 Angel Toval1*
Angel Toval1* Patricio Solis-Urra1,2
Patricio Solis-Urra1,2 Esmée A. Bakker1,3
Esmée A. Bakker1,3 Lucía Sánchez-Aranda1
Lucía Sánchez-Aranda1 Javier Fernández-Ortega1Carlos Prieto1Rosa María Alonso-Cuenca1,4
Javier Fernández-Ortega1Carlos Prieto1Rosa María Alonso-Cuenca1,4 Alberto González-García5Isabel Martín-Fuentes1
Alberto González-García5Isabel Martín-Fuentes1 Beatriz Fernandez-Gamez1
Beatriz Fernandez-Gamez1 Marcos Olvera-Rojas1
Marcos Olvera-Rojas1 Andrea Coca-Pulido1Darío Bellón1
Andrea Coca-Pulido1Darío Bellón1 Alessandro Sclafani1Javier Sanchez-Martinez1Ricardo Rivera-López6Norberto Herrera-Gómez1,4Rafael Peñafiel-Burkhardt6Víctor López-Espinosa6Sara Corpas-Pérez4María Belén García-Ortega6Alejandro Vega-Cordoba6
Alessandro Sclafani1Javier Sanchez-Martinez1Ricardo Rivera-López6Norberto Herrera-Gómez1,4Rafael Peñafiel-Burkhardt6Víctor López-Espinosa6Sara Corpas-Pérez4María Belén García-Ortega6Alejandro Vega-Cordoba6 Emilio J. Barranco-Moreno1
Emilio J. Barranco-Moreno1 Francisco J. Morales-Navarro1Raúl Nieves1Alfredo Caro-Rus1
Francisco J. Morales-Navarro1Raúl Nieves1Alfredo Caro-Rus1 Francisco J. Amaro-Gahete7,8,9
Francisco J. Amaro-Gahete7,8,9 Jose Mora-Gonzalez1Sol Vidal-Almela1Anna Carlén1,10
Jose Mora-Gonzalez1Sol Vidal-Almela1Anna Carlén1,10 Jairo H. Migueles1Kirk I. Erickson11Eduardo Moreno-Escobar4,9
Jairo H. Migueles1Kirk I. Erickson11Eduardo Moreno-Escobar4,9 Rocío García-Orta6,9
Rocío García-Orta6,9 Irene Esteban-Cornejo1,8,9
Irene Esteban-Cornejo1,8,9 Francisco B. Ortega1,8,12*
Francisco B. Ortega1,8,12*- 1Department of Physical and Sports Education, Sport and Health University Research Institute (iMUDS), Faculty of Sport Sciences, University of Granada, Granada, Spain
- 2Faculty of Education and Social Sciences, University Andres Bello, Viña del Mar, Chile
- 3Department of Primary and Community Care, Radboud University Medical Center, Nijmegen, Netherlands
- 4Cardiology Service, San Cecilio Clinical University Hospital, Granada, Spain
- 5Department of Nursing, Faculty of Health Sciences, University of Granada, Granada, Spain
- 6Cardiology Service, Virgen de Las Nieves University Hospital, Granada, Spain
- 7Department of Physiology, Faculty of Medicine, University of Granada, Granada, Spain
- 8CIBER de Fisiopatología de la Obesidad y Nutrición (CIBEROBN), Instituto de Salud Carlos III, Granada, Spain
- 9Instituto de Investigación Biosanitaria ibs.GRANADA, Granada, Spain
- 10Department of Clinical Physiology in Linköping, and Department of Health, Medicine and Caring Sciences, Linköping University, Linköping, Sweden
- 11AdventHealth Research Institute, Neuroscience, Orlando, FL, United States
- 12Faculty of Sport and Health Sciences, University of Jyväskylä, Jyväskylä, Finland
Introduction: Patients with coronary artery disease (CAD) have a higher risk of developing cognitive impairment and mental health disorders compared to the general population. Physical exercise might improve their brain health. The overall goal of the HEART-BRAIN randomized controlled trial (RCT) is to investigate the effects of different types of exercise on brain health outcomes in patients with CAD, and the underlying mechanisms.
Methods: This three-arm, single-blinded RCT will include 90 patients with CAD (50–75 years). Participants will be randomized into: (1) control group—usual care (n = 30), (2) aerobic high-intensity interval training (HIIT) (n = 30), or (3) HIIT combined with resistance exercise training (n = 30). The 12-week intervention includes 3 supervised sessions (45-min each) per week for the exercise groups. Outcomes will be assessed at baseline and post-intervention. The primary outcome is to determine changes in cerebral blood flow assessed by magnetic resonance imaging. Secondary outcomes include changes in brain vascularization, cognitive measures (i.e., general cognition, executive function and episodic memory), and cardiorespiratory fitness. Additional health-related outcomes, and several potential mediators and moderators will be investigated (i.e., brain structure and function, cardiovascular and brain-based biomarkers, hemodynamics, physical function, body composition, mental health, and lifestyle behavior).
Conclusion: The HEART-BRAIN RCT will provide novel insights on how exercise can impact brain health in patients with CAD and the potential mechanisms explaining the heart-brain connection, such as changes in cerebral blood flow. The results may have important clinical implications by increasing the evidence on the effectiveness of exercise-based strategies to delay cognitive decline in this high-risk population.
Clinical trial registration:
1 Introduction
More than 300 million people globally are currently living with coronary artery disease (CAD), also called coronary heart disease (Stark et al., 2024), which consists of a narrowing or blockage of the coronary arteries mainly caused by atherosclerosis. CAD is the most prevalent cardiovascular disease and a leading cause of mortality and morbidity worldwide (Malakar et al., 2019; WHO, 2021; Timmis et al., 2022; Tsao et al., 2023; Stark et al., 2024). In turn, CAD incurs a significant economic burden, with annual costs estimated at €77 billion in the EU and $239.9 billion in the USA (Luengo-Fernandez et al., 2023; Tsao et al., 2023). Recent studies have shown that individuals with CAD are at high risk of accelerated decline in cognitive and mental health compared to aged-matched adults without CAD, supporting a nexus between the heart and the brain (Tully et al., 2014; van Buchem et al., 2014; Roger, 2017; Vaccarino et al., 2020; Schievink et al., 2022). Indeed, the cardiovascular risk factors associated with CAD similarly predispose individuals to cerebrovascular disease, in turn affecting their cerebral perfusion. While pharmaceutical therapies have traditionally been the cornerstone of CAD treatment, exercise is an effective non-pharmaceutical intervention for improving cardiometabolic health in these patients (Sandercock et al., 2013; Pelliccia et al., 2021; Dibben et al., 2023; Virani et al., 2023). However, the potential effect of exercise on brain health among individuals with CAD, as well as the mechanisms underlying the heart-brain connection, remain unknown.
A key physiological mechanism modulating the heart-brain connection might involve the intricate machinery responsible for supplying blood to the brain. Chronic cerebral hypoperfusion, marked by reduced cerebral blood flow (CBF), limits the brain’s access to vital oxygen and nutrients (Daulatzai, 2017; Roger, 2017; Han et al., 2019; Long and Holtzman, 2019). Therefore, a disrupted CBF could play an important role in accelerating cognitive decline and increasing the risk of dementia and mental health disorders in patients with CAD. In turn, exercise could serve as a pivotal factor to enhance CBF, offering a promising non-pharmaceutical adjunct therapy. Limited evidence suggests that exercise may increase CBF and induce brain angiogenesis (i.e., growth of new capillaries). However, these findings are mainly derived from observational and animal studies (Rogers et al., 1990; Swain et al., 2003). These hypotheses need to be tested in randomized controlled trials (RCTs) in humans. The most advanced neuroimaging techniques (particularly in magnetic resonance imaging, MRI) allow non-invasive (no contrast) methods to assess in vivo CBF using the Arterial Spin Labelled sequence (ASL-MRI) and cerebral vascularization using magnetic resonance angiography (MRA) (Suzuki et al., 2018). These state-of-the-art techniques can provide novel information about the connection of these two possible mechanisms (i.e., changes in CBF and cerebral vascularization) with cognition and mental health.
Physical exercise is strongly recommended in the clinical management of patients with CAD to reduce disease progression and the risk of major cardiovascular events (Taylor et al., 2004; Dibben et al., 2023). Yet, the mechanisms by which different types of exercise induce a variety of physiological responses are still not fully understood. For instance, modalities such as aerobic high-intensity interval training (will be referred to as HIIT from here on) or its combination with resistance training are understudied. HIIT may offer superior health benefits, such as larger improvements in cardiorespiratory fitness, compared to moderate intensity continuous training (MICT) in patients with CAD (Tully et al., 2014; van Buchem et al., 2014; Roger, 2017; Schievink et al., 2022). However, it is unknown if HIIT is also superior for improving brain health outcomes. On the other hand, resistance training and the combination of aerobic and resistance training remain understudied, despite recommendations by the World Health Organization (WHO) (Bull et al., 2020) and the European and American clinical guidelines for CAD management (Pelliccia et al., 2021; Byrne et al., 2023; Virani et al., 2023), all advocating for the combination of aerobic and resistance training for optimal health benefits. Since one of the most documented benefits of exercise is the improvement in cardiorespiratory fitness (Ross et al., 2016; Committee PAGA, 2018; Lang et al., 2024), and this marker has been consistently linked to better brain health outcomes (Smith et al., 2021; Maleki et al., 2022), cardiorespiratory fitness might serve as a potential mediator of the beneficial effects of exercise on the HEART-BRAIN outcomes.
Based on the existing research gaps, we have designed the HEART-BRAIN project, an RCT to investigate the effects of exercise training on brain health outcomes in patients with CAD, including the underlying mechanisms of the heart-brain connection. Herein, we describe the rationale and methodology of the HEART-BRAIN RCT.
1.1 Study objectives
The overall objective of the HEART-BRAIN trial is to investigate the effects of exercise on brain health outcomes in patients with CAD.
The primary objective of the study is to investigate the effects of HIIT and HIIT plus resistance training compared to usual care (i.e., no exercise intervention) on global and regional CBF in individuals with CAD.
Secondary objectives: to determine the effects of HIIT, and HIIT plus resistance training compared to usual care on (i) cerebral vascularization, (ii) cognitive measures (i.e., general cognition, executive function and episodic memory), and (iii) cardiorespiratory fitness. Additionally, we will investigate the role of potential moderators and mediators (see details in statistical analysis section) on the expected effects.
Tertiary objectives: to determine the effects of HIIT, and HIIT plus resistance training, compared to usual care on additional outcomes related to cardiovascular and brain health, such as brain structure and function, inflammatory, biomarkers in blood, saliva and fecal samples, cardiac, vascular and transcranial non-invasive hemodynamics, physical function, body composition, mental health and lifestyle behavior.
Our primary hypothesis is that both exercise groups will have a greater increase in CBF compared to the usual care control group, in which HIIT plus resistance training might have a larger effect size than HIIT alone.
2 Methods and analysis
2.1 Design and ethics
The HEART-BRAIN trial is a single-centered, three-armed, single-blinded RCT, in which 90 adults with CAD, will be (Figure 1) randomized into: (1) HIIT exercise program (n = 30), (2) HIIT plus resistance training exercise program (n = 30), hand (3) control group—usual care (n = 30). The group receiving usual care will be treated as standard care in Spain, which includes periodic medical revisions and medication control. The two exercise groups will undertake a 12-week supervised exercise program. All the study outcomes will be assessed at baseline and during the 12-week follow-up. Lifestyle behaviors will also be evaluated at mid-point (6 weeks).
