 Gabriela Gonzalez Aleman1†
Gabriela Gonzalez Aleman1† George D. Vavougios2,3†
George D. Vavougios2,3† Carmela Tartaglia4,5†
Carmela Tartaglia4,5† Nalakath A. Uvais6
Nalakath A. Uvais6 Alla Guekht7,8
Alla Guekht7,8 Akram A. Hosseini9,10
Akram A. Hosseini9,10 Vincenzina Lo Re11,12Catterina Ferreccio13,14
Vincenzina Lo Re11,12Catterina Ferreccio13,14 Giovanni D'Avossa15Hernan P. Zamponi16Mariana Figueredo Aguiar17Agustin Yecora16,17Mohammad Zia Ul Haq Katshu18
Giovanni D'Avossa15Hernan P. Zamponi16Mariana Figueredo Aguiar17Agustin Yecora16,17Mohammad Zia Ul Haq Katshu18 Vasileios T. Stavrou2,3
Vasileios T. Stavrou2,3 Stylianos Boutlas2Konstantinos I. Gourgoulianis2Camila Botero1Francisco González Insúa1Santiago Perez-Lloret19
Stylianos Boutlas2Konstantinos I. Gourgoulianis2Camila Botero1Francisco González Insúa1Santiago Perez-Lloret19 Mikhail Zinchuk7Anna Gersamija7
Mikhail Zinchuk7Anna Gersamija7 Sofya Popova7
Sofya Popova7 Yulia Bryzgalova7
Yulia Bryzgalova7 Ekaterina Sviatskaya7
Ekaterina Sviatskaya7 Giovanna Russelli11,12
Giovanna Russelli11,12 Federica Avorio11,12
Federica Avorio11,12 Sophia Wang20,21
Sophia Wang20,21 Paul Edison22,23
Paul Edison22,23 Yoshiki Niimi24
Yoshiki Niimi24 Hamid R. Sohrabi25
Hamid R. Sohrabi25 Elizabeta B. Mukaetova Ladinska26,27Daria Neidre28
Elizabeta B. Mukaetova Ladinska26,27Daria Neidre28 Gabriel A. de Erausquin28,29,30*
Gabriel A. de Erausquin28,29,30*- 1Department of Psychology, School of Psychology and Psychopedagogy, Universidad Catolica Argentina, Buenos Aires, Argentina
- 2Department of Neurology, Medical School, University of Cyprus, Nicosia, Cyprus
- 3Department of Respiratory Medicine, University of Thessaly, Larissa, Greece
- 4Tanz Centre for Research in Neurodegenerative Diseases, University of Toronto, Toronto, ON, Canada
- 5Memory Clinic, Department of Neurology, Toronto Western Hospital, Toronto, ON, Canada
- 6Department of Psychiatry, Iqraa International Hospital and Research Centre, Calicut, India
- 7Department of Neurology, Moscow Research and Clinical Centre for Neuropsychiatry, Moscow, Russia
- 8Department of Neurology, Pirogov Russian National Research Medical University, Moscow, Russia
- 9Nottingham University Hospitals NHS Trust, Nottingham, United Kingdom
- 10Nottingham Sir Peter Mansfield Imaging Centre, University of Nottingham, Nottingham, United Kingdom
- 11Neurology Service, Department of Diagnostic and Therapeutic Services, IRCCS ISMETT, Palermo, Italy
- 12Department of Experimental Medicine and Clinical Neuroscience, University of Pittsburgh Medical Center (UPMC), Palermo, Italy
- 13Department of Public Health School of Medicine, Pontificia Universidad Catolica de Chile, Santiago, Chile
- 14Advanced Center for Chronic Diseases, ACCDiS, Santiago, Chile
- 15School of Psychology and Sports Sciences, Bangor University, Bangor, United Kingdom
- 16Secretariat for Mental Health and Addictions, Ministry of Health, Government of Jujuy, San Salvador de Jujuy, Argentina
- 17Instituto San Lazaro de Neurociencias, Fundacion de Lucha contra los Trastornos Neurologicos y Psiquiatricos en Minorias, FULTRA, San Salvador de Jujuy, Argentina
- 18Institute of Mental Health, University of Nottingham, Nottinghamshire Healthcare NHS Foundation Trust, Nottingham, United Kingdom
- 19Health Observatory, Vice Rectorate for Research, Universidad Catolica Argentina, Buenos Aires, Argentina
- 20Department of Psychiatry, Indiana University School of Medicine, Indianapolis, IN, United States
- 21Indiana Alzheimer's Disease Research Center, Indianapolis, IN, United States
- 22Department of Brain Sciences, Faculty of Medicine, Imperial College London, London, United Kingdom
- 23Cardiff University, Cardiff, United Kingdom
- 24Faculty of Medicine, University of Tokyo, Tokyo, Japan
- 25Murdoch University Centre for Healthy Ageing, School of Psychology, Murdoch University, Murdoch, WA, Australia
- 26Department of Psychology and Visual Sciences, University of Leicester, Leicester, United Kingdom
- 27The Evington Centre, Leicester General Hospital, Leicester, United Kingdom
- 28Laboratory for Brain Development, Modulation and Repair, Glenn Biggs Institute for Alzheimer's and Neurodegenerative Diseases, University of Texas Health San Antonio, San Antonio, TX, United States
- 29Laboratory of Electrophysiology Imaging, Radiology Research Institute, University of Texas Health San Antonio, San Antonio, TX, United States
- 30Department of Neurology, Joe & Teresa Long School of Medicine, University of Texas Health San Antonio, San Antonio, TX, United States
Cognitive changes associated with PASC may not be uniform across populations. We conducted individual-level pooled analyses and meta-analyses of cognitive assessments from eight prospective cohorts, comprising 2,105 patients and 1,432 controls from Argentina, Canada, Chile, Greece, India, Italy, Russia, and the UK. The meta-analysis found no differences by country of origin. The profile and severity of cognitive impairment varied by age, with mild attentional impairment observed in young and middle-aged adults, but memory, language, and executive function impairment in older adults. The risk of moderate to severe impairment doubled in older adults. Moderately severe or severe impairment was significantly associated with infection diagnoses (chi-square = 26.57, p ≤ 0.0001) and the severity of anosmia (chi-square = 31.81, p ≤ 0.0001). We found distinct age-related phenotypes of cognitive impairment in patients recovering from COVID-19. We identified the severity of acute illness and the presence of olfactory dysfunction as the primary predictors of dementia-like impairment in older adults.
Introduction
COVID-19 is a disease caused by the coronavirus SARS-CoV-2. SARS-CoV-2 infection can cause severe respiratory disease, resulting in pneumonia and death. COVID-19 has now spread to 222 countries and territories worldwide, with more than 704 million cases and >7 million deaths [worldometers.info/coronavirus]. Since its emergence, our understanding of COVID-19 has evolved to recognize its systemic features and potentially long-lasting consequences. As the exposure of the population to SARS-CoV-2 accelerated, these symptoms became increasingly recognized as a syndrome known as post-acute sequelae of COVID-19 (PASC) or long COVID (Nalbandian et al., 2021; Proal and VanElzakker, 2021).
Epidemiological studies suggest that PASC continues to have a global impact. In 2021, a systematic review of studies involving >250,000 survivors of COVID-19 found that PASC was evident in more than half, and PASC symptoms that persisted for 6 months or longer after the acute phase of infection affected multiple organs, leading to respiratory, cardiovascular and neurological symptoms (Groff et al., 2021). In an analysis of nearly 1.5 million COVID-19 patients followed up for 2 years after the initial infection, the risk for cognitive impairment remained higher in the group exposed to COVID-19 (Taquet et al., 2022). In 2022, the Human Phenotype Ontology meta-analyzed findings from 81 PASC cohorts, indicating that cognitive impairment and other neuropsychiatric symptoms were consistent symptoms in PASC (Deer et al., 2021).
Neuropsychiatric PASC may be distinct from other multi-systemic manifestations. This may be explained by a biological interplay between SARS-CoV-2 infection and neurodegeneration (de Erausquin et al., 2021; Li et al., 2022). For instance, levels of neurodegenerative biomarkers such as total tau, p-tau181, glial fibrillary acidic protein (GFAP), and neurofilament light (NfL) were increased following COVID-19 infection in patients without a history of neurodegenerative disease (Frontera et al., 2022). Notably, plasma NfL, a marker of axonal damage, was high after SARS-CoV-2 infection in the absence of neurological manifestations, (Verde et al., 2022) but in association with increased levels of inflammatory cytokines (Hirzel et al., 2022). An interpretation of these findings suggests that SARS-CoV-2 may damage the central nervous system either directly (Meinhardt et al., 2021), or mediated by an abnormal immune response (Jarius et al., 2022). Regardless of the underlying mechanism, data from the UK Biobank show brain volume reductions in limbic and olfactory pathways (Douaud et al., 2022), placing anosmia and cognitive deficits within the same syndromic spectrum (Deer et al., 2021; de Erausquin et al., 2021; Zamponi et al., 2021; Galderisi et al., 2024). Taken together, these associations between clinical phenotypes, imaging, and underlying biology indicate that neurocognitive disorders may be a distinct phenomenon among other PASC manifestations (de Erausquin et al., 2021; Frontera and Simon, 2022).
