 Natalie Rall1
Natalie Rall1 Niaman Nazir
Niaman Nazir Grace Giron
Grace Giron
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Anesthesiol. , 19 July 2024
Sec. Neuroanesthesiology
Volume 3 - 2024 | https://doi.org/10.3389/fanes.2024.1388407
Background: Timing of endovascular treatment (EVT) for acute ischemic stroke (AIS) is important for achieving improved patient outcomes. Studies have evaluated how the type of anesthesia administered may impact the timing of EVT for AIS and patient outcomes, but there is limited data regarding how the presence of an anesthesia team can influence these metrics. Against this background, this study aims to compare time metrics and patient outcomes pre- vs. postroutine involvement of a dedicated anesthesia team dealing with EVT cases.
Methods: All patients at our institution who were between 18 and 100 years of age and evaluated for stroke and determined to be candidates for EVT during the period between November 2018 and November 2020 were considered for this study. Time metrics associated with EVT, which are commonly tracked by stroke centers, were compared pre- vs. postroutine involvement of a dedicated anesthesia team dealing with EVT cases. Secondary outcomes were a modified Rankin scale at time of discharge, an NIH Stroke Scale score at time of presentation and discharge, and incidence of intraprocedural hypotension.
Results: A total of 255 patients were included. A comparison of pre- (n = 119) vs. postneuroanesthesia team involvement (n = 136) in EVT for AIS revealed a statistically significant decrease in median time from puncture to TICI score >2b in the in-house group from 49.00 min preinvolvement to 23.00 min postinvolvement (P = 0.02) and puncture to TICI >2b (39.5 vs. 34 min, P = 0.01) for all patient categories when controlling for anesthesia type. The rate of incidence of intraprocedural hypotension (mean arterial pressure < 65 mmHg) also decreased significantly from 79% to 44% (P = 0.04), although it was not significant when controlling for anesthesia type (P = 0.05).
Conclusions: Routine involvement of a dedicated anesthesia team for EVT in patients with AIS could potentially improve stroke metrics and patient outcomes, although more studies are necessary to validate this model of care.
Endovascular treatment (EVT) of strokes allows for clots to be retrieved or dissolved through clot retrieval devices or a tissue plasminogen activator (tPA), respectively, even after the window for intravenous tPA expires. Studies have shown that decreased time to the start of EVT and decreased time to reperfusion during EVT are associated with better clinical outcomes, including a higher level of functional independence, decreased incidence of intracranial hemorrhage, and decreased or neutral effects on mortality (1–3). In addition, a large pool of studies has evaluated how anesthesia type [general anesthesia (GA) vs. conscious sedation (CS)] may influence both patient outcomes and timing of EVT for acute ischemic stroke (AIS) (4–9). For instance, induction time associated with general anesthesia could lead to a delayed start of procedures, or patient movement under conscious sedation could lead to procedure complications that may cause further delays in timing that could impact outcomes (4, 5). While studies have shown the importance of decreasing time to the start of EVT, there is limited data regarding how a routine involvement of a dedicated anesthesia team may influence stroke metrics and patient outcomes.
The Society of Neuroscience in Anesthesiology and Critical Care (SNACC) guidelines state the following: “given the emergent and complex nature of the interventional procedures for AIS, frequent association of multiple comorbidities in stroke patients, and the need for strict hemodynamic management and ensuring homeostasis, an anesthesiologist/anesthesia team should be present to provide sedation and hemodynamic monitoring” (10). At our comprehensive stroke center, there was no routine involvement of an anesthesia team for EVT of strokes prior to November 2019, in which patients received conscious sedation by a procedure nurse. Our neuroanesthesia team became involved only if there was inadvertent oversedation, excessive patient movement, significant patient comorbidities, or inability to protect the patient's airway. Evaluating the patient mid-procedure, sedating, or inducing general anesthesia, and securing an airway mid-EVT are all not ideal clinical practices; thus, it was determined that the in-house anesthesia team would anesthetize every EVT case for AIS. Against this background, this study aims to compare stroke time metrics and other stroke data pre- vs. postroutine involvement of a dedicated anesthesia team for EVT cases to determine whether having such a team will improve patient outcomes (1, 2).
