
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Aging Neurosci., 05 February 2025
Sec. Neurocognitive Aging and Behavior
Volume 17 - 2025 | https://doi.org/10.3389/fnagi.2025.1501640
This article is part of the Research TopicProgress in the Assessment and Intervention of Neurocognitive Aging and Neurodegenerative DiseasesView all 16 articles
 Kerong Chen1†Sitong Zhou2†Shiyu Lu3†
Kerong Chen1†Sitong Zhou2†Shiyu Lu3† Yuliang Qin2
Yuliang Qin2 Xinyao Li2
Xinyao Li2 Yi Li1Tianyun Liu1Mei Zhang1Kun Xu1Hongping Shi1Xiaoman Lv2Kai Yuan4*Hongling Shi1*
Yi Li1Tianyun Liu1Mei Zhang1Kun Xu1Hongping Shi1Xiaoman Lv2Kai Yuan4*Hongling Shi1* Dongdong Qin2*
Dongdong Qin2*Objective: To analyze the literature on the efficacy of repetitive transcranial magnetic stimulation (rTMS) in treating dysarthria in patients with Parkinson's disease (PD) and provide a reference for targeted clinical treatment of dysarthria in PD patients.
Methods: A systematic search was conducted in English and Chinese databases, including Embase, Cochrane, Medline, PubMed, CNKI, Wanfang, Chinese Biomedical Literature Database, and VIP Database, for relevant literature on rTMS treatment for dysarthria in PD patients. The search timeframe was from the inception of each database to October 2023. Literature was screened according to inclusion and exclusion criteria. Two researchers extracted information on study subjects, age, intervention methods, intervention duration, intervention frequency, evaluation indicators, and intervention results from the included literature. The modified Jadad scale was used to evaluate the quality of the literature.
Results: A total of seven studies were included, mainly focusing on the frequency, duration, and stimulation site of rTMS for dysarthria in PD patients. Six studies indicated that rTMS treatment improved dysarthria in PD patients.
Conclusion: Repetitive transcranial magnetic stimulation has a positive effect on improving dysarthria in PD patients, but further research is needed to determine its efficacy.
Parkinson's disease (PD) is a common progressive neurodegenerative disorder frequently encountered in clinical practice. Its primary pathological features include the progressive loss of dopaminergic neurons in the substantia nigra pars compacta and the formation of Lewy bodies. Genetic and epidemiological studies indicate that PD results from the interplay of multiple factors, including genetics, environmental factors, and neurological aging (Bloem et al., 2021). Epidemiological surveys reveal that the prevalence of PD in Western countries reaches 2%−3% among individuals aged 65 years and older and exceeds 4% in those aged 80 years and above (Simon et al., 2020). A community-based study in China showed that the prevalence of PD among the elderly population aged 60 years and older was 1.37% [95% CI (1.02%, 1.73%)], with an estimated total of 3.62 million PD patients in China (Qi et al., 2021). As the world's most populous country, the number of PD patients in China is projected to reach 5 million by 2030, accounting for nearly half of the global PD patient population (Parkinson's Disease Movement Disorders Group Neurologist Branch of Chinese Medical Doctor Association, 2020).
Research has demonstrated that dysarthria is present in 70%−90% of PD patients in the early stages of the disease and even in the prodromal phase (prodromal PD, pPD), making it one of the most common symptoms of PD (Ma et al., 2014; Schalling et al., 2017; Collaborators, 2019; Fereshtehnejad et al., 2019). Dysarthria in PD is primarily characterized by abnormalities in the force, speed, range, amplitude, stability, or accuracy of the movements required for speech production, including respiration, phonation, resonance, and rhythm. Clinical manifestations mainly include lingual muscle rigidity and tremors, leading to reduced mouth opening, imprecise lip closure, monotonous intonation, short sentences, reduced stress, slurred speech, and either excessively fast or slow speech rate. These symptoms significantly impact patients' communication abilities, resulting in reduced social interaction and diminished quality of life (Li and Li, 2021; Lu et al., 2022). Currently, commonly used dysarthria training methods include oral motor exercises, articulatory movement and speech ability training, as well as voice and breathing exercises. However, high-quality evidence supporting the efficacy of these methods remains limited (Han, 2019), and clinical treatment often requires prolonged periods with suboptimal outcomes.
Repetitive transcranial magnetic stimulation (rTMS) is a non-invasive neuromodulation technique that delivers repetitive stimulation to specific areas of the cerebral cortex using pulsed magnetic fields (Lin et al., 2020). High-frequency rTMS (≥5 Hz) excites neurons, increasing local cortical excitability, regional cerebral blood flow, and metabolism (Elahi et al., 2009). While, low-frequency rTMS (≤1 Hz) inhibits neurons, thereby modulating cortical excitability and central nervous system plasticity (Du et al., 2019). rTMS has a regulatory effect on both local and remote neural functions (Brandt et al., 2021). Due to its non-invasive, effective, and cost-efficient nature, rTMS has emerged as a promising rehabilitation technology with widespread applications in the treatment and neurorehabilitation of various neurological and psychiatric disorders, such as neuropathic pain, severe depression, post-acute stroke motor dysfunction, epilepsy, cerebrovascular diseases, and Parkinson's disease (PD) (Ma et al., 2020). In the context of PD, rTMS is primarily employed to alleviate motor symptoms, depression, cognitive dysfunction, and other associated impairments (Chi, 2020).
