 Ondrej Bezdicek1*†‡
Ondrej Bezdicek1*†‡ Josef Mana1†‡
Josef Mana1†‡ Filip Růžička1Filip Havlik1†
Filip Růžička1Filip Havlik1† Anna Fečíková1
Anna Fečíková1 Tereza Uhrová1Evžen Růžička1†Dušan Urgošík2Robert Jech1†
Tereza Uhrová1Evžen Růžička1†Dušan Urgošík2Robert Jech1†- 1Department of Neurology and Centre of Clinical Neuroscience, First Faculty of Medicine and General University Hospital in Prague, Charles University, Prague, Czechia
- 2Department of Stereotactic and Radiation Neurosurgery, Na Homolce Hospital, Prague, Czechia
Background: Everyday functioning and instrumental activities of daily living (IADL) play a vital role in preserving the quality of life in patients with Parkinson’s disease (PD) after deep brain stimulation of the subthalamic nucleus (STN-DBS).
Objective: The main goal of the current study was to examine IADL change in pre-and post-surgery of the STN-DBS. We also analyzed the influence of the levodopa equivalent daily dose (LEDD) and global cognitive performance (Dementia Rating Scale; DRS-2) as covariates in relation to IADL.
Methods: Thirty-two non-demented PD patients were administered before and after STN-DBS neurosurgery the Penn Parkinson’s Daily Activities Questionnaire (PDAQ; self-report), the DRS-2 and Beck Depression Inventory (BDI-II) to assess IADL change, global cognition, and depression.
Results: We found a positive effect of STN-DBS on IADL in the post-surgery phase. Moreover, lower global cognition and lower LEDD are predictive of lower IADL in both pre-surgery and post-surgery examinations.
Summary/Conclusion: STN-DBS in PD is a safe method for improvement of everyday functioning and IADL. In the post-surgery phase, we show a relation of IADL to the severity of cognitive impairment in PD and to LEDD.
Highlights
- There is a significant effect of STN-DBS treatment on everyday functioning improvement 1 year after the surgery in Parkinson’s disease patients.
- We found also positive effects of cognitive performance, and LEDD as well as a negative effect of depressive symptoms on everyday functioning both before and after STN-DBS surgery.
- We provide a table detailing what changes can one expect in a patient’s everyday functioning depending on their pre- and post-surgery LEDD.
Introduction
Deficits in everyday functioning are highly associated with the evolution of Parkinson’s disease (PD) (Young et al., 2010; Giovannetti et al., 2012; Altieri et al., 2021; Becker et al., 2022). Especially in clinically advanced stages when patients are suffering from deteriorating cognitive impairment such as mild cognitive impairment (PD-MCI) and later from dementia due to PD (PDD), instrumental activities of daily living (IADL) such as meal preparation, shopping, and medication management are afflicted (Pirogovsky et al., 2014; Foster and Doty, 2021). A standardized assessment of IADL can be specific for the diagnosis of PDD (Christ et al., 2013). Those PD-MCI patients who show more impaired cognitive- than motor-driven IADL have a higher hazard of conversion to PDD (Becker et al., 2020). Regarding PD motor dysfunction subtypes, de novo PD patients with postural instability-gait difficulties motor subtype present on average larger deterioration in IADL than those with tremor dominant subtype (Hariz and Forsgren, 2011).
Deep brain stimulation (DBS) of the subthalamic nucleus (STN-DBS) is a standard treatment for medication-refractory movement symptoms of PD (Perlmutter and Mink, 2006; Bronstein et al., 2011; Okun, 2014; Mueller et al., 2020). A number of works have shown that this therapy is highly effective in regaining control over PD motor symptoms and improving patients’ quality of life (QoL), as well as in reducing the levodopa equivalent daily dose (LEDD) (Tomlinson et al., 2010; Bratsos et al., 2018; Tödt et al., 2022).
Hence DBS is a treatment option for advanced PD when the side effects of dopaminergic treatment are intolerable (Moro and Lang, 2006; Bronstein et al., 2011) and there are the differential effects of levodopa vs. DBS on brain motor activity (Mueller et al., 2020), a relation between LEDD and IADL in PD in pre- and post-surgery should come under closer scrutiny.
The effect on QoL is stable in time in a 1-year perspective and the IADL performance correlates with the improvement in QoL (Gorecka-Mazur et al., 2019). On the contrary, activity limitations are the strongest predictor of QoL (Soh et al., 2013). However, the improvement after 12 months after the surgery was noticeable only in some IADLs, especially in shopping and food preparation (Gorecka-Mazur et al., 2019).
Previous research of IADL in PD patients after STN-DBS used general IADL scales, such as Lawton’s IADL scale, to investigate everyday performance (Gorecka-Mazur et al., 2019) or the Unified Parkinson’s Disease Rating Scale (UPDRS part II) or the Schwab and England Activities of Daily Living (Deuschl et al., 2006; Kleiner-Fisman et al., 2010; Odekerken et al., 2013; Jiang et al., 2015; Tödt et al., 2022). In the current study, we sought to use a disease-specific questionnaire developed to assess IADLs in PD (Brennan et al., 2016a). The Penn Parkinson’s Daily Activities Questionnaire (PDAQ) shows a high discriminant validity between PD with normal cognition in comparison to PD-MCI and PDD (Brennan et al., 2016a).
Cognitive impairment is a core non-motor feature of Parkinson’s disease (PD) and a major source of disability in PDD (Cahn et al., 1998; Bronnick et al., 2006). Especially, impaired global cognition and deficits in attention and visual memory are the most predictive of developing a PDD (Lawson et al., 2021). PD-MCI as a pre-dementia phase and PDD both represent risk factors that are associated with poorer everyday functioning and IADL (Litvan et al., 2012; Martin et al., 2013; Pirogovsky et al., 2013; Pirogovsky et al., 2014; Hoogland et al., 2017; Schmitter-Edgecombe et al., 2021).
Thus, the principal aim of the study was to assess post-surgery change (i.e., decline or improvement) in self-reported IADL in relation to the pre-surgery evaluation. Second, we aimed to outline the relationship of IADL to dopaminergic medication, depressive symptoms and cognitive performance in PD patients treated with STN DBS.
Materials and Methods
Participants
Parkinson’s disease patients were recruited from the Movement Disorders Center, Department of Neurology, First Faculty of Medicine and General University Hospital in Prague. All patients were examined by a neurologist specializing in movement disorders and met the UK PD Society Brain Bank criteria (Hughes et al., 1992). All of them were suffering from motor fluctuations and/or disabling dyskinesias and were indicated for treatment with STN DBS (demographic and clinical details in Table 1). Exclusion criteria were as follows: PD dementia according to MDS criteria (Emre et al., 2007), atypical or secondary parkinsonism, severe or moderate depression according to Beck Depression Inventory (BDI-II) and psychiatric evaluation, florid psychotic manifestations (hallucinations or delusions), anticholinergic medications and other medical or neurological conditions potentially resulting in cognitive impairment (e.g., epileptic seizure, tumor, stroke, or head trauma). All PD patients were under dopaminergic therapy (i.e., levodopa, dopamine agonist, or a combination of them), and levodopa’s equivalent daily dose for each patient was calculated before and after surgery (Tomlinson et al., 2010). Bilateral STN DBS implantation was performed as previously described (Jech et al., 2006; Urgosik et al., 2011; Jech et al., 2012). STN DBS parameters are reported in Table 1. A total of 32 PD patients (mean age 55.5 ± 7.8 years pre-surgery, 56% males) participated in the study. Patients were assessed before (4.9 ± 5.6 months) and 1 year after the surgery (12.4 ± 0.9 months). All patients gave their written informed consent for participation. The study was approved by the Ethics Committee of the General University Hospital in Prague, Czechia.
