
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Aging Neurosci., 27 March 2025
Sec. Parkinson’s Disease and Aging-related Movement Disorders
Volume 17 - 2025 | https://doi.org/10.3389/fnagi.2025.1505326
This article is part of the Research TopicPathophysiology, Treatment and Rehabilitation of Neurodegenerative Diseases in Geriatric PopulationView all 20 articles
 Zhihai Wang1
Zhihai Wang1 Baofu Song2Cong Liu3Huihui Ma1Zirong Bai4,5Marcelo A. S. Carneiro6
Baofu Song2Cong Liu3Huihui Ma1Zirong Bai4,5Marcelo A. S. Carneiro6 Layale Youssef7
Layale Youssef7 Chao Chen8
Chao Chen8 Lingli Zhang1
Lingli Zhang1 Dan Wang1Dexin Wang1*
Dan Wang1Dexin Wang1*Objective: Parkinson’s disease (PD) is a chronic neurodegenerative disorder characterized by progressive changes in both motor and non-motor symptoms. Boxing exercise can improve PD symptoms. This review aimed to determine the effects of boxing exercise on lower extremity strength, balance, mobility, gait, depression, quality of life, disease severity, exercise safety, and adherence in patients with PD.
Design: A systematic review.
Setting and participants: Articles were selected if they included participants diagnosed with PD and used boxing exercise as the main intervention.
Methods: Systematic review study based on PRISMA criteria. Searches were implemented in PubMed, EMBASE, Web of Science, and Cochrane Library until February 2024. We selected studies reporting on the pre-post assessment of a boxing intervention with lower extremity strength, balance, mobility, gait, depression, quality of life, disease severity, exercise safety, and adherence in patients with PD. Two independent reviewers conducted study selection, data extraction, and quality assessment. The Physiotherapy Evidence Database and ROBINS-I 2.0 criteria evaluated the literature’s quality.
Results: Out of 4,301 records, 13 studies were included, involving 402 PD patients aged 53–89, with 72.4% being male. Interventions lasted 6–96 weeks, primarily in community settings and gymnasiums. Moderate-quality evidence suggested boxing exercises is feasible and effective for enhancing lower extremity strength, balance, mobility, gait, depression, quality of life, disease severity, exercise safety and adherence in PD patients.
Conclusions and implications: Boxing exercise can effectively improve both motor and non-motor symptoms in PD patients, with safety and high adherence. This review systematically summarizes the emerging evidence on the application of boxing exercise in the rehabilitation of patients with PD. Future research should include more homogenous PD patient populations and conducting randomized controlled trials.
Parkinson’s disease (PD) is a prevalent neurodegenerative disorder, recognized as the second most common worldwide (Chou et al., 2017). It is estimated that 10 million individuals worldwide are affected by PD, with a prevalence rate of 1 to 2 per 1,000 individuals which increases with age (Ou et al., 2021). Thus, the number of people with PD is expected to exceed 12 million by 2040 (Dorsey and Bloem, 2018). PD is characterized primarily by a triad symptom: rigidity, tremor, and bradykinesia (Bloem et al., 2021). It includes motor symptoms such as hypokinesia, rigidity, tremor, and postural instability, alongside non-motor symptoms including depression, anxiety, fatigue, and sleep disturbances, which are frequently overlooked (Kalia and Lang, 2015). These multiple symptoms can lead to functional limitations, such as reduced mobility, impairment in gait speed, increasing the risk of falls, fractures and brain injuries. This significantly impacts the quality of life, increases premature mortality, and hence imposes a substantial burden on families and society (Song et al., 2017). Given these implications, it is crucial to identify and implement effective intervention strategies to alleviate symptoms and slow the progression of PD in affected patients.
PD is currently considered incurable, with pharmacotherapy serving as the primary treatment approach (Fox et al., 2018). However, the high cost of medications and their decreasing efficacy over time, and adverse side effects such as orthostatic hypotension, somnolence, and hallucinations significantly impair health and muscle function (Fahn, 2018). Furthermore, pharmacologic interventions are also insufficient to addressing non-motor impairments of PD (Pedersen et al., 2012). Recent evidence has strongly suggested that exercise can effectively complement pharmacotherapy, particularly high-intensity exercise, which may slow PD progression by promoting neuroplasticity (Frazzitta et al., 2014; Tollár et al., 2018). In this regard, boxing exercise (a type of high-intensity exercise) has become increasingly popular among patients with PD (Blacker et al., 2023; Combs et al., 2013; Patel et al., 2023; Sangarapillai et al., 2021). It is estimated that over 4,500 patients with PD globally are currently participating in boxing programs (Morris et al., 2019). Current studies have shown that boxing exercise can effectively improve gait function (Combs et al., 2013; Sangarapillai et al., 2021; Shearin et al., 2021), mobility (Combs et al., 2013; Combs et al., 2011; Domingos et al., 2022), and balance (Combs et al., 2013; Domingos et al., 2022; Sonne et al., 2021) in individuals with PD. Additionally, boxing has been found to reduce depressive symptoms (Patel et al., 2023), alleviate disease severity (Patel et al., 2023; Sangarapillai et al., 2021), and enhance quality of life (Combs et al., 2013; Combs et al., 2011; Sangarapillai et al., 2021). Notably, patients have demonstrated high adherence to boxing interventions without experiencing falls or other adverse events (Blacker et al., 2023; Sangarapillai et al., 2021). Boxing exercise is a sport that integrates speed, strength, and endurance (Dawson et al., 2020; Sonne et al., 2021). For instance, boxing exercise requires rapid lower limb movements in various directions and planes (Shearin et al., 2021). It also involves upper limb punching which requires quick arm movements, trunk rotation, and postural adjustments (Combs et al., 2011). Compared to other forms of exercise, such as aerobic and resistance training, boxing offers a comprehensive range of activities, including aerobic, strength, stretching, balance, and agility exercises, involving a wide spectrum of movement benefits (Patel et al., 2023). Nonetheless, ensuring adherence to an exercise program and the safety profile of the program itself remain crucial concerns for participants (Morris et al., 2019; Rhodes et al., 1999). To the authors’ knowledge, only one systematic review (Morris et al., 2019) has reviewed the evidence on the benefits and risks of boxing exercises for PD patients. This systematic review (Morris et al., 2019) included just one small randomized controlled trial (Combs et al., 2013) and one case series evaluation (Combs et al., 2011). The results indicate that the benefits, precautions, contraindications, and limitations of boxing exercises for PD patients remain verified.
Considering the increasing burden of PD with patients and the potential of boxing exercise as an intervention, there is an urgent need to systematically explore the effects of this exercise. To our knowledge, there is a lack of latest systematic reviews to addressed this gap. Building on the above considerations, the primary aim of the present study was to evaluate the efficacy of boxing exercises on various aspects including motor symptoms (lower extremity strength, balance, mobility, and gait), non-motor symptoms (depression, quality of life, and disease severity), exercise safety and adherence individuals with PD. In addition, this systematic review aims to identify research gaps and propose suggestions for future studies, thereby providing robust evidence-based recommendations for clinical practice.
This systematic review was performed in compliance with the PRISMA guidelines (Page et al., 2021) and has been registered in the PROSPERO database (CRD42024518202).
We retrieved literature published in the English language from the inception of the databases up to February 2024, by accessing PubMed, Web of Science, EMBASE, and Cochrane Library. Our search strategy incorporated a combination of MeSH terms and free-text terms, with the specific strategies for each database detailed in Table 1. Furthermore, we evaluated existing systematic reviews and the reference lists of the included studies to supplement our search for the relevant literature. In addition, after the exclusion of duplicate publications, the gray literature was excluded, including conference abstracts and/or papers, thesis and/or dissertations, meta-analyses, systematic reviews, commentaries, and editorials. In case of disagreements, a third reviewer (HM) evaluated the article.
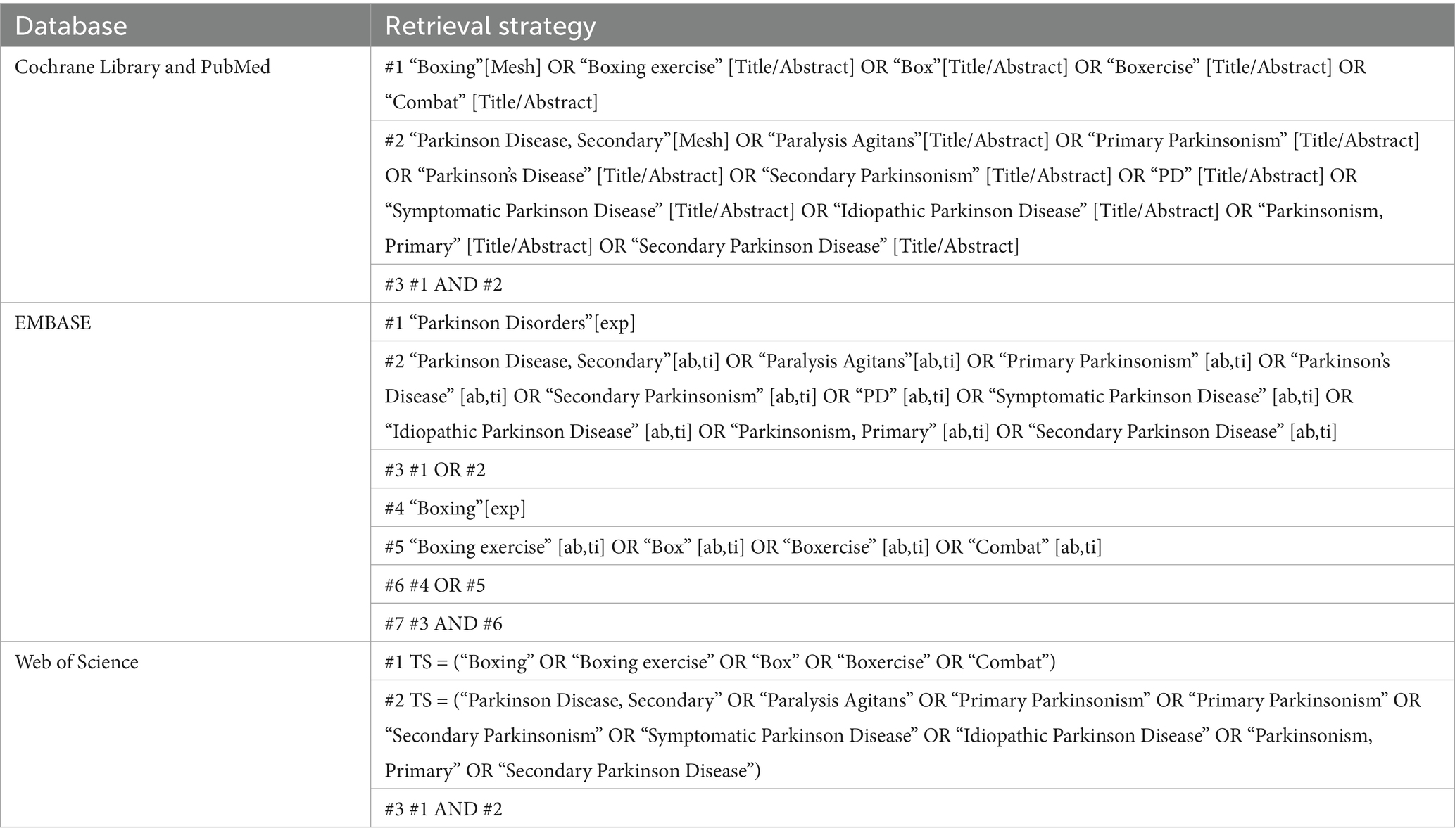
Table 1. The database search strategy.