The present study aims to systematically evaluate the clinical efficacy of rTMS in treating dysarthria in PD patients, with the ultimate goal of providing evidence-based guidance for the clinical application of rTMS in the management of PD-related dysarthria.
A comprehensive literature search was conducted in EMBASE, Cochrane, Medline, PubMed, China National Knowledge Infrastructure (CNKI), Wanfang Database, Chinese Biomedical Literature Database, and VIP Database. The search terms were divided into three groups: (1) population: Chinese search terms included “Parkinson's disease,” “idiopathic Parkinson's disease,” “Lewy body Parkinson's disease” and “primary parkinsonism.” English search terms included “Parkinson's disease,” “idiopathic Parkinson's disease,” “Lewy Body Parkinson's disease,” “Parkinson's disease,” “idiopathic Parkinson's disease,” “primary Parkinsonism,” and “paralysis agitans;” (2) symptoms: Chinese search terms included “dysarthria,” “voice disorders,” “hypokinetic dysarthria,” and “language disorders.” English search terms included “dysarthria,” “hypokinetic dysarthria,” and “language disorders;” (3) intervention: the Chinese search term was “repetitive transcranial magnetic stimulation” and English search terms included “repetitive transcranial magnetic stimulation,” “rTMS,” “transcranial magnetic stimulation,” and “noninvasive brain stimulation.” The entire search process was completed in December 2023.
Inclusion criteria: (1) studies focusing on dysarthria in Parkinson's disease; (2) studies involving rTMS as an intervention; (3) studies with assessments including scales and test indicators; (4) studies published in Chinese or English. Exclusion criteria: (1) full text not available; (2) duplicate publications; (3) lack of relevant measurement indicators; (4) review articles.
Literature screening and data extraction were conducted independently by two researchers following predetermined criteria. Any disagreements were resolved through discussion or, if necessary, adjudication by a third party. EndNote software was used to manage the references. Initial screening involved reviewing titles and abstracts, and full-text reviews were performed for studies that potentially met the inclusion criteria to confirm eligibility. Data were extracted and organized using Excel and included information on study participants, age, intervention methods, duration and frequency of interventions, evaluation indicators, and intervention outcomes.
The quality assessment of all included studies was performed by two researchers. The methodological quality of the included studies was evaluated using the simple assessment method recommended by the Cochrane Collaboration. The evaluation criteria included key indicators of internal validity, such as the correctness of randomization methods, the correctness of allocation concealment, the use of intention-to-treat analysis, the implementation of blinding, the reporting of dropouts and withdrawals, and the comparability of baseline data.
Studies were rated as follows:
• Grade A: all quality assessment criteria were met, indicating the lowest possibility of bias.
• Grade B: one or more of the quality assessment criteria were only partially met, indicating a moderate possibility of corresponding bias.
• Grade C: one or more of the quality assessment criteria were not met at all, indicating a high possibility of bias.
After independently assessing the quality of the literature, the two researchers discussed the quality of each study according to the above evaluation criteria and reached a consensus on the final decision to include or exclude the study.
After reading the full text, the following data were extracted: (1) inclusion criteria and sample size; (2) sampling and grouping methods and processes; (3) basic information of the study subjects; (4) study conditions; (5) rTMS treatment device type; (6) parameter settings, including frequency, intensity, location, number of sessions (sequences), duration, and treatment compliance; and (7) means and standard deviations of continuous outcome measures.
The initial search yielded 125 relevant studies, including 15 in Chinese and 110 in English. After excluding 88 studies due to duplicate publication, overlap, or obvious non-compliance with the inclusion criteria, and further excluding case-control and descriptive studies based on title and abstract screening, 37 clinical controlled studies were included. By retrieving full texts, reading, and conducting quality assessments, 30 non-randomized controlled trials and clinical trials without a control group were excluded. Finally, seven studies were included, comprising two in Chinese and five in English. The literature screening process and results are presented in Figure 1.

Figure 1. PRISMA flow diagram of the search process for studies.
Among the seven included studies, two were published in Chinese (Wang et al., 2022a,b), and five were published in English (Hartelius et al., 2010; Eliasova et al., 2013; Brabenec et al., 2019, 2021; Gómez-Rodellar et al., 2023). The basic characteristics of the included studies are summarized in Table 1.

Table 1. Basic characteristics of included literature.
The quality of the included randomized controlled trials was assessed using the evaluation criteria from the Cochrane Collaboration Handbook, version 5.1.0. The results showed that all seven studies were rated as grade B in terms of quality, as detailed in Table 2.
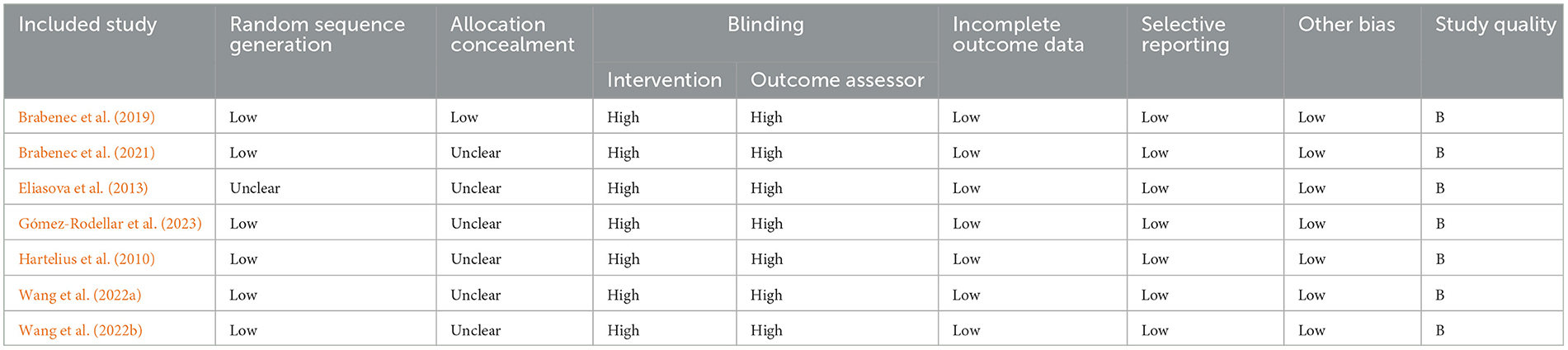
Table 2. Quality assessment of included studies.