The impact of the pandemic has not been uniform across human groups or regions of the world. Notably, and beyond obvious comorbidities that increase the risk of various diseases, such as obesity or diabetes mellitus (Lee et al., 2024), susceptibility to the infection's deleterious effects has been higher across groups from specific ancestries. In the U.S.A., the highest morbidity and mortality rates were found in Amerindian minorities, followed by African Americans and Hispanics (Lundberg et al., 2023). Similarly, Amerindian (Maya) ancestry was associated with Southern Mexico's highest morbidity and mortality rates (Rangel-Méndez et al., 2023). In the U.K., the highest morbidity and mortality rates were reported for Bangladeshi and Pakistani minorities, followed by Black Africans and Black Caribbean [Office for National Statistics (ONS), 2023] Notably, these differential effects have disappeared after the Omicron variant of SARS-CoV-2 became prevalent [Office for National Statistics (ONS), 2023]. Therefore, substantial human host factors influence SARS-CoV-2 infection, and several recent studies point to genetics as the primary contributor (Nakanishi et al., 2021; Garg et al., 2024). A genetic predisposition may be causally linked to some (but not all) PASC symptoms (Shenoy et al., 2023; Tang et al., 2023).
Genetically based protein alterations can lead to large differences in differential response to SARS-CoV-2 infection, and some manifestations of PASC may be influenced by genetic variants shared with other diseases. For cognitive decline, the APOE gene has long been implicated in the risk of Alzheimer's disease, and the e4/e4 genotype has been shown to increase susceptibility to COVID-19, excess neuroinflammation, and reduced antiviral response (Kuo et al., 2020; Farrer et al., 1997; Severe Covid-19 GWAS Group et al., 2020). Thus, APOE may play a causal role in the severity of neurological symptoms in infection. SARS-CoV-2 infection significantly alters molecular pathways implicated in brain inflammation, and certain viral entry factors are highly expressed in cells in the blood-brain barrier. Indeed, PASC cognitive sequelae may resemble early Alzheimer's disease, and olfactory dysfunction may be an accurate predictor of the severity of cognitive sequelae (Gonzalez-Aleman et al., 2022).
In sum, cognitive changes associated with PASC may not be uniform across populations, and refining clinical phenotypes is essential to pursuing biomarkers of genetic studies in the future. We carried out individual-level pooled data analyses from Argentina, Canada, Chile, Greece, India, Italy, Russia, and the United Kingdom (UK), harmonizing following published protocols (de Erausquin et al., 2022) to define cognitive impairment profiles.
Results
Description of the overall sample
The whole sample consisted of 3,537 (2,105 infected and 1,432 uninfected controls, Table 1). Participants ranged in age from 18 to 97 years. The mean duration of formal education was 10.66 ± 4.5 years, and the mean age was 52.81 ± 15.76 years; 36.5% were men and 64.5% were women.
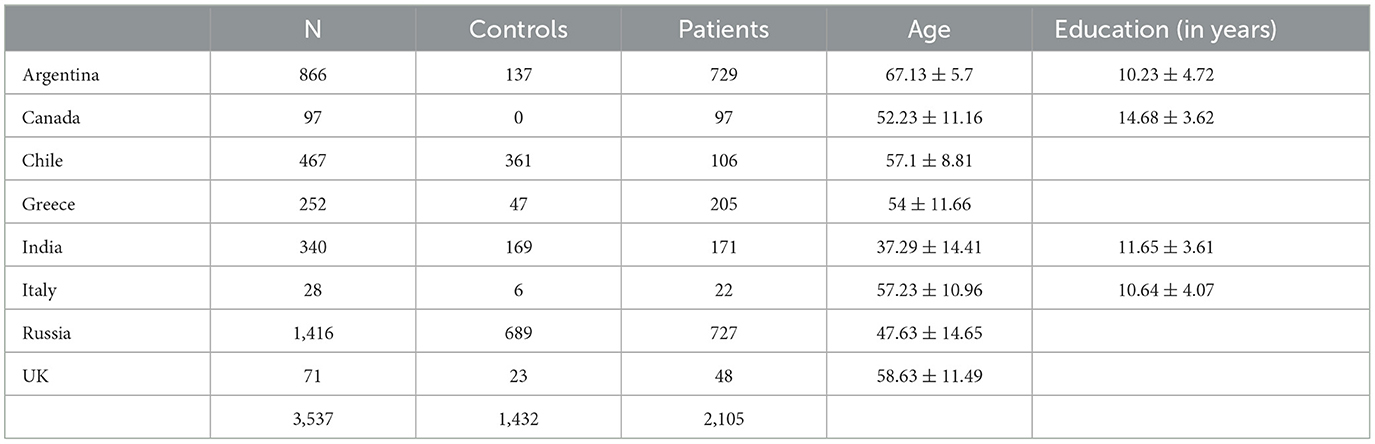
Table 1. Description of cohorts participants.
Pooled analysis of individual-level data
The cognitive performance of pooled, individual-level data was compared first task-wise for the entire sample. The infection performed significantly worse than the controls on the Trail Making Test (Part B), Symbol Digit Coding, Memory Delayed Recall, Recognition, Verbal Semantic Fluency (animals), and Naming (Figure 1). By contrast, a meta-analysis to test for differences between patients and controls by country of origin found that all patients showed impairment in executive function as indicated by performance only on the Trail Making Test-part B (Figure 2), suggesting loss of cognitive flexibility.
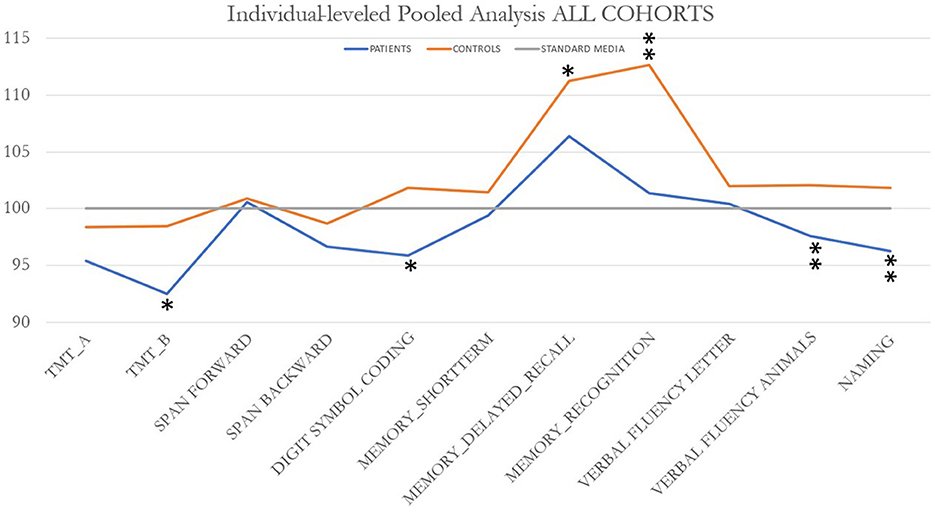
Figure 1. Profiles of cognitive impairment in PASC patients across all cohorts. Significant differences were found on Trail Making Test (Part B) (*p = 0.012); Symbol Digit Coding (Weschler intelligence battery; **p ≤ 0.0001); Memory delayed recall (**p = 0.009); recognition (**p < 0.0001), verbal semantic fluency (animals) (**p ≤ 0.0001); and naming (**p < 0.0001).