Two independent researchers (ZW and CL) conducted a systematic search and selection of literature, consulting a third researcher (HM) to reach a consensus in cases of disagreement.
The eligibility criteria were as follows: (1) adults diagnosed with PD; (2) interventions featuring boxing exercises, either solo or combined with other forms of exercise or physiotherapy; (3) outcomes included strength, balance, mobility, gait, depression, quality of life, disease severity, safety and adherence; (4) study designs including randomized controlled trials (RCTs), controlled clinical trials, cohort studies, case series, case–control studies, and quasi-experimental studies; (5) original articles peer-reviewed without limitations on publication date, published until February 2024; (6) published in English language.
The exclusion criteria were as follows: (1) studies involving participants with stroke, traumatic brain injury, and/or non-motor neurological diseases; (2) interventions other than boxing; (3) unavailable full texts; (4) review articles (including meta-analyses and systematic reviews), conference abstracts, dissertations, and commentaries; (5) duplicate publications.
Upon identifying eligible studies from each database, the retrieved literature was first imported into EndNote X9 (Milne-Ives et al., 2020) to consolidate and eliminate duplicates. Two researchers (ZW and CL) independently screened the titles and abstracts to identify potentially relevant articles. A full-text review was then performed for further selection of the initially selected literature. When data were incomplete or unextractable, the authors were contacted to provide the missing information. The extracted content included essential details such as authors, publication year, country, and study design; participant baseline information including sample size, gender, mean age of participants, and mean Hoehn and Yahr score; intervention details like type, specifics, regimen, duration, or dosage; and the main findings.
The methodological quality of the included literature was independently assessed by two researchers (ZW and CL), with any disagreements resolved through discussion with a third researcher (HM) to reach a consensus. The Physiotherapy Evidence Database (PEDro) was used to evaluate the quality of RCTs, which consisted of 11 evaluation criteria. Each criterion met was given one point, with a maximum score of 10. The first evaluation criteria did not contribute to the final score. According to the scale, scores are categorized as follows: <4 indicates poor quality, 4–5 fair quality, 6–8 good quality, and 9–10 high quality (Fernández-Landa et al., 2023). For non-randomized controlled trials (non-RCTs), the ROBINS-I 2.0 criteria were used, which consisted of seven items that primarily assessed the risk of bias as low, moderate, serious, critical, or lacking information (Sterne et al., 2016).
A systematic search yielded 4,301 records as documented in the PRISMA flow diagram (Figure 1). After removing duplicates and screening the gray literature, including conference abstracts and/or papers, thesis and/or dissertations, meta-analyses, systematic reviews, commentaries, and editorials, 44 articles were preliminarily selected according to eligibility criteria. Following a thorough full-text evaluation, 31 articles were excluded for not meeting the inclusion criteria due to irrelevant outcomes (n = 3), not a boxing intervention (n = 12), review or systematic review article (n = 3), and conference abstract (n = 13). Therefore, the final analysis included 13 studies (Blacker et al., 2023; Combs et al., 2013; Combs et al., 2011; Dawson et al., 2020; Domingos et al., 2022; Hermanns et al., 2021; Horbinski et al., 2021; Moore et al., 2021; Patel et al., 2023; Sangarapillai et al., 2021; Shearin et al., 2021; Sonne et al., 2021; Urrutia et al., 2020).
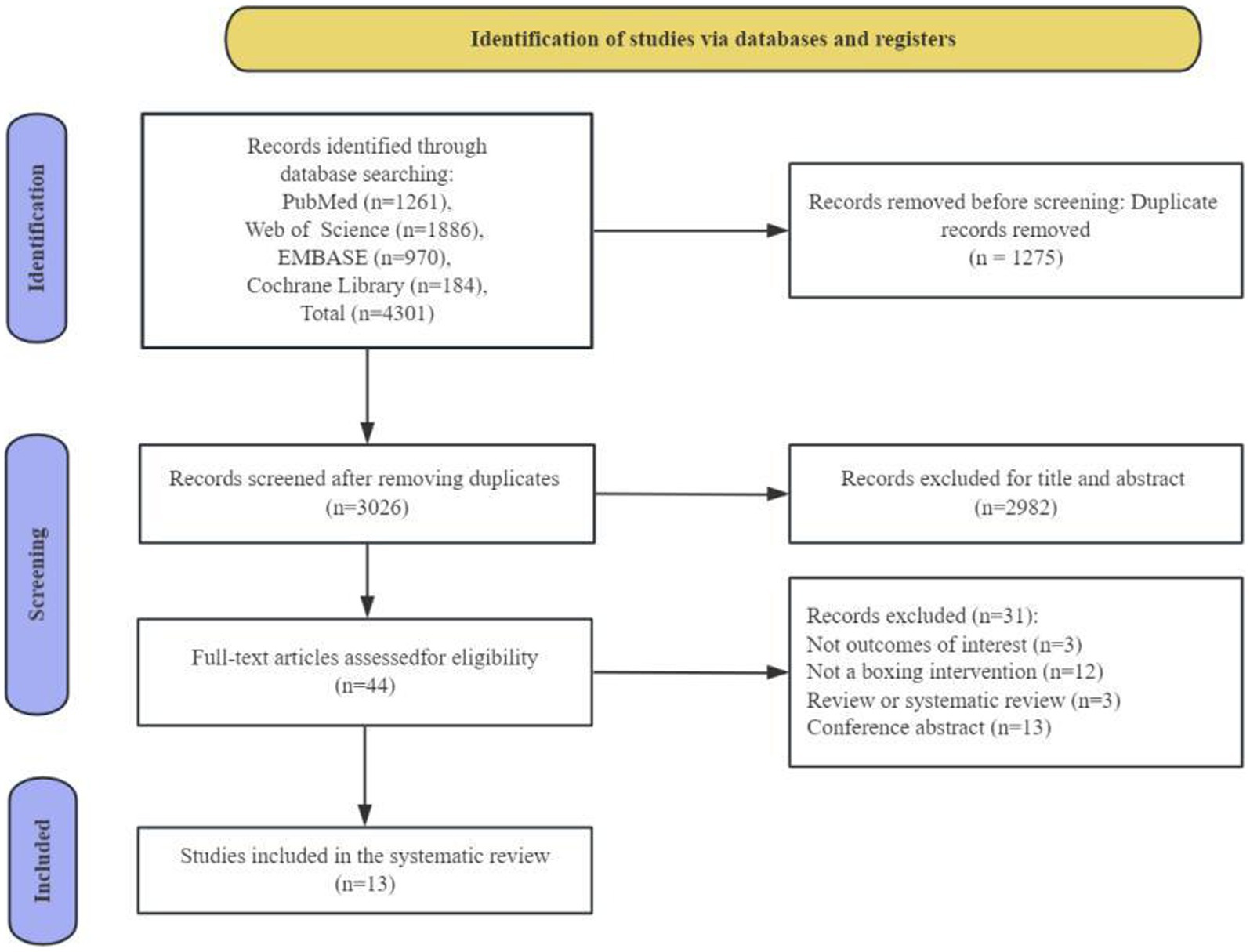
Figure 1. Flow diagram of the systematic review for inclusion/exclusion of studies.
The quality assessment results are detailed in Tables 2, 3. Using the PEDro scale, three RCTs were evaluated, indicating a low risk of bias with an average score of 8.33. This suggests that the results of the systematic review are trustworthy. Notably, one study achieved the maximum score of 10. The absence of blinding for therapists and participants in two studies may be due to inherent experimental design constraints, presenting significant challenges to blinding and potentially impacting the methodological integrity of the included studies. The ROBINS-I 2.0 tool was used to assess the quality of ten non-RCTs studies, indicating an overall low risk of bias. Nevertheless, given that all included studies involved exercise interventions with human participants, there was an increased risk of bias due to deviations from the intended interventions.
