
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Aging, 07 April 2025
Sec. Healthy Longevity
Volume 6 - 2025 | https://doi.org/10.3389/fragi.2025.1510257
 María-Itatí Palacio
María-Itatí Palacio Rosa-María BermejoAna-María Lucas-OchoaAna-María González-CuelloEmiliano Fernández-Villalba
Rosa-María BermejoAna-María Lucas-OchoaAna-María González-CuelloEmiliano Fernández-Villalba María-Trinidad Herrero*
María-Trinidad Herrero*Swallowing disorders, which are generally underdiagnosed, affect the elderly, leading to a decreased quality of life and complications, including aspiration pneumonia and death. Understanding the neurophysiology of swallowing and the causes of its dysfunction is a fundamental tool for the prevention, early diagnosis, and treatment of dysphagia. New technologies open a wide range of possibilities for the implementation of new care protocols for this disorder.
All around the world religious, cultural and familial traditions play a significant role in eating, drinking and swallowing (Jardine et al., 2020). The ease with which we and swallow is surprising given the complex neurological control system involved. The development of feeding and swallowing involves a set of interactions that begin in the embryonic and fetal periods and continue throughout childhood until mature swallowing is achieved (Reid et al., 2016).
Oropharyngeal dysphagia is a swallowing disorder defined by the difficulty in safely and efficiently forming and/or moving the food bolus from the oral cavity to the esophagus. Presbyphagia, on the other hand, is the swallowing disorder caused by normal ageing. In patients with dysphagia or presbyphagia, quality of life, eating habits and diet are altered. The health of these patients deteriorates and, in many cases, these disorders lead to aspiration pneumonia and death (Clavé et al., 2015).
The economic consequences of dysphagia in hospitalized patients are significant, as patients with dysphagia generate costs up to 48% higher than those without dysphagia and are 33.2% more likely to be transferred to a post-acute care facility. Dysphagia increases the likelihood of a longer hospital stay and even death in patients who suffer from it (Patel et al., 2018). In their daily lives, people affected by undiagnosed dysphagia or presbyphagia may make intuitive adjustments to their diet, use strategies to control food intake and be able to eat small amounts of food and liquids (Ballesteros-Pomar et al., 2020). However, in the context of additional deterioration, particularly an acute health change or surgery, swallowing problems can destabilize and have a negative impact on overall diagnosis, prolong hospital days, increase hospital readmissions, increase the need for prolonged treatments and require long-term rehabilitation care (Allen et al., 2020).
Therefore, understanding the anatomical and physiological processes of swallowing and its alterations is essential, especially in older adults (Matsuo and Palmer, 2008).
Swallowing is the safe transport of food and liquids from the oral cavity to the esophagus (Ambrocio et al., 2023). It is not only essential for nutritional intake but also plays a role in managing internal secretions of the upper (saliva, bile, and nasal secretions) and lower (tracheal or bronchial) aerodigestive tracts. The physiological mechanism of swallowing is divided into four well-defined phases: the oral preparatory phase, the oral transport phase, the pharyngeal phase, and the esophageal phase; the first two are voluntary, and the last two are reflexive (Costa, 2018). For the motor program of swallowing to be adequate and aligned with the needs of each moment, the coupled participation of various cortical and cranial areas, five cranial nerves (V, VII, IX, X, and XII), the first three cervical segments, and the muscles of the mouth, pharynx, and esophagus is necessary, coordinated among themselves from the nuclei of the brainstem (Tables 1, 2) (Krishnamurthy et al., 2021).
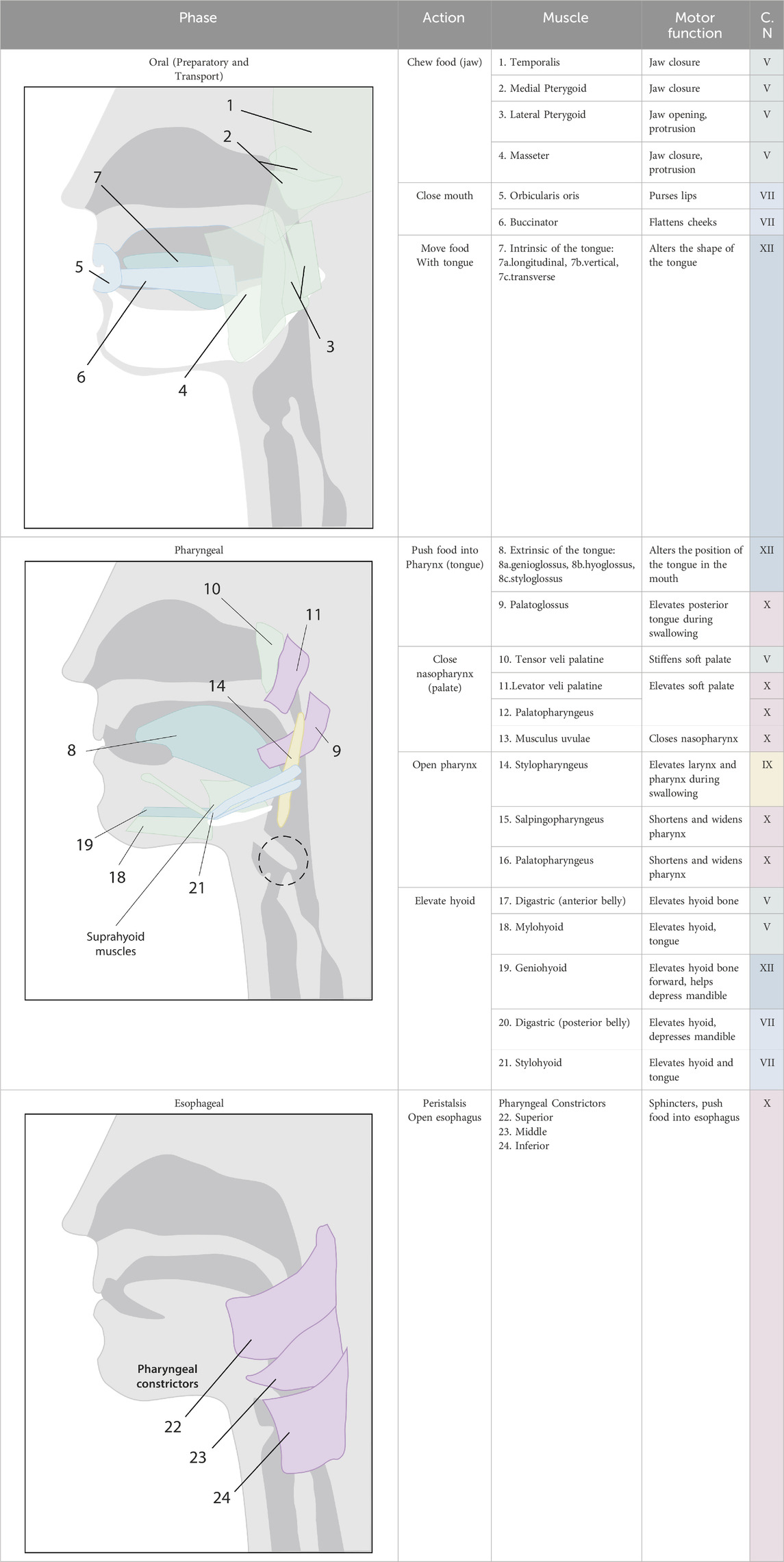
Table 1. Schematic representation of the muscles involved in each phase of swallowing and their motor innervation. Muscles 7 (a, b and c), 8 (a, b and c), 13, 15–17, and 20 are not depicted in the diagrams. Colors correspond to the innervation of each cranial nerve.
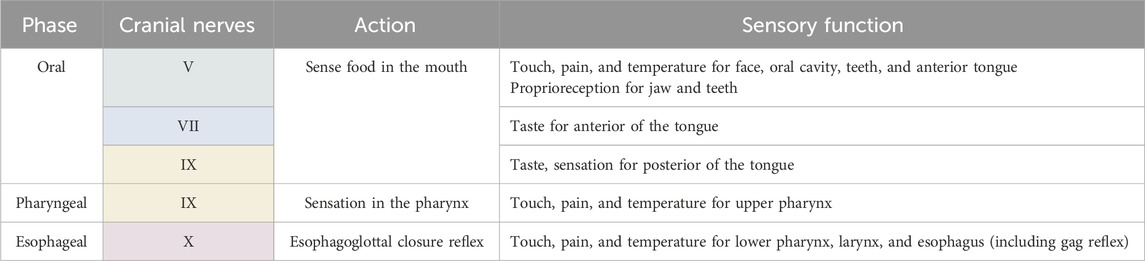
Table 2. Schematic representation of sensory afferents and their actions in each phase of swallowing. Colors correspond to each cranial nerve and are similar to those in Table 1.
The development of the foundations of swallowing begins in the womb and progresses during infancy and the early years of childhood (Kalhoff et al., 2024). Starting from the 10th week of gestation, pharyngeal swallowing movements begin, and between the 18th and 24th weeks, fetal sucking movements develop (Figure 1). Consistent swallowing appears in the 22nd week, and active sucking emerges around the 34th to 37th weeks of gestation.

Figure 1. Relevant processes in the development of swallowing during gestation and the first few months of life. The swallowing reflex is preserved throughout life.
Both of these primitive motor reflexes (sucking and swallowing) are indispensable for he newborn´s survival (López Ortega et al., 2024; Rogers and Arvedson, 2005). They are involuntary reflexes which originate in the brainstem and disappear during early childhood development (although they may persist or reappear in neurological conditions as pathological signs of frontal release).
After 36 weeks of gestation, the maturation of the sucking-swallowing-breathing triad is complete, allowing healthy newborns to ingest liquid orally and swallow it (Kalhoff et al., 2024). The coordination of sucking, swallowing, and breathing is one of the most complex neuromotor programs in newborns, although the maturation of the stomatognathic system is not yet complete at birth (Palacio Ortega et al., 2024). Gradually, through sensorimotor learning, experience, neurological maturation, sensory integration, and desensitization of the gag reflex, the motor function of swallowing develops and is perfected, allowing for conscious and correct feeding (Kiyohara et al., 2012).
There are two types of swallowing: reflexive swallowing and voluntary swallowing. Reflexive or automatic swallowing refers to the swallowing of oropharyngeal secretions without the occurrence of the oral preparatory phase. It is unintentional and triggered by laryngopharyngeal sensory stimuli. It occurs unconsciously both when we are awake and during sleep. It has a weaker association with the corticobulbar tract and shows activation in the sensorimotor cortex, the lateral postcentral gyrus, and the right insula, although it generates greater activation in the left hemisphere (Kiyohara et al., 2012). It is a protective reflex action (to ensure the safety of the upper respiratory tract against any escape of food particles or saliva) and may also be related to emotions.
Voluntary swallowing occurs when a person has the desire to eat or drink while awake and conscious. It is part of feeding behavior, and there is an orderly activation of the muscles involved in each phase. Voluntary swallowing has a multiregional brain representation, stronger in the lateral sensorimotor and premotor cortex, the insula, the temporal cortex, the amygdala, the cerebellum, and the dorsal brainstem. It has a bilateral non-asymmetrical activation in both hemispheres, regardless of the subject’s lateralization (Kern et al., 2001).
Automatic and voluntary swallowing has been shown to be processed in areas of the cerebral cortex. Both types of swallowing are associated with the activation of several functionally distinct cortical areas in the prefrontal, temporal, and parietal lobes (Martin et al., 2001). The motor areas of the cerebral cortex that initiate spontaneous or voluntary swallowing have been recently identified. For many years, medical literature has stated that swallowing was primarily controlled by the brainstem (Penfield and Boldrey, 1937). However, more recent research has provided evidence that cortical and subcortical structures play a fundamental role in the control of swallowing, showing constant activity in multiple cortical areas (Figure 2): 1) The lateroventral precentral gyrus. In the face area (BA4), there is a somatotopic representation of the oral, pharyngeal, and esophageal muscles, with an asymmetric motor representation, independent of laterality (Hamdy et al., 1996). 2) The premotor cortex, with a focus of activation within the lateral premotor area (BA 6) (Wei et al., 2024). 3) The supplementary motor area would play an important role in mediating and preparing complex sequences of movements (Vasant and Hamdy, 2013). 4) The anterior cingulate cortex (BA24) is part of the limbic system and is important for processing motivation and attention towards voluntary actions and sensory stimuli (Vogt, 2005; Humbert and Robbins, 2007). 5) The lateral postcentral gyrus is where the primary somatosensory cortex of the face is located (Toogood et al., 2017). 6) The insula plays a role in mediating both sensory and motor aspects of the function of the alimentary tract involving the oropharynx, esophagus, and possibly other areas of the gastrointestinal tract (Binkofski et al., 1998; Deng et al., 2021).
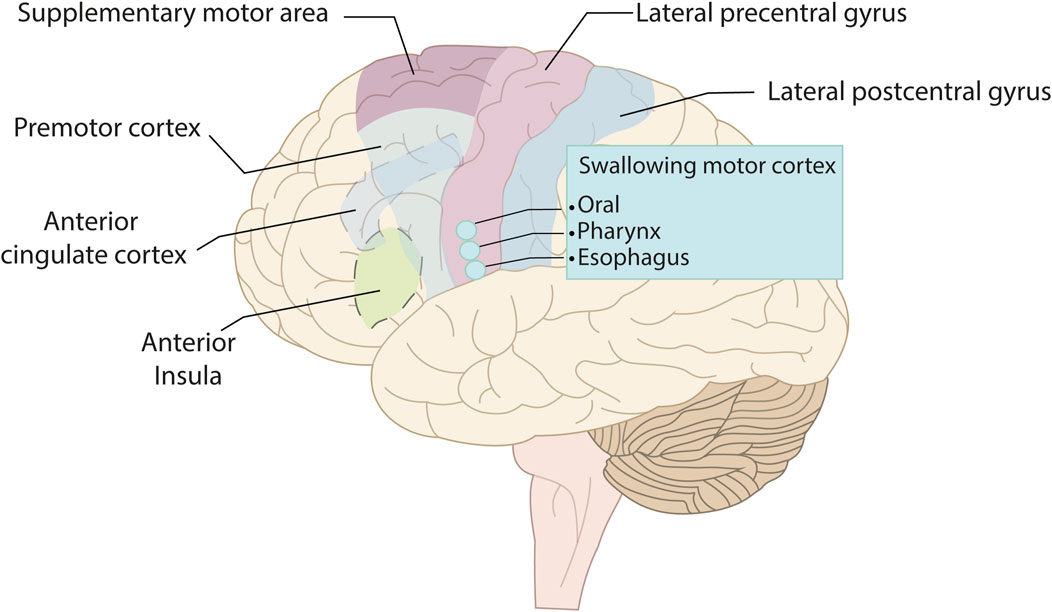
Figure 2. Lateral view of the left hemisphere showing the cortical areas involved in swallowing: The precentral gyrus, the swallowing motor cortex (located within the primary motor cortex), the premotor cortex, the supplementary motor area, the anterior cingulate cortex, the anterior insula, and the lateral postcentral gyrus.
