 Ying Ge
Ying Ge Wowa Zhao
Wowa Zhao
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Aging Neurosci. , 24 June 2024
Sec. Parkinson’s Disease and Aging-related Movement Disorders
Volume 16 - 2024 | https://doi.org/10.3389/fnagi.2024.1399285
This article is part of the Research Topic Effectiveness of Exercise and Diet on Movement Disorders View all 9 articles
Aim: To investigate the correlation between motor function and health-related quality of life (HrQOL) in early to mid-stage patients with Parkinson disease (PwP).
Methods: This cross-sectional study recruited PwP from April 2020 to December 2023 at the outpatient clinic of Peking Union Medical College Hospital in Beijing, China. The motor symptoms were assessed using Movement Disorder Society–sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) part 3. Balance function was evaluated using the Berg Balance Scale (BBS), and the risk of fall using Timed Up-and-Go test (TUG), and Five Times Sit-to-Stand test (FTSST). Freezing of gait questionnaire (FOGQ) was used to evaluate the severity of gait. The Intelligent Device for Energy Expenditure and Physical Activity (IDEEA) recorded gait cycle parameters, and the isokinetic dynamometer measured muscle strength. The Parkinson’s Disease Questionnaire-39 (PDQ-39) was used to measure HrQOL. All assessments were tested during the on state. Spearman correlation was conducted to evaluate the correlation between motor function and HrQOL.
Results: 243 patients with mean age of 69.33 years were enrolled. The PDQ-39 score was strongly correlated with FOG in H&Y stage III (r = 0.653, p < 0.001) and moderately correlated in H&Y stage I (r = 0.471, p < 0.001) and H&Y stage II (r = 0.386, p < 0.001). Furthermore, the FOG was strongly correlated with mobility domain at H&Y stage III (r = 0.694, p < 0.001) and moderately correlated at H&Y stage I (r = 0.431, p < 0.001) and H&Y stage II (r = 0.434, p < 0.001). All motor function scores were correlated with PDQ-39 scores at H&Y stage III (p < 0.05).
Conclusion: Motor function correlated with HrQOL in early to mid-stage PwP, and FOG was the main factor, especially affecting mobility, activities of daily life and communication. HrQOL in patients at different disease stages were variously affected by motor function, and HrQOL and multiple dimensions was significantly associated with motor function in patients at H&Y stage III.
Parkinson’s disease (PD) is a chronic progressive neurodegenerative disorder characterized by both motor and non-motor symptoms (Bloem et al., 2021). The prevalence of PD is increasing among elderly patients in China (Qi et al., 2021). The main motor features are resting tremor, bradykinesia, rigidity, shuffling gait, and postural instability, which have negative impacts on health-related quality of life (HrQOL) of PwP (Beitz, 2014). Early in the course of the disease, symptoms are usually mild, the drug response is usually reliable and the patient functions well. As the disease progresses, there is an increasing impact on and dependence on activities of daily living (Sveinbjornsdottir, 2016).
There is an increasing clinical focus on HrQOL which provides a multi-dimensional view of the patient’s well-being, and a guiding principle for researchers and clinicians (Bock et al., 2022). Strong evidence indicates that motor and non-motor symptoms in PwP limit their independence, essential activities of daily living and social participation. Impairment in these domains can alter social roles by affecting employment status, home management, friendships, and other relationships. Conversely, a decline in HrQOL can have a negative impact on motor and non-motor symptoms (Galeoto et al., 2022).
Previous studies (Gomez-Esteban et al., 2007; Kurihara et al., 2020; Bock et al., 2022) have demonstrated a significant negative correlation between motor symptoms and HrQOL. However, their assessments were self-reported and did not specifically explore which aspect of motor symptoms had the determinant impact on HrQOL at different disease stages. Scalzo et al. (2012) recruited thirty-six patients and found that the impairment in balance while performing functional activities and the reduction in walking capacity negatively affect the perception of HrQOL. But the study had some limitation such as small sample size and incomplete assessment of motor function. There are numerous studies (San Martín Valenzuela et al., 2020; Szefler-Derela et al., 2020; Li et al., 2021) showing improvements in motor function and quality of life through rehabilitation. However, there is still a lack of consensus on how to implement more effective rehabilitation training programs. Therefore, this observational cross-sectional study aims to investigate the relationship between motor function and HrQOL across different disease severity and hypothesizes that balance function and risk of falling would have the greatest impact on HrQOL.
This cross-sectional observational study was approved by the Ethics Committee and Institutional Review Board of the Peking Union Medical College Hospital and written informed consent was obtained from each patient before beginning the study.
The inclusion criteria were as follows: (a) diagnosis of primary Parkinson’s disease according to the Movement Disorder Society Clinical Diagnostic Criteria for Parkinson’s disease, (b) Hoehn and Yahr (H&Y) stages I-III, (c) stable medication regimen for at least 4 weeks before the study. Exclusion criteria included (a) atypical Parkinson’s syndrome, (b) severe nervous system disease other than PD or motor system disease, (c) severe cognitive disorder, or mental disorder, (d) severe visual or hearing impairment, (e) poor compliance, (f) refusal to sign the written informed consent.