This study conducted a comprehensive evaluation of rTMS in the treatment of dysarthria in Parkinson's disease (PD) to assess its therapeutic efficacy. rTMS produces brief pulse stimulation in a non-invasive manner, generating induced currents in the cortex that lead to axonal depolarization and action potential generation in neurons (Iglesias, 2020). Common stimulation targets for rTMS in the treatment of speech disorders in PD include the primary motor cortex (M1), superior temporal gyrus (STG), and dorsolateral prefrontal cortex (DLPFC).
In this systematic review, seven included studies utilized the aforementioned stimulation sites, strictly adhering to the inclusion and exclusion criteria. However, the analysis results may still contain some errors. The number of included studies was relatively small, and the quality of the literature varied. The evaluation methods and indicators were not uniform across the included studies, making it difficult to weigh the effectiveness of the literature during the analysis process, and high-quality studies were scarce. Furthermore, there were differences in the methods of the included studies, such as insufficient use of randomization methods and inconsistencies in outcome measurement methods. These differences and limitations may lead to serious bias in the study results. Therefore, after data extraction, a quantitative analysis could not be performed, and a descriptive systematic review method was used to analyze the effects of rTMS on speech function in PD patients with dysarthria. Future research should increase the sample size, establish unified analysis methods, include more high-quality studies, exclude low-quality studies, and conduct long-term follow-ups on clinical samples. This will provide high-quality, reliable, and valid data for an effective systematic review.
The methodological quality of the studies included in this research was graded as level B. Most studies did not specify whether allocation concealment and assessor blinding were performed. Due to the nature of the intervention, it is challenging to achieve blinding of study participants, which may lead to certain biases in the outcome measures. Moreover, this study only searched Chinese and English databases. As there have been relatively few relevant publications in recent years, both domestically and internationally, only seven articles were ultimately included in this study, with five in English and two in Chinese. Gray literature and studies published in other languages were not considered, which may result in a degree of publication bias.
Dysarthria is a speech disorder caused by paralysis, weakness, or incoordination of speech-related muscles due to central or peripheral nerve damage. Speech production requires mapping phonological representations onto the articulation network, and accurate speech output depends on the auditory-motor integration process mediated by the dorsal language pathway (Wang et al., 2023). Specifically, the cortical regions involved in auditory-motor integration include the superior temporal gyrus (STG), primary motor cortex (M1), dorsolateral prefrontal cortex (DLPFC), and premotor cortex, which are closely related to the occurrence of PD speech disorders (Li et al., 2022; Steurer et al., 2022; Wang et al., 2023). Studies have demonstrated that rTMS can induce an increase in dopamine levels in the nigrostriatal system (Khedr et al., 2007). Research on rodents has indicated that rTMS can effectively reduce the loss of dopaminergic neurons in the nigrostriatal pathway and improve cognitive and motor functions (Zong et al., 2022). Current evidence suggests that low-frequency rTMS (≤1 Hz) has an inhibitory effect on target neurons, which helps to reduce excessive neural activity that may lead to Parkinsonian dysarthria and other motor symptoms (Zhang et al., 2022). Dysarthria in PD patients is primarily attributed to impaired activation and coordination of speech-related muscles, resulting from the progressive degeneration of the nigrostriatal pathway (Dashtipour et al., 2018). Additionally, reduced excitability of the basal ganglia to the cortex leads to physiological deficits in the larynx, joints, and respiratory system, as well as decreased cortical activity in areas of the speech production network (Narayana et al., 2022). Speech disorders in PD patients may also result from damage to the central or peripheral nerves, causing dysfunctions in the muscle movements involved in speech production (Iglesias, 2020). However, the brain's neural pathways possess plasticity, enabling the establishment of new pathways through stimulation of the neural network. This plasticity can promote the recovery of motor function in the organs of articulation, thus enhancing speech fluency and normalization in patients with dysarthria (Zhu et al., 2019). High-frequency rTMS enhances cortical excitability and modulates neural activity in specific brain regions involved in motor control and speech production, such as the supplementary motor area (SMA) and prefrontal cortex, and can be used to treat dysarthria (Brabenec et al., 2021). rTMS enhances brain neuroplasticity by modulating synaptic activity through both long-duration excitation and inhibition. It regulates neurotransmitter and neuromodulator levels, affects ion channels, and alters the expression of genes involved in plasticity. These effects promote the reactivation of the classical brain network and recruit underactive brain regions surrounding the lesion, ultimately improving speech and language function and accelerating speech recovery. Through functional reorganization, rTMS facilitates cortical remodeling (Hoogendam et al., 2010; Murdoch and Barwood, 2013; Wang et al., 2015; Valero-Cabré et al., 2017; Zhou and Dan, 2021). Additionally, rTMS has been shown to improve cerebral blood flow and metabolism, regulate ionic balance, inhibit apoptosis, and induce persistent changes in cortical excitability. It also affects neurotransmitter release and activates gene and protein expression, further enhancing cortical functional remodeling (Wang F. et al., 2022). By modulating the excitability of the cerebral cortex, rTMS can control motor function in the mouth, face, and tongue, thereby improving the motor function necessary for speech and language production. Therefore, different frequencies of rTMS can be utilized to regulate brain excitability, activate the nigrostriatal pathway, and increase levels of neurotransmitters such as dopamine, thereby improving the motor and coordination functions of muscle groups related to movement, respiration, and phonation, ultimately ameliorating dysarthria (Figure 2).