The initiation of the reflexive or automatic swallowing mechanism is triggered by the stimulation of sensory receptors located in the tongue, soft palate, uvula, posterior pharyngeal wall, and larynx. Voluntary swallowing is initiated by a direct action controlled by the cerebral cortex (Prosiegel and Ekberg, 2019).
The motor program of swallowing is divided into four stages (ideation and planning, programming, execution, and movement generation) and is a succession of excitatory and inhibitory mechanisms of motor nerve signals that are fed back by afferent sensory stimuli (Figure 3).
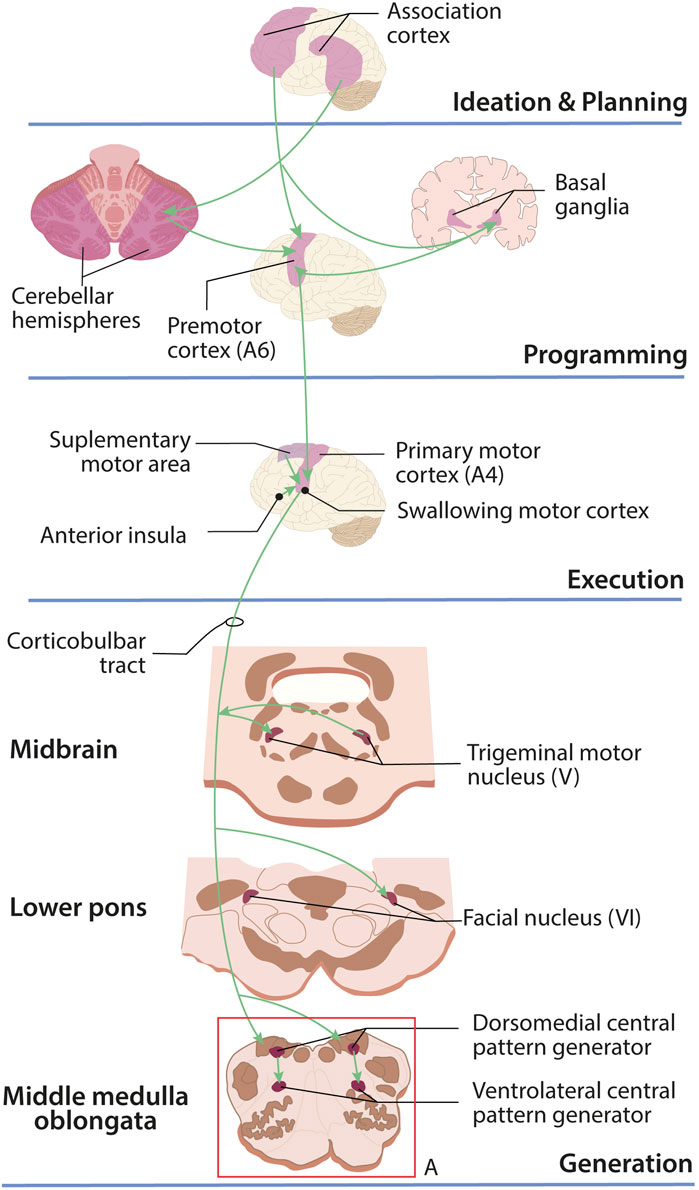
Figure 3. Motor control of swallowing in the central nervous system. The ideation of voluntary swallowing begins in the frontal cortex. Planning takes place in the prefrontal and somatosensory association cortices; planning is a joint effort between the cerebellum, motor cortex, and basal ganglia; for execution, the supplementary motor area, swallowing cortex, and insula send signals through the corticobulbar tract that will be received by the pattern generators (A) located in the medulla oblongata whose motor and sensory neurons will initiate and moderate swallowing.
The ideation of voluntary swallowing originates in the frontal cortex. Movement planning occurs (following ideation in voluntary swallowing and in response to sensory stimuli in reflexive swallowing) in the prefrontal association cortex together with the somatosensory association cortex (Knollhoff et al., 2022). Upon receiving the signal, movement programming of the swallowing musculature is jointly performed by both cerebellar hemispheres and the basal ganglia, which work in parallel to program the movement of the swallowing musculature and then transmit this information to the premotor cortex, inhibiting the muscles that must remain relaxed.
For movement execution, the swallowing cortex (located in the anterolateral motor cortex) receives information from the premotor cortex and simultaneously receives impulses from the supplementary motor area and the anterior insula, which are sent via the corticobulbar tract (Li-Jessen et al., 2020). Swallowing movements are produced by central pattern generators (CPGs) located in the medulla oblongata, which receive signals via the corticobulbar tract.
The swallowing network includes two main CPGs (Figure 3A). A dorsal CPG containing the generator neurons involved in triggering, shaping, and synchronizing the sequential or rhythmic swallowing pattern. It is located in the dorsal medulla oblongata, within the nucleus of the solitary tract and the adjacent reticular formation. The second CPG is ventrolateral and distributes motor outputs to cranial nerves V and VII located in the pons and to cranial nerves IX, X, XI, and XII in the medulla oblongata. This latter CPG is located in the ventrolateral medulla oblongata, in the reticular formation surrounding the nucleus ambiguous (Pitts and Iceman, 2023).
The corticobulbar tract also sends information directly to the four nuclei of the cranial nerves involved in swallowing (Figure 4): a) The motor nucleus of the trigeminal nerve (V) b) The facial motor nucleus (VII). c) The hypoglossal nucleus (XII) and d) The nucleus ambigus, with cranial nerves IX, X, and XI (the latter is not involved in swallowing). Two sensory nuclei are also involved, which receive information from peripheral structures: a) the nucleus of the solitary tract (with cranial nerves VII, IX, and X) and b) specific regions of the trigeminal sensory nuclei (V). Sensory information has three functions: helping to initiate swallowing, modifying the threshold for pharyngeal swallowing, altering the level of muscle recruitment during swallowing, recognizing the characteristics of the stimulus (Wei et al., 2024).
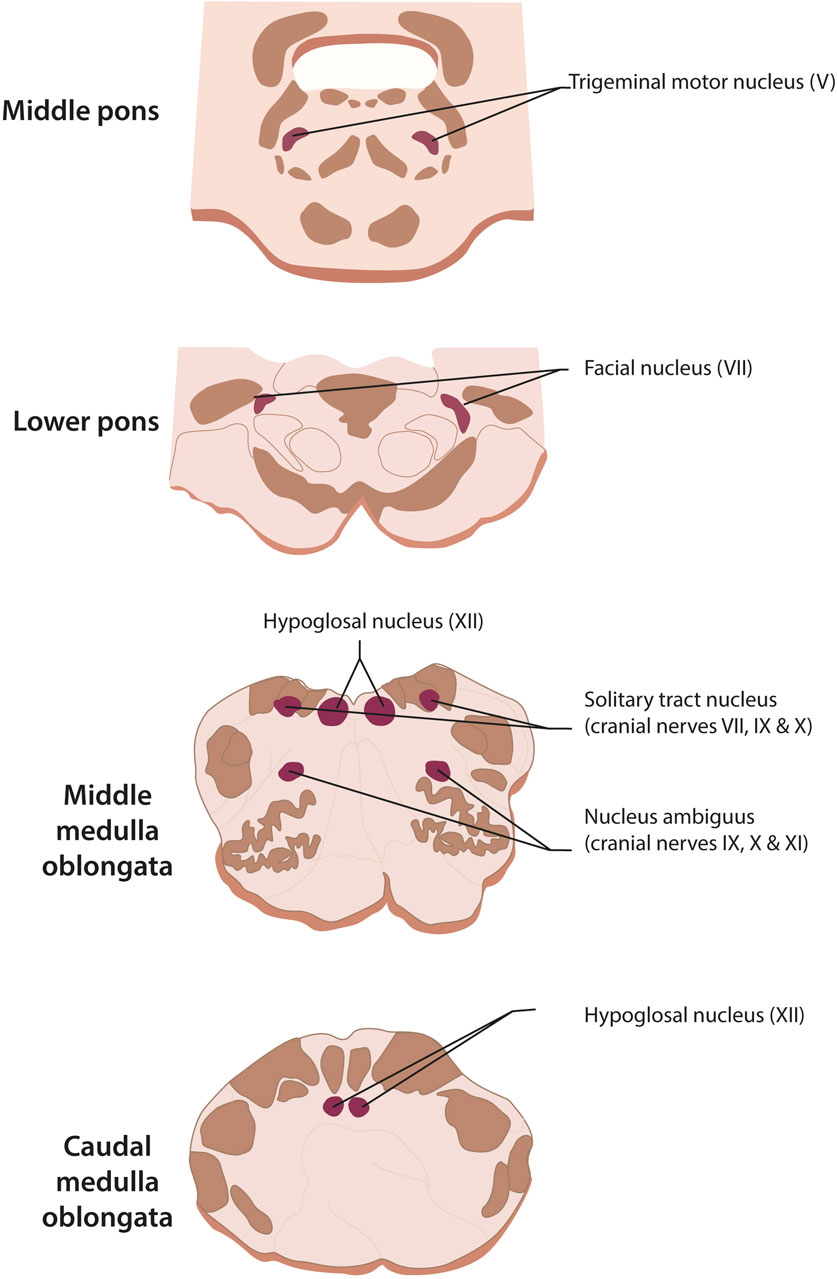
Figure 4. Cranial nerve nuclei which are involved in swallowing. Motor nuclei: nucleus ambiguus (cranial nerves IX, X, and XI, the latter not involved in swallowing), trigeminal motor nucleus (for V), facial motor nucleus (cranial nerve VII), and hypoglossal nucleus. Sensory nuclei: nucleus of the solitary tract (cranial nerves VII, IX, and X) and specific regions of the trigeminal nucleus (cranial nerve V).
The four phases of swallowing are coordinated with each other through central pattern generators (CPGs) and peripheral reflexes. Signals generated by CPGs must be amplified by peripheral sensory afferents that feed back onto the CPGs, producing each specific phase of swallowing (Lang, 2009). The first phase of swallowing is the oral phase. Within this phase, two phases can be identified: the preparatory and the transport phase. The oral preparatory phase is voluntary, and it is where mastication and bolus formation take place. The airway is normally open, and the duration of this phase depends on factors such as motor efficiency and the subject’s desire to savor the food (Ertekin and Aydogdu, 2003). The oral transport phase begins with the transport of the bolus towards the pharynx. The tongue movement presses the bolus against the hard palate and directs it backwards. By the contraction of the hyoglossus muscle, the tongue adopts a channel shape, the palatoglossal seal opens and allows the food to advance. This phase is voluntary, and its duration depends on the viscosity and size of the bolus and the state of the higher brain functions. The oral phase ends when the food bolus exerts pressure on the anterior palatal arches, the back of the tongue, and the palate (Costa, 2018).
The pharyngeal phase is the set of processes that occur between the passage through the isthmus of the maw until the bolus passes through the upper esophageal sphincter. This phase is reflexive, lasts approximately 1 s and is initiated by the stimulation of pharyngeal mechanoreceptors and tongue proprioceptors that send information to the CNS. In this phase, four events occur: a) closure of the velopharyngeal sphincter, b) closure of the laryngeal sphincter, c) propulsion of the bolus through the pharynx and d) opening of the UES, transforming the oropharynx into a swallowing pathway (Rodríguez and Belinchón, 2020).
From the moment the bolus passes through the upper esophageal sphincter (UES), the esophageal phase begins and ends when the bolus reaches the stomach, thanks to the peristaltic wave produced by the esophageal muscle layers. The lower esophageal sphincter (LES), which is physiological and not anatomical, opens due to the presence of the bolus and the esophageal peristalsis itself, allowing entry into the stomach after which it recovers its tone, preventing gastroesophageal reflux. It has a duration of between 8 and 20 s and is also involuntary (Costa, 2018). The interruption or deterioration of any phase of the swallowing mechanism can compromise the safety and effectiveness of it. Each of the processes must be functionally evaluated to identify the physiological or structural cause that produces swallowing dysfunction.
Dysphagia is the difficulty in moving food or liquids from the mouth to the stomach, due to the impairment of one or more phases of swallowing, which alters its efficiency and safety (McCarty et al., 2021). Moreover, its efficiency is compromised when the individual is unable to carry out the processes of eating correctly, which may result in malnutrition and/or dehydration. The alteration of safety (aspiration or penetration into the airway) results in respiratory infections, with aspiration pneumonia being the cause of death in 50% of cases (Hurtte et al., 2023). It is estimated that dysphagia affects 8% of the world’s population, and its incidence increases in the elderly population (Nagano et al., 2023). In older adults living independently, the prevalence of dysphagia is between 30% and 40% and increases to 60% in institutionalized elderly patients. In elderly patients with neurological disorders and/or dementia, the prevalence increases to 64% and 80%, respectively (Baijens et al., 2016). Additionally, swallowing disorders produce a series of medical, social and psychological sequelae that can lead to malnutrition, dehydration, pneumonia, chronic lung disease and decreased quality of life (Milewska et al., 2020). Fear of choking, changes in food, eating and drinking slowly, fatigue and embarrassment about eating in public affect participation in social events. The preparation of special diets can also increase the financial burden and stress of caregivers and families (Smith et al., 2023).