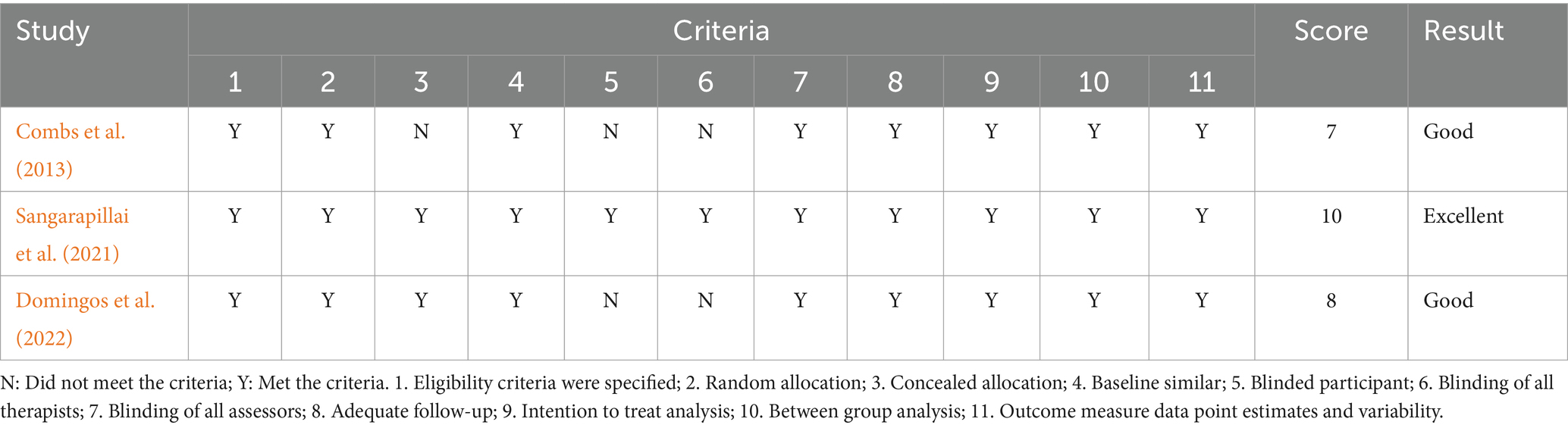
Table 2. Randomized controlled trial (PEDro scale).
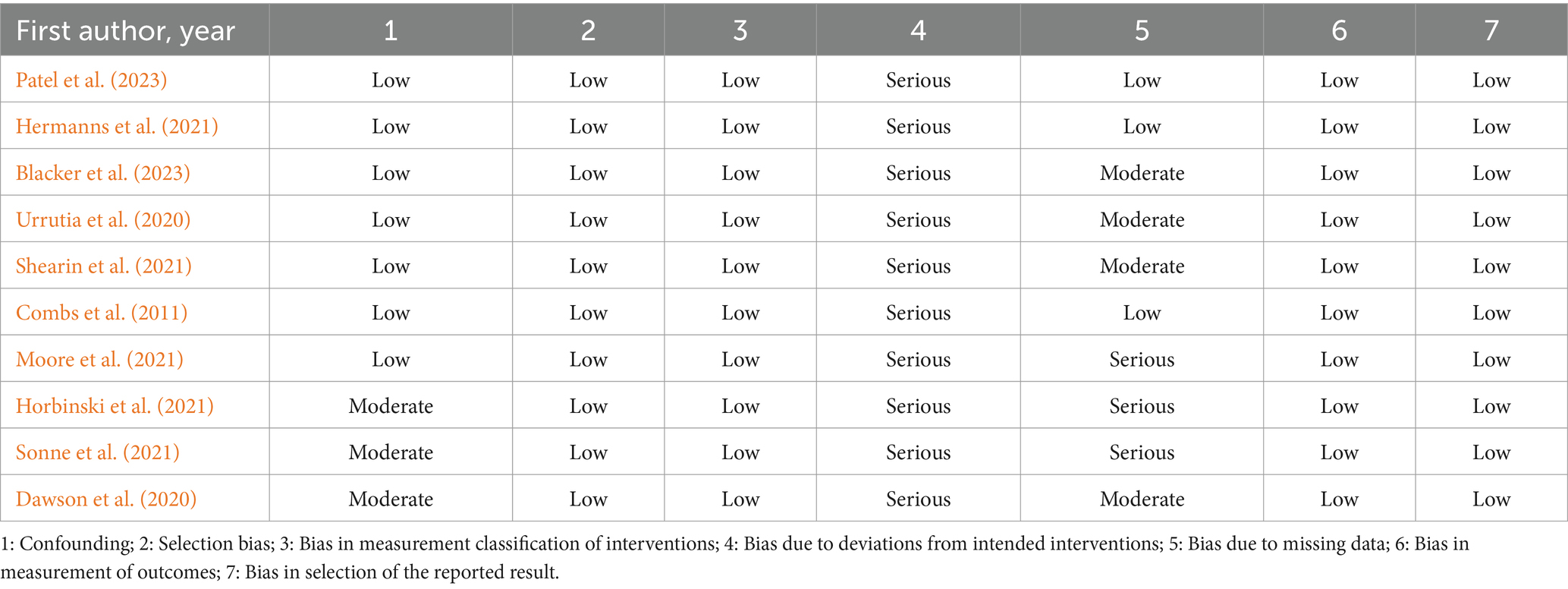
Table 3. Non-randomized controlled trial (ROBINS-I 2.0).
The analysis covered 13 publications (Blacker et al., 2023; Combs et al., 2013; Combs et al., 2011; Dawson et al., 2020; Domingos et al., 2022; Hermanns et al., 2021; Horbinski et al., 2021; Moore et al., 2021; Patel et al., 2023; Sangarapillai et al., 2021; Shearin et al., 2021; Sonne et al., 2021; Urrutia et al., 2020) from four countries: the United States, Australia, Canada, and the Netherlands. Notably, 10 of these studies (76.9%) were conducted in the United States (Combs et al., 2013; Combs et al., 2011; Dawson et al., 2020; Hermanns et al., 2021; Horbinski et al., 2021; Moore et al., 2021; Patel et al., 2023; Shearin et al., 2021; Sonne et al., 2021; Urrutia et al., 2020), with the majority published between 2020 and 2023 (84.6%) (Blacker et al., 2023; Dawson et al., 2020; Domingos et al., 2022; Hermanns et al., 2021; Horbinski et al., 2021; Moore et al., 2021; Patel et al., 2023; Sangarapillai et al., 2021; Shearin et al., 2021; Sonne et al., 2021; Urrutia et al., 2020). The study designs included three RCTs (Combs et al., 2013; Dawson et al., 2020; Domingos et al., 2022) and ten non-RCTs (Blacker et al., 2023; Combs et al., 2011; Dawson et al., 2020; Hermanns et al., 2021; Horbinski et al., 2021; Moore et al., 2021; Patel et al., 2023; Shearin et al., 2021; Sonne et al., 2021; Urrutia et al., 2020). All participants were adult patients with a confirmed diagnosis of PD, totaling 402 patients. Patient ages ranged from 40 to 90 years, with a male gender bias (72.4% male). The average disease duration and Hoehn and Yahr scores varied from 2.4 to 7.9 years and stages 1–4, respectively. Three studies omitted details on disease severity (Dawson et al., 2020; Domingos et al., 2022; Horbinski et al., 2021), one failed to specify the gender distribution of its participants (Sangarapillai et al., 2021), and one study exclusively examined male participants (Combs et al., 2011). Detailed information for each included study is provided in Table 4.
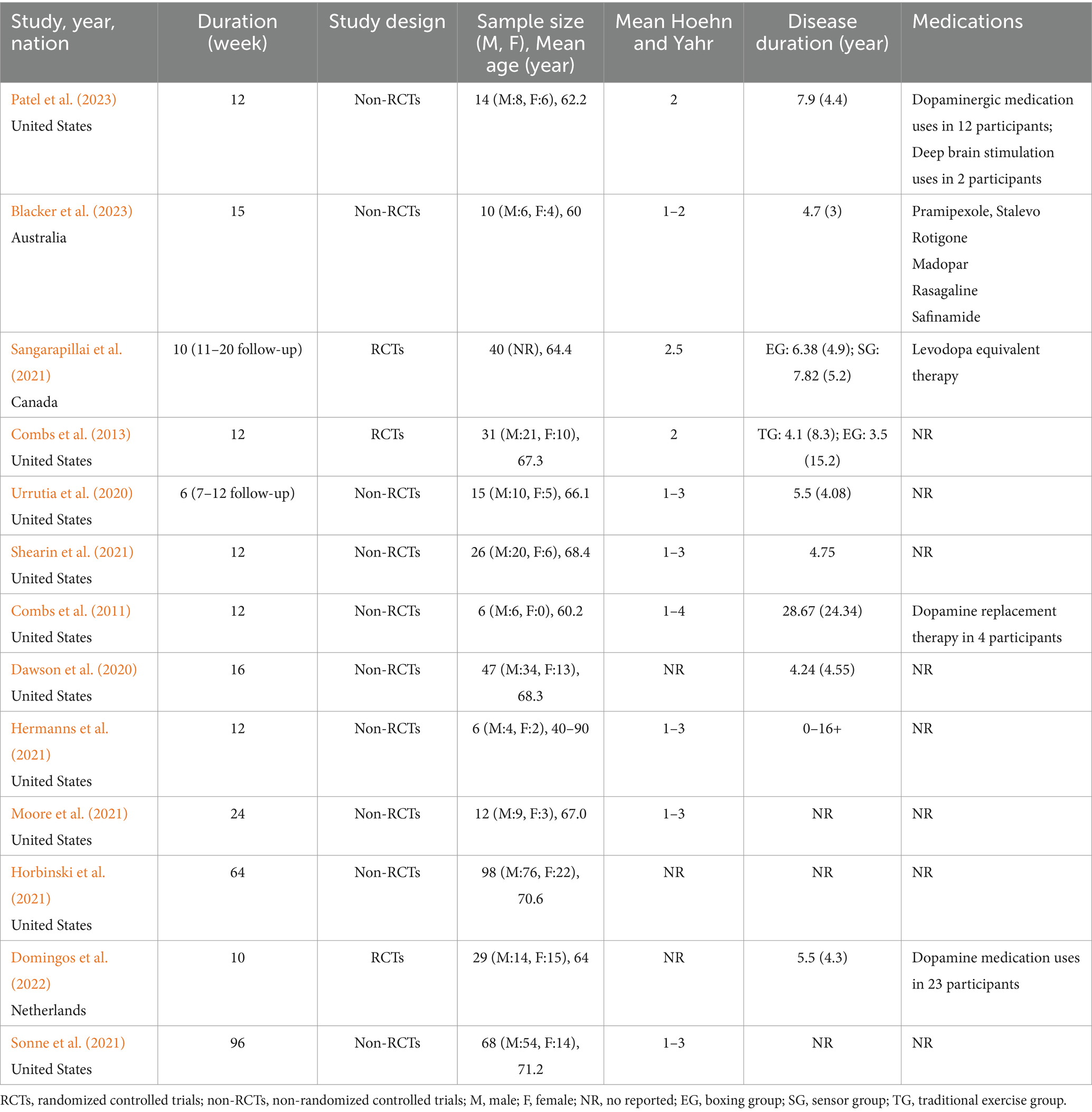
Table 4. Characteristic of studies included (n = 13).