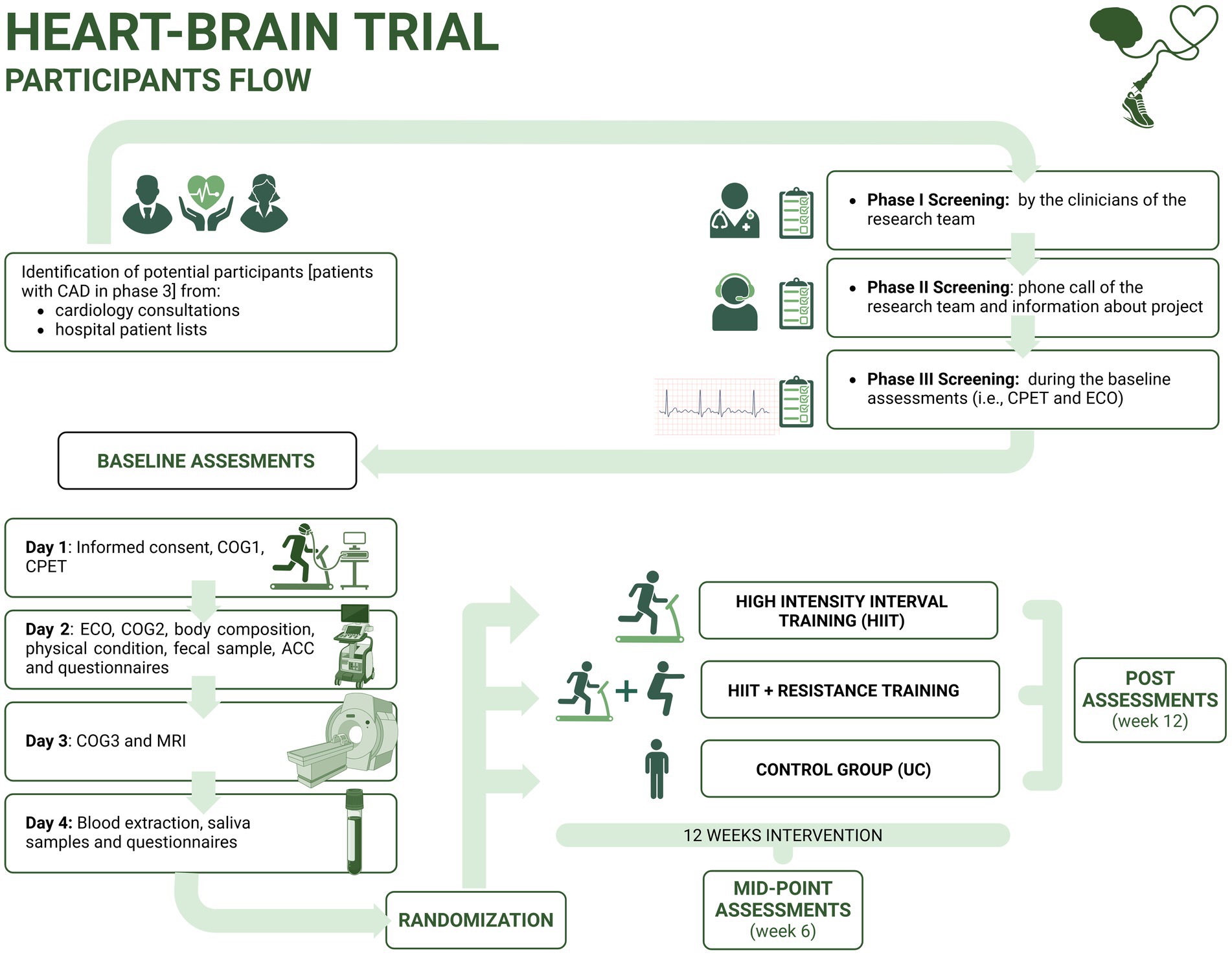
Figure 1. Visual representation of the study design in the HEART-BRAIN trial. ACC, Accelerometry; CAD, coronary artery disease; CPET, cardiopulmonary exercise test; ECO, echography; COG, cognitive function tests; MRI, magnetic resonance imaging; UC, usual care. *Post-intervention assessment includes similar outcomes compared to baseline assessment.
Eligible participants will receive written information about the study objectives and design, and will provide informed consent before participation. The trial protocol is in accordance with the principles of the Declaration of Helsinki and was approved by the Research Ethics Board of the Andalusian Health Service (CEIM/CEI Provincial de Granada; #1776-N-21 on December 21st, 2021). The RCT is registered on Clinicaltrials.gov (NCT06214624; submission date: December 22nd, 2023) and the study protocol and statistical analysis plan were uploaded before the last participants were randomized (submission date: January 29th, 2024). The study has been designed following the Standard Protocol Items for Randomized Interventional Trials (SPIRIT) (Chan et al., 2013a,b) and the SPIRIT-Outcomes 2022 Extension (Butcher et al., 2022) (Supplementary Table S1). Any significant changes to the protocol will be reported to the trial registry and the Research Ethics Board, which is in line with the SPIRIT guidelines. Moreover, participants in the HEART-BRAIN trial are insured under a social responsibility policy from the University of Granada, which covers ancillary services, post-trial care or compensation if necessary. There are no financial rewards provided to participants for their involvement in the study.
2.2 Recruitment and screening
Participants with CAD will be recruited from two public hospitals in Granada, Spain: the “Hospital Universitario Virgen de las Nieves” and the “Hospital Universitario Clínico San Cecilio.” Recruitment started in May 2022, and we plan to enroll a minimum of 90 patients, aged 50–75, including both sexes, with stable CAD (phase III) proven by invasive coronary angiography or CT with at least one coronary stenosis with ≥50% luminal reduction. Initial screening will be based on the clinical history of the patient (i.e., we will not perform invasive coronary angiography or CT as part of this study). A complete list of eligibility criteria is presented in Table 1. Eligible patients will be screened by the clinical and research team in three steps (Figure 1): (1) screening by the clinicians of the research team (i.e., based on clinical history); (2) screening based on a phone call conducted by the research team; and (3) screening during the baseline assessments including the cardiopulmonary exercise test (CPET) and echocardiography. Participants will be recruited in waves of 10 to 20 people throughout the year. In accordance with the CONSORT flow diagram (Schulz et al., 2010), we will note the number of patients assessed for eligibility by the clinical and research team, the number of excluded patients (indicating reason for exclusion) during the enrollment phase and the number of randomized participants. For the allocation, the number of participants allocated to the intervention groups and the number of participants who received the intervention (with reasons for nonadherence to the allocated arm) will be noted. The number of participants who were lost to follow-up (dropouts) and who discontinued the intervention (including reasons) will be reported. Finally, the number of participants that were included in the analyses using the intention-to-treat and per-protocol databases will be described together with the reasons for the exclusion from the analytic database.
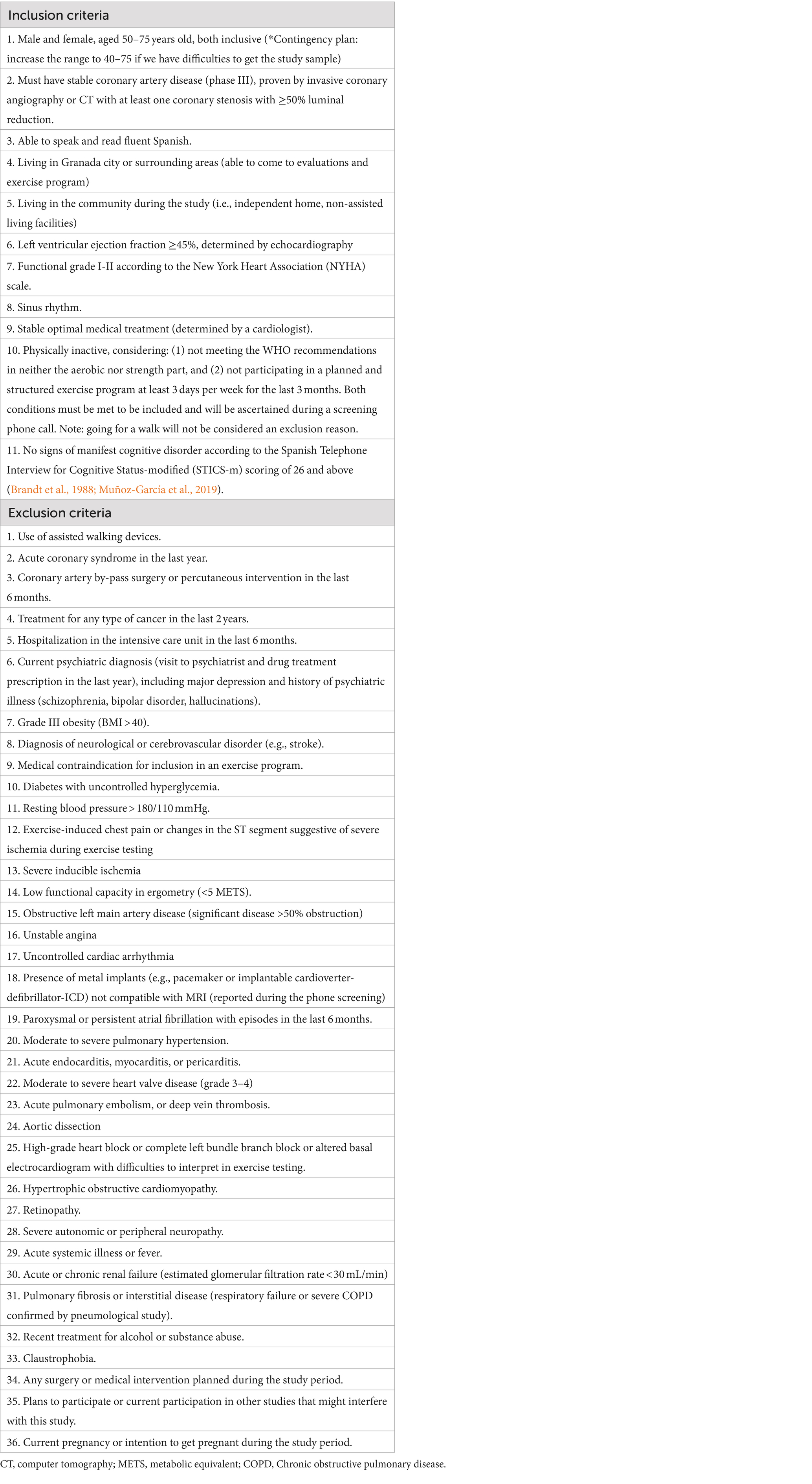
Table 1. HEART-BRAIN inclusion and exclusion criteria for selecting participants.
2.3 Randomization
Randomization will occur on a rolling basis and only after the completion of all baseline assessments, through REDCap Software (Harris et al., 2019). Participants will be randomized using a 1:1:1 ratio and stratified by age (<65 years or ≥ 65 years) and sex (female or male). To ensure adequate allocation concealment, this procedure will be carried out by a blinded external researcher (Dr. Cabanas-Sanchez, Autonomous University of Madrid, Spain).
2.4 Blinding
Participants cannot be blinded due to the nature of the interventions, as they will inevitably become aware of their group allocation. Nonetheless, the principal investigator (PI) and the research team members participating in the post-intervention evaluations (who are not involved in monitoring the exercise sessions) will be blinded to the group assignments. Unblinding will only occur in case of an unexpected adverse event involving a participant and will only be done by the PI or a physician.
2.5 Interventions
A detailed and broader description of the program will be further extended in the Consensus on Exercise Reporting Template (CERT) study protocol of the HEART-BRAIN trial (manuscript in preparation). Briefly, participants will be randomized to one of the following three groups.
HIIT: 12-week duration, 3 times/week. This consists of a 4×4 HIIT (preferably on a treadmill, other exercise ergometers, e.g., cross-trainer cycle or cycle ergometer, will be available for participants with injuries or walking limitations will be available for participants with injuries or walking limitations): 4 intervals of 4 min at high intensity (85–95% of HRmax), interspersed with 3 intervals of 3 min of active resting at ~70% of HRmax. All sessions include 10 min of warm-up and 10 min of cool-down, resulting in a total session time of 45 min. During the familiarization period (first two weeks), participants will progress from moderate-intensity training to the target HIIT. Training intensity of the 2-week familiarization will be individualized according to the initial status of the participant to adapt to the type of exercise as well as identify the different intensity zones. The duration will be similar to the main part of the intervention.
HIIT plus resistance training: 12-week duration, 3 times/week. The aerobic part consists of a 3×4 HIIT (preferably on treadmill), with 3 intervals of 4 min at high intensity (85–95% of HRmax), interspersed with 2 intervals of 3 min of active resting (~70% of HRmax). The resistance part consists of 2 rounds of an 8-exercise circuit (a combination of upper and lower body exercises using elastic bands and body weight) with a ratio of 20 s of effort followed by 40 s of resting. Sessions will have 5 min of warm-up on the treadmill and 5 min of cool-down walking around the gym, for a total session time of 45 min.
Control group – usual care: The control group will be treated as usual in outpatient Phase III, which in Spain includes periodic medical revisions where the clinician may provide patients with lifestyle and clinical advice (e.g., inform about exercise limitations, if any, and nutrition recommendations, stress management) and medication control. In addition, in the control group, we will apply the wait-list strategy, offering participants the HIIT supervised program described above, once data collection for pre-and post-intervention assessments is completed.
All intervention groups will receive the same usual care. The HIIT program and the HIIT part of the combined HIIT plus resistance training program have been designed based on the guidelines for the delivery and monitoring of HIIT in clinical populations (Taylor et al., 2019) and meet the aerobic recommendations of the WHO guidelines, as it surpasses the minimum of 75 min of vigorous intensity or 150 min of moderate intensity per week, or a combination of them (Bull et al., 2020). The combined HIIT plus resistance training program meets the aerobic and resistance components of the WHO recommendations, as it has 3 sessions of resistance training per week while WHO guidelines recommend at least 2 sessions involving major muscle groups. Both exercise programs have been designed to provide an estimated isocaloric workload (same energy expenditure) in terms of intensity and duration. The isoenergetic calculations of the training programs were based on the metabolic equivalents of tasks (METs) for exercise prescription as defined by the compendium of the American College of Sports Medicine (Ainsworth et al., 2011; Bayles, 2023).
Exercise programs will take place in the Sport and Health University Research Institute (iMUDS) at the University of Granada. Accredited expert trainers with a BSc degree in sports sciences will lead all supervised sessions with a ratio of 1:1 (one trainer, one participant). Exceptionally (e.g., scheduling conflicts), a ratio of 1:2 will be used.
