by the monitor.
Inclusion criteria
All hemodynamic data was collected from patients with at least 18 years old and had an American Society of Anesthesiologists (ASA) physical status of 2–4 who underwent scheduled major abdominal surgery with an anticipated operative duration of at least 90 min. The surgeries were performed in a center where anesthesiologists had previously received training in the use of the HPI software for predicting and managing arterial hypotension during surgery.
The sample size for this observational, retrospective study was determined based on the availability of relevant patient data within the study period and the need to detect clinically meaningful differences in outcomes. The sample size was influenced by the existing data and the inherent variability in the time-weighted average (TWA) of hypotension across different surgical populations. This variability necessitates a larger sample to ensure robust and generalizable findings. We also recognize that the TWA of hypotension can vary significantly between individuals and surgical procedures, further justifying our sample size.
Method description
Data extraction and processing
Data were extracted in real-time from patients undergoing elective surgery who required intraoperative monitoring through an invasive arterial line connected to the Edwards Hemosphere monitoring system with the HPI software. The data extraction process followed the instructions provided in the Hardware Connection Guide available on the VitalDB website.
Once the monitoring system was successfully connected to a personal computer, the data processing phase began. Each individual reading from the monitoring system was considered as an independent “case.”
The processing of each reading involved obtaining three essential elements: hemodynamic parameters not provided by the monitor (Table 2), the phenotype of the case, and the trend of the HPI over time (Equation 1). These elements were crucial for the subsequent analysis and decision-making process. To extract the hemodynamic parameters not provided by the monitor, mathematical calculations and algorithms were applied to the available data. These calculations allowed for the estimation of parameters such as systemic vascular resistance (SVR). The inclusion of these additional parameters provided a more comprehensive understanding of the patient's hemodynamic status. The phenotype of each case was determined based on the processed data. The algorithm used a combination of the obtained hemodynamic parameters, their trends over time, and predefined thresholds to classify the patient into different phenotypes or subtypes of hemodynamic instability. This classification was crucial for tailoring the appropriate treatment interventions for each patient.
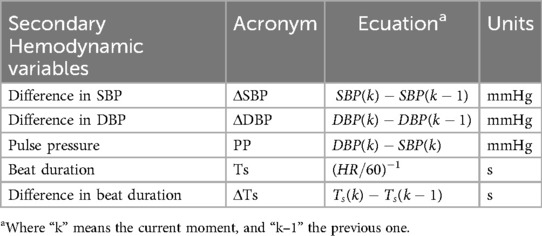
Table 2. Hemodynamic parameters not provided by the monitor.
Hemodynamic instability (HI) was defined as an HPI value greater than 80% based on the results of the hypotension prediction analysis compared to the actual occurrence of hypotensive events in the HPI validation study. The study defined different types of HI based on a clinical decision-making therapeutic protocol grounded in cardiovascular pathophysiology. Intraoperative HI is a critical condition associated with significant postoperative morbidity and mortality. Accurate identification and classification of IHI subtypes are essential for effective therapeutic intervention. Based on cardiovascular pathophysiology, we have defined five distinct patterns of IHI: absolute hypovolemia, relative hypovolemia, vasoplegia, myocardial depression, and myocardial depression with vasoplegia. Absolute hypovolemia is characterized by a stroke volume variation (SVV) greater than 13% and an arterial elastance (Eadyn) greater than 1, indicating a significant reduction in intravascular volume that can compromise cardiac output. Relative hypovolemia presents with an SVV greater than 13% and an Eadyn less than 1, reflecting a redistribution of intravascular volume without an absolute loss, still affecting preload and cardiac function. Vasoplegia, defined by an SVV less than 13% and a peak arterial pressure derivative (dP/dt) greater than 400 mmHg/s, suggests excessive vasodilation with decreased systemic vascular resistance. Myocardial depression with vasoplegia, characterized by an SVV less than 13%, a dP/dt less than 400 mmHg/s, and a systemic vascular resistance index (SVRI) less than 1,500 dyn s/cm5/m2, indicates myocardial contractile dysfunction combined with vasodilation, presenting a particularly challenging management scenario. Myocardial depression, defined by an SVV less than 13%, a dP/dt less than 400 mmHg/s, and an SVRI greater than 1,500 dyn s/cm5/m2, reflects decreased myocardial contractility without significant vasodilation.