First, patients completed the demographic questionnaire, including patients’ information, height, weight, BMI (weight in kilograms divided by the square of height in meters). Then the balance function, risk of fall, FOGQ, MDS-UPDRS, lower extremity muscle strength and HrQOL were evaluated, respectively. H&Y stages and drug On-phase were provided by a neurologist and all assessments were performed in 1 day and in the drug On-phase by a physical therapist.
HrQOL was ascertained by the PDQ-39 (The 39-item Parkinson’s disease questionnaire), a tool for the systematic assessment of the impact of PD on an individual’s quality of life. It is a well-validated measure using 5 levels of severity to measure health status of 8 domains, including mobility (10 items), activities of daily living (6 items), emotional well-being (6 items), stigma (4 items), social support (3 items), cognitions (4 items), communication (3 items) and bodily discomfort (3 items) (Jenkinson et al., 1997). The higher scores indicate lower levels of quality of life. The Chinese version PDQ-39 was proved a reliable and valid measure in both research and clinical trials (Zhang and Chan, 2012).
The Berg balance scale (BBS) is a 14-item test, using scores from 0 to 4 for each item, designed to measure static and dynamic standing balance. The total score ranges from 0 to 56, with higher scores indicating better balance, and a score of less than 46 out of 56 indicates the presence of risk falls (Alagumoorthi et al., 2022).
The timed up-and-go test (TUG), and the five times sit to stand test (FTSST) were used to evaluate the risk of fall of PwP. The TUG Test measured the time in which participants take to rise from the chair, walk at a normal, self-selected pace to a line marked on a hardwood floor three meters from the start line, turn around, walk back to the chair and sit down (Nightingale et al., 2019). The proposed cut-off score of 11.5 s was suggested for discriminating between PwP who did and did not fall (Nocera et al., 2013). The FTSST measured the time in which participants take to stand up and sit down as quickly as possible for five repetitions (Goldberg et al., 2012). The proposed cut-off score for discrimination between PwP who did and did not fall was 16.0 s (Duncan et al., 2011).
Temporal–spatial gait parameters of PD were acquired using IDEEA activity monitor (Minisun, Fresno, CA) (de la Cámara et al., 2019). Participants completed four flat 10 m walking trials with the device on as required by the test. The data collected on stride length, stride speed and foot angle off the ground are used as the main indicators to assess the PD patient’s walking function.
Knee flexor and extensor isokinetic peak torque were evaluated using the isokinetic dynamometer (ISOMOVE, Tecnobody Company, Italy) (Hasan et al., 2021). Participants were seated on the dynamometer, and the belts were used at the thigh, pelvis, and trunk to avoid compensatory movements. The testing procedure consisted of respective five knee flexor and extensor contractions. Participants were asked to perform the movement with their maximal strength.
The MDS-UPDRS is the most widely used clinical scoring system to measure the severity and progression of PD (Martinez-Martin et al., 2015). MDS-UPDRS Part III evaluates 18 motor examination items by the rater (Ueno et al., 2020). Each item is scored from 0 to 4, with higher scores indicating poorer motor function.
Summary statistics, including means and standard deviations for continuous variables, and counts and percentages for categorical data, were employed for variable description. The Spearman correlation coefficient r was used to evaluate the correlation between PDQ-39 and motor function. Correlations were deemed weak when coefficients were < 0.30, moderate from 0.30 to 0.59, and strong >0.60 (Yoon et al., 2017). The significance level was set at p = 0.05. Statistical analyses were performed with SPSS 25.0 (SPSS Inc., Chicago, IL, United States).
243 PD patients, aged 60 to 80 years old, admitted to the department of rehabilitation in Peking Union Medical College Hospital from April 2020 to December 2023 were recruited. Patients had a mean age 69.33 years (SD = 6.61), with 45.7% being women. Demographic and clinical characteristics of PwP at different H&Y stages are shown in Table 1.
