
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Aging Neurosci. , 27 October 2022
Sec. Parkinson’s Disease and Aging-related Movement Disorders
Volume 14 - 2022 | https://doi.org/10.3389/fnagi.2022.1029824
This article is part of the Research Topic Insights in Parkinson’s Disease and Aging-related Movement Disorders: 2022 View all 12 articles
 Tanya Gurevich1,2*
Tanya Gurevich1,2* David Arkadir3
David Arkadir3 Samih Badarny4,5Sandra Benizri6Oren Cohen2,7
Samih Badarny4,5Sandra Benizri6Oren Cohen2,7 Ruth Djaldetti2,8
Ruth Djaldetti2,8 Sharon Hassin-Baer2,9
Sharon Hassin-Baer2,9 Meir Kestenbaum2,10Zeev Nitsan11
Meir Kestenbaum2,10Zeev Nitsan11 Yair Zlotnik12
Yair Zlotnik12 Gilad Yahalom13
Gilad Yahalom13Parkinson’s disease (PD) is taking a staggering toll on healthcare systems worldwide, with the bulk of the expenditures invested in the late stages of the disease. Considering the rising life expectancy and the increasing prevalence of PD across the globe, a clear understanding of the early signs and treatment options available for advanced PD (APD), will facilitate tailoring management programs and support services. This task is complicated by the lack of both global consensus in defining APD and standardized care guidelines. This perspective prepared by a panel of movement disorder specialists, proposes to extend and optimize currently accepted PD coding to better reflect the diverse disease manifestations, with emphasis on non-motor features. The panel seeks to promote timely diagnosis by adjustment of evaluation tools for use by community neurologists and suggests modification of eligibility criteria for advanced therapy. Moreover, it advocates multidisciplinary assessments of APD patients to drive personalized, patient-centered and holistic management. Overall, earlier and more targeted intervention is expected to markedly improve patient quality of life.
Parkinson’s disease (PD) currently affects 41 in 100,000 individuals between the ages of 40 and 49 and 1,607 in 100,000 individuals over the age of 80 (Pringsheim et al., 2014; Elbaz et al., 2016; Dorsey and Bloem, 2018). In Israel, the prevalence in 2007 was estimated at 256:100,000 (Chillag-Talmor et al., 2011). By 2040, PD is expected to affect approximately 14.2 million individuals worldwide (Dorsey and Bloem, 2018). Its onset is influenced by a host of genetic and environmental factors, with age serving as a central determinant, as well as the most critical risk factor of disease progression and responsiveness to treatment (Levy, 2007; Collier et al., 2011). The disease takes a marked toll on healthcare resources, incurring an estimated $51.9 billion in direct and indirect costs in 2017 in the United States alone (Yang et al., 2020). The largest proportion of expenditures is invested in patients in late stages of the disease, as unidirectional phenotype shifts result in progressive disability and severely compromised patient quality of life (Lim et al., 2009). Given the rising life expectancy across the globe, and increased PD prevalence in the world (GBD 2016 Parkinson’s Disease Collaborators, 2018), PD burden on public healthcare systems is expected to grow, and will require reconsideration of health policies and programs to adequately address the growing needs of the PD population. In this viewpoint, special attention is given to advanced PD (APD), also referred to as complex PD, estimated to impact 10% of the PD patient population (Worth, 2013; Giugni and Okun, 2014).
Historically, motor syndrome was the main recognized clinical manifestation of PD and the prevalence of severe disability and mortality within 5 and 10 years of onset was 25 and 65%, respectively (Maier Hoehn, 1992). Yet, since the introduction of levodopa, the mainstay of modern PD treatment, PD-associated motor syndrome has proven responsive to the pharmaceutical treatments and mortality rates have declined, albeit remaining higher than in age-matched controls (Chen et al., 2006). Owing to the remarkable progress in the treatment of motor manifestations, PD is now considered a relatively slowly-progressing, chronic disease with distinctly different manifestations at its various stages, with the APD stage being the most challenging for patients and healthcare providers.
This stage is characterized by moderate to severe motor deficits (Hoehn & Yahr stage III-V during off periods), generally accompanied by troublesome motor and non-motor symptoms: fluctuations, dyskinesias, frequent off-periods, postural instability leading to frequent falls with increased risk of fractures, sleep disturbances, hallucinations, and cognitive decline, among others. However, with close support, patients are not entirely dependent at this stage and are still capable of independent activity, and may be effectively managed by timely adjustment of the treatment. As PD patients progress to the advanced stage, they typically require intensive and individualized multidisciplinary pharmacological and non-pharmacological care to manage disease and treatment-related complications (Figure 1). Furthermore, as PD symptoms become less controlled with conventional therapies, targeted treatment options, including device-assisted therapies (DAT), such as deep brain stimulation or continuous levodopa-carbidopa infusions via pumps, are needed to improve response fluctuations.