Our Institutional Review Board waived the requirement for informed consent because of the retrospective nature of this study. The primary study objectives were to compare the following time metrics pre- vs. postroutine anesthesia team involvement for the treatment of AIS with EVT: (1) door-to-arrival in interventional radiology (IR), (2) IR arrival-to-puncture, and (3) puncture-to-satisfactory thrombolysis in cerebral infarction scale (TICI) defined as >2b. Additional outcomes included the incidence of intraprocedural hypotension [mean arterial pressure (MAP) < 65 mmHg], a National Institute of Health Stroke Scale (NIHSS) score at presentation and time of discharge, and a modified Rankin scale (mRS) score at time of discharge (11, 12). The type of anesthesia administered [conscious sedation, general anesthesia, or monitored anesthesia care (MAC)] was also recorded.
Patient data for all specified outcomes were obtained from our institution's stroke center intervention reports and patient medical records. All patients aged between 18 and 100 years with AIS who were determined to be candidates for EVT between 6 November 2018 and 6 November 2020 were considered for inclusion in the study. Patients with incorrect information or inaccessible and/or duplicate charts were excluded from the study. Patients were also excluded if they were enrolled in other studies or initially considered for EVT but only had an angiogram and/or IV tPA. The included patients were categorized into either the pre- or postroutine anesthesia team involvement group. Data were also subcategorized based on the patients’ arrival type: emergency department (ED), transfer, or in-house. The first two and last two data points of the anesthetic timeline were excluded because of the likelihood that these may be errant measurements.
Descriptive statistics were calculated. Categorical variables were summarized by frequencies and percentages, and continuous variables were summarized by means and standard deviations. Chi-square tests were conducted to make global comparisons of categorical variables across groups. Independent two-sample t-tests were used to make global comparisons of the means across the two groups. In instances where data were skewed, a non-parametric Wilcoxon two-sample test was used to compare medians across the two groups. Primary and secondary objectives were also compared across the two groups controlling for anesthesia type using regression models. Data management and statistical analysis were performed using SAS software [version 9.4, Copyright (c) 2002–2012, SAS Institute Inc., Cary, NC, USA]. Two-sided P-values less than 0.05 were considered statistically significant.
A total of 402 patients were identified within the study period. Of these 402 patients, 255 patients were included in the final data analysis; of these 255, 119 patients were in the preanesthesia team involvement group, and 136 were in the postinvolvement group (Figure 1). The mean age was 64.65 vs. 66.86 years in the pre- and postgroups, respectively. In both groups, 53% were male and 47% female. Preinvolvement, 34 patients (29%) arrived from the ED, 76 (64%) were outside hospital transfers, and 9 (7%) were already in-house. Postinvolvement, 32 patients (24%) arrived from the ED, 93 (68%) were outside hospital transfers, and 11 (8%) were already in-house. Of the total number of patients (N = 255), we had missing values of 166 (65%) for mRS and 153 (60%) for NIHSS at discharge. Stratifying by preinvolvement and postinvolvement groups, the pattern of distribution was 74 missing for mRS and 59 missing for NIHSS in the preinvolvement group. Similarly, it was 92 missing for mRS and 94 missing for NIHSS in the postinvolvement group. There was no statistically significant difference between the two groups with respect to the category of patient arrival or NIHSS score on arrival. These demographic characteristics are summarized in Table 1. The differences in the mRS score at discharge and NIHSS score at discharge were not statistically significant, even when adjusted for anesthesia type, and when using multiple imputation to account for missing values (Table 2).