The classification of these subtypes is based on the necessity to identify the underlying pathophysiological mechanism to select the appropriate therapy.
The systemic vascular resistance index (SVRI) was calculated by subtracting the central venous pressure (CVP) from the MAP, dividing by the cardiac index (CI), and multiplying by 80. If continuous measurement of CVP was not available, a fixed value of 5 mmHg was used.
We only consider that the patient has entered a hypotensive episode when we received three consecutive cases (samples) with the same phenotype, because the sample rate of the HPI system is 3 cases per minute.
Graphical representation
Various types of graphs were used in the HPI-DSS to visually represent the trends and results. Line charts were used to display the progression of the HPI over time, showing both the “HPI in the last 5 min” and the “HPI since the beginning of the surgical operation”. These line charts provided a comprehensive view of the HPI trends throughout the surgical procedure. Spider plots were utilized to depict the current state of the patient, including any present phenotype, and the phenotype of the last episode. These plots enabled an assessment of the patient's evolution and facilitated the identification of patterns or changes in the patient's condition (Figures 2, 3).
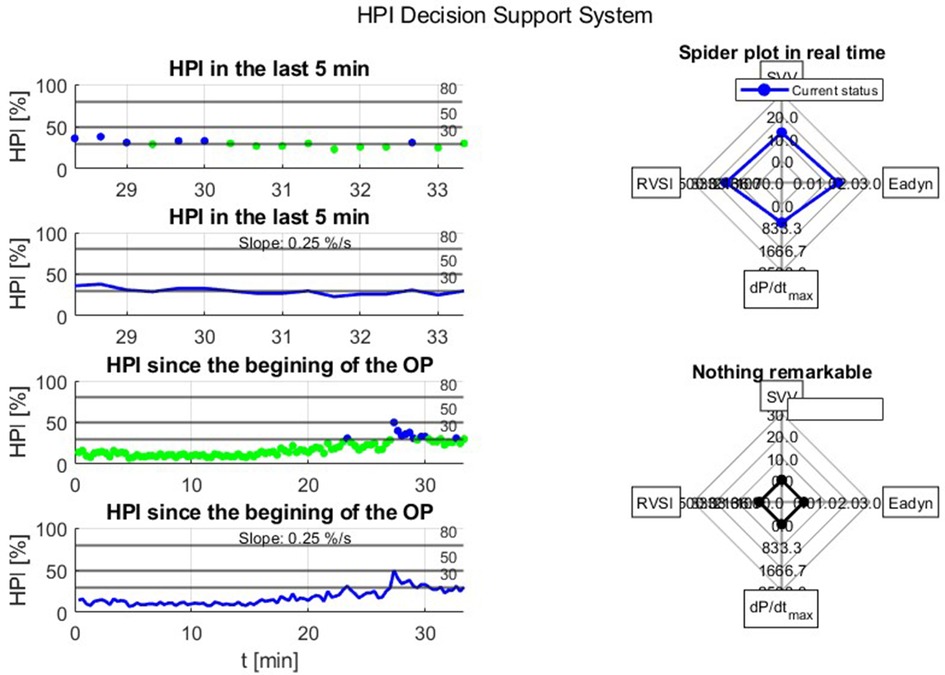
Figure 2. Normal operation of the decision support system HPI.