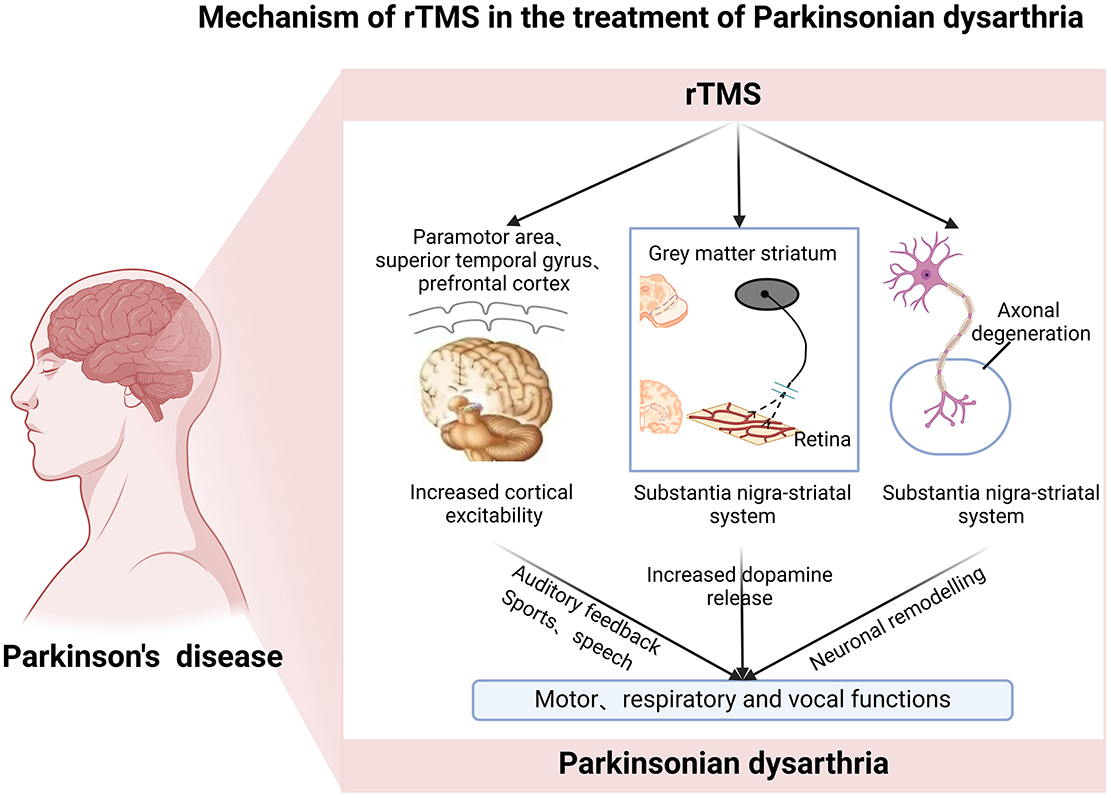
Figure 2. Roles and mechanisms of rTMS in the treatment of Parkinsonian dysarthria.
In this study, a total of seven articles (Hartelius et al., 2010; Eliasova et al., 2013; Brabenec et al., 2021; Wang et al., 2022a,b; Gómez-Rodellar et al., 2023) were included to explore the clinical efficacy of rTMS for Parkinsonian dysarthria. Among them, two randomized controlled trials (RCTs) (Eliasova et al., 2013; Brabenec et al., 2021) that included the 3F Test–Dysarthric Profile (3FT—subtests of facial dynamics, phonation, and phonetics) as outcome measures showed that rTMS can improve symptoms of Parkinsonian dysarthria, such as insufficient airflow, frequency/amplitude perturbation, and impaired speech rate and rhythm, to a certain extent.
One RCT that measured outcomes using the Frenchay Dysarthria Assessment indicated that rTMS can improve articulation movements, articulation clarity, ability to control loudness (Wang et al., 2022b), and ability to control speech rate in Parkinsonian dysarthria.
Two other studies used speech and voice as outcome measures. The results showed that rTMS can enhance respiratory support, coordination of respiration and phonation, and the regularity of vocal fold closure in patients with Parkinsonian dysarthria.
