 Danielle S. Powell
Danielle S. Powell Esther S. Oh2,3
Esther S. Oh2,3 Nicholas S. Reed
Nicholas S. Reed Frank R. Lin
Frank R. Lin Jennifer A. Deal
Jennifer A. Deal
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Aging Neurosci. , 28 February 2022
Sec. Neurocognitive Aging and Behavior
Volume 13 - 2021 | https://doi.org/10.3389/fnagi.2021.769405
This article is part of the Research Topic Impact of Hearing Loss on Aging Processes: Current Understanding, Mechanisms, and Treatment Strategies View all 23 articles
Although a causal association remains to be determined, epidemiologic evidence suggests an association between hearing loss and increased risk of dementia. If we determine the association is causal, opportunity for targeted intervention for hearing loss may play a fundamental role in dementia prevention. In this discussion, we summarize current research on the association between hearing loss and dementia and review potential casual mechanisms behind the association (e.g., sensory-deprivation hypothesis, information-degradation hypothesis, common cause). We emphasize key areas of research which might best inform our investigation of this potential casual association. These selected research priorities include examination of the causal mechanism, measurement of co-existing hearing loss and cognitive impairment and determination of any bias in testing, potential for managing hearing loss for prevention of dementia and cognitive decline, or the potential to reduce dementia-related symptoms through the management of hearing loss. Addressing these research gaps and how results are then translated for clinical use may prove paramount for dementia prevention, management, and overall health of older adults.
Hearing loss is the leading potentially modifiable risk factor for dementia; up to 8% of global dementia cases are estimated as being attributable to hearing loss (Livingston et al., 2017, 2020). Following foundational initial research from over 5 decades ago, recent years have seen a steep rise in scientific investigation of the hearing-dementia association. As far back as 1968, participants demonstrated poorer performance on word-recall cognitive tasks in an experimental condition designed to mimic hearing loss and decreased speech intelligibility compared to normal listening conditions (Rabbitt, 1968). Two decades later, a seminal case-control study (Uhlmann et al., 1989) reported greater odds of dementia in those with hearing loss compared to normal hearing.
Even with our expanding knowledge of the association between hearing loss and dementia, significant gaps in our understanding persist. In this article, we aim to (1) provide a foundational understanding of hearing loss presentation and diagnosis; (2) review current hearing loss epidemiology (3) provide context to the existing research on the relationship between hearing loss and dementia to guide dementia prevention and intervention recommendations or research; (4) discuss the leading theories on the pathways behind the hearing-dementia association; and (5) present four crucial areas for future research. With the demographic changes in the coming decades, we conclude with calls for inter-disciplinary collaboration and posit a unique opportunity to alter the landscape of cognitive aging and dementia care. Understanding the role and presentation of hearing loss in the adult population allows for better appreciation of where the field of auditory science may fit into a broader picture of dementia prevention and interventions.
The act of hearing involves two inter-related processes and components of the auditory system – the peripheral auditory system and the central auditory system (Musiek and Baran, 2018) and additional non-auditory influences such as cognitive processing, education, situational influences, and self-perception, among others (Figure 1). Yet, both parts of the auditory system must work in tandem for an individual to appropriately detect and understand a sound. This process is essential for auditory interaction with the environment and is instrumental for quality communication. Yet most commonly, it is the peripheral auditory system that is considered in discussion of hearing loss. The few epidemiologic studies that include a formalized measure of hearing primarily consider peripheral hearing ability alone. Moreover, many epidemiologic studies rely on the self-reported measures of hearing. While measures of self-report hearing have their utility, self-report hearing is complex and represents perceived functional ability of hearing, incorporating aspects of the peripheral and central auditory system as well as the social environment, psychosocial aspects, and listening demands.
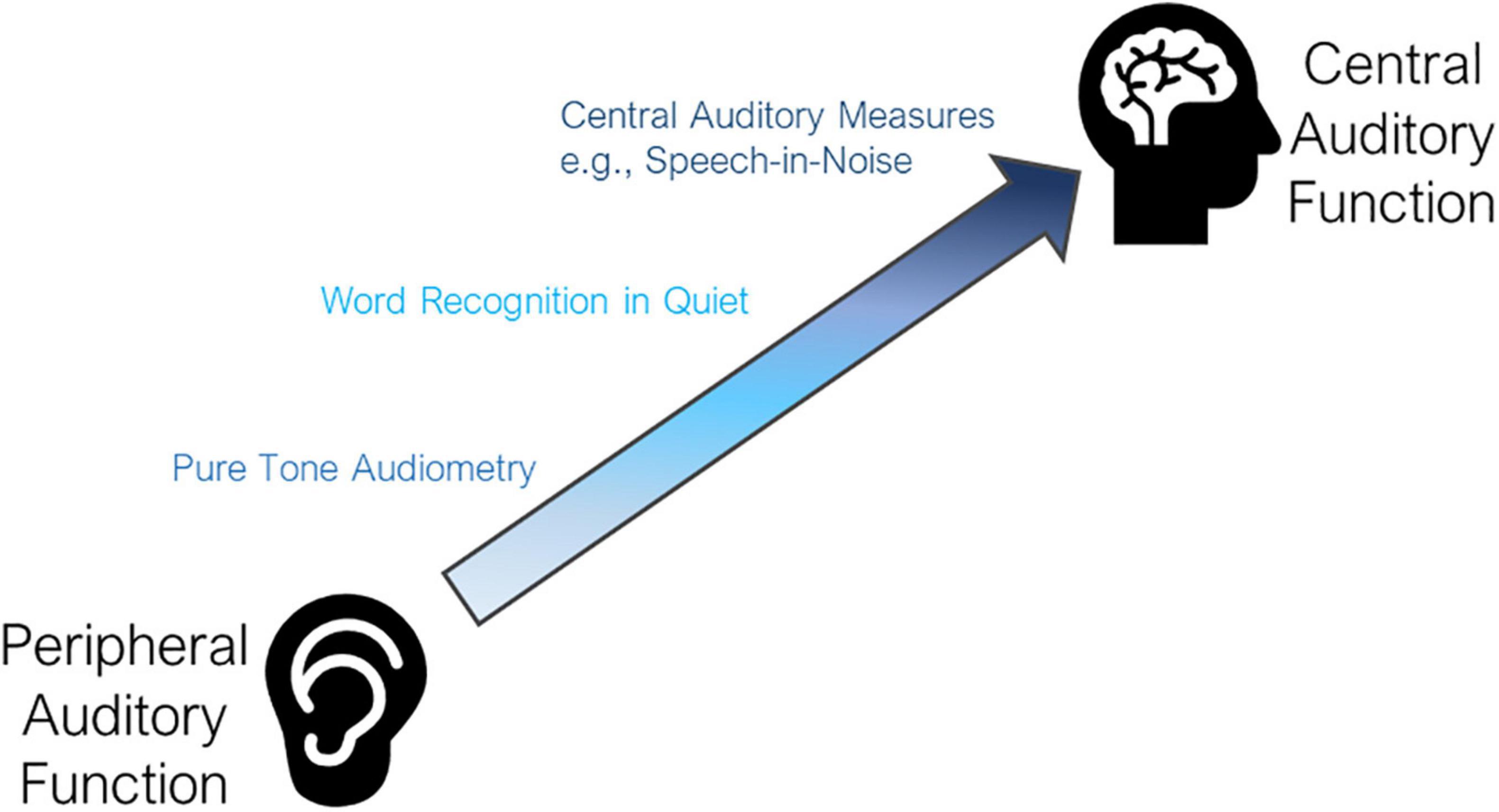
Figure 1. Levels of auditory function. The auditory system spans between peripheral and central auditory function, gaining complexity and higher cognitive processing as you activate more central auditory function. Pure tone audiometry is the most common metric for measurement of peripheral function. Word recognition (i.e., repeating back a single word heard without the use of visual cues) requires additional input of central auditory function. Central auditory measures such as speech-in-noise testing are the most complex and objective measures of central auditory function commonly performed.
The peripheral auditory system includes the outer ear (pinna), ear drum (tympanic membrane), middle ear bones (malleus, incus, and stapes), and cochlea (Musiek and Baran, 2018). These components work together to transform auditory sound waves or acoustic energy of the surrounding environment captured by the outer ear and ear drum into mechanical energy in the middle ear space, and, eventually, encoding information as an electrical signal in the cochlea to be sent along the central auditory system to the brain (Musiek and Baran, 2018). While a discussion of the complete anatomy and physiology of the peripheral auditory system is beyond the focus of this article, an individual’s ability to detect the presence of auditory stimuli initiates within and is dependent upon the peripheral system.
The most common clinical tool for measurement of peripheral hearing acuity in adults is pure tone audiometry (Katz, 2015), with results graphically recorded on an audiogram (Figure 2). This gold standard for testing is performed in a sound-proof booth using calibrated headphones. An auditory stimulus (i.e., pure tone) is presented at particular frequencies [measured in Hertz (Hz)] commonly within the range of 250–8000 Hz. The presentation level of each pure tone begins at an audible listening level for each individual and is decreased to ascertain the lowest threshold level [i.e., the volume in decibels hearing level (dB HL)], at which the individual indicates detection of the tone. In the epidemiologic literature, results are often summarized using the World Health Organization criteria as a four-frequency pure tone average (PTA), or the average of responses at 500, 1000, 2000, and 4000 Hz (Katz, 2015). Hearing loss may also be discussed within common clinical categories (i.e., normal [PTA < 20 dB], mild [20 to <35 dB], moderate [35 to <50 dB], moderately severe [50 to <65 dB], severe [65 to < 80 dB], or profound [80 dB or greater]) (World Report on Hearing, 2021) or other categorizations (Clark, 1981) which are not currently adhered to in clinical audiology.