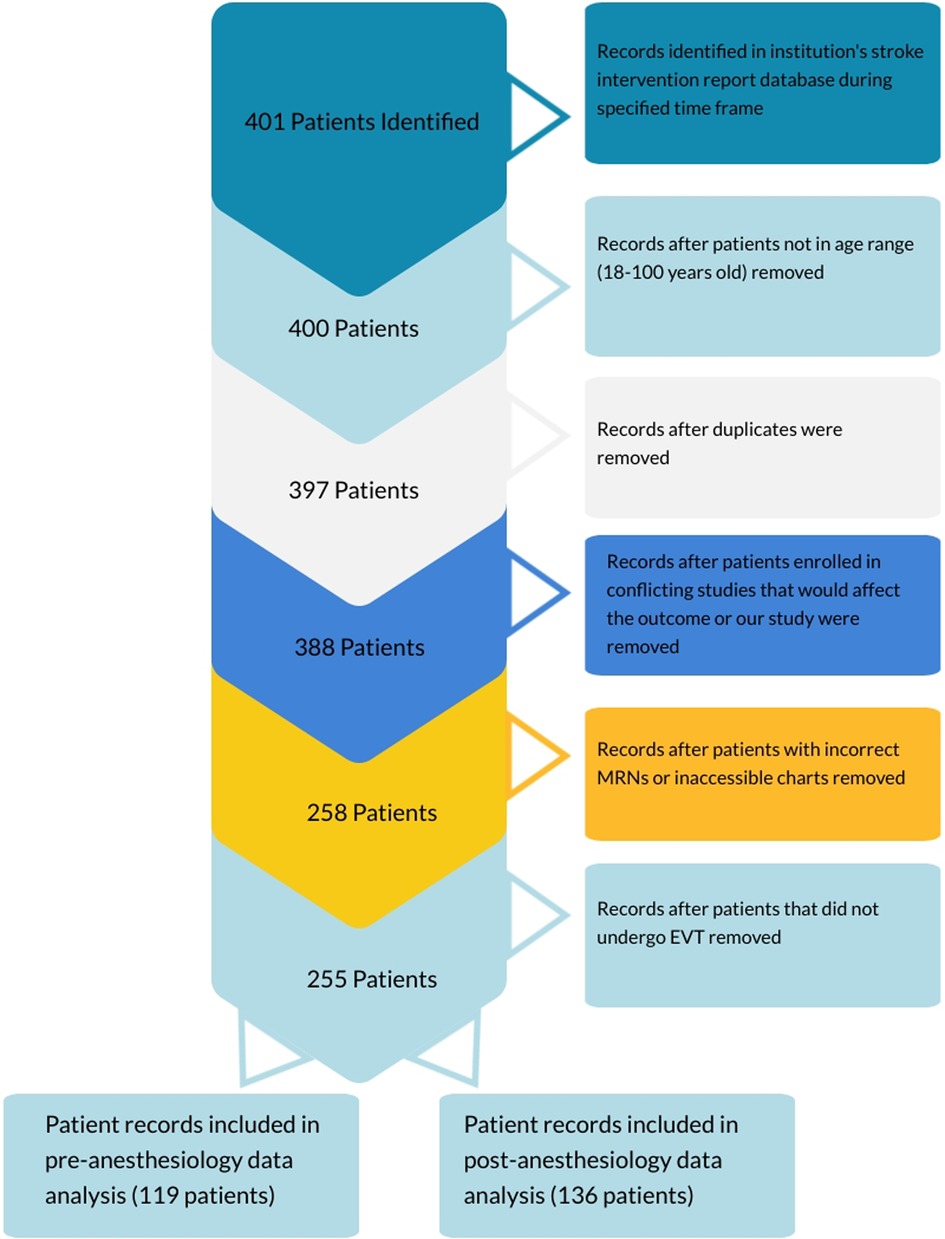
Figure 1 Study flowchart.
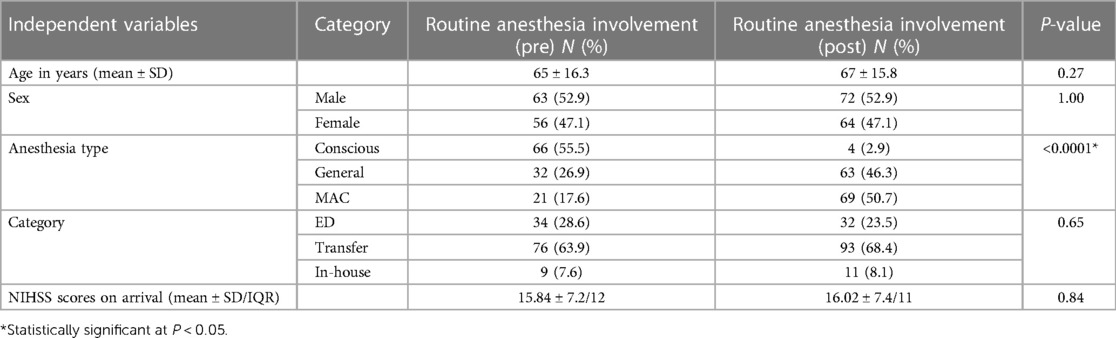
Table 1 Characteristics of patients undergoing EVT.