The boxing exercise program primarily employed a circuit training approach, incorporating boxing drills, resistance training, agility exercises, and endurance training (Blacker et al., 2023; Combs et al., 2011; Dawson et al., 2020; Song et al., 2017). Participants engaged in these activities using gloves and punching bags, without any physical contact with others. The interventions were mainly conducted in community (Combs et al., 2013; Combs et al., 2011; Domingos et al., 2022; Moore et al., 2021; Patel et al., 2023; Shearin et al., 2021; Urrutia et al., 2020) and gymnasiums (Dawson et al., 2020; Hermanns et al., 2021), although four studies did not specify the locations (Blacker et al., 2023; Horbinski et al., 2021; Sangarapillai et al., 2021; Sonne et al., 2021). The duration of the interventions varied from 6 to 96 weeks, with sessions occurring 1–3 times per week and lasting an average of 60–90 min. Sample sizes ranged from a minimum of 6 participants (Combs et al., 2011; Hermanns et al., 2021) to a maximum of 68 participants (Sonne et al., 2021). In terms of intensity, three studies implemented high-intensity programs (Moore et al., 2021; Sangarapillai et al., 2021; Urrutia et al., 2020), two studies instructed participants to complete the entire program at maximal intensity (Combs et al., 2013; Combs et al., 2011), one study used moderate intensity (Shearin et al., 2021), another progressed from low to high intensity (Blacker et al., 2023), and one relied on coach-directed intensity without standardization (Patel et al., 2023). Five studies did not report the exercise intensity (Dawson et al., 2020; Domingos et al., 2022; Hermanns et al., 2021; Horbinski et al., 2021; Sonne et al., 2021). The primary outcome measures included lower extremity strength (15 s and 30 s sit-to-stand; 30 s Chair Stand, 30 s CST), balance (Fullerton Advanced Balance scale, FAB; Berg Balance Scale, BBS; Mini-Balance Evaluation Systems Test, Mini-BESTest; ABC, Activity Specific Balance Confidence Scale; 30 s single leg stance), mobility (Timed up and go, TUG; dual-task TUG, dTUG), gait (10 Meter Walk Test, 10MWT; 6 min walk test, 6MWT; 6 min walk distance, 6MWD), depression (Center for epidemiologic studies depression, CES-D; Hamilton Depression Rating Scale, HDRS), quality of life (Parkinson’s Disease Questionaire-39, PDQ-39; Parkinson’s Disease Quality of Life scale, PDQL; Brief quality-of-life survey the Euroquol-5D, EQ-5D), and disease severity (Unified Parkinson Disease Rating Scale, UPDRS; Movement Disorders Society Unified Parkinson’s Disease Rating Scale part III, MDSUPDRS III). These measures aimed to comprehensively evaluate the effects of boxing exercises on both motor and non-motor functions in patients with PD. Table 5 provides detailed information on the specific outcome measures and main results.
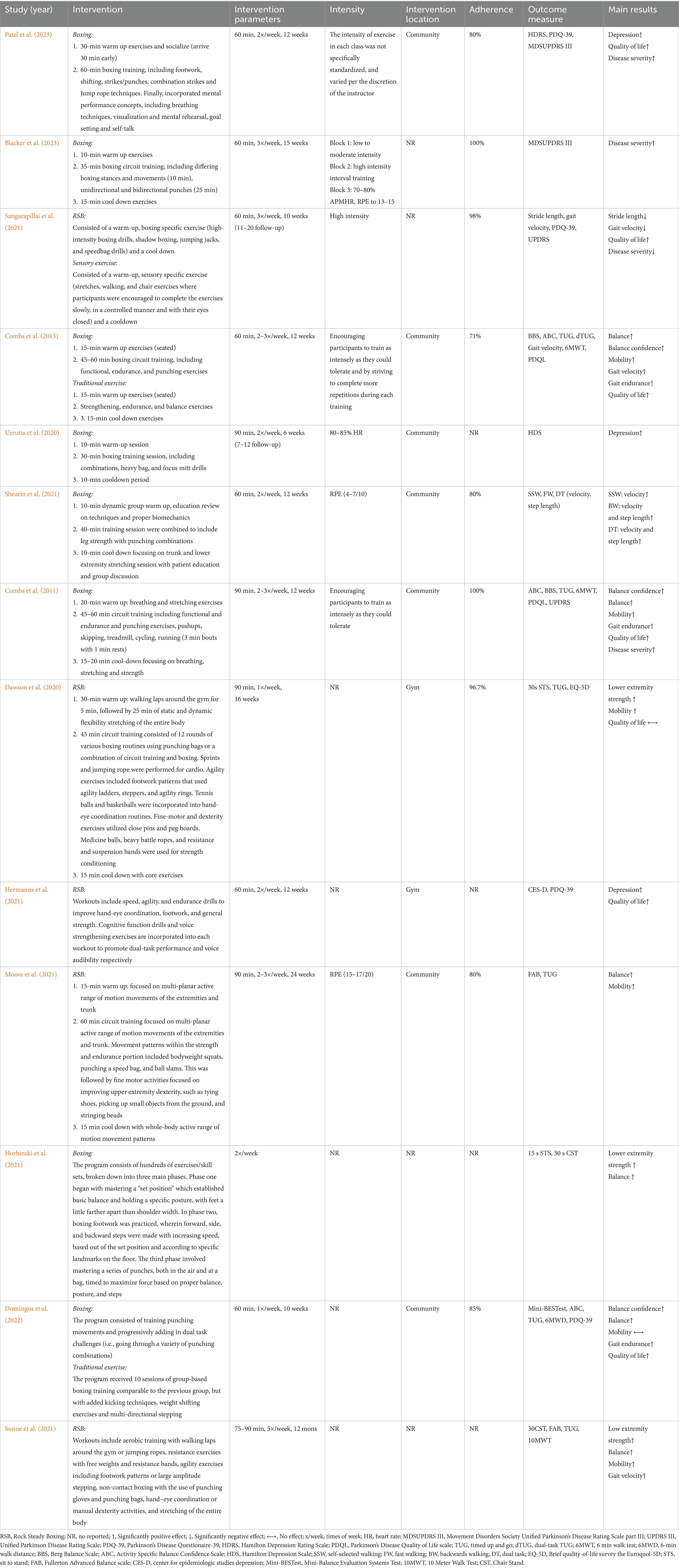
Table 5. Characteristic of interventions and results of studies included (n = 13).
Three studies (Dawson et al., 2020; Horbinski et al., 2021; Sonne et al., 2021) reported the effect of boxing on the lower extremity strength of patients, consistently indicating that boxing can effectively enhance their lower extremity strength. Sonne et al. (2021) observed a significant increase in the number of repetitions during the 30-s CST after 18 months of twice-weekly boxing exercise interventions. However, no significant improvement was observed at the 24-month mark compared to baseline data. Dawson et al. (2020) found that 16 weeks of weekly boxing training sessions, each lasting 90 min, resulted in a significant improvement in the number of repetitions during the 30-s STS test. Moreover, Horbinski et al. (2021) reported that twice-weekly boxing exercise effectively enhanced the performance in the 15-s STS test.
Six studies (Combs et al., 2013; Combs et al., 2011; Domingos et al., 2022; Horbinski et al., 2021; Moore et al., 2021; Sonne et al., 2021) have reported the positive effects of boxing exercise on the balance abilities of patients, consistently noting varying degrees of improvement. Horbinski et al. (2021) found that participants who underwent twice-weekly boxing training significantly improved their performance in the 30-s single-leg stance test. Sonne et al. (2021) observed significant enhancements in the FAB Scale performance of patients at 6, 12, and 18 months after starting boxing interventions (no data were obtained at 24 months). Moore et al. (2021) also reported a significant increase in FAB Scale performance following a 24-week community boxing intervention for patients. Combs et al. (2011) demonstrated significant improvements in patients’ BBS and ABC scores during the 12 to 36-week intervention period, particularly among those with moderate to severe PD. When comparing 12 weeks of boxing exercise to traditional exercise therapy, Combs et al. (2013) found improvements in BBS and ABC performance in both groups, although only the traditional exercise group showed significant pre-to-post intervention differences, potentially due to specific balance training. Additionally, when comparing pure boxing exercise to boxing training combined with kicking techniques, both groups indicated significant improvements in Mini-BESTest and ABC performance after a 10-week intervention, with no significant differences between them (Domingos et al., 2022).
Six studies (Combs et al., 2013; Combs et al., 2011; Dawson et al., 2020; Domingos et al., 2022; Moore et al., 2021; Sonne et al., 2021) reported the effects of boxing exercise on the mobility of patients, consistently reporting significant improvements post-intervention. Combs et al. (2011) and Dawson et al. (2020) found that 12 weeks of thrice-weekly boxing training, as well as weekly boxing training over 16 weeks, significantly enhanced the TUG test performance in patients. Additionally, those who underwent 6 and 12 months of such training showed substantial improvements in TUG performance compared to their baseline assessments. Moore et al. (2021) corroborated these findings, noting that 24 weeks of biweekly to triweekly boxing training effectively improved TUG performance. However, no significant improvement was observed in the 18th and 24th months, as reported by Sonne et al. (2021). The investigation by Combs et al. (2013) further revealed that boxing significantly improved both TUG and dTUG performance compared to traditional exercise therapy over 12 weeks, but did not find a clear advantage in boxing. At the same time, 10 weeks of boxing training alone improved TUG performance in patients more effectively than boxing exercise combined with kicking techniques (Domingos et al., 2022).