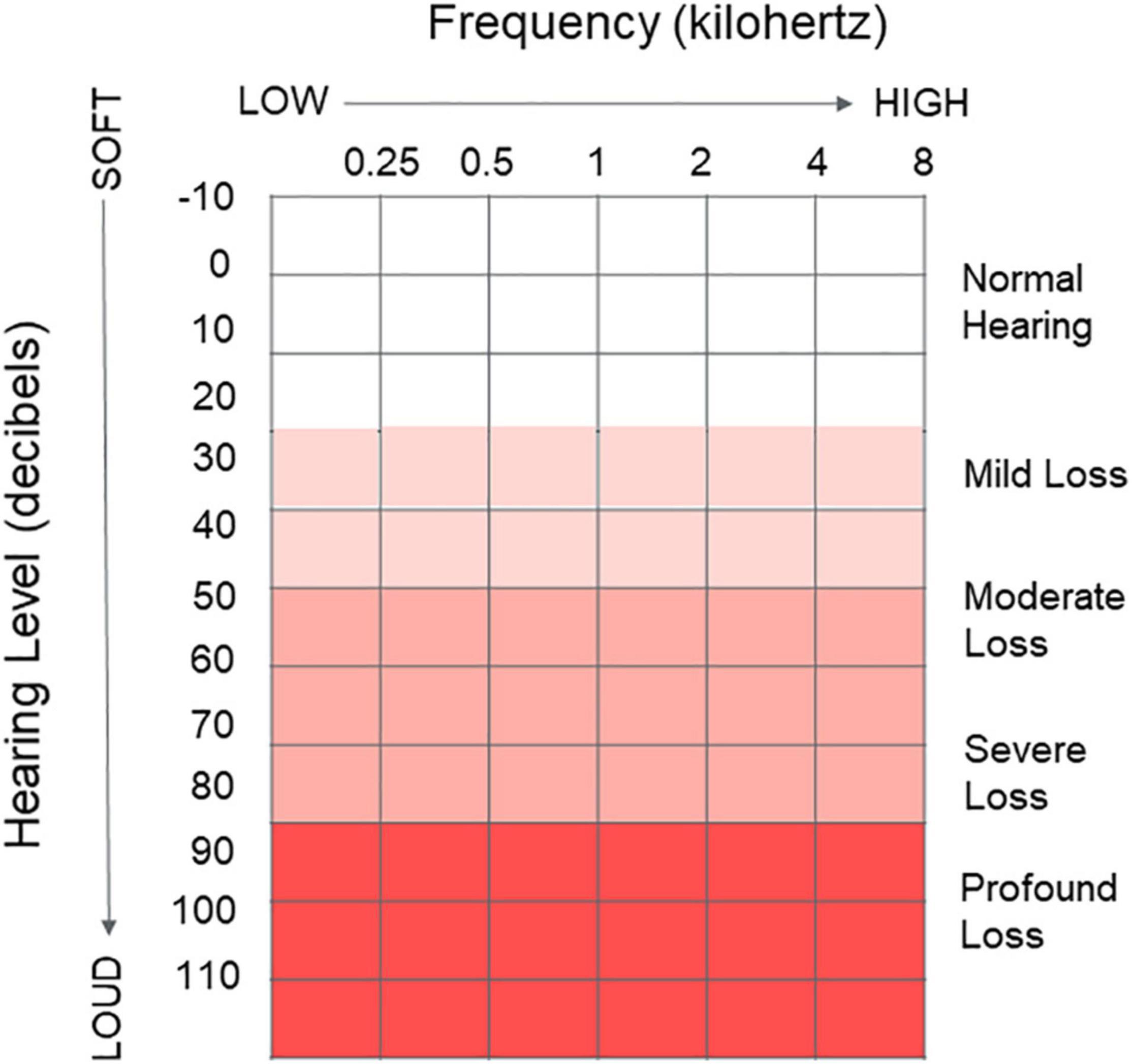
Figure 2. Audiogram. Graphical clinical tool used to depict peripheral hearing ability and record peripheral hearing thresholds as measured via pure tone audiometry. X axis represents the frequency (kHz) of sound going from low frequency to high frequency 0.25–8 kHz. Y axis represents the volume of the presented pure tone, going from very soft to very loud (–10 to 110 dB). Common clinical categories to describe hearing loss are indicated ranging from normal hearing to a profound hearing loss. The lowest volume at each frequency an individual indicates they can hear the tone is recorded for each ear on the graph.
Following passage through the peripheral auditory system, the electrical signal created by the cochlea is sent to the auditory nerve where it is then decoded by the brain (Musiek and Baran, 2018; Figure 2). Central hearing ability is therefore dependent upon the integrity of the auditory signal passed from the peripheral auditory system as well as additional cognitive processing (Gates, 2012; Humes et al., 2012). While peripheral hearing ability may be simplified as the ability to detect sound, central hearing ability then is the ability for the brain to understand and make sense of environmental sounds, requiring significant higher-level processing (i.e., identifying signals of interest from ambient noise, giving spatial awareness, adding together several pure tone signals to create complex signals such as speech, etc.).
Measurement of central auditory function is often completed through the presentation of speech within the presence of increasing volume of selected types of background noise (i.e., speech-in-noise testing) or specialized tests of central auditory processing ability that involve specific tasks like listening to degraded or temporally modified speech (Gates, 2012). However, this testing is far less frequently completed in either adult clinical visits or large-scale epidemiologic studies as compared to smaller research studies. Measurement tools for central auditory function transcends the auditory pathway with varied emphasis on how much peripheral auditory function has on performance. Measures might include the presentation of carefully selected single words via tests of word recognition, or presentation of sentences which additionally might provide context clues for word identification either in quiet or increasing levels of background noise. While central hearing ability encompasses more than speech-in-noise ability as noted, current clinical audiologic testing primarily considers basic speech-in-noise ability and not necessarily higher-level auditory cognitive processing tasks [i.e., the differentiation of sound sources within a complex environment (Bregman, 1993)]. However, tests of auditory cognitive ability designed to account for general cognitive ability or specific cognitive domains, in addition to peripheral hearing ability, have been developed (Goll et al., 2010, 2011, 2012; Grube et al., 2016) yet are in limited clinical use. It is conceivable these targeted auditory cognitive tests, with further study and if adopted more widely, may aid in understanding of the connection between neurobiological and specific central auditory ability and dementia subtypes and 1 day be included within clinical neurological work-ups as an additional indicator or early-stage dementia. However, until differentiation is feasible, the interdependence between central auditory function and cognitive processing blurs the distinction between the two processing abilities. In addition, heterogeneity in prior study has created significant barriers to pooled evidence and causal inference regarding the role of central hearing ability within cognitive impairment and testing. While more detailed description is beyond the scope of this article, a functional understanding of both aspects of the hearing system is important when considering dementia prevention strategies.
Age-related hearing loss (ARHL), also known as presbycusis, accounts for the largest percentage of hearing loss cases around the world and presents as a gradual decrease in hearing ability. The outer hair cells and other sensory cells in the cochlea are progressively damaged and unable to regenerate (Pickles, 2013). The result is the impaired encoding of sound, decreased precision, and a distorted auditory signal sent to the brain. This form of hearing loss commonly leads to decreased detection of the higher frequency sounds of speech before lower frequency sounds. The result is reduced ability to hear high-frequency consonants (i.e., /s/, /f/, th/), the parts of speech that provide crispness and clarity. In turn, many with ARHL do not necessarily report difficulty with volume of speech but instead indicate speech sounds muddled or garbled, especially when in the presence of background noise. For everyday function, this may lead to difficulty communicating or interacting with others depending on the listening environment. Those with ARHL may have difficulty hearing or understanding what others are saying in a crowded or noisy setting, such as a restaurant. They may also have difficulty hearing and understanding the television, on the phone, when someone speaks from another room or with their back turned.
The impact of a given pattern of hearing function as represented on the audiogram on communicative performance may vary widely from individual to individual (George et al., 2007; Chang et al., 2009). An individual’s functional performance with their hearing depends on not only their peripheral hearing (audiogram) but also their central hearing ability (i.e., central auditory processing, speech-in-noise performance), personal motivation, self-efficacy, listening environments and demands. The availability of cognitive resources to help support interpretation of a degraded auditory signal may also have a significant role in individual experience.
Hearing loss currently impacts an estimated 20% of the global population, or more than 1.5 billion people (World Report on Hearing, 2021). By 2050, estimates now project nearly 2.5 billion people with hearing loss, such that nearly 1 in 4 individuals will have some degree of loss (World Report on Hearing, 2021). The breakdown in hearing loss prevalence by age category varies by country, with Western countries demonstrating greater prevalence at older ages. In the United States, over two-thirds of adults age 70 years and older have a bilateral hearing loss (i.e., hearing loss in both ears) (Lin et al., 2011; Goman and Lin, 2016; Figure 3). It was estimated over 44 million older adults would have hearing loss in 2020 with expected increase to over 73 million by 2060 (Goman et al., 2017). However, analysis in a nationally representative sample of older adults suggests that while the overall prevalence of hearing loss is increasing due to greater numbers of older adults, the age-specific prevalence of hearing loss in the United States appears to be decreasing over the last decade, by about 2% in adults compared to the prior decade (Hoffman et al., 2017). This age-specific decrease may be related to improvements in health care or access to care and prevention of known risk factors for hearing loss, improved education, environmental noise protections [e.g., workplace hearing protection, time limits for noise exposure, community noise level limits], and management of vascular or disease risk factors.