Previous evidence has demonstrated that rTMS is beneficial for improving prosody, loudness, and rhythm, enhancing speech function (Brabenec et al., 2021; Li et al., 2023), and significantly increasing voice quality, loudness, and vocal intensity, as well as tongue flexibility and range of motion in patients with Parkinsonian dysarthria. These findings are consistent with the results of the current study (Wang et al., 2022b). However, Li T showed that low-frequency rTMS cannot significantly improve comprehension and repetition abilities in patients with aphasia (Li et al., 2020), and DIAS (Dias et al., 2006) and ELIASOVA et al. (Lerner et al., 2019). found that the application of rTMS in patients with Parkinsonian language disorders did not result in significant changes in acoustic assessment indicators (fundamental frequency and vocal intensity). These findings are inconsistent with the aforementioned results, and the discrepancies may be attributed to factors such as differences in stimulation sites. To determine whether rTMS can improve language function in patients with Parkinsonian dysarthria, more high-quality studies need to be included for analysis in the future.
rTMS, as a non-invasive brain stimulation technique, has shown potential for improving dysarthria in patients with PD. Studies indicate that many patients experience improvements in speech intelligibility and fluency following rTMS treatment. However, findings regarding its long-term efficacy and durability are inconsistent. Some patients maintain improved speech function for several months, while others experience symptom relapse within a shorter time.
Among the seven studies included, the duration of efficacy observation ranged from 1 to 10 weeks. Longer treatment durations appeared to yield better outcomes in language function for PD patients. For instance, L. Hartelius et al. conducted a 1-week rTMS intervention with 10 PD patients and found no significant differences in fricative duration, sustained vowel articulation, or mediated motor rate compared to pre-treatment levels (Hartelius et al., 2010). In contrast, a 10-week study by Lubos Brabenec et al. demonstrated that functional improvements in language, including articulation accuracy, spontaneous speech, reading, bimanual motor tasks, intonation quality, and speech intelligibility, which persisted for at least 8 weeks post-treatment (Brabenec et al., 2019, 2021). Additionally, Xiaowen Wang's 30-day rTMS treatment study showed further improvements in voice function compared to the follow-up period (Eliasova et al., 2013).
In clinical applications, adverse reactions to rTMS include seizures, headaches, nausea, and vomiting. Among these adverse reactions, seizures are the most severe, and research has shown that this reaction is mostly induced by high-frequency stimulation (Li et al., 2015; Shah-Basak et al., 2016; Bucur and Papagno, 2019; Duncan et al., 2020; Li et al., 2020). Therefore, special attention should be paid to the safety of rTMS during its clinical application. In this study, a total of seven articles were included, and none of them reported adverse events related to the use of rTMS treatment. rTMS treatment was generally well-tolerated in the seven studies included in this paper. Of these, three studies explicitly reported the absence of adverse effects (Hartelius et al., 2010; Eliasova et al., 2013; Brabenec et al., 2021), while the remaining four studies did not provide details regarding the presence or absence of adverse effects associated with rTMS (Wang et al., 2015; Brabenec et al., 2019; Wang F. et al., 2022; Gómez-Rodellar et al., 2023). In all the included studies, most patients were willing to receive rTMS stimulation treatment. The rTMS treatment provided in each study was easy to use, had good operability, and patients had a high acceptance of the treatment. However, due to the limited number of studies included in this review, the safety of rTMS in the treatment of Parkinsonian dysarthria requires further investigation.
This study preliminarily confirms that rTMS has a certain effect on improving patients' articulation function, which brings positive influences on the prevention and symptom intervention for patients with Parkinsonian dysarthria. However, considering the included studies, there are differences in the intervention protocols, suggesting that the intervention plans for rTMS treatment in patients with Parkinsonian dysarthria need further improvement. Due to the differences in assessment tools and expression methods, it is difficult to conduct a combined analysis of the intervention effects of rTMS on related symptoms in patients with Parkinsonian dysarthria. This may be because there is currently no specific assessment tool for Parkinsonian dysarthria. Moreover, there are limited studies on the application of rTMS treatment in patients with Parkinsonian dysarthria, resulting in a small amount of data obtained, which further limits data pooling and quantitative analysis.
This systematic review demonstrates that rTMS treatment for Parkinsonian dysarthria is safe and feasible, and has a certain effect on intervening related symptoms of Parkinsonian dysarthria, providing a potentially effective intervention method for clinical treatment of Parkinsonian dysarthria. However, this study has certain limitations. Firstly, the sample size of the included literature is small and limited to Chinese and English literature, which may lead to publication bias. Secondly, there are differences in the assessment scales among the literature, so a large number of effect size combined analyses could not be performed, which may affect the research results. Thirdly, in the included studies, the assessors did not implement blinding when evaluating patients, which may lead to the possibility of measurement bias due to confounding subjective factors. In future research, the safety of rTMS should be quantified using physiological indicators; adding imaging evaluation can obtain more objective and scientific rTMS efficacy; the regulation of rTMS stimulation intensity, pulse number, and intervention time is a new direction for exploring the optimal efficacy of rTMS. Furthermore, due to the limited number of included studies and heterogeneity among the studies, this research could not quantitatively analyze and evaluate the intervention effect of rTMS on related symptoms of Parkinsonian dysarthria. Future studies still need to further improve the rTMS protocol and conduct large-sample randomized controlled trials to further verify the results.