Six studies (Combs et al., 2013; Combs et al., 2011; Domingos et al., 2022; Sangarapillai et al., 2021; Shearin et al., 2021; Sonne et al., 2021) reported the effects of boxing on the gait parameters of patients, including gait velocity, gait endurance, stride length, stride width, and other sub-indices. Shearin et al. (2021) found that after 12 weeks of twice-weekly boxing training, patients showed significant improvements in self-selected gait velocity and step cadence, as well as backward walking velocity, gait velocity, step length, and gait variability index during dual-task conditions. Additionally, long-term intervention studies, such as Combs et al. (2011), have observed a significant increase in the walking distance on the 6MWT after 12 weeks of boxing exercise. For patients with mild PD, increased step cadence and stride length, along with decreased step width, were noted during GaitRite Walkway System tests at weeks 12, 24, and 36. Furthermore, the study results indicated that patients with moderate to severe disease required a longer training duration to achieve improvements in gait function compared to those with mild disease. Sonne’s study (Sonne et al., 2021) suggested that although there was no significant improvement in patients’ 10MWT time after 12 months of boxing training, there was an upward trend. Combs et al. (2013) research further demonstrated that 12 weeks of two to three times per week boxing training effectively improved patients’ 6MWT performance and gait velocity in the GaitRite Walkway System test compared to traditional exercise therapy. Research further demonstrated that 12 weeks of two to three times per week boxing training effectively improved patients’ 6MWT performance and gait velocity in the GaitRite Walkway System test compared to traditional exercise therapy (Sangarapillai et al., 2021). Domingos et al. (2022) compared the effects of boxing training alone versus boxing training combined with kicking techniques over 12 weeks. The results revealed no significant difference in the 6MWD between the two groups.
Three studies (Hermanns et al., 2021; Patel et al., 2023; Urrutia et al., 2020) reported the effects of boxing on depressive symptoms in elderly patients, consistently finding that participation in boxing can improve these symptoms. Two studies (Hermanns et al., 2021; Patel et al., 2023) reported that participating in boxing exercises for 12 weeks, with sessions lasting 60 min and held twice per week, effectively improved scores on the HDRS. Additionally, research by Urrutia et al. (2020) showed that even a brief period of 6 weeks of high-intensity boxing training significantly improved HDRS scores. However, this improvement was not maintained at the 12-week follow-up assessment, reverting to baseline levels.
Seven studies (Combs et al., 2013; Combs et al., 2011; Dawson et al., 2020; Domingos et al., 2022; Hermanns et al., 2021; Patel et al., 2023; Sangarapillai et al., 2021) reported the effects of boxing on the quality of life in patients. Six of these studies agreed that participation in such training can significantly improve patients’ quality of life (Combs et al., 2013; Combs et al., 2011; Domingos et al., 2022; Hermanns et al., 2021; Patel et al., 2023; Sangarapillai et al., 2021). Specifically, four studies (Combs et al., 2013; Combs et al., 2011; Hermanns et al., 2021; Patel et al., 2023) showed significant improvements in both PDQL and PDQ-39 scores following a 12-week program of boxing exercises, conducted two to three times per week for 60–90 min per session. Additionally, another two studies (Domingos et al., 2022; Sangarapillai et al., 2021) reported significant reductions in PDQ-39 scores with a shorter, 10-week training cycle involving one to three sessions of 60 min each per week. In contrast, research by Dawson et al. (2020) observed no significant change in EQ-5D scores after a 16-week course of weekly boxing exercise, each lasting 90 min.
Four studies (Blacker et al., 2023; Combs et al., 2011; Patel et al., 2023; Sangarapillai et al., 2021) reported the effect of boxing exercise on the disease severity in patients. Most of these studies suggest that boxing exercises can effectively decelerate the progression of PD. Specifically, Patel et al. (2023) reported a significant reduction in the Movement Disorder Society-Sponsored Revision of the MDS-UPDRS III scores among elderly patients after 12 weeks of boxing training. Similarly, Blacker et al. (2023) observed a significant decrease in patients’ MDS-UPDRS III scores following 15 weeks of boxing training. A case series study noted that 12 weeks of boxing training significantly lowered the UPDRS scores of elderly patients, with this positive trend persisting during follow-up assessments at weeks 24 and 36 (Combs et al., 2011). However, Sangarapillai et al. (2021) found no significant improvement in the UPDRS scores of elderly patients after 10 weeks of boxing training compared to those who underwent sensory training, and symptom severity increased after a subsequent 10-week washout period.
Seven studies (Blacker et al., 2023; Combs et al., 2011; Dawson et al., 2020; Domingos et al., 2022; Moore et al., 2021; Sangarapillai et al., 2021; Shearin et al., 2021) reported the effects of boxing on exercise safety and adherence in patients. Moore et al. (2021) and Shearin et al. (2021) reported an adherence rate of 80% among patients participating in boxing exercises. Dawson et al. (2020) reported a high participant adherence rate (96.7%) and retention rate (100%), with similar persistence (98%) and retention rates (100%) observed in studies by Sangarapillai et al. (2021) and Blacker et al. (2023). These findings collectively suggest that patients not only accept this intervention but also maintain participation over the long term. Combs et al. (2011) indicated high adherence, with all patients completing at least 24 training sessions within 12 weeks, and no adverse events occurred during the intervention, indicating high safety. Domingos’ (Domingos et al., 2022) study showed that 85% of participants completed the training course without any falls or other adverse events.
The aim of this systematic review was to evaluate the effects of boxing exercise on lower extremity strength, balance, mobility, gait, depression, quality of life, disease severity, exercise safety and adherence in patients with PD. The primary findings of this systematic review suggest that long-term boxing exercise can effectively improve patients’ lower extremity strength (15-s and 30-s sit-to-stand, 30-s CST), balance (Functional Reach, Berg Balance Scale, Mini-BESTest, 30-s single-leg stance), mobility (TUG, dTUG), gait parameters (step length, stride width, 10MWT, and 6MWT), depression (CES-D, HDRS), quality of life (PDQ-39, PDQL, and EQ-5D), and disease severity (UPDRS). Additionally, adherence to boxing-based exercise was high among PD patients, and no adverse events were reported after long-term interventions. These findings provide the latest evidence supporting the positive effects of boxing on individuals with PD.
Research has shown that boxing exercises can significantly improve lower extremity strength, balance abilities, and self-confidence in balance control for patients with PD. The observed improvement in abilities may be attributed to the specific activities performed during each exercise session. Boxing, as an all-encompassing training method, incorporates aerobic, strength, and agility exercises, which challenge the participants’ lower extremity strength and balance ability (Combs et al., 2013; Combs et al., 2011; Sangarapillai et al., 2021). Strength is a vital component of physical fitness (Xu et al., 2023), and a strong correlation exists between lower extremity strength and balance ability. However, it is worth noting that only three out of 13 studies have assessed the impact of boxing on lower extremity strength in patients (Dawson et al., 2020; Horbinski et al., 2021; Sonne et al., 2021). Additionally, there is a paucity of literature on the effects of boxing exercises on the upper extremity strength in patients. Unlike traditional exercise programs that focus on static and dynamic balance drills, such as one-legged standing, boxing training enhances balance indirectly through activities integral to boxing techniques. These include dynamic balance maneuvers like reaching overhead while punching speed bags, as well as multidirectional reaching and stepping when following a trainer’s lead during focus mitt drills, both of which require participants to maintain and adjust their balance (Combs et al., 2011). Moreover, dual-task training, a key component of the boxing intervention, plays a significant role in improving balance (Domingos et al., 2022). Patients with PD undergoing physical movements simultaneously with high cognitive demand tasks experience heightened scrutiny of their balance control abilities. Studies indicate that these patients tend to exhibit diminished balance and gait function during dual-task scenarios (Kelly et al., 2012; Raffegeau et al., 2019). However, dual-task training has been found to effectively enhance their balance and gait performance (De Freitas et al., 2020; Strouwen et al., 2017). Consequently, the distinctive training approach of boxing not only improves the physical balance abilities of patients, but also strengthens their sense of self-efficacy when facing balance challenges. Additional research by Combs et al. suggested that patients with milder symptoms may show earlier improvements in balance compared to those with moderate to severe symptoms (Combs et al., 2013). The latter group may require a longer period of training to achieve the maximum benefits (Combs et al., 2011). This discrepancy could be due to the greater tolerance and capacity of mild PD patients to perform more repetitions within the boxing training framework (Combs et al., 2011).