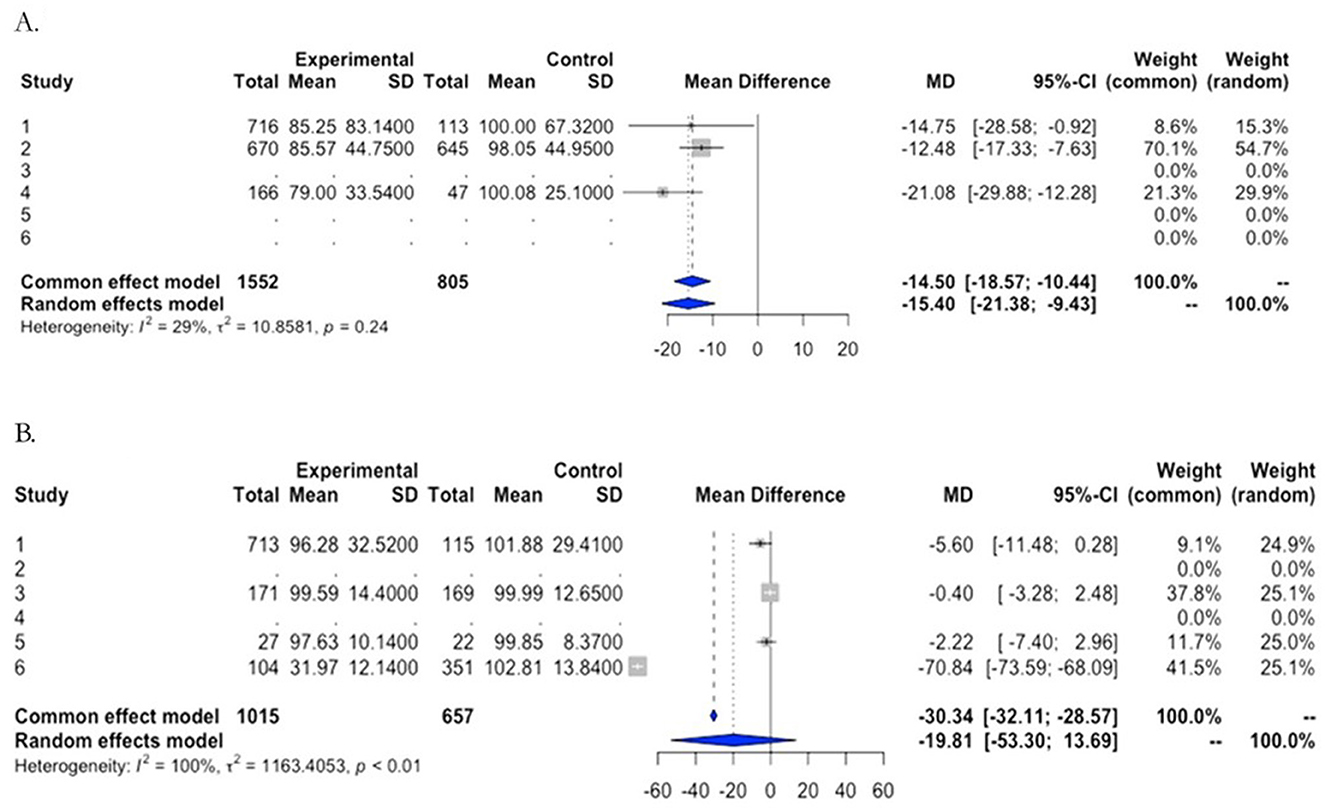
Figure 2. Meta-analyses of cognitive impairment by cohort. Forest plots of comparison of Trail Making Test B (A) and, as an example of a negative result, the Naming test (B).
Based on visual inspection of frequency plots by age, a bimodal distribution of overall impairment was identified, and an empirical cut-off point was identified at 59 years of age (Figure 3). Specifically, the distribution of mild cognitive impairment (1 domain only) by age was examined, along with the distribution of moderate to severe cognitive impairment (2 or 3 domains) (Figure 3). We tested the hypothesis of independence of these distributions and found it to be highly significant (t = −10.95, df = 642.86, p ≤ 0.0001). The median age in the mild cognitive decline group was 57.6, and in the moderate to severe cognitive impairment group, it was 65.8 years. Therefore, subjects 60 years of age or older (older adults) and subjects younger than 59 years of age (middle-aged and young adults) were treated as independent samples henceforth. The results are shown in Tables 2, 3.
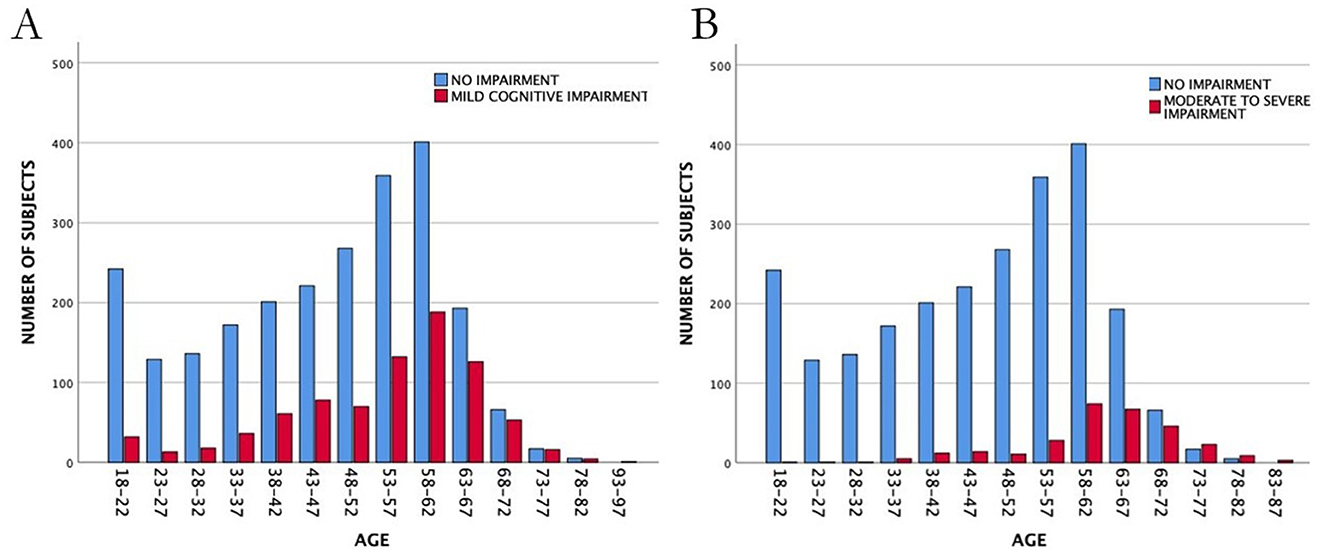
Figure 3. Frequency distributions for individuals with mild (A) or moderate to severe (B) cognitive impairment by age, regardless of diagnosis and across all cohorts. Whereas mild cognitive impairment follows a normal distribution largely overlapping (and not significantly different) from normal cognition, moderate to severe cognitive impairment is skewed toward older age and significantly different from the rest of the population (see main text).
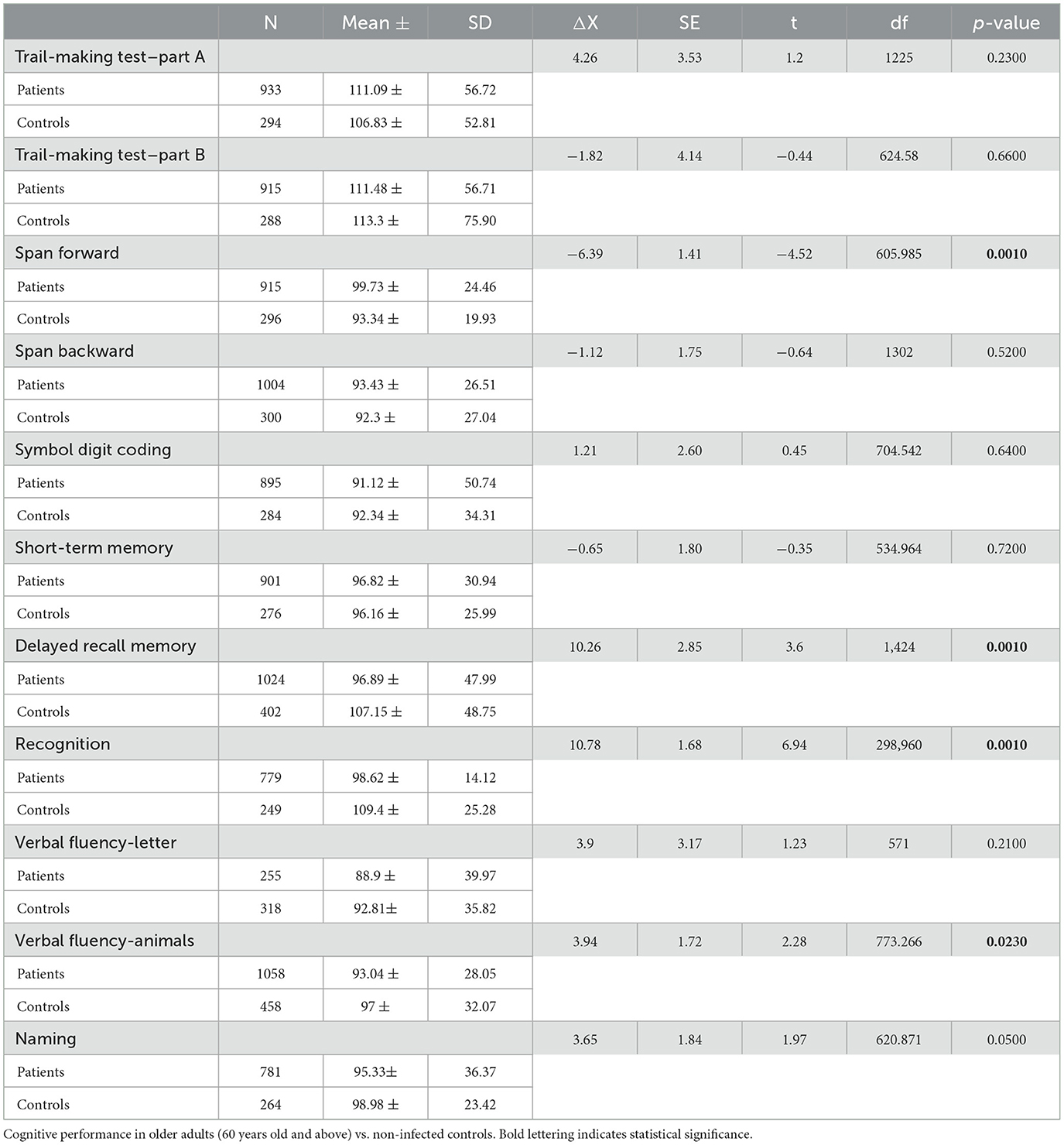
Table 2. Pooled data all cohorts.