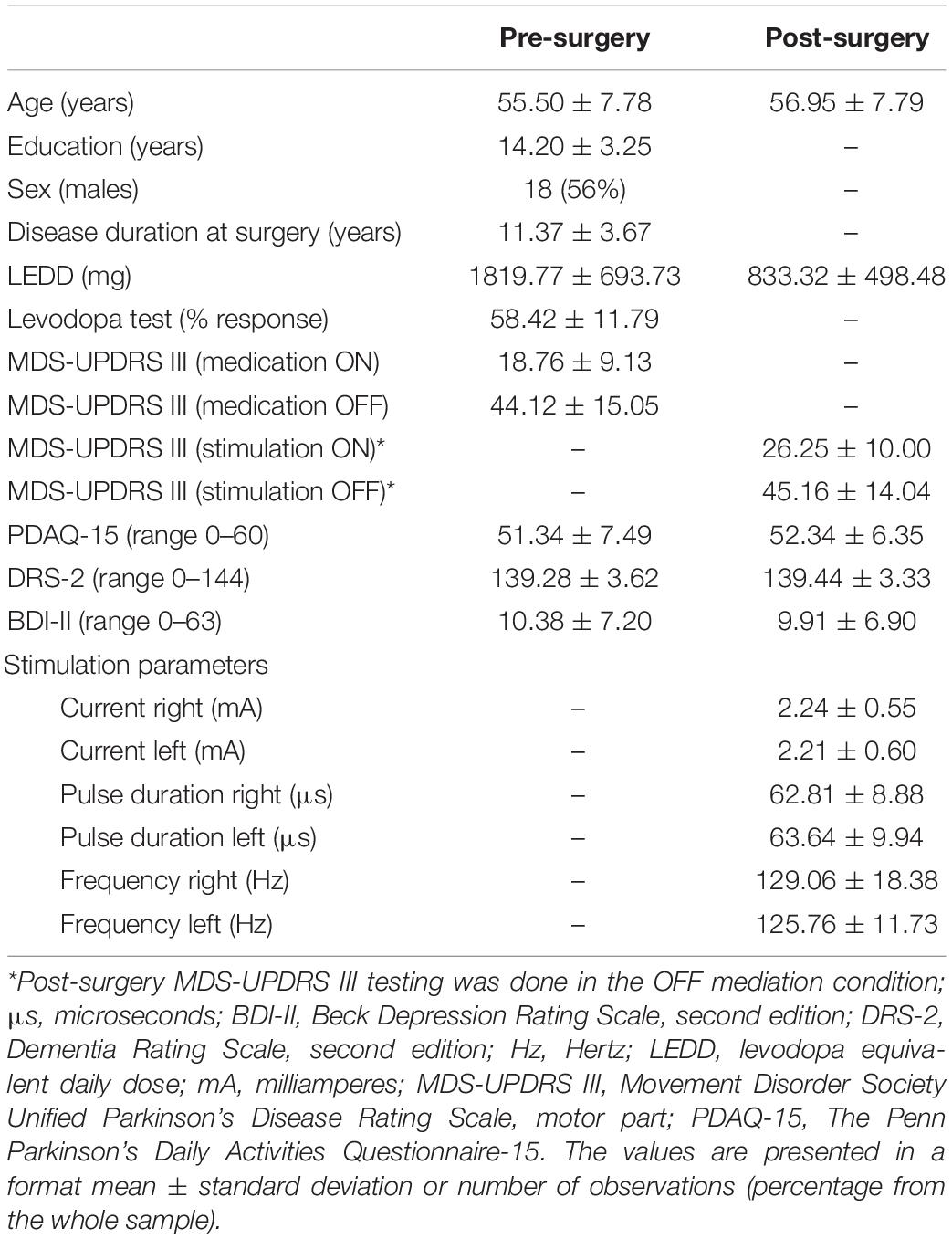
Table 1. Demographic, clinical, and cognitive characteristics of the sample (N = 32).
Assessments
Neuropsychological Examination
All patients underwent a comprehensive and recommended pre-surgery (pre-test) evaluation including neuropsychological, psychiatric, and neurological examinations by a trained movement disorders specialist in each field (Kubu, 2018). The patients were followed up in a post-surgery (post-test) 1 year after the neurosurgery with the identical protocol (mean retest interval 12.4 ± 0.9 months). The pre-surgery neuropsychological assessment was performed with regular dopaminergic therapy (ON medication), in the post-surgery phase, patients were examined in both STN DBS ON with optimal stimulation parameters and the ON medication condition.
The neuropsychological assessment in pre-test–post-test followed the standard Movement Disorder Society neuropsychological battery at Level I for PD-MCI (Litvan et al., 2012; Bezdicek et al., 2016; Bezdicek et al., 2017): the cognitive performance was assessed by Mattis Dementia Rating Scale, second edition (DRS-2) (Jurica et al., 2001; Bezdicek et al., 2015). The IADLs and everyday functioning were measured by the PDAQ self-report (Shulman et al., 2016). The PDAQ brief version is an item-response theory (IRT)-based questionnaire consisting of 15 items, showing very good psychometric properties that were developed specifically for IADL deficits in PD (Brennan et al., 2016a,b). Finally, depressive symptoms were assessed with the Beck Depression Scale, second edition (BDI-II) (Beck et al., 1996; Ciharova et al., 2020).
Neurological and Psychiatric Examination
All patients underwent a comprehensive clinical evaluation that included medical history, medication status, and motor status by the Movement Disorders Society Unified Parkinson’s Disease Rating Scale, part three (MDS-UPDRS-III). Scores of patients who underwent the older version of the Unified Parkinson’s Disease Rating Scale (UPDRS-III) were converted to the MDS-UPDRS III scale using the method described by Hentz et al. (2015). All PD patients were treated with dopaminergic therapy, consisting of levodopa, dopamine agonists or a combination of them, and assessed in medication ON. Four days before the patient’s visit, dopamine agonists were substituted with equivalent doses of levodopa. The LEDD was calculated at each assessment time-point according to Tomlinson et al. (2010).
A psychiatric evaluation was done before the surgery to exclude pre-psychotic or florid psychotic symptoms or mood disorders including suicidal thoughts or any other potential risky neuropsychiatric complications after the neurosurgery (Foley et al., 2018).
Causal Assumptions
Our causal assumptions are represented in the form of a directed acyclic graph (DAG) depicted in Figure 1. Representing study design via a DAG offers several benefits including serving as an explicit statement of causal assumptions that can be questioned by other researchers, providing a framework for the interpretation of results and indicating which covariates should be controlled during the analysis (Pearl, 2009; McElreath, 2020). In short, in the current study, we assume that clinicians based their decision on whether to treat a PD patient with STN DBS in part of the patient’s preoperative IADL, objective cognitive performance and LEDD. While the level of depressive symptoms as assessed by BDI-II is not directly considered for STN DBS treatment in our center, patients with the depressive syndrome as assessed by an independent psychiatric evaluation are rejected for STN DBS due to possible suicidal attempts, and since the depressive symptom also likely leads to high BDI-II score, we assume a common cause relationship between pre-surgery BDI-II and STN DBS surgery as indicated by the dashed double-headed arrow in Figure 1. On the other hand, DBS treatment itself is assumed to influence postoperative IADL, objective cognitive performance, level of depressive symptoms and LEDD. Cross-sectionally (i.e., either pre-or post-surgery), LEDD is assumed to influence depressive symptoms directly and objective cognitive performance and IADL both directly as well as indirectly via the effect of depressive symptoms. Finally, because IADL was repeatedly assessed by an IRT-based PDAQ questionnaire we expect item- and patient-specific effects on the outcomes.