Based on the affected swallowing phase, dysphagia can be classified into oropharyngeal dysphagia (oral and pharyngeal phases) and esophageal dysphagia (esophageal phase). Oropharyngeal dysphagia is the most prevalent one and is further divided into two disorders of two of the phases, the oral and pharyngeal (Malhi, 2016). Oral dysphagia presents signs such as difficulty initiating swallowing, problems forming the bolus and controlling it within the oral cavity. Prolonged bolus retention is associated with drooling, sialorrhea, and the need for multiple swallowing attempts. Oral dysphagia can be caused by incomplete lip closure, reduced strength or incompetence of the mastication muscles, and/or a limitation or incoordination of tongue movement (Rech et al., 2018). Pharyngeal phase dysphagia is usually due to problems with lingual, pharyngeal propulsion, or opening of the upper esophageal sphincter. This phase is under involuntary control and the alterations that may occur are: delayed swallowing reflex, decreased velopharyngeal closure (with nasal regurgitation), decreased epiglottic movement, poor laryngeal elevation, and disorders or lesions of the upper esophageal sphincter. These alterations cause bolus retention in the pharynx, which can lead to coughing, nasopharyngeal regurgitation, sialorrhea or xerostomia, fragmented swallowing, dysarthria, choking, and even aspiration or penetration into the airway (Roy et al., 2007). Esophageal dysphagia (ED) presents as difficulty continuing to swallow and may be associated with chest pain or pressure, reflux, food regurgitation, repeated swallowing attempts, and symptoms of aspiration, such as coughing and choking. The main cause of ED is inflammation or stenosis of the esophageal wall. Neurological diseases can also cause alteration of the smooth or striated muscle of the esophagus, or of the motor neurons that control esophageal peristalsis and relaxation of the lower esophageal sphincter (Louis and Nakhal, 2022).
Oropharyngeal dysphagia (OD), accounting for 80% of all diagnosed dysphagias, is a symptom rather than a disease itself. Any abnormality of the critical oropharyngeal structures involved in swallowing or of the neural controls can impair swallowing and cause OD. The causes of OD can be grouped into three categories (Figure 5): neurological, structural, and other etiologies (Wilkinson et al., 2021). Ageing itself is not a cause of dysphagia, although there are age-related changes that affect all phases of swallowing (González Cortés et al., 2018). Neurological causes affect the transmission of information to and from the CNS. Consequently, the function of the oropharyngeal neuromuscular system is altered. These causes can be divided into three types: a) Acute onset: such as stroke, traumatic brain injury, and neoplasms. b) Neurodegenerative: Parkinson’s disease, dementia, myopathies, motor neuron disease, multiple sclerosis, and myasthenia gravis. c) Developmental: cerebral palsy, Down syndrome, hydrocephalus, and Chiari malformation (Malandraki and Robbins, 2013).
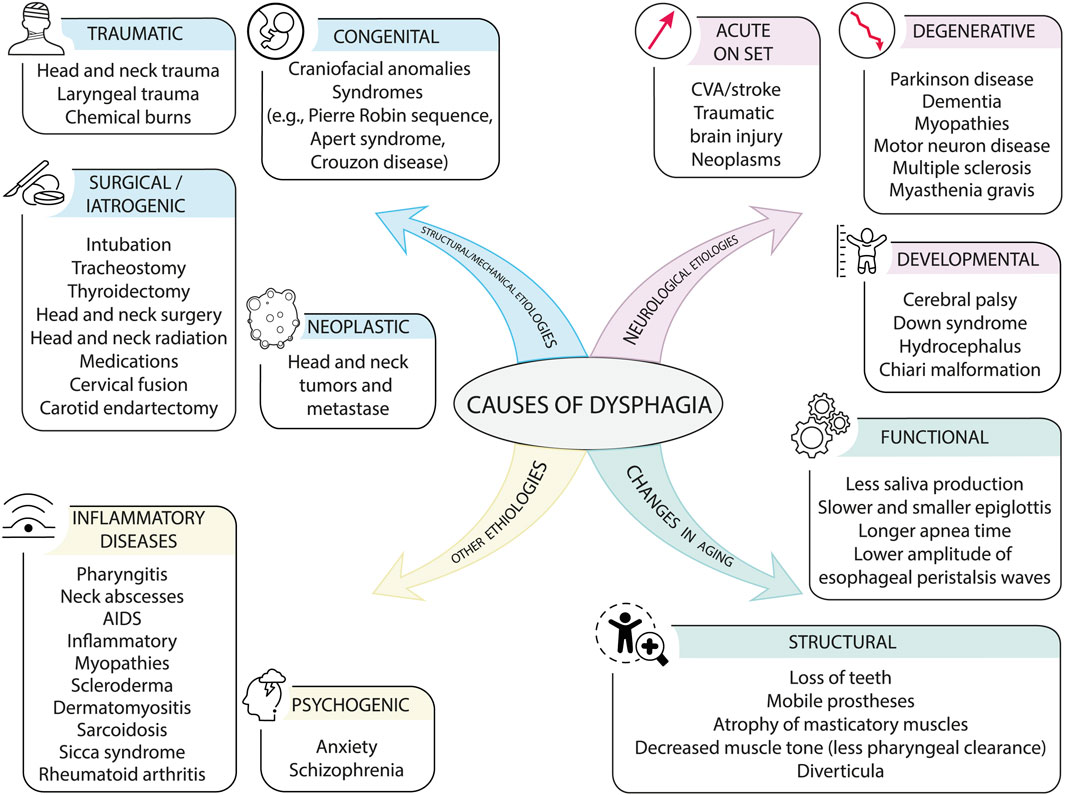
Figure 5. Causes of dysphagia. Causes of dysphagia can be divided into neurological, structural, other etiologies, and age-related changes, although the latter may not be a cause of dysphagia but rather an early symptom.
Mechanical and structural causes are those that alter the anatomical and/or physiological integrity of the oropharyngeal mechanism and cause difficulty in swallowing. They are divided into: a) congenital causes, such as craniofacial anomalies and/or syndromes (e.g., Pierre Robin sequence, Apert syndrome, Crouzon disease). b) traumatic causes, including head and neck trauma, laryngeal trauma, and chemical burns. c) surgical or iatrogenic causes: intubation, tracheotomy, thyroidectomy, head and neck surgery and radiotherapy, medication, cervical fusion, carotid endarterectomy. d) Neoplastic causes such as tumors and head and neck cancer (Rommel and Hamdy, 2016).
Finally, there are other causes of dysphagia, including inflammatory diseases such as pharyngitis, cervical abscesses, AIDS, inflammatory myopathies, scleroderma, dermatomyositis, sarcoidosis, Sjögren’s syndrome, rheumatoid arthritis, and psychogenic disorders such as anxiety and schizophrenia (Massa et al., 2022). In patients under 60 years of age, morphological and structural causes predominate, while in patients over 60 years of age, neurological alterations are the most frequent (Tulunay-Ugur and Eibling, 2018).
Depending on the underlying cause and the affected swallowing phase, dysphagia can manifest in different ways. In the oral phase, problems may be associated with food crushing, abnormal chewing, poor bolus formation and transport, poor tongue mobility, poor or absent lip closure, excessive salivation, numbness of the mouth, and/or dry mouth. As a result, food may accumulate in the vestibule of the mouth and in the cheeks, causing saliva leaks or food leakage from the mouth (Dylczyk-Sommer, 2020).
A consequence of the severity of pharyngeal dysphagia, regardless of its cause, is that the protective function of the larynx is altered: the cough reflex is weakened, triggering the passage of food or secretions into the airway. The consequences of airway invasion can be retention, penetration, and/or aspiration of saliva or food. Retention is defined as the accumulation of saliva or food in the vallecula or pyriform sinuses. Penetration occurs when saliva or food enters the laryngeal vestibule, and aspiration is associated with the presence of saliva or food below the vocal cords, being the most severe of the three (Speyer et al., 2022).
When a patient or their family notices difficulties with swallowing, they inform the doctor, who carries out an assessment of OD. The aim of the assessment is to determine the efficacy and safety of swallowing. Efficacy is demonstrated when the patient is able to ingest all the calories and water, they need to be well-nourished and hydrated. Swallowing is safe when the individual is able to ingest food and drink without respiratory complications arising (Alsaied and Postma, 2019). There are two types of assessments to achieve this goal: non-instrumental or clinical assessment and instrumental assessment, which is carried out using complementary tests with specific tools.
Non-instrumental assessment of dysphagia is effective for: 1) identifying the potential causes of swallowing problems; 2) estimating the safety of swallowing and the risk of aspiration; 3) supporting decisions about oral feeding or alternatives; and 4) deciding on treatment strategies and identifying the need for additional instrumental assessment (Farneti et al., 2018). Clinical assessment encompasses several aspects, and, in the absence of a systematic review, five types of necessary examinations can be established: patient medical history; assessment of cognition and communication; physical examination; administration of a screening test; evaluation of oral intake with different textures; and observation of oral hygiene (Clavé et al., 2008). During medical history, sociodemographic data, health information, and comorbidity and other risk factors for dysphagia should be collected. An initial observation of the level of consciousness and degree of postural control should also be made, as well as whether the patient is able to sit up and remain upright. The physical examination of oral function includes the motor and structural examination of all oral functions, including examination of the cranial nerves and the velopharyngeal, cough, and swallowing reflexes (Clavé et al., 2011).
Once the medical history, physical examination, and assessment of cognitive status have been carried out, it is necessary to know the patient’s perception of their disorder and their quality of life. The most used subjective screening questionnaires for dysphagia are the Swallowing Quality of Life Questionnaire (SWAL-QOL) and the Eating Assessment Tool (EAT-10), both validated and very simple to apply. The SWAL-QOL consists of 44 items and provides information on self-perception of quality of life and the impact of swallowing on the patient (McHorney et al., 2002). The EAT-10 assesses ten items and can be answered by patients or their caregivers. Statements about the experience of swallowing are rated on a scale of 0–4, where 0 indicates no problem and 4 indicates a severe problem. A score greater than 3 indicates that the individual is at high risk of dysphagia (Sánchez-Sánchez et al., 2021; Zhang P. et al., 2023).
To complete the clinical assessment and make it useful for diagnosis, an oral intake assessment must be performed. The most commonly used methods of assessing oral intake are: the water test, the Gugging Swallowing Screen (GUSS), and the Volume-Viscosity Swallow Test (V-VST) (Clavé et al., 2015). The water test is the most widely used in nursing. In the test, 10 mL of water is administered to the patient and the presence of the following symptoms is observed: drooling, number of swallows, coughing, and dysphonia (Depippo et al., 1992). This is repeated four times with the same volume of water (10 mL) and ends with the administration of 50 mL of water in a glass. The test is positive if any symptom is present and negative if none are present. The drawback of this test is that it is only performed with large volumes, a single texture (water), and uses coughing as the sole sign of detecting aspiration. In patients with an altered cough reflex and/or low pharyngeal sensitivity, it will not be possible to detect the existence of silent aspirations and/or penetrations.
The GUSS test is divided into 2 parts: a preliminary or indirect assessment (swallowing saliva) and the direct swallowing test, with 3 different textures (semi-solids, liquids, and solids), which are performed sequentially. In the direct swallowing test, swallowing, involuntary coughing, drooling, and voice change are monitored. In the indirect test, alertness is added. Each observation is quantified by points, from 0 to 5, assigning 0 points to pathological swallowing, 1 point to delayed swallowing, and 2 points to normal swallowing. Patients evaluated must score at least 5 points in each test; if not, the test is stopped due to a high risk of aspiration. The GUSS test is validated, although the texture variation is limited (pudding, liquid, and solid) (Trapl et al., 2007).
The V-VST involves administering 5, 10, and 20 mL of food in nectar, pudding, and liquid textures, prepared with commercial thickener and in a pre-established order. It always starts with a safe bolus for the patient of 5 mL of nectar viscosity. The following signs should be observed: presence of cough, vocal changes, oral residue, fragmented swallowing, incompetence of lip closure, and pharyngeal residue. While performing the test, oxygen saturation is monitored. A decrease in basal O2 saturation ≥3% is a sign of aspiration. If, during the test, the patient presents alterations in any of the observed signs, the volume and viscosity evaluated at that time will be considered an unsafe bolus for the patient, so it will be necessary to increase the viscosity and/or decrease the volume to be able to continue with the test (Zugasti Murillo et al., 2023; Zhang P. et al., 2023). The diagnostic sensitivity of the V-VST for alterations in the safety and efficacy of swallowing is 88.1% and 89.8%, respectively. This test also helps determine the safest and most effective bolus volume and viscosity for the patient’s oral intake.
A patient who, after the clinical assessment, has shown signs of dysphagia, should undergo a complementary instrumental examination with tools that help to diagnose the functional disorder. Instrumental assessment techniques include: fiberoptic endoscopic evaluation of swallowing (FEES), videofluoroscopy (VFS), and high-resolution esophageal manometry (HRM). Each has advantages and limitations. These tools allow for the acquisition of images and objective data on the swallowing process (Scottish Intercollegiate Guidelines Network, 2010).
FEES is performed with a flexible fiberoptic scope connected to a light source through the nasal cavity to the nasopharynx. It provides anatomical information of the larynx and vocal cord function and allows assessment of the location of secretions and the patient’s ability to clear them. The assessment can also be performed with foods of different textures and volumes, thus assessing the passage of the bolus to the hypopharynx, aspiration, penetration, and the presence of residue (Triggs and Pandolfino, 2019).