Both training programs are individually tailored. Exercise prescription, monitoring, and decisions for progression will be based on the percentage of HRmax and the 10-point Borg Rating of Perceived Exertion scale (RPE) (Morishita et al., 2019). HRmax will be determined during the CPET with electrocardiogram (ECG) and gas exchange analyzer performed at baseline (see Section 2.3.2). Furthermore, symptoms and blood pressure will be monitored before, during, and after the exercise sessions. Participants taking beta-blocker medications often have a blunted HR response (Taylor et al., 2019), which could also affect the HRmax obtained in the CEPT. Thus, while the HRmax will be used as a reference for exercise intensity, participants will be encouraged to learn and use RPE. This indicator will be used as a reference in case of discordance between HR and RPE targets. In addition, the trainers will use their judgment to adapt the intensity, particularly during the resistance training, because RPE might be less reliable in inexperienced participants (Taylor et al., 2019).
2.6 Adherence, attendance, and compliance
Since the term adherence has been used with different meanings in the literature, in our study we will refer to two concepts more unequivocally used: attendance and compliance. Attendance will be defined as the percentage of sessions attended by the participant (recorded by the trainers) divided by the number of exercise sessions offered (12 weeks × 3 sessions/week = 36, yet holidays and logistic reasons may lead to slight deviations among waves and participants). Compliance will be defined as the percentage of sessions in which the specified amount of time (i.e., HIIT 6.5 min and HIIT plus resistance training 4.5 min) is spent within the target HR intensity, divided by the number of exercise sessions with valid data (e.g., sessions with technical issues of the HR bands will be excluded). The familiarization phase (i.e., the first two weeks of the exercise intervention) will not be considered for the compliance calculation. The amount of time, i.e., HIIT 6.5 min; HIIT plus resistance training 4.5 min, in the target HR intensity is based on the exercise protocol and the guidelines for HIIT prescription and monitoring in clinical populations (Taylor et al., 2019): “for the first high-intensity interval, allow the entire 4-min period to reach the HR target zone, for subsequent high intensity intervals (i.e., 2nd, 3rd, and/or 4th), allow 2-min (halfway) to reach the HR target zone.”
All protocol deviations will be recorded and reported (e.g., change in pre-defined inclusion/exclusion criteria, baseline and post assessments, data cleaning/processing).
2.7 Safety and adverse events
Although HIIT has been shown to be low risk in patients with CAD (Rognmo et al., 2012; Wewege et al., 2018; Taylor et al., 2020), the safety of our participants is the highest priority in the study. For these purposes, we followed the guidelines for using HIIT in clinical populations and have applied in our study the recommended exclusion criteria (Taylor et al., 2019). Further, CPET together with cardiac and vascular ultrasound will be performed at baseline and serve as a clinical assessment to confirm the absence of underlying conditions that contraindicate exercise.
The center where the exercise training sessions will be delivered (iMUDS) is located in the Hospital area next to the emergency unit (200 meters) and the ambulance unit (600 meters). A trained allied health professional (nurse or physician) will be present in the center during the training sessions to guarantee a timely response in case of an adverse event. The center has a fully equipped trolley with a first aid kit and automatic defibrillator and obtained the Andalusian Certification of “Cardioprotected Center” (Decreto 22/2012 of February 14th). Furthermore, all members of the project team will receive certified training courses in cardiopulmonary resuscitation and the use of a semi-automatic defibrillator.
In case of an adverse event, we will follow the protocol recommended by the Spanish Council of Cardiopulmonary Resuscitation (CERCP). The number and reasons for adverse events (e.g., falls, injuries, musculoskeletal problems, major cardiovascular events, and any other events potentially related to the implementation of the trial protocol) occurring at any time during the study will be collected, reported, and separately described for each study arm. The participants allocated to the exercise group will be able to communicate any adverse events during their regular contact with the project team (i.e., 3 sessions/week), whereas those allocated to usual care will be asked to report any adverse event promptly, and will be called by phone for these regards at weeks 3, 9 and 12. Adverse events will be described in a table in the main HEART-BRAIN manuscript. Each adverse event will be clinically ascertained to judge whether the event was due to exercise in the corresponding study arm using an adverse event algorithm (i.e., Liverpool Causality Assessment Tool) (Gallagher et al., 2011) and recorded according to the Common Terminology Criteria for Adverse Events, (CTCAE) (Shah, 2022) by an experienced cardiologist (EME) after discussion and consensus with the rest of the cardiologists involved in the project.
2.8 Outcomes
The primary, secondary, and additional outcomes, the assessment instruments, and the data collection time points are summarized in Table 2. All outcome-related measures, data processing, and statistical analyses will be performed by staff blinded to the intervention assignment.
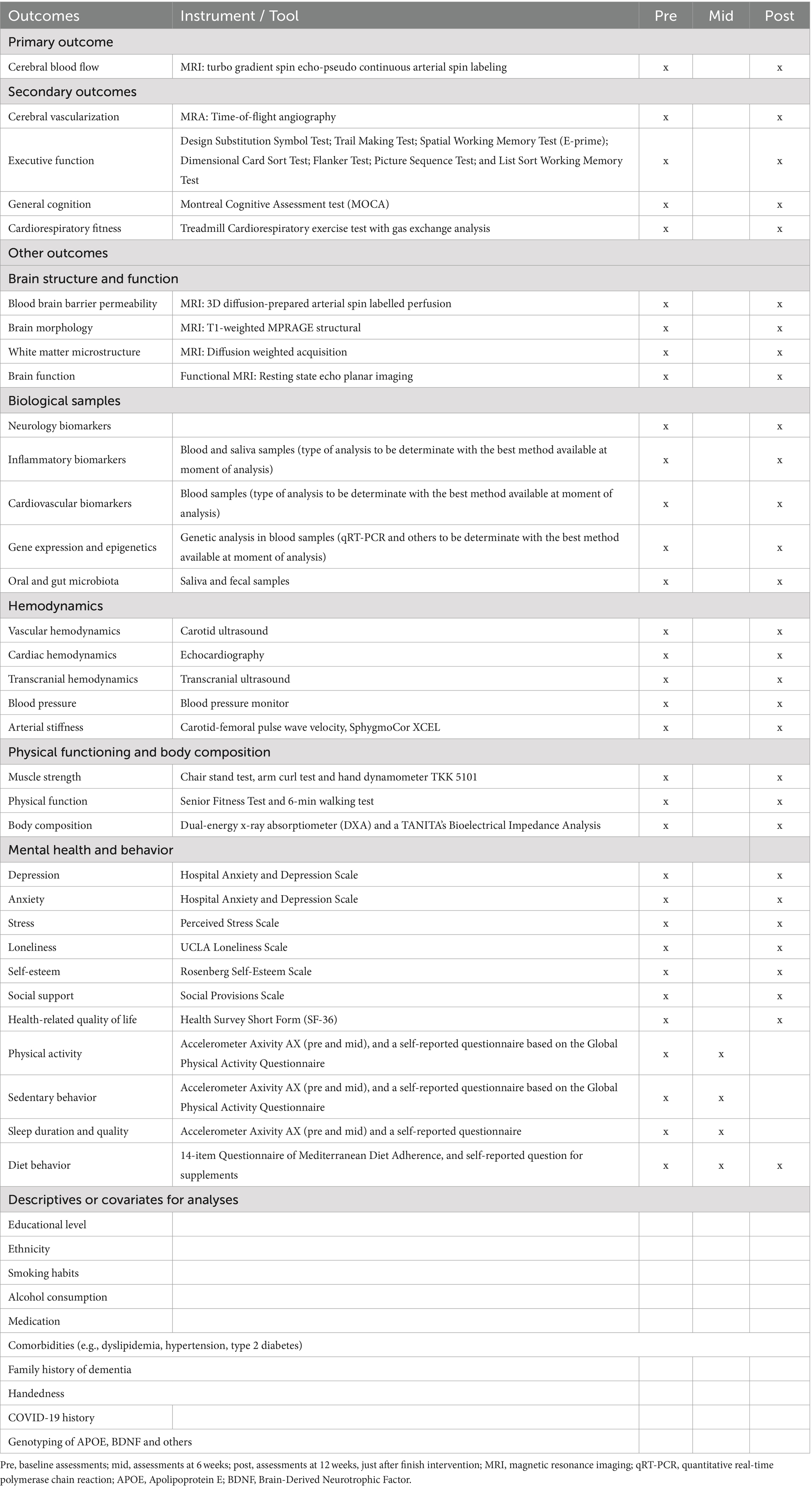
Table 2. Outcomes instruments and time points of data collection.
2.8.1 Primary outcome measures
Change in cerebral blood flow (timepoint: baseline and 12-weeks): CBF (mL/100 g/min) will be measured using the MRI technique of pseudo-continuous arterial spin labeling (pCASL) (Wang et al., 2013; Kilroy et al., 2014). We will analyze both global and regional CBF, as determined by voxel-wise analysis to measure local perfusion (acquisition parameters in Table 3).
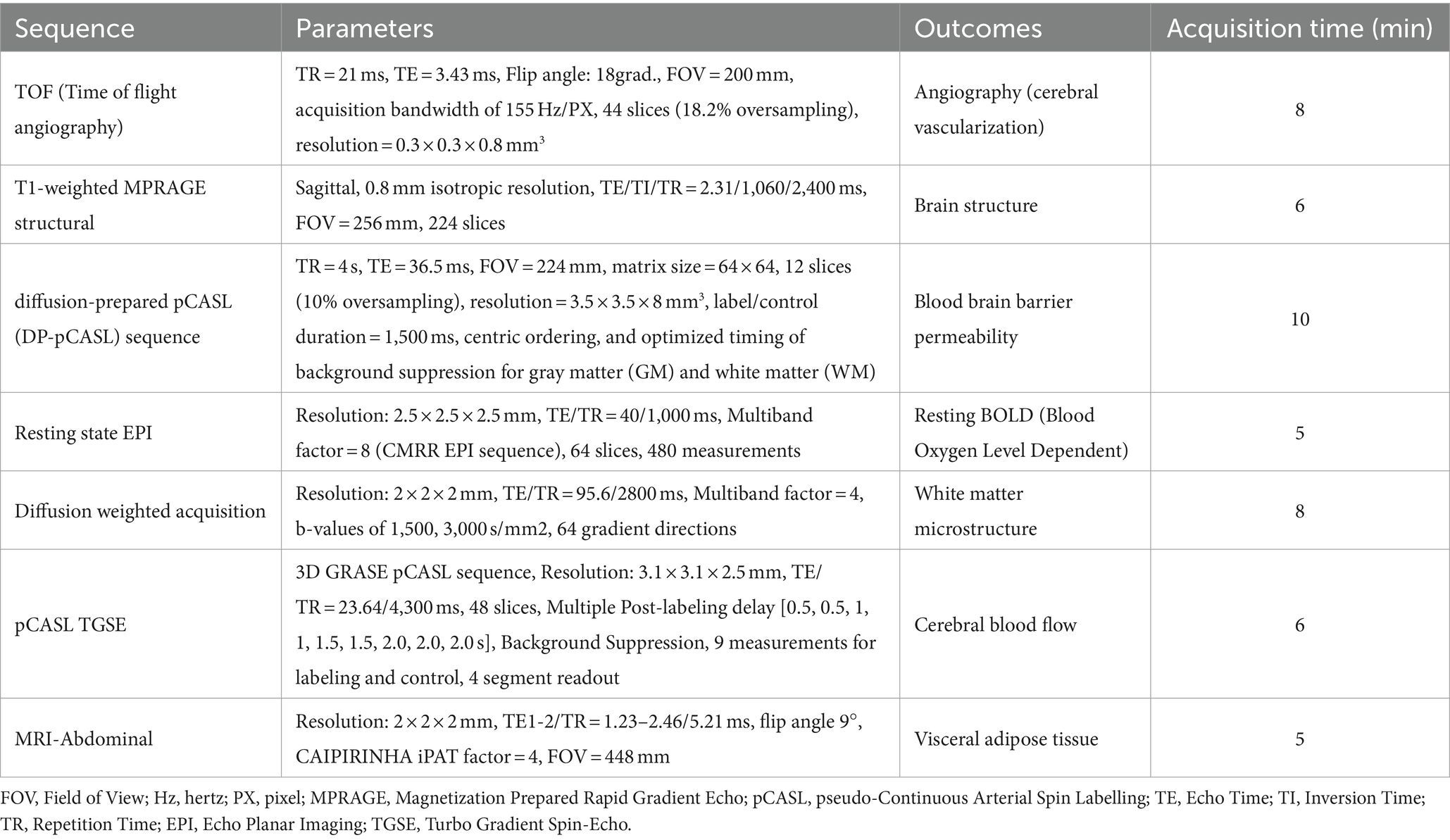
Table 3. Brain magnetic resonance imaging (MRI) parameters of the HEART-BRAIN trial.