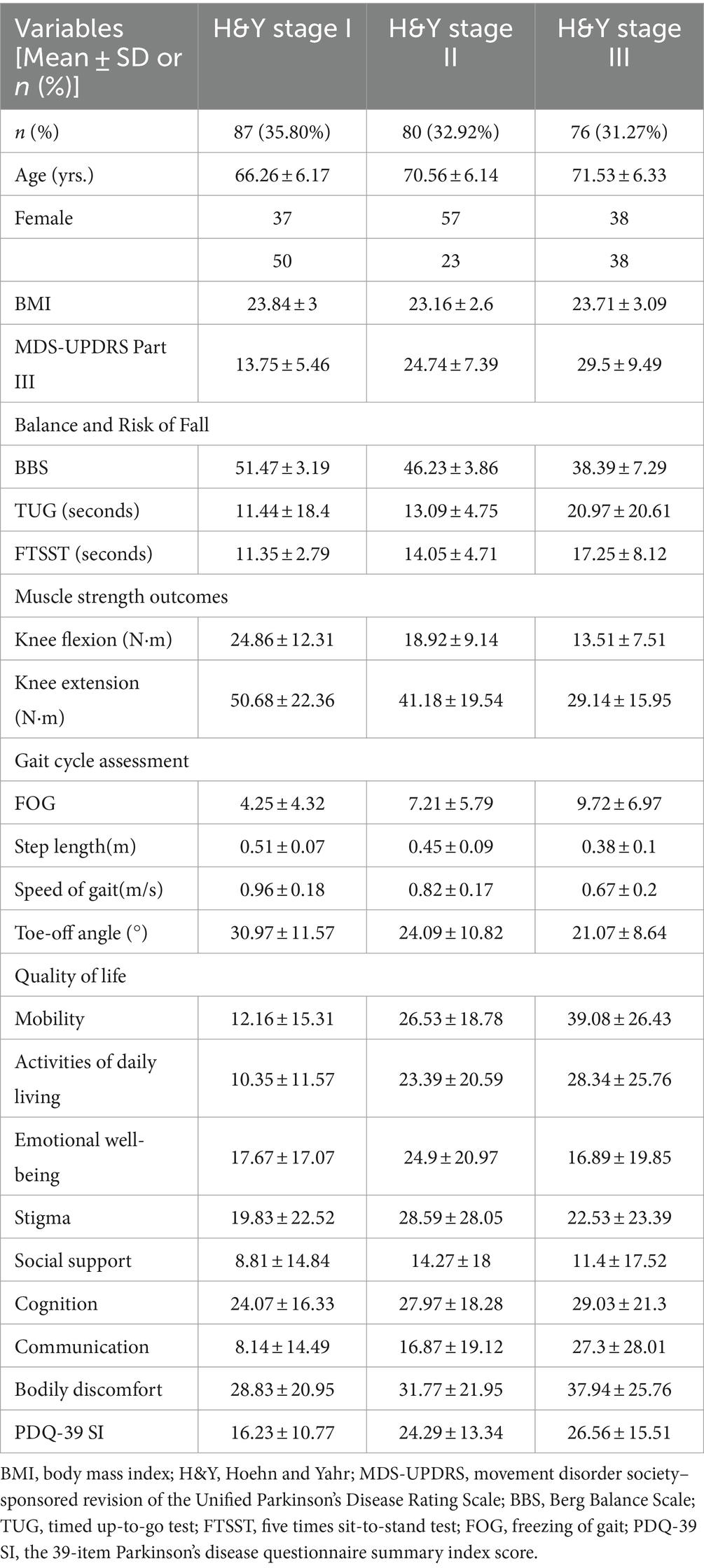
Table 1. Demographic and clinical features of patients with Parkinson’s disease among different H&Y stages (PD) (n = 243).
Correlation analyses were conducted to evaluate different association of motor function and HrQOL at different H&Y stages (Table 2). The PDQ-39 score was strongly correlated with FOG at H&Y stage III (r = 0.653, p < 0.001) and moderately correlated at H&Y stage I (r = 0.471, p < 0.001) and H&Y stage II (r = 0.386, p < 0.001). Additionally, the PDQ-39 score was significantly correlated with MDS-UPDRS Part III, TUG, step length and toe off angle at H&Y stage I, and BBS, TUG and FTSST at H&Y stage II. All motor function scores were correlated with PDQ-39 scores at H&Y stage III (p < 0.05). This study found that age and BMI had no evident correlation with PDQ-39 SI (p < 0.05).
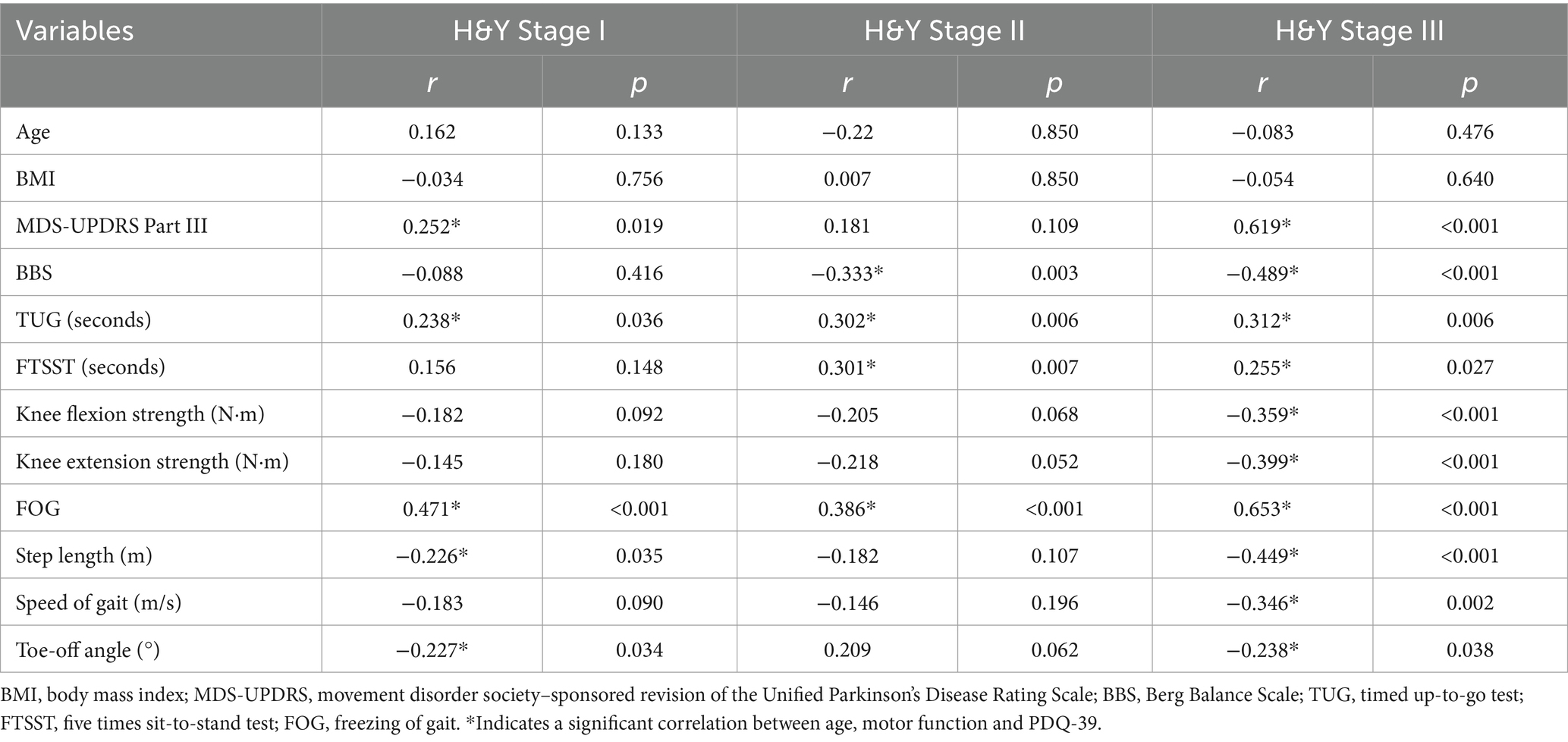