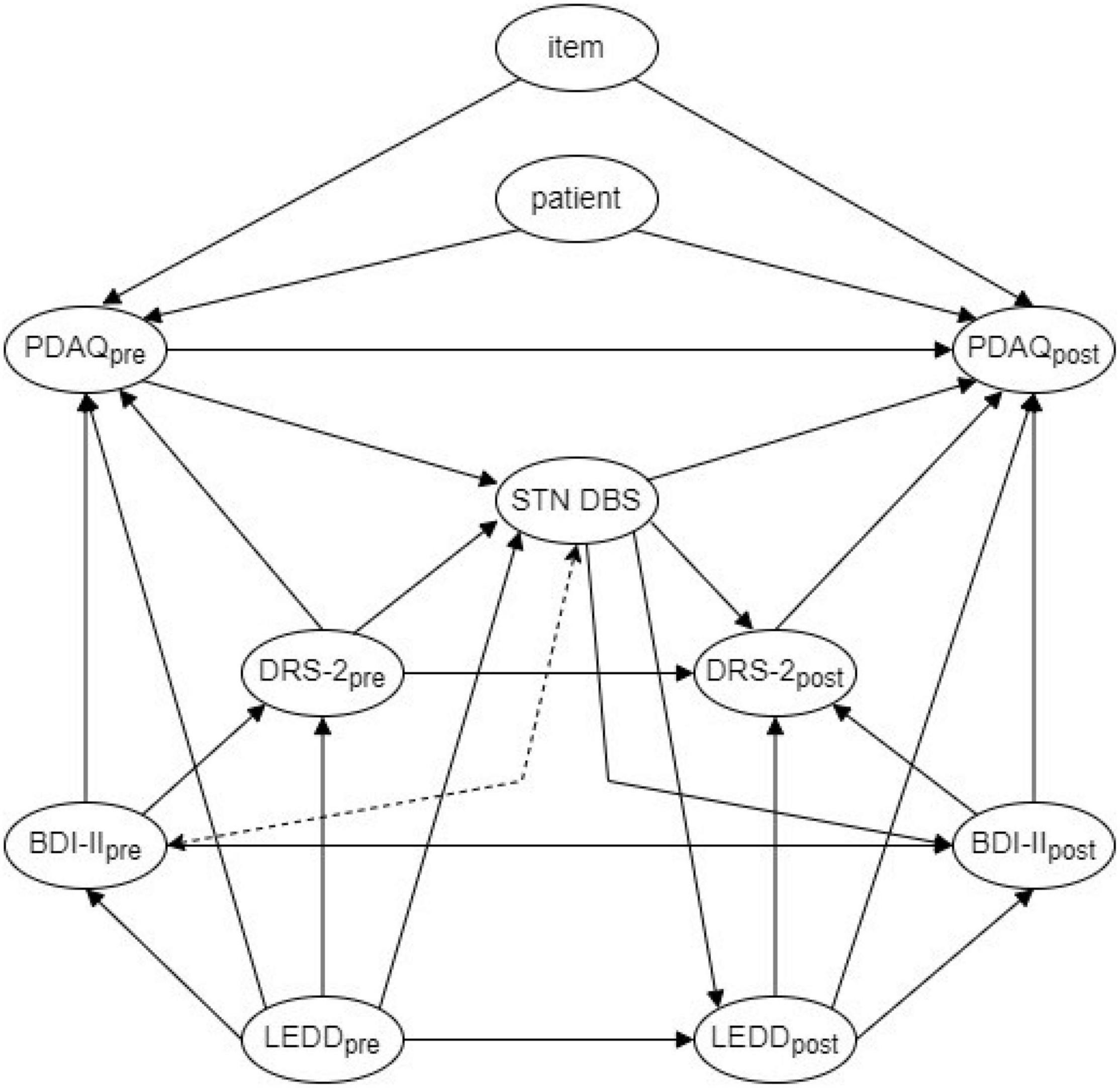
Figure 1. A directed acyclic graph representing causal assumptions of the relationships between included variables. STN DBS, subthalamic nucleus deep brain stimulation; BDI-II, Beck Depression Inventory before DBS treatment (BDI-IIpre) and after DBS treatment (BDI-IIpost); DRS-2, Dementia Rating Scale, second edition before DBS treatment (DRS-2pre) and after DBS treatment (DRS-2post); LEDD, levodopa equivalent daily dose before DBS treatment (LEDDpre) and after DBS treatment (LEDDpost); PDAQ, The Penn Parkinson’s Daily Activities Questionnaire before DBS treatment (PDAQpre) and after DBS treatment (PDAQpost). STN DBS was considered to be adjusted for in each of our analyses due to the lack of a control group. Dashed double arrow between BDI-IIpre and STN DBS indicates a common cause assumption—this is because even though BDI-II is not used directly to decide whether patients receive STN DBS in our center, patients with clinical depression according to an independent psychiatric evaluation are both rejected to STN DBS and at risk of high BDI-II.
Since our sample contains only patients treated with STN DBS and no control group, we were not able to estimate either the total or direct effect of DBS on IADL. However, based on the DAG in Figure 1, we can estimate the direct effects of objective cognitive performance, depressive symptoms and LEDD on IADL as well as direct post-surgery change in IADL in STN DBS patients by controlling for LEDD, objective cognitive performance and depressive symptoms as well as item- and patient-specific effects.
Statistical Analysis
Following the implications of DAG presented in Figure 1, the data were analyzed by a generalized linear mixed model (GLMM) with responses to each item of PDAQ as an outcome, the time of assessment (pre- vs. post-surgery), LEDD, DRS-2, and BDI-II as fixed effects and item- and patient-specific random effects. Interactions of the time of assessment and all LEDD (medication), DRS-2 (cognitive performance), and BDI-II (depressive symptoms) were also included and modeled as fixed effects to explore whether the effect of the latter three variables on IADL changes after as compared to before STN DBS surgery. Since PDAQ consists of 15 items scored by the patient’s self-reported difficulty in performing each specific IADL on a Likert scale ranging from 0 (“cannot do”) to 4 (“no difficulty”), the outcome was modeled by an order-logit response function. The ordered-logit is a generalization of the binary logistic response function that was designed to handle ordinal variables (Liddell and Kruschke, 2018; Bürkner and Vuorre, 2019). The results of an ordered-logit model consist of regression parameters for effect estimates on a logit scale (similar to common logistic regression).
The model was fitted using the Hamiltonian Monte Carlo (HMC) sampling algorithm in Stan version 2.21.0 (Stan Development Team, 2021) accessed via brms package (Bürkner and Vuorre, 2019) in R version 4.0.5 (R Core Team, 2021) using four independent chains with 1,500 total and 500 warm-up iterations. Full Bayesian statistical inference was used to specify the model and evaluate the results. We used Student-t priors with zero mean, a scale of 2.5 and three degrees of freedom for Intercepts and random effects’ variance components and regularizing Normal priors with zero mean and standard deviation of 0.5 for the fixed effects. GLMM parameters were described on a logit scale by their medians, 95% highest density posterior probability intervals (PPIs) and the probability of being positive (i.e., the probability that a predictor has a positive effect on IADL). A 95% PPI can be interpreted such that a given parameter lies within this interval with a 95% probability. If desired, an effect can be regarded statistically significant (on a 5% level) if the corresponding 95% PPI excludes zero. To evaluate post-surgery change in IADL on the outcome scale we provide posterior predictions comparing the contrast between post-surgery minus pre-surgery responses to PDAQ across patients and items. Scripts with all analyses from this article are deposited here: https://github.com/josefmana/dbs_postop_iADL.
Results
Characterizing the Sample
Characteristics of the sample are presented in Table 1. A total of 32 patients with PD and bilateral STN-DBS implanted with DBS devices between 2018 and 2019 met the inclusion criteria. Patients’ responses to each PDAQ item before and after the STN-DBS surgery are depicted in Supplementary Figure 1.