2.8.2 Secondary outcome measures
Change in cerebral vascularization (baseline to 12 weeks): Cerebral vascularization will be measured using the time-of-flight-magnetic resonance angiography (TOF-MRA). This sequence allows imaging flow within vessels revealing the cerebrovascular anatomy without the need to administer contrast. Thus, the analysis of TOF-MRA provides the number, distribution, and morphology of intracranial vessels (acquisition parameters in Table 3).
Change in cognitive outcomes (baseline to 12 weeks): A comprehensive neuropsychological battery will assess several domains of cognition (Table 4). General cognition will be assessed by the Montreal Cognitive Assessment (MoCA) test (Ojeda et al., 2016). Additionally, the battery includes paper-and-pencil tests [Trail making test (Reitan, 1958) and Digit Symbol Substitution Test (Wechsler, 2008)], National Institutes of Health (NIH) Toolbox tests (Dimensional Change Card Sort Test, Flanker Test, Picture Sequence Memory Test, and List Sort Working Memory Test) (Zelazo et al., 2013) and a programmed test in E-prime software (Spatial Working Memory Test) (Erickson et al., 2011). Detailed information about the cognitive tests has been previously described (Solis-Urra et al., 2023). The cognitive indicators will be transformed into standardized z-scores by calculating the difference between each individual raw score and the group average score at baseline, and then dividing by the standard deviation at baseline. We will determine the effects of the interventions on the cognitive outcomes (e.g., general cognition, cognitive flexibility, inhibition control, working memory, processing speed and episodic memory). To guarantee reliable evaluations, all paper-and-pencil tests will be independently scored by two trained evaluators, with any discrepancies resolved through mutual agreement.
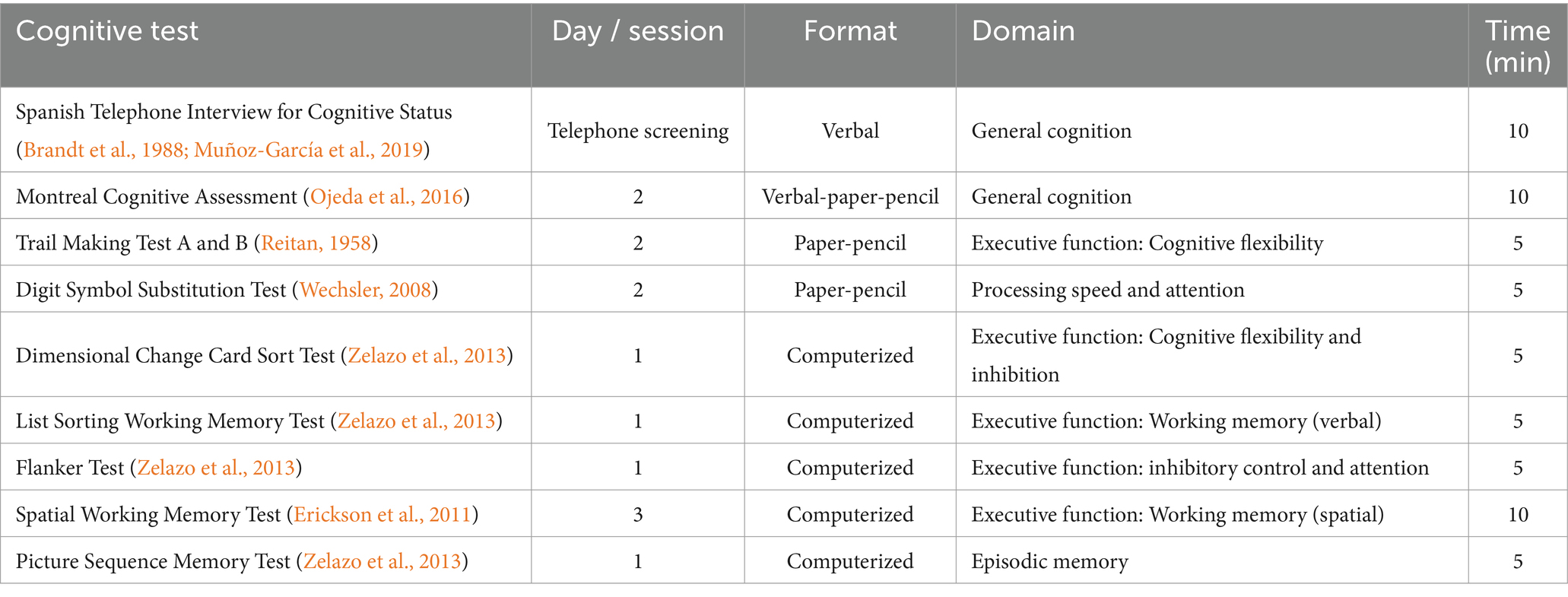
Table 4. Cognitive tests included in the HEART-BRAIN trial.
Change in cardiorespiratory fitness (baseline to 12 weeks): Cardiorespiratory fitness will be assessed by a standardized ramp CPET to exhaustion on a treadmill (h/p/cosmos, Nussdorf, Germany), in accordance with the American College of Sports Medicine Guidelines (Bayles, 2023). We decided to use a ramp protocol with small increments, and opted for a standardized, instead of individualized, protocol to be able to compare the time-to-exhaustion (test duration, excluding warm-up) between participants as an additional indicator of exercise capacity and cardiorespiratory fitness, in addition to the peak oxygen uptake. CPET will be carried out by trained staff and under the supervision of a physician. The protocol begins with a 3-min warm-up phase, during which the speed gradually increases to 4.8 km/h. Following this, the slope will be increased by 1% every 30 s until exhaustion or any other indication for test cessation (Bayles, 2023), followed by a 3-min recovery phase. This ramp protocol equates the 3-min increment Bruce tests, as indicated in the American College of Sports Medicine Guidelines (Bayles, 2023). The respiratory exchange will be monitored with a dilution flow system (Omincal, Maastricht Instruments, Maastricht, Netherlands), generating output data at 5-s intervals. A 12-lead electrocardiogram (AMEDTEC ECGpro, GmbH, Aue, Germany) will be continuously monitored by a physician during the test. Heart rate will also be registered with a Polar H10 monitor (including chest band and watch). Systolic and diastolic blood pressures will be measured with an automatic sphygmomanometer (Tango M2; SunTech Medical Inc., NC, United States) every 3 min during exercise, and after 3 and 5 min of recovery. The RPE will be asked every 3 min during the test (Mezzani et al., 2012). Peak oxygen uptake (Peak V̇O2) will be defined as the highest rolling 30-s average during the test. Since the heart rate response might be blunted due to beta-blockers and the oxygen uptake plateau is not always observed, staff will note whether participants reach a respiratory exchange ratio (RER) of 1.1 or higher, as RER is one of the most robust indicators of maximal effort in these patients.
2.8.3 Other outcome measures
2.8.3.1 Brain structure and function
CBF (primary outcome), cerebral vascularization (secondary outcome), along with other brain structure and function outcomes will be assessed by MRI at the Mind, Brain and Behavior Research Centre (CIMCYC) at the University of Granada. A Siemens Magnetom PRISMA Fit 3 T scanner with a 64-channel head coil will be used. Table 3 shows the imaging sequences that will be performed for each participant in acquisition order. Participants will be asked to wear comfortable clothing, MRI eligibility criteria will be checked (e.g., not having metallic implants or claustrophobia), and participants will provide additional informed consent specifically for MRI scans. When doubts exist about the compatibility of certain implants, an experienced radiologist will check the composition and material of the implant and inform about the compatibility with MRI before the scanning takes place. Standard MRI sequences will be conducted for approximately 60 min. A radiologist will review structural sequences to detect any incidental findings. If any of them are discovered, the radiologist will communicate with the participant for further examination. Besides CBF and cerebral vascularization, the following brain MRI outcomes will be examined (acquisition parameters are shown in Table 3):
Change in blood–brain barrier (BBB) permeability (baseline and 12 weeks): BBB permeability will be assessed by a recently developed neuroimaging technique that measures water exchange across the BBB using 3D diffusion-prepared arterial spin-labelled perfusion MRI (Shao et al., 2019).
Change in brain morphology (baseline and 12 weeks): MRI will measure brain morphology including volume, area, cortical thickness, and shapes by a T1-weighted MPRAGE (Magnetization Prepared Rapid Gradient Echo) structural sequence.
Change in white matter microstructure (baseline and 12 weeks): MRI will measure white matter microstructure by a diffusion-weighted acquisition sequence.
Change in brain function (baseline and 12 weeks): MRI will measure brain function during resting state and measures of brain activity and connectivity will be calculated.
2.8.3.2 Biological samples
The HEART-BRAIN trial aims to examine various biomarkers by the analysis of blood, saliva, and fecal samples. A trained nurse will collect blood samples from participants under fasting conditions (08:00 to 10:00 a.m.) at the Virgen de las Nieves University Hospital. For post-assessments, blood extraction will be done within the first 3–5 days after the last training session. Briefly, three ethylenediaminetetraacetic acid (EDTA) tubes, two citrate tubes, two serum tubes, and one PAXGENE tube will be collected corresponding to a total of approximately 30 mL of blood per participant visit. Part of the blood samples obtained from each participant will be processed directly at the Hospital (1 EDTA, 1 citrate, and 1 serum tube), and the remaining samples will be aliquoted and stored at −80°C for later studies. For future DNA analyses we will use the whole-blood sample in a EDTA tube, centrifugated at 2,000×g for 10 min, extract the plasma and finally extract the buffy coat that will be stored at −80°C. Saliva samples will be collected into sterilized plastic containers and aliquoted into 1.5 mL Eppendorf, and stored at −80°C for future analysis (yet to be determined). Standardized procedures will be used to maximize the stability of the saliva samples (Ostheim et al., 2020; Bahbah et al., 2021; Dongiovanni et al., 2023; Kumari et al., 2023). Fecal samples will also be collected under standardized conditions using sterile plastic containers and stored at −80°C. Table 5 outlines the specifications of the samples, initial analyses, and preliminary analysis plans. Nevertheless, samples will be analyzed using the best available methods at the time of processing. Blood analyses will cover conventional biochemical measurements, cardiovascular, brain-peripheral, and inflammatory biomarkers, telomere length, and genetic analysis. Saliva and fecal samples will undergo metagenomic analysis to study the microbiome. Some of the analyses will be conducted as additional funding is obtained. Briefly, the main outcomes planned from biological samples include:
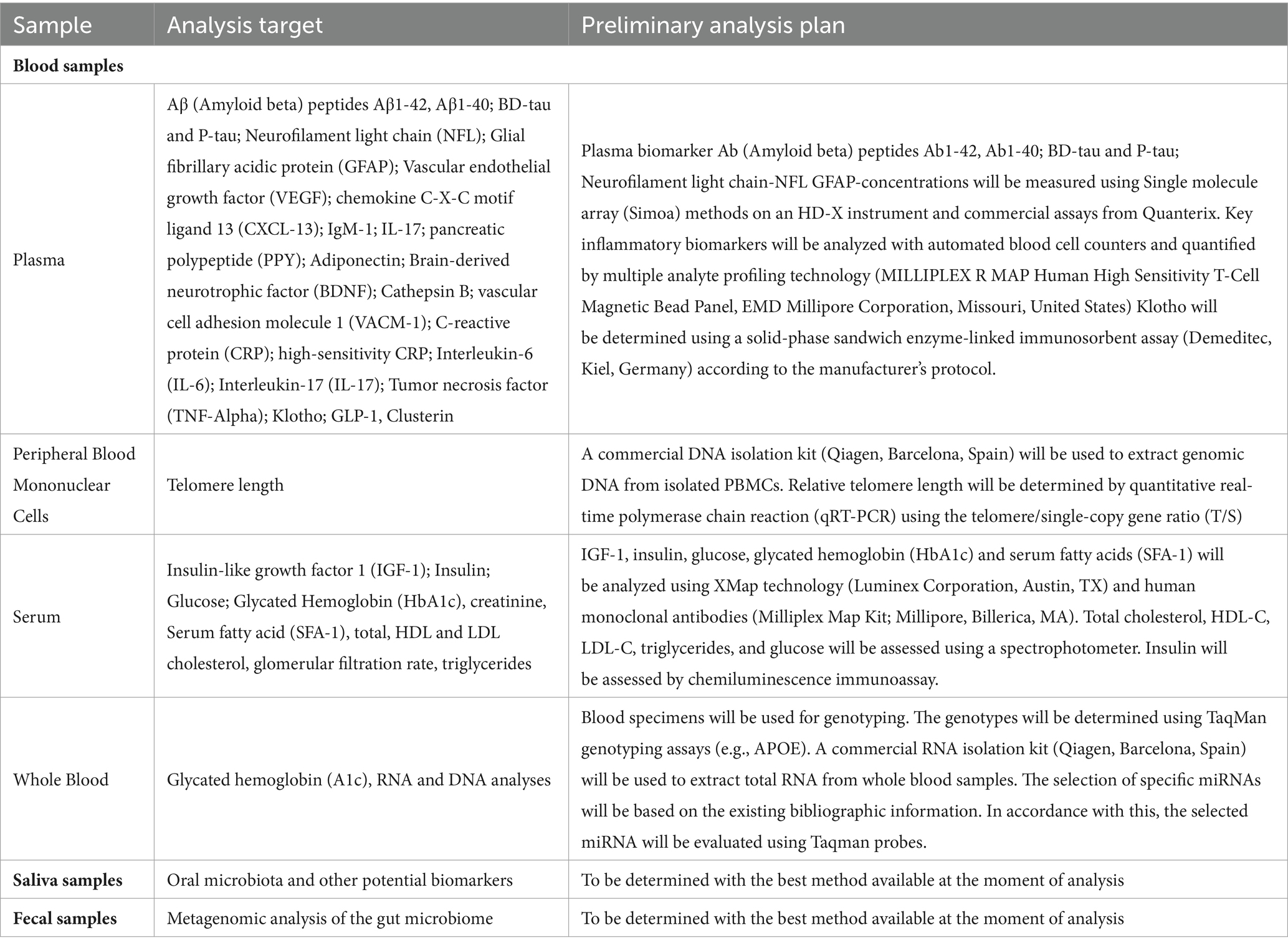
Table 5. Biological samples and targeted analysis plan.