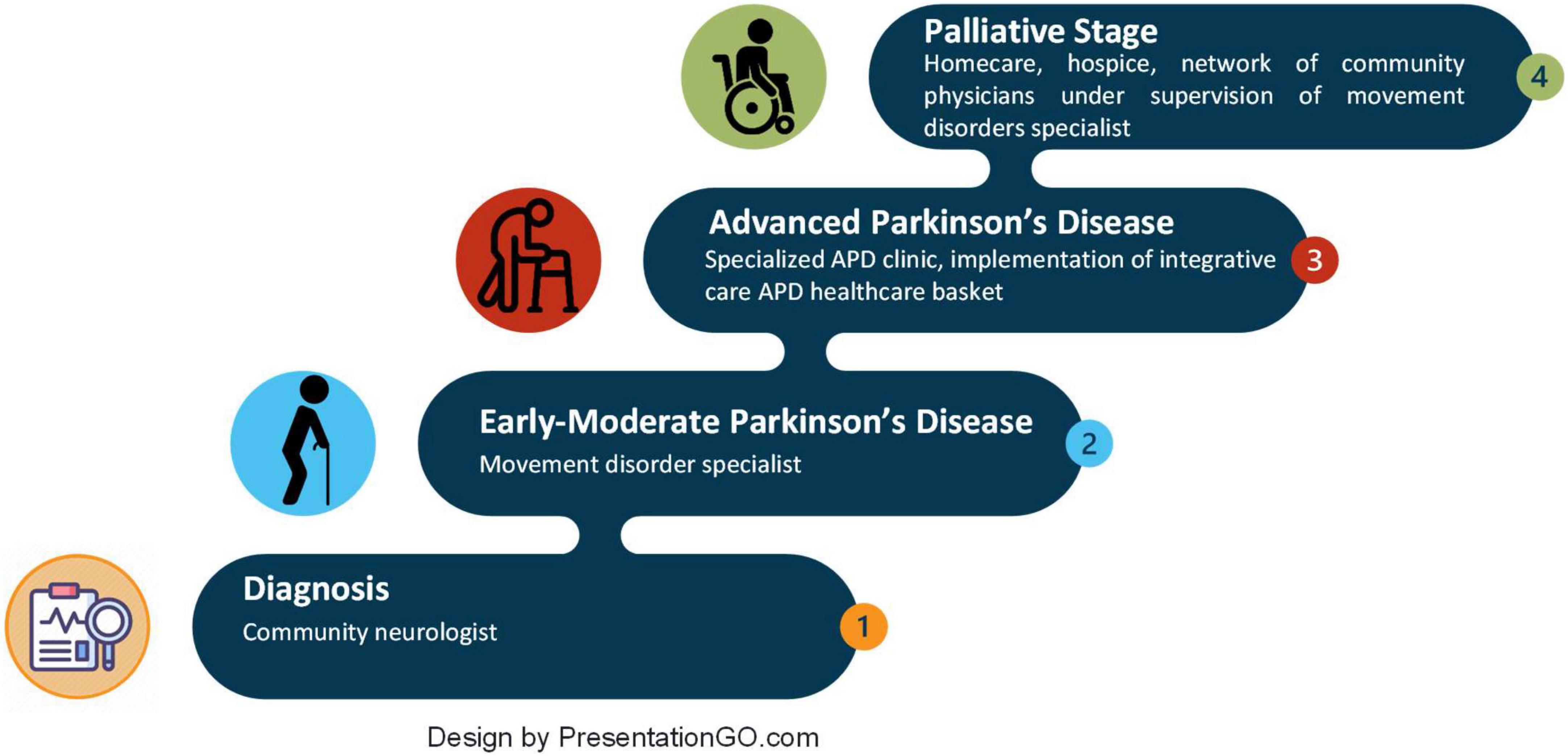
Figure 1. Parkinson’s disease stages and stage-appropriate healthcare facilities.
