
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Aging Neurosci. , 20 July 2023
Sec. Neurocognitive Aging and Behavior
Volume 15 - 2023 | https://doi.org/10.3389/fnagi.2023.1217080
 Edoardo Nicolò Aiello1
Edoardo Nicolò Aiello1 Federica Solca1
Federica Solca1 Silvia Torre1Valerio Patisso2Alberto De Lorenzo2Mauro Treddenti2
Silvia Torre1Valerio Patisso2Alberto De Lorenzo2Mauro Treddenti2 Eleonora Colombo1Alessio Maranzano1
Eleonora Colombo1Alessio Maranzano1 Claudia Morelli1Alberto Doretti1
Claudia Morelli1Alberto Doretti1 Federico Verde1,3
Federico Verde1,3 Vincenzo Silani1,3
Vincenzo Silani1,3 Nicola Ticozzi1,3
Nicola Ticozzi1,3 Barbara Poletti1,4*
Barbara Poletti1,4*Background: This study aimed at clarifying the role of bulbar involvement (BI) as a risk factor for cognitive impairment (CI) in non-demented amyotrophic lateral sclerosis (ALS) patients.
Methods: Data on N = 347 patients were retrospectively collected. Cognition was assessed via the Edinburgh Cognitive and Behavioral ALS Screen (ECAS). On the basis of clinical records and ALS Functional Rating Scale-Revised (ALSFRS-R) scores, BI was characterized as follows: (1) BI at onset—from medical history; (2) BI at testing (an ALSFRS-R-Bulbar score ≤11); (3) dysarthria (a score ≤3 on item 1 of the ALSFRS-R); (4) severity of BI (the total score on the ALSFRS-R-Bulbar); and (5) progression rate of BI (computed as 12-ALSFRS-R-Bulbar/disease duration in months). Logistic regressions were run to predict a below- vs. above-cutoff performance on each ECAS measure based on BI-related features while accounting for sex, disease duration, severity and progression rate of respiratory and spinal involvement and ECAS response modality.
Results: No predictors yielded significance either on the ECAS-Total and -ALS-non-specific or on ECAS-Language/-Fluency or -Visuospatial subscales. BI at testing predicted a higher probability of an abnormal performance on the ECAS-ALS-specific (p = 0.035) and ECAS-Executive Functioning (p = 0.018). Lower ALSFRS-R-Bulbar scores were associated with a defective performance on the ECAS-Memory (p = 0.025). No other BI-related features affected other ECAS performances.
Discussion: In ALS, the occurrence of BI itself, while neither its specific features nor its presence at onset, might selectively represent a risk factor for executive impairment, whilst its severity might be associated with memory deficits.
Bulbar involvement (BI) has been historically linked to cognitive impairment (CI) in amyotrophic lateral sclerosis (ALS) (Zago et al., 2022). However, bulbar onset and dysarthria have been only recently acknowledged, at a meta-analytic level, as actual risk factors for frontotemporal-spectrum disorders in this population (Yang et al., 2021). Relatedly, recent neuropathological evidence has supported such a phenotypic association within a network-based framework, according to which medullary pathology would readily spread to bulbar sensory-motor cortices and, in turn, to the frontal and temporal areas connected to them (Shellikeri et al., 2020).
However, among the studies included in the abovementioned meta-analysis by Yang et al. (2021) for the specific aim of testing whether bulbar onset and dysarthria could represent risk factors for CI in ALS, only a minority (i.e., 3 out of 14) performed some sort of adjustment for bulbar confounders during task execution (Kasper et al., 2016; Trojsi et al., 2017; Watanabe et al., 2020). Moreover, none of these reports employed an ALS-specific measure that could control for BI as much as possible—such as the Edinburgh Cognitive and Behavioral ALS Screen (ECAS) (Abrahams et al., 2014). At most, among such studies (Yang et al., 2021), the confounding effect of BI was accounted for via mere attempts, performed either a priori—e.g., by selecting untimed cognitive tests that minimally relied on verbal responses (Massman et al., 1996) or by excluding patients unable to execute a minimum number of cognitive tests (Oh et al., 2014)—or a posteriori—e.g., by analytically comparing the rates of CI between dysarthric and non-dysarthric patients (Massman et al., 1996; Rippon et al., 2006). Hence, given that accommodating for BI when assessing cognition in ALS patients is essential (Woolley and Rush, 2017), the conclusions drawn by Yang et al. (2021) appear to be based, to a non-negligible extent, on biased studies.
Unfortunately, the same methodological issues also affect other relevant reports on the topic that were not included in Yang et al. (2021) meta-analysis (Portet et al., 2001; Schreiber et al., 2005; Röttig et al., 2006; Sterling et al., 2010; Morimoto et al., 2012; Zalonis et al., 2012; Mannarelli et al., 2014; Burke et al., 2016). Therein, the attempts to control for the confounding effect of BI on cognition in ALS, which were mostly performed a posteriori, led to indeterminate conclusions (Portet et al., 2001; Schreiber et al., 2005; Röttig et al., 2006; Sterling et al., 2010; Morimoto et al., 2012; Zalonis et al., 2012; Mannarelli et al., 2014; Burke et al., 2016). Most importantly, the vast majority of these works (Massman et al., 1996; Portet et al., 2001; Schreiber et al., 2005; Rippon et al., 2006; Röttig et al., 2006; Sterling et al., 2010; Morimoto et al., 2012; Zalonis et al., 2012; Mannarelli et al., 2014; Oh et al., 2014; Burke et al., 2016; Woolley and Rush, 2017; Yang et al., 2021) approached the association between BI and CI in ALS via simple correlational/predictive statistics. Indeed, most of these studies (1) did not disentangle the contribution of BI at onset from that at the time of cognitive testing, (2) did not focus on the severity and progression rate of BI itself, and (3) did not covary for other motor-functional features that possibly increase the risk of CI this population—i.e., respiratory dysfunctions (Huynh et al., 2020b; Shah et al., 2021) and an advanced disease (Crockford et al., 2018; Chiò et al., 2019).