Results of the Generalized Linear Mixed Model
The HMC sampling algorithm successfully converged to stable posterior distribution (all s < 1.01). Fixed effects’ parameters are presented in Table 2. There was a 99.4% probability that patients report improved IADL post- as compared to pre-surgery when covariates are kept constant (the main effect of the time of assessment). Moreover, 95% PPI of this effect excluded zero and the effect can thus be regarded as statistically significant. Similarly, for DRS-2, there was a 98.8% probability that it has a positive main effect on IADL (i.e., higher scores in DRS-2 positively affected IADL regardless of the time of assessment) with 95% PPI excluding zero. On the other hand, while both LEDD and BDI-II showed a trend of the positive main effect on IADL, their 95% PPIs included zero. There was a trend of an interaction between the time of assessment and LEDD, DRS-2, and BDI-II. However, the 95% PPI for these effects included zero as well as moderate negative values and these effects thus cannot be regarded as statistically significant.
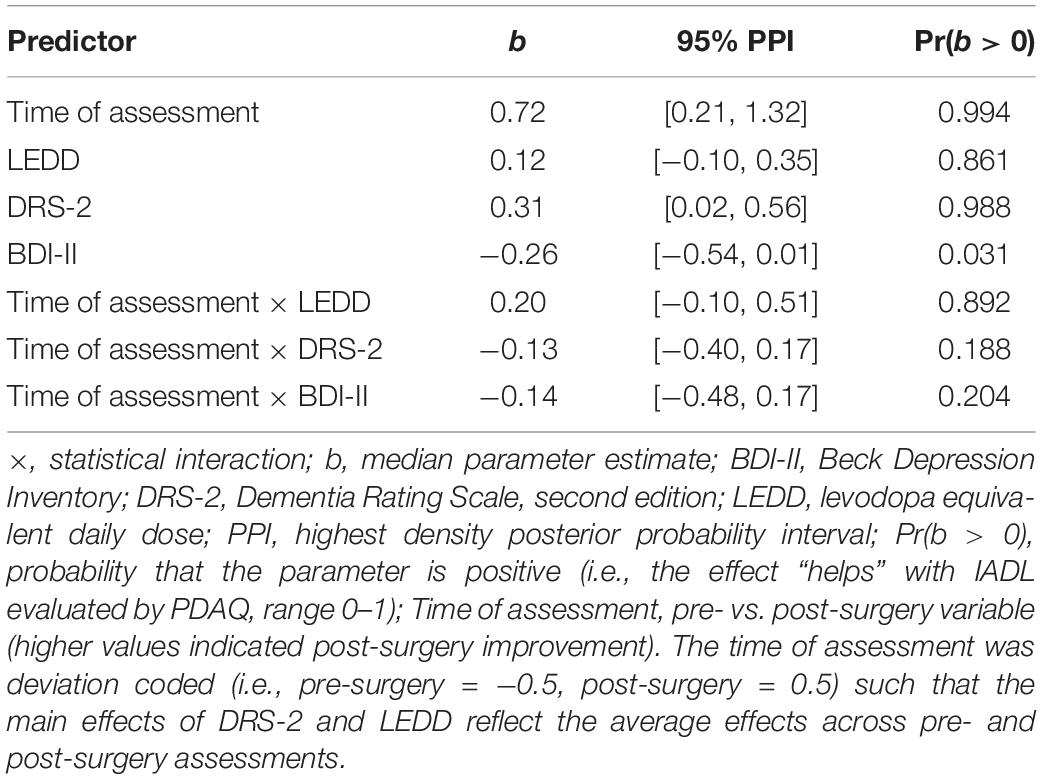
Table 2. Fixed effect parameters of the ordered-logit generalized linear mixed model.
Figure 2 depicts the main effects of assessment time, LEDD, DRS-2, and BDI-II on responses to PDAQ on the outcome scale (i.e., probabilities that a patient responds with each of the options 0–4). Figure 2 shows that when evaluating difficulties in IADL patients rarely selected options 0–2 (“cannot do,” “a lot,” and “somewhat,” respectively). The main effects of the time of assessment, DRS-2, BDI-II, and LEDD were primarily due to increased frequency of response four (“none”) at the expense of response three (“a little”) after the surgery and in patients with high LEDD and DRS-2 and low BDI-II scores. When LEDD, DRS-2, and BDI-II were statistically held at the average in-sample pre-surgery level, the post-surgery probability that a patient responds to any PDAQ item with option zero (“cannot do”) decreased by 0.1% (95% PPI [−0.4, 0.0], pre: 0.3% [0.1, 0.7], post: 0.1% [0.0, 0.4]), the probability of response one (“a lot”) decreased by 0.4% (95% PPI [−1.2, −0.1], pre: 0.9% [0.3, 2.1], post: 0.5% [0.1, 1.1]), the probability of response two (“somewhat”) decreased by 1.9% (95% PPI [−4.6, −0.3], pre: 4.1% [1.7, 8.4], post: 2.1% [0.6, 4.7]), the probability of response three (“a little”) decreased by 12.3% (95% PPI [−22.2, −3.4], pre: 36.1% [21.8, 51.1], post: 22.9% [10.1, 39.5]), and the probability of response four (“none”) increased by 15.0% (95% PPI [3.1, 26.4], pre: 58.5% [39.2, 77.1], post: 74.4% [55.6, 90.1]). In other words, the direct effect of DBS on IADL improvement is due to a significantly lower frequency of patients with little IADL difficulties (response three “a little” in all PDAQ items) and a significantly higher frequency of patients with no IADL difficulties (response four “none” in all PDAQ items) 1 year after the STN-DBS surgery. This pattern of responses holds across different LEDD levels (see Table 3).
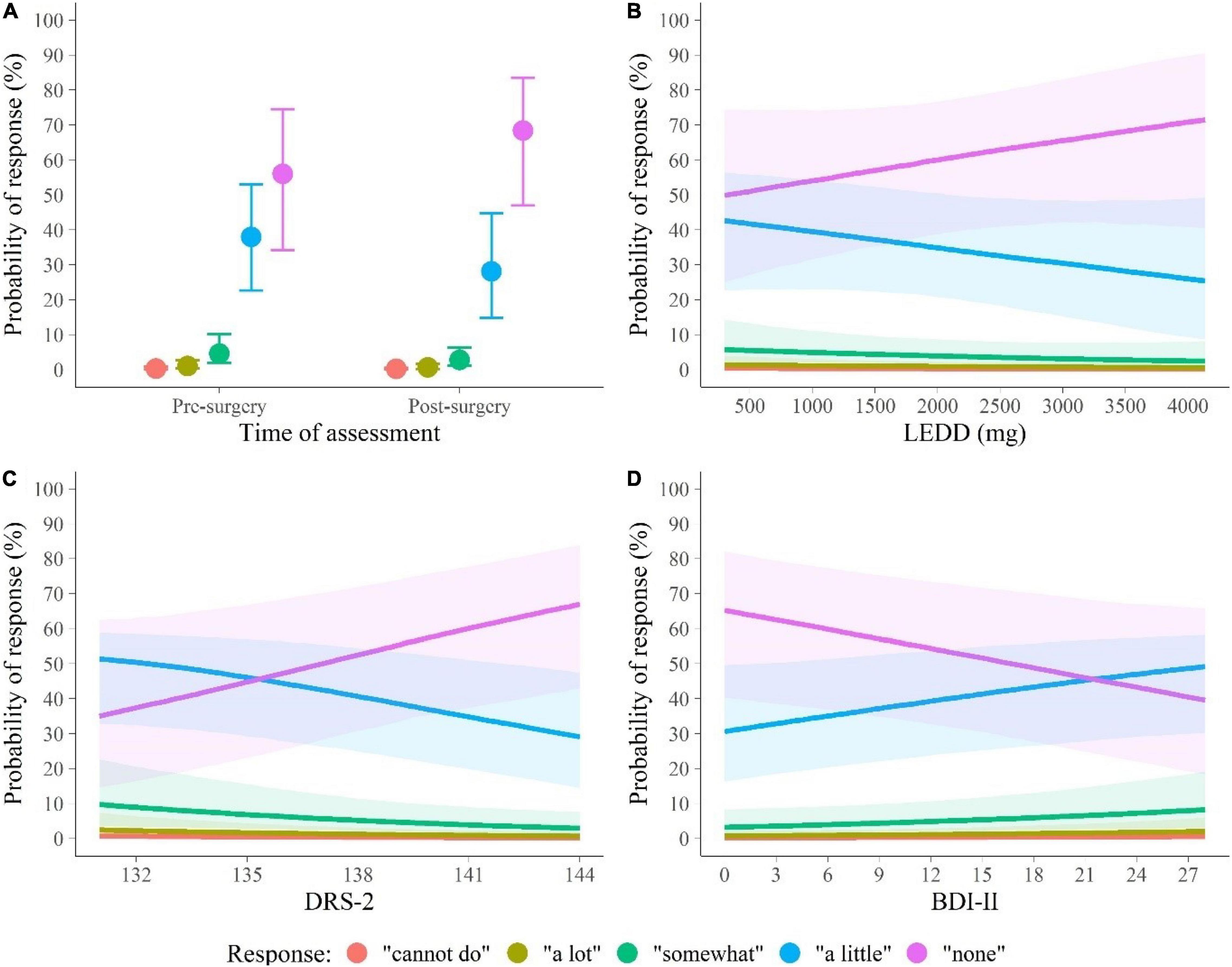
Figure 2. Summary of the marginal distributions of main effects of (A) the time of assessment, (B) LEDD, (C) DRS-2, and (D) BDI-II on IADL. BDI-II, Beck Depression Inventory; DRS-2, Dementia Rating Scale, second edition; IADL, instrumental activities of daily living; LEDD, levodopa equivalent daily dose. Points (lines) represent the median probability of each response (labeled by distinct colors) to the items of Penn Parkinson’s Daily Activities Questionnaire-15 (PDAQ-15), and whiskers (shades) represent 95% posterior probability intervals (PPIs).