Despite the wealth of knowledge of PD pathology and its natural course, there is a lack of global consensus regarding the precise definition of APD. This is largely due to its heterogenic origins, the vast variety of subphenotypes, variable trajectories and prognostics, as well as the absence of robust biomarkers for disease progression. In turn, it has challenged development of standardized care guidelines, and has brought to a lag in appropriate alignment of diagnostic instruments and grading scales for classification of disease severity and evaluation of treatment and management strategies. Furthermore, it has stymied early APD identification, and tailoring of interventional programs and appropriate allocation of funds. The most popular assessment tools use PD duration as an anchor and primarily focus on cardinal overt motor features. They have been proven to lack universality due to different phenotypes and rates of disease progression and generally fail to recognize the true weight of non-motor features on patient performance and quality of life (Braak et al., 2003; Wolters, 2008). Recent initiatives to develop comprehensive toolkits for evaluating PD status have been steered by the increasing understanding that motor disability, non-motor manifestations, treatment-related complications, and comorbidities are central contributors to APD and its associated limited activities of daily living (ADL), disability and greatly impaired quality of life (Korczyn, 1999; Martinez-Martin et al., 2011; Ray Chaudhuri et al., 2013). All these aspects are well-represented in the recently defined Delphi criteria for APD, which integrate degree of control achieved with oral anti-PD medications, assessment of an array of motor and non-motor symptoms, as well as patient functioning and independence (Antonini et al., 2018). The cross-sectional, multinational, observational OBSERVE-PD review of 2,615 PD patient charts (Fasano et al., 2019) found most significant agreement between physician global assessment and APD diagnosis based on the Delphi criteria, with regards to current treatment programs, limited ADL, motor fluctuations and time from diagnosis. In a subanalysis of the Israeli cohort of 120 patients, physician judgment in classifying APD correlated with select Delphi criteria (Djaldetti et al., 2018). Recently, the intensified therapy component of the “5-2-1” criteria proposed by the Delphi expert consensus panel for identifying APD, has been shown to correlate with established disease burden predictors, including extended disease duration, increased motor and non-motor burden, and compromised quality of life (Fasano et al., 2019; Aldred et al., 2020; Santos-Garcia et al., 2020; Barer et al., 2022) and is included in the recently published MANAGE-PD comprehensive screening tool (Antonini et al., 2019). Integration of wearable sensors into clinical practice are projected to provide objective, quantitative digital patient function-related markers, and thereby improve the sensitivity, accuracy and feasibility of the assessment of motor and non-motor symptoms of PD and diagnosis of APD (Mirelman et al., 2021).
In line with the global efforts to moderate PD impact on quality of life, the authors, representing a panel of Israeli movement disorders specialists, propose to define APD in the International Classification of Disease 11th revision (ICD-11) as a unique health entity that demands adjusted healthcare provider attitudes and relevant social services. Modification of the ICD-11 PD coding should include severity- and fluctuation-based subcodes that accurately capture APD and distinguish it from early-stage PD. While very few diseases have been assigned severity-based subcodes in ICD-10 (diabetes, alcoholic liver disease, renal insufficiency, residual schizophrenia), the growing evidence of the distinct clinical manifestations and medical needs of this patient subpopulation, justifies reconsideration of its coding status.
In addition, we call for optimization of the Delphi criteria by extending them to include a more extensive list of non-motor features, such as autonomic disturbances (e.g., orthostatic hypotension, urinary incontinence), pain, daytime somnolence, and apathy. Furthermore, in the opinion of the Israeli panel, the Delphi criteria for APD from motor fluctuations, regardless of their duration and severity, should be the main eligibility criteria for advanced therapy. Evaluation of PD patients should be based on a structured questionnaire applied as a preliminary tool geared to be implemented by community neurologists or case managers (e.g., nurse practitioners). Patients with suspected APD should undergo multidisciplinary evaluation, ideally in specialized APD centers, to define the extent of disability, outline an individualized treatment program, and weigh the need for rehabilitation and social support services. Routine evaluations should be adequately sensitive to allow for timely diagnosis of palliative-stage PD, which should be addressed by end-of-life palliative/hospice referral (Akbar et al., 2021).
Management protocols should implement personalized patient-centered and holistic approaches to target the heterogenic manifestations and course of PD. These should include tools for timely diagnosis and treatment of osteoporosis. Furthermore, patients should be informed of opportunities to participate in relevant clinical trials. In addition to the clinical benefits of integrated and coordinated care (Nijkrake et al., 2009; van der Eijk et al., 2011; Loewenbrück et al., 2020; Tenison et al., 2020), such programs have been associated with improved psychological health indicators and self-management capacities (Coulter et al., 2015; Minkman, 2016). Rehabilitation facilities should be staffed by multidisciplinary teams of physiotherapists, speech and swallowing therapists, occupation therapists and social workers. Such programs should be coordinated by specialized nurses (or nurse practitioners) under the supervision of a movement disorders specialist (Cohen et al., 2021).