Boxing exercise has been found to effectively enhance the mobility and gait functions of patients with PD, which are crucial for their quality of life (Curtze et al., 2016). As a multi-planar and full-body exercise, boxing requires the coordinated action of both upper and lower limbs within various footwork directions. The uniqueness of this training is its program diversity, such as variations in movement combinations, training complexity, e.g., coordinating upper and lower limbs in dual tasks, and dynamic adaptability, which involves adjustments according to the coach’s instructions (Shearin et al., 2021). As participants gradually master the techniques of boxing, the intensity of the exercise can be increased by enhancing punching speed and footwork power (Shearin et al., 2021). Additionally, as the training progresses, there is a corresponding increase in the complexity of movements, such as longer sequences and combinations of actions. Patients must also cognitively process instructions from the coach while performing movement tasks, such as advancing, retreating, and throwing punches. These elements challenge the patients’ dynamic neuromuscular control and improve their ability to complete various neuromechanical tasks, significantly improving their mobility and gait functions, including gait endurance, step length, stride width, and gait velocity. Studies suggest that enhanced motor control ability is fundamental for improved mobility, which requires the integration of visual, proprioceptive, and vestibular information (Miller Koop et al., 2019). High-intensity boxing may increase the quality and quantity of afferent information sent to cortical and subcortical areas, facilitating the processing and integration of sensory information in participants (Alberts et al., 2011). Imaging data also suggests that high-intensity exercise can lead to increased connectivity between subcortical and cortical structures, which may underlie the improvements in mobility and gait function (Alberts et al., 2016). However, research by Sangarapillai et al. (2021) and Domingos et al. (2022) found that after 10 weeks of boxing, patients did not show significant improvements in stride length, gait velocity, and mobility. This could be due to the shorter intervention period and lower frequency (10 weeks, 1–2 times per week), whereas previous studies had intervention periods of 12 weeks, 2–3 times per week (Combs et al., 2013; Combs et al., 2011; Moore et al., 2021; Sonne et al., 2021). It is noteworthy that some studies did not report medication use during the intervention period, which may obscure or exaggerate the effects of boxing training. To our knowledge, no studies have directly compared the effects of combined boxing training and medication therapy versus medication therapy alone or boxing training alone. However, research by Dibble et al. demonstrated that a 12-week combined intervention of exercise and medication therapy yielded superior improvements in muscle strength, UPDRS motor scores, and mobility in PD patients compared to resistance training or dopamine replacement therapy alone (Dibble et al., 2015). This suggests that the combined effects of exercise and medication therapy may be complementary. Currently, there is a lack of high-quality randomized controlled trials in this field, and future research is needed to validate the role of medication therapy in the outcomes of boxing training interventions.
Research has confirmed that boxing can effectively reduce depressive symptoms in patients with PD. The benefits of boxing are twofold: on one hand, it appears to alleviate depression by promoting the release of β-endorphin and increasing the availability of key neurotransmitters such as serotonin, dopamine, and norepinephrine, as well as by raising the levels of brain-derived neurotrophic factor (Basso and Suzuki, 2017; Fan et al., 2020). These physiological changes play a crucial role in alleviating depressive symptoms. Moreover, compared to repetitive exercises like walking or cycling on a stationary bike, boxing involves participants in complex movements and combinations that actively challenge cognitive functions, significantly enhancing their physical and psychological experiences (Patel et al., 2023). The social aspect of boxing is also significant. The camaraderie developed during training provides invaluable social support, which is vital for improving mood and reducing feelings of isolation (Hermanns et al., 2021). Physical activities, including boxing, have been shown to enhance self-esteem, self-evaluation, and a sense of accomplishment (Biddle and Asare, 2011; Wipfli et al., 2011), and are positively linked to self-efficacy (Wipfli et al., 2011). These factors may represent the underlying psychological mechanisms through which physical activities, including boxing, regulate depressive symptoms in patients. Notably, research indicates that just 6 weeks of high-intensity boxing training can significantly improve depressive symptoms in patients with PD.
The quality of life for patients with PD is primarily influenced by motor and non-motor symptoms, including balance, gait function, depression, and sleep disturbances (Balestrino and Martinez-Martin, 2017). Significant improvements in balance, gait function, and other motor abilities have been observed in participants after boxing interventions, contributing to an overall enhancement in quality of life. Enhancing quality of life is a major goal in public health research and practice (Fayers and Machin, 2015). As individuals age, their life satisfaction becomes linked to their health and mortality rates (Lim et al., 2017). Given that patients often struggle with gait disorders and cognitive decline, boxing, a physical activity that combines exercise with cognitive stimulation, could play a significant role in improving their overall quality of life. Studies have shown that participating in boxing can be a pleasurable experience for individuals, leading to high levels of satisfaction and a more positive attitude toward coping with the disease (Brunet et al., 2022; Hermanns et al., 2021). The enjoyable nature of boxing and the strong sense of community belonging it fosters may encourage a more positive attitude toward coping with the disease (Domingos et al., 2022). However, Dawson et al. (2020) reported that 16 weeks of boxing training, once a week for 90 min per session, did not significantly reduce patients’ EQ-5D scores. The choice of quality-of-life assessment tool is crucial. The EQ-5D is a widely used generic health status scale that assesses patients’ quality of life from five aspects: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. It is applicable to various diseases and patient groups. In contrast, the commonly used PDQ-39 specifically assesses the quality of life of patients by summarizing scores from 39 items, such as motor function, emotional state, and cognitive function, providing a comprehensive reflection of the patients’ quality of life status (Sangarapillai et al., 2021). This suggests that selecting the appropriate measurement tool significantly impacts the evaluation of intervention effects.
Scientific literature has suggested that boxing exercises significantly slow down the progression disease in PD of patients. This is likely due to the high-intensity nature of boxing, which promotes neural plasticity and thus delays disease progression (Frazzitta et al., 2014; Tollár et al., 2018). Boxing training typically involves circuit training, incorporating various components such as aerobic exercise, strength training, and footwork drills. Studies have showed that increased levels of brain-derived neurotrophic factor (BDNF) after high-intensity exercise are closely linked to improved motor function (Farrukh et al., 2023; Landers et al., 2019). It is hypothesized that boxing primarily stimulates the release of neurotrophic factors like BDNF, particularly since BDNF is essential for maintaining the survival and synthesis of dopaminergic neurons in the basal ganglia, thereby reducing disease severity (Combs et al., 2013; Morris et al., 2019). However, it is important to consider the research by Sangarapillai et al. (2021), which indicated that after 10 weeks of boxing training, participants did not show immediate significant improvements in disease severity compared to a sensory training group, with symptoms regressing during the subsequent 10-week washout period. This finding contradicts most studies that advocate boxing as a means to moderately improve disease severity and offer potential neuroprotective benefits (Blacker et al., 2023; Combs et al., 2011; Patel et al., 2023). The discrepancy in results may be due to the use of subjective scales by Sangarapillai et al. to monitor exercise intensity, potentially deviating from objective methods such as heart rate monitoring (Sangarapillai et al., 2021). This underscores the significance of exercise intensity on the symptom severity in patients and emphasizes the need for more precise methods of monitoring exercise intensity in future studies to clarify the specific impact of boxing on PD symptomatology.
The study revealed that the adherence rate for patients participating in a boxing exercise program was consistently above 80%, with no reports of adverse events. Notably, the reasons for patient dropout were unrelated to the boxing exercises themselves, but rather due to conflicts with their time and work commitments (Combs et al., 2011; Domingos et al., 2022). The primary reasons for dropout included scheduling conflicts with boxing training sessions (Patel et al., 2023), transportation difficulties (Shearin et al., 2021), family emergencies (Shearin et al., 2021), and other medical issues unrelated to PD (Combs et al., 2011; Patel et al., 2023; Shearin et al., 2021). Like other recommended forms of exercise, such as Tai Chi (Li et al., 2014; Vergara-Diaz et al., 2018) and dance (Volpe et al., 2013), these activities demonstrate high levels of adherence. Recently, attention has shifted to boxing exercises that are high dosage, sustained over the long term and are engaging, enjoyable and motivating for people living with PD (Blacker et al., 2023; Domingos et al., 2022; Patel et al., 2023; Sangarapillai et al., 2021; Shearin et al., 2021). One of the key advantages of boxing as an exercise modality is its community-based nature, which facilitates accessible and sustained exercise. The boxing program also includes a variety of therapeutic exercises, such as strength training, balance exercises, and agility drills, which not only enhance physical well-being but also foster social interaction, making it an engaging and sustainable form of exercise. In contrast, traditional treatments for PD patients are often confined to hospitals or home settings and typically involve short-term interventions lasting only 2–6 weeks (Carroll et al., 2017; Morris et al., 2019). These brief interventions may lead to higher dropout rates, as patients may struggle to maintain motivation and engagement over longer periods. Low adherence may lead to poor health outcomes and potential increased healthcare costs in people with PD. Therefore, boxing emerges as a highly compliant and safe physical rehabilitation strategy. It is recommended that this type of intervention be further promoted among more PD patients in the future to improve their quality of life and health condition. By integrating diverse exercise elements and fostering social interaction, boxing offers a comprehensive approach to enhancing the lives of PD patients.
The duration of boxing exercise interventions in various studies ranged from 10 to 96 weeks, with a frequency of 1–3 times per week and each session lasting 60–90 min. Five studies required patients to undergo high-intensity training programs (Combs et al., 2013; Combs et al., 2011; Moore et al., 2021; Sangarapillai et al., 2021; Urrutia et al., 2020), one reported moderate exercise intensity (Shearin et al., 2021), and another’s exercise intensity ranged from moderate to high (Blacker et al., 2023). Although current research cannot provide definitive conclusive information, the dosage of boxing exercise programs is consistent with the American Physical Therapy Association clinical practice guidelines for PD patients. According to these guidelines, patients should participate in aerobic exercise for 30–60 min, once or twice a week, or engage in moderate to high-intensity resistance training for 30–40 min per session, at least three times a week (Osborne et al., 2022). Regular physical activity reduces inflammation and oxidative stress, thereby protecting the nervous system (Hlebichuk et al., 2023). Studies have shown that high-intensity multimodal training provides additional benefits over low-intensity programs, including improved disease severity, stamina, and reduced fatigue (Landers et al., 2019). Moreover, high-intensity, high-frequency agility training significantly enhances depression symptoms, quality of life, and mobility performance in PD patients (Tollar et al., 2018). Notably, compared to moderate-intensity exercise, high-intensity exercise has a greater impact on regulating BDNF, resulting in increased post-training BDNF levels (Shulman et al., 2013). These findings are crucial for designing rehabilitation programs for neurodegenerative diseases since BDNF offers neuroprotection against brain degeneration, promotes the survival of dopaminergic neurons, and directly affects motor function (Rahmani et al., 2019). In conclusion, this systematic review reinforces the notion that high-intensity exercise interventions are a viable and effective rehabilitation approach for PD patients. Therefore, we advocate for high-intensity boxing exercise as an effective physical rehabilitation program for these patients.