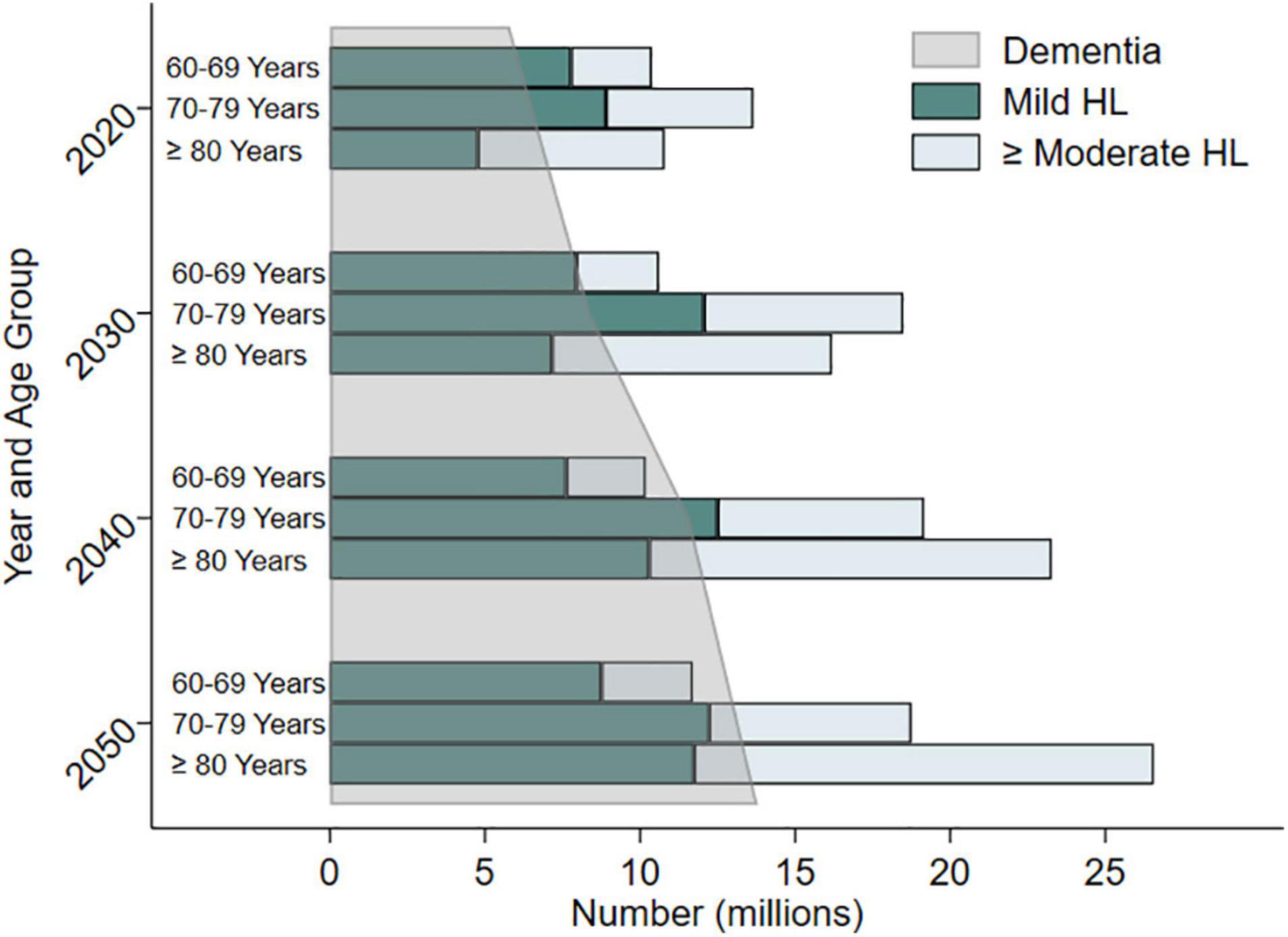
Figure 3. Estimated and projected trends in prevalence of hearing loss (mild hearing loss and moderate or greater hearing loss) and dementia in older adults by age categories in the United States from 2020 to 2050. Data compiled from Goman et al. (2017) and the Alzheimer’s Disease Facts and Figures 2020 Report. Adapted from Powell et al. (2021).
Globally, the cost of unaddressed hearing loss is estimated at over $980 billion annually (World Report on Hearing, 2021). Economic costs of lost productivity due to hearing loss is estimated widely at $1.8–$194 billion in the United States alone. Excess medical costs due to hearing loss was estimated at $3.3–$12.8 billion (Huddle et al., 2017). Individually, over a span of 10 years, the difference in mean total healthcare costs for someone with hearing loss compared to someone without hearing loss is over $22,000 in the United States (Reed et al., 2019), due in part to increased rate of hospitalizations, higher risk of hospital readmission, and longer hospital stays. This economic cost may take a toll on societies and families managing the social, economic, and healthcare needs of older adults. While hearing loss has its greatest prevalence among older adults, significant hearing loss is not necessarily an inevitable consequence of aging, as everyone has a different hearing trajectory shaped by genetic, environmental, and health related factors from across the life course.
The prevalence of hearing loss varies by non-modifiable factors such as certain identified syndromes and genetic factors (World Report on Hearing, 2021). Additional non-modifiable factors include race/ethnicity and possibly biological sex (Curhan et al., 2017). While a lower prevalence of hearing loss is noted among women compared to men, thought primarily related to behavioral and lifestyle choices (i.e., increased noise exposure), some evidence suggests a biological protective effect of estrogen among women (Hultcrantz et al., 2006; Shuster et al., 2019). Additionally, hearing loss has a lower prevalence in Black adults compared to Hispanic or non-Hispanic White adults (Bainbridge and Wallhagen, 2014; Goman and Lin, 2016), suspected in part due to a protective effect of melanin in the inner ear (Lin et al., 2017).
Additional potential causative risk factors for hearing loss across the life course have also been identified (World Report on Hearing, 2021). While many risk factors for hearing loss stem from prenatal or perinatal causes/determinants (i.e., intrauterine infections, delivery complications), other risk factors for hearing loss in adolescence and adulthood have also been identified (World Report on Hearing, 2021). These include: otitis media (i.e., ear infections), viral infections or pathogens (e.g., measles, mumps, meningitis, HIV, Lassa virus, Ebola), chronic disease (e.g., hypertension, cardiovascular disease, diabetes), smoking, use of ototoxic medications (i.e., cisplatin, carboplatin, gentamicin) head trauma, excessive noise exposure from occupational, recreational, or environmental noise, ear-related conditions such as Meniere’s disease, autoimmune disease, or vestibular schwannomas, and nutritional deficiencies from nutrients like Vitamin A, zinc, and iron. As stated, one of the greatest risk factors for hearing loss is increasing age due to age-related sensorineural hearing loss. This is a multifactorial condition thought influenced by genetics, environmental factors, lifestyle, and illnesses. While it is not yet determined if all of these factors are causal, each is correlated with increased risk of hearing loss.
Historically, hearing loss has been considered a benign component of the aging process resulting primarily in impaired communication. However, research over the last few decades has highlighted hearing loss as a precipitating factor for additional functional and neuropsychiatric disorders in older adults and has spurred changes in thought within the medical and public health community (Lopez et al., 2011; Lin et al., 2013; Kamil et al., 2014). Importantly, hearing loss is generally considered modifiable through amplification (i.e., hearing aids or amplification devices). The overall goal of amplification is to aid in the restoration of auditory input from impaired peripheral hearing and serve as a tool to help manage the presence of background or competing noise for communication and comfort. Therefore, the scientific and clinical community has begun to recognize the potential protective benefit of hearing loss management, particularly for neuropsychiatric conditions like depression and dementia (Rutherford et al., 2018). Therapeutic opportunity exists, as hearing aids are vastly underutilized: on average only ∼30% of eligible adults obtain hearing aids in the United States (Bainbridge and Wallhagen, 2014), with similar uptake reflected in peer countries (World Report on Hearing, 2021). Recent investigation suggests trends in improved uptake of amplification devices in the United States, however disparities and divergences are noted for lower income older adults (Reed et al., 2021). While significant barriers and disparities in hearing health care and accessibility of care and services remain, as will be discussed later, the potential room for intervention growth and public health benefit is substantial. Management of hearing loss through amplification options may not only decrease risk for neuropsychiatric conditions (Rutherford et al., 2018), but may also improve treatment adherence, patient satisfaction, and improve overall health-related quality of life for older adults (Bigelow et al., 2020). Understanding subgroups of older adults who may receive particular benefit from increased amplification use may therefore save health care costs, reduce burden, and improve outcomes – including dementia.