Table 2. Coefficient of correlation of Spearman (r) and p-value between age, motor function and PDQ-39 among different H&Y stages.
Then, the correlation between motor function and the 8 dimensions of PDQ-39 was further analyzed (Table 3). The FOG was strongly correlated with mobility at H&Y stage III (r = 0.694, p < 0.001) and moderately correlated at H&Y stage I (r = 0.431, p < 0.001) and H&Y stage II (r = 0.434, p < 0.001). And mobility was correlated with all motor function assessment scores at H&Y stage III (p < 0.001), with FOG and BBS score being the most correlated factors. UPDRS Part III, FOG and BBS were the most correlated factors of activities of daily life at H&Y stage II & III (p < 0.001). Furthermore, communication was strongly correlated with UPDRS Part III and FOG at H&Y stage III (p < 0.001).
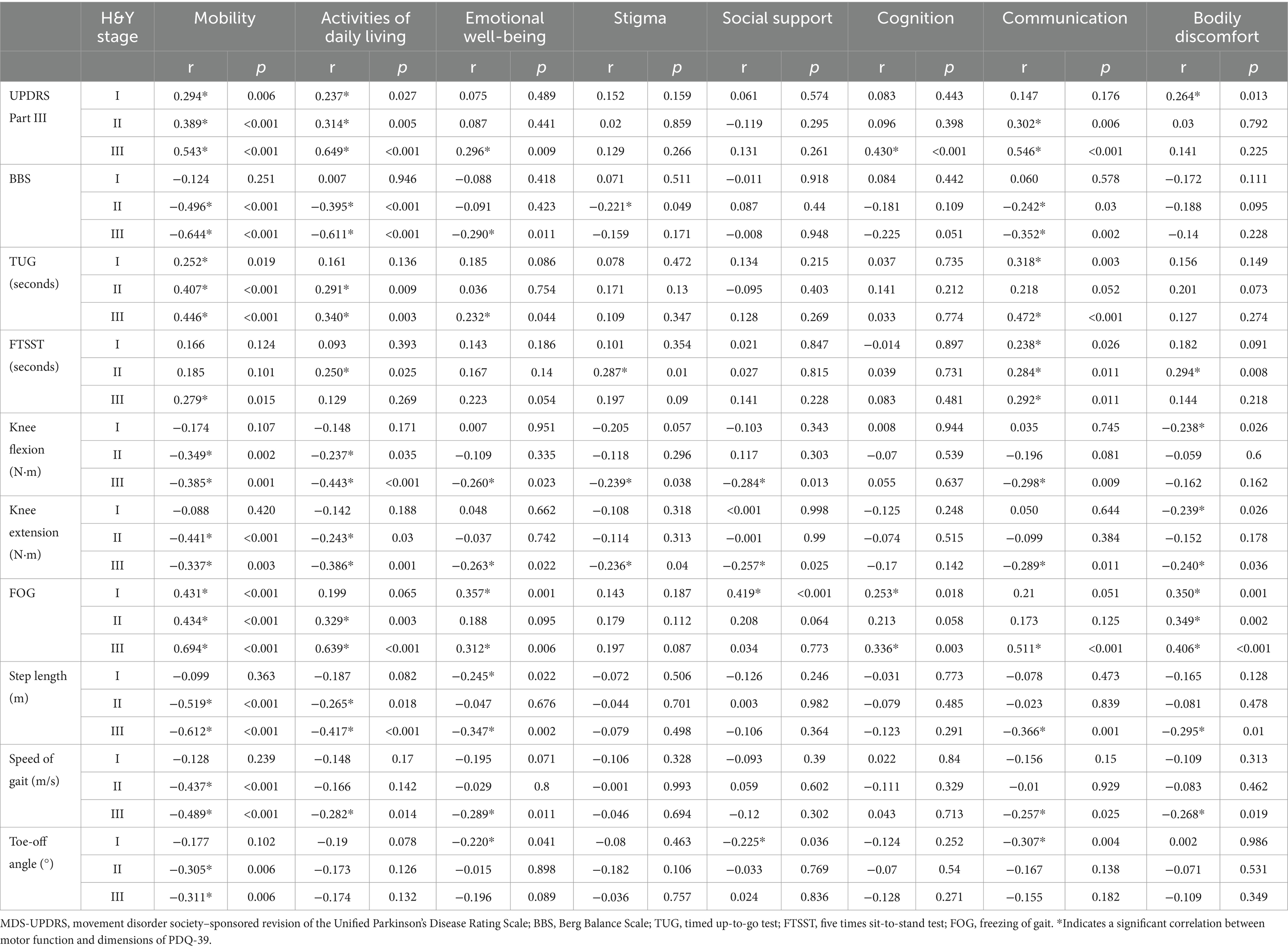
Table 3. Coefficient of correlation of Spearman between motor function and dimensions of PDQ-39.