However, the current systematic review has several limitations. Firstly, upon reviewing the included studies, we found significant diversity in the implemented methodology and design. Only three studies were RCTs, while the other 10 employed non-RCTs designs. This heterogeneity in study design and intervention characteristics—such as type and duration of exercise—introduces potential biases. Consequently, we refrained from calculating effect sizes, which somewhat limits the clinical significance of research findings. Secondly, there was notable variation in the study samples concerning disease stage, age, and gender. Additionally, many studies did not report the use of levodopa or other PD medications. Therefore, our results should be interpreted with caution, as they do not offer clear guidance on the dosage and mode of intervention based on participants’ age range and disease severity. Thirdly, although all studies used comprehensive, current, and validated assessment tools, inconsistency in outcome measurement tools was apparent. Lastly, our review was constrained to English-language articles, possibly missing research published in other languages. To conclusively determine the safety and efficacy of boxing exercises for improving motor and non-motor symptoms in PD patients, future research should include more homogenous PD patient populations and conducting RCTs. When designing exercise programs for elderly patients, it is essential to consider key factors such as individualized assessment, selection of exercise types, intensity and frequency of exercise, safety and supervision, and long-term adherence.
Boxing exercises have demonstrated positive effects on both motor and non-motor symptoms in patients with PD, including improvements in lower extremity strength, balance, mobility, gait, depression, quality of life, and disease severity, particularly for patients with mild and moderate symptoms. This form of exercise is not only safe but also has high adherence, making it a valuable addition to medication and functional surgery. While evidence supporting the benefits of boxing exercises for PD patients continues to grow, there is still a need to establish the most effective treatment protocols. Future research on the effects of boxing exercise on PD patients requires scientific design, large sample size, long-term comprehensive intervention, and clear reporting standards.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
ZW: Conceptualization, Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. BS: Methodology, Writing – review & editing. CL: Conceptualization, Methodology, Writing – review & editing. HM: Methodology, Writing – review & editing. ZB: Methodology, Writing – review & editing. MC: Methodology, Writing – review & editing. LY: Methodology, Writing – review & editing. CC: Supervision, Writing – review & editing. LZ: Supervision, Writing – review & editing. DaW: Supervision, Writing – review & editing. DeW: Supervision, Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. The study was supported by Research and Innovation Grant for Graduate Students, Shanghai University of Sport (Project No. YJSCX-2024-026); The research on Key Technologies for Enhancing Athletic Performance in Combat Sports at the Paris Olympic Games through Scientific and Technological Assistance (22010503800); The program for Overseas High-level Talents at Shanghai Institutions of Higher Learning under Grant No. TP2019072; Shanghai Key Lab of Human Performance (Shanghai University of Sport) (11DZ2261100).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Alberts, J. L., Linder, S. M., Penko, A. L., Lowe, M. J., and Phillips, M. (2011). It is not about the bike, it is about the pedaling: forced exercise and Parkinson's disease. Exerc. Sport Sci. Rev. 39, 177–186. doi: 10.1097/JES.0b013e31822cc71a
Alberts, J. L., Phillips, M., Lowe, M. J., Frankemolle, A., Thota, A., Beall, E. B., et al. (2016). Cortical and motor responses to acute forced exercise in Parkinson's disease. Parkinsonism Relat. Disord. 24, 56–62. doi: 10.1016/j.parkreldis.2016.01.015
Balestrino, R., and Martinez-Martin, P. (2017). Neuropsychiatric symptoms, behavioural disorders, and quality of life in Parkinson's disease. J. Neurol. Sci. 373, 173–178. doi: 10.1016/j.jns.2016.12.060
Basso, J. C., and Suzuki, W. A. (2017). The effects of acute exercise on mood, cognition, neurophysiology, and neurochemical pathways: a review. Brain Plast. 2, 127–152. doi: 10.3233/bpl-160040
Biddle, S. J., and Asare, M. (2011). Physical activity and mental health in children and adolescents: a review of reviews. Br. J. Sports Med. 45, 886–895. doi: 10.1136/bjsports-2011-090185
Blacker, D. J., Fazio, R., Tucak, C., Beranek, P., Pollard, C., Shelley, T., et al. (2023). FIGHT-PD: a feasibility study of periodized boxing training for Parkinson disease. PM R 16, 36–46. doi: 10.1002/pmrj.12986
Bloem, B. R., Okun, M. S., and Klein, C. (2021). Parkinson's disease. Lancet 397, 2284–2303. doi: 10.1016/s0140-6736(21)00218-x
Brunet, J., Price, J., Wurz, A., McDonough, M., and Nantel, J. (2022). Boxing with Parkinson's disease: findings from a qualitative study using self-determination theory. Disabil. Rehabil. 44, 3880–3889. doi: 10.1080/09638288.2021.1891465
Carroll, L. M., Volpe, D., Morris, M. E., Saunders, J., and Clifford, A. M. (2017). Aquatic exercise therapy for people with Parkinson disease: a randomized controlled trial. Arch. Phys. Med. Rehabil. 98, 631–638. doi: 10.1016/j.apmr.2016.12.006
Chou, K. L., Elm, J. J., Wielinski, C. L., Simon, D. K., Aminoff, M. J., Christine, C. W., et al. (2017). Factors associated with falling in early, treated Parkinson's disease: the NET-PD LS1 cohort. J. Neurol. Sci. 377, 137–143. doi: 10.1016/j.jns.2017.04.011
Combs, S. A., Diehl, M. D., Chrzastowski, C., Didrick, N., McCoin, B., Mox, N., et al. (2013). Community-based group exercise for persons with Parkinson disease: a randomized controlled trial. NeuroRehabilitation 32, 117–124. doi: 10.3233/nre-130828
Combs, S. A., Diehl, M. D., Staples, W. H., Conn, L., Davis, K., Lewis, N., et al. (2011). Boxing training for patients with Parkinson disease: a case series. Phys. Ther. 91, 132–142. doi: 10.2522/ptj.20100142
Curtze, C., Nutt, J. G., Carlson-Kuhta, P., Mancini, M., and Horak, F. B. (2016). Objective gait and balance impairments relate to balance confidence and perceived mobility in people with Parkinson disease. Phys. Ther. 96, 1734–1743. doi: 10.2522/ptj.20150662
Dawson, R. A., Sayadi, J., Kapust, L., Anderson, L., Lee, S., Latulippe, A., et al. (2020). Boxing exercises as therapy for Parkinson disease. Top. Geriatr. Rehabil. 36, 160–165. doi: 10.1097/tgr.0000000000000275
De Freitas, T. B., Leite, P. H. W., Doná, F., Pompeu, J. E., Swarowsky, A., and Torriani-Pasin, C. (2020). The effects of dual task gait and balance training in Parkinson's disease: a systematic review. Physiother. Theory Pract. 36, 1088–1096. doi: 10.1080/09593985.2018.1551455
Dibble, L. E., Foreman, K. B., Addison, O., Marcus, R. L., and LaStayo, P. C. (2015). Exercise and medication effects on persons with Parkinson disease across the domains of disability: a randomized clinical trial. J. Neurol. Phys. Ther. 39, 85–92. doi: 10.1097/npt.0000000000000086
Domingos, J., de Lima, A. L. S., Steenbakkers-van der Pol, T., Godinho, C., Bloem, B. R., and de Vries, N. M. (2022). Boxing with and without kicking techniques for people with Parkinson's disease: an explorative pilot randomized controlled trial. J. Parkinsons Dis. 12, 2585–2593. doi: 10.3233/jpd-223447
Dorsey, E. R., and Bloem, B. R. (2018). The Parkinson pandemic-a call to action. JAMA Neurol. 75, 9–10. doi: 10.1001/jamaneurol.2017.3299
Fahn, S. (2018). The 200-year journey of Parkinson disease: reflecting on the past and looking towards the future. Parkinsonism Relat. Disord. 46, S1–s5. doi: 10.1016/j.parkreldis.2017.07.020
Fan, B., Jabeen, R., Bo, B., Guo, C., Han, M., Zhang, H., et al. (2020). What and how can physical activity prevention function on Parkinson's disease? Oxidative Med. Cell. Longev. 2020:4293071. doi: 10.1155/2020/4293071
Farrukh, S., Habib, S., Rafaqat, A., Sarfraz, A., Sarfraz, Z., and Tariq, H. (2023). Association of exercise, brain-derived neurotrophic factor, and cognition among older women: a systematic review and meta-analysis. Arch. Gerontol. Geriatr. 114:105068. doi: 10.1016/j.archger.2023.105068
Fayers, P. M., and Machin, D. (2015). Quality of life: The assessment, analysis and reporting of patient-reported outcomes (3rd ed.). Chichester, West Sussex: John Wiley & Sons.