The expected rise in dementia cases around the world requires action on dementia prevention and intervention across innovative and multi-disciplinary channels to meet the pressing societal and health needs. With no known dementia cure, epidemiologic research then seeks to discern risk factors associated with the progression of dementia pathology, progression of dementia symptoms, or with dementia diagnosis to delay or minimize the impact of clinical symptoms (Livingston et al., 2020). If we can identify such risk factors, we may cultivate increased focus and direction for research to possibly delay dementia onset. Delaying the onset of dementia by just 5 years through intervention could lead to a 57% reduction in the number of dementia cases (Sperling et al., 2011) and 40% lower cost for care and services in 30 years (Zissimopoulos, 2014). Epidemiologic research has provided much of the foundational evidence for the association between hearing loss and dementia. This research has allowed for recognition of how the under-utilization of hearing loss treatment strategies presents an opportunity for potential advancement. With potential collaboration across the unique disciplines associated with cognitive aging and auditory science, opportunity for novel intervention and prevention strategies to enrich our evidence base for dementia prevention exists.
In this review, we highlight evidence of the association and potential causal effect primarily within studies utilizing completed objective measures of auditory function (i.e., audiogram, validated speech-in-noise testing). While consideration of self-reported hearing is important, it integrates aspects of not only peripheral auditory function but also of an individual’s perceived hearing and communication ability, incorporating environmental and communication demands, mental health, listening motivation and expectations, and central auditory function.
Heterogeneity in study methodology and design creates challenges to synthesize data from hearing and cognition research. Heterogeneity exists across audiometric and cognitive parameters as well as sample sizes, populations studied, and consideration of confounders, to name a few. Within auditory science, heterogeneity includes aspects such as differing means to define hearing loss, pure tone frequencies used, or how hearing ability is categorized. For cognitive research, variability in the neurocognitive tests used, domains investigated, utilization of cognitive screeners, patient or physician report, and ways of defining cognitive change (i.e., cognitive decline, subjective cognitive impairment, mild cognitive impairment, or diagnosed dementia) all create obstacles for evidence synthesis.
The Lancet Commission (Livingston et al., 2017, 2020) reported a pooled relative risk of 1.9 times greater risk of incident dementia among hearing impaired individuals 55 years of age and older compared to those with normal hearing. However, only three longitudinal studies (Lin et al., 2011; Gallacher et al., 2012; Deal et al., 2016) on the association between peripheral hearing impairment and incident dementia met the Commissions specified inclusion criteria of audiometrically (objective) measured hearing, longitudinal evaluation (at least 5 years), and covariate adjustment. While requirement of longitudinal evaluation and covariate adjustment require little justification, audiometrically measured hearing allows for measurement of a more isolated effect of peripheral hearing loss due to cochlear damage rather than the more convoluted measurement of central auditory function or self-report hearing. As audiometry serves as the gold-standard for objective measures of hearing, its validity has been well investigated in a variety of populations. As audiometry is a measure of peripheral function, it is likely not strongly influenced by cortical changes from dementia and can be appropriately completed within populations even with early dementia (Uhlmann et al., 1989; McClannahan et al., 2021). These aspects support minimal concern of the association resulting from reverse causation with dementia leading to impaired audiometry and PTA, although other studies suggest differing conclusions (Brenowitz et al., 2020). Detailed summaries of current evidence have been provided in a handful of other publications (Albers et al., 2015; Fortunato et al., 2016; Thomson et al., 2017; Loughrey et al., 2018; Yuan et al., 2018; Sharma et al., 2021).
A previous meta-analysis (Loughrey et al., 2018) found the odds of cognitive impairment for those with age related hearing loss was 1.22 (95% CI: 1.09, 1.36) and odds of dementia was 1.28 (95% CI: 1.02, 1.59) times higher than those with normal hearing. Prior work has noted an association between hearing loss and declines in global cognitive function, executive function, processing speed, and memory (Lin et al., 2011; Loughrey et al., 2018; Alattar et al., 2020; Gao et al., 2020; Brewster et al., 2021). However, what constitutes hearing ability or cognitive impairment often differs across studies. Some studies have included continuous measures of hearing as decibels hearing level (dB HL) (Armstrong et al., 2019), while others have categorized hearing ability by clinically recognized categories [i.e., mild or greater loss (Lin et al., 2011, 2013; Deal et al., 2016; World Report on Hearing, 2021)] or have only considered specific frequency ranges (Uhlmann et al., 1989; Gates et al., 1996) as compared to the common clinically utilized range of 500–4000 Hz or 500–8000 Hz. The diverse definitions of hearing loss make it challenging to synthesize the current evidence base as the degree of hearing difficulty varies by categorization used and represents different levels of resultant impairment and functional ability. For example, categorization of those with any measured hearing loss (i.e., Pure Tone Average [PTA] ≥ 25 dB HL) vs. consideration of those with a moderate or greater hearing loss (PTA > 40 dB HL) as the hearing-impaired group likely constitutes different comparison groups and underlying idea of what is a hearing “loss” across different studies.
Varied measures of cognition used have also placed challenging demands on synthesis of prior results. A plethora of validated neurocognitive assessments exist both across cognitive domains and as global screeners. Variation in domain, mode of administration, if accommodations for hearing loss were considered, whether cognitive status was determined by provider or proxy report exist across studies, among others. While the importance of evaluating cognitive ability in multiple ways should not be ignored due to the complexity of cognitive processing and complex diagnostic presentation, synthesis of results across studies remains aloof.
While an association between cognitive decline/dementia and peripheral auditory function is well established (Livingston et al., 2020), the relationship between cognitive decline/dementia with central auditory function has been less studied in the epidemiologic literature. Given the interdependence between central auditory function and cognitive processing, it becomes difficult to distinguish between the two processing abilities. For speech to be properly understood, the auditory stimuli must first maintain sufficient integrity to be accurately encoded by the peripheral auditory system and must then be decoded by the central auditory system (Humes, 2021). For the auditory signal to be decoded by the central auditory system, higher level cognitive processing is required. Research over the last few decades has attempted to distinguish the boundaries between central auditory dysfunction (CAD) and cognitive impairment (CHABA, 1988; Humes et al., 2013a). Heterogeneity in defining central auditory function and cognitive processing has led to significant barriers to evidence synthesis and causal inference. As with peripheral hearing loss, a diverse array of definitions, tests, cognitive domains, and sample populations has been utilized for studies across disciplines.
Prior systematic reviews have revealed mixed quality and potential bias in previous work on central auditory function and cognition (Dryden et al., 2017). Dryden et al. (2017) report an overall weak correlation between cognitive performance and speech perception/central auditory function depending on the cognitive domain and speech-in-noise assessment used. The strongest correlation was observed between central auditory function and processing speed. It has yet to be determined what degree un-aided peripheral hearing ability has in the moderating or modifying of the association between central hearing (e.g., decoding of speech stimuli or speech perception ability in noise) and cognitive performance. Overall, results demonstrate an interconnection in cortical resources utilized for both processes (Humes, 2013; Humes et al., 2013b; Humes and Young, 2016; Sardone et al., 2019), presenting challenges for inference but also noteworthy opportunity to identify novel targets for intervention or prevention.
It has been hypothesized CAD may serve as an early marker and therefore a possible prodromal symptom of cognitive decline (Gates et al., 1996). We know AD pathology reaches the auditory cortex. Nearly 30 years ago, Sinha et al. (1993) demonstrated the presence of plaques and neurofibrillary tangles within the medial geniculate body and central nucleus of the inferior colliculus in patients diagnosed with AD compared to those without a diagnosis. Additionally, neurofibrillary plaques and tangles were found in the primary auditory and auditory association cortices of patients diagnosed with AD. While, Braak staging (Braak and Braak, 1991, 1997) suggests these auditory cortices are some of the final brain regions affected by AD pathology. However, evidence indicates functional disconnection effects from the involvement in higher order cortical areas may affect the primary auditory cortex in early Alzheimer’s disease (Sardone et al., 2019). Importantly, the cortical areas associated with age related hearing loss and compensatory cortical activation to support language processing like the cingulate cortex are also involved in cognitive function like episodic memory and are affected early in the AD disease process, having specific implications for complex auditory processing (Goll et al., 2010, 2011, 2012; Sardone et al., 2019). These ideas support CAD as a marker of AD, but with unclear indication of CAD as an early marker (Sardone et al., 2020). How this presentation of pathology at later stages of progression translates to earlier identification of AD, beyond abilities from currently identified neurological and biological biomarkers is unclear. Yet behavioral testing of central auditory function suggests utility. Gates et al. (2011) demonstrated in a sample of volunteers from a dementia surveillance cohort over nine times greater hazard for incident dementia (95% CI: 3.6, 26.7) among those with severe CAD compared to those with proposed normal function. A pilot study in a well-characterized aging cohort found poor cognitive performance on memory, language, executive function, and global function for those with poor speech-in-noise performance regardless of peripheral hearing status (Mamo et al., 2019). The associations for some domains were attenuated after excluding those with a moderate or greater hearing loss, suggesting peripheral hearing may play a role in performance within certain cognitive domains that are dependent on speech tasks.
Many prior studies have employed the Dichotic Sentence Identification test (DSI) as a measure of central auditory function. The DSI presents a meaningless but grammatically correct sentence to each ear simultaneously and the listener is to then identify the sentences, with designated systematically differing modes of reporting the sentence items (Fifer et al., 1983). This diagnostic tool, primarily used currently in research settings, was designed to be less susceptible to peripheral hearing ability when presented at a conversational level of 50 dB HL. Therefore, some propose poor performance on the DSI test may be more reflective of cognitive ability rather than incorporating influence from peripheral hearing and the simple inability to hear the test (Jerger, 2019). DSI has been used to differentiate memory impairment among those demonstrating mild memory impairment without dementia (Gates et al., 2008). However, the DSI test and many other central auditory function assessments have minimal clinical utility due to complex presentation requirements and time-intensiveness.
