
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CORRECTION article
Front. Aging Neurosci. , 08 December 2022
Sec. Neuroinflammation and Neuropathy
Volume 14 - 2022 | https://doi.org/10.3389/fnagi.2022.1101574
This article is part of the Research Topic Biomarkers of Perioperative Stroke in Older Patients View all 23 articles
 Faqiang Zhang1†
Faqiang Zhang1† Mu Niu2†
Mu Niu2† Long Wang3†Yanhong Liu1Likai Shi1Jiangbei Cao1Weidong Mi1
Long Wang3†Yanhong Liu1Likai Shi1Jiangbei Cao1Weidong Mi1 Yulong Ma1*
Yulong Ma1* Jing Liu1*
Jing Liu1*by Zhang, F., Niu, M., Wang, L., Liu, Y., Shi, L., Cao, J., Mi, W., Ma, Y., and Liu, J. (2022). Front. Aging Neurosci. 14:865244. doi: 10.3389/fnagi.2022.865244
In the original article, there was a mistake in Figure 1 as published. “ASA physical status V” should be “ASA physical status ≥ IV.” In addition the corresponding n number was give as 391, but should be 1,091. In addition, the corresponding n number for “Missing data for any confounder” was 3,144 but should be 2,444. The revised Figure 1 appears below.
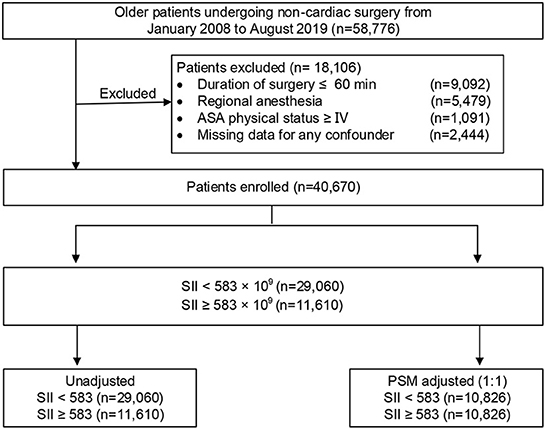
Figure 1. Study profile. ASA, American Society of Anesthesiologists; PSM, propensity score matching.
There was also an error in Materials and methods, “Inclusion and exclusion criteria,” Paragraph 1. “Patients who presented with an American Society of Anesthesiologists (ASA) classification of V” should be “Patients who presented with an American Society of Anesthesiologists (ASA) classification of ≥IV.” The corrected paragraph appears below:
“Patients who underwent non-cardiac surgery between January 2008 and August 2019 at Chinese PLA General Hospital were initially screened from a perioperative retrospective database. The inclusion criteria were as follows: (1) aged 65 yr or older; (2) underwent non-cardiac surgery; (3) received general anesthesia; and (4) were with duration of surgery > 60 min. Patients who presented with an American Society of Anesthesiologists (ASA) classification of ≥IV, were performed under regional anesthesia, or had missing clinical data were excluded. Among patients who underwent multiple surgeries during the study period, only the first eligible surgery was considered. A flow diagram of the patient selection process is displayed in Figure 1.” In the original article, there was also a mistake in the Abstract, “Conclusion” as published. The Abstract conclusion stated, “after non-cardiac surgery in elderly older patients.” This should be “after non-cardiac surgery in older patients.” The corrected paragraph appears below:
“Conclusion: Preoperative SII, which includes neutrophil, platelet, and lymphocyte counts obtained from routine blood analysis, was a potential prognostic biomarker for predicting perioperative ischemic stroke after non-cardiac surgery in older patients. An elevated SII, based on an optimal cut-off value of 583, was an independent risk factor for perioperative ischemic stroke.”
In the original article, there was also an error in Table 1 and Supplementary Tables 2–4. The covariates previously stated “Class III and IV” and “Arterial fibrillation.” The corrected covariates are “Class III” and “Atrial fibrillation or VHD.” The corrected Table 1 appears below. The corrected Supplementary Tables 2–4 appear in the Supplementary Material of the original article.