PD is a progressive multi-system neurodegenerative disease affecting people mainly in later years of life. Treatment should focus on functional capacity and quality of life throughout the entire course of disease (Barbosa et al., 2022). However, rehabilitation training is likely to have a more obvious impact in the early to mid-stage of the disease and may prevent or slow down further functional decline (Kluger et al., 2014). This study aims to identify the most impaired motor function caused by the disease and the most relevant HrQOL factors, and then provide a target for rehabilitation training to improve HrQOL in early to mid-stage PD.
FOG is a unique and disabling clinical phenomenon characterized by brief episodes of inability to step or by extremely short steps that typically occur on initiating gait or on turning while walking. Physiological, functional imaging, and clinical pathological studies point to disturbances in frontal cortical regions, the basal ganglia, and the midbrain locomotor region as the probable origins of FOG (Gao et al., 2020). FOG is very common in PD and one of the most relevant features of PD closely related to falls (Bloem et al., 2004; Bekkers et al., 2018; Zhang et al., 2021). Frequent falls lead to injury, fear of falling, reduced mobility and social isolation (Thanvi and Treadwell, 2010). Mehdizadeh et al. (2016) showed that regardless of balance impairments, fear of fall has a negative association with HRQOL in PwP. This study showed that FOG was correlated with HrQOL at H&Y stages I ~ III,which accord with the finding of Ellis et al. (2011) and Nakano et al. (2021). Further analysis showed FOG was correlated with mobility, ADL, and communication. Previous study (Cosentino et al., 2020) proved that physical therapy may improve FOG, for instance, action observation, treadmill combined with cueing, and prolonged home-based exercise trainings. In this study, step length and speed of gait have moderate correlation and toe-off angle had weak correlation with PDQ-39 SI at H&Y stages III, which mainly affected mobility domain. In rehabilitation practice, targeted training, e.g., LSVT BIG (Flood et al., 2020) can be made to address these gait problems of patients.
This study found the moderate association between balance function and HrQOL at H&Y stages II& III, but with no significant association at H&Y stages I. This study shows that patients at H&Y stage I have the highest BBS score and little or mild balance impairment, which is not significantly associated with their HrQOL. Poor balance will lead to poor HrQOL (Nakano et al., 2021), which was found in patients at H&Y stages II& III in this study. Meanwhile, Scalzo et al. (2012) found that patients with severe balance dysfunctions assessed by the BBS and who scored lower distances in the 6 min walking test had worse HrQOL. Furthermore, longer time of TUG and FTSST led to poor HrQOL, which means that high risk of fall negatively affected HrQOL. According to the further analysis, BBS, TUG and FTSST mainly affected mobility and ADL domains. Bailey et al. (2022) also found that PwP who performed better on the 4 m walk speed test, the standing balance test, had higher scores on the total PDQ-39, mobility, ADL, cognition and bodily discomfort domains. Conventional understanding suggests that patients at H&Y stage II do not experience balance symptoms, but this study showed that their balance function had deteriorated and negatively affected their HrQOL. Therefore, balance training should be considered earlier in clinical practice.
Muscle strength in PwP is impaired compared with healthy controls (Skinner et al., 2019; Renee et al., 2021), with the largest deficits observed in the lower extremity in the “OFF” medication state and of concentric contractions (Gamborg et al., 2023). Yokote et al. (2022) found that lower muscle strength correlates with gait performance in advanced Parkinson Disease. As a meta-analysis (Hart et al., 2023) reported that the prevalence of probable sarcopenia, a condition associated with the loss of skeletal muscle strength and mass, ranged from 23.9–66.7% in the PwP population. This study showed moderately correlation between knee strength and HrQOL in patients at H&Y stages III. Therefore, muscle strength training, especially in patients at H&Y stages III may improve in gait performance and HrQOL and prevent the presence of sarcopenia.