Investigation of various means to define and measure central auditory function suggest an association with subjective memory complaints/impairment (Idrizbegovic et al., 2011; Fausto et al., 2018). In a small sample, subjective memory complaints were associated with poor performance on certain central auditory processing evaluations but not with peripheral hearing ability (Jayakody et al., 2020), potentially further supporting speech-in-noise difficulty as a marker of cognitive function. Yet proper implementation of this information for dementia prevention and intervention remains unclarified.
Across measures of central auditory processing, an association has been observed between biomarkers such as CSF tau, cortical thickness and volumetric measures of AD-related brain regions (Tuwaig et al., 2017), although existing supporting evidence remains limited. Given the rapidly expanding identification of dementia related biomarkers, what central auditory processing measures may add to our existing repertoire is an important consideration for future research and identification of pre-clinical dementia, whether considering generic ‘dementia’ and all subtypes, or considering more targeted research on AD specifically given its epidemiologic importance. Consideration of sensory loss more broadly (i.e., hearing, vision, and olfactory ability) has received more recent attention as indicators of pre-clinical dementia. For example, advances in retinal imaging may shed light on early brain changes associated with Alzheimer’s disease (Snyder et al., 2016; Zhang et al., 2021). Yet, like central auditory processing, there is much we still must determine regarding these measures and neurological pathways to understand any potential role of sensory biomarkers in identification of preclinical dementia.
Due to low-risk auditory rehabilitation tools such as hearing aids, hearing loss in older adults is readily considered modifiable and therefore makes it a worthy target of interest among dementia risk factors. The current limited use of hearing aids and challenges with accessibility of hearing devices and services have been a focus of both health research and public policy in recent years (National Academies of Sciences, Engineering, and Medicine, 2016), bringing new force behind the idea of hearing loss management as a means for dementia intervention. Existing data and reports of the use of hearing aids for cognitive decline stem largely from observational and cross-sectional study and present mixed findings (Amieva et al., 2015; Maharani et al., 2018; Ray et al., 2018; Dawes et al., 2019; Amieva and Ouvrard, 2020). In observational studies, we are often not able to completely control for factors which determine or influence if an individual pursues or uses hearing aids or other forms of hearing treatment (e.g., socioeconomic status, education background, social support and engagement, access to healthcare) — many of these factors are also protective against cognitive decline. These challenges present difficulty when trying to isolate the potential protective effect from hearing aids from that of these external factors, potentially influencing estimated effects due to aspects of selection into study of hearing aid use. Well-designed pilot interventions and clinical trials have taken up this challenge in recent years to determine if the use of hearing aids may alter subsequent risk of dementia (Brewster et al., 2020). These clinical trials present unique opportunity inherent within study design by minimizing this potential bias from confounding factors through design tools like randomization and masking (Celentano and Szklo, 2020). One of the largest and longest clinical trials to date on the use of hearing aids for dementia prevention is currently underway in The Aging and Cognitive Health Evaluation in Elders (ACHIEVE) clinical trial (Deal et al., 2018). While not powered to detect a difference for memory scores, the ACHIEVE pilot study demonstrated suggestion of an efficacy signal in memory test performance for participants randomized to hearing treatment, including hearing aid use, compared to a health education control (Deal et al., 2017). The pilot study also indicated positive proximal outcomes of improved participant perception of hearing handicap and improved social network. We have yet to determine how age and rapidity of hearing loss onset and its proximity to hearing aid uptake may modify dementia risk. The influence of other rehabilitation strategies on dementia risk, such as basic communication strategies, cochlear implants, or auditory training, is vastly understudied.
The complexities and interdependence between central auditory function and cognitive processing present challenges for causal inference. Therefore, current hypotheses of mechanistic pathways predominantly view peripheral hearing loss as a potential cause of dementia and consider central auditory function as a marker of cognitive decline. Current hypotheses of the causal mechanistic pathways have been well articulated in other works (Lin and Albert, 2014; Wayne and Johnsrude, 2015; Griffiths et al., 2020; Johnson et al., 2021; Powell et al., 2021). Clarifying this mechanistic pathway has far-reaching implications for research, the design, implementation, and evaluation of dementia prevention strategies, and the translation of the evidence to recommendations for patient care or health policy. A smaller body of evidence currently supports the notion that dementia leads to hearing loss (CHABA, 1988; Baltes and Lindenberger, 1997). A larger collection of evidence supports the notion hearing loss may contribute toward cognitive decline— directly through what is commonly known as the sensory deprivation hypothesis, or indirectly through the information-degradation hypothesis (Wayne and Johnsrude, 2015). Alternatively, hearing loss and dementia may result from an additional external factor through what is considered the common-cause hypothesis (Wayne and Johnsrude, 2015; Powell et al., 2021). In this article, we briefly review evidence to support each hypothesized pathway as depicted in our modified mechanistic framework (Figure 4).
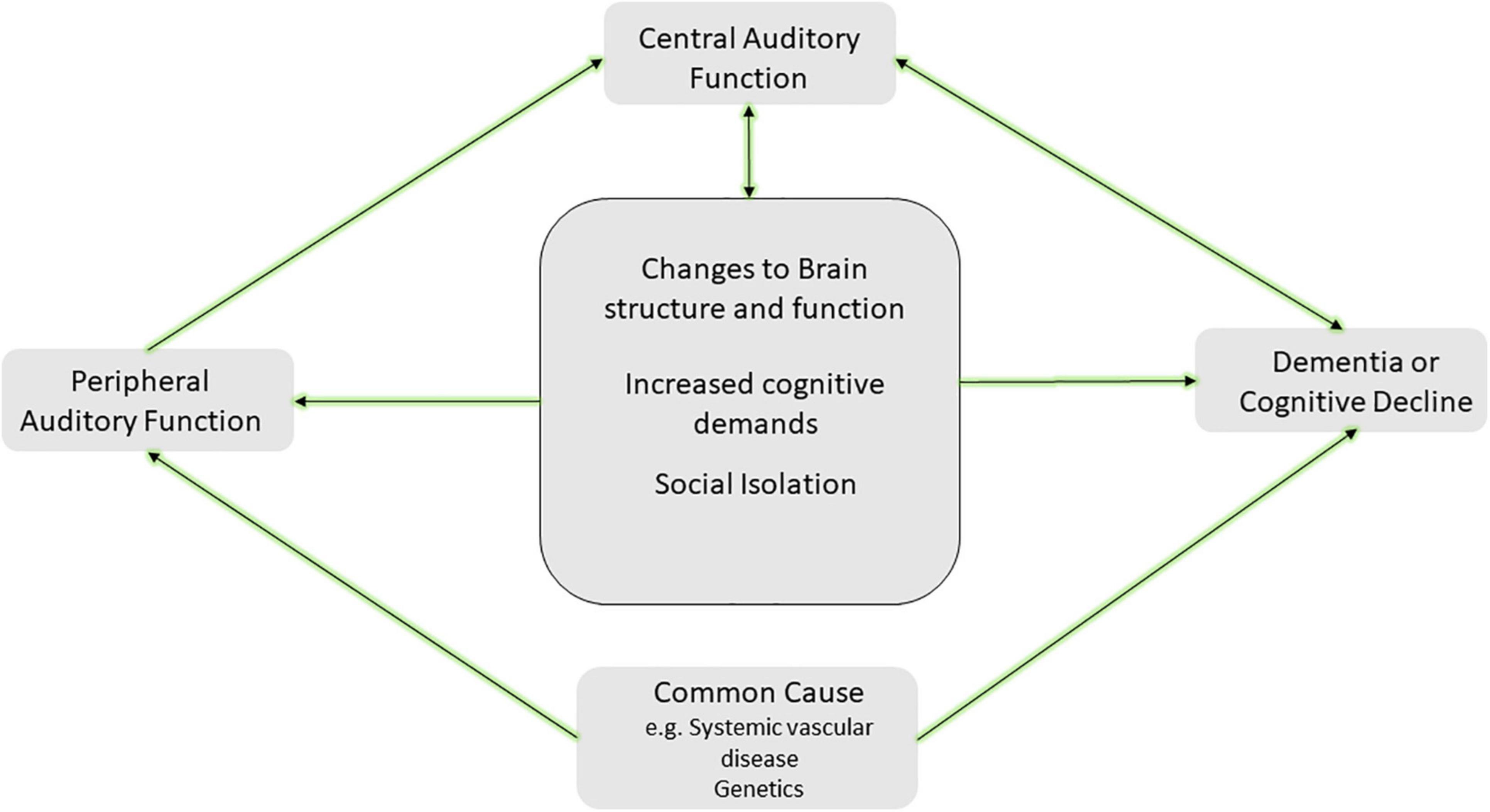
Figure 4. Hypothesized framework for the mechanism of the hearing and dementia association. The center square includes potential causal paths between peripheral hearing loss and cognitive decline or dementia, including changes to brain structure and function (i.e., sensory deprivation hypothesis), increased cognitive demands (i.e., information degradation hypothesis), and other effects such as social isolation. Additionally, a common cause such as systemic vascular disease or genetic factors may lead to both peripheral hearing loss and cognitive decline and dementia. Further inclusion of central auditory function resulting from direct and indirect effects of this causal pathway is depicted and may serve as a marker of cognitive decline or dementia. It is likely more than one of the pathways depicted may explain the link between hearing and dementia. Adapted from Powell et al. (2021).