Although this review highlights the overall efficacy of rTMS treatment in improving dysarthria in PD patients, significant heterogeneity exists among the included studies. Differences in study design, such as variations in rTMS frequency, stimulation sites, intervention duration, and participant selection criteria, may contribute to inconsistent outcomes. For instance, some studies targeted motor regions specifically associated with speech production, while others employed broader stimulation sites, potentially influencing efficacy. Additionally, the lack of uniform evaluation metrics, such as inconsistent methods for assessing speech intelligibility and motor control, limits the comparability of results. Potential biases, including small sample sizes, inadequate blinding, and variability in the severity of dysarthria, further complicate the interpretation of findings. Despite these limitations, the results suggest that rTMS can play a role in clinical practice by offering a non-invasive therapeutic option for managing dysarthria in PD patients. However, standardized protocols and larger, well-designed trials are still needed to confirm these findings and guide the development of evidence-based clinical guidelines.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
KC: Writing – original draft, Writing – review & editing. SZ: Writing – original draft, Writing – review & editing. SL: Writing – original draft, Writing – review & editing. YQ: Writing – review & editing. XLi: Writing – review & editing. YL: Writing – review & editing. TL: Writing – review & editing. MZ: Writing – review & editing. KX: Writing – review & editing. HongpS: Writing – review & editing. XLv: Writing – review & editing. KY: Supervision, Writing – original draft, Writing – review & editing. HonglS: Funding acquisition, Supervision, Writing – original draft, Writing – review & editing. DQ: Funding acquisition, Supervision, Validation, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by the National Clinical Key Specialty Project, Clinical Key Specialty Project of Yunnan Province, the Hospital Foundation of the Third People's Hospital of Yunnan Province (2024SSYKT49), Applied Basic Research Programs of Science and Technology Commission Foundation of Yunnan Province (202301AS070053), Scientific Research Projects for High-level Talents of Yunnan University of Chinese Medicine (2019YZG01), and Young Top-Notch Talent in 10,000 Talent Program of Yunnan Province (YNWR-QNBJ-2019-235).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Bloem, B. R., Okun, M. S., and Klein, C. (2021). Parkinson's disease. Lancet 397, 2284–2303. doi: 10.1016/S0140-6736(21)00218-X
Brabenec, L., Klobusiakova, P., Barton, M., Mekyska, J., Galaz, Z., Zvoncak, V., et al. (2019). Non-invasive stimulation of the auditory feedback area for improved articulation in Parkinson's disease. Parkinson. Relat. Disord. 61, 187–192. doi: 10.1016/j.parkreldis.2018.10.011
Brabenec, L., Klobusiakova, P., Simko, P., Kostalova, M., Mekyska, J., and Rektorova, I. (2021). Non-invasive brain stimulation for speech in Parkinson's disease: a randomized controlled trial. Brain Stimul. 14, 571–578. doi: 10.1016/j.brs.2021.03.010
Brandt, S. J., Oral, H. Y., Arellano-Bravo, C., Plawecki, M. H., Hummer, T. A., and Francis, M. M. (2021). Repetitive transcranial magnetic stimulation as a therapeutic and probe in schizophrenia: examining the role of neuroimaging and future directions. Neurotherapeutics 18, 827–844. doi: 10.1007/s13311-021-01046-1
Bucur, M., and Papagno, C. (2019). Are transcranial brain stimulation effects long-lasting in post-stroke aphasia? A comparative systematic review and meta-analysis on naming performance. Neurosci. Biobehav. Rev. 102, 264–289. doi: 10.1016/j.neubiorev.2019.04.019
Chi, H. (2020). Analysis of the clinical efficacy and safety of repetitive transcranial magnetic stimulation in the treatment of Parkinson's disease. Chin. Prac. Med. 15, 79–81. doi: 10.14163/j.cnki.11-5547/r.2020.04.036
Collaborators, G. N. (2019). Global, regional, and national burden of neurological disorders, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 18, 459–480. doi: 10.1016/S1474-4422(18)30499-X
Dashtipour, K., Tafreshi, A., Lee, J., and Crawley, B. (2018). Speech disorders in Parkinson's disease: pathophysiology, medical management and surgical approaches. Neurodegener. Dis. Manag. 8, 337–348. doi: 10.2217/nmt-2018-0021
Dias, A. E., Barbosa, E. R., Coracini, K., Maia, F., Marcolin, M. A., and Fregni, F. (2006). Effects of repetitive transcranial magnetic stimulation on voice and speech in Parkinson's disease. Acta Neurol. Scand. 113, 92–99. doi: 10.1111/j.1600-0404.2005.00558.x
Du, J., Yang, F., Hu, J., Hu, J., Xu, Q., Cong, N., et al. (2019). Effects of high- and low-frequency repetitive transcranial magnetic stimulation on motor recovery in early stroke patients: evidence from a randomized controlled trial with clinical, neurophysiological and functional imaging assessments. Neuroimage Clin. 21:101620. doi: 10.1016/j.nicl.2018.101620
Duncan, E. S., Pradeep, A. A., and Small, S. L. (2020). A review of biological interventions in chronic aphasia. Ann. Indian Acad. Neurol. 23, S82–S94. doi: 10.4103/aian.AIAN_549_20
Elahi, B., Elahi, B., and Chen, R. (2009). Effect of transcranial magnetic stimulation on Parkinson motor function–systematic review of controlled clinical trials. Mov. Disord. 24, 357–363. doi: 10.1002/mds.22364