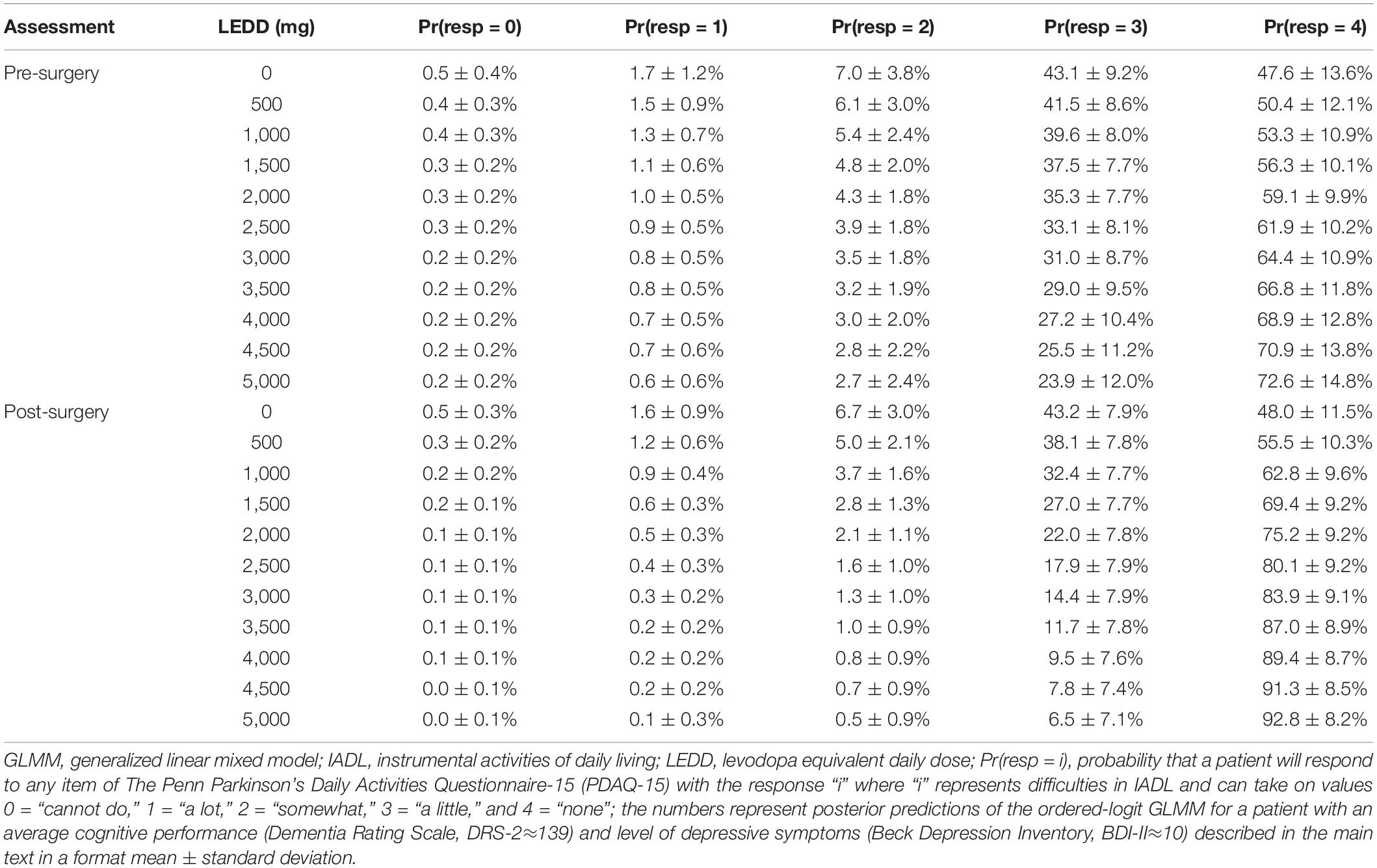
Table 3. Expected response probabilities of difficulty in IADL stratified by the time of assessment and levodopa equivalent daily dose derived from the ordered-logit GLMM.
Discussion
This study examined IADL in a cohort of PD patients undergoing STN-DBS treatment by using pre-test (pre-surgery) and post-test (post-surgery) measurements. Regarding the complexity of DBS neurosurgical treatment, only IADL self-report and cognitive, depressive, and clinical correlates were included in the current research. In comparison to other studies that concentrated either on IADL predictors or the quantification of the degree of IADL deficits in PD-NC in comparison to PD-MCI (Rosenthal et al., 2010; Pirogovsky et al., 2013; Foster, 2014; Fellows and Schmitter-Edgecombe, 2019; Becker et al., 2020; Cholerton et al., 2020; Foster and Doty, 2021; Schmitter-Edgecombe et al., 2021; Becker et al., 2022), or comparison and development of specific methods and sensitive IADL items for PD (Brennan et al., 2016a,b; Fellows and Schmitter-Edgecombe, 2019; Sulzer et al., 2020; Schmitter-Edgecombe et al., 2021), whereas our study focused selectively on the comparison of IADL in PD before and after STN-DBS with a PD-specific questionnaire (Brennan et al., 2016a,b). We based our estimate of the post-surgery IADL change on an explicit causal model allowing for easier model criticism and derivation of proper covariates to include in our model (Pearl, 2009; McElreath, 2020).