In VFS, equipment is used that provides a real-time visualization of the anatomy and physiology of swallowing, along with different consistencies of barium sulphate prepared with commercial thickener. It is the gold standard for assessing OD and swallowing safety (Giraldo-Cadavid et al., 2017). This assessment allows for identification of failures in the safety and efficacy of swallowing, quantification of the oropharyngeal motor response, measurement of hyoid movement, opening of the UES, and establishment of the presence of silent aspiration (without the cough reflex) (Helliwell et al., 2023). Since barium aspiration can pose safety problems, water-soluble contrast agents are usually the preferred option. On the other hand, it must be ensured that the benefits of exposure to ionizing radiation outweigh the risks to which the patient is exposed (RCSLT. Videofluoroscopic evaluation of oropharyngeal swallowing function VFS, 2013). The inability to transport the VFS equipment and the impossibility of performing the test in people with low consciousness limit its use.
HRM is performed with a flexible catheter with sensors (one per centimeter), which is introduced through the nostrils, through the esophagus and into the stomach. The pressure data from these sensors are presented as a colour-coded topographic graph of esophageal pressure activity (Yazaki et al., 2024). HRM provides a simultaneous and integrated assessment of pharyngeal, esophageal, upper esophageal sphincter, and lower esophageal sphincter function in real time. It is considered the gold standard for identifying and classifying esophageal motility disorders (Fox et al., 2021).
Presbyphagia, also known as ‘primary dysphagia’, is the result of the effects of the normal ageing process on the swallowing organs in healthy older adults (Martin et al., 1991). It is understood as a transitional state between healthy swallowing and oropharyngeal dysphagia, resulting from all the anatomical and functional changes that occur with ageing, be they central and/or peripheral (Figure 4) (Ambiado Lillo and Borjas Galvis, 2021; Labeit et al., 2022).
During ageing, physiological functions gradually deteriorate. This functional degradation is caused by nine molecular and cellular phenomena associated with normal ageing, classified as primary, antagonistic, and integrative (Hou et al., 2019). Primary changes include genomic instability, telomere attrition, epigenetic alterations, and loss of proteostasis. Antagonistic features (mitochondrial dysfunction, cellular senescence, and deregulated nutrient sensing) are compensatory responses to primary damage but can become detrimental over time. Integrative features (stem cell exhaustion and altered intercellular communication) arise as a result of the cumulative damage produced by primary and antagonistic features and would be responsible for the functional decline associated with ageing (López-Otín et al., 2023). The manifestation of these processes affecting swallowing are changes in the nervous, skeletal, muscular, sensory, and respiratory systems (Figure 6).
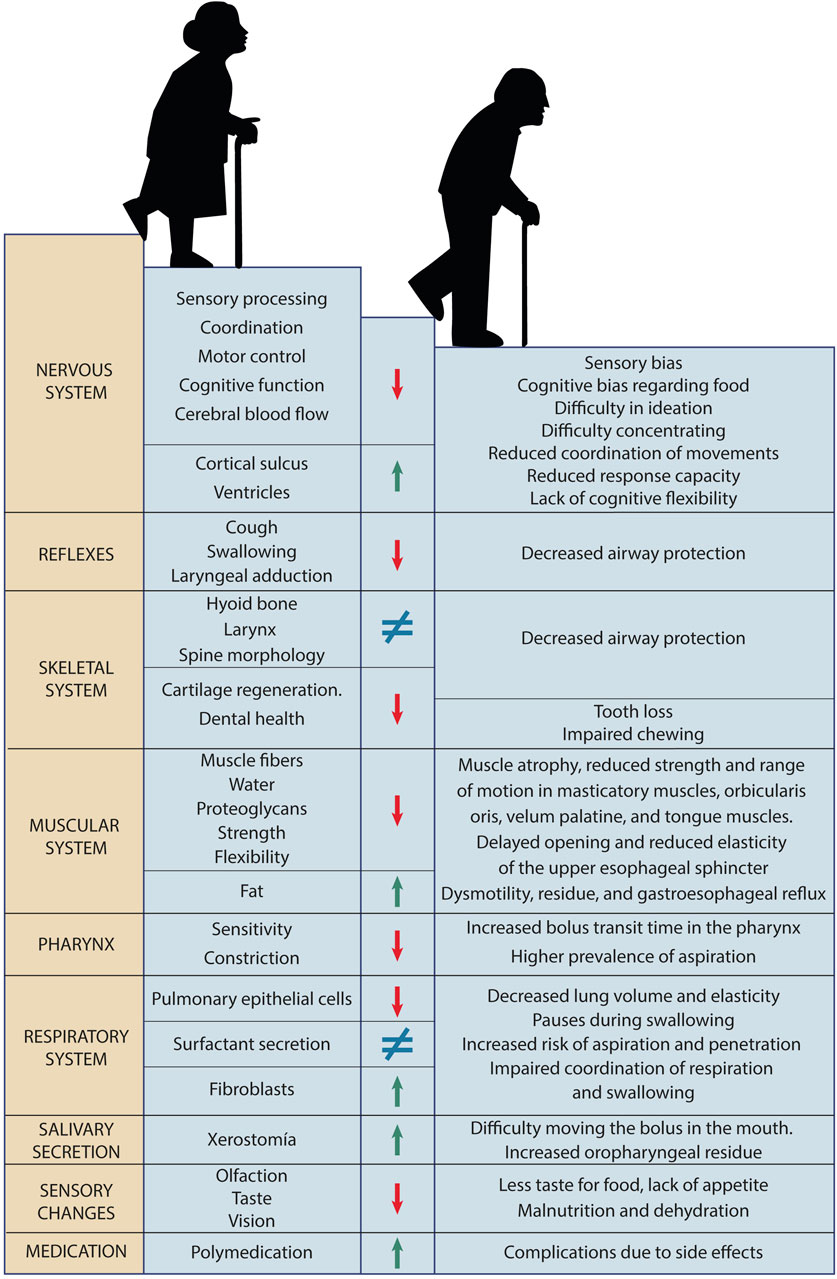
Figure 6. Changes during aging. Affected system, structures and functions affected, improvement or worsening, and impact on swallowing.
Neurodegeneration during ageing decreases activation of areas corresponding to sensory processing, sensorimotor integration, coordination, and motor control (Figure 7). The volume of some neuronal nuclei and the capacity to process information decrease. As anatomical manifestations of changes in the nervous system, cerebral blood flow is reduced, the cortical sulcus widens, and the ventricles enlarge, and dysmotility associated with a decrease in myenteric neurons of the esophagus occurs (Feng et al., 2023). Moreover, the decrease in cognitive function in ageing causes cognitive bias regarding food characteristics, difficulty in ideation and concentration. Older adults have a lower response capacity, poor coordination of movements, and lack of flexibility to adjust the speed of eating and food intake (Harada et al., 2013). Changes in the nervous system during ageing often also lead to a deterioration of swallowing reflexes, the cough reflex (which protects the airways), and laryngeal adduction (Katsumata et al., 1995; Ebihara et al., 2012).
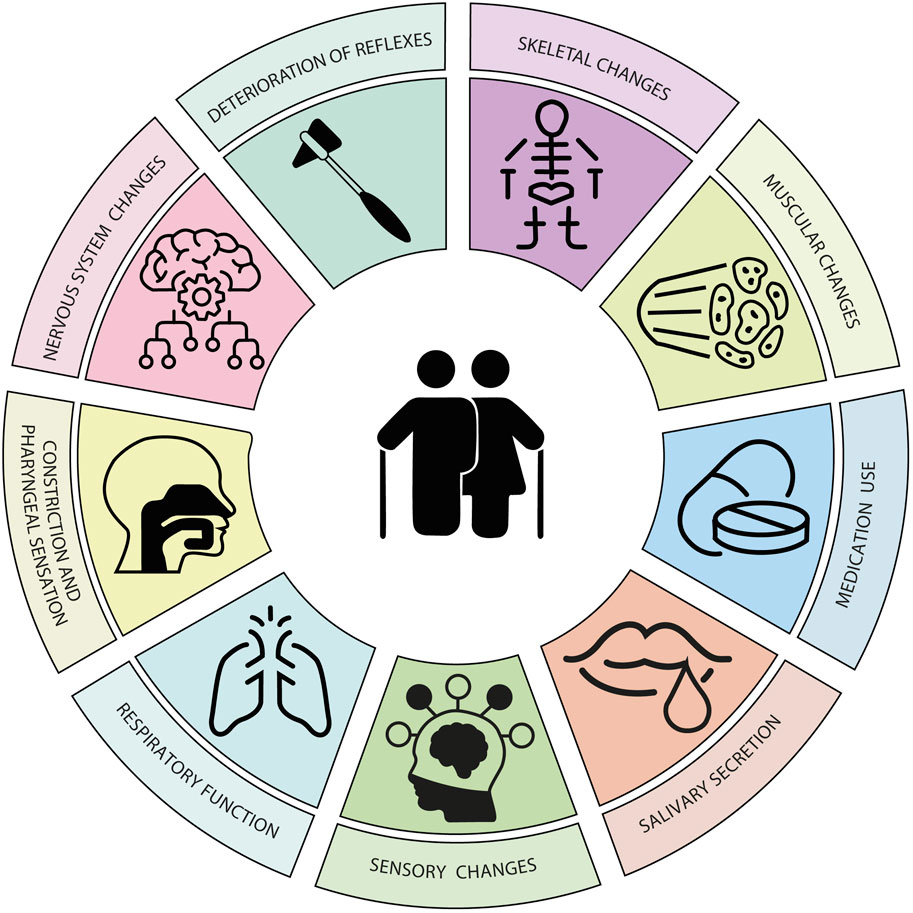
Figure 7. Age-related changes affecting swallowing. The combination of skeletal, muscular, sensory, and respiratory changes, along with decreased reflexes, salivation, laryngeal constriction and sensation, and increased medication use in this stage of life contributes to the onset of presbyphagia.
The skeletal system involved in swallowing is also affected by the changes of ageing. The positions of the hyoid bone and larynx are altered due to variations in the morphology of the spine and the reduction of muscle tone (Kang et al., 2010). Aged cartilage (due to the accumulation of senescent chondrocytes) changes shape and becomes less elastic, weakening the protective capacity of the airways of the epiglottis and arytenoid cartilages (Williams and Day, 2003; Coryell et al., 2021). With ageing, the neurovascular structures of the dental pulp are also affected and teeth become sensitive, painful, when injured and infected. Both the loss of teeth and the use of poorly adapted prostheses negatively influence swallowing (Bartlett and O’Toole, 2019).
Total muscle mass in older adults, water content in muscles, and proteoglycans in tendons decreases, while fat accumulation increases (Larsson et al., 2019). This causes a decrease in muscle contraction force, with less flexibility and less coordination in swallowing functions (Dao et al., 2020). The orbicularis oris muscle (causing leakage), the masticatory muscles, the velum palatine, and the muscles of the tongue are affected, showing muscle atrophy, reduced strength, and reduced range of motion (McCoy and Desai, 2018). Similarly, the number of muscle fibers of the UES decreases and the impulses that maintain cricopharyngeal tension also gradually decrease. This results in a delayed opening time and less amount of UES openings. On the other hand, muscle connective tissue increases, which generates less elasticity and distensibility of the sphincter. The degree and duration of UES opening are abnormal, which increases the risk of aspiration, pharyngeal residue, and gastroesophageal reflux (Cock and Omari, 2018).
The impairment of respiratory function with ageing is caused by the decrease in the number of pulmonary epithelial cells, the increase in the proportion of fibroblasts, and the alteration of surfactant. All this causes a decrease in lung volume and elasticity, reducing the ability of older adults to clear respiratory waste, increasing the risk of aspiration and penetration (Brandenberger and Mühlfeld, 2017). The weakening of respiratory function causes older adults to take longer pauses in breathing during swallowing and this compromises the coordination of both functions (Skloot, 2017).
Sensory perception also progressively deteriorates with ageing. Older adults have thinner oral mucosa, weaker secretion, fewer chemoreceptors, and reduced taste perception. This reduction in smell and taste can lead to a decreased appetite and malnutrition or dehydration (Lin, 2020). Decreased pharyngeal constriction and sensation prolongs bolus transit time through the pharynx and increases the prevalence of post-swallow aspiration (Namasivayam-MacDonald et al., 2018). The prevalence of xerostomia or dry mouth increases with age. Reduced saliva production affects food propulsion in the mouth, increases oropharyngeal residue, and the risk of poor oral hygiene (Toan and Ahn, 2021). When combined with the high consumption of medications by older adults, there is a greater risk of adverse effects on swallowing function.
Although swallowing is often preserved with age, it can exhibit signs of deterioration due to physiological changes, which worsen as the ageing process progresses. Most of these abnormalities are usually clinically silent because the patient compensates intuitively and effectively by changing the consistency of the diet and the duration of feeding (Dominguez et al., 2022; Cavallaro et al., 2022). In the presence of weakness or acute illness, a person with undiagnosed presbyphagia or aged swallowing can transition to oropharyngeal dysphagia (Namasivayam-Macdonald and Riquelme, 2019).
Over the past 2 decades, treatments for dysphagia have evolved from 1) compensatory strategies to 2) rehabilitation strategies and subsequently to 3) neurostimulation techniques that facilitate neuroplasticity for functional recovery (Figure 8). Compensatory interventions are used to modify body postures and/or bolus characteristics to reduce the risk of aspiration. The most commonly used interventions are the chin-down posture, the Mendelsohn maneuver (voluntary prolongation of the hyolaryngeal elevation and the opening of the upper esophageal sphincter), the supraglottic swallow, and the super-supraglottic swallow (to close the vocal cords and supraglottic structures) (Calandra-Buonaura et al., 2021). Food and liquid modifications are made after assessing the safe volume and viscosity for the patient. Commercial thickeners are best suited for modifying food textures, and gelled water is recommended for safe ingestion of liquids (Newman et al., 2016).

Figure 8. Swallowing treatments: a range of compensatory strategies, rehabilitation exercises, and neurostimulation techniques can be used alone or in combination.