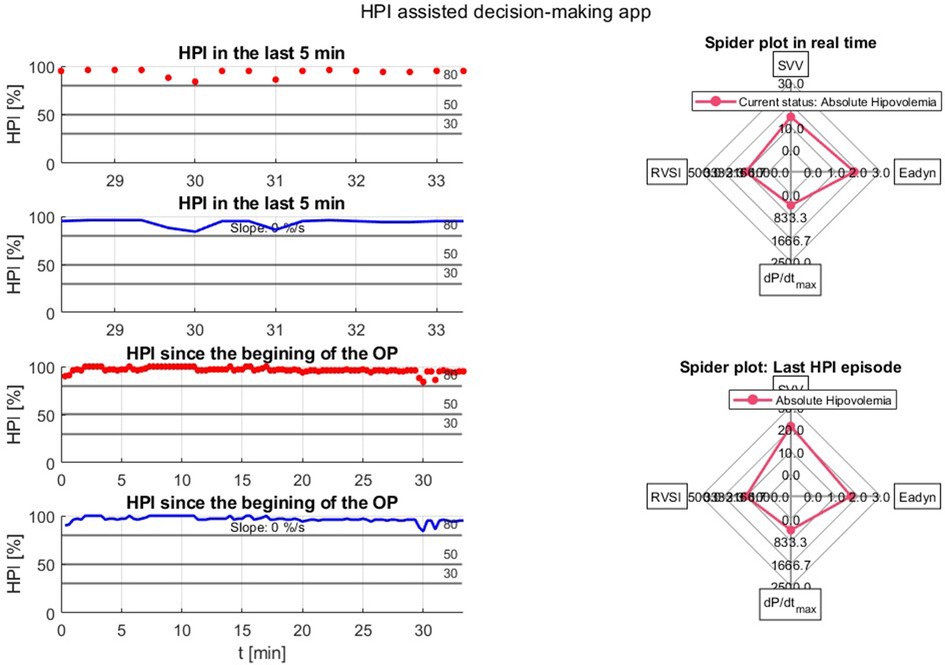
Figure 3. Hipotensive event in the decision support system HPI.
An alert pop-up system was implemented in the HPI-DSS to show changes in the patient's HPI value (Table 3). The system consisted of three types of alerts: Stability (HPI < 50) (Figures 4, 5), Alert (HPI < 80) (Figure 6), and Warning (HPI > 80) (Figure 7). Each alert type in the decision assistance system provided a suggested course of action based not only on the severity of the HPI value but also in combination with multiple parameters such as SVV, Eadyn, and dP/dt. For example, an alert for impending hypotension would suggest interventions based on a low HPI value combined with a high SVV and low dP/dt. This integrated approach ensures that the recommended actions are tailored to the patient's specific hemodynamic profile, providing a more targeted and effective management strategy. For the Stability notification, two scenarios were differentiated: when the HPI was below 30 and when it was above 30 but below 50. This differentiation allowed for appropriate action to be taken based on the specific HPI range. In the warning notification, not only was immediate action suggested, but a specific treatment recommendation based on the diagnosed phenotype was also provided. This enhanced the clinical decision-making process and ensured timely intervention.
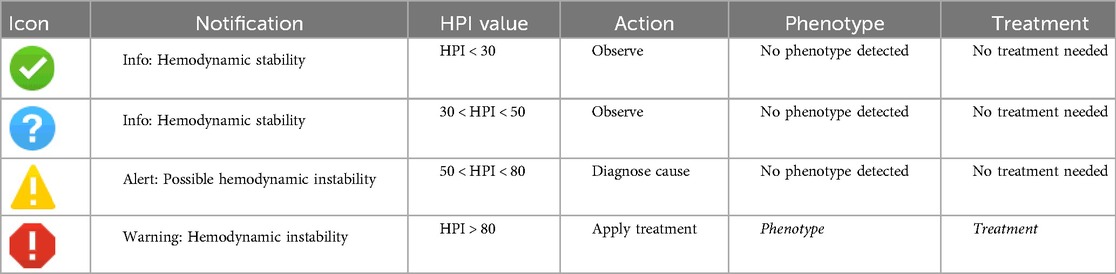
Table 3. HPI alert system.
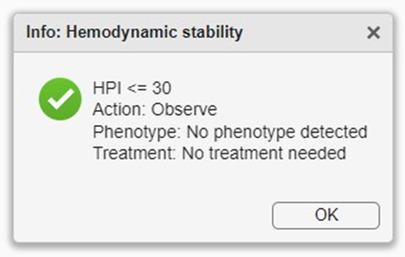
Figure 4. Stability notification with HPI < 30.