Eliasova, I., Mekyska, J., Kostalova, M., Marecek, R., Smekal, Z., and Rektorova, I. (2013). Acoustic evaluation of short-term effects of repetitive transcranial magnetic stimulation on motor aspects of speech in Parkinson's disease. J. Neural Transm. 120, 597–605. doi: 10.1007/s00702-012-0953-1
Fereshtehnejad, S. M., Yao, C., Pelletier, A., Montplaisir, J. Y., Gagnon, J. F., and Postuma, R. B. (2019). Evolution of prodromal Parkinson's disease and dementia with Lewy bodies: a prospective study. Brain 142, 2051–2067. doi: 10.1093/brain/awz111
Gómez-Rodellar, A., Mekyska, J., Gómez-Vilda, P., Brabenec, L., Šimko, P., and Rektorová, I. (2023). A pilot study on the functional stability of phonation in EEG bands after repetitive transcranial magnetic stimulation in Parkinson's disease. Int. J. Neural Syst. 33:2350028. doi: 10.1142/S0129065723500284
Han, J. (2019). Post-stroke dysarthria treated by acupuncture combined with speech-language training: bibliometric analysis and verification of clinical efficacy. China Tissue Eng. Res. 23, 1013–1017. doi: 10.3969/j.issn.2095-4344.1119
Hartelius, L., Svantesson, P., Hedlund, A., Holmberg, B., Revesz, D., and Thorlin, T. (2010). Short-term effects of repetitive transcranial magnetic stimulation on speech and voice in individuals with Parkinson's disease. Folia Phoniatr. Logop. 62, 104–109. doi: 10.1159/000287208
Hoogendam, J. M., Ramakers, G. M., and Di Lazzaro, V. (2010). Physiology of repetitive transcranial magnetic stimulation of the human brain. Brain Stimul. 3, 95–118. doi: 10.1016/j.brs.2009.10.005
Iglesias, A. H. (2020). Transcranial magnetic stimulation as treatment in multiple neurologic conditions. Curr. Neurol. Neurosci. Rep. 20:1. doi: 10.1007/s11910-020-1021-0
Khedr, E. M., Rothwell, J. C., Shawky, O. A., Ahmed, M. A., Foly, N., and Hamdy, A. (2007). Dopamine levels after repetitive transcranial magnetic stimulation of motor cortex in patients with Parkinson's disease: preliminary results. Mov. Disord. 22, 1046–1050. doi: 10.1002/mds.21460
Lerner, A. J., Wassermann, E. M., and Tamir, D. I. (2019). Seizures from transcranial magnetic stimulation 2012-2016: results of a survey of active laboratories and clinics. Clin. Neurophysiol. 130, 1409–1416. doi: 10.1016/j.clinph.2019.03.016
Li, Q., Millard, K., Tetnowski, J., Narayana, S., and Cannito, M. (2023). Acoustic analysis of intonation in persons with Parkinson's disease receiving transcranial magnetic stimulation and intensive voice treatment. J. Voice 37, 203–214. doi: 10.1016/j.jvoice.2020.12.019
Li, S., and Li, T. (2021). The effect of positive emotional music therapy on anxiety and depression in patients with Parkinson's disease. Chinese J. Phys. Med. Rehabil. 43, 639–641. doi: 10.3760/cma.j.issn.0254-1424.2021.07.014
Li, T., Zeng, X., Lin, L., Xian, T., and Chen, Z. (2020). Effects of repetitive transcranial magnetic stimulation with different frequencies on post-stroke aphasia: a PRISMA-compliant meta-analysis. Medicine 99:e20439. doi: 10.1097/MD.0000000000020439
Li, T., Zhu, X., Wu, X., Gong, Y., Jones, J. A., Liu, P., et al. (2022). Continuous theta burst stimulation over left and right supramarginal gyri demonstrates their involvement in auditory feedback control of vocal production. Cereb. Cortex 33, 11–22. doi: 10.1093/cercor/bhac049
Li, Y., Qu, Y., Yuan, M., and Du, T. (2015). Low-frequency repetitive transcranial magnetic stimulation for patients with aphasia after stoke: a meta-analysis. J. Rehabil. Med. 47, 675–681. doi: 10.2340/16501977-1988
Lin, L., Wang, H., and Liao, W. (2020). Research progress on repetitive transcranial magnetic stimulation for the treatment of motor symptoms in Parkinson's disease. Chin. J. Phys. Med. Rehabil. 42, 570–573. doi: 10.3760/cma.j.issn.0254-1424.2020.06.021
Lu, Y., Liu, C., Liu, H., and Wang, W. (2022). The status quo and influencing factors of social alienation in patients after aortic dissection surgery. Prac. J. Clin. Med. 19, 9–12. doi: 10.3969/j.issn.1672-6170.2022.05.003
Ma, C. L., Su, L., Xie, J. J., Long, J. X., Wu, P., and Gu, L. (2014). The prevalence and incidence of Parkinson's disease in China: a systematic review and meta-analysis. J. Neural Transm. 121, 123–134. doi: 10.1007/s00702-013-1092-z
Ma, Z., Gong, Z., Wen, W., Yao, R., Wang, C., and Su, C. (2020). A clinical study of high-frequency repetitive transcranial magnetic stimulation in patients with post-stroke attention deficit. Chin. Rehabil. 35, 175–178. doi: 10.3870/zgkf.2020.04.002
Murdoch, B. E., and Barwood, C. H. (2013). Non-invasive brain stimulation: a new frontier in the treatment of neurogenic speech-language disorders. Int. J. Speech Lang. Pathol. 15, 234–244. doi: 10.3109/17549507.2012.745605
Narayana, S., Franklin, C., Peterson, E., Hunter, E. J., Robin, D. A., Halpern, A., et al. (2022). Immediate and long-term effects of speech treatment targets and intensive dosage on Parkinson's disease dysphonia and the speech motor network: randomized controlled trial. Hum. Brain Mapp. 43, 2328–2347. doi: 10.1002/hbm.25790
Parkinson's Disease and Movement Disorders Group and Neurologist Branch of Chinese Medical Doctor Association (2020). Chinese Guidelines for the Treatment of Parkinson's Disease, 4th Edn. Chinese Journal of Neurology.