Rehabilitation exercises aim to restore swallowing function. These include: head lift or Shaker exercise and chin tuck with resistance (CTAR) to strengthen the suprahyoid muscles, increase hyoid bone movement during swallowing, and increase the opening of the upper esophageal sphincter (Park and Hwang, 2021); the Masako maneuver or tongue-holding swallow to strengthen the base of the tongue and pharyngeal wall movement (Balou et al., 2019); expiratory muscle strength training (EMST) to synchronize breathing and swallowing and improve protective coughing (Pauloski and Yahnke, 2022); and sensory stimulation with temperature and taste contrasts. Poor oral health, in combination with dysphagia, has been identified as a dominant risk factor for aspiration pneumonia. It is believed that aspiration of saliva contaminated with bacteria is the primary pathogenic mechanism of pulmonary infections in patients with dysphagia. For this reason, oral healthcare is a supplementary recommendation for any dysphagia treatment (Dziewas et al., 2021).
Both peripheral and central (cortical and cerebellar) neurostimulation treatments can promote neuroplasticity in patients with dysphagia by modulating synaptic strength. Peripheral neurostimulation is primarily used to increase sensory information to the central nervous system, while central brain stimulation is used to induce plasticity changes in the cortex and/or cerebellum directly (Cheng and Hamdy, 2022). Neurostimulation techniques include transcutaneous electrical stimulation (TES) (Miller et al., 2022), repetitive transcranial magnetic stimulation (rTMS) (Sheng et al., 2023), transcranial direct current stimulation (tDCS) (Bengisu et al., 2024), both for cortical areas, and pharyngeal electrical stimulation (PES) (Labeit et al., 2024), targeting the pharyngeal sensory and motor cortices in the peripheral sensory afferent system. Transcutaneous electrical stimulation is used to activate the sensory nerves (sensory transcutaneous electrical stimulation) or the muscles (neuromuscular electrical stimulation) involved in swallowing function by stimulating the axonal motor nerve endings and muscle fibers (Pauloski and Yahnke, 2022).
Modified PES induces a higher frequency of involuntary swallowing. Activations of cortical regions related to swallowing have been observed and resulted in greater efficiency of the swallowing process after prolonged intervention. Therefore, it is believed that modified pharyngeal electrical stimulation could reorganize the neural network related to swallowing, making it a promising neurostimulation therapeutic method for severe neurogenic dysphagia (Zhang X. et al., 2023). Thus, the results obtained with neurostimulation techniques, including non-invasive brain stimulation and stimulation methods targeting the afferent neural pathways of swallowing, are positive. However, there is inter-subject variability in the responsiveness to these treatments (Simons and Hamdy, 2017). Genetic predisposition, brain configuration, and the level of neuronal activation prior to neurostimulation are some of the factors that may influence this variability (Rosenbek, 2014).
Ramón y Cajal was one of the first to suggest that the nervous system has an inherent ability to adapt and reorganize itself in response to experience, learning, and new physiological or even pathological conditions that arise during development or as a result of its interaction with the environment (Ramón y Cajal, 1909). Neuroplasticity or neural plasticity refers to the changes that occur in neural pathways to enhance their function through synaptogenesis, reorganization, strengthening, and suppression of networks (Pauloski and Yahnke, 2022). An example of neuroplasticity is the increase in the number of branches and synapses in older adults, thus compensating for the loss of neurons that occurs throughout life. It has been shown that the dendritic arborizations of pyramidal neurons in the cerebral cortex are 25% longer in healthy 80-year-old individuals than in 50-year-old subjects (Portera Sánchez, 2002).
The objectives of rehabilitation processes after the loss of a previously acquired function are the reconnection of neural networks and the development of new connections between neurons. Cerebral neuroplasticity not only functions as an automatic mechanism but also occurs when external stimuli are perceived, new ideas are generated, different emotions are felt, or newly learned movements are performed correctly (Saway et al., 2024). In this way, when neuroplasticity is used as a therapeutic tool, new neural connections are generated, which will form the basis for new learning (Kolb and Muhammad, 2014). This idea is fundamental to understanding how swallowing function can be recovered after a neurological injury, such as a stroke.
Regardless of the chosen treatment, there are 15 principles underlying effective neurorehabilitation that promotes neuroplasticity (Figure 9). (Maier et al., 2019) These principles govern the typology and timing of rehabilitative practice. Each temporal characteristic of the sessions and the duration of therapy must be planned to obtain the best physical and cognitive performance of the patient. Repetition during sessions and rest between repetitions improve the subject’s skills and induce profound changes in the brain’s ability to retain and process information (Anaya and Branscheidt, 2019). When planning a session, the specificity of the tasks must be considered, as this shapes the internal sensorimotor representation of the skill and facilitates motor learning and subsequent retention. When the session is goal-oriented, it promotes the achievement of a goal and leads to greater performance in motor learning than non-specific sessions (Afridi et al., 2023). Including variations of exercises in each rehabilitation session promotes generalization to similar tasks, even if these are not trained. Variability is correlated with greater neuronal activity and connectivity in the areas of the motor learning network during acquisition and is associated with better retention. If increasing difficulty is established throughout the treatment, it will result in a performance with fewer errors and less need to process information (Reid et al., 2016). During therapy, the subject’s exposure to multisensory information improves the ability to detect, discriminate, and recognise information, favouring connectivity between the motor and sensory cortices (Yang et al., 2021). The role of the therapist during the sessions is very important for sequencing the exercises and providing feedback to the patient. Rhythmic cues, usually auditory, facilitate motor execution and create a mental representation of the rhythm. The detection of regularity and the tracking of tempo increase activity in the areas of the motor network and the cerebellum (Nahum et al., 2013). Explicit feedback provides the subject with information about the quantitative or qualitative results of the task, correction, accuracy, success or failure, once the task is completed. Negative results can accelerate motor learning, while positive results ensure long-term retention. Implicit feedback is that which is given on the execution of the movement in the form of verbal descriptions, demonstrations or repetitions of recordings and which generates lasting adaptations (Silva-Batista et al., 2023). The therapist must also modulate the selection of effectors because not using a damaged muscle due to fear or comfort leads to a loss of neural function and correct behavior. Observing the action by the patient, as well as performing it, primarily recruits the premotor and parietal cerebral cortical areas, which could facilitate the execution of movement and motor learning by enhancing the excitability of the motor system. Performing mental practice gives the subject the ability to mentally simulate actions without overt behavior. This practice would recruit premotor areas, somatosensory cortex and subcortical areas as does effective practice, but also activation was found in the anterior cingulate cortex, which is linked to the cognitive aspects of motor control. The performance of group sessions benefits social interaction and the actions of one participant are both a response and a stimulus for the behavior of another. Self-perception of one’s own performance influences motor skill performance and learning but is also influenced by the evaluation or discouragement from others (Maier et al., 2019). Most patients with neurological damage will experience deficits that will change their lives beyond the acute phase. Therefore, neurorehabilitation is an important component of recovery. Although there are significant variations in the type of therapy, its duration and/or intensity; the application of the 15 principles based on neuroplasticity will facilitate the planning of neurorehabilitation treatment to achieve the established therapeutic goals.
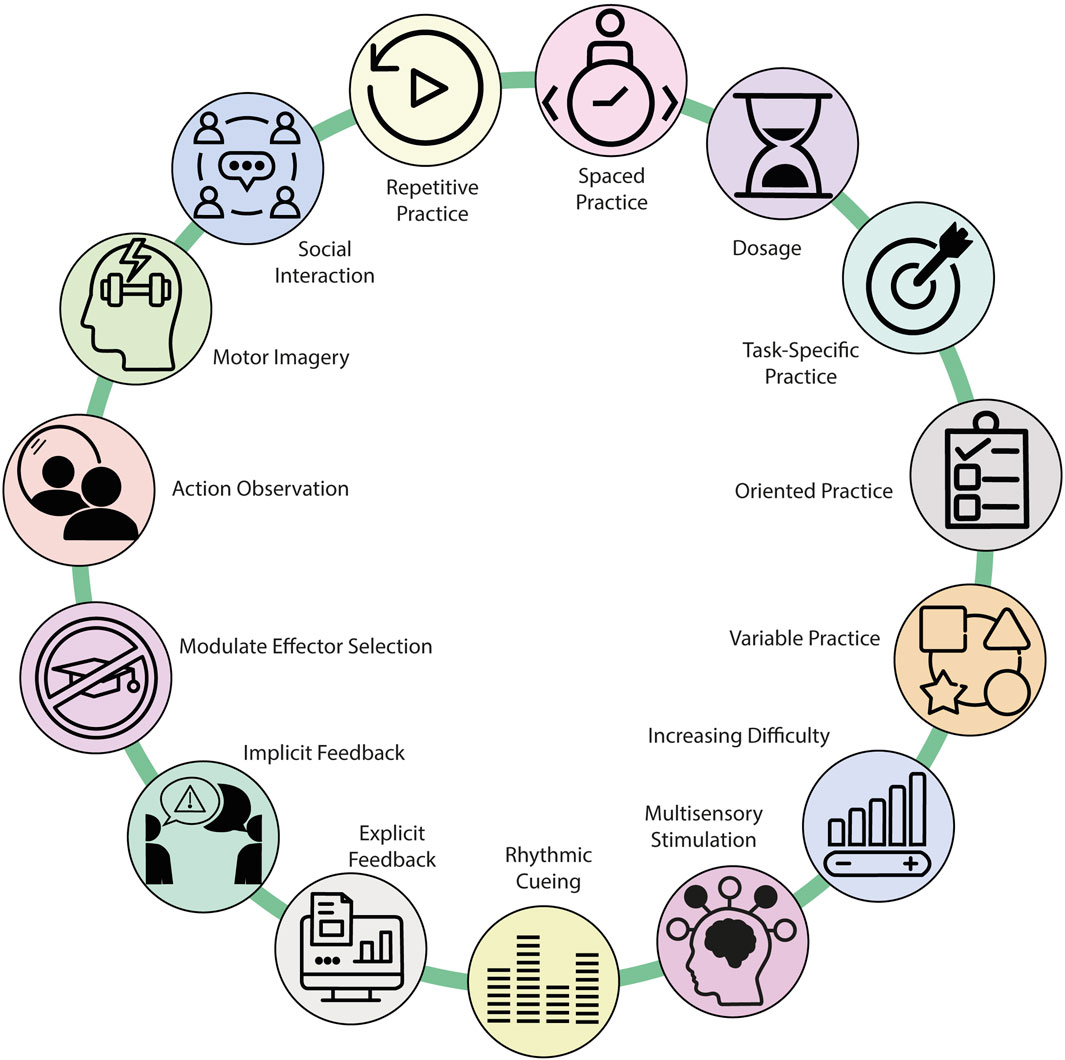
Figure 9. Neuroplasticity-driven principles of neurorehabilitation for achieving rehabilitation treatment goals.
The consequences of dysphagia include malnutrition, dehydration, and in many cases, death from aspiration pneumonia (Mandell and Niederman, 2019). Prevention is presented as a tool to mitigate the deficits caused by impaired swallowing in older adults. Currently, there are no records of structured prevention practices because clinical practice shows that, often, both doctors and patients interpret dysphagia as a normal consequence of ageing and underestimate it (Tulunay-Ugur and Eibling, 2018).
Dysphagia prevention would only be possible before or during presbyphagia as the theory suggests that presbyphagia and dysphagia are on a continuum and that one progresses through this continuum as one ages (Namasivayam-MacDonald et al., 2018).Detection and assessment to determine swallowing disorders should be carried out as soon as possible in at-risk groups. Likewise, the adult population should be educated to self-detect early signs of dysphagia. The administration of subjective questionnaires, objective screening tests, dental and oral healthcare, attention to diet, and strength and endurance exercises for the swallowing muscles would, taken together, be an effective programme for the prevention of dysphagia during ageing (Chen et al., 2021).
The administration of a self-perception questionnaire to apparently healthy people over the age of 65 can enable the early diagnosis of presbyphagia and facilitate its rehabilitation (Cavallaro et al., 2022). The validated screening protocol for use with older adults living in the community and their caregivers and/or family members is the EAT-10 (Bartlett et al., 2022). Once self-perceived swallowing problems have been identified and to objectify the swallowing disorder, it is necessary to perform screening tests such as the GUSS, the V-VST, and also a test to assess chewing ability, the Test of Masticating and Swallowing Solids (TOMASS) (Huckabee et al., 2018) proposed for older adult patients who have well-fitted dental pieces and/or dentures. The results of objective screening tests will also facilitate the control of bolus volume and viscosity in the oral preparatory and oral propulsion stages for the ingestion of solids and liquids (Jiang et al., 2024). Dental care (replacement of missing teeth, repair of diseased teeth, and/or adjustment of dentures) improves chewing, bolus formation, and management. In turn, promoting oral hygiene will serve to reduce bacterial colonisation and prevent respiratory infections in case of penetration or aspiration. To complete the prevention plan, a strength and resistance exercise programme would be necessary (Carnaby et al., 2020). Although very little research has been done to elucidate the role of preventive exercises in the population, significant improvements in swallowing physiology have been found after the application of 8-week comprehensive swallowing treatment protocols (Balou et al., 2019) and tongue strengthening exercise programmes in older adults. These interventions, although scarce, have managed to increase isometric pressure and improve swallowing in older adults (Namasivayam-MacDonald et al., 2018).