Based on our model and data, the post-surgery IADL of PD patients improves compared to the pre-surgery level. At the same time, higher cognitive performance and higher LEDD are indicative of higher IADL both before and after STN-DBS surgery. More specifically, our analysis focused on the direct effects of all included predictors, in other words, the estimation of IADL post-surgery improvement was thus adjusted on LEDD, DRS-2, and BDI-II. While this approach allowed us to derive a more accurate estimate of the direct effect DBS can have on IADL performance in a cohort of implanted patients, this effect will be in the real-life clinical settings contaminated by DBS effects on other variables predictive of IADL change. Indeed, according to our results, the IADL declines when LEDD is decreased both before and after surgery, however, a decrease in LEDD is often a desirable outcome of DBS treatment (Molinuevo et al., 2000; Russmann et al., 2004). Surprisingly, there was a trend of an interaction between the time of assessment and LEDD indicating that higher LEDD may be more important for IADL improvement post-surgery than pre-surgery.
As a consequence of the above described putatively opposing effects of DBS and post-surgery LEDD reduction, medical professionals may want to carefully consider how much to reduce the LEDD after STN-DBS surgery in PD patients to avoid negative effects on IADL. In the current study, these considerations are quantitatively represented in Table 3 which can be used to guide decisions on how much to decrease the LEDD after STN-DBS surgery while avoiding adverse effects on IADL. For instance, based on Table 3, one can expect that a patient with pre-surgery LEDD of 2,500 mg will report no difficulties (response four) in IADL about 62% of the time while reporting little difficulties (response three) about 33% of the time. If a physician was to reduce this patient’s LEDD after the surgery to 1,000 mg, one can expect that patient’s IADL would remain similar to the pre-surgery level reporting no difficulties about 63% of the time and little difficulties about 33% of the time. However, if the LEDD was discontinued altogether, the expectation of IADL difficulties would increase to a level where one would expect the patient to report no problems only 48% of the time and little problems about 43% of the time. In this case, it would thus be advisable not to reduce LEDD below 1,000 mg if the patient wanted to avoid possible adverse effects on IADL. This finding can be considered as an example of the “masked” effect (McElreath, 2020) with LEDD playing a crucial role in modulating the effect of STN-DBS on IADLs.
The present study suffers from several limitations that must be clearly stated. First, we did not apply multiple IADL assessment methods (i.e., observed everyday activities, self- and informant-reports) which would show different facets of IADL (Fellows and Schmitter-Edgecombe, 2019; Schmitter-Edgecombe et al., 2021). However, it is questionable in our PD sample with PD-NC or PD-MCI in the early stages of cognitive decline if self-rating is not more sensitive to the impact of cognitive changes on IADL function than informant reports (Cholerton et al., 2020). Second, our research is not longitudinal and we are not able to trace long-lasting changes in IADL due to STN-DBS. Third, we do not report data on individual stimulation volumes and functional zones of the STN and their contribution to IADL changes (Tödt et al., 2022). Fourth, a modest sample size regarding DBS research and the apparent lack of cognitive decline after STN-DBS surgery in our sample might have prevented us from observing any significant interaction between the time of assessment and cognitive performance. Fifth, an important limitation of the study is the lack of a control group. The influence of LEDD and global cognition on the improvement of IADL at 1 year of follow-up could be independent of the effect of DBS on motor symptoms. Such comparison cannot be performed due to a lack of a control group. However, based on previous research, the neurostimulation, as compared with medication alone, caused greater improvements from baseline to 6 months and DBS and levodopa have a differential effect on brain motor activity in PD (Deuschl et al., 2006; Mueller et al., 2020).
The current study shows a clear beneficial STN-DBS-induced change in IADL approximately 1-year perspective after the operation. Importantly, we show the IADL post-surgery improvement is related also to LEDD post-surgery medication dose that should not decrease under a certain limit to maintain the positive IADL effect of the surgery. Based on our study, STN-DBS seems as a cognitively safe procedure for the treatment of motor symptoms in PD 1 year after the surgery, however, a lower global cognitive functioning in the pre-surgery phase is associated with lower IADL functioning before and after the operation. Understanding the role of IADL functioning in PD in the pre-surgery phase may help identify those at risk for everyday activities and possibly help to improve interventions to promote functional independence after the electrode implantation.
Data Availability Statement
The original contributions presented in this study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by the Ethics Committee of the General University Hospital in Prague, Czechia. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
OB: conceptualization, data curation, investigation, methodology, supervision, writing—original draft and review and editing. JM: conceptualization, data curation, investigation, formal analysis, methodology, software, visualization, writing—original draft and review and editing. FR, FH, AF, TU, and DU: investigation and writing—review and editing. ER: conceptualization, funding acquisition, investigation, resources, and writing—review and editing. RJ: conceptualization, data acquisition and curation, funding acquisition, investigation, resources, supervision, and writing—review and editing. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the National Institute for Neurological Research, Czech Republic, Programme EXCELES, ID Project No. LX22NPO5107, funded by the European Union—Next Generation EU and also by the Charles University: Cooperatio Program in Neuroscience, also by AZV NV19-04-00233 offered by the Czech Ministry of Health, GA UK 254121 offered by Grant Agency of Charles University and JPND 733051123 offered by the EU Joint Programme on Neurodegenerative Disease Research.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to thank all the patients, family members, and staff from all the units that participated in the study. In particular, we would also like to thank Markéta Fialová, Radka Steinbachová, and Anna Rezková for their management of data collection.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnagi.2022.886491/full#supplementary-material
References
Altieri, M., Garramone, F., and Santangelo, G. (2021). Functional autonomy in dementia of the Alzheimer’s type, mild cognitive impairment, and healthy aging: a meta-analysis. Neurol. Sci. 42, 1773–1783. doi: 10.1007/s10072-021-05142-0
Beck, A. T., Steer, R. A., and Brown, G. (1996). Manual For The Beck Depression Inventory-II. San Antonio, TX: Pearson.
Becker, S., Bäumer, A., Maetzler, W., Nussbaum, S., Timmers, M., Van Nueten, L., et al. (2020). Assessment of cognitive-driven activity of daily living impairment in non-demented Parkinson’s patients. J. Neuropsychol. 14, 69–84. doi: 10.1111/jnp.12173
Becker, S., Pauly, C., Lawton, M., Hipp, G., Bowring, F., Sulzer, P., et al. (2022). Quantifying activities of daily living impairment in Parkinson’s disease using the Functional Activities Questionnaire. Neurol. Sci. 43, 1047–1054. doi: 10.1007/s10072-021-05365-1
Bezdicek, O., Michalec, J., Nikolai, T., Havrankova, P., Roth, J., Jech, R., et al. (2015). Clinical validity of the Mattis Dementia Rating Scale in differentiating mild cognitive impairment in Parkinson’s disease and normative data. Dement. Geriatr. Cogn. Disord. 39, 303–311. doi: 10.1159/000375365
Bezdicek, O., Nikolai, T., Michalec, J., Růžička, F., Havránková, P., Roth, J., et al. (2016). The diagnostic accuracy of parkinson’s disease mild cognitive impairment battery using the movement disorder society task force criteria. Mov. Disord. Clin. Pract. 4, 237–244. doi: 10.1002/mdc3.12391
Bezdicek, O., Sulc, Z., Nikolai, T., Stepankova, H., Kopecek, M., Jech, R., et al. (2017). A parsimonious scoring and normative calculator for the Parkinson’s disease mild cognitive impairment battery. Clin. Neuropsychol. 31, 1231–1247. doi: 10.1080/13854046.2017.1293161
Bratsos, S., Karponis, D., and Saleh, S. N. (2018). Efficacy and Safety of Deep Brain Stimulation in the Treatment of Parkinson’s Disease: a systematic review and meta-analysis of randomized controlled trials. Cureus 10:e3474. doi: 10.7759/cureus.3474
Brennan, L., Siderowf, A., Rubright, J. D., Rick, J., Dahodwala, N., Duda, J. E., et al. (2016a). Development and initial testing of the penn Parkinson’s daily activities questionnaire. Mov Disord 31, 126–134. doi: 10.1002/mds.26339
Brennan, L., Siderowf, A., Rubright, J. D., Rick, J., Dahodwala, N., Duda, J. E., et al. (2016b). The penn Parkinson’s daily activities questionnaire-15: psychometric properties of a brief assessment of cognitive instrumental activities of daily living in Parkinson’s disease. Parkinsonism Relat. Disord. 25, 21–26. doi: 10.1016/j.parkreldis.2016.02.020
Bronnick, K., Ehrt, U., Emre, M., De Deyn, P. P., Wesnes, K., Tekin, S., et al. (2006). Attentional deficits affect activities of daily living in dementia-associated with Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 77, 1136–1142. doi: 10.1136/jnnp.2006.093146
Bronstein, J. M., Tagliati, M., Alterman, R. L., Lozano, A. M., Volkmann, J., Stefani, A., et al. (2011). Deep brain stimulation for Parkinson disease: an expert consensus and review of key issues. Arch. Neurol. 68:165. doi: 10.1001/archneurol.2010.260
Bürkner, P.-C., and Vuorre, M. (2019). Ordinal regression models in psychology: a tutorial. Adv. Methods Pract. Psychol. Sci. 2, 77–101.