Hence, by addressing a large cohort of non-demented ALS patients, the present study aimed at assessing, via multiple regression models, the association between a comprehensive set of BI-related features and a disease-specific cognitive measure (i.e., the ECAS) net of other motor-functional variables.
The current retrospective cohort included N = 347 ALS patients (Brooks et al., 2000) consecutively referred to IRCCS Istituto Auxologico Italiano, Milano, Italy between 2016 and 2023 who were administered the ECAS (Poletti et al., 2016) and for whom onset data and ALS Functional Rating Scale-Revised (ALSFRS-R) (Cedarbaum et al., 1999) scores were available. Patients did not present with (1) a co-morbid diagnosis of frontotemporal dementia (FTD) (Gorno-Tempini et al., 2011; Rascovsky et al., 2011), (2) ALS-unrelated neurological/psychiatric disorders, (3) severe/unstable general-medical conditions, and (4) uncorrected sensory deficits.
The cognitive section of the Italian ECAS (Poletti et al., 2016) (range = 0–136) includes 5 subscales assessing Language (ECAS-L; range = 0–28), Fluency (ECAS-F; range = 0–24), Executive Functioning (ECAS-EF; range = 0–48), Memory (ECAS-M; range = 0–24), and Visuospatial abilities (ECAS-VS; range = 0–12). ECAS-ALS-specific (i.e., ECAS-L + ECAS-F + ECAS-EF; range = 0–100) and -non-specific subscores (i.e., ECAS-M + ECAS-VS; range = 0–36) were also computed. ALSFRS-R items (Cedarbaum et al., 1999) were grouped as follows: (1) ALSFRS-R-Bulbar (items 1–3; range = 0–12); (2) ALSFRS-R-Spinal (items 4–9; range = 0–24); and (3) ALSFRS-R-Respiratory (items 10–12; range = 0–12). Progression rate (ΔFS) was computed according to Kimura et al. (2006) formula for each ALSFRS-R subscale—i.e., by weighting on disease duration (in months) the difference between the maximum and the actual ALSFRS-R subscore. Disease staging was retrieved according to both King’s college (Roche et al., 2012) and Milano-Torino (MiToS) (Chiò et al., 2015) systems.
Logistic regressions were run separately for each ECAS measure by addressing, as the outcome, a below- vs. above-cutoff performance [based on age- and education-stratified Italian normality thresholds (Poletti et al., 2016)], and, as predictors, (1) bulbar onset—retrieved from patients’ medical history—(2) presence of BI at testing—defined as an ALSFRS-R-Bulbar score ≤11—(3) presence of dysarthria—defined as a score ≤3 on item 1 of the ALSFRS-R—(4) severity of BI—i.e., the total score on the ALSFRS-R-Bulbar—and (5) progression rate of BI—i.e., ΔFS-Bulbar scores. Within these models, sex, disease duration (in months), severity and progression rate of respiratory and spinal involvement (i.e., ALSFRS-R-Spinal, ALSFRS-R-Respiratory, ΔFS-Spinal and ΔFS-Respiratory scores) and ECAS response modality (i.e., oral vs. written) were covaried. Collinearity was diagnosed in the presence of a Variance Inflation Factor (VIF) >10 and of a Tolerance Index (TI) < 0.1.
Analyses were run via IBM® SPSS® Statistic (IBM Corp., 2021) and jamovi 2.3 (the jamovi project, 2022).
Table 1 summarizes patients’ background and clinical features, and Table 2 reports the complete results of the logistic regression models.
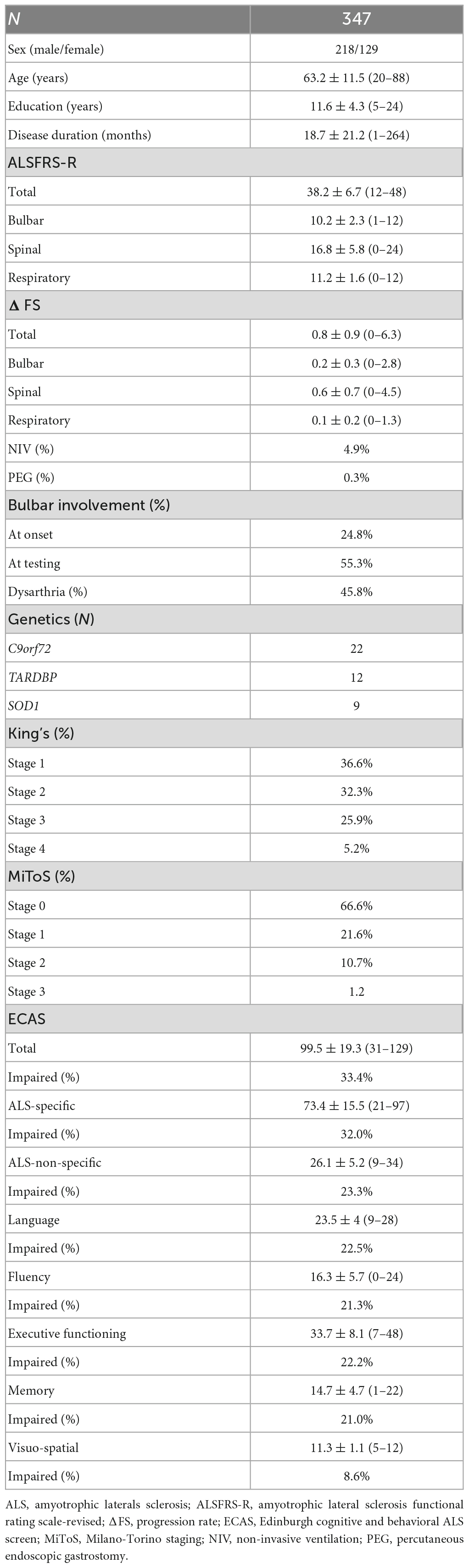
Table 1. Patients’ demographic, clinical, and cognitive measures.