The panel also suggests standardization of DAT eligibility and prioritization of its use to early-stage APD patients, while minimizing its use in palliative-stage patients. Furthermore, integration of telemedicine and nurse practitioners can tighten surveillance and improve treatment optimization efforts.
These can be further supported by establishment of a network of community physicians, led by movement disorder specialists, to promote case-sharing, research dissemination and exchange of professional know-how.
Expanded APD-geared health baskets clearly outline eligibility for reimbursement for a part/full time paid attendant, mobility allowance, and rehabilitation services. In parallel, attention should be paid to informal and non-specialized caregivers by providing them PD-specific education and support (Rosqvist et al., 2021). Patients and caregivers should be made aware of PD-oriented organizations and social networking groups.
In summary, the globally rising life expectancy has increased the prevalence of PD in general, and of APD, in particular. Appreciation of the heterogeneity of PD etiology and manifestations has underscored the need for updated PD coding. Precise and standardized definition and evaluation of APD will promote earlier APD identification and timely referral to adequate therapies and specialists. Moreover, it will enhance holistic management, which is expected to markedly improve APD patient quality of life. Future works should focus on validating the proposed extension of the Delphi APD criteria, and on tailoring treatment to APD phenotypes.
TG: draft preparation and literature search. All authors conceptualized, critically revised, and approved the submitted version.
Medical writing assistance and APD advisory board were funded by AbbVie. Medical writing assistance was provided by Ebiodata, Israel.
Author TG was member of the advisory board on Advanced Parkinson’s disease 23.07.2020 supported by Abbvie, consultant and/or scientific advisor/lecturer for Neuroderm, AbbVie, Cytora, Allergan, Teva, and Medison, and received research support from Parkinson’s Foundation and Israel Innovation Authority. Author SH-B had received funding for research from Abbvie and speaker honoraria from Abbvie, Medison, and Allergan, consultancy fees from Neuroderm, Abbvie, and Takeda and Teva, and advisory fees from Teva and Abbvie. Author MK was consultant and lecturer for Teva, Medison, and Abbvie. Author ZN participated in advisory boards, received speaker fees from Abbvie and Teva, and had received educational travel bursaries from Abbvie and Teva. Author YZ participated in advisory boards, received speaker fees from Abbvie, Medison, and Teva, and had received educational travel bursaries from Abbvie and Teva. Author GY was consultant for Abbvie and Takeda.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Akbar, U., McQueen, R. B., Bemski, J., Carter, J., Goy, E. R., Kutner, J., et al. (2021). Prognostic predictors relevant to end-of-life palliative care in Parkinson’s disease and related disorders: a systematic review. J. Neurol. Neurosurg. Psychiatry 92, 629–636. doi: 10.1136/jnnp-2020-323939
Aldred, J., Anca-Herschkovitsch, M., Antonini, A., Bajenaru, O., Bergmann, L., Bourgeois, P., et al. (2020). Application of the ‘5-2-1’ screening criteria in advanced Parkinson’s disease: interim analysis of duoglobe. Neurodegener. Dis. Manag. 10, 309–323. doi: 10.2217/nmt-2020-0021
Antonini, A., Odin, P., Jalundhwala, Y. J., Schmidt, P. N., Skalicky, A. M., Kleinman, L., et al. (2019). Manage-pd: a clinician-reported tool to identify patients with Parkinson’s disease inadequately controlled on oral medications – results from vignette-based validation. Neurology 92(15 Suppl.), 239–240. doi: 10.1016/j.jns.2019.10.1252