Fernández-Landa, J., Santibañez-Gutierrez, A., Todorovic, N., Stajer, V., and Ostojic, S. M. (2023). Effects of creatine monohydrate on endurance performance in a trained population: a systematic review and meta-analysis. Sports Med. 53, 1017–1027. doi: 10.1007/s40279-023-01823-2
Fox, S. H., Katzenschlager, R., Lim, S. Y., Barton, B., de Bie, R. M. A., Seppi, K., et al. (2018). International Parkinson and movement disorder society evidence-based medicine review: update on treatments for the motor symptoms of Parkinson's disease. Mov. Disord. 33, 1248–1266. doi: 10.1002/mds.27372
Frazzitta, G., Maestri, R., Ghilardi, M. F., Riboldazzi, G., Perini, M., Bertotti, G., et al. (2014). Intensive rehabilitation increases BDNF serum levels in parkinsonian patients: a randomized study. Neurorehabil. Neural Repair 28, 163–168. doi: 10.1177/1545968313508474
Hermanns, M., Mastel-Smith, B., Donnell, R., Quarles, A., Rodriguez, M., and Wang, T. (2021). Counterpunching to improve the health of people with Parkinson's disease. J. Am. Assoc. Nurse Pract. 33, 1230–1239. doi: 10.1097/jxx.0000000000000598
Hlebichuk, J. L., Gretebeck, R. J., Garnier-Villarreal, M., Piacentine, L. B., Singh, M., and Gretebeck, K. A. (2023). Physical activity, inflammation, and physical function in older adults: results from the health & retirement study. Biol. Res. Nurs. 25, 24–32. doi: 10.1177/10998004221111217
Horbinski, C., Zumpf, K. B., McCortney, K., and Eoannou, D. (2021). Longitudinal observational study of boxing therapy in Parkinson's disease, including adverse impacts of the COVID-19 lockdown. BMC Neurol. 21:326. doi: 10.1186/s12883-021-02359-6
Kalia, L. V., and Lang, A. E. (2015). Parkinson's disease. Lancet 386, 896–912. doi: 10.1016/s0140-6736(14)61393-3
Kelly, V. E., Eusterbrock, A. J., and Shumway-Cook, A. (2012). A review of dual-task walking deficits in people with Parkinson's disease: motor and cognitive contributions, mechanisms, and clinical implications. Parkinsons Dis. 2012:918719. doi: 10.1155/2012/918719
Landers, M. R., Navalta, J. W., Murtishaw, A. S., Kinney, J. W., and Pirio Richardson, S. (2019). A high-intensity exercise boot camp for persons with Parkinson disease: a phase ii, pragmatic, randomized clinical trial of feasibility, safety, signal of efficacy, and disease mechanisms. J. Neurol. Phys. Ther. 43, 12–25. doi: 10.1097/npt.0000000000000249
Li, F., Harmer, P., Liu, Y., Eckstrom, E., Fitzgerald, K., Stock, R., et al. (2014). A randomized controlled trial of patient-reported outcomes with tai chi exercise in Parkinson's disease. Mov. Disord. 29, 539–545. doi: 10.1002/mds.25787
Lim, H. J., Min, D. K., Thorpe, L., and Lee, C. H. (2017). Trajectories of life satisfaction and their predictors among Korean older adults. BMC Geriatr. 17, 1–14. doi: 10.1186/s12877-017-0485-5
Miller Koop, M., Rosenfeldt, A. B., and Alberts, J. L. (2019). Mobility improves after high intensity aerobic exercise in individuals with Parkinson's disease. J. Neurol. Sci. 399, 187–193. doi: 10.1016/j.jns.2019.02.031
Milne-Ives, M., de Cock, C., Lim, E., Shehadeh, M. H., de Pennington, N., Mole, G., et al. (2020). The effectiveness of artificial intelligence conversational agents in health care: systematic review. J. Med. Internet Res. 22:e20346. doi: 10.2196/20346
Moore, A., Yee, E., Willis, B. W., Prost, E. L., Gray, A. D., and Mann, J. B. (2021). A community-based boxing program is associated with improved balance in individuals with Parkinson's disease. Int. J. Exerc. Sci. 14, 876–884. doi: 10.70252/BNAX9498
Morris, M. E., Ellis, T. D., Jazayeri, D., Heng, H., Thomson, A., Balasundaram, A. P., et al. (2019). Boxing for Parkinson's disease: has implementation accelerated beyond current evidence? Front. Neurol. 10:1222. doi: 10.3389/fneur.2019.01222
Osborne, J. A., Botkin, R., Colon-Semenza, C., DeAngelis, T. R., Gallardo, O. G., Kosakowski, H., et al. (2022). Physical therapist management of parkinson disease: a clinical practice guideline from the American Physical Therapy Association. Phys. Ther. 102:pzab302. doi: 10.1093/ptj/pzab302
Ou, Z., Pan, J., Tang, S., Duan, D., Yu, D., Nong, H., et al. (2021). Global trends in the incidence, prevalence, and years lived with disability of Parkinson's disease in 204 countries/territories from 1990 to 2019. Front. Public Health 9:776847. doi: 10.3389/fpubh.2021.776847
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372:n71. doi: 10.1136/bmj.n71
Patel, R. A., Blasucci, L., and Mahajan, A. (2023). A pilot study of a 12-week community-based boxing program for Parkinson's disease. J. Clin. Neurosci. 107, 64–67. doi: 10.1016/j.jocn.2022.12.006
Pedersen, K. F., Alves, G., Larsen, J. P., Tysnes, O. B., Møller, S. G., and Brønnick, K. (2012). Psychometric properties of the Starkstein apathy scale in patients with early untreated Parkinson disease. Am. J. Geriatr. Psychiatry 20, 142–148. doi: 10.1097/JGP.0b013e31823038f2
Raffegeau, T. E., Krehbiel, L. M., Kang, N., Thijs, F. J., Altmann, L. J. P., Cauraugh, J. H., et al. (2019). A meta-analysis: Parkinson's disease and dual-task walking. Parkinsonism Relat. Disord. 62, 28–35. doi: 10.1016/j.parkreldis.2018.12.012
Rahmani, F., Saghazadeh, A., Rahmani, M., Teixeira, A. L., Rezaei, N., Aghamollaii, V., et al. (2019). Plasma levels of brain-derived neurotrophic factor in patients with Parkinson disease: a systematic review and meta-analysis. Brain Res. 1704, 127–136. doi: 10.1016/j.brainres.2018.10.006
Rhodes, R. E., Martin, A. D., Taunton, J. E., Rhodes, E. C., Donnelly, M., and Elliot, J. (1999). Factors associated with exercise adherence among older adults. An individual perspective. Sports Med. 28, 397–411. doi: 10.2165/00007256-199928060-00003
Sangarapillai, K., Norman, B. M., and Almeida, Q. J. (2021). Boxing vs sensory exercise for Parkinson's disease: a double-blinded randomized controlled trial. Neurorehabil. Neural Repair 35, 769–777. doi: 10.1177/15459683211023197
Shearin, S., Braitsch, M., and Querry, R. (2021). The effect of a multi-modal boxing exercise program on cognitive locomotor tasks and gait in persons with Parkinson disease. NeuroRehabilitation 49, 619–627. doi: 10.3233/nre-210218
Shulman, L. M., Katzel, L. I., Ivey, F. M., Sorkin, J. D., Favors, K., Anderson, K. E., et al. (2013). Randomized clinical trial of 3 types of physical exercise for patients with Parkinson disease. JAMA Neurol. 70, 183–190. doi: 10.1001/jamaneurol.2013.646
Song, R., Grabowska, W., Park, M., Osypiuk, K., Vergara-Diaz, G. P., Bonato, P., et al. (2017). The impact of tai chi and Qigong mind-body exercises on motor and non-motor function and quality of life in Parkinson's disease: a systematic review and meta-analysis. Parkinsonism Relat. Disord. 41, 3–13. doi: 10.1016/j.parkreldis.2017.05.019
Sonne, J. W., Joslyn, K., Reus, K., Angulo, M., Guettler, S., and Beato, M. C. (2021). A retrospective analysis of group-based boxing exercise on measures of physical mobility in patients with Parkinson disease. Am. J. Lifestyle Med. 18, 558–566. doi: 10.1177/15598276211028144
Sterne, J. A., Hernán, M. A., Reeves, B. C., Savović, J., Berkman, N. D., Viswanathan, M., et al. (2016). ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 355:i4919. doi: 10.1136/bmj.i4919
Strouwen, C., Molenaar, E., Münks, L., Keus, S. H. J., Zijlmans, J. C. M., Vandenberghe, W., et al. (2017). Training dual tasks together or apart in Parkinson's disease: results from the DUALITY trial. Mov. Disord. 32, 1201–1210. doi: 10.1002/mds.27014
Tollar, J., Nagy, F., Kovacs, N., and Hortobagyi, T. (2018). A high-intensity multicomponent agility intervention improves Parkinson patients' clinical and motor symptoms. Arch. Phys. Med. Rehabil. 99:e1, 2478–2484.e1. doi: 10.1016/j.apmr.2018.05.007
Tollár, J., Nagy, F., Kovács, N., and Hortobágyi, T. (2018). Two-year agility maintenance training slows the progression of parkinsonian symptoms. Med. Sci. Sports Exerc. 51, 237–245. doi: 10.1249/MSS.0000000000001793
Urrutia, M., Ivy, C., Pohl, P. S., and Denney, L. (2020). Boxing to improve sleep quality and daytime sleepiness in individuals with Parkinson disease pilot study. Top. Geriatr. Rehabil. 36, 170–175. doi: 10.1097/tgr.0000000000000277
Vergara-Diaz, G., Osypiuk, K., Hausdorff, J. M., Bonato, P., Gow, B. J., Miranda, J. G., et al. (2018). Tai chi for reducing dual-task gait variability, a potential mediator of fall risk in Parkinson's disease: a pilot randomized controlled trial. Glob. Adv. Health Med. 7:2164956118775385. doi: 10.1177/2164956118775385
Volpe, D., Signorini, M., Marchetto, A., Lynch, T., and Morris, M. E. (2013). A comparison of Irish set dancing and exercises for people with Parkinson's disease: a phase II feasibility study. BMC Geriatr. 13:54. doi: 10.1186/1471-2318-13-54
Wipfli, B., Landers, D., Nagoshi, C., and Ringenbach, S. (2011). An examination of serotonin and psychological variables in the relationship between exercise and mental health. Scand. J. Med. Sci. Sports 21, 474–481. doi: 10.1111/j.1600-0838.2009.01049.x
Keywords: Parkinson’s disease, boxing, exercise, movement disorder, rehabilitation, physiotherapy
Citation: Wang Z, Song B, Liu C, Ma H, Bai Z, Carneiro MAS, Youssef L, Chen C, Zhang L, Wang D and Wang D (2025) Effects of boxing exercise in people with Parkinson’s disease: a systematic review. Front. Aging Neurosci. 17:1505326. doi: 10.3389/fnagi.2025.1505326
Edited by:
Roger David Adams, University of Canberra, AustraliaReviewed by:
James William Hendry Sonne, University of South Carolina, United StatesCopyright © 2025 Wang, Song, Liu, Ma, Bai, Carneiro, Youssef, Chen, Zhang, Wang and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dexin Wang, d2FuZ2RleGluZ0BzdXMuZWR1LmNu
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.