Change in cardiovascular biomarkers (baseline and 12 weeks): Blood samples will be used to determine concentrations of cardiovascular biomarkers including glucose, insulin, triglycerides, high-density lipoprotein (HDL), low-density lipoprotein (LDL), and total cholesterol.
Change in brain-peripheral biomarkers (baseline and 12 weeks): Blood and saliva samples will be used to determine the concentration of peripheral brain biomarkers such as brain-derived neurotrophic factor (BDNF), vascular endothelial growth factor (VEGF), insulin-like growth factor 1 (IGF-1), cathepsin B (CTSB), amyloid and tau protein levels, as well as novel neurodegenerative biomarkers based on new evidence available at the time of the analysis.
Change in inflammatory biomarkers (baseline and 12 weeks): Blood samples will be used to determine concentrations of inflammatory peripheral biomarkers such as tumor necrosis factor-alpha (TNF-alpha), interleukins, and both traditional and high-sensitivity C-reactive proteins.
Change in gene expression and epigenetics (baseline and 12 weeks): Blood samples will be stored for epigenetic and gene expression changes.
Change in oral and gut microbiota (baseline and 12 weeks): Saliva and fecal samples will be used to determine oral and gut microbiota including the most representative phyla (i.e., firmicutes, Bacteroidetes, and proteobacteria).
2.8.3.3 Hemodynamics
Hemodynamic changes (baseline and 12 weeks): Non-invasive hemodynamic parameters will be measured using ultrasound (Vivid E95, GE Healthcare) at three levels: (1) vascular (main carotid artery and vertebral artery, with measurements of intima-media thickness, flow, and wall strain, as well as registration of presence of atherosclerotic plaques), (2) cardiac (i.e., cardiac dimensions and volumes, systolic and diastolic function such as ejection fraction, strain deformation, and myocardial work), and (3) transcranial (i.e., systolic and diastolic flow velocity in the middle cerebral artery). Image acquisition and analysis will be carried out by cardiologists with expertise in ultrasonography.
Change in blood pressure (baseline and 12 weeks): Resting systolic and diastolic blood pressure will be assessed by a validated automated blood pressure monitor (Omron M3, Intellisense, OMRON Healthcare Europe, Spain) in the sitting position after 5 min of rest and with the left arm resting on a table at heart level. Three readings will be collected with 2-min intervals in between. Blood pressure will be calculated as the average of the last two blood pressure readings (Williams et al., 2018).
Change in arterial stiffness (baseline and 12 weeks): Arterial stiffness will be assessed using the pulse wave analysis and carotid-femoral pulse wave velocity (aortic-PWV) by applanation tonometry determined by the SphygmoCor® XCEL PWA/PWV (AtCor Medical, Sydney, Australia).
2.8.3.4 Physical functioning and body composition
Additional physical function and body composition outcomes will include:
Change in physical function and fitness (baseline and 12 weeks): The Senior Fitness Test, including the 6-min walking test will be used to assess overall physical functioning. Senior Fitness Test battery assesses upper and lower body strength, aerobic capacity, walking speed, balance, and flexibility (Langhammer and Stanghelle, 2015). Perceived physical fitness (cardiorespiratory fitness, muscular strength, speed-agility, flexibility and overall fitness) will be assessed using the International Fitness Scale (IFIS) (Merellano-Navarro et al., 2017). In addition, muscular strength with be measured with a combination of some of the Senior Fitness Test and handgrip strength test. In brief, each participant will be encouraged to perform the maximal isometric force twice with each hand using a hand dynamometer (TKK 5101 Grip D, Takey, Tokyo Japan). The maximum value of each hand will be taken and averaged in kilograms (kg) as an indicator of upper-body muscular strength. Lower body muscular strength will be assessed using the chair stand test (number of repetitions). Upper body muscular strength will be assessed using the arm curl test (number of repetitions). Perceived strength will be assessed using a single item from the IFIS (Merellano-Navarro et al., 2017).
Change in body composition (Baseline and 12 weeks): Body mass index (BMI, kg/m2) will be computed from height and weight measured with SECA instruments following standardized procedures. Body composition (i.e., lean mass, kg, fat mass, kg, and bone mineral content and density, z-score) will be assessed using a dual-energy x-ray absorptiometer and a TANITA’s Bioelectrical Impedance Analysis (TANITA MC-980MA-N plus, Amsterdam, Netherlands). We will also conduct MRI of the abdominal region to obtain information on overall visceral adipose tissue, specific-organ adipose tissue, and subcutaneous abdominal adiposity.
2.8.3.5 Mental health and lifestyle behaviors
A battery of questionnaires will be administered to evaluate the following dimensions in relation to mental health and lifestyle behavior:
Baseline and 12 weeks change in depressive symptoms will be assessed using the Global Deterioration Scale (Izal and Montorio, 1993), and the Hospital Anxiety and Depression Scale (HADS) (Zigmond and Snaith, 1983); change in anxiety symptoms will be assessed using the HADS questionnaire (Zigmond and Snaith, 1983); change in stress will be assessed using the Perceived Stress Scale (Remor, 2006); change in loneliness will be assessed using the UCLA Loneliness Scale (Russell et al., 1980); change in self-esteem will be assessed using the Rosenberg Self-Esteem Scale (Robins, 2001); change in social support will be assessed using the Social Provisions Scale (Cutrona and Russell, 1987).
Change in health-related quality of life (baseline and 12 weeks) will be assessed using the SF-36 form Alonso et al. (1995), which provides an 8-scale profile of functional health and well-being scores (i.e., physical functioning; role limitations due to physical problems; bodily pain; general health perceptions; energy/vitality; social functioning; role limitations due to emotional problems; and mental health) as well as psychometrically-based Physical Component Score (PCS) and Mental Component Score (MCS).
Change in physical activity and sedentary behaviors (baseline, 6 and 12 weeks): Physical activity and sedentary behavior will be measured using the accelerometer Axivity AX at baseline and 6-weeks. The accelerometer will be attached to the non-dominant wrist for 9 consecutive days, the sampling frequency will be set at 100 Hz, and the accelerometer raw data processing will be conducted using open-source software tools to ensure transparency and replicability of the methods (Migueles et al., 2019). Additionally, participants will complete the short version self-reported International Physical Activity Questionnaire (Troiano et al., 2020) at baseline and 12 weeks.
Change in duration and sleep quality (baseline and 6 weeks): Sleep duration (hours/night) will be computed from the accelerometer Axivity AX and diaries, and an open-source software will be used to process the raw data recordings (Migueles et al., 2019). In addition, participants will complete a single-item question on usual sleep duration. Sleep quality (e.g., sleep regularity, sleep efficiency, latency, number and total time of waking up after sleep onset) will also be assessed using the accelerometer Axivity AX.
Change in diet behaviors (baseline, 6 and 12 weeks): Diet behaviors will be self-reported using the 14-item Questionnaire of Mediterranean Diet Adherence (PREDIMED-14) with an additional question for supplement intake.
Additional variables related to health, lifestyle and genotype will be measured for descriptive purposes, for covariate adjustment in the analyses when necessary or for interaction with the intervention effects. Examples include biological sex, ethnicity, educational level, smoking habits, alcohol consumption, medication, comorbidities (e.g., dyslipidemia, hypertension, or type 2 diabetes), family history of dementia, handedness, and COVID-19 history. Additionally, genotyping at baseline will be conducted for well-known Single Nucleotide Polymorphisms (SNP) for brain health, such as Apolipoprotein E (APOE) and BDNF genotypes, and additional relevant SNPs based on an updated literature search. The genotyping analysis is conducted to test gene-exercise interaction as we have done in previous RCTs (Solis-Urra et al., 2023).
2.9 Sample size and statistical analysis
A detailed description of the statistical analysis plan, including a sample size calculation, for the HEART-BRAIN trial has been pre-registered and published on Clinicaltrials.gov (NCT06214624; submission date: January, 2024).
2.9.1 Sample size
We have used G*Power (version 3.1.9.7. Universität Düsseldorf, Germany) (Faul et al., 2007) to calculate the sample size. The HEART-BRAIN project has been designed to detect a low-to-medium effect size in the primary outcome, cerebral blood flow (i.e., Cohen d = 0.35) (Anazodo et al., 2015) for repeated-measures ANOVA, within-between interaction, with a two-sided alpha of 5% and power of 80%. The sample size has been adjusted for an expected 7% dropout during the intervention [based on 3-month dropout rates of our previous RCTs (Solis-Urra et al., 2023)]. Finally, the estimated sample size was 90 participants (30 in each study arm).
2.9.2 Framework and timing
A superiority hypothesis testing framework will be used. In the main analyses, we will compare whether both exercise interventions (HIIT alone or HIIT plus resistance training) are superior to usual care (no exercise training). The final analyses will be performed after collecting and processing the data of the primary and secondary outcomes. The time points for data collection of each outcome are explained in Section 2.4.
2.9.3 Statistical interim analyses and stopping guidance
No pre-specified interim analyses will be performed, and therefore, a stopping guidance is not applicable. Basic analyses (not including the primary outcome) have been performed as required by the final report for the funding agencies, after completion of the first 58 participants. The basic analyses have been performed by a researcher who is not involved in data collection (EAB). The results of the basic analyses have not been discussed with other members of the research team involved in the evaluations or interventions to avoid any bias during the implementation of the study, data collection or processing. These basic analyses have not led to any protocol deviations.
2.9.4 Brief description of the primary and secondary analyses
The main analyses will consist of the intention-to-treat analyses for the primary and secondary outcomes using a constrained baseline (meaning baseline adjusted) linear mixed model, which accounts for baseline differences among the study groups. The model will include fixed effects for time (two levels) and treatment (three levels) as well as the unique participant identifier as a random effect. If the global test of significance indicates between-group differences, pairwise comparisons will be explored. Although no adjustments for multiplicity will be performed, family-wise type 1 error rate on the primary outcome will be retained by using a hierarchical analytic approach. The prespecified hierarchical hypotheses will be tested using the prespecified sequence: HIIT plus resistance training versus usual care, HIIT versus usual care, and HIIT plus resistance training versus HIIT. No additional adjustments for covariates will be made (except for baseline adjustments of the outcome). The main statistical analyses will be performed by an independent researcher (EAB), who is not involved in the recruitment, evaluations, and interventions, and who will be blinded to treatment allocation by coding the intervention arms (e.g., A, B, C). The same approach will be applied to secondary and tertiary outcomes.
2.9.5 Moderation, mediation, and other secondary analyses
Although the RCT is not powered for subgroup analyses, we will perform moderation analyses by exploratory subgroup analyses for age, sex, education level, baseline level of the study outcome (stratified on the median), and APOE genotype. Likewise, we plan to explore potential mechanisms driving effects on outcomes. For example, we will run a formal mediation analysis to test whether changes in cardiorespiratory fitness explain exercise-derived changes in brain and cognitive outcomes, and whether changes in CBF or vascularization mediate exercise-derived changes in cognitive outcomes. Examples of the potential mediators and moderators on the effects of exercise on CBF are detailed in Supplementary Table S2. When the data analysis phase is reached, the most up-to-date literature will be reviewed to perform these exploratory analysis.
The majority of published cardiac rehabilitation studies reported a low percentage of females enrolled, as confirmed by this review (Cugusi and Mercuro, 2019) with an overall average of 16.4% in females vs. 78.6% in males. Thus, we expect a small percentage of females, preventing us to perform subgroup analysis on sex. Nevertheless, we will calculate the participation prevalence ratio, which compares the female representation in a study to the percentage of females in the general population of CAD patients.
2.9.6 Confidence intervals and p values
All statistical tests will be two-tailed. P for significance will be set at 0.05 and 95% confidence intervals will be estimated. No adjustments for multiplicity will be made as multiplicity adjustments may be of lesser importance in the case of distinct treatment arms (Li et al., 2017). Since only one primary outcome has been defined, other outcomes do not require adjustment for multiple testing. However, we will include a hierarchical analytic approach for the exercise interventions tested and the primary outcome.