A growing body of evidence indicates prolonged sensory deprivation has an adverse effect on the brain, with enduring changes to brain structure and function. Due to auditory deprivation from ARHL, neural deafferentation, cortical re-allocation for support of other processes, and atrophy in brain regions important for speech perception processing may occur. The resultant reorganization may add to existing brain pathology (e.g., amyloid burden, neuronal loss) at the detriment of general cognitive performance by altering critical brain regions which could otherwise be utilized for higher-level cognitive processing. Reduced gray matter density and reductions in temporal lobe volume are observed in those with peripheral hearing loss (Lin et al., 2014; Wingfield and Peelle, 2015; Armstrong et al., 2019), as prolonged sensory deprivation may lead to changes and decreases in cortical brain volume in conjunction with that seen with expected cognitive aging or neurodegenerative disease (Lin et al., 2014; Eckert et al., 2019). The brain regions most notably affected are pertinent for semantic memory and preclude advancement along the continuum of cognitive decline, including frontal and pre-frontal regions, the superior temporal gyrus and Heschel’s gyrus (Husain et al., 2011). Cortical regions enlisted for speech understanding like the frontal cortex and hippocampus are also associated with reductions in whole-brain gray matter volume (Rudner et al., 2019). Even among those older adults considered free of dementia, hearing loss appears to be associated with reduced white matter microstructural integrity in cortical regions crucial for cognitive processing (Rigters et al., 2017; Alfandari et al., 2018; Armstrong et al., 2019; Croll et al., 2020). Research has yet to determine importance of the duration of sensory deprivation or evidence for a sensitive period in age of onset of hearing loss and how this relates to the structural changes observed. While cortical changes and reorganization from hearing loss is evident even among those in the earliest stages of cognitive impairment (Campbell and Sharma, 2014; Sharma and Glick, 2017), the extent of cortical reorganization necessary to evoke brain atrophy and changes to cognitive performance is unclear. Prolonged sensory deprivation, therefore, may result in physical reductions in cortical volume in addition to that experienced from dementia pathology alone. This sensory deprivation may necessitate cortical reorganization resulting in further restriction of cortical capacity available for cognitive processing. How and if these brain volume changes represent specific pathologic changes for types of dementia remains to be clarified. Longitudinal study of the role of peripheral hearing loss and association with AD amyloid pathology on PET imaging did not suggest an association (Parker et al., 2020) but work in this space using specified biomarkers of dementia has been understudied.
While the sensory deprivation hypothesis suggests physical changes to the brain due to prolonged hearing loss which subsequently impacts cognitive processing, the information degradation hypothesis proposes the association stems from increased demands on cognitive processing in order to compensate for impoverished sensory input. The additional processing required to compensate for degraded auditory perception draws on the same resources needed for other higher-level cognitive processing and semantic encoding (Peelle, 2018). These increased cognitive demands required to appropriately encode auditory stimuli requires extensive listening effort particularly with memory, attention, and executive function (Wingfield et al., 2005; Tun et al., 2009, 2012; Pichora-Fuller et al., 2016; Peelle, 2018). An individual’s ability to compensate for subsequent diminished cognitive performance is heterogeneous and may contribute toward the known variability in cognitive performance, presentation, and clinical symptoms among similar existing brain pathology. With hearing loss, this increased cognitive and listening effort may increase cognitive load at any time of day as the auditory system never “turns off,” thereby drawing on the cognitive buffer of the individual and their ability to compensate for cognitive changes and resulting in earlier presentation of clinical symptoms and dementia (Whitson et al., 2018). The compensatory mechanisms activated on cognitive tasks between older and younger adults with sensory deficits differ, with older adults demonstrating increased fatigue on dual tasks that rely on both listening and understanding (Schneider et al., 2002). Essentially, the information degradation hypothesis implies acute cognitive impairment. If we are able to restore auditory input, we may therefore see at least some restoration of cognitive performance on higher-level tasks.
Alternatively, both hearing loss and cognitive impairment may merely stem from the same underlying mechanism (Baltes and Lindenberger, 1997; Wayne and Johnsrude, 2015). Given the presumed independent effect of peripheral hearing on cognitive processing when measured through audiometry, investigation of a common cause which may be associated with hearing and cognition has largely been evaluated via pure tone audiometry. A potential common mechanism might include the overall neural degeneration common with aging, resulting in both decreased auditory ability and decreased cognitive performance (Surprenant and Neath, 2006; Wayne and Johnsrude, 2015). Additionally, a given dementia pathology (most commonly discussed as AD pathology) may lead to early CAD and impaired hearing prior to more general cognitive decline (Johnson et al., 2021). Decreased processing speed with age may lead to slower cognitive functioning overall as well as slower processing speed for sensory integration and perception (CHABA, 1988; Salthouse, 1996). Dementia pathology from a central cause may therefore produce early dysfunction within the central auditory system resulting in impaired hearing ability (i.e., auditory scene analysis or ability in complex listening environments) prior to the presentation of more general cognitive decline or impairments. As described in the review by Griffiths et al. (2020), it is also possible degraded peripheral signals lead to dysfunctional pattern processing within the central auditory system (particularly the medial temporal lobe) and interacts with existing neurodegenerative or AD pathology, resulting in the observed association. With this hypothesis, whether the increased neuronal activity from degraded auditory input causing or increasing AD pathology, or the degraded auditory input from hearing loss may reduced activity for auditory cognitive processes within the medial temporal lobe remains to be clarified, however, either speculation supports early identification of hearing loss prior to prolonged duration of decreased auditory input and broad hearing-dementia intervention strategies.
It is possible both auditory and neural functioning are altered by systemic vascular pathology impacting the spiral ganglion or stria vascularis of the auditory system and bran vasculature. Therefore, vascular disease in older adults may also subsequently lead to concurrent cognitive and sensory changes (Eckert et al., 2013; Laughlin et al., 2013; Livingston et al., 2017), although this hypothesis is challenging to confirm due to the long prodromal stage of some dementias like AD. Exploration of a common genetic risk between AD and hearing loss using a weighted sum of AD polymorphisms and AD inflammatory pathway suggests a possible genetic link with poorer speech-in-noise performance and self-reported difficulty hearing in background noise (Brenowitz et al., 2020). However, study of Apolipoprotein ε4 (APOE ε4) has shown no association with hearing loss (Morita et al., 2019), nor does it modify the association between hearing loss and cognitive decline (Alattar et al., 2020). Other work suggests the presence of one or more APOEε4 alleles may actually be marginally associated with better hearing in older adults as measured via pure tone audiometry, perhaps because APOE ε4 is more common in Black adults, but hearing loss is more prevalent in White adults (Mener et al., 2016). While APOE ε4 serves as a strong risk factor for dementia, based on current evidence, it does not appear to be a driving factor in the hearing-dementia association. Although the genetic determinants of ARHL are largely unknown, identifying what (if any) genetic determinants exist may provide further insight toward additional avenues of a common cause between hearing loss and dementia (Wells et al., 2019). Overall, few studies have investigated the role of genetic risk on causality in the hearing-dementia link, therefore some question of association with shared genes remains (Mitchell et al., 2020).
Other risk factors for dementia may also mediate the association of hearing and cognition including: loneliness, social isolation, depression, decreased physical activity, or frailty. Studies have demonstrated the presence of hearing loss leads to increased social isolation and/or loneliness for some older adults as individuals with hearing loss may withdraw from previously enjoyed activities or social interactions due to the inability to engage and communicate with others. Links between social isolation or loneliness and dementia are well established (Rutherford et al., 2018; Maharani et al., 2019; Rafnsson et al., 2020; Shukla et al., 2020). The evidence for link between hearing loss and depression, which may serve as a risk factor and/or prodromal sign of dementia, remains mixed (Rutherford et al., 2018). While an increasing body of evidence suggests increased risk of depression with hearing loss, the direction of association remains to be clarified. The heterogeneous course of depression in older adults as it relates to hearing loss has received minimal investigation (Brewster et al., 2018). It is possible hearing loss leads to reduced physical activity and physical functioning, each a known risk factor for dementia, due to decreased auditory awareness with surroundings and anxiety (Chen et al., 2015; Choi et al., 2016; Martinez-Amezcua et al., 2021). Some evidence suggests a greater prevalence of frailty among those with hearing loss, another condition which has been suggested as an independent risk factor or early marker of dementia (Panza et al., 2015; Liljas et al., 2017). Each proposed potential mediator and pathway presents an identified opportunity for targeted intervention, yet how each may fit within a larger dementia framework remains to be clarified.
Multiple potential pathways area likely involved in the association between hearing and dementia, but with unknown understanding of the specific contribution of each pathway and if this contribution varies by the individual. While common risk factors (i.e., age, education, vascular disease) are thought to contribute toward the association (Whalley et al., 2004; Humes, 2013; Wayne and Johnsrude, 2015), these factors likely do not explain the full story. Even in large epidemiologic studies which have attempted to control for these additional factors, the association persists, suggesting additional pathways are likely involved but have yet to be differentiated.