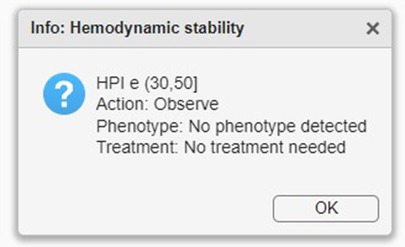
Figure 5. Stability notification with 30 < HPI < 50.
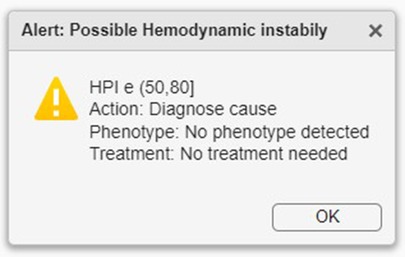
Figure 6. Alert notification.
Figure 7. Warning notification.
Our algorithm is based on the HPI-guided hemodynamic management proposed by Lorente et al (10), and is grounded on the hypotension alert provided by HPI in combination with SVV, the maximum rise of arterial pressure (dP/dtmax) as a surrogate for assessing left ventricular contractility, and dynamic arterial elastance (Eadyn) for determining the pressure-responsiveness. This hemodynamic optimization protocol aims to prevent the main mechanisms leading to arterial hypotension: hypovolemia, impaired contractility, and vasoplegia. When HPI rises above 80%, the HPI-DSS first check the SVV, if SVV is <13% and dP/dtmax is >400 mmHg s, a vasoconstrictor is recommended, whereas an inotrope is recommended if dP/dtmax is <400 mmHg s. On the other hand, if SVV is >13% and the Eadyn value is >1, a fluid bolus of 250 ml of colloid is recommended, while a vasoconstrictor is recommended if the Eadyn is <1.
In addition to the graphical representation and alert system, the application also facilitated communication and reporting. Sample numbers and HPI slopes were communicated to the relevant healthcare providers through text messages. This real-time communication allowed for prompt awareness and response to changes in the patient's hemodynamic status. Furthermore, the HPI-DSS generated comprehensive reports summarizing the patient's hemodynamic parameters, HPI trends, and phenotype classification. These reports were automatically generated at the end of each surgical procedure and could be easily accessed and shared with the healthcare team for further analysis and documentation.
The entire methodology was implemented using MATLAB® (R2023a), a programming and numerical computing platform. MATLAB provided the necessary tools for data extraction, processing, graphical representation, alert system implementation, communication, and reporting.
Discussion
Our decision support system based on the HPI model provides significant value by offering healthcare professionals real-time information and precise recommendations for managing hemodynamics and preventing arterial hypotension during the intraoperative and postoperative periods. By combining clinical expertise with objective data and algorithms, our system enhances the accuracy and efficiency of decision-making, optimizing patient care and reducing the risks associated with IOH.
Many organizations, including some European medical societies, developed and approved Goal-Directed Hemodynamic Therapy (GDHT) protocols for perioperative hemodynamic management(11, 12) but the complexity and diversity of the GDHT algorithms make them difficult to implement, so the compliance with this algorithm is often poor (13). Joosten et al. assessed the effects of using a real time clinical decision-support system, Assisted Fluid Management (AFM), to guide GDFT during major abdominal surgery. They showed that patients in the AFM group spent more time during surgery with hemodynamic stability, defined as time with stroke volume variation <13% (14). Similarly, for patients with intermediate to high risk surgery, computer-assisted personalized hemodynamic management significantly reduces intraoperative hypotension compared to manual targeting (15).
The HPI is a monitoring tool based on ML and one of the first ML-derived predictive algorithms used in the perioperative period (6). Recent trials have compared the HPI-guided approach with standard intraoperative hemodynamic management, with or without GDHT that did not incorporate HPI. The results overwhelmingly favored the implementation of HPI-guided management, leading to a notable decrease in IOH (10, 16, 17). HPI-based management has proven to be a proactive and effective strategy, ensuring hemodynamic stability. However, to achieve a significant reduction in IOH with the HPI-based approach, it is crucial for responsible clinicians to fully comply with the treatment protocol (18). To address this issue, implementing an HPI-based assisted decision system could assist clinicians in adhering to hemodynamic protocols, promoting consistency and optimal patient care, ultimately leading to a decrease in IOH. One of the key strengths of the HPI-DSS is its ability to provide predictive indicators of impending hypotensive episodes. By analyzing real-time hemodynamic data, the software generates an HPI-based assisted decision support that helps anesthesiologists identify patients at risk of developing hypotension. This early warning system enables proactive interventions, such as fluid administration, vasopressor use, or adjustments in anesthesia management, to maintain stable blood pressure. Furthermore, the visual representations of HPI trends and the patient's hemodynamic profile offer a clear and accessible overview, facilitating quick assessment of the severity and trajectory of hypotensive events. The graphical interface enhances the usability of the software, enabling efficient and intuitive navigation for healthcare professionals.