Cahn, D. A., Sullivan, E. V., Shear, P. K., Pfefferbaum, A., Heit, G., and Silverberg, G. (1998). Differential contributions of cognitive and motor component processes to physical and instrumental activities of daily living in Parkinson’s disease. Arch. Clin. Neuropsychol. 13, 575–583.
Cholerton, B., Poston, K. L., Tian, L., Quinn, J. F., Chung, K. A., Hiller, A. L., et al. (2020). Participant and study partner reported impact of cognition on functional activities in parkinson’s disease. Mov. Disord. Clin. Pract. 7, 61–69. doi: 10.1002/mdc3.12870
Christ, J. B., Fruhmann Berger, M., Riedl, E., Prakash, D., Csoti, I., Molt, W., et al. (2013). How precise are activities of daily living scales for the diagnosis of Parkinson’s disease dementia? A pilot study. Parkinsonism Relat. Disord. 19, 371–374. doi: 10.1016/j.parkreldis.2012.11.004
Ciharova, M., Cígler, H., Dostálová, V., Šivicová, G., and Bezdicek, O. (2020). Beck depression inventory, second edition, Czech version: demographic correlates, factor structure and comparison with foreign data. Int. J. Psychiatry Clin. Pract. 24, 371–379. doi: 10.1080/13651501.2020.1775854
Deuschl, G., Schade-Brittinger, C., Krack, P., Volkmann, J., Schäfer, H., Bötzel, K., et al. (2006). A randomized trial of deep-brain stimulation for Parkinson’s disease. N. Engl. J. Med. 355, 896–908. doi: 10.1056/NEJMoa060281
Emre, M., Aarsland, D., Brown, R., Burn, D. J., Duyckaerts, C., Mizuno, Y., et al. (2007). Clinical diagnostic criteria for dementia associated with Parkinson’s disease. Mov. Disord. 22, 1689–1707; quiz1837. doi: 10.1002/mds.21507
Fellows, R. P., and Schmitter-Edgecombe, M. (2019). Multimethod assessment of everyday functioning and memory abilities in Parkinson’s disease. Neuropsychology 33, 169–177. doi: 10.1037/neu0000505
Foley, J. A., Foltynie, T., Limousin, P., and Cipolotti, L. (2018). Standardised neuropsychological assessment for the selection of patients undergoing DBS for Parkinson’s Disease. Parkinsons Dis. 2018:4328371. doi: 10.1155/2018/4328371
Foster, E. R. (2014). Instrumental activities of daily living performance among people with Parkinson’s disease without dementia. Am. J. Occup. Ther. 68, 353–362. doi: 10.5014/ajot.2014.010330
Foster, E. R., and Doty, T. (2021). Cognitive correlates of instrumental activities of daily living performance in parkinson disease without dementia. Arch. Rehabil. Res. Clin. Transl. 3:100138. doi: 10.1016/j.arrct.2021.100138
Giovannetti, T., Britnell, P., Brennan, L., Siderowf, A., Grossman, M., Libon, D. J., et al. (2012). Everyday action impairment in Parkinson’s disease dementia. J. Int. Neuropsychol. Soc. 18, 787–798. doi: 10.1017/S135561771200046X
Gorecka-Mazur, A., Furgala, A., Krygowska-Wajs, A., Pietraszko, W., Kwinta, B., and Gil, K. (2019). Activities of daily living and their relationship to health-related quality of life in patients with parkinson disease after subthalamic nucleus deep brain stimulation. World Neurosurg. 125, e552–e562. doi: 10.1016/j.wneu.2019.01.132
Hariz, G.-M., and Forsgren, L. (2011). Activities of daily living and quality of life in persons with newly diagnosed Parkinson’s disease according to subtype of disease, and in comparison to healthy controls. Acta Neurol. Scand. 123, 20–27. doi: 10.1111/j.1600-0404.2010.01344.x
Hentz, J. G., Mehta, S. H., Shill, H. A., Driver-Dunckley, E., Beach, T. G., and Adler, C. H. (2015). Simplified conversion method for unified Parkinson’s disease rating scale motor examinations. Mov. Disord. 30, 1967–1970. doi: 10.1002/mds.26435
Hoogland, J., Boel, J. A., De Bie, R. M. A., Geskus, R. B., Schmand, B. A., Dalrymple-Alford, J. C., et al. (2017). Mild cognitive impairment as a risk factor for Parkinson’s disease dementia. Mov. Disord. 32, 1056–1065. doi: 10.1002/mds.27002
Hughes, A. J., Daniel, S. E., Kilford, L., and Lees, A. J. (1992). Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: a clinico-pathological study of 100 cases. J. Neurol. Neurosurg. Psychiatry 55, 181–184. doi: 10.1136/jnnp.55.3.181
Jech, R., Mueller, K., Urgošík, D., Sieger, T., Holiga, Š, Růžička, F., et al. (2012). The Subthalamic microlesion story in Parkinson’s disease: electrode insertion-related motor improvement with relative cortico-subcortical hypoactivation in fMRI. PLoS One 7:e49056. doi: 10.1371/journal.pone.0049056
Jech, R., Ruzicka, E., Urgosik, D., Serranova, T., Volfova, M., Novakova, O., et al. (2006). Deep brain stimulation of the subthalamic nucleus affects resting EEG and visual evoked potentials in Parkinson’s disease. Clin. Neurophysiol. 117, 1017–1028. doi: 10.1016/j.clinph.2006.01.009
Jiang, J.-L., Chen, S.-Y., Hsieh, T.-C., Lee, C.-W., Lin, S.-H., and Tsai, S.-T. (2015). Different effectiveness of subthalamic deep brain stimulation in Parkinson’s disease: a comparative cohort study at 1 year and 5 years. J. Formos. Med. Assoc. 114, 835–841. doi: 10.1016/j.jfma.2013.09.006
Jurica, P. J., Leitten, C. L., and Mattis, S. (2001). Dementia Rating Scale-2 (DRS-2) Professional Manual. Lutz, FL: Psychological Assessment Resources.
Kleiner-Fisman, G., Stern, M. B., and Fisman, D. N. (2010). Health-related quality of life in parkinson disease: correlation between health utilities index iii and unified parkinson’s disease rating scale (UPDRS) in U.S. male veterans. Health Qual. Life Outcomes 8:91. doi: 10.1186/1477-7525-8-91
Kubu, C. S. (2018). The role of a neuropsychologist on a movement disorders deep brain stimulation team. Arch. Clin. Neuropsychol. 33, 365–374. doi: 10.1093/arclin/acx130
Lawson, R. A., Williams-Gray, C. H., Camacho, M., Duncan, G. W., Khoo, T. K., Breen, D. P., et al. (2021). Which neuropsychological tests? Predicting cognitive decline and dementia in Parkinson’s Disease in the ICICLE-PD cohort. J. Parkinsons Dis. 11, 1297–1308. doi: 10.3233/JPD-212581
Liddell, T. M., and Kruschke, J. K. (2018). Analyzing ordinal data with metric models: what could possibly go wrong? J. Exp. Soc. Psychol. 79, 328–348.