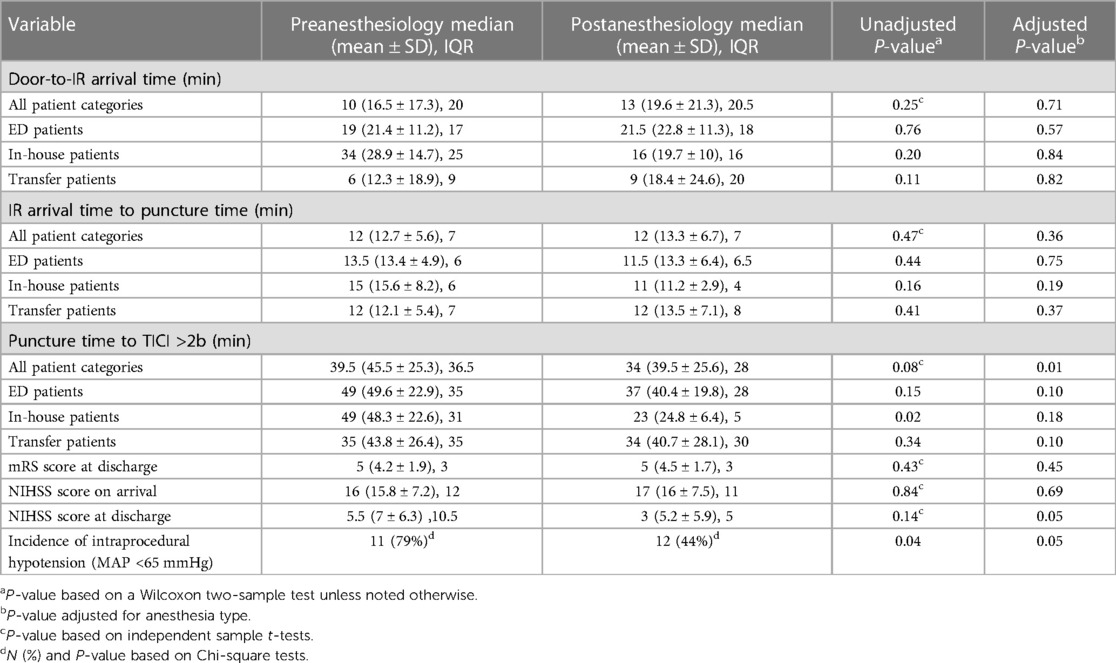
Table 2 Comparison of primary and secondary objectives.
Preroutine anesthesia team involvement, 66 patients (53%) received CS, 32 (29%) received GA, and 21 (18%) received MAC. Postinvolvement, 4 patients (3%) received CS, 63 (46%) received GA, and 69 (51%) received MAC. Differences in the type of anesthetic or sedation received were statistically significant in all groups (Table 1).
The median time from puncture to TICI score >2b significantly decreased in the in-house group from 49.00 min preinvolvement to 23.00 min postinvolvement (P = 0.02). These times also decreased for both categories of patients, those presenting to the ED and transfer patients, but the differences were not statistically significant. When controlling for anesthesia type, only puncture to TICI >2b (39.5 vs. 34 min, P = 0.01) for all patient categories showed statistical significance (Table 2). Other differences in metrics related to EVT were statistically insignificant, but these are given in Table 2. The rate of incidence of intraprocedural hypotension in the preinvolvement group was significantly higher (79%) than that in the postinvolvement group (44%) (P = 0.04), although statistical significance was lost when controlling for anesthesia type (P = 0.05).
Time to intervention for AIS patients is an important factor in achieving improved patient outcomes (1, 2). An anesthesia team that frequently cares for AIS patients receiving EVT is familiar with the location of the neurointerventional radiology suite and their staff and workflow, and theoretically, should decrease time to intervention once the patient reaches the IR suite. Moreover, they have the advantage of being present from the time the patient enters the neurointerventional radiology suite until they arrive in the intensive care unit and can continually assess the patient. This is supported by a single-center retrospective study that showed improved efficiency and increased adherence to physiological parameters supported by guidelines with the routine involvement of anesthesiologists (13).