However, the HPI-DSS does have limitations that need to be addressed. An important consideration in the performance of the HPI-DSS is the inherent uncertainty associated with the FloTrac platform. While the FloTrac system has evolved, significant clinical variations persist in its ability to calculate cardiac output, especially during the administration of vasopressors or changes in arterial waveform characteristics (19). This uncertainty must be explicitly acknowledged and addressed when evaluating the utility and reliability of the HPI-DSS. Data accuracy is a critical concern, as the reliability and quality of hemodynamic data extracted from monitoring systems can be affected by noise, artifacts, and calibration errors. Ensuring accurate data acquisition is essential for the HPI software—and the HPI-DSS—to generate reliable predictions. Regular calibration checks and quality control measures should be implemented to minimize data inaccuracies and improve the overall reliability of the software. Additionally, usability is another crucial aspect of any decision support tool, including the HPI-DSS. The user interface and overall usability of the software have been carefully designed and tested to ensure ease of use and user satisfaction. Incorporating user feedback and iterative testing can help identify and address any usability issues, further improving the software's interface and functionality.
Implementing the HPI-DSS requires addressing potential biases that may arise from skewed or incomplete training data. Ensuring representative and unbiased training data is crucial for accurate recommendations. Regular evaluation and refinement of the algorithm can help mitigate biases arising from flawed assumptions or inherent biases in the training data, enhancing the reliability and effectiveness of the decision support system. Despite potential biases, the HPI-DSS offers several advantages over closed-loop systems, providing flexibility and adaptability for personalized decision-making based on individual patient variability and real-time changes in hemodynamic status. By incorporating healthcare professionals' clinical expertise with objective data from the HPI software, informed decision-making is facilitated, leading to improved patient management and clinical outcomes.
By utilizing the HPI decision support system, healthcare professionals can receive real-time information and recommendations to guide their management of arterial hypotension, benefiting both physicians responsible for critical decisions during surgery and nurses monitoring patients' hemodynamic status and implementing interventions.
Furthermore, the HPI-DSS also has research implications, allowing for large-scale data collection and analysis to further understand the impact of IOH on patient outcomes and evaluate the effectiveness of interventions. Prospective clinical trials in diverse surgical settings are needed to validate the software's effectiveness and assess its impact on patient outcomes. Customization based on individual patient characteristics and surgical procedures should be explored to improve prediction accuracy and provide personalized recommendations for IOH management. Ultimately, integrating the HPI-DSS into clinical practice can enhance patient safety, improve surgical outcomes, and optimize perioperative hemodynamic management.
For the HPI-DSS to be widely adopted in clinical practice, it is crucial that our findings are validated through extensive real-world testing. Such studies should be conducted by independent groups to ensure objectivity and mitigate any potential biases. These efforts will help ascertain the generalizability and robustness of the HPI-DSS across diverse clinical settings.