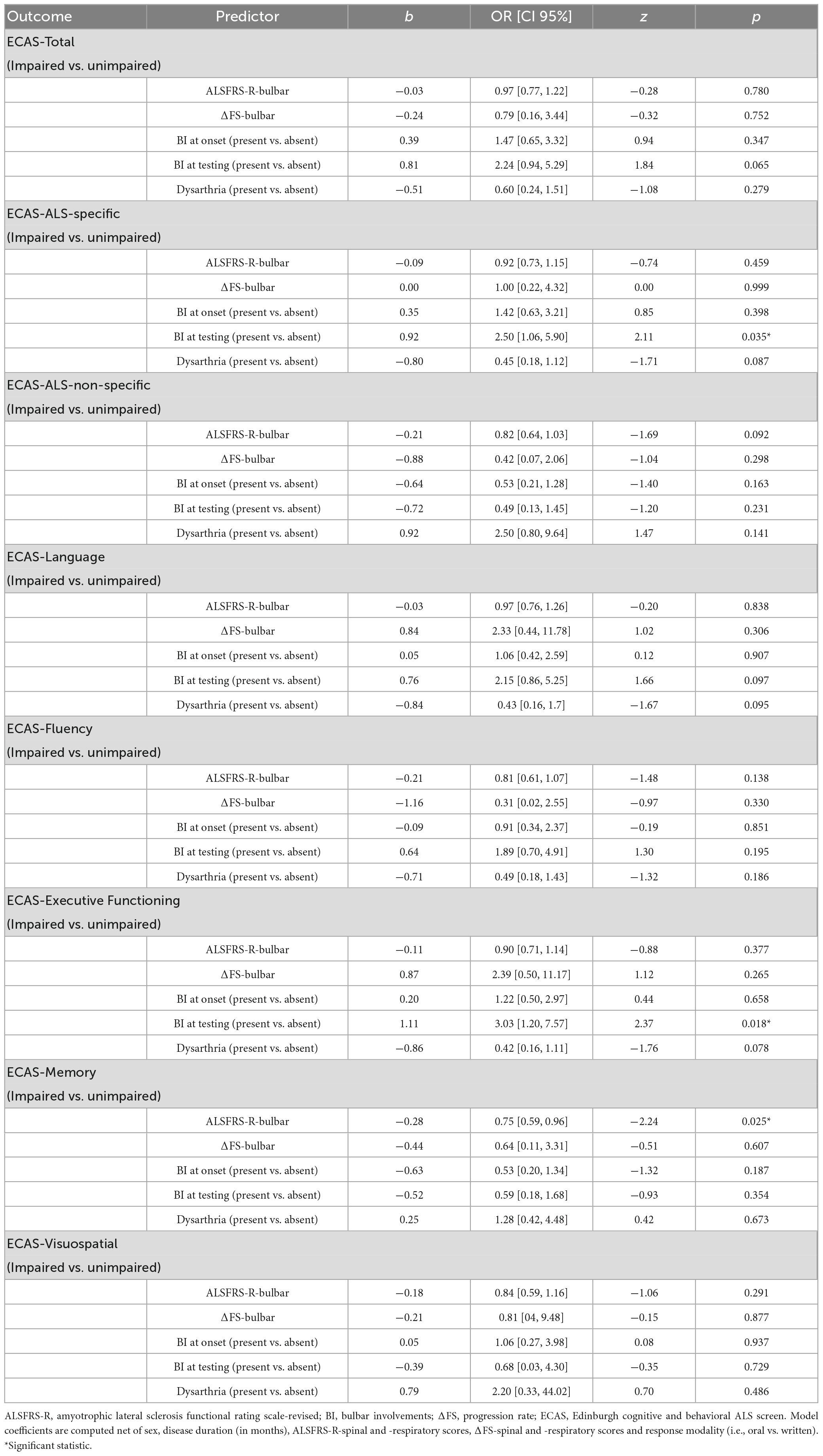
Table 2. Effects of bulbar features on ECAS performances as yielded by the logistic regression models.