2.9.7 Analysis populations
We plan to use two approaches for the statistical analyses:
1. Intention-to-treat (main analysis): This will be used for our primary analyses and includes all randomized participants. With this approach, all randomized participants are included in the analysis, based on the groups to which they were initially randomly assigned to. This implies that some participants will have valid data at both time points, while some might have missing data at baseline or post-intervention assessment, which is sometimes named as “available-case intention-to-treat.”
2. Per-protocol and additional sensitivity analyses: This dataset will be used for our secondary analyses and includes all participants with ≥70% attendance. Additionally, sensitivity analyses will be performed using the per-protocol database and excluding participants who had injuries or other health problems during the post-assessment evaluations. We will also analyze the effects of attendance and compliance by conducting an analysis including individuals who, in addition to attending ≥70% of the sessions, also had ≥70% compliance to the training protocol based on the time within the HIIT heart rate target zones.
2.10 Data management and sharing
The HEART-BRAIN trial will use two data storage systems: (i) the REDCap platform, an online software for the management of research databases in clinical trials and translational research. RedCap will be used for the storage and management of all non-imaging information, guarantying its trace and safety (Harris et al., 2019); (ii) the HEART-BRAIN desktop computer will also contain participants’ pseudonymized data collected on paper-based forms, that will be scanned and stored, as well as the MRI data. Physical copies of data collection forms and documents will be securely stored in a locked cabinet at the iMUDS facility. Upon enrolment in the trial, participants will be assigned a unique code to be used consistently across all forms and data collection reports, i.e., pseudonymized data, to reduce the risk of exposure resulting from unintended unauthorized access or disclosure. In addition, information linking the pseudonym to the identifiable information must be kept separately and subjected to ensure non-attribution to an identified or identifiable individual. The PI will have access to the final dataset and will provide reasonable and responsible access to the pseudonymized data to other researchers. Participants will consent to the use of their pseudonymized data for secondary research, as outlined in the informed consent process. After each assessment, all data will undergo thorough quality control checks to ensure the accuracy of the assessment and will be archived following standardized storage protocols of our research facility. Examples of quality control measures include visual inspection of imaging data, double correction of paper-pencil cognitive tests, and verification of data validity and integrity in REDCap. Our study protocol and statistical analysis plan were uploaded to clinicaltrial.gov prespecifying our methods to ensure the reliability of the results. The study will adhere to the FAIR principles (Findability, Accessibility, Interoperability, and Reusability), and meta-data will be made publicly available. A DOI (Digital Object Identifier) is issued to every published record. Governance, ethical considerations, and shared trial oversight will be prioritized, aligning with current best practices. Study results, including positive, negative, or inconclusive, will be disseminated through peer-reviewed journals, and national and international conferences, and shared via social media and press releases with participants, caregivers, physicians, and the broader medical and scientific community.
The protocol, statistical analyses plan and data management plan will be shared open access. Data files, including pseudonymized individual participant data, will be shared under restricted access and upon reasonable request (contact FBO) due to privacy issues and EU-GDPR regulations. In principle, all collected individual participant data will be available for sharing under the “as open as possible, as closed as necessary” principle. The shared data files will be pseudonymized, and only include participants who provided informed consent for sharing, and sharing is only possible when the data is used for research purposes related to exercise and cardiovascular and brain health. The individual participant data will be available 12 months after the primary outcome paper is published. The specific process of data access will be determined in a later stage. In short, data will be made available upon reasonable requests to the PI (FBO). The data requests must contain the purpose and aim of the research, target variables, and data analysis plan before data sharing. Data will only be shared for research and public health purposes. A data access committee will be created to approve the appropriate data requests. A data monitoring committee does not exist in the funding system in Spain.
3 Discussion
Growing evidence supports the benefits of exercise on the cardiovascular health of individuals with CAD (Goldhammer et al., 2005; Niessner et al., 2006; Lavie and Milani, 2011; Pareja-Galeano et al., 2015; Anderson et al., 2016; Muscella et al., 2020). Yet, the mechanisms by which different types of exercise might improve brain health or attenuate the cognitive and mental health declines observed in patients with CAD remain to be elucidated. Well-designed intervention studies unraveling the effects and mechanisms by which exercise impacts brain health in patients with CAD will have important clinical and scientific implications. The findings will facilitate moving towards a more ‘personalized medicine’ approach to exercise prescription in patients with CAD. Thus, the present work provides a comprehensive description of the HEART-BRAIN RCT, following the SPIRIT guidelines for interventional RCTs (Chan et al., 2013a,b; Butcher et al., 2022). The HEART-BRAIN project aims to examine the effects of two different 12-week supervised exercise interventions (HIIT and HIIT plus resistance training) compared to usual care on brain and cardiovascular health in patients with CAD. The primary outcome is CBF assessed by a cutting-edge technique called ASL-MRI.
Among the few studies that have evaluated the effects of exercise on brain health in individuals with CAD, most of them have focused on health-related quality of life and mental health outcomes (Gomes-Neto et al., 2017; Yu et al., 2023). Other key domains of brain health such as cognition, biological markers of brain health, brain morphology and function, or cerebrovascular outcomes remain unexplored.
This study will contribute to the advancement of scientific knowledge in different ways. Firstly, it stands as an innovative intervention of two different exercise programs in accordance with the most updated guidelines (Mezzani et al., 2012; Taylor et al., 2019; Bull et al., 2020; Bayles, 2023). By providing a comprehensive description and pre-specified plan of the study protocol, we ensure transparency and enable the scientific community to replicate the protocols and intervention, fostering the dissemination of scientific knowledge.
Thus, the novelty of our study lies in the comprehensive evaluation of outcomes related to brain health, including MRI assessments measuring cerebral blood flow, vascularization, and blood–brain barrier permeability, as well as the assessment of cognitive function and various mental health outcomes. Additionally, this RCT compares two exercise modalities, including the combination of HIIT plus resistance training, whose effect on brain health in patients with CAD remains unexplored. Furthermore, one of the main novelties of the HEART-BRAIN trial is that it will investigate not only the effects produced by these two exercise modalities but also the causal mechanisms behind the effects, with a primary focus on the brain. Current guidelines promoting physical exercise for patients with CAD are primarily based on cardiometabolic adaptations (Mezzani et al., 2012; Taylor et al., 2019; Bull et al., 2020; Bayles, 2023). The unique outcomes expected from the present study will contribute to the existing guidelines by providing a comprehensive understanding of the impact of HIIT and HIIT plus resistance training on brain health, as well as its underlying mechanisms. We expect that the intervention and the obtained results will serve as a valuable resource for healthcare and exercise professionals, facilitating them to effectively prescribe exercise to patients with CAD. This represents an effective transfer of scientific knowledge to practical settings. This study underscores the importance of systematic and well-defined methodological reports addressing the transparency gaps within the scientific community, ensuring the comprehensive sharing of study information and facilitating replication.
3.1 Strengths and limitations
HEART-BRAIN has several strengths that bolster the reliability and validity of the expected results, such as: (i) well-designed RCT framework ensuring random allocation of participants, minimizing selection bias, and enhancing the validity of the causal inferences drawn from the data; (ii) extensive brain health mapping, including comprehensive assessments of the different domains of brain health; (iii) comprehensive set of variables, including objective, gold-standard test (e.g., CPET) and patient-reported outcomes (e.g., QoL) to encompass both physical and brain health; (iv) continuous heart rate monitoring throughout the exercise sessions allowing for a rigorous compliance analysis, (v) time and (estimated) caloric matched exercise groups, ensuring that any observed effects can be attributable to the type of exercise rather than differences in exercise duration or intensity; (vi) flexibility is offered to help participants overcome barriers frequently reported about exercise participation (e.g., trainers adapt to the time that fits best participants’ schedule); (vii) our mechanistic approach will provide insights on how exercise can impact brain health in patients with CAD and the potential mechanisms explaining the heart-brain connection, such as changes in CBF; and (viii) this study holds significant clinical relevance as it specifically targets potential improvements in brain health among patients with CAD, a population known to experience accelerated cognitive decline.
The study also has some limitations that must be acknowledged. Since the HEART-BRAIN RCT is implementing HIIT, certain criteria have been established to maximize safety. For example, only individuals with a stable and controlled disease during the outpatient phase will be included. Future trials recruiting a more generalizable group of patients with CAD (i.e., including individuals in a more severe condition) are needed. The RCT is not powered for subgroup analyses, and we expect low female representation (<30%) based on disease prevalence and previous research on cardiac rehabilitation programs. Further, our study is of relative short duration (12 weeks). While notable physiological changes may manifest within this timeframe, certain significant adaptations may require a longer intervention and follow-up period. Although inherent to exercise-based RCTs, another limitation is the single (and not double) blinding. These limitations should be taken into consideration when interpreting the study’s findings.
Ethics statement
The studies involving humans were approved by Research Ethics Board of the Andalusian Health Service (CEIM/CEI Provincial de Granada; #1776-N-21 on December 21st, 2021). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
AT: Writing – original draft, Writing – review & editing. PS-U: Writing – original draft, Writing – review & editing. EB: Writing – original draft, Writing – review & editing, Formal analysis. LS-A: Writing – original draft, Writing – review & editing. JF-O: Writing – original draft, Writing – review & editing. CP: Writing – original draft, Writing – review & editing. RA-C: Writing – original draft, Writing – review & editing. AG-G: Writing – original draft, Writing – review & editing. IM-F: Writing – original draft, Writing – review & editing. BF-G: Writing – original draft, Writing – review & editing. MO-R: Writing – original draft, Writing – review & editing. AC-P: Writing – original draft, Writing – review & editing. DB: Writing – original draft, Writing – review & editing. AS: Writing – original draft, Writing – review & editing. JS-M: Writing – original draft, Writing – review & editing. RR-L: Writing – original draft, Writing – review & editing. NH-G: Writing – original draft, Writing – review & editing. RP-B: Writing – original draft, Writing – review & editing. VL-E: Writing – original draft, Writing – review & editing. SC-P: Writing – original draft, Writing – review & editing. MG-O: Writing – original draft, Writing – review & editing. AV-C: Writing – original draft, Writing – review & editing. EB-M: Writing – original draft, Writing – review & editing. FM-N: Writing – original draft, Writing – review & editing. RN: Writing – original draft, Writing – review & editing. AC-R: Writing – original draft, Writing – review & editing. FA-G: Writing – original draft, Writing – review & editing. JM-G: Writing – original draft, Writing – review & editing. SV-A: Writing – original draft, Writing – review & editing. AC: Writing – original draft, Writing – review & editing. JM: Writing – original draft, Writing – review & editing. KE: Writing – original draft, Writing – review & editing. EM-E: Writing – original draft, Writing – review & editing. RG-O: Writing – original draft, Writing – review & editing. IE-C: Writing – original draft, Writing – review & editing. FO: Funding acquisition, Project administration, Resources, Supervision, Writing – original draft, Writing – review & editing, Conceptualization, Formal analysis. All authors contributed intellectually to the design and development of the methodology and approved the final manuscript of this study protocol. Our authorship aligns with the ICMJE author contributions criteria (Editors ICoMJ, 2018).
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The HEART-BRAIN Project is supported with the Grant PID2020-120249RB-I00 funded by MCIN/AEI/10.13039/501100011033. Additional support was obtained from the Andalusian Government (Junta de Andalucía, Plan Andaluz de Investigación, ref. P20_00124) and the CIBER de Fisiopatología de la Obesidad y Nutrición (CIBEROBN), Instituto de Salud Carlos III, Granada, Spain. Moreover, EB has received funding from the European Union’s Horizon 2020 research and innovation programme under the Marie Skłodowska-Curie grant agreement No. [101064851]. AT has received funding from the Junta de Andalucia, Spain, under the Postdoctoral Research Fellows (Ref. POSTDOC_21_00745). IE-C is supported by RYC2019-027287-I grant funded by MCIN/AEI/10.13039/501100011033/and “ESF Investing in your future.” IM-F is supported by the Spanish Ministry of Science, Innovation and Universities (JDC2022-049642-I). AC was funded by postdoctoral research grants from the Swedish Heart-Lung Foundation (grant number 20230343), the County Council of Ostergotland, Sweden (grant number RÖ-990967), the Swedish Society of Cardiology, and the Swedish Society of Clinical Physiology. BF-G is supported by the Spanish Ministry of Education, Culture and Sport (PID2022-137399OB-I00) funded by MCIN/AEI/10.13039/501100011033 and FSE+. MO-R, LS-A and JF-O are supported by the Spanish Ministry of Science, Innovation and Universities (FPU 22/02476, FPU 21/06192 and FPU 22/03052, respectively). JM is supported by the Spanish Ministry of Science, Innovation and Universities under Beatriz Galindo’s 2022 fellowship program (BG22/00075). JS-M is supported by the National Agency for Research and Development (ANID)/Scholarship Program/DOCTORADO BECAS CHILE/2022-(Grant N°72220164). SV-A is supported by a Health and Behavior International Collaborative Award by the Society of Behavioral Medicine. This work is part of a PhD thesis conducted in the Doctoral Programme in Biomedicine of the University of Granada, Granada, Spain. The sponsors or funding agencies had no role in the design and conduct of the study, in the collection, analysis, and interpretation of data, in the preparation of the manuscript, or in the review or approval of the manuscript.