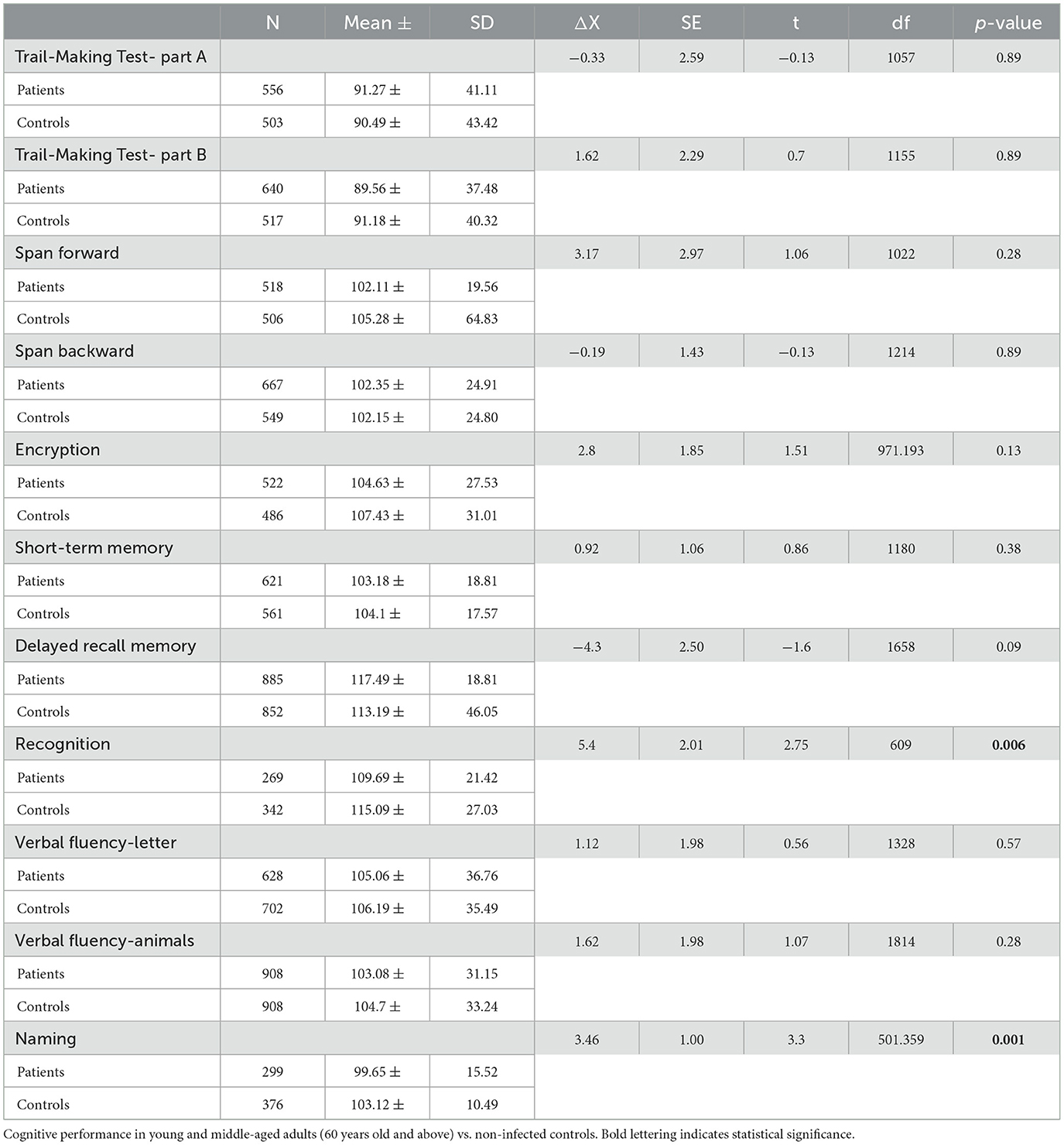
Table 3. Pooled data all cohorts.
Older adults were significantly impaired when compared to controls on Digit Span Forward performance (t = −4.52, p ≤ 0.001); delayed recall (t = 3.6, p < 0.001); recognition tasks (t = 6.94, p < 0.001); and the semantic verbal fluency task (t = 2.28, p = 0.02). In young and middle-aged adults, we found milder deficits in recognition and naming only (t = 2.75 and p = 0.006 and t = 3.3 and p = 0.001, respectively). Findings suggest mild attentional focus in young and middle-aged adults, whereas older adults display impairment in memory, language, and executive function.
Severity of impairment: age-dependent phenotypes
To classify the severity of impairment, we used the deficit criterion as a difference of 1.5 standard deviations in performance on the tests administered. In young and middle-aged adults, we obtained four groups with distinct cognitive performance (Table 4):
• normal cognition (68.2%).
• impairment in one cognitive dimension (23.4%).
• impairment in two cognitive dimensions (6.5%).
• impairment in three cognitive dimensions impaired (1.8%).
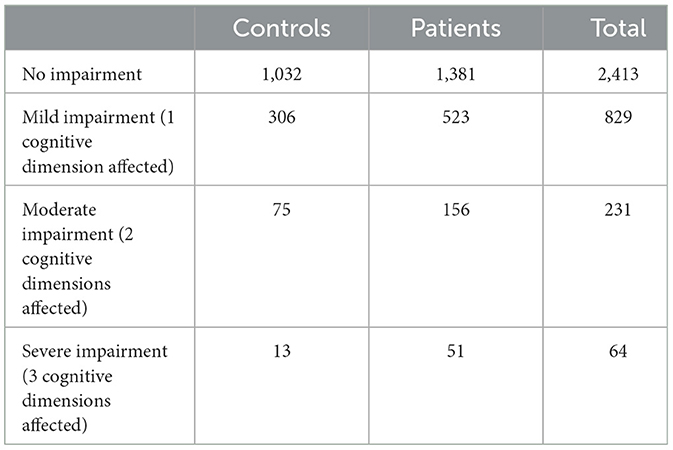
Table 4. Frequency of cognitive impairment in all cohorts with (patients) and without infection (controls).
By strong contrast, older adults showed a distribution skewed toward more severe impairment:
• normal cognition (68.2%).
• impairment in one cognitive dimension (30.1%).
• impairment in two cognitive dimensions (11.3%).
• impairment in three cognitive dimensions impaired (3.7%).
The odds ratio (OR) of moderate to severe cognitive impairment (2 or 3 cognitive dimensions affected) was calculated for the entire sample (OR = 1.75), for young and middle-aged adults (OR = 0.71), and older adults (OR = 1.49). Thus, the risk was doubled in older adults compared to middle-aged and young adults.
Predictors of risk of moderately severe or severe impairment
Moderately severe or severe impairment (2 or 3 dimensions) was significantly associated with infection diagnoses (chi-square = 26.57, p ≤ 0.0001) and with the presence and severity of anosmia (chi-square = 31.81, p ≤ 0.0001). No association was found between gender and cognitive dysfunction (chi-square = 0.74; p = 0.38) and between gender and anosmia (chi-square = 2.37; p = 0.12). The distribution of subjects by country is shown in Table 1, along with the average age and years of formal education; neither of these variables contributed to risk. On the other hand, the risk of moderate to severe cognitive impairment was nearly doubled in the presence of anosmia compared with its absence (OR = 1.89) (Table 5). Lastly, we also examined OR for cognitive impairment according to the severity of COVID-19 during the acute illness, considering the need for hospitalization, oxygen therapy, and admission to the intensive care unit. The risk of cognitive decline doubled when patients were hospitalized (OR = 2.06) or required intensive care (OR = 2.01). If they required oxygen therapy, the odds ratio was 1.47 (Table 6). Confidence intervals for each odds ratio are reported in Tables 5, 6, along with a normal deviation (z-statistic) calculated as ln(OR)/SE {ln(OR)} and the corresponding p-value.