This study found that motor function correlated with HrQOL especially in mobility and activities of life. The most interesting finding of the current study showed that motor function has strong correlation with communication at H&Y stages III. Communication impairment is common in PD and may be due to motor language control and cognitive-linguistic disorder (Smith and Caplan, 2018). PDQ-39 has one question on speech and two question on communication with other people. Motor function assessments represent disease severity and the relationship with motor language control or cognitive-linguistic disorder should be further explored.
Strengths of the study include the identification of FOG as the most important factor affecting HRQOL, and the differential association between motor function and HRQOL in patients at different H&Y stages, supported by a robust sample size. Additionally, the potential correlation between motor function and communication function warrants further investigation. However, this study has some limitations. This analysis was cross-sectional and therefore conclusions were restricted to one point in time. Therefore, further studies should be done to investigate whether increasing or decreasing motion function results in HrQOL changes in PwP. In the future, there will be a need for a larger and longer cohort.
In conclusion, motor function correlated with HrQOL in early to mid-stages PwP, and FOG was the main factor, especially in mobility, activities of daily life and communication. In addition, HrQOL was correlated with gait and risk of fall at H&Y stage I, and gait, balance, and risk of fall at H&Y stages II. All motor function were associated with HrQOL and multiple dimensions in patients at H&Y stage III. Therefore, Physical therapy should be targeted according to disease stages to obtain the most improvement of HrQOL.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the Ethics Committee and Institutional Review Board of the Peking Union Medical College Hospital. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
YG: Formal analysis, Writing – original draft. WZ: Investigation, Writing – review & editing. LZ: Project administration, Methodology, Writing – review & editing. XZ: Supervision, Writing – review & editing. XS: Writing – review & editing. JL: Writing – review & editing. YL: Conceptualization, Funding acquisition, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by Beijing Municipal Commission of Science and Technology under Grant number Z191100004419009.
The authors thank Dr. Xinhua Wan, Dr. Lei Qiao and Dr. Honglin Hao for their kind support and help in the diagnosis and drug treatment of the patients. We are grateful to the patients and their family participating in this study. The work reported in this article would be incredible without them.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Alagumoorthi, G., Beulah Jebakani, D., Thirunavukarasu, S., Ramachandaran, V., and Kumaresan, A. (2022). Effectiveness of Wii sports-based strategy training in reducing risk of falling, falls and improving quality of life in adults with idiopathic Parkinson's disease-a randomized comparative trial. Clin. Rehabil. 36, 1097–1109. doi: 10.1177/02692155221089030
Bailey, M., Anderson, S., Stebbins, G., Barnes, L., Shulman, L. M., Tartakovsky, J., et al. (2022). Comparison of motor, non-motor, and quality of life phenotype in black and white patients with Parkinson's disease. Parkinsonism Relat. Disord. 96, 18–21. doi: 10.1016/j.parkreldis.2022.01.018
Barbosa, E. R., Limongi, J. C. P., Chien, H. F., Barbosa, P. M., and Torres, M. R. C. (2022). How I treat Parkinson's disease. Arq. Neuropsiquiatr. 80, 94–104. doi: 10.1590/0004-282X-ANP-2022-S126
Beitz, J. M. (2014). Parkinson's disease: a review. Front. Biosci. (Schol. Ed.) 6, 65–74. doi: 10.2741/s415
Bekkers, E. M. J., Dijkstra, B. W., Heremans, E., Verschueren, S. M. P., Bloem, B. R., and Nieuwboer, A. (2018). Balancing between the two: are freezing of gait and postural instability in Parkinson's disease connected? Neurosci. Biobehav. Rev. 94, 113–125. doi: 10.1016/j.neubiorev.2018.08.008
Bloem, B. R., Hausdorff, J. M., Visser, J. E., and Giladi, N. (2004). Falls and freezing of gait in Parkinson's disease: a review of two interconnected, episodic phenomena. Mov. Disord. 19, 871–884. doi: 10.1002/mds.20115
Bloem, B. R., Okun, M. S., and Klein, C. (2021). Parkinson's disease. Lancet 397, 2284–2303. doi: 10.1016/S0140-6736(21)00218-X
Bock, M. A., Brown, E. G., Zhang, L., and Tanner, C. (2022). Association of Motor and Nonmotor Symptoms with Health-Related Quality of life in a large online cohort of people with Parkinson disease. Neurology 98, e2194–e2203. doi: 10.1212/WNL.0000000000200113