No collinearity was detected among predictors (VIF ≤5.41; TI ≥ 0.19). No target predictors yielded significance on the ECAS-Total (ps ≥ 0.065), ECAS-ALS-non-specific (ps ≥ 0.092), ECAS-L (ps ≥ 0.095), ECAS-F (ps ≥ 0.138), and ECAS-VS (ps ≥ 0.291). At variance, BI at testing was associated with a higher probability of an impaired performance on the ECAS-ALS-Specific (b = 0.92; z = 2.11; OR = 2.5, CI 95% [1.06, 5.9]). Indeed, patients with BI at testing were more likely to perform defectively on this subscale (M = 0.39; SE = 0.08) when compared to those without (M = 0.20; SE = 0.06). Such a finding happened to be carried by the ECAS-EF: indeed, the probability of an abnormal performance on the ECAS-EF was found to be significantly higher in patients with BI (M = 0.26; SE = 0.07) when compared to those without BI (M = 0.10; SE = 0.04) at testing (b = 1.11; z = 2.37; OR = 3.03, CI 95% [1.2, 7.57]). Finally, patients with lower ALSFRS-R-Bulbar scores were found to be more likely to perform defectively on the ECAS-M (b = −0.28; z = −2.24; OR = 0.75, CI 95% [0.59, 0.96]). Indeed, the probability of an abnormal performance on the ECAS-M was lower (M = 0.08; SE = 0.04) in patients with higher (M + 1*SD) ALSFRS-R-Bulbar scores, and higher (M = 0.24; SE = 0.06) in patients with lower (M-1*SD) scores on this measure. No other BI-related variables yielded significance (ps > 0.05).
The present report clarifies the role of BI as a risk factor for CI in ALS by simultaneously encompassing, within a large patient cohort, an extensive range of both BI-related predictors and other motor-functional covariates, as well as by addressing a disease-specific measures of cognition that compensates for motor disabilities (i.e., the ECAS).
This study suggests that, net of overall motor-functional status, BI itself, and neither its presence at onset, severity, progression rate or phenotype (i.e., the occurrence of dysarthria), increases the probability of executive deficits non-demented ALS patients. Indeed, ALS patients with BI at testing were more likely to perform defectively on the ECAS-EF than those without BI at testing. Additionally, the current investigation suggests that patients with a more severe BI (i.e., lower ALSFRS-R-Bulbar scores) are more likely to present with memory deficits (i.e., an impaired performance on the ECAS-M).
The fact that neither BI at onset nor dysarthria herewith represented risk factors for CI in this ALS cohort is in contrast with Yang et al. (2021) meta-analysis: however the statistical approach chosen for this study, as well as the extensive range of BI-related features and motor-functional confounders taken into account, grant a larger extent of generalizability to the present results. At the same time, in respect to BI at onset, this report aligns with two previous meta-analyses on the cognitive phenotype of ALS (Raaphorst et al., 2010; Beeldman et al., 2016)—wherein no association was detected between BI at onset and an increased risk for CI. Relatedly, a report by Zalonis et al. (2012), which selectively aimed to test whether executive measures could discriminate bulbar- from spinal-onset ALS patients, failed to corroborate this hypothesis. As to the present lack of association between dysarthria and an increased risk for CI, such a finding is likely due to the fact that the cognitive measure herewith employed—i.e., the ECAS—aprioristically accommodates for this motor confounder.
Overall, the present report supports the view that, from a network-based perspective (Shellikeri et al., 2017, 2020), ALS patients with BI may present with a greater involvement of extra-motor cortices when compared to those without BI (Steinbach et al., 2021). This stance is also supported by the neuroradiological report by Cistaro et al. (2012), who showed that, when compared to patients without BI, bulbar ALS patients show distinct functional brain features that correlate with the degree of CI.
Remarkably, BI at testing herewith represented a risk factor only for executive dysfunction, as it did not affect either overall cognitive efficiency or other cognitive domains/functions. While this finding is consistent with previous reports on the topic, which commonly link BI to executive deficits in ALS (Schreiber et al., 2005; Sterling et al., 2010; Morimoto et al., 2012; Mannarelli et al., 2014; Burke et al., 2016), it does not align with the literature concerning the association between BI and language impairment in this population (Pinto-Grau et al., 2018; Aiello et al., 2022a,b; Sbrollini et al., 2022). This inconsistency might be due to a measure-related issue—since, as previously suggested (Aiello et al., 2022c; McMillan et al., 2022; Solca et al., 2023), the ECAS-L does not represent a comprehensive language measure in ALS. Thus, it is advised that future studies address the link between BI and language impairment in this population by employing an extensive set of language tests. Similarly, no bulbar feature was herewith found to be associated with verbal fluency deficits, despite this link being frequently reported in previous investigations (Kew et al., 1993; Abrahams et al., 1996, 1997, 2000, 2005). This result is surprising—given that phonemic fluency tasks included within the ECAS-F have systemically proven sensitive to executive dysfunctions in this population (Kew et al., 1993; Abrahams et al., 1996, 1997, 2000, 2005). At the same time, it might be hypothesized that, since these tasks aprioristically accommodate for bulbar confounders (Abrahams et al., 2014; Canu et al., 2023), the further, a posteriori analytical expedient aimed at controlling for other BI-related features might have resulted in the lack of detection of the abovementioned association. However, an association between the severity of BI and memory deficits has herewith yielded. Such a finding—which is consistent with previous reports (Schreiber et al., 2005)—might be linked to the one regarding the ECAS-EF, and thus accounted for by the fact that memory deficits in this population are, at least to an extent, secondary to executive dysfunctions (Consonni et al., 2017; Barulli et al., 2019).