Acknowledgments
We thank Dr. Veronica Cabanas-Sanchez for performing the randomization of the study. The article has been published as a preprint in MedRxiv with the DOI: 10.1101/2024.05.22.24307744 (Toval et al., 2024).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnagi.2024.1437567/full#supplementary-material
References
Ainsworth, B. E., Haskell, W. L., Herrmann, S. D., Meckes, N., Bassett, D. R. Jr., Tudor-Locke, C., et al. (2011). 2011 compendium of physical activities: a second update of codes and MET values. Med. Sci. Sports Exerc. 43, 1575–1581. doi: 10.1249/MSS.0b013e31821ece12
Alonso, J., Prieto, L., and Antó, J. (1995). The Spanish version of the SF-36 health survey (the SF-36 health questionnaire): an instrument for measuring clinical results. Med. Clin. 104, 771–776.
Anazodo, U. C., Shoemaker, J. K., Suskin, N., Ssali, T., Wang, D. J., and St Lawrence, K. S. (2015). Impaired cerebrovascular function in coronary artery disease patients and recovery following cardiac rehabilitation. Front. Aging Neurosci. 7:224. doi: 10.3389/fnagi.2015.00224
Anderson, L., Oldridge, N., Thompson, D. R., Zwisler, A.-D., Rees, K., Martin, N., et al. (2016). Exercise-based cardiac rehabilitation for coronary heart disease: Cochrane systematic review and meta-analysis. J. Am. Coll. Cardiol. 67, 1–12. doi: 10.1016/j.jacc.2015.10.044
Bahbah, E. I., Noehammer, C., Pulverer, W., Jung, M., and Weinhaeusel, A. (2021). Salivary biomarkers in cardiovascular disease: an insight into the current evidence. FEBS J. 288, 6392–6405. doi: 10.1111/febs.15689
Bayles, M. P. (2023). ACSM's exercise testing and prescription. Philadelphia, USA: Lippincott williams & wilkins.
Brandt, J., Spencer, M., and Folstein, M. (1988). The telephone interview for cognitive status. Neuropsychiatry Neuropsychol. Behav. Neurol. 1, 111–117.
Bull, F. C., Al-Ansari, S. S., Biddle, S., Borodulin, K., Buman, M. P., Cardon, G., et al. (2020). World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 54, 1451–1462. doi: 10.1136/bjsports-2020-102955
Butcher, N. J., Monsour, A., Mew, E. J., Chan, A.-W., Moher, D., Mayo-Wilson, E., et al. (2022). Guidelines for reporting outcomes in trial protocols: the SPIRIT-outcomes 2022 extension. JAMA Cardiol. 328, 2345–2356. doi: 10.1001/jama.2022.21243
Byrne, R. A., Rossello, X., Coughlan, J., Barbato, E., Berry, C., Chieffo, A., et al. (2023). 2023 ESC guidelines for the management of acute coronary syndromes: developed by the task force on the management of acute coronary syndromes of the European Society of Cardiology (ESC). J. Eur. Heart J. 44, 3720–3826. doi: 10.1093/eurheartj/ehad191
Chan, A. W., Tetzlaff, J. M., Altman, D. G., Laupacis, A., Gøtzsche, P. C., Krleža-Jerić, K., et al. (2013a). SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann. Intern. Med. 158, 200–207. doi: 10.7326/0003-4819-158-3-201302050-00583
Chan, A. W., Tetzlaff, J. M., Gøtzsche, P. C., Altman, D. G., Mann, H., Berlin, J. A., et al. (2013b). SPIRIT 2013 explanation and elaboration: guidance for protocols of clinical trials. BMJ 346:e7586. doi: 10.1136/bmj.e7586
Committee PAGA . (2018). 2018 physical activity guidelines advisory committee scientific report. US Department of Health and Human Services Washington, DC.
Cugusi, L., and Mercuro, G. (2019). A systematic overview to quantify the gender imbalance in cardiovascular rehabilitation trials. Eur. J. Prev. Cardiol. 26, 776–781. doi: 10.1177/2047487318811415
Cutrona, C. E., and Russell, D. W. (1987). The provisions of social relationships and adaptation to stress. Adv. Pers. Relat. 1, 37–67.
Daulatzai, M. A. (2017). Cerebral hypoperfusion and glucose hypometabolism: key pathophysiological modulators promote neurodegeneration, cognitive impairment, and Alzheimer's disease. J. Neurosci. Res. 95, 943–972. doi: 10.1002/jnr.23777
Dibben, G. O., Faulkner, J., Oldridge, N., Rees, K., Thompson, D. R., Zwisler, A. D., et al. (2023). Exercise-based cardiac rehabilitation for coronary heart disease: a meta-analysis. Eur. Heart J. 44, 452–469. doi: 10.1093/eurheartj/ehac747
Dongiovanni, P., Meroni, M., Casati, S., Goldoni, R., Thomaz, D. V., Kehr, N. S., et al. (2023). Salivary biomarkers: novel noninvasive tools to diagnose chronic inflammation. Int. J. Oral Sci. 15:27. doi: 10.1038/s41368-023-00231-6
Erickson, K. I., Voss, M. W., Prakash, R. S., Basak, C., Szabo, A., Chaddock, L., et al. (2011). Exercise training increases size of hippocampus and improves memory. Proc. Natl. Acad. Sci. USA 108, 3017–3022. doi: 10.1073/pnas.1015950108
Faul, F., Erdfelder, E., Lang, A. G., and Buchner, A. (2007). G*power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 39, 175–191. doi: 10.3758/BF03193146
Gallagher, R. M., Kirkham, J. J., Mason, J. R., Bird, K. A., Williamson, P. R., Nunn, A. J., et al. (2011). Development and inter-rater reliability of the Liverpool adverse drug reaction causality assessment tool. Plos One 6:e28096. doi: 10.1371/journal.pone.0028096
Goldhammer, E., Tanchilevitch, A., Maor, I., Beniamini, Y., Rosenschein, U., and Sagiv, M. (2005). Exercise training modulates cytokines activity in coronary heart disease patients. Int. J. Cardiol. 100, 93–99. doi: 10.1016/j.ijcard.2004.08.073
Gomes-Neto, M., Duraes, A. R., Reis, H. F. C., Neves, V. R., Martinez, B. P., and Carvalho, V. O. (2017). High-intensity interval training versus moderate-intensity continuous training on exercise capacity and quality of life in patients with coronary artery disease: a systematic review and meta-analysis. Eur. J. Prev. Cardiol. 24, 1696–1707. doi: 10.1177/2047487317728370
Han, H., Zhang, R., Liu, G., Qiao, H., Chen, Z., Liu, Y., et al. (2019). Reduction of cerebral blood flow in community-based adults with subclinical cerebrovascular atherosclerosis: a 3.0 T magnetic resonance imaging study. NeuroImage 188, 302–308. doi: 10.1016/j.neuroimage.2018.12.021
Harris, P. A., Taylor, R., Minor, B. L., Elliott, V., Fernandez, M., O'Neal, L., et al. (2019). The REDCap consortium: building an international community of software platform partners. J. Biomed. Inform. 95:103208. doi: 10.1016/j.jbi.2019.103208
Izal, M., and Montorio, I. (1993). Adaptation of the geriatric depression scale in Spain: a preliminary study. Clin. Gerontol. 13, 83–91. doi: 10.1300/J018v13n02_07
Kilroy, E., Apostolova, L., Liu, C., Yan, L., Ringman, J., and Wang, D. J. (2014). Reliability of two-dimensional and three-dimensional pseudo-continuous arterial spin labeling perfusion MRI in elderly populations: comparison with 15O-water positron emission tomography. J. Magn. Reson. Imaging 39, 931–939. doi: 10.1002/jmri.24246
Kumari, S., Samara, M., Ampadi Ramachandran, R., Gosh, S., George, H., Wang, R., et al. (2023). A review on saliva-based health diagnostics: biomarker selection and future directions. Biomed. Mater. Devices 2, 121–138. doi: 10.1007/s44174-023-00090-z
Lang, J. J., Prince, S. A., Merucci, K., Cadenas-Sanchez, C., Chaput, J. P., Fraser, B. J., et al. (2024). Cardiorespiratory fitness is a strong and consistent predictor of morbidity and mortality among adults: an overview of meta-analyses representing over 20.9 million observations from 199 unique cohort studies. Br. J. Sports Med. 58, 556–566. doi: 10.1136/bjsports-2023-107849
Langhammer, B., and Stanghelle, J. K. (2015). The senior fitness test. J. Physiother. 61:163. doi: 10.1016/j.jphys.2015.04.001
Lavie, C. J., and Milani, R. V. (2011). Cardiac rehabilitation and exercise training in secondary coronary heart disease prevention. Prog. Cardiovasc. Dis. 53, 397–403. doi: 10.1016/j.pcad.2011.02.008
Li, G., Taljaard, M., Van den Heuvel, E. R., Levine, M. A., Cook, D. J., Wells, G. A., et al. (2017). An introduction to multiplicity issues in clinical trials: the what, why, when and how. Int. J. Epidemiol. 46, 746–755. doi: 10.1093/ije/dyw320
Long, J. M., and Holtzman, D. M. (2019). Alzheimer disease: an update on pathobiology and treatment strategies. Cell Metab. 179, 312–339. doi: 10.1016/j.cell.2019.09.001
Luengo-Fernandez, R., Walli-Attaei, M., Gray, A., Torbica, A., Maggioni, A. P., Huculeci, R., et al. (2023). Economic burden of cardiovascular diseases in the European Union: a population-based cost study. Eur. Heart J. 44, 4752–4767. doi: 10.1093/eurheartj/ehad583
Malakar, A. K., Choudhury, D., Halder, B., Paul, P., Uddin, A., and Chakraborty, S. (2019). A review on coronary artery disease, its risk factors, and therapeutics. J. Cell. Physiol. 234, 16812–16823. doi: 10.1002/jcp.28350
Maleki, S., Hendrikse, J., Chye, Y., Caeyenberghs, K., Coxon, J. P., Oldham, S., et al. (2022). Associations of cardiorespiratory fitness and exercise with brain white matter in healthy adults: a systematic review and meta-analysis. Brain Imaging Behav. 16, 2402–2425. doi: 10.1007/s11682-022-00693-y
Merellano-Navarro, E., Collado-Mateo, D., García-Rubio, J., Gusi, N., and Olivares, P. R. (2017). Validity of the international fitness scale "IFIS" in older adults. Exp. Gerontol. 95, 77–81. doi: 10.1016/j.exger.2017.05.001
Mezzani, A., Hamm, L. F., Jones, A. M., McBride, P. E., Moholdt, T., Stone, J. A., et al. (2012). Aerobic exercise intensity assessment and prescription in cardiac rehabilitation: a joint position statement of the European Association for Cardiovascular Prevention and Rehabilitation, the American Association of Cardiovascular and Pulmonary Rehabilitation, and the Canadian Association of Cardiac Rehabilitation. J. Cardiopulm. Rehabil. Prev. 32, 327–350. doi: 10.1097/HCR.0b013e3182757050
Migueles, J. H., Rowlands, A. V., Huber, F., Sabia, S., and van Hees, V. T. (2019). GGIR: a research community–driven open source R package for generating physical activity and sleep outcomes from multi-day raw accelerometer data. J. Meas. Phys. Behav. 2, 188–196. doi: 10.1123/jmpb.2018-0063
Morishita, S., Tsubaki, A., Nakamura, M., Nashimoto, S., Fu, J. B., and Onishi, H. (2019). Rating of perceived exertion on resistance training in elderly subjects. Expert. Rev. Cardiovasc. Ther. 17, 135–142. doi: 10.1080/14779072.2019.1561278
Muñoz-García, M., Cervantes, S., Razquin, C., Guillén-Grima, F., Toledo, J. B., Martínez-González, M., et al. (2019). Validation study of a Spanish version of the modified telephone interview for cognitive status (STICS-m). Gac. Sanit. 33, 415–420. doi: 10.1016/j.gaceta.2018.05.004
Muscella, A., Stefàno, E., and Marsigliante, S. (2020). The effects of exercise training on lipid metabolism and coronary heart disease. Am. J. Physiol. Heart Circ. Physiol. 319, H76–H88. doi: 10.1152/ajpheart.00708.2019
Niessner, A., Richter, B., Penka, M., Steiner, S., Strasser, B., Ziegler, S., et al. (2006). Endurance training reduces circulating inflammatory markers in persons at risk of coronary events: impact on plaque stabilization? Atherosclerosis 186, 160–165. doi: 10.1016/j.atherosclerosis.2005.06.047
Ojeda, N., del Pino, R., Ibarretxe-Bilbao, N., Schretlen, D., and Peña, J. (2016). Test de evaluación cognitiva de Montreal: normalización y estandarización de la prueba en población española. Rev. Neurol. 63, 488–496. doi: 10.33588/rn.6311.2016241
Ostheim, P., Tichý, A., Sirak, I., Davidkova, M., Stastna, M. M., Kultova, G., et al. (2020). Overcoming challenges in human saliva gene expression measurements. Sci. Rep. 10:11147. doi: 10.1038/s41598-020-67825-6
Pareja-Galeano, H., Garatachea, N., and Lucia, A. (2015). Exercise as a polypill for chronic diseases. Prog. Mol. Biol. Transl. Sci. 135, 497–526. doi: 10.1016/bs.pmbts.2015.07.019
Pelliccia, A., Sharma, S., Gati, S., Bäck, M., Börjesson, M., Caselli, S., et al. (2021). 2020 ESC guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur. Heart J. 42, 17–96. doi: 10.1093/eurheartj/ehaa605
Reitan, R. M. (1958). Validity of the trail making test as an indicator of organic brain damage. Percept. Mot. Skills 8, 271–276. doi: 10.2466/pms.1958.8.3.271
Remor, E. (2006). Psychometric properties of a European Spanish version of the perceived stress scale (PSS). Span. J. Psychol. 9, 86–93. doi: 10.1017/S1138741600006004
Robins, R. (2001). Measuring global self-esteem: construct validation of a single-item measure and the Rosenberg self-esteem scale. Pers. Soc. Psychol. Bull. 27, 151–161. doi: 10.1177/0146167201272002
Roger, V. L. (2017). The heart–brain connection: from evidence to action. Eur. Heart J. 38, 3229–3231. doi: 10.1093/eurheartj/ehx387
Rogers, R. L., Meyer, J. S., and Mortel, K. F. (1990). After reaching retirement age physical activity sustains cerebral perfusion and cognition. J. Am. Geriatr. Soc. 38, 123–128. doi: 10.1111/j.1532-5415.1990.tb03472.x
Rognmo, Ø., Moholdt, T., Bakken, H., Hole, T., Mølstad, P., Myhr, N. E., et al. (2012). Cardiovascular risk of high-versus moderate-intensity aerobic exercise in coronary heart disease patients. Circulation 126, 1436–1440. doi: 10.1161/CIRCULATIONAHA.112.123117
Ross, R., Blair, S. N., Arena, R., Church, T. S., Després, J.-P., Franklin, B. A., et al. (2016). Importance of assessing cardiorespiratory fitness in clinical practice: a case for fitness as a clinical vital sign: a scientific statement from the American Heart Association. Circulation 134, e653–e699. doi: 10.1161/CIR.0000000000000461
Russell, D., Peplau, L. A., and Cutrona, C. E. (1980). The revised UCLA loneliness scale: concurrent and discriminant validity evidence. J. Pers. Soc. Psychol. 39, 472–480. doi: 10.1037/0022-3514.39.3.472
Sandercock, G., Hurtado, V., and Cardoso, F. (2013). Changes in cardiorespiratory fitness in cardiac rehabilitation patients: a meta-analysis. Int. J. Cardiol. 167, 894–902. doi: 10.1016/j.ijcard.2011.11.068
Schievink, S. H., van Boxtel, M. P., Deckers, K., van Oostenbrugge, R. J., Verhey, F. R., and Köhler, S. (2022). Cognitive changes in prevalent and incident cardiovascular disease: a 12-year follow-up in the Maastricht aging study (MAAS). Eur. Heart J. 43, e2–e9. doi: 10.1093/eurheartj/ehx365
Schulz, K. F., Altman, D. G., and Moher, D. (2010). CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMC Med. 8:18. doi: 10.1186/1741-7015-8-18
Shah, S. (2022). Common terminology criteria for adverse events. Bethesda, MD: National Cancer Institute.