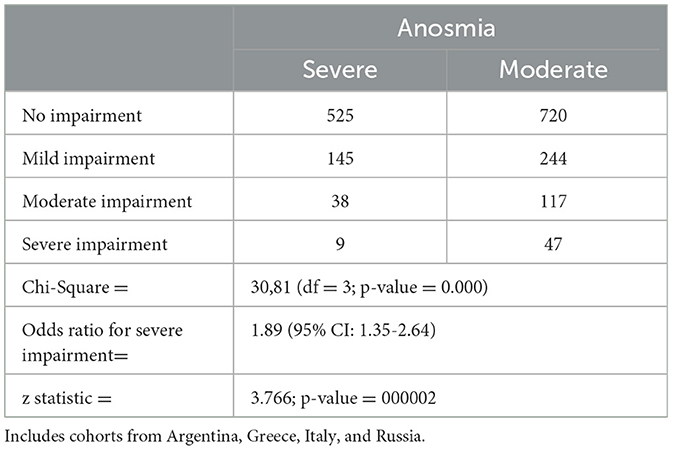
Table 5. Risk of severe cognitive impairment with moderate vs. severe anosmia.
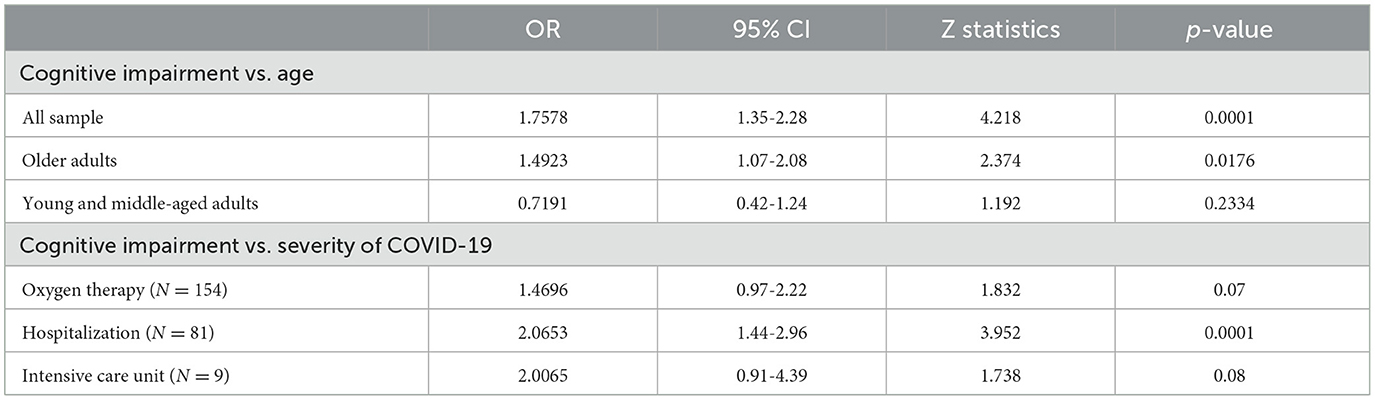
Table 6. Risk of severe cognitive impairment in young vs. older adults (top) and stratified by severity of acute COVID-19 illness.
Discussion
We studied multiple samples of adults exposed to SARS-CoV-2 infection and collected them in a variety of settings (community as well as polyclinics or hospitals) in developed and underdeveloped countries, including individuals from multiple under-represented ancestries. Our analysis confirms that cognitive deficits are frequently present, but with different phenotypes determined by age at exposure and severity of anosmia. Older age and anosmia were found to be risk factors for severe phenotypes of cognitive impairment consistent with dementia-like syndrome. On the other hand, meta-analysis identified impaired verbal fluency in cases vs. controls independent of age. Notably, we did not detect inter-sample differences, which could be attributed to ancestry effects.
Attentional skills and executive functioning were significantly impaired in younger patients (59 and younger) across cohorts, but deficits were both infrequent and mild. A systematic literature review and retrospective meta-analysis on slightly < 1,000 mostly European patients revealed that following COVID-19, patients suffer from impaired memory, attention, and executive function verbal and specifically verbal fluency, regardless of acute disease severity (Daroische et al., 2021), but nearly half of the assessments were carried out by phone, reducing accuracy. More consistent with our findings, a community sample of young and middle-aged (< 54 years old) from Canada identified significant impairments in executive function (measured and reported) associated with acute infection severity (Hall et al., 2022), and identical results were reported in a smaller sample in Russia (Manukyan et al., 2022), and the USA (Apple et al., 2022). Of note, mild subjective impairment in younger adults is disproportionate to objective findings on formal testing and is associated with pre-existing psychiatric complaints (Apple et al., 2022).
Older adults were at over twice the risk of suffering memory, language, and executive function impairment that would be indistinguishable from early Alzheimer's disease with mild to moderate dementia. Once again, this finding is consistent with multiple previous reports in the literature (de Erausquin et al., 2021; Galderisi et al., 2024; Li et al., 2022; Tang et al., 2023; Gonzalez-Aleman et al., 2022; Miners et al., 2020) and many others. Similarly, as in most of the published literature, anosmia was significantly associated with cognitive impairment (Gonzalez-Aleman et al., 2022; Global Burden of Disease Long COVID Collaborators et al., 2022; Llana et al., 2023, 2022; Sohrabi et al., 2012; Yahiaoui-Doktor et al., 2019) and specifically with memory loss in recovering COVID-19 patients (Gonzalez-Aleman et al., 2022; Llana et al., 2022; Sohrabi et al., 2012). The prevalence of dementia-like cognitive impairment in these cohorts strongly contrasts with the published prevalence of only 5% Alzheimer's type dementia in people aged 65 to 74 (Alzheimer's Association, 2024). Regardless of the presumed mechanism of PASC-related cognitive impairment, with current reported rates of infection worldwide, a sharp increase in dementia-like syndromes would place a massive strain on health systems already burdened by this problem in aging populations (Alzheimer's Association, 2024).
The relationship between neurodegeneration and olfactory dysfunction is well established. For instance, poor olfactory discrimination has been shown to predict cognitive decline in older community-dwelling adults (Sohrabi et al., 2012). In the population-based LIFE-Adult Study (n = 6,783), better olfactory function was associated with better performance on cognitive tests even after adjustment for known confounders (Yahiaoui-Doktor et al., 2019).
Older age, anosmia, and cognitive decline are correlated with Alzheimer's disease and related dementia (ADRD). Entorhinal cortex thinning and anosmia are early hallmarks of memory decline (Murphy, 2019). Indeed, memory function and olfaction are intrinsically connected via neuroanatomical and functional pathways, leading to the hypothesis that exposure of the olfactory network to SARS-CoV-2 infection could account for tandem anosmia and cognitive impairment in at least a subset of COVID-19 and produce ADRD-like neuropathology (de Erausquin et al., 2021; Zamponi et al., 2021; Gonzalez-Aleman et al., 2022; de Erausquin et al., 2022). The current findings confirm the interconnection of anosmia and cognitive impairment following SARS-CoV-2 infection in a multinational sample.
Several independent studies have also provided support for the neuropathological and functional substrate of this hypothesis. In mammalian animal models, the olfactory networks have been identified as a potential route of neuroinvasion for SARS-CoV-2, which was shown to infect both brain endothelial cells and neurons in rhesus monkey (Jiao et al., 2021) and nasal epithelial, olfactory sensory neurons, and hippocampal dendritic spines in rodents (Kishimoto-Urata et al., 2022). In humans, a post-mortem study of COVID-19 patients identified viral particles in the olfactory neurons and their projections (Thakur et al., 2021). These findings were associated with microgliosis and elevated neuroinflammatory markers in cerebrospinal fluid Thakur et al., 2021, and both findings have been independently confirmed (Boutajangout et al., 2021; Poloni et al., 2021). An extensive review of neuropathological findings in 184 patients who died from complications of acute COVID-19 found microglial activation in close to half and detectable virus in the human cerebrum, cerebellum, cranial nerves, olfactory bulb, as well as in the olfactory epithelium (Lou et al., 2021).