Cosentino, C., Baccini, M., Putzolu, M., Ristori, D., Avanzino, L., and Pelosin, E. (2020). Effectiveness of physiotherapy on freezing of gait in Parkinson's disease: a systematic review and meta-analyses. Mov. Disord. 35, 523–536. doi: 10.1002/mds.27936
de la Cámara, M., Higueras-Fresnillo, S., Martinez-Gomez, D., and Veiga, Ó. L. (2019). Interday reliability of the IDEEA activity monitor for measuring movement and nonmovement Behaviors in older adults. J. Aging Phys. Act. 27, 141–154. doi: 10.1123/japa.2017-0365
Duncan, R. P., Leddy, A. L., and Earhart, G. M. (2011). Five times sit-to-stand test performance in Parkinson's disease. Arch. Phys. Med. Rehabil. 92, 1431–1436. doi: 10.1016/j.apmr.2011.04.008
Ellis, T., Cavanaugh, J. T., Earhart, G. M., Ford, M. P., Foreman, K. B., and Dibble, L. E. (2011). Which measures of physical function and motor impairment best predict quality of life in Parkinson's disease? Parkinsonism Relat. Disord. 17, 693–697. doi: 10.1016/j.parkreldis.2011.07.004
Flood, M. W., O'Callaghan, B. P. F., Diamond, P., Liegey, J., Hughes, G., and Lowery, M. M. (2020). Quantitative clinical assessment of motor function during and following LSVT-BIG (R) therapy. J. Neuroeng. Rehabil. 17:92. doi: 10.1186/s12984-020-00729-8
Galeoto, G., Berardi, A., Colalelli, F., Pelosin, E., Mezzarobba, S., Avanzino, L., et al. (2022). Correlation between quality of life and severity of Parkinson's disease by assessing an optimal cut-off point on the Parkinson's disease questionnaire (PDQ-39) as related to the Hoehn & Yahr (H & Y) scale. Clin. Ter. 173, 243–248. doi: 10.7417/CT.2022.2427
Gamborg, M., Hvid, L. G., Thrue, C., Johansson, S., Franzen, E., Dalgas, U., et al. (2023). Muscle strength and power in people with Parkinson disease: a systematic review and meta-analysis. J. Neurol. Phys. Ther. 47, 3–15. doi: 10.1097/NPT.0000000000000421
Gao, C., Liu, J., Tan, Y., and Chen, S. (2020). Freezing of gait in Parkinson's disease: pathophysiology, risk factors and treatments. Transl. Neurodegener. 9:12. doi: 10.1186/s40035-020-00191-5
Goldberg, A., Chavis, M., Watkins, J., and Wilson, T. (2012). The five-times-sit-to-stand test: validity, reliability and detectable change in older females. Aging Clin. Exp. Res. 24, 339–344. doi: 10.1007/BF03325265
Gomez-Esteban, J. C., Zarranz, J. J., Lezcano, E., Tijero, B., Luna, A., Velasco, F., et al. (2007). Influence of motor symptoms upon the quality of life of patients with Parkinson's disease. Eur. Neurol. 57, 161–165. doi: 10.1159/000098468
Hart, A., Cordova-Rivera, L., Barker, F., Sayer, A. A., Granic, A., and Yarnall, A. J. (2023). The prevalence of sarcopenia in Parkinson's disease and related disorders-a systematic review. Neurol. Sci. 44, 4205–4217. doi: 10.1007/s10072-023-07007-0
Hasan, S., Kandasamy, G., Alyahya, D., Alonazi, A., Jamal, A., Unnikrishnan, R., et al. (2021). Effect of resisted Sprint and plyometric training on lower limb functional performance in collegiate male football players: a randomised control trial. Int. J. Environ. Res. Public Health 18:6702. doi: 10.3390/ijerph18136702
Jenkinson, C., Fitzpatrick, R., Peto, V., Greenhall, R., and Hyman, N. (1997). The Parkinson's disease questionnaire (PDQ-39): development and validation of a Parkinson's disease summary index score. Age Ageing 26, 353–357. doi: 10.1093/ageing/26.5.353
Kluger, B. M., Brown, R. P., Aerts, S., and Schenkman, M. (2014). Determinants of objectively measured physical functional performance in early to mid-stage Parkinson disease. PM R 6, 992–998. doi: 10.1016/j.pmrj.2014.05.013
Kurihara, K., Nakagawa, R., Ishido, M., Yoshinaga, Y., Watanabe, J., Hayashi, Y., et al. (2020). Impact of motor and nonmotor symptoms in Parkinson disease for the quality of life: the Japanese quality-of-life survey of Parkinson disease (JAQPAD) study. J. Neurol. Sci. 419:117172. doi: 10.1016/j.jns.2020.117172
Li, R., Zhang, Y., Jiang, Y., Wang, M., Ang, W. H. D., and Lau, Y. (2021). Rehabilitation training based on virtual reality for patients with Parkinson's disease in improving balance, quality of life, activities of daily living, and depressive symptoms: a systematic review and meta-regression analysis. Clin. Rehabil. 35, 1089–1102. doi: 10.1177/0269215521995179
Martinez-Martin, P., Rodriguez-Blazquez, C., Mario, A., Arakaki, T., Arillo, V. C., Chana, P., et al. (2015). Parkinson's disease severity levels and MDS-unified Parkinson's disease rating scale. Parkinsonism Relat. Disord. 21, 50–54. doi: 10.1016/j.parkreldis.2014.10.026
Mehdizadeh, M., Lajevardi, L., Habibi, S. A. H., Arab Baniasad, M., Baghoori, D., Daneshjoo, F., et al. (2016). The association between fear of falling and quality of life for balance impairments based on hip and ankle strategies in the drug on-and off-phase of patients with idiopathic Parkinson' disease. Med. J. Islam Repub. Iran 30:453