Shao, X., Ma, S. J., Casey, M., D'Orazio, L., Ringman, J. M., and Wang, D. J. J. (2019). Mapping water exchange across the blood-brain barrier using 3D diffusion-prepared arterial spin labeled perfusion MRI. Magn. Reson. Med. 81, 3065–3079. doi: 10.1002/mrm.27632
Smith, E. C., Pizzey, F. K., Askew, C. D., Mielke, G. I., Ainslie, P. N., Coombes, J. S., et al. (2021). Effects of cardiorespiratory fitness and exercise training on cerebrovascular blood flow and reactivity: a systematic review with meta-analyses. Am. J. Physiol. Heart Circ. Physiol. 321, H59–h76. doi: 10.1152/ajpheart.00880.2020
Solis-Urra, P., Molina-Hidalgo, C., García-Rivero, Y., Costa-Rodriguez, C., Mora-Gonzalez, J., Fernandez-Gamez, B., et al. (2023). Active gains in brain using exercise during aging (AGUEDA): protocol for a randomized controlled trial. Front. Hum. Neurosci. 17:1168549. doi: 10.3389/fnhum.2023.1168549
Stark, B., Johnson, C., and Roth, G. A. (2024). Global prevalence of coronary artery disease: an update from the global burden of disease study. J. Am. Coll. Cardiol. 83:2320. doi: 10.1016/S0735-1097(24)04310-9
Suzuki, Y., Helle, M., Koken, P., Van Cauteren, M., and van Osch, M. J. (2018). Simultaneous acquisition of perfusion image and dynamic MR angiography using time-encoded pseudo-continuous ASL. Magn. Reson. Med. 79, 2676–2684. doi: 10.1002/mrm.26926
Swain, R. A., Harris, A. B., Wiener, E. C., Dutka, M. V., Morris, H. D., Theien, B. E., et al. (2003). Prolonged exercise induces angiogenesis and increases cerebral blood volume in primary motor cortex of the rat. Neuroscience 117, 1037–1046. doi: 10.1016/S0306-4522(02)00664-4
Taylor, R. S., Brown, A., Ebrahim, S., Jolliffe, J., Noorani, H., Rees, K., et al. (2004). Exercise-based rehabilitation for patients with coronary heart disease: systematic review and meta-analysis of randomized controlled trials. Am. J. Med. 116, 682–692. doi: 10.1016/j.amjmed.2004.01.009
Taylor, J. L., Holland, D. J., Keating, S. E., Leveritt, M. D., Gomersall, S. R., Rowlands, A. V., et al. (2020). Short-term and Long-term feasibility, safety, and efficacy of high-intensity interval training in cardiac rehabilitation: the FITR heart study randomized clinical trial. JAMA Cardiol. 5, 1382–1389. doi: 10.1001/jamacardio.2020.3511
Taylor, J. L., Holland, D. J., Spathis, J. G., Beetham, K. S., Wisløff, U., Keating, S. E., et al. (2019). Guidelines for the delivery and monitoring of high intensity interval training in clinical populations. Prog. Cardiovasc. Dis. 62, 140–146. doi: 10.1016/j.pcad.2019.01.004
Timmis, A., Vardas, P., Townsend, N., Torbica, A., Katus, H., De Smedt, D., et al. (2022). European Society of Cardiology: cardiovascular disease statistics 2021. J. Eur. Heart J. 43, 716–799. doi: 10.1093/eurheartj/ehab892
Toval, A., Solis-Urra, P., Bakker, E. A., Sanchez-Aranda, L., Fernandez-Ortega, J., Prieto, C., et al. (2024) Exercise and brain health in patients with coronary artery disease: study protocol for the HEART-BRAIN randomized controlled trial. medRxiv. 2024:2024.05.22.24307744.
Troiano, R. P., Stamatakis, E., and Bull, F. C. (2020). How can global physical activity surveillance adapt to evolving physical activity guidelines? Needs, challenges and future directions. Br. J. Sports Med. 54, 1468–1473. doi: 10.1136/bjsports-2020-102621
Tsao, C. W., Aday, A. W., Almarzooq, Z. I., Anderson, C. A., Arora, P., Avery, C. L., et al. (2023). Heart disease and stroke statistics—2023 update: a report from the American Heart Association. Circulation 147, e93–e621. doi: 10.1161/CIR.0000000000001123
Tully, P. J., Cosh, S. M., and Baumeister, H. (2014). The anxious heart in whose mind? A systematic review and meta-regression of factors associated with anxiety disorder diagnosis, treatment and morbidity risk in coronary heart disease. J. Psychosom. Res. 77, 439–448. doi: 10.1016/j.jpsychores.2014.10.001
Vaccarino, V., Badimon, L., Bremner, J. D., Cenko, E., Cubedo, J., Dorobantu, M., et al. (2020). Depression and coronary heart disease: 2018 position paper of the ESC working group on coronary pathophysiology and microcirculation. Eur. Heart J. 41, 1687–1696. doi: 10.1093/eurheartj/ehy913
van Buchem, M. A., Biessels, G. J., Brunner la Rocca, H. P., de Craen, A. J., van der Flier, W. M., Ikram, M. A., et al. (2014). The heart-brain connection: a multidisciplinary approach targeting a missing link in the pathophysiology of vascular cognitive impairment. J. Alzheimers Dis. 42, S443–S451. doi: 10.3233/JAD-141542
Virani, S. S., Newby, L. K., Arnold, S. V., Bittner, V., Brewer, L. C., Demeter, S. H., et al. (2023). 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA guideline for the Management of Patients with Chronic Coronary Disease: a report of the American Heart Association/American College of Cardiology Joint Committee on clinical practice guidelines. Circulation 148, e9–e119. doi: 10.1161/CIR.0000000000001168
Wang, D. J., Alger, J. R., Qiao, J. X., Gunther, M., Pope, W. B., Saver, J. L., et al. (2013). Multi-delay multi-parametric arterial spin-labeled perfusion MRI in acute ischemic stroke – comparison with dynamic susceptibility contrast enhanced perfusion imaging. Neuro Image Clin. 3, 1–7. doi: 10.1016/j.nicl.2013.06.017
Wewege, M. A., Ahn, D., Yu, J., Liou, K., and Keech, A. (2018). High-intensity interval training for patients with cardiovascular disease—is it safe? A systematic review. J. Am. Heart Assoc. 7:e009305. doi: 10.1161/JAHA.118.009305
Williams, B., Mancia, G., Spiering, W., Agabiti Rosei, E., Azizi, M., Burnier, M., et al. (2018). 2018 ESC/ESH guidelines for the management of arterial hypertension. Eur. Heart J. 39, 3021–3104. doi: 10.1093/eurheartj/ehy339
Yu, H., Zhao, X., Wu, X., Yang, J., Wang, J., and Hou, L. (2023). High-intensity interval training versus moderate-intensity continuous training on patient quality of life in cardiovascular disease: a systematic review and meta-analysis. Sci. Rep. 13:13915. doi: 10.1038/s41598-023-40589-5
Zelazo, P. D., Anderson, J. E., Richler, J., Wallner-Allen, K., Beaumont, J. L., and Weintraub, S. II (2013). NIH toolbox cognition battery (CB): measuring executive function and attention. Monogr. Soc. Res. Child Dev. 78, 16–33. doi: 10.1111/mono.12032
Keywords: ischemic disease, coronary heart disease, cerebral blood flow, cognition, executive function, fitness, HIIT, resistance training (RT)
Citation: Toval A, Solis-Urra P, Bakker EA, Sánchez-Aranda L, Fernández-Ortega J, Prieto C, Alonso-Cuenca RM, González-García A, Martín-Fuentes I, Fernandez-Gamez B, Olvera-Rojas M, Coca-Pulido A, Bellón D, Sclafani A, Sanchez-Martinez J, Rivera-López R, Herrera-Gómez N, Peñafiel-Burkhardt R, López-Espinosa V, Corpas-Pérez S, García-Ortega MB, Vega-Cordoba A, Barranco-Moreno EJ, Morales-Navarro FJ, Nieves R, Caro-Rus A, Amaro-Gahete FJ, Mora-Gonzalez J, Vidal-Almela S, Carlén A, Migueles JH, Erickson KI, Moreno-Escobar E, García-Orta R, Esteban-Cornejo I and Ortega FB (2024) Exercise and brain health in patients with coronary artery disease: study protocol for the HEART-BRAIN randomized controlled trial. Front. Aging Neurosci. 16:1437567. doi: 10.3389/fnagi.2024.1437567
Edited by:
Henning Boecker, University Hospital Bonn, GermanyReviewed by:
Marcel Weber, University Hospital Bonn, GermanyFikru Belema Bedada, Howard University, United States
Copyright © 2024 Toval, Solis-Urra, Bakker, Sánchez-Aranda, Fernández-Ortega, Prieto, Alonso-Cuenca, González-García, Martín-Fuentes, Fernandez-Gamez, Olvera-Rojas, Coca-Pulido, Bellón, Sclafani, Sanchez-Martinez, Rivera-López, Herrera-Gómez, Peñafiel-Burkhardt, López-Espinosa, Corpas-Pérez, García-Ortega, Vega-Cordoba, Barranco-Moreno, Morales-Navarro, Nieves, Caro-Rus, Amaro-Gahete, Mora-Gonzalez, Vidal-Almela, Carlén, Migueles, Erickson, Moreno-Escobar, García-Orta, Esteban-Cornejo and Ortega. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Angel Toval, am9zZWFuZ2VsLnRvdmFsQHVnci5lcw==; Francisco B. Ortega, b3J0ZWdhZkB1Z3IuZXM=