This study have several limitations. First, the evaluation of bulbar features herewith relied either on patients’ medical history or on the dedicated ALSFRS-R subscale. Hence, future studies are necessary that employ specific clinical scales aimed at assessing BI in ALS (Yunusova et al., 2019)—e.g., the Center for Neurologic Study Bulbar Function Scale (CNS-BFS) (Smith et al., 2018). Relatedly, the present study relied solely on clinical measures, but not on instrumental examinations, which would have better characterized the nature and extent of BI of the present cohort (Yunusova et al., 2019). Third, it must be borne in mind that the ECAS subscale yields a first-level measure of cognition within each target domain or function. Hence, further investigations that embrace the present experimental design by addressing a battery of second-level, domain-/function-specific cognitive tests are needed. Fourth, this report solely addressed patients without a co-morbid diagnosis of FTD, thus not being informative of the role of BI as a risk factor for full-blown dementing states in this population. However, in this respect, it is worth noting that a recent report by the present research group (Colombo et al., 2023) suggested that BI, along with genetic risk factors (i.e., C9orf72 hexanucleotide repeat expansion), are associated with concurrent behavioral variant-FTD. Finally, the retrospective nature of the current study does not allow to draw inferences on how the association between BI and CI in this population might change over time. Future studies that delve into such matter should be undertaken that involve a longitudinal design (Colombo et al., 2023) addressing technology-aided cognitive assessment procedures fully overcoming patients’ motor disabilities across all disease stages (Cipresso et al., 2011; Poletti et al., 2017a,b, 2018a,b).
In conclusions, this study suggests that the occurrence of BI itself, whilst neither its specific clinical characteristics nor its presence at disease onset, selectively represents a risk factor for executive impairment in non-demented ALS patients, as well as that the severity of BI might be associated with memory deficits in this population. Overall, the present findings suggest that non-demented ALS patients presenting with BI should be carefully assessed for their executive—and possibly mnestic—status, given that deficits within such a set of cognitive functions are known to detrimentally impact on patients’ prognosis (Poletti et al., 2018a; Huynh et al., 2020a).
This set of raw data is accessible under request because it includes sensitive information. Raw data have been stored at the following link: https://doi.org/10.5281/zenodo.8103679.
The studies involving human participants were reviewed and approved by the Ethics Committees of IRCCS Istituto Auxologico Italiano (I.D.: 2013_06_25). The patients/participants provided their written informed consent to participate in this study.
EA: conceptualization, analyses, drafting, and revision. FS, ST, VP, ADL, MT, EC, and AM: data collection and revision. CM, AD, FV, and VS: resources and revision. BP and NT: resources, drafting, and revision. All authors contributed to the article and approved the submitted version.
This work was supported by the Italian Ministry of Health - Ricerca Corrente.
We thankful to patients and their caregivers. We acknowledge the ERN Euro-NMD for support.
VS received compensation for consulting services and/or speaking activities from AveXis, Cytokinetics, Italfarmaco, Liquidweb S.r.l., Novartis Pharma AG, and Zambon, receives or has received research supports from the Italian Ministry of Health, AriSLA, and E-Rare Joint Transnational Call. He is in the Editorial Board of Amyotrophic Lateral Sclerosis and Frontotemporal Degeneration, European Neurology, American Journal of Neurodegenerative Diseases, Frontiers in Neurology and Exploration of Neuroprotective Therapy. BP received compensation for consulting services and/or speaking activities from Liquidweb S.r.l. She is Associate Editor for Frontiers in Neuroscience. NT received compensation for consulting services from Amylyx Pharmaceuticals and Zambon Biotech SA. He is Associate Editor for Frontiers in Aging Neuroscience.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abrahams, S., Goldstein, L., Al-Chalabi, A., Pickering, A., Morris, R., Passingham, R., et al. (1997). Relation between cognitive dysfunction and pseudobulbar palsy in amyotrophic lateral sclerosis. J. Neurol. Neurosurg. Psychiatry. 62, 464–472. doi: 10.1136/jnnp.62.5.464
Abrahams, S., Goldstein, L., Suckling, J., Ng, V., Simmons, A., Chitnis, X., et al. (2005). Frontotemporal white matter changes in amyotrophic lateral sclerosis. J. Neurol. 252, 321–331. doi: 10.1007/s00415-005-0646-x
Abrahams, S., Goldstein, L. H., Kew, J. J., Brooks, D. J., Lloyd, C. M., Frith, C. D., et al. (1996). Frontal lobe dysfunction in amyotrophic lateral sclerosis: a PET study. Brain 119, 2105–2120. doi: 10.1093/brain/119.6.2105
Abrahams, S., Leigh, P., Harvey, A., Vythelingum, G., Grise, D., and Goldstein, L. (2000). Verbal fluency and executive dysfunction in amyotrophic lateral sclerosis (ALS). Neuropsychologia 38, 734–747. doi: 10.1016/S0028-3932(99)00146-3
Abrahams, S., Newton, J., Niven, E., Foley, J., and Bak, T. (2014). Screening for cognition and behaviour changes in ALS. Amyotrop.h Lateral Scler Frontotemporal. Degener. 15, 9–14. doi: 10.3109/21678421.2013.805784
Aiello, E., Feroldi, S., De Luca, G., Guidotti, L., Arrigoni, E., Appollonio, I., et al. (2022a). Primary progressive aphasia and motor neuron disease: a review. Front. Aging Neurosci. 14:1003792. doi: 10.3389/fnagi.2022.1003792
Aiello, E., Feroldi, S., Preti, A., Zago, S., and Appollonio, I. (2022b). Dysgraphic features in motor neuron disease: a review. Aphasiology 36, 1249–1274. doi: 10.1080/02687038.2021.1942774
Aiello, E., Iazzolino, B., Pain, D., Peotta, L., Palumbo, F., Radici, A., et al. (2022c). The diagnostic value of the Italian version of the edinburgh cognitive and behavioral ALS screen (ECAS). Amyotroph. Lateral. Scler Frontotemporal. Degener. 23, 527–531.