Antonini, A., Stoessl, A. J., Kleinman, L. S., Skalicky, A. M., Marshall, T. S., Sail, K. R., et al. (2018). Developing consensus among movement disorder specialists on clinical indicators for identification and management of advanced Parkinson’s disease: a multi-country delphi-panel approach. Curr. Med. Res. Opin. 34, 2063–2073. doi: 10.1080/03007995.2018.1502165
Barer, Y., Gurevich, T., Chodick, G., Giladi, N., Gross, R., COhen, R., et al. (2022). Advanced-stage Parkinson’s disease: from identification to characterization using a nationwide database. Mov. Disord. Clin. Pract. 9, 458–467. doi: 10.1002/mdc3.13458
Braak, H., Del Tredici, K., Rub, U., de Vos, R. A., Jansen Steur, E. N., and Braak, E. (2003). Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol. Aging 24, 197–211. doi: 10.1016/S0197-4580(02)00065-9
Chen, H., Zhang, S. M., Schwarzschild, M. A., Hernán, M. A., and Ascherio, A. (2006). Survival of Parkinson’s disease patients in a large prospective cohort of male health professionals. Mov. Disord. 21, 1002–1007. doi: 10.1002/mds.20881
Chillag-Talmor, O., Giladi, N., Linn, S., Gurevich, T., El-Ad, B., Silverman, B., et al. (2011). Use of a refined drug tracer algorithm to estimate prevalence and incidence of Parkinson’s disease in a large israeli population. J. Parkinsons Dis. 1, 35–47. doi: 10.3233/JPD-2011-11024
Cohen, N., Manor, Y., Green, Y., Tahel, G., Badichi, I., Ben-Or, G., et al. (2021). Multidisciplinary intensive outpatient rehabilitation program for patients with moderate-to-advanced Parkinson’s disease. NeuroRehabilitation 49, 47–55. doi: 10.3233/NRE-210031
Collier, T. J., Kanaan, N. M., and Kordower, J. H. (2011). Ageing as a primary risk factor for Parkinson’s disease: evidence from studies of non-human primates. Nat. Rev. Neurosci. 12, 359–366. doi: 10.1038/nrn3039
Coulter, A., Entwistle, V. A., Eccles, A., Ryan, S., Shepperd, S., and Perera, R. (2015). Personalised care planning for adults with chronic or long-term health conditions. Cochrane Database Syst. Rev. 2015:CD010523. doi: 10.1002/14651858.CD010523.pub2
Djaldetti, R., Hassin-Baer, S., Anca-Herschkovitsch, M., Gross, R., Cohen, R., Banayan, H., et al. (2018). Advanced Parkinson’s disease diagnosis and treatment trends in israel-sub-analysis of the observe-pd multi-country, cross-sectional study. Mov. Disord. 33, 14–17.
Dorsey, E. R., and Bloem, B. R. (2018). The parkinson pandemic-a call to action. JAMA Neurol. 75, 9–10. doi: 10.1001/jamaneurol.2017.3299
Elbaz, A., Carcaillon, L., Kab, S., and Moisan, F. (2016). Epidemiology of Parkinson’s disease. Rev. Neurol. 172, 14–26. doi: 10.1016/j.neurol.2015.09.012
Fasano, A., Fung, V. S. C., Lopiano, L., Elibol, B., Smolentseva, I. G., Seppi, K., et al. (2019). Characterizing advanced Parkinson’s disease: observe-pd observational study results of 2615 patients. BMC Neurol. 19:50. doi: 10.1186/s12883-019-1276-8
GBD 2016 Parkinson’s Disease Collaborators (2018). Global, regional, and national burden of Parkinson’s disease, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. 17, 939–953.
Giugni, J. C., and Okun, M. S. (2014). Treatment of advanced Parkinson’s disease. Curr. Opin. Neurol. 27, 450–460. doi: 10.1097/WCO.0000000000000118
Korczyn, A. D. (1999). Parkinson’s disease: one disease entity or many? J. Neural Transm. Suppl. 56, 107–111. doi: 10.1007/978-3-7091-6360-3_5
Levy, G. (2007). The relationship of parkinson disease with aging. Arch. Neurol. 64, 1242–1246. doi: 10.1001/archneur.64.9.1242
Lim, S.-Y., Fox, S. H., and Lang, A. E. (2009). Overview of the extranigral aspects of parkinson disease. Arch. Neurol. 66, 167–172. doi: 10.1001/archneurol.2008.561
Loewenbrück, K. F., Stein, D. B., Amelung, V. E., Bitterlich, R., Brumme, M., Falkenburger, B., et al. (2020). Parkinson network eastern saxony (panos): reaching consensus for a regional intersectoral integrated care concept for patients with Parkinson’s disease in the region of eastern saxony, germany. J. Clin. Med. 9:2906. doi: 10.3390/jcm9092906