Nakano, T., Kajiyama, Y., Revankar, G. S., Hashimoto, R., Watanabe, Y., Kishima, H., et al. (2021). Neural networks associated with quality of life in patients with Parkinson's disease. Parkinsonism Relat. Disord. 89, 6–12. doi: 10.1016/j.parkreldis.2021.06.007
Nightingale, C. J., Mitchell, S. N., and Butterfield, S. A. (2019). Validation of the timed up and go test for assessing balance variables in adults aged 65 and older. J. Aging Phys. Act. 27, 230–233. doi: 10.1123/japa.2018-0049
Nocera, J. R., Stegemoller, E. L., Malaty, I. A., Okun, M. S., Marsiske, M., and Hass, C. J. (2013). National Parkinson Foundation quality improvement initiative I. Using the timed up & go test in a clinical setting to predict falling in Parkinson's disease. Arch. Phys. Med. Rehabil. 94, 1300–1305. doi: 10.1016/j.apmr.2013.02.020
Qi, S., Yin, P., Wang, L., Qu, M., Kan, G. L., Zhang, H., et al. (2021). Prevalence of Parkinson's disease: a community-based study in China. Mov. Disord. 36, 2940–2944. doi: 10.1002/mds.28762
Renee, S., Elisabeth, P., Niruthikha, M., Allyson, F., and Louise, A. (2021). People with mild PD have impaired force production in all lower limb muscle groups: a cross-sectional study. Physiother. Res. Int. 26:e1897. doi: 10.1002/pri.1897
San Martín Valenzuela, C., Moscardó, L. D., López-Pascual, J., Serra-Añó, P., and Tomás, J. M. (2020). Effects of dual-task group training on gait, cognitive executive function, and quality of life in people with Parkinson disease: results of randomized controlled DUALGAIT trial. Arch. Phys. Med. Rehabil. 101, 1849–56.e1. doi: 10.1016/j.apmr.2020.07.008
Scalzo, P. L., Flores, C. R., Marques, J. R., Robini, S. C., and Teixeira, A. L. (2012). Impact of changes in balance and walking capacity on the quality of life in patients with Parkinson's disease. Arq. Neuropsiquiatr. 70, 119–124. doi: 10.1590/S0004-282X2012000200009
Skinner, J. W., Christou, E. A., and Hass, C. J. (2019). Lower extremity muscle strength and force variability in persons with Parkinson disease. J. Neurol. Phys. Ther. 43, 56–62. doi: 10.1097/NPT.0000000000000244
Smith, K. M., and Caplan, D. N. (2018). Communication impairment in Parkinson's disease: impact of motor and cognitive symptoms on speech and language. Brain Lang. 185, 38–46. doi: 10.1016/j.bandl.2018.08.002
Sveinbjornsdottir, S. (2016). The clinical symptoms of Parkinson's disease. J. Neurochem. 139, 318–324. doi: 10.1111/jnc.13691
Szefler-Derela, J., Arkuszewski, M., Knapik, A., Wasiuk-Zowada, D., Gorzkowska, A., and Krzystanek, E. (2020). Effectiveness of 6-week Nordic walking training on functional performance, gait quality, and quality of life in Parkinson's disease. Medicina (Kaunas) 56:356. doi: 10.3390/medicina56070356
Thanvi, B., and Treadwell, S. D. (2010). Freezing of gait in older people: associated conditions, clinical aspects, assessment and treatment. Postgrad. Med. J. 86, 472–477. doi: 10.1136/pgmj.2009.090456
Ueno, T., Kon, T., Haga, R., Nishijima, H., Arai, A., and Tomiyama, M. (2020). Assessing the relationship between non-motor symptoms and health-related quality of life in Parkinson's disease: a retrospective observational cohort study. Neurol. Sci. 41, 2867–2873. doi: 10.1007/s10072-020-04406-5
Yokote, A., Hayashi, Y., Yanamoto, S., Fujioka, S., Higa, K., and Tsuboi, Y. (2022). Leg muscle strength correlates with gait performance in advanced Parkinson disease. Intern. Med. 61, 633–638. doi: 10.2169/internalmedicine.7646-21
Yoon, J. E., Kim, J. S., Jang, W., Park, J., Oh, E., Youn, J., et al. (2017). Gender differences of nonmotor symptoms affecting quality of life in Parkinson disease. Neurodegener Dis 17, 276–280. doi: 10.1159/000479111
Zhang, J. L., and Chan, P. (2012). Reliability and validity of PDQ-39: a quality-of-life measure for patients with PD in China. Qual. Life Res. 21, 1217–1221. doi: 10.1007/s11136-011-0026-1
Keywords: Parkinson’s disease, motor function, health-related quality of life, balance, gait
Citation: Ge Y, Zhao W, Zhang L, Zhao X, Shu X, Li J and Liu Y (2024) Correlation between motor function and health-related quality of life in early to mid-stage patients with Parkinson disease: a cross-sectional observational study. Front. Aging Neurosci. 16:1399285. doi: 10.3389/fnagi.2024.1399285
Edited by:
Adérito Ricardo Duarte Seixas, Escola Superior de Saúde Fernando Pessoa, PortugalReviewed by:
José Alexandre Bachur, University of Franca, BrazilCopyright © 2024 Ge, Zhao, Zhang, Zhao, Shu, Li and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ying Liu, cHVtY2g5ODg3QDE2My5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.