Barulli, M., Piccininni, M., Di Dio, C., Musaro, C., Grasso, A., Tursi, M., et al. (2019). Episodic memory and learning rates in amyotrophic lateral sclerosis without dementia. Cortex 117, 257–265. doi: 10.1016/j.cortex.2019.03.003
Beeldman, E., Raaphorst, J., Twennaar, M., de Visser, M., Schmand, B., and de Haan, R. (2016). The cognitive profile of ALS: a systematic review and meta-analysis update. J. Neurol. Neurosurg. Psychiatry. 87, 611–619. doi: 10.1136/jnnp-2015-310734
Brooks, B., Miller, R., Swash, M., and Munsat, T. (2000). El Escorial revisited: revised criteria for the diagnosis of amyotrophic lateral sclerosis. Amyotroph. Lateral Scler. Other Motor Neuron Disord. 1, 293–299. doi: 10.1080/146608200300079536
Burke, T., Elamin, M., Bede, P., Pinto-Grau, M., Lonergan, K., Hardiman, O., et al. (2016). Discordant performance on the ‘Reading the Mind in the Eyes’ test, based on disease onset in amyotrophic lateral sclerosis. Amyotroph. Lateral. Scler. Frontotemporal. Degener. 17, 467–472. doi: 10.1080/21678421.2016.1177088
Canu, E., Castelnovo, V., Rancoita, P., Leocadi, M., Lamanuzzi, A., Spinelli, E., et al. (2023). Italian reference values and brain correlates of verbal fluency index–vs standard verbal fluency test–to assess executive dysfunction in ALS. Amyotroph. Lateral. Scler. Frontotemporal. Degener.* 1–9. doi: 10.1080/21678421.2023.2167606
Cedarbaum, J., Stambler, N., Malta, E., Fuller, C., Hilt, D., Thurmond, B., et al. (1999). The ALSFRS-R: a revised ALS functional rating scale that incorporates assessments of respiratory function. J. Neurol. Sci. 169, 13–21. doi: 10.1016/S0022-510X(99)00210-5
Chiò, A., Hammond, E., Mora, G., Bonito, V., and Filippini, G. (2015). Development and evaluation of a clinical staging system for amyotrophic lateral sclerosis. J. Neurol. Neurosurg. Psychiatry 86, 38–44. doi: 10.1136/jnnp-2013-306589
Chiò, A., Moglia, C., Canosa, A., Manera, U., Vasta, R., Brunetti, M., et al. (2019). Cognitive impairment across ALS clinical stages in a population-based cohort. Neurology 93, e984–e994. doi: 10.1212/WNL.0000000000008063
Cipresso, P., Meriggi, P., Carelli, L., Solca, F., Meazzi, D., Poletti, B., et al. (2011). “The combined use of brain computer interface and eye-tracking technology for cognitive assessment in amyotrophic lateral sclerosis,” in 2011 5th International conference on pervasive computing technologies for healthcare (PervasiveHealth) and workshops, (Dublin: IEEE), 320–324. doi: 10.4108/icst.pervasivehealth.2011.246018
Cistaro, A., Valentini, M., Chiò, A., Nobili, F., Calvo, A., Moglia, C., et al. (2012). Brain hypermetabolism in amyotrophic lateral sclerosis: a FDG PET study in ALS of spinal and bulbar onset. Eur. J. Nucl. Med. Mol. Imaging 39, 251–259. doi: 10.1007/s00259-011-1979-6
Colombo, E., Poletti, B., Maranzano, A., Peverelli, S., Solca, F., Colombrita, C., et al. (2023). Motor, cognitive and behavioural profiles of C9orf72 expansion-related amyotrophic lateral sclerosis. J. Neurol. 270, 898–908. doi: 10.1007/s00415-022-11433-z
Consonni, M., Rossi, S., Cerami, C., Marcone, A., Iannaccone, S., Francesco Cappa, S., et al. (2017). Executive dysfunction affects word list recall performance: evidence from amyotrophic lateral sclerosis and other neurodegenerative diseases. J. Neuropsychol. 11, 74–90. doi: 10.1111/jnp.12072
Crockford, C., Newton, J., Lonergan, K., Chiwera, T., Booth, T., Chandran, S., et al. (2018). ALS-specific cognitive and behavior changes associated with advancing disease stage in ALS. Neurology 91, e1370–e1380. doi: 10.1212/WNL.0000000000006317
Gorno-Tempini, M., Hillis, A., Weintraub, S., Kertesz, A., Mendez, M., Cappa, S., et al. (2011). Classification of primary progressive aphasia and its variants. Neurology 76, 1006–1014. doi: 10.1212/WNL.0b013e31821103e6
Huynh, W., Sharplin, L., Caga, J., Highton-Williamson, E., and Kiernan, M. (2020b). Respiratory function and cognitive profile in amyotrophic lateral sclerosis. Eur. J. Neurol. 27, 685–691. doi: 10.1111/ene.14130
Huynh, W., Ahmed, R., Mahoney, C., Nguyen, C., Tu, S., Caga, J., et al. (2020a). The impact of cognitive and behavioral impairment in amyotrophic lateral sclerosis. Expert Rev. Neurother. 20, 281–293. doi: 10.1080/14737175.2020.1727740
Kasper, E., Zydatiss, K., Schuster, C., Machts, J., Bittner, D., Kaufmann, J., et al. (2016). No change in executive performance in ALS patients: a longitudinal neuropsychological study. Neurodegener. Dis. 16, 184–191. doi: 10.1159/000440957