Qi, S., Yin, P., Wang, L., Qu, M., Kan, G. L., Zhang, H., et al. (2021). Prevalence of Parkinson's disease: a community-based study in China. Mov. Disord. 36, 2940–2944. doi: 10.1002/mds.28762
Schalling, E., Johansson, K., and Hartelius, L. (2017). Speech and communication changes reported by people with Parkinson's disease. Folia Phoniatr. Logop. 69, 131–141. doi: 10.1159/000479927
Shah-Basak, P. P., Wurzman, R., Purcell, J. B., Gervits, F., and Hamilton, R. (2016). Fields or flows? A comparative metaanalysis of transcranial magnetic and direct current stimulation to treat post-stroke aphasia. Restor. Neurol. Neurosci. 34, 537–558. doi: 10.3233/RNN-150616
Simon, D. K., Tanner, C. M., and Brundin, P. (2020). Parkinson disease epidemiology, pathology, genetics, and pathophysiology. Clin. Geriatr. Med. 36, 1–12. doi: 10.1016/j.cger.2019.08.002
Steurer, H., Schalling, E., Franzén, E., and Albrecht, F. (2022). Characterization of mild and moderate dysarthria in Parkinson's disease: behavioral measures and neural correlates. Front. Aging Neurosci. 14:870998. doi: 10.3389/fnagi.2022.870998
Valero-Cabré, A., Amengual, J. L., Stengel, C., Pascual-Leone, A., and Coubard, O. A. (2017). Transcranial magnetic stimulation in basic and clinical neuroscience: a comprehensive review of fundamental principles and novel insights. Neurosci. Biobehav. Rev. 83, 381–404. doi: 10.1016/j.neubiorev.2017.10.006
Wang, F., Xu, X., Li, J., Liang, S., Huang, Y., and Li, X. (2022). Clinical observation of transcranial magnet stimulation combined with rehabilitation nursing for spastic dysarthria after acute cerebral infarction. Chin. Evid. Based Nurs. 8, 984–986. doi: 10.12102/j.issn.2095-8668.2022.07.026
Wang, K., Zou, L., Chen, J., Du, Y., and Qin, B. (2015). Research progress of repetitive transcranial magnetic stimulation in stroke rehabilitation therapy. China Rehabil. J. 30, 177–180. doi: 10.3870/zgkf.2015.03.005
Wang, R., Chen, X., Khalilian-Gourtani, A., Yu, L., Dugan, P., Friedman, D., et al. (2023). Distributed feedforward and feedback cortical processing supports human speech production. Proc. Natl. Acad. Sci. U.S.A. 120:e2300255120. doi: 10.1073/pnas.2300255120
Wang, X., Huang, Z., Qian, H., Yuan, H., and Liu, J. (2022a). Effects of high-frequency repetitive transcranial magnetic stimulation on bilateral M1 area combined with articulation training on hypokinetic dysarthria in patients with Parkinson's disease. Prac. Geriatr. 36, 508–511. doi: 10.3969/j.Issn.1003-9198.2022.05.019
Wang, X., Zhu, Q., Chen, Y., Qian, H., Yuan, H., and Zhao, G. (2022b). Effects of high-frequency repetitive transcranial magnetic stimulation combined with voice training on vocal function in patients with Parkinson's disease. Chin. J. Rehabil. 32, 155–161. doi: 10.3724/SP.J.1329.2022.02010
Zhang, Y., Chai, J., and Xu, B. (2022). Application and prospect of repetitive transcranial magnetic stimulation in Parkinson's disease. Int. Core J. Eng. 8, 547–553. doi: 10.6919/ICJE.202204_8(4).0066
Zhou, Z., and Dan, C. (2021). Research progress of acupuncture therapy combined with repetitive transcranial. magnetic stimulation therapy in stroke rehabilitation. China Rehabil. J. 36, 239–244. doi: 10.3870/zgkf.2021.04.011
Zhu, P., Zhong, Y., Xu, S., and Shan, C. (2019). Mechanisms of action of different paradigms of repetitive transcranial magnetic stimulation and progress in improving motor function after stroke. China Rehabil. J. 34, 605–660. doi: 10.3870/zgkf.2019.11.012
Keywords: Parkinson's disease, dysarthria, repetitive transcranial magnetic stimulation, efficacy, systematic review
Citation: Chen K, Zhou S, Lu S, Qin Y, Li X, Li Y, Liu T, Zhang M, Xu K, Shi H, Lv X, Yuan K, Shi H and Qin D (2025) A systematic review of the efficacy of repetitive transcranial magnetic stimulation in treating dysarthria in patients with Parkinson's disease. Front. Aging Neurosci. 17:1501640. doi: 10.3389/fnagi.2025.1501640
Received: 25 September 2024; Accepted: 15 January 2025;
Published: 05 February 2025.
Edited by:
Xudong Zhao, Institute of Biophysics Chinese Academy of Sciences, ChinaReviewed by:
Dhiraj Kumar, National Eye Institute (NIH), United StatesCopyright © 2025 Chen, Zhou, Lu, Qin, Li, Li, Liu, Zhang, Xu, Shi, Lv, Yuan, Shi and Qin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kai Yuan, MTkwODc2MDcyQHFxLmNvbQ==; Hongling Shi, a21zaGwxQDEyNi5jb20=; Dongdong Qin, cWluZG9uZzEwOEAxNjMuY29t
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.