Whether viral particles can persist in surviving patients remains an open and much more complex question to address. As suggested above, inflammatory processes independent of neuroinvasion may mediate an alternate mechanism. Analysis of frontal lobe transcriptomes donated by COVID-19 patients revealed that exposure to SARS-CoV-2 was associated with molecular signatures of aging mediated by type I/III interferon (Mavrikaki et al., 2022). The same innate immune pathway is associated with Alzheimer's disease pathobiology and immune-mediated neuronal injury in rodents (Roy et al., 2022). More directly relevant to this discussion, post-mortem brain tissue donated by COVID-19 patients revealed abnormalities in shared pathways associated with Alzheimer's disease, including those involved innate immunity, tau hyperphosphorylation, as well as a site-specific calbindin hypoactivity in the hippocampus (Reiken et al., 2022). Lastly, interleukins IL-1β, IL-6, and tumor necrosis factor plasma levels are elevated in PASC sufferers (Schulthei et al., 2022), and are also correlated to cognitive impairment in Alzheimer's disease (Silva et al., 2021), and with severity of hyposmia after COVID-19 (Liang et al., 2022).
Stimulation of the peripheral immune system by a disease-associated molecular pattern (DAMP) has been shown to result in an upregulation of complement-related genes in the hippocampus, even in the case of sterile DAMPs (Michalovicz et al., 2015). In the context of COVID-19, induction of type I interferon signaling and proinflammatory cytokines may affect brain function via vascular pathways; alternatively, direct infection of the olfactory neuroepithelium may alter brain function via molecular mimicry or inflammatory events through its projections to areas in the extended olfactory network. These events and the molecules involved may trigger neurodegenerative diseases such as neuropathology (Vavougios et al., 2022). Aside from molecules that can mediate these events directly and, in a dose-response manner (e.g., IL-6), adult neurogenesis sites such as the hippocampi and the olfactory network would be particularly vulnerable, accounting for the selective vulnerability of these networks and the resulting anosmia-cognitive impairment phenotype we report on. Of course, our results do not exclude other possible interpretations, such as vascular lesions or dysfunction of the olfactory pathway.
The results of our study should be interpreted in the context of its strengths and potential limitations. The main strength of our study is the use of prospective, harmonized data from a global collaboration of scientists working in different settings and with many underrepresented populations. The pooled analysis of individual-level data provides a unique insight into the phenotypes and clinical associations of cognitive impairment following COVID-19, which show several consistent aspects across centers. This was possible due to the inclusion of long-running cohorts functioning in the real-world setting initiated at the beginning of the pandemic. Another significant strength is that in most published studies, cognitive dysfunction may affect hospitalized patients in general, aside from diagnosis, whereas our cohorts include largely community-based samples with only an accurately proportional number of hospitalized cases.
Conversely, the most relevant limitation of our study is that this is a pooled analysis of heterogeneous studies rather than a multicentre study. Our approach's merit lies in assessing what amounts to real-world data and different approaches in diverse healthcare settings. For example, the population in Thessaly, Greece, represents an admixture of rural and urban areas and a small island complex. Similarly, data from the Canadian site is multi-ethnic as they serve a diverse community in an urban center, and the data from Argentina describe an Amerindian population rarely included in multinational studies. The heterogeneity of variables included in the analysis per study is another potential limitation. Studies included varying degrees of clinical, demographic, anthropometric, neuropsychological, fitness, and respiratory function assessments. Covariate analyses have accounted for these differences as far as reasonable.
We found distinct age-related phenotypes of cognitive impairment in patients recovering from COVID-19. Premorbid complaints emerged as the major predictor of mild impairment in young and middle-aged adults. In contrast, the severity of acute illness and the presence of olfactory dysfunction were the primary predictors of dementia-like impairment in older adults.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by multiple committees as samples from several countries are included. Approvals are available. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
GE: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Writing – original draft, Writing – review & editing. GG: Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. GV: Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Writing – original draft, Writing – review & editing. CT: Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Writing – review & editing. NU: Data curation, Funding acquisition, Investigation, Methodology, Writing – review & editing. AGu: Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Writing – review & editing. AH: Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Writing – review & editing. VL: Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Writing – review & editing. CF: Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Writing – review & editing. GD'A: Formal analysis, Methodology, Writing – review & editing. HZ: Data curation, Investigation, Writing – review & editing. MF: Data curation, Funding acquisition, Investigation, Methodology, Writing – review & editing. AY: Data curation, Funding acquisition, Investigation, Methodology, Writing – review & editing. MU: Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Writing – review & editing. VS: Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Writing – review & editing. SB: Data curation, Investigation, Methodology, Writing – review & editing. KG: Conceptualization, Funding acquisition, Investigation, Methodology, Writing – review & editing. CB: Data curation, Formal analysis, Writing – review & editing. FG: Data curation, Formal analysis, Methodology, Writing – review & editing. SP-L: Formal analysis, Methodology, Writing – review & editing. MZ: Data curation, Investigation, Methodology, Writing – review & editing. AGe: Data curation, Investigation, Methodology, Writing – review & editing. SP: Data curation, Investigation, Methodology, Writing – review & editing. YB: Data curation, Investigation, Methodology, Writing – review & editing. ES: Data curation, Investigation, Writing – review & editing. GR: Data curation, Investigation, Writing – review & editing. FA: Data curation, Investigation, Writing – review & editing. SW: Methodology, Writing – review & editing. PE: Methodology, Writing – review & editing. YN: Methodology, Writing – review & editing. HS: Methodology, Writing – review & editing. EBM-L: Conceptualization, Methodology, Writing – review & editing. DN: Investigation, Project administration, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The authors were funded completely of partially by: Fundacion FULTRA, Argentina (GG, HZ, AY, MF), National Institute of Aging Grants # U19AG076581, P30AG059305, and P30AG066546 (GE), ISIDORe (PID: 23245) (GV), COVALENT study, included herein received funding from EU-OSHA (SB, KG), University Hospital Foundation (CT), IQRAA International Hospital and Research Center, Calicut, Kerala, India (NU, MU), Italian Health Ministry, Ricerca Corrente 2023 (VL, GR, FA), ANID/CONICYT FONDECYT Regular 1212066; ANID/FONDAP/15130011 (CF), NIA K23AG06255, NIA R21AG074179, NIA P30AG072976 (SW), JPND/Italian Ministry/(European Union) Medical Research Council and National Institute for Health Research, UK (PE), Western Australia Department of Jobs, Tourism, Science and Innovation grant for the Effect of COVID-19 on mental health of the elderly (HS). In addition, GV, KG, and VS would like to thank the personnel of the COVID-19 outpatient clinic and as well as research collaborators on long COVID research: Nico Biagi, Dimitrios Mysiris, Kyriaki Astara, Eleana Pitaraki, Konstantinos Tourlakopoulos, Eirini Papayianni, Glykeria Tsirimona, Ílias E. Dimeas, Pelagia Foka, Olga Papaggeli, Georgia Xiromerisiou, Sotirios Zarogiannis, Zoe Daniil 2, and Georgios Hadjigeorgiou.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Alzheimer's Association (2024). Alzheimer's Disease Facts and Figures. Alzheimers. Dement. 2024:20. Available at: https://www.alz.org/media/Documents/alzheimers-facts-and-figures.pdf
Apple, A. C., Oddi, A., Peluso, M. J., Asken, B. M., Henrich, T. J., Kelly, J. D., et al. (2022). Risk factors and abnormal cerebrospinal fluid associate with cognitive symptoms after mild COVID-19. Ann. Clin. Transl. Neurol. 9, 221–226. doi: 10.1002/acn3.51498