Kew, J., Goldstein, L., Leigh, P., Abrahams, S., Cosgrave, N., Passingham, R., et al. (1993). The relationship between abnormalities of cognitive function and cerebral activation in amyotrophic lateral sclerosis: a neuropsychological and positron emission tomography study. Brain 116, 1399–1423. doi: 10.1093/brain/116.6.1399
Kimura, F., Fujimura, C., Ishida, S., Nakajima, H., Furutama, D., Uehara, H., et al. (2006). Progression rate of ALSFRS-R at time of diagnosis predicts survival time in ALS. Neurology 66, 265–267. doi: 10.1212/01.wnl.0000194316.91908.8a
Mannarelli, D., Pauletti, C., Locuratolo, N., Vanacore, N., Frasca, V., Trebbastoni, A., et al. (2014). Attentional processing in bulbar-and spinal-onset amyotrophic lateral sclerosis: insights from event-related potentials. Amyotroph. Lateral Scler. Frontotemporal. Degener. 15, 30–38. doi: 10.3109/21678421.2013.787628
Massman, P., Sims, J., Cooke, N., Haverkamp, L., Appel, V., and Appel, S. (1996). Prevalence and correlates of neuropsychological deficits in amyotrophic lateral sclerosis. J. Neurol. Neurosurg. Psychiatry 61, 450–455. doi: 10.1136/jnnp.61.5.450
McMillan, C., Wuu, J., Rascovsky, K., Cosentino, S., Grossman, M., Elman, L., et al. (2022). Defining cognitive impairment in amyotrophic lateral sclerosis: an evaluation of empirical approaches. Amyotroph. Lateral. Scler. Frontotemporal. Degener. 23, 517–526. doi: 10.1080/21678421.2022.2039713
Morimoto, N., Kurata, T., Sato, K., Ikeda, Y., Sato, S., and Abe, K. (2012). Frontal dysfunctions of ALS-PBP patients in relation to their bulbar symptoms and rCBF decline. J. Neurol. Sci. 319, 96–101. doi: 10.1016/j.jns.2012.04.020
Oh, S., Park, A., Kim, H., Oh, K., Choi, H., Kwon, M., et al. (2014). Spectrum of cognitive impairment in Korean ALS patients without known genetic mutations. PLoS One 9:e87163. doi: 10.1371/journal.pone.0087163
Pinto-Grau, M., Hardiman, O., and Pender, N. (2018). The study of language in the amyotrophic lateral sclerosis-frontotemporal spectrum disorder: a systematic review of findings and new perspectives. Neuropsychol. Rev. 28, 251–268. doi: 10.1007/s11065-018-9375-7
Poletti, B., Carelli, L., Faini, A., Solca, F., Meriggi, P., Lafronza, A., et al. (2018a). The arrows and colors cognitive test (ACCT): a new verbal-motor free cognitive measure for executive functions in ALS. PLoS One 13:e0200953. doi: 10.1371/journal.pone.0200953
Poletti, B., Solca, F., Carelli, L., Faini, A., Madotto, F., Lafronza, A., et al. (2018b). Cognitive-behavioral longitudinal assessment in ALS: the Italian edinburgh cognitive and behavioral ALS screen (ECAS). Amyotroph. Lateral. Scler. Frontotemporal. Degener. 19, 387–395. doi: 10.1080/21678421.2018.1473443
Poletti, B., Carelli, L., Solca, F., Lafronza, A., Pedroli, E., Faini, A., et al. (2017a). An eye-tracker controlled cognitive battery: overcoming verbal-motor limitations in ALS. J. Neurol. 264, 1136–1145. doi: 10.1007/s00415-017-8506-z
Poletti, B., Carelli, L., Solca, F., Lafronza, A., Pedroli, E., Faini, A., et al. (2017b). An eye-tracking controlled neuropsychological battery for cognitive assessment in neurological diseases. Neurol. Sci. 38, 595–603. doi: 10.1007/s10072-016-2807-3
Poletti, B., Solca, F., Carelli, L., Madotto, F., Lafronza, A., Faini, A., et al. (2016). The validation of the Italian Edinburgh cognitive and behavioural ALS screen (ECAS). Amyotroph. Lateral. Scler. Frontotemporal. Degener. 17, 489–498. doi: 10.1080/21678421.2016.1183679
Portet, F., Cadilhac, C., Touchon, J., and Camu, W. (2001). Cognitive impairment in motor neuron disease with bulbar onset. Amyotroph. Lateral. Scler. Other Motor. Neuron. Disord. 2, 23–29. doi: 10.1080/146608201300079382
Raaphorst, J., De Visser, M., Linssen, W., De Haan, R., and Schmand, B. (2010). The cognitive profile of amyotrophic lateral sclerosis: a meta-analysis. Amyotroph. Lateral. Scler. 11, 27–37. doi: 10.3109/17482960802645008
Rascovsky, K., Hodges, J., Knopman, D., Mendez, M., Kramer, J., Neuhaus, J., et al. (2011). Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia. Brain 134, 2456–2477. doi: 10.1093/brain/awr179
Rippon, G., Scarmeas, N., Gordon, P., Murphy, P., Albert, S., Mitsumoto, H., et al. (2006). An observational study of cognitive impairment in amyotrophic lateral sclerosis. Arch. Neurol. 63, 345–352. doi: 10.1001/archneur.63.3.345
Roche, J., Rojas-Garcia, R., Scott, K., Scotton, W., Ellis, C., Burman, R., et al. (2012). A proposed staging system for amyotrophic lateral sclerosis. Brain 135, 847–852. doi: 10.1093/brain/awr351
Röttig, D., Leplow, B., Eger, K., Ludolph, A., Graf, M., and Zierz, S. (2006). Only subtle cognitive deficits in non–bulbar amyotrophic lateral sclerosis patients. J. Neurol. 253, 333–339. doi: 10.1007/s00415-005-0992-8