Conclusion
The Hypotension Prediction Index Decision support system offers a model for decision support in the management of intraoperative hypotension. By leveraging real-time hemodynamic data and providing predictive indicators, the software empowers anesthesiologists to proactively address and manage hypotensive episodes, leading to improved patient safety and outcomes. However, further research, validation, customization, and integration efforts are necessary to address limitations and enhance the applicability and effectiveness of the HPI-DSS in various clinical settings.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Infanta Leonor University Hospital Ethics Committee, Madrid, Spain. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
MV-B: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. JR-M: Conceptualization, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AR-E: Investigation, Visualization, Writing – review & editing. PF-V-B: Investigation, Supervision, Visualization, Writing – review & editing. JL: Conceptualization, Validation, Visualization, Writing – review & editing. AA-G: Investigation, Supervision, Visualization, Writing – review & editing. MM-G: Conceptualization, Data curation, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
JR-M: Payments for conferences and served as advisor board from Edwards Lifesciences. JL: Payments for conferences and served as advisor board from Edwards Lifesciences. MM-G: has been employee and is currently clinical consultant for Edwards Lifesciences. MV-B, AR-E and PF-V-B declare that this review was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. Edwards Lifesciences was not involved in the design, conduct of the review, collection, management, analysis, or interpretation of the data, preparation, and review of the manuscript, or in the decision to publish.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Pinsky MR, Cecconi M, Chew MS, De Backer D, Douglas I, Edwards M, et al. Effective hemodynamic monitoring. Crit Care. (2022) 26:294. doi: 10.1186/s13054-022-04173-z
2. Calvo-Vecino JM, Ripollés-Melchor J, Mythen MG, Casans-Francés R, Balik A, Artacho JP, et al. Effect of goal-directed haemodynamic therapy on postoperative complications in low–moderate risk surgical patients: a multicentre randomised controlled trial (FEDORA trial). Br J Anaesth. (2018) 120:734–44. doi: 10.1016/j.bja.2017.12.018
3. Chong MA, Wang Y, Berbenetz NM, McConachie I. Does goal-directed haemodynamic and fluid therapy improve peri-operative outcomes? Eur J Anaesthesiol. (2018) 35:469–83. doi: 10.1097/EJA.0000000000000778
4. Wesselink EM, Kappen TH, Torn HM, Slooter AJC, van Klei WA. Intraoperative hypotension and the risk of postoperative adverse outcomes: a systematic review. Br J Anaesth. (2018) 121:706–21. doi: 10.1016/j.bja.2018.04.036
5. Futier E, Lefrant J-Y, Guinot P-G, Godet T, Lorne E, Cuvillon P, et al. Effect of individualized vs standard blood pressure management strategies on postoperative organ dysfunction among high-risk patients undergoing major surgery: a randomized clinical trial. JAMA. (2017) 318:1346–57. doi: 10.1001/jama.2017.14172
6. Hatib F, Jian Z, Buddi S, Lee C, Settels J, Sibert K, et al. Machine-learning algorithm to predict hypotension based on high-fidelity arterial pressure waveform analysis. Anesthesiology. (2018) 129:663–74. doi: 10.1097/ALN.0000000000002300
7. Ripollés-Melchor J, Ruiz-Escobar A, Fernández-Valdes-Bango P, Lorente JV, Jiménez-López I, Abad-Gurumeta A, et al. Hypotension prediction index: from reactive to predictive hemodynamic management, the key to maintaining hemodynamic stability. Front Anesthesiol. (2023) 2:1138175. doi: 10.3389/fanes.2023.1138175
8. Michard F. Decision support for hemodynamic management: from graphical displays to closed loop systems. Anesth Analg. (2013) 117:876–82. doi: 10.1213/ANE.0b013e31827e5002
9. Maheshwari K, Malhotra G, Bao X, Lahsaei P, Hand WR, Fleming NW, et al. Assisted fluid management software guidance for intraoperative fluid administration. Anesthesiology. (2021) 135:273–83. doi: 10.1097/ALN.0000000000003790