Prepping patients for groin puncture and placing them on monitors are time-consuming, regardless of the type of sedation or anesthetic delivered. There was no difference in IR-to puncture times preroutine anesthesia team involvement vs. postroutine anesthesia team involvement for ED, in-house and transfer patient categories. Also, in our study, general anesthesia was used more frequently after the involvement of an anesthesia team. Interestingly, three randomized controlled trials and a post hoc analysis of SIESTA have shown that general anesthesia delays groin puncture (4, 14–16). While our results do not support this conclusion, our sample size is much smaller. In contrast, a retrospective, single-center study showed a statistically significant decrease in door-to-arterial puncture time, room-to-arterial puncture time, and procedure time but no differences in functional outcomes at 90 days with routine anesthesiologist involvement in EVTs (13). Our specialized anesthesia team's familiarity with the IR suite and workflow may have contributed to our findings, although it is unknown whether this practice model is preferable.
Differences in puncture time to TICI >2b for all categories postroutine anesthesia team involvement showed a trend toward a decrease in time and became statistically significant when adjusted for anesthesia type. However, puncture time to TICI >2b differed significantly by anesthesia type only in the preinvolvement group, which may be the reason for our obtaining a significant p-value after controlling for anesthesia type. Puncture time to TICI >2b times was statistically significant for in-house patients, but none of the individual categories were significant when adjusted for anesthetic type. The reasons for decreased times were probably multifactorial and potentially related to changes in physiology when anesthetics are used, such as vasodilation and the ability to consistently maintain physiologic parameters. Another advantage of having an anesthesia team is the ability to rapidly diagnose and treat hypotension. A national survey of 109 interventional radiology and neurointerventional radiology sedation nurses who work with patients with AIS found that only 8.4% of sedation team nurses were comfortable administering vasoactive infusions (17). In our study, the incidence of intraprocedural hypotension was significantly reduced in the postroutine anesthesia team involvement group, although this did not reach statistical significance when adjusted for anesthetic type.
Standardizing the type of anesthetic and following society guidelines, such as those put forth by the SNACC, may mitigate issues related to time delay, thereby decreasing time to TICI >2b and improving functional patient outcomes (10). It has been shown that a decrease in stroke onset time to reperfusion time is a better indicator of reperfusion quality as indicated by a TICI 2c/3 score, and better reperfusion quality is associated with better outcomes (18–20). Therefore, one might conclude that a decrease in time to reperfusion from stroke onset would increase the chances of better outcomes. The lack of an NIHSS score at discharge and mRS at discharge for a large proportion of these patients gives us fewer data points. However, our study lays the groundwork for a future prospective study, following up the patients for a longer time to determine functional outcomes.
There have been multiple studies examining whether the use of GA or CS in EVT cases is more advantageous for patient outcomes (4–9, 14, 21). The AnStroke trial demonstrated no difference between the use of GA or CS if hypotension was avoided (4). The SIESTA trial concluded that CS had no particular advantage and, furthermore, more patients were functionally independent in the GA vs. CS group (37.0% vs. 18.2%, respectively) (15). Finally, GOLIATH found that GA was associated with a lower mRS score at 90 days with an odds ratio (OR) of 1.91 when compared with CS (95% confidence interval (CI), 1.03–3.56) (15, 22). Our study did not demonstrate a statistically significant improvement in NIHSS and mRS between the groups, even after adjusting for anesthesia type; however, this may be attributed to factors such as interobserver differences in scoring as well as incomplete data.
The limitations of this study include using data from a single center; thus, the results may not translate to other institutions. The analysis of our dataset did not show a difference in patient outcomes. In addition, the 8-month data related to the postinvolvement group were part of the COVID-19 pandemic period, with a trend toward MAC and maintaining a spontaneously ventilating patient to avoid an aerosol-generating procedure, possibly interfering with internal and external validity. There was incomplete data for many patients due to a lack of standardized patient charting for neurological outcomes at discharge. Also, no data were available after discharge, such as mRS at 30 days poststroke. It should be noted that both the mRS and the NIHSS scales had issues pertaining to interobserver reliability as well as determination of disability, which was subjective in nature (23). Efforts made to minimize these limitations included thorough chart searches using uniform search terms for each variable. To improve data collection for future studies, we suggest documenting all data in the electronic medical record (EMR) or another searchable database. The strengths of this study include few missing data in the time metric categories, thorough anesthesia documentation, particularly after routine EVT care was initiated, and quick adoption of the new policy as evidenced by changes in the medical record. That said, we also recognize that the routine involvement of a dedicated anesthesia team for EVT may not be feasible in all practice settings. Future studies may be able to further investigate stroke metrics and patient outcomes by collecting data from multiple institutions and ensuring complete datasets during hospital stay and at specified intervals postintervention.