Maier Hoehn, M. M. (1992). The natural history of Parkinson’s disease in the pre-levodopa and post-levodopa eras. Neurol. Clin. 10, 331–339. doi: 10.1016/S0733-8619(18)30213-5
Martinez-Martin, P., Rodriguez-Blazquez, C., Kurtis, M. M., and Chaudhuri, K. R. (2011). The impact of non-motor symptoms on health-related quality of life of patients with Parkinson’s disease. Mov. Disord. 26, 399–406. doi: 10.1002/mds.23462
Minkman, M. (2016). The development model for integrated care: a validated tool for evaluation and development. J. Integr. Care 24, 38–52. doi: 10.1108/JICA-01-2016-0005
Mirelman, A., Ben Or Frank, M., Melamed, M., Granovsky, L., Nieuwboer, A., Rochester, L., et al. (2021). Detecting sensitive mobility features for Parkinson’s disease stages via machine learning. Mov. Disord. 36, 2144–2155. doi: 10.1002/mds.28631
Nijkrake, M. J., Keus, S. H., Oostendorp, R. A., Overeem, S., Mulleners, W., Bloem, B. R., et al. (2009). Allied health care in Parkinson’s disease: referral, consultation, and professional expertise. Mov. Disord. 24, 282–286. doi: 10.1002/mds.22377
Pringsheim, T., Jette, N., Frolkis, A., and Steeves, T. D. (2014). The prevalence of Parkinson’s disease: a systematic review and meta-analysis. Mov. Disord. 29, 1583–1590. doi: 10.1002/mds.25945
Ray Chaudhuri, K., Rojo, J. M., Schapira, A. H., Brooks, D. J., Stocchi, F., Odin, P., et al. (2013). A proposal for a comprehensive grading of Parkinson’s disease severity combining motor and non-motor assessments: meeting an unmet need. PLoS One 8:e57221. doi: 10.1371/journal.pone.0057221
Rosqvist, K., Kylberg, M., Lofqvist, C., Schrag, A., Odin, P., and Iwarsson, S. (2021). Perspectives on care for late-stage Parkinson’s disease. Parkinsons Dis. 2021:9475026. doi: 10.1155/2021/9475026
Santos-Garcia, D., de Deus Fonticoba, T., Suarez Castro, E., Aneiros Diaz, A., and McAfee, D. (2020). 5-2-1 criteria: a simple screening tool for identifying advanced pd patients who need an optimization of Parkinson’s treatment. Parkinsons Dis. 2020:7537924. doi: 10.1155/2020/7537924
Tenison, E., Smink, A., Redwood, S., Darweesh, S., Cottle, H., van Halteren, A., et al. (2020). Proactive and integrated management and empowerment in Parkinson’s disease: designing a new model of care. Parkinson Dis. 2020:8673087. doi: 10.1155/2020/8673087
van der Eijk, M., Faber, M. J., Al Shamma, S., Munneke, M., and Bloem, B. R. (2011). Moving towards patient-centered healthcare for patients with Parkinson’s disease. Parkinson. Relat. Disord. 17, 360–364. doi: 10.1016/j.parkreldis.2011.02.012
Wolters, E. C. (2008). Variability in the clinical expression of Parkinson’s disease. J. Neurol. Sci. 266, 197–203. doi: 10.1016/j.jns.2007.08.016
Worth, P. F. (2013). When the going gets tough: how to select patients with Parkinson’s disease for advanced therapies. Pract. Neurol. 13:140. doi: 10.1136/practneurol-2012-000463
Keywords: Parkinson’s disease stage-appropriate healthcare facilities, Delphi criteria, burden on public health care systems, clinical challenges, tailored management programs, patient-centered holistic management, intensified device aided therapies, advanced Parkinson’s disease
Citation: Gurevich T, Arkadir D, Badarny S, Benizri S, Cohen O, Djaldetti R, Hassin-Baer S, Kestenbaum M, Nitsan Z, Zlotnik Y and Yahalom G (2022) Management of advanced Parkinson’s disease in Israel: Clinicians viewpoint and action items. Front. Aging Neurosci. 14:1029824. doi: 10.3389/fnagi.2022.1029824
Received: 27 August 2022; Accepted: 12 September 2022;
Published: 27 October 2022.
Edited by:
Muthuraman Muthuraman, Johannes Gutenberg University Mainz, GermanyReviewed by:
Svetlana Tomic, Osijek Clinical Hospital Center, CroatiaCopyright © 2022 Gurevich, Arkadir, Badarny, Benizri, Cohen, Djaldetti, Hassin-Baer, Kestenbaum, Nitsan, Zlotnik and Yahalom. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tanya Gurevich, dGFueWFnQHRsdm1jLmdvdi5pbA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.