Litvan, I., Goldman, J. G., Tröster, A. I., Schmand, B. A., Weintraub, D., Petersen, R. C., et al. (2012). Diagnostic criteria for mild cognitive impairment in Parkinson’s disease: movement disorder society task force guidelines. Mov. Disord. 27, 349–356. doi: 10.1002/mds.24893
Martin, R. C., Triebel, K. L., Kennedy, R. E., Nicholas, A. P., Watts, R. L., Stover, N. P., et al. (2013). Impaired financial abilities in Parkinson’s disease patients with mild cognitive impairment and dementia. Parkinsonism Relat. Disord. 19, 986–990. doi: 10.1016/j.parkreldis.2013.06.017
McElreath, R. (2020). Statistical Rethinking: A Bayesian Course With Examples in R and Stan. London: Chapman and Hall/CRC.
Molinuevo, J. L., Valldeoriola, F., Tolosa, E., Rumià, J., Valls-Solé, J., Roldán, H., et al. (2000). Levodopa withdrawal after bilateral subthalamic nucleus stimulation in advanced parkinson disease. Arch. Neurol. 57, 983–988. doi: 10.1001/archneur.57.7.983
Moro, E., and Lang, A. E. (2006). Criteria for deep-brain stimulation in Parkinson’s disease: review and analysis. Exp. Rev. Neurother. 6, 1695–1705. doi: 10.1586/14737175.6.11.1695
Mueller, K., Urgošík, D., Ballarini, T., Holiga, Š, Möller, H. E., Růžička, F., et al. (2020). Differential effects of deep brain stimulation and levodopa on brain activity in Parkinson’s disease. Brain Commun. 2:fcaa005. doi: 10.1093/braincomms/fcaa005
Odekerken, V. J. J., Van Laar, T., Staal, M. J., Mosch, A., Hoffmann, C. F. E., Nijssen, P. C. G., et al. (2013). Subthalamic nucleus versus Globus pallidus bilateral deep brain stimulation for advanced Parkinson’s disease (NSTAPS study): a randomised controlled trial. Lancet Neurol. 12, 37–44. doi: 10.1016/S1474-4422(12)70264-8
Okun, M. S. (2014). Deep-brain stimulation–entering the era of human neural-network modulation. N. Engl. J. Med. 371, 1369–1373. doi: 10.1056/NEJMp1408779
Pearl, J. (2009). Causality: Models, Reasoning, and Inference. Cambridge: Cambridge University Press.
Pirogovsky, E., Martinez-Hannon, M., Schiehser, D. M., Lessig, S. L., Song, D. D., Litvan, I., et al. (2013). Predictors of performance-based measures of instrumental activities of daily living in nondemented patients with Parkinson’s disease. J. Clin. Exp. Neuropsychol. 35, 926–933. doi: 10.1080/13803395.2013.838940
Pirogovsky, E., Schiehser, D. M., Obtera, K. M., Burke, M. M., Lessig, S. L., Song, D. D., et al. (2014). Instrumental activities of daily living are impaired in Parkinson’s disease patients with mild cognitive impairment. Neuropsychology 28, 229–237. doi: 10.1037/neu0000045
R Core Team (2021). R: A Language and Environment for Statistical Computing. Vienna: R Foundation for Statistical Computing.
Rosenthal, E., Brennan, L., Xie, S., Hurtig, H., Milber, J., Weintraub, D., et al. (2010). Association between cognition and function in patients with Parkinson disease with and without dementia. Mov. Disord. 25, 1170–1176. doi: 10.1002/mds.23073
Russmann, H., Ghika, J., Combrement, P., Villemure, J. G., Bogousslavsky, J., Burkhard, P. R., et al. (2004). L-Dopa-induced dyskinesia improvement after STN-DBS depends upon medication reduction. Neurology 63, 153–155. doi: 10.1212/01.wnl.0000131910.72829.9d
Schmitter-Edgecombe, M., McAlister, C., and Greeley, D. (2021). A comparison of functional abilities in individuals with mild cognitive impairment and Parkinson’s disease with mild cognitive impairment using multiple assessment methods. J. Int. Neuropsychol. Soc. 1–12. doi: 10.1017/S1355617721001077 [Epub ahead of print].
Shulman, L. M., Armstrong, M., Ellis, T., Gruber-Baldini, A., Horak, F., Nieuwboer, A., et al. (2016). Disability rating scales in parkinson’s disease: critique and recommendations. Mov. Disord. 31, 1455–1465. doi: 10.1002/mds.26649
Soh, S.-E., Mcginley, J. L., Watts, J. J., Iansek, R., Murphy, A. T., Menz, H. B., et al. (2013). Determinants of health-related quality of life in people with Parkinson’s disease: a path analysis. Qual. Life Res. 22, 1543–1553. doi: 10.1007/s11136-012-0289-1
Stan Development Team (2021). Stan Modeling Language User’s Guide and Reference Manual (Version 2.21.0). Available online at: http://mc-stan.org/
Sulzer, P., Liebig, L., Csoti, I., Graessel, E., Wurster, I., Berg, D., et al. (2020). A time-efficient screening tool for activities of daily living functions in Parkinson’s disease dementia. J. Clin. Exp. Neuropsychol. 42, 867–879. doi: 10.1080/13803395.2020.1825634
Tödt, I., Al-Fatly, B., Granert, O., Kühn, A. A., Krack, P., Rau, J., et al. (2022). The contribution of subthalamic nucleus deep brain stimulation to the improvement in motor functions and quality of life. Mov. Disord. 37, 291–301. doi: 10.1002/mds.28952
Tomlinson, C. L., Stowe, R., Patel, S., Rick, C., Gray, R., and Clarke, C. E. (2010). Systematic review of levodopa dose equivalency reporting in Parkinson’s disease. Mov. Disord. 25, 2649–2653. doi: 10.1002/mds.23429
Urgosik, D., Jech, R., Ruzicka, E., and Ruzicka, F. (2011). Deep brain stimulation in movement disorders: a prague-center experience. Cas Lek Cesk 150, 223–228.
Keywords: activities of daily living, deep brain stimulation, cognition, everyday abilities, subthalamic nucleus
Citation: Bezdicek O, Mana J, Růžička F, Havlik F, Fečíková A, Uhrová T, Růžička E, Urgošík D and Jech R (2022) The Instrumental Activities of Daily Living in Parkinson’s Disease Patients Treated by Subthalamic Deep Brain Stimulation. Front. Aging Neurosci. 14:886491. doi: 10.3389/fnagi.2022.886491
Received: 28 February 2022; Accepted: 30 May 2022;
Published: 17 June 2022.
Edited by:
Fabio Pilato, Policlinico Universitario Campus Bio-Medico, ItalyReviewed by:
Massimo Marano, Campus Bio-Medico University, ItalyCarla Piano, Agostino Gemelli University Polyclinic (IRCCS), Italy
Copyright © 2022 Bezdicek, Mana, Růžička, Havlik, Fečíková, Uhrová, Růžička, Urgošík and Jech. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ondrej Bezdicek, b25kcmVqLmJlemRpY2VrQGxmMS5jdW5pLmN6
†ORCID: Ondrej Bezdicek, orcid.org/0000-0002-5108-0181; Josef Mana, orcid.org/0000-0002-7817-3978; Filip Havlik, orcid.org/0000-0003-4442-6743; Evžen Růžička, orcid.org/0000-0002-4893-9661; Robert Jech, orcid.org/0000-0002-9732-8947
‡These authors have contributed equally to this work