In conclusion, our results indicate that routine involvement of a dedicated anesthesia team for EVT in patients with AIS could potentially improve stroke metrics and patient outcomes, although more studies are necessary to validate this model of care.
The original contributions presented in the study are included in the article/Supplementary Material, and further inquiries can be directed to the corresponding author.
The studies involving humans were approved by the University of Kansas Medical Center Institutional Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
NR: Writing – review & editing, Writing – original draft. WO: Writing – review & editing, Writing – original draft. NN: Writing – review & editing, Writing – original draft. GG: Writing – review & editing. EP: Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
We would like to acknowledge the Neuroanesthesia Team, Stroke Team, and neurointerventional radiologists at the University of Kansas Health System for their assistance with data collection and study implementation.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Khatri P, Abruzzo T, Yeatts SD, Nichols C, Broderick JP, Tomsick TA. Good clinical outcome after ischemic stroke with successful revascularization is time-dependent. Neurology. (2009) 73(13):1066–72. doi: 10.1212/WNL.0b013e3181b9c847
2. Khatri P, Yeatts SD, Mazighi M, Broderick JP, Liebeskind DS, Demchuk AM, et al. Time to angiographic reperfusion and clinical outcome after acute ischaemic stroke: an analysis of data from the interventional management of stroke (IMS III) phase 3 trial. Lancet Neurol. (2014) 13(6):567–74. doi: 10.1016/S1474-4422(14)70066-3
3. Mulder M, Jansen IGH, Goldhoorn RB, Venema E, Chalos V, Compagne KCJ, et al. Time to endovascular treatment and outcome in acute ischemic stroke: MR CLEAN registry results. Circulation. (2018) 138(3):232–40. doi: 10.1161/CIRCULATIONAHA.117.032600
4. Löwhagen Hendén P, Rentzos A, Karlsson JE, Rosengren L, Leiram B, Sundeman H, et al. General anesthesia versus conscious sedation for endovascular treatment of acute ischemic stroke: the AnStroke trial (anesthesia during stroke). Stroke. (2017) 48(6):1601–7. doi: 10.1161/STROKEAHA.117.016554
5. Brinjikji W, Murad MH, Rabinstein AA, Cloft HJ, Lanzino G, Kallmes DF. Conscious sedation versus general anesthesia during endovascular acute ischemic stroke treatment: a systematic review and meta-analysis. Am J Neuroradiol. (2015) 36(3):525–9. doi: 10.3174/ajnr.A4159
6. Dhakal LP, Diaz-Gomez JL, Freeman WD. Role of anesthesia for endovascular treatment of ischemic stroke: do we need neurophysiological monitoring? Stroke. (2015) 46(6):1748–54. doi: 10.1161/STROKEAHA.115.008223
7. Lee CZ, Gelb AW. Anesthesia management for endovascular treatment. Curr Opin Anesthesiol. (2014) 27(5):484–8. doi: 10.1097/ACO.0000000000000103
8. Athiraman U, Sultan-Qurraie A, Nair B, Tirschwell DL, Ghodke B, Havenon AD, et al. Endovascular treatment of acute ischemic stroke under general anesthesia: predictors of good outcome. J Neurosurg Anesthesiol. (2018) 30(3):223–30. doi: 10.1097/ANA.0000000000000449
9. Brinjikji W, Pasternak J, Murad MH, Cloft HJ, Welch TL, Kallmes DF, et al. Anesthesia-related outcomes for endovascular stroke revascularization: a systematic review and meta-analysis. Stroke. (2017) 48(10):2784–91. doi: 10.1161/STROKEAHA.117.017786
10. Talke PO, Sharma D, Heyer EJ, Bergese SD, Blackham KA, Stevens RD. Republished: society for neuroscience in anesthesiology and critical care expert consensus statement: anesthetic management of endovascular treatment for acute ischemic stroke. Stroke. (2014) 45(8):e138–50. doi: 10.1161/STROKEAHA.113.003412
11. Banks JL, Marotta CA. Outcomes validity and reliability of the modified Rankin scale: implications for stroke clinical trials: a literature review and synthesis. Stroke. (2007) 38(3):1091–6. doi: 10.1161/01.STR.0000258355.23810.c6