Boutajangout, A., Frontera, J., Debure, L., Vedvyas, A., Faustin, A., Wisniewski, T., et al. (2021). Plasma biomarkers of neurodegeneration and neuroinflammation in hospitalized COVID-19 patients with and without new neurological symptoms. Alzheimers. Dement. 17:57892. doi: 10.1002/alz.057892
Daroische, R., Hemminghyth, M. S., Eilertsen, T. H., Breitve, M. H., and Chwiszczuk, L. J. (2021). Cognitive impairment after COVID-19-a review on objective test data. Front. Neurol. 12:699582. doi: 10.3389/fneur.2021.699582
de Erausquin, G. A., Snyder, H., Brugha, T. S., Seshadri, S., Carrillo, M., Sagar, R., et al. (2022). Chronic neuropsychiatric sequelae of SARS-CoV-2: protocol and methods from the Alzheimer's Association Global Consortium. Alzheimers Dement. 8:e12348. doi: 10.1002/trc2.12348
de Erausquin, G. A., Snyder, H., Carrillo, M., Hosseini, A. A., Brugha, T. S., Seshadri, S., et al. (2021). The chronic neuropsychiatric sequelae of COVID-19: the need for a prospective study of viral impact on brain functioning. Alzheimer's and Dementia 17, 1056–1065. doi: 10.1002/alz.12255
Deer, R. R., Rock, M. A., Vasilevsky, N., Carmody, L., Rando, H., Anzalone, A. J., et al. (2021). Characterizing long COVID: deep phenotype of a complex condition. EBioMedicine 74:103722. doi: 10.1016/j.ebiom.2021.103722
Douaud, G., Lee, S., Alfaro-Almagro, F., et al. (2022). SARS-CoV-2 is associated with changes in brain structure in UK Biobank. Nature 604, 697–707. doi: 10.1038/s41586-022-04569-5
Farrer, L. A., Cupples, L. A., Haines, J. L., Hyman, B., Kukull, W. A., Mayeux, R., et al. (1997). Effects of age, sex, and ethnicity on the association between apolipoprotein E genotype and Alzheimer disease - a meta-analysis. JAMA-J Am Med Assoc 278, 1349–1356. doi: 10.1001/jama.1997.03550160069041
Frontera, J. A., Boutajangout, A., Masurkar, A. V., Betensky, R. A., Ge, Y., Vedvyas, A., et al. (2022). Comparison of serum neurodegenerative biomarkers among hospitalized COVID-19 patients versus non-COVID subjects with normal cognition, mild cognitive impairment, or Alzheimer's dementia. Alzheimers. Dement. 18, 899–910. doi: 10.1002/alz.12556
Frontera, J. A., and Simon, N. M. (2022). Bridging knowledge gaps in the diagnosis and management of neuropsychiatric sequelae of COVID-19. JAMA Psychiatry 79, 811–817. doi: 10.1001/jamapsychiatry.2022.1616
Galderisi, S., Perrottelli, A., Giuliani, L., Pisaturo, M. A., Monteleone, P., Pagliano, P., et al. (2024). Cognitive impairment after recovery from COVID-19: frequency, profile, and relationships with clinical and laboratory indices. Eur. Neuropsychopharmacol. 79, 22–31. doi: 10.1016/j.euroneuro.2023.11.001
Garg, E., Arguello-Pascualli, P., Vishnyakova, O., Halevy, A. R., Yoo, S., Brooks, J. D., et al. (2024). Canadian COVID-19 host genetics cohort replicates known severity associations. PLoS Genet. 20:e1011192. doi: 10.1371/journal.pgen.1011192
Global Burden of Disease Long COVID Collaborators, Hanson, S. W., Abbafati, C., Aerts, J. G., Al-Aly, Z., Ashbaugh, C., et al. (2022). Estimated global proportions of individuals with persistent fatigue, cognitive, and respiratory symptom clusters following symptomatic COVID-19 in 2020 and 2021. JAMA 328, 1604–1615. doi: 10.1001/jama.2022.18931
Gonzalez-Aleman, G., Zamponi, H. P., Juarez-Aguaysol, L., Bahl, A., Sanchez, D., Reyes-Dumeyer, D., et al. (2022). Olfactory dysfunction but not COVID-19 severity predicts severity of cognitive sequelae following SARS-CoV-2 infection in Amerindian older adults. Alzheimer's Dementia 18:e066868. doi: 10.1002/alz.066868
Groff, D., Sun, A., Ssentongo, A. E., Ba, D. M., Parsons, N., Poudel, G. R., et al. (2021). Short-term and long-term rates of postacute sequelae of SARS-CoV-2 infection: a systematic review. JAMA Network Open 4:e2128568. doi: 10.1001/jamanetworkopen.2021.28568
Hall, P. A., Meng, G., Hudson, A., Sakib, M. N., Hitchman, S. C., MacKillop, J., et al. (2022). Cognitive function following SARS-CoV-2 infection in a population-representative Canadian sample. Brain Behav Immun Health 21:100454. doi: 10.1016/j.bbih.2022.100454
Hirzel, C., Grandgirard, D., Surial, B., Wider, M. F., Leppert, D., Kuhle, J., et al. (2022). Neuro-axonal injury in COVID-19: the role of systemic inflammation and SARS-CoV-2 specific immune response. Ther. Adv. Neurol. Disord. 15:17562864221080528. doi: 10.1177/17562864221080528
Jarius, S., Pache, F., Körtvelyessy, P., Jelčić, I., Stettner, M., Franciotta, D., et al. (2022). Cerebrospinal fluid findings in COVID-19: a multicenter study of 150 lumbar punctures in 127 patients. J. Neuroinflammation 19:19. doi: 10.1186/s12974-021-02339-0
Jiao, L., Yang, Y., Yu, W., Zhao, Y., Long, H., Gao, J., et al. (2021). The olfactory route is a potential way for SARS-CoV-2 to invade the central nervous system of rhesus monkeys. Signal Transd. Target. Ther. 6:169. doi: 10.1038/s41392-021-00591-7
Kishimoto-Urata, M., Urata, S., Kagoya, R., Imamura, F., Nagayama, S., Reyna, R. A., et al. (2022). Prolonged and extended impacts of SARS-CoV-2 on the olfactory neurocircuit. Sci. Rep. 12:5728. doi: 10.1038/s41598-022-09731-7
Kuo, C. L., Pilling, L. C., Atkins, J. L., Masoli, J. A. H., Delgado, J., Kuchel, G. A., et al. (2020). APOE e4 genotype predicts severe COVID-19 in the UK Biobank Community Cohort. J. Gerontol. A Biol. Sci. Med. Sci. 75, 2231–2232. doi: 10.1093/gerona/glaa131
Lee, A., Seo, J., Park, S., Cho, Y., Kim, G., Li, J., et al. (2024). Type 2 diabetes and its genetic susceptibility are associated with increased severity and mortality of COVID-19 in UK Biobank. Commun Biol. 7:122. doi: 10.1038/s42003-024-05799-1
Li, C., Liu, J., Lin, J., and Shang, H. (2022). COVID-19 and risk of neurodegenerative disorders: A Mendelian randomization study. Transl. Psychiatry 12:283. doi: 10.1038/s41398-022-02052-3
Liang, Y., Mao, X., Kuang, M., Zhi, J., Zhang, Z., Bo, M., et al. (2022). Interleukin-6 affects the severity of olfactory disorder: a cross-sectional survey of 148 patients who recovered from Omicron infection using the Sniffin' Sticks test in Tianjin, China. Int. J. Infect. Dis. 123, 17–24. doi: 10.1016/j.ijid.2022.07.074
Llana, T., Mendez, M., Garces-Arilla, S., Hidalgo, V., Mendez-Lopez, M., Juan, M. C., et al. (2023). Association between olfactory dysfunction and mood disturbances with objective and subjective cognitive deficits in long-COVID. Front. Psychol. 14:1076743. doi: 10.3389/fpsyg.2023.1076743
Llana, T., Mendez, M., Zorzo, C., Fidalgo, C., Juan, M.-. C., et al. (2022). Anosmia in COVID-19 could be associated with long-term deficits in the consolidation of procedural and verbal declarative memories. Front. Neurosci. 16:1082811. doi: 10.3389/fnins.2022.1082811
Lou, J. J., Movassaghi, M., Gordy, D., Olson, M. G., Zhang, T., Khurana, M. S., et al. (2021). Neuropathology of COVID-19 (neuro-COVID): clinicopathological update. Free Neuropathol. 2:2–2. doi: 10.17879/freeneuropathology-2021-2993
Lundberg, D. J., Wrigley-Field, E., Cho, A., Raquib, R., Nsoesie, E. O., Paglino, E., et al. (2023). COVID-19 mortality by race and ethnicity in US metropolitan and nonmetropolitan areas, March 2020 to February (2022). JAMA Netw Open. 6:e2311098. doi: 10.1001/jamanetworkopen.2023.11098
Manukyan, P., Deviaterikova, A., Velichkovsky, B. B., and Kasatkin, V. (2022). The impact of mild COVID-19 on executive functioning and mental health outcomes in young adults. Healthcare 10:1891. doi: 10.3390/healthcare10101891
Mavrikaki, M., Lee, J. D., Solomon, I. H., and Slack, F. J. (2022). Severe COVID-19 is associated with molecular signatures of aging in the human brain. Nature Aging 2, 1130–1137. doi: 10.1038/s43587-022-00321-w
Meinhardt, J., Radke, J., Dittmayer, C., Franz, J., Thomas, C., Mothes, R., et al. (2021). Olfactory transmucosal SARS-CoV-2 invasion as a port of central nervous system entry in individuals with COVID-19. Nat. Neurosci. 24, 168–175. doi: 10.1038/s41593-020-00758-5
Michalovicz, L. T., Lally, B., and Konat, G. W. (2015). Peripheral challenge with a viral mimic upregulates expression of the complement genes in the hippocampus. J. Neuroimmunol. 285, 137–142. doi: 10.1016/j.jneuroim.2015.06.003
Miners, S., Kehoe, P. G., and Love, S. (2020). Cognitive impact of COVID-19: looking beyond the short term. Alzheimers. Res. Ther. 12:170. doi: 10.1186/s13195-020-00744-w
Murphy, C. (2019). Olfactory and other sensory impairments in Alzheimer disease. Nature Rev. Neurol. 15, 11–24. doi: 10.1038/s41582-018-0097-5
Nakanishi, T., Pigazzini, S., Degenhardt, F., Cordioli, M., Butler-Laporte, G., Maya-Miles, D., et al. (2021). Age-dependent impact of the major common genetic risk factor for COVID-19 on severity and mortality. J. Clin. Invest. 131:e152386. doi: 10.1172/JCI152386
Nalbandian, A., Sehgal, K., Gupta, A., Madhavan, M. V., McGroder, C., Stevens, J. S., et al. (2021). Post-acute COVID-19 syndrome. Nat. Med. 27, 601–615. doi: 10.1038/s41591-021-01283-z
Office for National Statistics (ONS) (2023). Updating Ethnic and Religious Contrasts in Deaths Involving Coronavirus (COVID-19):24 January 2020 to 23 November 2022. Washington, DC: U.S. Census Bureau.