New technologies are a reality in our daily lives and have become tools that facilitate processes, both at home and in the workplace and healthcare (Sejdic et al., 2020). Artificial intelligence (AI) is a commonly used term to refer to the field of science aimed at equipping machines with the ability to perform functions such as logic, reasoning, planning, learning, and perception. Thus, these autonomous entities are capable of correctly interpreting external data, learning from that data, and using that knowledge to achieve specific tasks and goals through flexible adaptation (Kaplan and Haenlein, 2019). AI encompasses various technological aspects: planning, robotics, natural language processing, perception, knowledge, and machine learning. In medicine, machine learning has been used to create models for detecting and diagnosing diseases (Foster et al., 2014), for triage (Wu et al., 2020), for epidemiological analysis (Schneeweiss and Avorn, 2005), and as a support for clinical decision-making by predicting disease risk (Gultepe et al., 2014; Myszczynska et al., 2020) The usefulness of AI in dysphagia ranges from screening and detecting the disorder, even in asymptomatic patients, to the administration of rehabilitation treatments to patients who would otherwise not have had access to treatment (Coyle and Sejdić, 2020). Dysphagia screening in large populations is costly. For this purpose, an expert system (ES) based on machine learning has been developed, which calculates the risk of OD from the analysis of the clinical history data of all elderly hospitalized patients during their admission to a hospital. The software developed (AIMS-OD) provides systematic and universal screening of OD in real time during hospital admission, allowing the selection of the most appropriate diagnostic and therapeutic strategies for each patient (Martin et al., 2023). In the evaluation of dysphagia, the use of cervical auscultation (CA) has been implemented to analyse the sounds emanating from the neck during swallowing and which could reflect abnormal physiological events during the same (Borr et al., 2007). This evaluation method depends on the therapist who must be trained and have extensive experience. Currently, AI allows high-resolution cervical auscultation (HRCA) recordings to be made, through accelerometers placed on the patient’s neck. These recordings are analysed with a neural network trained to detect abnormal opening and closing of the UES, with over 90% accuracy (Coyle and Sejdić, 2020). In the laboratory, an adaptive reinforcement machine learning algorithm has been shown to have diagnostic value and efficacy for dysphagia by also analysing the patient’s swallowing sounds, recorded with an electronic stethoscope (Suzuki et al., 2022). The possibility of collecting data non-invasively through swallowing sounds has expanded the modalities of dysphagia assessment. The development of a real-time portable assessment tool, incorporated into a smartphone, allows for bedside patient assessment or remote assessment of those patients who are unable to move. This portable model (GOKURI) consists of three units: a neck band with a microphone, an amplifier, and an interface that displays results and statistics (Kou et al., 2022). Currently, the identification of a wet voice as a sign of aspiration depends on the experience and auditory ability of the evaluator. With new technologies, the spectrogram and voice data of a patient, performing four phonatory tasks, can be analysed with a deep learning model. These data, which are non-invasive to obtain, are a reliable tool for the diagnosis of dysphagia (Kim et al., 2023). Monitoring the displacement of the hyoid bone during swallowing in real time is another diagnostic method currently performed with VFS. In cases where the hyoid bone is lower and has little mobility, it suggests that the risk of dysphagia would be high. With machine learning and AI, it has been possible to avoid the radiation of VFS since the tracking of hyoid movement is performed with accelerometers placed on the patient’s neck and the data is analysed automatically. This method has an accuracy of over 89% (Matsuda et al., 2022). The use of new technologies has also extended to the treatment of dysphagia with the development of a prototype of an intelligent assistant that monitors adherence and provides feedback to the patient. This prototype is based on the need for the affected subject to visualise the practice, in order to promote neuroplasticity and self-perception. It is a mobile application that, when placed in front of the patient, acts as a mirror and a source of feedback to help with the use of safe compensatory strategies (Freed et al., 2016).
The integration of advanced technologies into the field of dysphagia management has significantly enhanced the diagnostic process and treatment outcomes. These new technologies offer more precise and objective assessments, reducing reliance on subjective evaluations. Early detection of dysphagia enables proactive intervention, mitigating the risk of complications such as aspiration pneumonia. Additionally, personalized treatment plans tailored to the individual characteristics and needs of the patient can optimize outcomes and improve patient satisfaction. Furthermore, remote monitoring and telemedicine capabilities expand access to dysphagia services, particularly in underserved regions. By streamlining diagnosis and treatment, these technologies can also lead to reduced healthcare expenditures.
While these advancements offer substantial benefits, the implementation of new technologies in dysphagia care is not free of challenges. Key areas for future research and development include ensuring the reliability and efficacy of these technologies through rigorous clinical validation. Moreover, integrating these technologies seamlessly into routine clinical practice is crucial to maximize their impact. Developing more sophisticated algorithms can further improve the accuracy and precision of diagnostic and treatment tools. Additionally, understanding the factors that influence the adoption and use of new technologies by patients and healthcare providers is essential for successful implementation. By addressing these limitations and investing in ongoing research, the full potential of new technologies in dysphagia management can be realized, leading to improved patient outcomes and a better quality of life.
Swallowing is a complex mechanism that involves cortical areas, five cranial nerves, the first three cervical segments, and muscles of the mouth, pharynx, and esophagus, coordinated from the brainstem. Dysphagia is a swallowing disorder that affects the quality of life of patients who suffer from it and endangers their lives due to the severity of its consequences. Presbyphagia, as a manifestation of physiological ageing, has been a commonly overlooked health problem, so it would be necessary to implement early detection and specific intervention measures. New technologies and AI generate possibilities for large-scale screening of dysphagia, prevention, and remote treatments implemented by assistive robotic platforms. The development of systems capable of interacting reliably with people through speech recognition, facial recognition, and real-time monitoring of functions and vital signs enables the early detection of signs. The prevention of dysphagia in ageing is possible, but it requires a multidisciplinary approach that combines early detection, adequate assessment, specific care programes, and new technologies, so that eating, during ageing, becomes satisfying and safe again.
MIP: Investigation, Conceptualization, Visualization, Writing–original draft, Writing–review and editing. RMB: Validation, Writing–review and editing. AMLO: Validation, Writing–review and editing. AMGC: Validation, Writing–review and editing. EFV: Validation, Writing–review and editing. MTH: Conceptualization, Funding acquisition, Project administration, Resources, Supervision, Writing–original draft, Writing–review and editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The study was supported by the grants from the Agencia Estatal de Investigación, Ministerio de Ciencia, Innovación y Universidades, co-funded by European Union, Next-Generation EU/PRTR Ref. Number: TED 2021-130942B-C21//MICIU/AEI/10.13039/501100011033, the “Fundación Primafrío” with the code number 39747 and COST Participatory Approaches with Older Adults (PAAR-net), with the code number CA22167, and China-Spain AI Technology Joint Laboratory with Hangzhou Dianzi University.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
The authors declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Afridi, A., Malik, A., and Rathore, F. (2023). Task oriented training for stroke rehabilitation: a mini review. Rehabil. Sci. corner 73 (11), 2295–2297. doi:10.47391/JPMA.23-98
Allen, J., Greene, M., Sabido, I., Stretton, M., and Miles, A. (2020). Economic costs of dysphagia among hospitalized patients. Laryngoscope 130 (4), 974–979. doi:10.1002/lary.28194
Alsaied, A. S., and Postma, G. N. (2019). In-office evaluation and management of dysphagia, Office Eval. Manag. Dysphagia. Vol. 52, 577–587. doi:10.1016/j.otc.2019.02.007
Ambiado Lillo, M., and Borjas Galvis, J. (2021). Presbifagia: Una Mirada a los Procesos de Alimentación y Deglución en los Adultos Mayores. Areté 21 (1), 105–112. doi:10.33881/1657-2513.art.21110
Ambrocio, K. R., Miles, A., Bhutada, A. M., Choi, D., and Garand, K. L. (2023). Defining normal sequential swallowing biomechanics. Dysphagia 38 (6), 1497–1510. doi:10.1007/s00455-023-10576-z
Anaya, M. A., and Branscheidt, M. (2019). Neurorehabilitation after stroke: from bedside to the laboratory and back. Stroke 50 (7), e180–e182. doi:10.1161/STROKEAHA.118.023878
Baijens, L. W. J., Clavé, P., Cras, P., Ekberg, O., Forster, A., Kolb, G. F., et al. (2016). “European society for swallowing disorders - European Union geriatric medicine society white paper: oropharyngeal dysphagia as a geriatric syndrome,” Clin. Interventions Aging, 11. 1403–1428. doi:10.2147/CIA.S107750
Ballesteros-Pomar, M., Cherubini, A., Keller, H., Lam, P., Rolland, Y., and Simmons, S. (2020). Texture-modified diet for improving the management of oropharyngeal dysphagia in nursing home residents: an expert review. J. Nutr. Health Aging. 24, 576–581. doi:10.1007/s12603-020-1377-5
Balou, M., Herzberg, E. G., Kamelhar, D., and Molfenter, S. M. (2019). An intensive swallowing exercise protocol for improving swallowing physiology in older adults with radiographically confirmed dysphagia. Clin. Interv. Aging 14, 283–288. doi:10.2147/CIA.S194723
Bartlett, D., and O’Toole, S. (2019). Tooth wear and aging. Aust. Dent. J. 64 (S1), S59–S62. doi:10.1111/adj.12681
Bartlett, R. S., Kenz, M. K., Wayment, H. A., and Thibeault, S. L. (2022). Correlation between EAT-10 and aspiration risk differs by dysphagia etiology. Dysphagia 37 (1), 11–20. doi:10.1007/s00455-021-10244-0
Bengisu, S., Demir, N., and Krespi, Y. (2024). Effectiveness of conventional dysphagia therapy (cdt), neuromuscular electrical stimulation (nmes), and transcranial direct current stimulation (tDCS) in acute post-stroke dysphagia: a comparative evaluation. Dysphagia 39 (1), 77–91. doi:10.1007/s00455-023-10595-w
Binkofski, F., Schnitzler, A., Enck, P., Frieling, T., Posse, S., Seitz, R. J., et al. (1998). Somatic and limbic cortex activation in esophageal distention: a functional magnetic resonance imaging study. Ann. Neurol. 44 (5), 811–815. doi:10.1002/ana.410440516
Borr, C., Hielscher-Fastabend, M., and Lücking, A. (2007). Reliability and validity of cervical auscultation. Dysphagia 22 (3), 225–234. doi:10.1007/s00455-007-9078-3
Brandenberger, C., and Mühlfeld, C. (2017). “Mechanisms of lung aging,” Cell. Tissue Res., 367, 469–480. doi:10.1007/s00441-016-2511-x
Calandra-Buonaura, G., Alfonsi, E., Vignatelli, L., Benarroch, E. E., Giannini, G., Iranzo, A., et al. (2021). “Dysphagia in multiple system atrophy consensus statement on diagnosis, prognosis and treatment,” Park. Relat. Disord., 86, 124–132. doi:10.1016/j.parkreldis.2021.03.027
Carnaby, G. D., LaGorio, L., Silliman, S., and Crary, M. (2020). Exercise-based swallowing intervention (McNeill Dysphagia Therapy) with adjunctive NMES to treat dysphagia post-stroke: a double-blind placebo-controlled trial. J. Oral Rehabil. 47 (4), 501–510. doi:10.1111/joor.12928
Cavallaro, G., Pontrelli, M., Sammali, M., Nelson, E., Quaranta, N., and Fiorella, M. L. (2022). Presbyphagia: the importance of an early diagnosis in the aging population. J. Gerontology Geriatrics 70 (4), 1–7. doi:10.36150/2499-6564-n502
Chen, S., Kent, B., and Cui, Y. (2021). Interventions to prevent aspiration in older adults with dysphagia living in nursing homes: a scoping review. BMC Geriatr. 21 (1), 429. doi:10.1186/s12877-021-02366-9
Cheng, I., and Hamdy, S. (2022). “Metaplasticity in the human swallowing system: clinical implications for dysphagia rehabilitation,” Neurol. Sci., 43. 199–209. doi:10.1007/s10072-021-05654-9
Clavé, P., Arreola, V., Romea, M., Medina, L., Palomera, E., and Serra-Prat, M. (2008). Accuracy of the volume-viscosity swallow test for clinical screening of oropharyngeal dysphagia and aspiration. Clin. Nutr. 27 (6), 806–815. doi:10.1016/j.clnu.2008.06.011
Clavé, P., Arreola, V., and Velasco, M. (2015). “Evaluación y diagnóstico de la disfagia orofaríngea,” in Guía de diagnóstico y de tratamiento nutricional y rehabilitador de la disfagia orofaríngea. Editors P. Clavé, and P. García, 3rd ed. (Barcelona: Editorial Glossa), 57–78.
Clavé, P., Rofes, L., Arreola, V., Almirall, J., Cabré, M., Campins, L., et al. (2011). Diagnosis and management of oropharyngeal dysphagia and its nutritional and respiratory complications in the elderly. Gastroenterology Res. Pract. 2011, 818979. doi:10.1155/2011/818979
Cock, C., and Omari, T. (2018). Systematic review of pharyngeal and esophageal manometry in healthy or dysphagic older persons (>60 years). Geriatr. (Basel)., 3, 67, doi:10.3390/geriatrics3040067
Coryell, P. R., Diekman, B. O., and Loeser, R. F. (2021). “Mechanisms and therapeutic implications of cellular senescence in osteoarthritis,” Nat. Rev. Rheumatol., 17. 47–57. doi:10.1038/s41584-020-00533-7
Costa, M. M. B. (2018). Neural control of swallowing. Arq. Gastroenterol. IBEPEGE - Inst. Bras. Estud. Pesqui. Gastroent. 55, 61–75. doi:10.1590/S0004-2803.201800000-45
Coyle, J. L., and Sejdić, E. (2020). High-resolution cervical auscultation and data science: new tools to address an old problem. Am. J. Speech Lang. Pathol. 29 (2S), 992–1000. doi:10.1044/2020_AJSLP-19-00155
Dao, T., Green, A. E., Kim, Y. A., Bae, S. J., Ha, K. T., Gariani, K., et al. (2020). “Sarcopenia and muscle aging: a brief overview,” Endocrinol. Metabolism, 35. 716–732. doi:10.3803/EnM.2020.405
Deng, H., Xiao, X., Yang, T., Ritola, K., Hantman, A., Li, Y., et al. (2021). A genetically defined insula-brainstem circuit selectively controls motivational vigor. Cell. 184 (26), 6344–6360.e18. doi:10.1016/j.cell.2021.11.019
Depippo, K. L., Holas, M. A., Reding, M. J., and Cornell, F. (1992). Validation of the 3-oz water swallow test for aspiration following stroke. Arch. Neurol. 49, 1259–1261. doi:10.1001/archneur.1992.00530360057018
Dominguez, L. J., Veronese, N., Baiamonte, E., Guarrera, M., Parisi, A., Ruffolo, C., et al. (2022). Nutrients Healthy aging and dietary patterns, 14 (4), 889. doi:10.3390/nu14040889
Dylczyk-Sommer, A. (2020). Dysphagia. Part 1: general issues. Anaesthesiol. Intensive Ther. 52 (3), 226–232. doi:10.5114/ait.2020.98074
Dziewas, R., Michou, E., Trapl-Grundschober, M., Lal, A., Arsava, E. M., Bath, P. M., et al. (2021). European Stroke Organisation and European Society for Swallowing Disorders guideline for the diagnosis and treatment of post-stroke dysphagia. Eur. Stroke J. 6 (3), LXXXIX–CXV. doi:10.1177/23969873211039721
Ertekin, C., and Aydogdu, I. (2003). Neurophysiology of swallowing. Vol. 114, clinical neurophysiology. Elsevier Ireland Ltd, 2226–2244.