12. Lyden P, Raman R, Liu L, Emr M, Warren M, Marler J. National institutes of health stroke scale certification is reliable across multiple venues. Stroke. (2009) 40(7):2507–11. doi: 10.1161/STROKEAHA.108.532069
13. McCusker RJ, Chinchilli VM, Fritch CD, Kochar PS, Sharma S. Demonstrating the value of routine anesthesiologist involvement in acute stroke care: a retrospective chart review. J Neurosurg Anesthesiol. (2023) 35(4):406–11. doi: 10.1097/ANA.0000000000000927
14. Schönenberger S, Uhlmann L, Hacke W, Schieber S, Mundiyanapurath S, Purrucker JC, et al. Effect of conscious sedation vs general anesthesia on early neurological improvement among patients with ischemic stroke undergoing endovascular thrombectomy: a randomized clinical trial. JAMA. (2016) 316(19):1986–96. doi: 10.1001/jama.2016.16623
15. Simonsen CZ, Yoo AJ, Sørensen LH, Juul N, Johnsen SP, Andersen G, et al. Effect of general anesthesia and conscious sedation during endovascular therapy on infarct growth and clinical outcomes in acute ischemic stroke: a randomized clinical trial. JAMA Neurol. (2018) 75(4):470–7. doi: 10.1001/jamaneurol.2017.4474
16. Pfaff JAR, Schonenberger S, Nagel S, Ringleb PA, Hacke W, Bendszus M, et al. Effect of general anesthesia versus conscious sedation for stroke thrombectomy on angiographic workflow in a randomized trial: a post hoc analysis of the SIESTA trial. Radiology. (2018) 286(3):1016–21. doi: 10.1148/radiol.2017171002
17. Korzewski M, Raingruber B, Van Leuven K. Procedural sedation/anesthesia protocol among acute ischemic stroke patients undergoing endovascular revascularization procedures: the nursing perspective on what is being practiced nationwide. J Radiol Nurs. (2016) 35(1):12–8. doi: 10.1016/j.jradnu.2016.01.002
18. Bourcier R, Goyal M, Liebeskind DS, Muir KW, Desal H, Siddiqui AH, et al. Association of time from stroke onset to groin puncture with quality of reperfusion after mechanical thrombectomy: a meta-analysis of individual patient data from 7 randomized clinical trials. JAMA Neurol. (2019) 76(4):405–11. doi: 10.1001/jamaneurol.2018.4510
19. Kaesmacher J, Dobrocky T, Heldner MR, Bellwald S, Mosimann PJ, Mordasini P, et al. Systematic review and meta-analysis on outcome differences among patients with TICI2b versus TICI3 reperfusions: success revisited. J Neurol Neurosurg Psychiatry. (2018) 89(9):910–7. doi: 10.1136/jnnp-2017-317602
20. Wang R, Aslan A, Khalili N, Garg T, Kotha A, Hamam O, et al. Groin puncture to recanalization time may be a strong predictor of mTICI 2c/3 over mTICI 2b in patients with large vessel occlusions successfully recanalized with mechanical thrombectomy. Diagnostics (Basel). (2022) 12(10):2557. doi: 10.3390/diagnostics12102557
21. Li X, Hu Z, Li Q, Guo Y, Xu S, Wang W, et al. Anesthesia for endovascular treatment in anterior circulation stroke: a systematic review and meta-analysis. Brain Behav. (2019) 9(1):e01178. doi: 10.1002/brb3.1178
22. Probst S, Corrado T, Bergese SD, Fiorella D. A dedicated cerebrovascular anesthesia team is a critical component of a comprehensive stroke center. J Neurointerv Surg. (2020) 12(3):227–8. doi: 10.1136/neurintsurg-2020-015860
Keywords: stroke, ischemic stroke, time to treatment, endovascular procedures, anesthesia
Citation: Rall N, Orr WN, Nazir N, Giron G and Plaza E (2024) Stroke metric changes pre- vs. postroutine anesthesiologist involvement for endovascular treatment of acute ischemic stroke. Front. Anesthesiol. 3: 1388407. doi: 10.3389/fanes.2024.1388407
Received: 19 February 2024; Accepted: 26 June 2024;
Published: 19 July 2024.
Edited by:
Gerhard Schneider, Technical University of Munich, GermanyReviewed by:
Dana Baron Shahaf, Rambam Health Care Campus, Israel© 2024 Rall, Orr, Nazir, Giron and Plaza. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Erin Plaza, ZXBsYXphQGt1bWMuZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.