Identification of research priorities given the transdisciplinary scope of study on hearing and dementia will aid in achieving foundational dementia research goals: to advance our identification of subgroups of adults who may present greater risk for cognitive decline/dementia or suggest novel options for intervention or prevention. Numerous pressing research questions and additional perspectives on the importance of these questions prevail (Wayne and Johnsrude, 2015; Whitson et al., 2018; Powell et al., 2021). Here we feature four research priorities which, in our opinion, will provide leading advancements in the possible causal role of hearing loss along the dementia continuum: (1) determination of the pathway of association, (2) management of potential bias due to sensory loss in cognitive testing, (3) determining if we can modify dementia risk by treating hearing loss, (4) understanding if biomarkers or indicators of sensory loss are useful for identification of pre-clinical dementia (Figure 5).
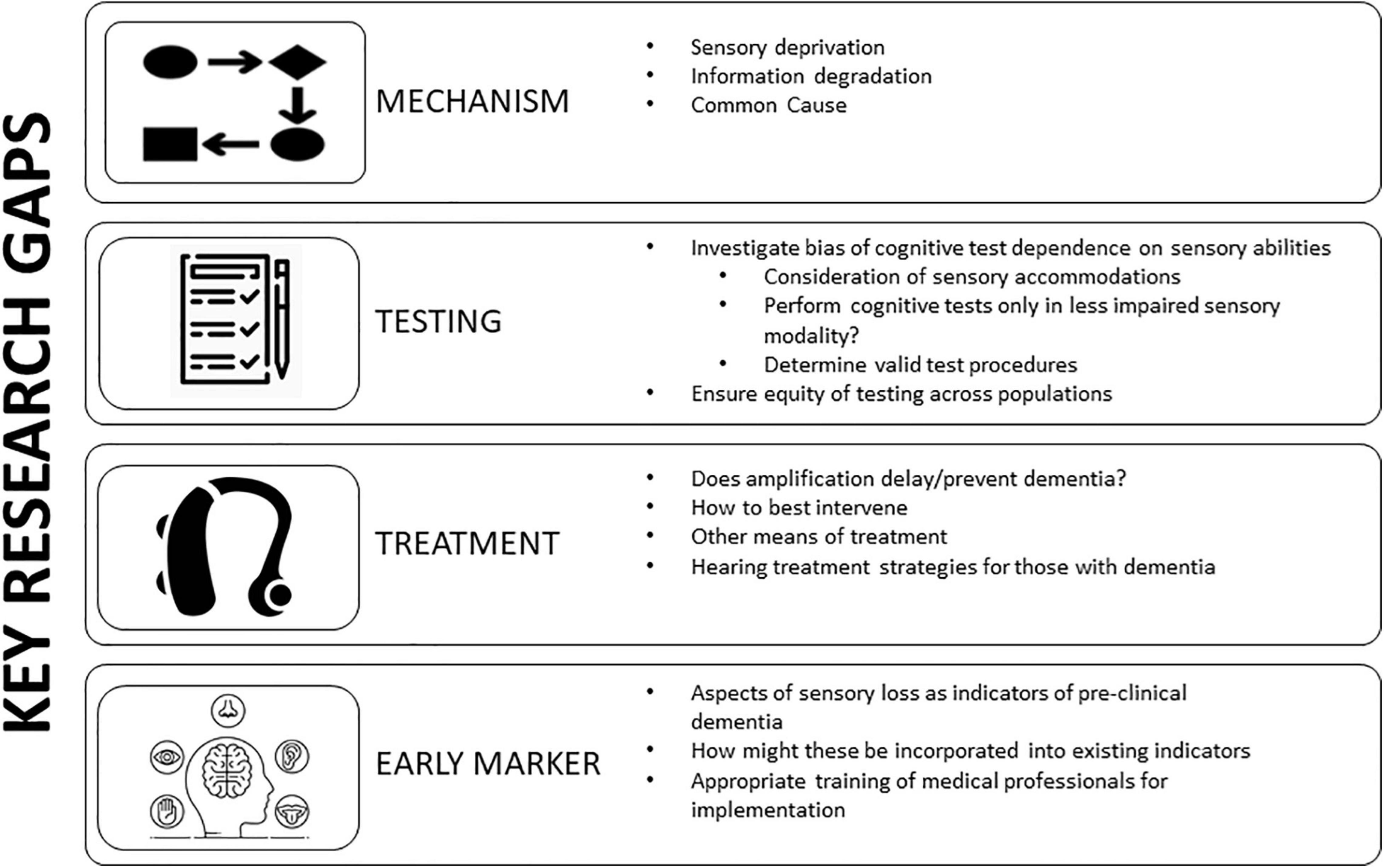
Figure 5. Key research gaps in hearing impairment and cognition. Targeted research on the mechanism behind the association between hearing and cognition will guide intervention and prevention strategies. Additional research gaps include an understanding of potential bias in cognitive testing due to dependence on sensory abilities and how best to study and minimize this bias. Further understanding of if treating hearing loss via amplification or another means influences dementia risk is vital for public health. Determination if markers of sensory impairment may serve as indicators of pre-clinical dementia and how this may be incorporated with existing biomarkers. Adapted from Powell et al. (2021).
Given the varied temporal contributions of each proposed mechanistic pathway, determination of which pathway(s) serve as the primary driver behind the association is vital. This determination may allow for improved study design and planning and well as more informed clinical intervention to delay or prevent the onset of cognitive symptoms and delay the progression along or alter the trajectory of the clinical course of dementia. With the current insufficient evidence to declare hearing loss has an independent effect on cognitive impairment for older adults, how we should intervene on hearing loss, when to do so, and if such interventions are effective in decreasing or delaying dementia risk will all largely depend on the underlying mechanism. We know the presentation of dementia symptomatology is heterogeneous across individuals even with the same underlying pathology. We have yet to determine by what manner hearing loss may influence a potential buffer which delays/prevents the presentation of symptoms in some individuals yet fails do so in others, leading to earlier symptomatology.
If the association between hearing loss and dementia is only due to a common cause, the potential for directly delaying or preventing changes in the presentation of dementia symptoms or pathology through hearing would be extremely limited as the underlying cause would remain untreated. The research intervention focus would ultimately turn toward the underlying common confounder, which could then have downstream effects for hearing and cognition. However, the use of hearing management such as hearing aids may support cognition through indirect pathways like improving social engagement and communication yet decreasing cognitive load and strain on central auditory function through improvement of peripheral auditory input, directly preventing dementia would remain elusive.
A direct effect of hearing loss on cognitive function is inferred with the sensory-deprivation and information degradation hypotheses. A long-term versus short term-effect is implied depending on the proposed pathway, yet both advocate that hearing loss, and notably untreated hearing loss, leads to downstream consequences for cognitive resources with important implications for approaches to intervention. The sensory deprivation hypothesis posits structural and functional changes in the brain due to lack of auditory stimulation. Therefore, preemptive identification of hearing loss and early adoption of treatment strategies which delay or prevent deafferentation or atrophy within the auditory or sensory regions of the brain are essential to prevent lasting structural damage. Importantly, auditory rehabilitation to prevent structural and functional changes in the brain through sensory deprivation may even have benefit at later stages of hearing loss by delaying additional neural reorganization or atrophy. For comparison, the information degradation hypothesis strongly supports hearing intervention at any time in the disease process. With restoration of the integrity of auditory stimuli via rehabilitation or hearing management, the cognitive demands and utilized cognitive resources for speech and environmental awareness would in theory be reduced, allowing for cognitive resources to again be allocated to overall cognitive processing and compensation.
It is imperative we determine how to disentangle CAD and cognitive decline if we are to consider its use in targeting prevention efforts or early identification of subgroups at greater risk for cognitive decline. How to differentiate between changes in cognitive processing and CAD, the temporality between each processing condition, and whether CAD may serve as an early marker for specific subtypes of dementia remains a challenging barrier for characterizing the link between hearing loss and dementia. While the majority of research to date has focused on the association between hearing loss and Alzheimer’s disease since the most common form of dementia and pathology observed, distinctions in association with other dementia pathologies is paramount. The dependence and entanglement of both forms of hearing on higher-level cognitive functioning stirs question of how to interpret the role of each process along the auditory pathway. If CAD may serve as an early marker of dementia remains to be determined.
As stated, it is likely multiple mechanistic pathways are involved in the hearing-dementia association. Determining if one pathway serves as the primary driver, or if the pathway is unique to the individual may provide an opportunity for a person-centered approach to dementia prevention and intervention. Furthermore, while not mutually exclusive, determining the role of central vs. peripheral hearing in the hearing-dementia association will further inform research and clinical use of hearing and prevention or as an early marker of dementia.
A goal of any neurocognitive test battery is to accurately measure cognitive function for all individuals. Yet the validity of cognitive assessments inherently depends on an individual’s auditory or visual ability to access test materials. This interdependence has led some to question whether there is a bias or confounding introduced by a sensory impairment during cognitive testing for older adults (Guerreiro and Van Gerven, 2017; Füllgrabe, 2020). An investigation testing this hypothesis used item response theory methods to disentangle the true effect of sensory impairment on test performance (Nichols et al., 2021) in two longitudinal aging cohorts. Results suggest some differences in performance related to sensory loss, particularly among those with the poorest health or greatest cognitive impairment. However, for the vast majority of participants, cognitive performance on testing was not found to be biased due to sensory impairment (Villeneuve et al., 2017; Bott et al., 2019, 2020). Further determination of how best to conduct cognitive testing among those with sensory loss is vital for clinical and research settings.