Poloni, T. E., Medici, V., Moretti, M., Vison,à, S. D., Cirrincione, A., Carlos, A. F., et al. (2021). COVID-19-related neuropathology and microglial activation in elderly with and without dementia. Brain Pathol. 31:e12997. doi: 10.1111/bpa.12997
Proal, A. D., and VanElzakker, M. B. (2021). Long COVID or post-acute sequelae of COVID-19 (PASC): an overview of biological factors that may contribute to persistent symptoms. Front. Microbiol. 12:698169. doi: 10.3389/fmicb.2021.698169
Rangel-Méndez, J. A., Jaimes-Gurrusquieta, L., Sánchez-Cruz, J. F., Zarate-Murillo, M. I., Domínguez-Méndez, J., Laviada-Molina, H. A., et al. (2023). Characteristics of COVID-19 and mortality-associated factors during the first year of the pandemic in southeast Mexico. Future Microbiol. 18, 1147–1157. doi: 10.2217/fmb-2023-0052
Reiken, S., Sittenfeld, L., Dridi, H., Liu, Y., Liu, X., Marks, A. R., et al. (2022). Alzheimer's-like signaling in brains of COVID-19 patients. Alzheimer's Dement. 18, 955–965. doi: 10.1002/alz.12558
Roy, E. R., Chiu, G., Li, S., Propson, N. E., Kanchi, R., Wang, B., et al. (2022). Concerted type I interferon signaling in microglia and neural cells promotes memory impairment associated with amyloid β plaques. Immunity 55, 879–894. doi: 10.1016/j.immuni.2022.03.018
Schulthei,ß, C., Willscher, E., Paschold, L., Gottschick, C., Klee, B., Henkes, S.-S., et al. (2022). The IL-1β, IL-6, and TNF cytokine triad is associated with post-acute sequelae of COVID-19. Cell Rep Med. 3:100663. doi: 10.1016/j.xcrm.2022.100663
Severe Covid-19 GWAS Group, Ellinghaus, D., Degenhardt, F., Bujanda, L., Buti, M., Albillos, A., et al. (2020). Genomewide association study of severe Covid-19 with respiratory failure. N. Engl. J. Med. 383, 1522–1534. doi: 10.1056/NEJMoa2020283
Shenoy, P. U., Udupa, H., Ks, J., Babu, S., Jain, N., Das, R., et al. (2023). The impact of COVID-19 on pulmonary, neurological, and cardiac outcomes: evidence from a Mendelian randomization study. Front Public Health. 11:1303183. doi: 10.3389/fpubh.2023.1303183
Silva, N. M. L. E., Gonçalves, R. A., Pascoal, T. A., Lima-Filho, R. A. S., Resende, E., Vieira, E. L. M, et al. (2021). Pro-inflammatory interleukin-6 signaling links cognitive impairments and peripheral metabolic alterations in Alzheimer's disease. Transl. Psychiatry 11:251. doi: 10.1038/s41398-021-01349-z
Sohrabi, H. R., Bates, K. A., Weinborn, M. G., Johnston, A. N., Bahramian, A., Taddei, K., et al. (2012). Olfactory discrimination predicts cognitive decline among community-dwelling older adults. Transl. Psychiatry 2, e118–e118. doi: 10.1038/tp.2012.43
Tang, C. M., Li, G., and Cheung, C. L. (2023). COVID-19 and cognitive performance: a Mendelian randomization study. Front Public Health. 11:1185957. doi: 10.3389/fpubh.2023.1185957
Taquet, M., Sillett, R., Zhu, L., Mendel, J., Camplisson, I., Dercon, Q., et al. (2022). Neurological and psychiatric risk trajectories after SARS-CoV-2 infection: an analysis of 2-year retrospective cohort studies including 1 284 437 patients. Lancet Psychiatry 9, 815–827. doi: 10.1016/S2215-0366(22)00260-7
Thakur, K. T., Miller, E. H., Glendinning, M. D., Al-Dalahmah, O., Banu, M. A., Boehme, A. K., et al. (2021). COVID-19 neuropathology at Columbia University Irving Medical Center/New York Presbyterian Hospital. Brain 144, 2696–2708. doi: 10.1093/brain/awab148
Vavougios, G. D., de Erausquin, G. A., and Snyder, H. M. (2022). Type I interferon signaling in SARS-CoV-2 associated neurocognitive disorder (SAND): mapping host-virus interactions to an etiopathogenesis. Front. Neurol. 13:1063298. doi: 10.3389/fneur.2022.1063298
Verde, F., Milone, I., Bulgarelli, I., Peverelli, S., Colombrita, C., Maranzano, A., et al. (2022). Serum neurofilament light chain levels in Covid-19 patients without major neurological manifestations. J. Neurol. 2022, 1–11. doi: 10.1007/s00415-022-11233-5
Yahiaoui-Doktor, M., Luck, T., Riedel-Heller, S. G., Loeffler, M., Wirkner, K., Engel, C., et al. (2019). Olfactory function is associated with cognitive performance: results from the population-based LIFE-Adult-Study. Alzheimer's Res. Ther. 11:43. doi: 10.1186/s13195-019-0494-z
Zamponi, H. P., Juarez-Aguaysol, L., Kukoc, G., Dominquez, M. E., Pini, B., Padilla, E. G., et al. (2021). Olfactory dysfunction and chronic cognitive impairment following SARS-CoV-2 infection in a sample of older adults from the Andes mountains of Argentina. Alzheimers. Dement. 17:e057897. doi: 10.1002/alz.057897
Keywords: COVID-19, cognitive decline, international cohort, age-dependent, long COVID
Citation: Gonzalez Aleman G, Vavougios GD, Tartaglia C, Uvais NA, Guekht A, Hosseini AA, Lo Re V, Ferreccio C, D'Avossa G, Zamponi HP, Figueredo Aguiar M, Yecora A, Ul Haq Katshu MZ, Stavrou VT, Boutlas S, Gourgoulianis KI, Botero C, González Insúa F, Perez-Lloret S, Zinchuk M, Gersamija A, Popova S, Bryzgalova Y, Sviatskaya E, Russelli G, Avorio F, Wang S, Edison P, Niimi Y, Sohrabi HR, Mukaetova Ladinska EB, Neidre D and de Erausquin GA (2025) Age-dependent phenotypes of cognitive impairment as sequelae of SARS-CoV-2 infection. Front. Aging Neurosci. 16:1432357. doi: 10.3389/fnagi.2024.1432357
Received: 13 May 2024; Accepted: 28 October 2024;
Published: 07 January 2025.
Edited by:
Fabrizia D'Antonio, Sapienza University of Rome, ItalyReviewed by:
Christian Barbato, National Research Council (CNR), ItalyBeatrice Paradiso, University of Milan, Italy
Copyright © 2025 Gonzalez Aleman, Vavougios, Tartaglia, Uvais, Guekht, Hosseini, Lo Re, Ferreccio, D'Avossa, Zamponi, Figueredo Aguiar, Yecora, Ul Haq Katshu, Stavrou, Boutlas, Gourgoulianis, Botero, González Insúa, Perez-Lloret, Zinchuk, Gersamija, Popova, Bryzgalova, Sviatskaya, Russelli, Avorio, Wang, Edison, Niimi, Sohrabi, Mukaetova Ladinska, Neidre and de Erausquin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gabriel A. de Erausquin, ZGVlcmF1c3F1aW5nQHV0aHNjc2EuZWR1
†These authors have contributed equally to this work