Farneti, D., Turroni, V., and Genovese, E. (2018). Aspiration: diagnostic contributions from bedside swallowing evaluation and endoscopy. Acta Otorhinolaryngol. Ital. 38 (6), 511–516. doi:10.14639/0392-100X-1967
Feng, H., Zhang, P. P., and Wang, X. W. (2023). Presbyphagia: dysphagia in the elderly. World J. Clin. Cases 11(11):2363–2373. doi:10.12998/wjcc.v11.i11.2363
Foster, K. R., Koprowski, R., and Skufca, J. D. (2014). Machine learning, medical diagnosis, and biomedical engineering research - commentary. Vol. Biomed. Eng. Online, 13, 94. doi:10.1186/1475-925X-13-94
Fox, M. R., Sweis, R., Yadlapati, R., Pandolfino, J., Hani, A., Defilippi, C., et al. (2021). Chicago classification version 4.0© technical review: update on standard high-resolution manometry protocol for the assessment of esophageal motility. Neurogastroenterol. Motil. 33 (4), e14120. doi:10.1111/nmo.14120
Freed, M., Burns, B., Heller, A., Sánchez, D., and Beaumont-Bowman, S. (2016). “A virtual assistant to help dysphagia patients eat safely at home,” in Twenty-fifth international joint conference on artificial intelligence (IJCAI-16). Editor S. Kambhampati (Palo Alto, California: AAAI Press), 4244–4245.
Giraldo-Cadavid, L. F., Leal-Leaño, L. R., Leon-Basantes, G. A., Bastidas, A. R., Garcia, R., Ovalle, S., et al. (2017). Accuracy of endoscopic and videofluoroscopic evaluations of swallowing for oropharyngeal dysphagia. Laryngoscope 127 (9), 2002–2010. doi:10.1002/lary.26419
González Cortés, M., Castro Macía, O., and Domínguez Collado, L. (2018). “Disfagia y envejecimiento,” in Disfagia orofaríngea: actualización y manejo en poblaciones específicas. Sociedad Gallega de Otorrinolaringología y Patología Cérvico-Facial. Editors M. Rodríguez Acevedo, P. Vaamonde Lago, P. T. González, A. Quintana Sanjuás, and M. González Cortés 1st ed, 181–188.
Gultepe, E., Green, J. P., Nguyen, H., Adams, J., Albertson, T., and Tagkopoulos, I. (2014). From vital signs to clinical outcomes for patients with sepsis: a machine learning basis for a clinical decision support system. J. Am. Med. Inf. Assoc. 21 (2), 315–325. doi:10.1136/amiajnl-2013-001815
Hamdy, S., Aziz’, Q., Rothwe, J. C., Singh, K. D., Hughes, D. G., Barlow, J., et al. (1996). The cortical topography of human swallowing musculature in health and disease Nat. Med., 2, 1217, 1224. doi:10.1038/nm1196-1217
Harada, C. N., Natelson Love, M. C., and Triebel, K. L. (2013). Normal cognitive aging. Clin. Geriatric Med. 29, 737–752. doi:10.1016/j.cger.2013.07.002
Helliwell, K., Hughes, V. J., Bennion, C. M., and Manning-Stanley, A. (2023). The use of videofluoroscopy (VFS) and fibreoptic endoscopic evaluation of swallowing (FEES) in the investigation of oropharyngeal dysphagia in stroke patients: a narrative review, Radiography (Lond) 29, 284–290. doi:10.1016/j.radi.2022.12.007
Huckabee, M. L., McIntosh, T., Fuller, L., Curry, M., Thomas, P., Walshe, M., et al. (2018). The Test of Masticating and Swallowing Solids (TOMASS): reliability, validity and international normative data. Int. J. Lang. Commun. Disord. 53 (1), 144–156. doi:10.1111/1460-6984.12332
Humbert, I. A., and Robbins, J. A. (2007). Normal swallowing and functional magnetic resonance imaging: a systematic review. Dysphagia 22, 266–275. doi:10.1007/s00455-007-9080-9
Hurtte, E., Young, J., and Gyawali, C. P. (2023). “Dysphagia. Vol. 50,” in Primary care - clinics in office practice. W.B. Saunders, 325–338.
Jardine, M., Miles, A., and Allen, J. (2020). A systematic review of physiological changes in swallowing in the oldest old. Dysphagia 35 (3), 509–532. doi:10.1007/s00455-019-10056-3
Jiang, Y., Chi, Y., Pan, R., Zhang, D., Huang, S., Ju, H., et al. (2024). Advancing stroke patient care: a network meta-analysis of dysphagia screening efficacy and personalization. Front. Neurol. 15, 1380287. doi:10.3389/fneur.2024.1380287
Kalhoff, H., Kersting, M., Sinningen, K., and Lücke, T. (2024). “Development of eating skills in infants and toddlers from a neuropediatric perspective,” Italian J. Pediatr., 50. doi:10.1186/s13052-024-01683-0
Kang, B. S., Oh, B. M., Kim, I. S., Chung, S. G., Kim, S. J., and Han, T. R. (2010). Influence of aging on movement of the hyoid bone and epiglottis during normal swallowing: a motion analysis. Gerontology 56 (5), 474–482. doi:10.1159/000274517
Kaplan, A., and Haenlein, M. (2019). Siri, Siri, in my hand: who’s the fairest in the land? On the interpretations, illustrations, and implications of artificial intelligence, 62. Business Horizons. Elsevier Ltd, 15–25.
Kern, M. K., Jaradeh, S., Arndorfer, R. C., and Shaker, R. (2001). Cerebral cortical representation of reflexive and volitional swallowing in humans Am. J. Physiol. Gastrointest. Liver Physiol., 280, G354–G360. doi:10.1152/ajpgi.2001.280.3.G354
Kim, H., Park, H. Y., Park, D. G., Im, S., and Lee, S. (2023). Non-invasive way to diagnose dysphagia by training deep learning model with voice spectrograms. Biomed. Signal Process Control. 86, 105259. doi:10.1016/j.bspc.2023.105259
Kiyohara, H., Umezaki, T., Sawatsubashi, M., Matsumoto, N., and Komune, S. (2012). Evaluation of volitional and reflexive swallowing in elderly patients with a history of pneumonia, Eval. Volitional Reflexive Swallowing Elder. Patients a Hist. Pneumonia 121, 174, 178. doi:10.1177/000348941212100306
Knollhoff, S. M., Hancock, A. S., Barrett, T. S., and Gillam, R. B. (2022). Cortical activation of swallowing using fNIRS: a proof of concept study with healthy adults. Dysphagia 37 (6), 1501–1510. doi:10.1007/s00455-021-10403-3
Kolb, B., and Muhammad, A. (2014). Harnessing the power of neuroplasticity for intervention, Harnessing power Neuroplast. intervention. Vol. 8, 377, doi:10.3389/fnhum.2014.00377
Kou, W., Galal, G. O., Klug, M. W., Mukhin, V., Carlson, D. A., Etemadi, M., et al. (2022). Deep learning–based artificial intelligence model for identifying swallow types in esophageal high-resolution manometry. Neurogastroenterol. Motil. 34 (7), e14290. doi:10.1111/nmo.14290
Krishnamurthy, R., Philip, R., Balasubramanium, R. K., and Rangarathnam, B. (2021). Effects of dual-task interference on swallowing in healthy aging adults. PLoS One 16 (6 June), e0253550. doi:10.1371/journal.pone.0253550
Labeit, B., Michou, E., Trapl-Grundschober, M., Suntrup-Krueger, S., Muhle, P., Bath, P. M., et al. (2024). Dietary intervention for post-stroke dysphagia - authors' reply, Dysphagia after stroke Res. Adv. Treat. interventions 23. 764, 765. doi:10.1016/S1474-4422(24)00267-9
Labeit, B., Muhle, P., von Itter, J., Slavik, J., Wollbrink, A., Sporns, P., et al. (2022). Clinical determinants and neural correlates of presbyphagia in community-dwelling older adults. Front. Aging Neurosci. 14, 912691. doi:10.3389/fnagi.2022.912691
Lang, I. M. (2009). Brain stem control of the phases of swallowing. Dysphagia 24, 333–348. doi:10.1007/s00455-009-9211-6
Larsson, L., Degens, H., Li, M., Salviati, L., Lee, Y., Thompson, W., et al. (2019). Sarcopenia: aging-related loss of muscle mass and function. Physiol. Rev. 99, 427–511. doi:10.1152/physrev.00061.2017
Li-Jessen, N., and Ridgway, C. (2020). “Neuroanatomy of voice and swallowing,” in Neurologic and neurodegenerative diseases of the larynx. Editors P. Weissbrod, and D. Francis, 1st ed. (Cham: Springer), 21–41.
Lin, F. R. (2020). “Making sense of the senses in aging research,” Journals Gerontology - Ser. A Biol. Sci. Med. Sci., 75, 529–530. doi:10.1093/gerona/glaa028
López Ortega, M., Palacio Ortega, M., Landeros, R., Bermejo Alegría, R., and Fernández Rego, F. (2024). “Desarrollo del aparato estomatognático y de la función de alimentación,” in Fisioterapia en Atención Temprana Una intervención dirigida al niño, la familia y el entorno. 1a. Editors F. Fernández Rego, and F. G. Torró (Madrid: Editorial Médica Panamericana), 97–113.
López-Otín, C., Blasco, M. A., Partridge, L., Serrano, M., and Kroemer, G. (2023). “Hallmarks of aging: an expanding universe,” Cell., 186. 243–278. doi:10.1016/j.cell.2022.11.001
Maier, M., Ballester, B. R., and Verschure, PFMJ (2019). Principles of neurorehabilitation after stroke based on motor learning and brain plasticity mechanisms. Vol. Front. Syst. Neurosci., 13, 74, doi:10.3389/fnsys.2019.00074
Malandraki, G., and Robbins, J. (2013). “Dysphagia,” in Handbook of clinical neurology (Elsevier B.V.), 255–271.
Malhi, H. (2016). Dysphagia: warning signs and management. Br. J. Nurs. 25 (10), 546–549. doi:10.12968/bjon.2016.25.10.546
Mandell, L. A., and Niederman, M. S. (2019). Aspiration pneumonia, editor. N. Engl. J. Med. 380(7):651–663. doi:10.1056/NEJMra1714562
Martin, A., Miró, J., Amadó, C., Ruz, F., Ruiz, A., and Clavé, P. (2023). A systematic and universal artificial intelligence method for oropharyngeal dysphagia screening: accuracy of machine learning is higher than classic multivariate analysis. Clin. Nutr. ESPEN 54, 680–681. doi:10.1016/j.clnesp.2022.09.653
Martin, R. E., Goodyear, B. G., Gati, J. S., and Menon, R. S. (2001). Cerebral cortical representation of automatic and volitional swallowing in humans J. Neurophysiol., 85, 938, 950. doi:10.1152/jn.2001.85.2.938
Martin, W., Jones, D., and Jones, B. (1991). “Aging and neurological disease,” in Normal and abnormal swallowing. Editors B. Jones, and M. Donner, 1st ed. (New York: Springer New York), 189–202.
Massa, L., Fattori, B., Nacci, A., Santoro, A., Palagini, L., Abelli, M., et al. (2022). “Psychopathological aspects of dysphagia: a systematic review on correlations with eating disorders and other psychiatric conditions,” Eat. Weight Disord., 27. 881–892. doi:10.1007/s40519-021-01227-z
Matsuda, Y., Ito, E., Kuroda, M., and Araki, K. (2022). A basic study for predicting dysphagia in panoramic X-ray images using artificial intelligence (AI)—Part 1: determining evaluation factors and cutoff levels. Int. J. Environ. Res. Public Health 19 (8), 4529. doi:10.3390/ijerph19084529
Matsuo, K., and Palmer, J. B. (2008). Anatomy and physiology of feeding and swallowing – normal and abnormal. Phys. Med. Rehabil. Clin. N. Am. 19(4):691. doi:10.1016/j.pmr.2008.06.001
McCarty, E. B., and Chao, T. N. (2021). Dysphagia, and Disorders, Swallowing. Medical clinics of north America 105, 939–954.