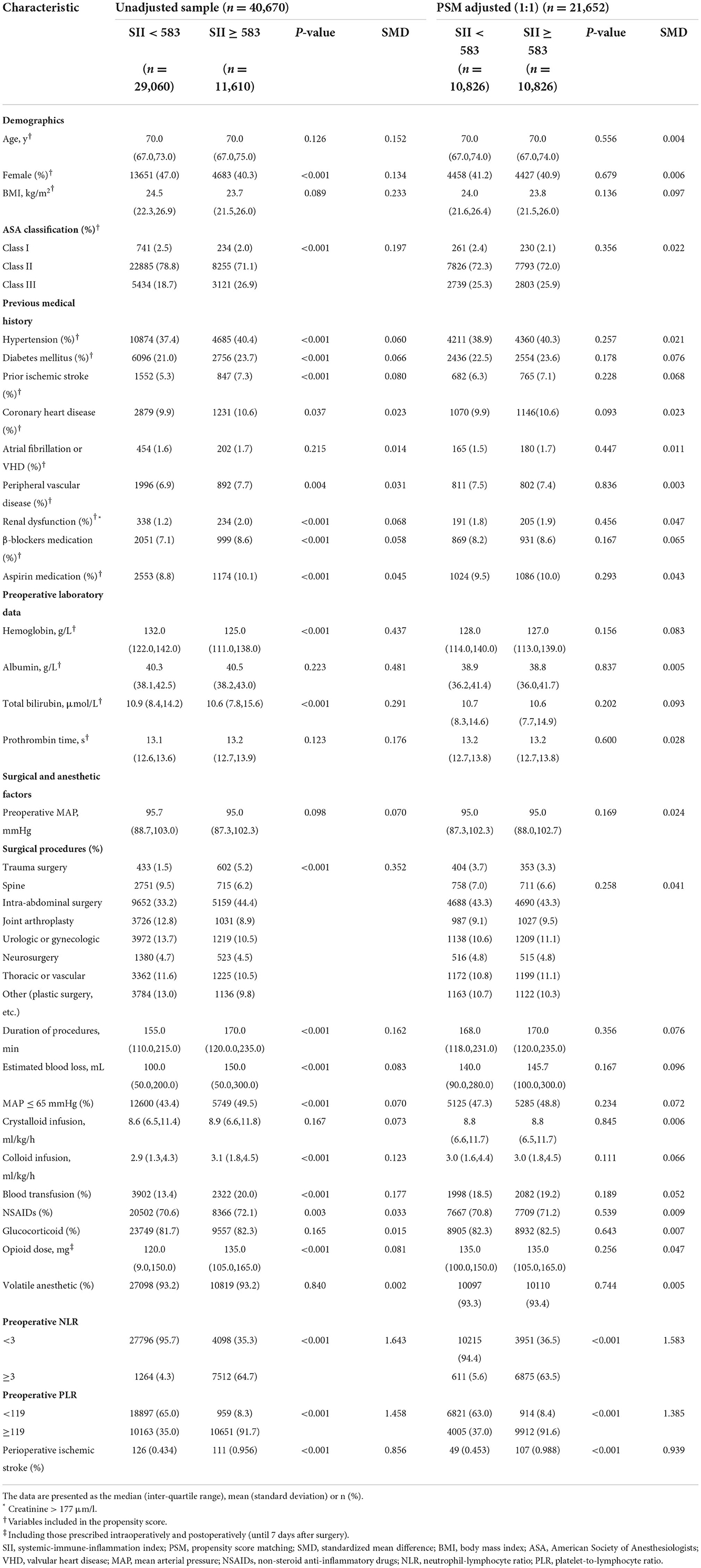
Table 1. Baseline characteristics of unadjusted sample and propensity score-matched sample (patients from 2008–2019).
In the original article there was also an error in Materials and methods, “Clinical outcome.” The definition of perioperative ischemic stroke was incomplete. The following information was not provided: “Diagnoses of stroke are confirmed by a combination of neuroimaging and clinical evidence of cerebrovascular ischemia during hospital stay.” The corrected paragraph appears below:
“The primary outcome of interest was perioperative ischemic stroke, defined as an episode of neurological dysfunction, such as motor, sensory, or cognitive dysfunction, caused by focal cerebral, spinal, or retinal infarction within 30 postoperative days (Sacco et al., 2013). Diagnoses of stroke are confirmed by a combination of neuroimaging and clinical evidence of cerebrovascular ischemia during hospital stay. In our study, perioperative ischemic stroke patients were identified if discharge records included at least 1 ICD-9-CM/ICD-10-CM diagnosis code for stroke (Supplementary Table 1).”
We apologize for these errors and state that this does not change the scientific conclusions of the article in any way. The original article has been updated.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Sacco, R. L., Kasner, S. E., Broderick, J. P., Caplan, L. R., Connors, J. J., Culebras, A., et al. (2013). An updated definition of stroke for the 21st century: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 44, 2064–2089. doi: 10.1161/STR.0b013e318296aeca
Keywords: systemic-immune-inflammation index (SII), perioperative stroke, postoperative complication, inflammation, older patients, biomarker
Citation: Zhang F, Niu M, Wang L, Liu Y, Shi L, Cao J, Mi W, Ma Y and Liu J (2022) Corrigendum: Systemic-immune-inflammation index as a promising biomarker for predicting perioperative ischemic stroke in older patients who underwent non-cardiac surgery. Front. Aging Neurosci. 14:1101574. doi: 10.3389/fnagi.2022.1101574
Received: 18 November 2022; Accepted: 28 November 2022;
Published: 08 December 2022.
Edited and reviewed by: Yujie Chen, Army Medical University, China
Copyright © 2022 Zhang, Niu, Wang, Liu, Shi, Cao, Mi, Ma and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yulong Ma, eXVsb25nbWExMjNAMTYzLmNvbQ==; Jing Liu, bGl1ajMwMUAxNjMuY29t
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.