10. Lorente JV, Ripollés-Melchor J, Jiménez I, Becerra AI, Mojarro I, Fernández-Valdes-Bango P, et al. Intraoperative hemodynamic optimization using the hypotension prediction index vs. Goal-directed hemodynamic therapy during elective major abdominal surgery: the predict-H multicenter randomized controlled trial. Front Anesthesiol. (2023) 2:1193886. doi: 10.3389/fanes.2023.1193886
11. Ripollés-Melchor J, Chappell D, Aya HD, Espinosa Á, Mhyten MG, Abad-Gurumeta A, et al. Fluid therapy recommendations for major abdominal surgery. Via RICA recommendations revisited. Part III: goal directed hemodynamic therapy. Rationale for maintaining vascular tone and contractility. Rev Esp Anestesiol Reanim. (2017) 64:348–59. doi: 10.1016/j.redar.2017.03.002
12. Bloc S, Alfonsi P, Belbachir A, Beaussier M, Bouvet L, Campard S, et al. Guidelines on perioperative optimization protocol for the adult patient 2023. Anaesth Crit Care Pain Med. (2023) 42:101264. doi: 10.1016/j.accpm.2023.101264
13. Boekel MF, Venema CS, Kaufmann T, van der Horst ICC, Vos JJ, Scheeren TWL. The effect of compliance with a perioperative goal-directed therapy protocol on outcomes after high-risk surgery: a before-after study. J Clin Monit Comput. (2021) 35:1193–202. doi: 10.1007/s10877-020-00585-w
14. Joosten A, Hafiane R, Pustetto M, Van Obbergh L, Quackels T, Buggenhout A, et al. Practical impact of a decision support for goal-directed fluid therapy on protocol adherence: a clinical implementation study in patients undergoing major abdominal surgery. J Clin Monit Comput. (2019) 33:15–24. doi: 10.1007/s10877-018-0156-x
15. Joosten A, Rinehart J, Van der Linden P, Alexander B, Penna C, De Montblanc J, et al. Computer-assisted individualized hemodynamic management reduces intraoperative hypotension in intermediate- and high-risk surgery: a randomized controlled trial. Anesthesiology. (2021) 135(2):258–72. doi: 10.1097/ALN.0000000000003807
16. Solares GJ, Garcia D, Monge Garcia MI, Crespo C, Rabago JL, Iglesias F, et al. Real-world outcomes of the hypotension prediction index in the management of intraoperative hypotension during non-cardiac surgery: a retrospective clinical study. J Clin Monit Comput. (2023) 37:211–20. doi: 10.1007/s10877-022-00881-7
17. Grundmann CD, Wischermann JM, Fassbender P, Bischoff P, Frey UH. Hemodynamic monitoring with hypotension prediction Index versus arterial waveform analysis alone and incidence of perioperative hypotension. Acta Anaesthesiol Scand. (2021) 65:1404–12. doi: 10.1111/aas.13964
18. Wijnberge M, Geerts BF, Hol L, Lemmers N, Mulder MP, Berge P, et al. Effect of a machine learning-derived early warning system for intraoperative hypotension vs standard care on depth and duration of intraoperative hypotension during elective noncardiac surgery: the HYPE randomized clinical trial. JAMA. (2020) 323:1052–60. doi: 10.1001/jama.2020.0592
19. Murata Y, Imai T, Takeda C, Mizota T, Kawamoto S. Agreement between continuous cardiac output measured by the fourth-generation FloTrac/vigileo system and a pulmonary artery catheter in adult liver transplantation. Sci Rep. (2022) 12(1):11198. Published 2022 July 1. doi: 10.1038/s41598-022-14988-z
Keywords: blood pressure, blood pressure determination methods, hemodynamics therapy, computer-assisted methods, hypotension prevention & control, machine learning
Citation: Valbuena-Bueno MA, Ripollés-Melchor J, Ruiz-Escobar A, Fernández-Valdes-Bango P, Lorente JV, Abad-Gurumeta A and Monge-García MI (2024) Hypotension prediction index decision support system: a new model for decision support in hemodynamic management. Front. Anesthesiol. 3:1405397. doi: 10.3389/fanes.2024.1405397
Received: 22 March 2024; Accepted: 5 August 2024;
Published: 29 August 2024.
Edited by:
Hong Liu, UC Davis Health, United StatesReviewed by:
Aveek Jayant, Homi Bhabha Cancer Hospital and Research Centre, IndiaDavid Li, UC Davis Medical Center, United States
Zhengmin Ma, The First Affiliated Hospital of Soochow University, China
Copyright: © 2024 Valbuena-Bueno, Ripollés-Melchor, Ruiz-Escobar, Fernández-Valdes-Bango, Lorente, Abad-Gurumeta and Monge-García. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Miguel A. Valbuena-Bueno, bWlndWVsLnZhbGJ1ZW5hLmJ1ZW5vQGFsdW1ub3MudXBtLmVz