McCoy, Y. M., and Desai, R. V. (2018). Presbyphagia versus dysphagia: identifying age-related changes in swallow function. Perspect. ASHA Special Interest Groups. 15. doi:10.1044/persp3.SIG15.15
McHorney, C. A., Robbins, J. A., Lomax, K., Rosenbek, J. C., Chignell, K., Kramer, A. E., et al. (2002). The SWAL-QOL and SWAL-CARE outcomes tool for oropharyngeal dysphagia in adults: III. Documentation of reliability and validity. Dysphagia 17 (2), 97–114. doi:10.1007/s00455-001-0109-1
Milewska, M., Grabarczyk, K., Dąbrowska-Bender, M., Jamróz, B., Dziewulska, D., Staniszewska, A., et al. (2020). The prevalence and types of oral- and pharyngeal-stage dysphagia in patients with demyelinating diseases based on subjective assessment by the study subjects. Mult. Scler. Relat. Disord., 37. doi:10.1016/j.msard.2019.101484
Miller, S., Peters, K., and Ptok, M. (2022). Review of the effectiveness of neuromuscular electrical stimulation in the treatment of dysphagia – an update. GMS Ger. Med. Sci. 20, Doc08. doi:10.3205/000310
Myszczynska, M. A., Ojamies, P. N., Lacoste, A. M. B., Neil, D., Saffari, A., Mead, R., et al. (2020). “Applications of machine learning to diagnosis and treatment of neurodegenerative diseases,” Nat. Rev. Neurol., 16. 440–456. doi:10.1038/s41582-020-0377-8
Nagano, A., Onaka, M., Maeda, K., Ueshima, J., Shimizu, A., Ishida, Y., et al. (2023). Prevalence and characteristics of the course of dysphagia in hospitalized older adults. Nutrients 15 (20), 4371. doi:10.3390/nu15204371
Nahum, M., Lee, H., and Merzenich, M. M. (2013). “Principles of neuroplasticity-based rehabilitation,” in Progress in brain research (Elsevier B.V.), 141–171.
Namasivayam-MacDonald, A. M., Barbon, C. E. A., and Steele, C. M. (2018). “A review of swallow timing in the elderly,” Physiology Behav., 184. 12–26. doi:10.1016/j.physbeh.2017.10.023
Namasivayam-Macdonald, A. M., and Riquelme, L. F. (2019). Presbyphagia to dysphagia: multiple perspectives and strategies for quality care of older adults. Semin. Speech Lang. 40 (3), 227–242. doi:10.1055/s-0039-1688837
Newman, R., Vilardell, N., Clavé, P., and Speyer, R. (2016). “Effect of bolus viscosity on the safety and efficacy of swallowing and the kinematics of the swallow response in patients with oropharyngeal dysphagia: white paper by the European society for swallowing disorders (ESSD),” Eff. Bolus Viscosity Saf. Efficacy Swallowing Kinemat. Swallow Response Patients Oropharyngeal Dysphagia White Pap. by Eur. Soc. Swallowing Disord. (ESSD), 31. 232–249. doi:10.1007/s00455-016-9696-8
Palacio Ortega, M., Bermejo Alegría, R., Herrán Landeros, C., and López Ortega, M. (2024). “Evaluación oromotora y de la alimentación,” in Fisioterapia en Atención Temprana Una intervención dirigida al niño, la familia y el entorno. 1a. Editors F. Fernández Rego, and G. Torró Ferrero (Madrid: Editorial Médica Panamericana), 213–220.
Park, J. S., and Hwang, N. K. (2021). “Chin tuck against resistance exercise for dysphagia rehabilitation: a systematic review,” J. Oral RehabilitationJournal Oral Rehabilitation, 48, 968–977. doi:10.1111/joor.13181
Patel, D. A., Krishnaswami, S., Steger, E., Conover, E., Vaezi, M. F., Ciucci, M. R., et al. (2018). Economic and survival burden of dysphagia among inpatients in the United States. Dis. Esophagus 31 (1), 1–7. doi:10.1093/dote/dox131
Pauloski, B. R., and Yahnke, K. M. (2022). Using ultrasound to document the effects of expiratory muscle strength training (EMST) on the geniohyoid muscle. Dysphagia 37 (4), 788–799. doi:10.1007/s00455-021-10328-x
Penfield, W., and Boldrey, E. (1937). Somatic motor and sensory representation in the cerebral cortex of man as estudied by electrical stimulation. Brain 60(4):389–443. doi:10.1093/brain/60.4.389
Pitts, T., and Iceman, K. E. (2023). Deglutition and the regulation of the swallow motor pattern. Physiology 38 (1), 0. doi:10.1152/physiol.00005.2021
Prosiegel, M. (2019). “Neurology of swallowing and dysphagia,” in Dysphagia: diagnosis and treatment. Editor O. Ekberg (Cham: Springer), 83–106.
Ramón y Cajal, S. (1909). Histologie du systeme nerveux de l’homme et des vertébrés, 1 y 2. Paris: A: Maloine.
RCSLT. Videofluoroscopic evaluation of oropharyngeal swallowing function (VFS): (2013). The role of speech and language therapists RCSLT Position Paper 2013. London; Available at: www.rcslt.org
Rech, R. S., Baumgarten, A., Colvara, B. C., Brochier, C. W., de Goulart, B. N. G., Hugo, F. N., et al. (2018). Association between oropharyngeal dysphagia, oral functionality, and oral sensorimotor alteration. Oral Dis. 24 (4), 664–672. doi:10.1111/odi.12809
Reid, L. B., Boyd, R. N., Cunnington, R., and Rose, S. E. (2016). Interpreting intervention induced neuroplasticity with fMRI: the case for multimodal imaging strategies. Vol. Neural Plast., 2016, 2643491, doi:10.1155/2016/2643491
Rodríguez, R. (2020). “Concepto y epidemiología de la disfagia. Fisiología de la deglución normal,” in Guía de disfagia Manejo de la disfagia en AP. Editor R. Belinchón, 1st ed. (Madrid: BrysemFARMA S.L.), 8–11.
Rogers, B., and Arvedson, J. (2005). Assessment of infant oral sensorimotor and swallowing function. Ment. Retard. Dev. Disabil. Res. Rev. 11, 74–82. doi:10.1002/mrdd.20055
Rommel, N., and Hamdy, S. (2016). “Oropharyngeal dysphagia: manifestations and diagnosis,” Nat. Rev. Gastroenterology Hepatology, 13. 49–59. doi:10.1038/nrgastro.2015.199
Rosenbek, J. C. (2014). “Plasticity in the neural pathways for swallowing: role in rehabilitation of dysphagia,” in Textbook of neural repair and rehabilitation (Cambridge University Press), 405–414.
Roy, N., Stemple, J., Merrill, R. M., and Thomas, L. (2007). Dysphagia in the elderly: preliminary evidence of prevalence, risk factors, and socioemotional effects, Dysphagia Elder. Prelim. Evid. Preval. Risk Factors, Socioemotional Eff 116, 858, 865. doi:10.1177/000348940711601112
Sánchez-Sánchez, E., Avellaneda-López, Y., García-Marín, E., Ramírez-Vargas, G., Díaz-Jimenez, J., and Ordonez, F. J. (2021). Knowledge and practice of health professionals in the management of dysphagia. Int. J. Environ. Res. Public Health 18 (4), 2139–2210. doi:10.3390/ijerph18042139
Saway, B. F., Palmer, C., Hughes, C., Triano, M., Suresh, R. E., Gilmore, J., et al. (2024). The evolution of neuromodulation for chronic stroke: from neuroplasticity mechanisms to brain-computer interfaces, Evol. neuromodulation chronic stroke Neuroplast. Mech. brain-computer interfaces 21, e00337, doi:10.1016/j.neurot.2024.e00337
Schneeweiss, S., and Avorn, J. (2005). A review of uses of health care utilization databases for epidemiologic research on therapeutics. J. Clin. Epidemiol. 58 (4), 323–337. doi:10.1016/j.jclinepi.2004.10.012
Scottish Intercollegiate Guidelines Network (2010). Management of patients with stroke: rehabilitation, prevention and management of complications, and discharge planning A national clinical guideline. Edimburg; 2010 Jun. Available at: www.sign.ac.uk.
Sejdic, E., Khalifa, Y., Mahoney, A. S., and Coyle, J. L. (2020). Artificial intelligence and dysphagia: novel solutions to old problems. Arq. Gastroenterol. 57 (4), 343–346. doi:10.1590/S0004-2803.202000000-66
Sheng, R., Chen, C., Chen, H., and Yu, P. (2023). “Repetitive transcranial magnetic stimulation for stroke rehabilitation: insights into the molecular and cellular mechanisms of neuroinflammation,” Front. Immunol., 14. doi:10.3389/fimmu.2023.1197422
Silva-Batista, C., Harker, G., Vitorio, R., Studer, M., Whetten, B., Lapidus, J., et al. (2023). Mobility Rehab visual feedback system for gait rehabilitation in older adults. J. Neuroeng Rehabil. 20 (1), 144. doi:10.1186/s12984-023-01260-2
Simons, A., and Hamdy, S. (2017). “The use of brain stimulation in dysphagia management,” Dysphagia, 32. 209–215. doi:10.1007/s00455-017-9789-z
Skloot, G. S. (2017). “The effects of aging on lung structure and function,” Clin. Geriatric Med., 33, 447–457. doi:10.1016/j.cger.2017.06.001
Smith, R., Bryant, L., and Hemsley, B. (2023). The true cost of dysphagia on quality of life: the views of adults with swallowing disability. Int. J. Lang. Commun. Disord. 58 (2), 451–466. doi:10.1111/1460-6984.12804
Speyer, R., Cordier, R., Farneti, D., Nascimento, W., Pilz, W., Verin, E., et al. (2022). White paper by the European society for swallowing disorders: screening and non-instrumental assessment for dysphagia in adults. Dysphagia 37 (2), 333–349. doi:10.1007/s00455-021-10283-7
Suzuki, K., Shimizu, Y., Ohshimo, S., Oue, K., Saeki, N., Sadamori, T., et al. (2022). Real-time assessment of swallowing sound using an electronic stethoscope and an artificial intelligence system. Clin. Exp. Dent. Res. 8 (1), 225–230. doi:10.1002/cre2.531
Toan, N. K., and Ahn, S. G. (2021). “Aging-related metabolic dysfunction in the salivary gland: a review of the literature,” Int. J. Mol. Sci., 22. doi:10.3390/ijms22115835
Toogood, J. A., Smith, R. C., Stevens, T. K., Gati, J. S., Menon, R. S., Theurer, J., et al. (2017). Swallowing preparation and execution: insights from a delayed-response functional magnetic resonance imaging (fMRI) study. Dysphagia 32 (4), 526–541. doi:10.1007/s00455-017-9794-2
Trapl, M., Enderle, P., Nowotny, M., Teuschl, Y., Matz, K., Dachenhausen, A., et al. (2007). Dysphagia bedside screening for acute-stroke patients: the gugging swallowing screen. Stroke 38 (11), 2948–2952. doi:10.1161/STROKEAHA.107.483933
Triggs, J., and Pandolfino, J. (2019). Recent advances in dysphagia management. Recent Adv. dysphagia Manag. 8. doi:10.12688/f1000research.18900.1
Tulunay-Ugur, O. E., and Eibling, D. (2018). Geriatric dysphagia. Vol. 34, clinics in geriatric medicine. W.B. Saunders, 183–189.
Vasant, D. H., and Hamdy, S. (2013). “Cerebral cortical control of deglutition,” in Principles of deglutition: a multidisciplinary text for swallowing and its disorders (New York: Springer), 55–65.
Vogt, B. A. (2005). Pain and emotion interactions in subregions of the cingulate gyrus. Nat. Rev. Neurosci. 6, 533–544. doi:10.1038/nrn1704
Wei, K. C., Wang, T. G., and Hsiao, M. Y. (2024). The cortical and subcortical neural control of swallowing: a narrative review. Dysphagia 39 (2), 177–197. doi:10.1007/s00455-023-10613-x
Wilkinson, J. M., Codipilly, D. C., and Wilfahrt, R. P. (2021). Dysphagia: evaluation and collaborative management. Am. Fam. Physician;103(2):97–106.
Williams, P. D., and Day, T. (2003). Antagonistic pleiotropy, mortality source interactions, and the evolutionary theory of senescence. Evol. Soc. Study Evol. 57, 1478–1488. doi:10.1111/j.0014-3820.2003.tb00356.x
Wu, G., Yang, P., Xie, Y., Woodruff, H. C., Rao, X., Guiot, J., et al. (2020). Development of a clinical decision support system for severity risk prediction and triage of COVID-19 patients at hospital admission: an international multicentre study. Eur. Respir. J. 56 (2), 2001104. doi:10.1183/13993003.01104-2020
Yang, H., Luo, Y., Hu, Q., Tian, X., and Wen, H. (2021). Benefits in alzheimer's disease of sensory and multisensory stimulation, Benefits Alzheimer’s Dis. Sens. Multisensory Stimul. 82, 463–484. doi:10.3233/JAD-201554
Yazaki, E., Woodland, P., and Sifrim, D. (2024). Uses of esophageal function testing: dysphagia, Uses Esophageal Funct. Test. Dysphagia. 643–654. doi:10.1016/j.giec.2014.06.008
Zhang, P., Yuan, Y., Lu, D., Li, T., Zhang, H., Wang, H., et al. (2023a). “Diagnostic accuracy of the eating assessment tool-10 (EAT-10) in screening dysphagia: a systematic review and meta-analysis,” Dysphagia, 38. 145–158. doi:10.1007/s00455-022-10486-6
Zhang, X., Wang, X., Liang, Y., Shan, Y., Song, R., Li, X., et al. (2023b). Neuroplasticity elicited by modified pharyngeal electrical stimulation: a pilot study. Brain Sci. 13 (1), 119. doi:10.3390/brainsci13010119
Keywords: presbyphagia, ageing, swallowing, prevention, new technologies, dysphagia
Citation: Palacio M-I, Bermejo R-M, Lucas-Ochoa A-M, González-Cuello A-M, Fernández-Villalba E and Herrero M-T (2025) Age-defying swallowing. Front. Aging 6:1510257. doi: 10.3389/fragi.2025.1510257
Received: 12 October 2024; Accepted: 07 February 2025;
Published: 07 April 2025.
Edited by:
Eugenia Bezirtzoglou, Democritus University of Thrace, GreeceCopyright © 2025 Palacio, Bermejo, Lucas-Ochoa, González-Cuello, Fernández-Villalba and Herrero. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: María-Trinidad Herrero, bXRoZXJyZXJAdW0uZXM=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.