Sbrollini, B., Preti, A., Zago, S., Papagno, C., Appollonio, I., and Aiello, E. (2022). Language impairment in motor neuron disease phenotypes different from classical amyotrophic lateral sclerosis: a review. Aphasiology 36, 1373–1396. doi: 10.1080/02687038.2021.1959017
Schreiber, H., Gaigalat, T., Wiedemuth-Catrinescu, U., Graf, M., Uttner, I., Muche, R., et al. (2005). Cognitive function in bulbar–and spinal–onset amyotrophic lateral sclerosis: a longitudinal study in 52 patients. J. Neurol. 252, 772–781. doi: 10.1007/s00415-005-0739-6
Shah, J., Pedraza, O., Festic, E., and Oskarsson, B. (2021). The relationship between ventilatory function and cognitive and behavioral impairment in ALS. Amyotroph. Lateral. Scler. Frontotemporal. Degener. 22(Suppl. 1), 62–67. doi: 10.1080/21678421.2021.1924206
Shellikeri, S., Karthikeyan, V., Martino, R., Black, S., Zinman, L., Keith, J., et al. (2017). The neuropathological signature of bulbar-onset ALS: a systematic review. Neurosci. Biobehav. Rev. 75, 378–392. doi: 10.1016/j.neubiorev.2017.01.045
Shellikeri, S., Keith, J., Black, S., Zinman, L., and Yunusova, Y. (2020). Neuropathology of speech network distinguishes bulbar from nonbulbar amyotrophic lateral sclerosis. J. Neuropathol. Exp. Neurol. 79, 284–295. doi: 10.1093/jnen/nlz130
Smith, R., Macklin, E., Myers, K., Pattee, G., Goslin, K., Meekins, G., et al. (2018). Assessment of bulbar function in amyotrophic lateral sclerosis: validation of a self-report scale (center for neurologic study bulbar function scale). Eur. J. Neurol. 25, 907–e66. doi: 10.1111/ene.13638
Solca, F., Aiello, E., Torre, S., Carelli, L., Ferrucci, R., Verde, F., et al. (2023). Prevalence and determinants of language impairment in non-demented amyotrophic lateral sclerosis patients. Eur. J. Neurol. 30, 606–611.
Steinbach, R., Prell, T., Gaur, N., Roediger, A., Gaser, C., Mayer, T., et al. (2021). Patterns of grey and white matter changes differ between bulbar and limb onset amyotrophic lateral sclerosis. NeuroImage Clin. 30:102674.
Sterling, L., Jawaid, A., Salamone, A., Murthy, S., Mosnik, D., McDowell, E., et al. (2010). Association between dysarthria and cognitive impairment in ALS: a prospective study. Amyotroph. Lateral. Scler. 11, 46–51. doi: 10.3109/17482960903207997
Trojsi, F., Siciliano, M., Femiano, C., Santangelo, G., Lunetta, C., Calvo, A., et al. (2017). Comorbidity of dementia with amyotrophic lateral sclerosis (ALS): insights from a large multicenter Italian cohort. J. Neurol. 264, 2224–2231. doi: 10.1007/s00415-017-8619-4
Watanabe, Y., Raaphorst, J., Izumi, Y., Yoshino, H., Ito, S., Adachi, T., et al. (2020). Cognitive and behavioral status in Japanese ALS patients: a multicenter study. J. Neurol. 267, 1321–1330.
Woolley, S., and Rush, B. (2017). Considerations for clinical neuropsychological evaluation in amyotrophic lateral sclerosis. Arch. Clin. Neuropsychol. 32, 906–916.
Yang, T., Hou, Y., Li, C., Cao, B., Cheng, Y., Wei, Q., et al. (2021). Risk factors for cognitive impairment in amyotrophic lateral sclerosis: a systematic review and meta-analysis. J. Neurol. Neurosurg Psychiatry 92, 688–693. doi: 10.1136/jnnp-2020-325701
Yunusova, Y., Plowman, E., Green, J., Barnett, C., and Bede, P. (2019). Clinical measures of bulbar dysfunction in ALS. Front. Neurol. 10:106. doi: 10.3389/fneur.2019.00106
Zago, S., Lorusso, L., Aiello, E., Ugolini, M., Poletti, B., Ticozzi, N., et al. (2022). Cognitive and behavioral involvement in ALS has been known for more than a century. Neurol. Sci. 43, 6741–6760. doi: 10.1007/s10072-022-06340-0
Keywords: bulbar, Frontotemporal Degeneration, cognition, neuropsychology, amyotrophic lateral sclerosis
Citation: Aiello EN, Solca F, Torre S, Patisso V, De Lorenzo A, Treddenti M, Colombo E, Maranzano A, Morelli C, Doretti A, Verde F, Silani V, Ticozzi N and Poletti B (2023) Bulbar involvement and cognitive features in amyotrophic lateral sclerosis: a retrospective study on 347 patients. Front. Aging Neurosci. 15:1217080. doi: 10.3389/fnagi.2023.1217080
Received: 04 May 2023; Accepted: 26 June 2023;
Published: 20 July 2023.
Edited by:
Andrea Calvo, University of Turin, ItalyReviewed by:
Nilo Riva, San Raffaele Hospital (IRCCS), ItalyCopyright © 2023 Aiello, Solca, Torre, Patisso, De Lorenzo, Treddenti, Colombo, Maranzano, Morelli, Doretti, Verde, Silani, Ticozzi and Poletti. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Barbara Poletti, Yi5wb2xldHRpQGF1eG9sb2dpY28uaXQ=; orcid.org/0000-0003-4398-2051
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.