While exclusion of those with severe sensory loss from testing might ensure completion of evaluations, this exclusion limits our understanding of the role of sensory loss in cognition. One way to assess cognitive function among those with hearing loss may be to utilize cognitive test batteries that are administered via visual modality rather than auditory. However, this strategy does not fully address issues that arise among those with dual sensory impairment (i.e., those with both vision and hearing loss).
An alternative approach to address sensory loss when administering cognitive assessments is to consider accommodations for the sensory loss (Littlejohn et al., 2021). If an individual usually wears a hearing aid or glasses, it would be important to remind the individual to bring these sensory aids for optimal completion of evaluations. Accommodations for sensory loss might include offering test instructions in written (i.e., large print) as well as oral format, ensuring the testing is completed in a quiet and well-lit environment, or provision of a personal amplifier such as a pocket-talker or a visual aid for test takers. Accounting for hearing and vision needs during study conception, design and analysis, as well as during test administration will be important for confidence in study results. Regardless of the different types of cognitive test used, it is imperative that we include individuals with different types and degrees of sensory loss in studies, in order to advance our understanding of the role of sensory loss in cognition (Pye et al., 2017; Littlejohn et al., 2021).
Recent decades have seen an accumulation of evidence for the impact of treating hearing loss on cognitive decline or dementia. Our observational studies have provided foundational and pivotal insights into the hearing-dementia association, however, evidence of causality for decreased or delayed cognitive decline due to hearing aid use is more challenging. From a neurocognitive perspective on this investigation, challenges include selection effects of older adults into studies. Individuals who pursue and obtain a hearing aid are generally a select group of adults— often with higher education, higher income, and greater health seeking behaviors— all of which are considered protective factors for cognitive decline (National Academies of Sciences, Engineering, and Medicine, 2016; Livingston et al., 2020; Reed et al., 2021).
Many barriers to obtaining hearing aids still exist within the United States and must be considered within the context of existing research on the use of hearing aids as dementia prevention or intervention. Hearing aid and aural rehabilitation services are not covered under Medicare or many private insurances, placing the cost of the device and services (often $1000 or more) on the individual and family. Further, an audiologic evaluation and aural rehabilitation appointments are not currently available through direct-access to patients under some American insurances, but require referral from a primary care physician or specialist (National Academies of Sciences, Engineering, and Medicine, 2016). This added barrier with a need for both patients and providers to understand how to navigate the healthcare system and for patients to attend additional medical appointments currently creates added barriers to hearing treatment which may prevent or deter some individuals from seeking care. While access to hearing devices and services is improved in some countries, global barriers remain as far as availability of trained professionals or cost of devices (World Report on Hearing, 2021). Additional challenges include collection of hearing data and data on hearing aid use, and unmeasured confounding. Data on hearing ability is often not collected or collected only in very limited form in many epidemiologic or non-auditory based studies. Additionally, data on hearing aid use and amount of use is virtually non-existent. Owning a hearing aid is not synonymous with using a hearing aid. Further, individuals vastly over-report their use of the hearing aid (Taubman et al., 1999), yet wearing a device regularly and often is the only means to ensure the brain has had the ability to adapt to increased auditory stimuli. What constitutes “regularly and often” remains to be clarified and may be individualized (Hickson et al., 2014). Without this information, it remains challenging for us to determine how hearing aid use may modify the hearing-dementia association, or any other health outcome for older adults.
Without understanding the mechanism(s) behind the hearing-dementia association, it is challenging to determine how and when is best to intervene on cognitive decline and dementia. Evidence for treatment of hearing loss throughout the dementia continuum is growing, yet many questions remain. Evidence of efficacy, effectiveness and cost efficiency will aid in determining the best aural rehabilitation choices for prevention — all areas with extensive gaps in evidence for hearing loss and dementia.
In addition to potentially serving as a dementia prevention strategy, hearing aids may present opportunity for intervention for neuropsychiatric symptoms (NPS) at all stages of dementia and negative health outcomes associated with NPS (Kales et al., 2014). Breakdowns in communication between those individuals with dementia/cognitive impairment and their caregivers along with decreased awareness of surroundings may contribute to behavioral changes commonly noted with more progressed disease (Littlejohn et al., 2021). The use of a hearing assistive device in older adults with cognitive impairment has been found to result in fewer and less severe NPSs and less severe depressive symptoms (Kim et al., 2020). Therefore, hearing aid use among dementia patients demonstrate improved communication, reduced NPS, decreased perception of hearing handicap, and improved quality of life for both individuals and their caregivers (Dawes et al., 2015, 2019; Mamo et al., 2018; Littlejohn et al., 2021).
Additional work is needed to determine how best to provide auditory rehabilitation for adults with cognitive impairment. A recent study (Hubbard et al., 2018) suggests treating hearing loss in cognitively impaired older adults yields benefits for both the older adult as well as caregiver dyads. A recent internationally gathered task force on identification and management of hearing and vision loss among those living with dementia (Littlejohn et al., 2021) highlighted six key areas of practice recommendations and identified targeted areas for improvement, including: awareness and knowledge, recognition and detection, evaluation, management, support, services and policies. However, the group acknowledged that a dearth of evidence across many of these areas left the basis of broad recommendations to be placed on expert and patient input at times, vowing to revisit recommendations in a few years in the hopes of improved scientific evidence. Even with expert recommendations for management, hearing is not automatically “restored” with the use of a hearing aid. Instead, hearing aids should be considered a tool to improve audibility and access to environmental and speech sounds. For a new hearing aid user, most individuals require an adjustment period as the brain re-habituates to increased access to the auditory environment and stimulation after a potentially prolonged period of sensory deprivation. This aspect of hearing loss management may be unclear or unknown to patients and non-auditory science researchers without the appropriate training and counseling. How to provide this counseling for persons with dementia and their families has, to our knowledge, not been studied.
While hearing aids serve as the most prominent means of hearing intervention, other means of aural rehabilitation are available such as personal amplifiers, general assistive listening devices, or auditory training strategies. Research is limited on the use of these alternative strategies for treatment of hearing loss along the dementia continuum, yet determination of a variety of accessible alternative strategies is fundamental for providing communication ability and social engagement for older adults. Hearing aids may not be feasible for some older adults (e.g., those with severe cognitive impairment) and likely do not meet the listening needs of many adults when used as the only form of rehabilitation. As mentioned, adaptation to increased auditory stimuli requires extensive cortical adjustment which may overwhelm some individuals without proper counseling and consideration. Non-technology driven alternative strategies (e.g., training in communication strategies such as speaking face-to-face, turning off or reducing the presence of competing background noise, talking from the same room, use of additional visual cues/aids, improving self-efficacy advocacy) (Nieman et al., 2017) require further evaluation to determine how these proven strategies might be utilized for older adults with cognitive impairment.
Importantly, the use of hearing aids has a primary role in management of peripheral hearing loss, contributing to the focused effort of public health research on peripheral rather than central hearing ability and the association with cognitive decline/dementia. If the pathway linking hearing to cognition is related (directly or in part) due to central auditory processing and ability, the use of hearing aids as a prevention and intervention option for dementia will have minimal effect given the state of current technology and auditory processing treatments. While hearing aid use may not delay the progression of dementia pathology if the association is due to a common cause, as stated above the use of hearing aids may still indirectly support intervention of progression of the clinical presentation of dementia symptoms through indirect pathways such as decreased cognitive load and improved social stimulation. Future advances in hearing aid technology which may better address cognitive and central auditory demands may provide even greater benefit. Currently, evidence for the role of central auditory processing and central hearing disorders for early identification of dementia will have heightened importance and emphasize the need for consideration of greater use in neuropsychological and medical evaluations.
The high prevalence of not only hearing loss, but also vision loss, among older adults presents opportunity for additional access points for identification of pre-clinical dementia if hearing or vision may serve as an early marker of dementia- a point which has yet to be determined and has received minimal study (Brenowitz et al., 2019; Johnson et al., 2021). We do not yet know if sensory loss indicators (i.e., optical coherence tomography, fundus photography, speech-in-noise testing, auditory scene analysis or auditory cognitive testing, electrophysiology, etc.) aid in earlier identification of cognitive change. If sensory loss does prove to be a valuable tool for identification of pre-clinical dementia, then we must determine how to use this tool in patient-provider planning and diagnosis as well as within our research models. Additionally, training on discussion with health care professionals for the appropriate referrals and how to convey results within each represented scope of practice is essential for appropriate dementia planning (Littlejohn et al., 2021).
Although research on the role of hearing loss on dementia risk initiated over 40 years ago, recent surge in the evidence supporting adverse outcomes across health and care among older adults with hearing loss has come to the attention of patients and their families, clinicians, and policy makers. The human and economic expense of caring for the expected growing number of adults reaching or past retirement age demands interdisciplinary collaboration. While the fields of cognitive science, neuroscience, and gerontology have been at the core of dementia research, allied-health disciplines such as auditory science present untapped opportunity to contribute toward efforts to reduce the burden of dementia across societies. A thorough understanding of the current evidence, identification of leading hypothesis and elucidation of the mechanism(s) driving the association between hearing and dementia, consideration of sensory loss during cognitive testing or in care strategies for those with dementia or dementia prevention, and targeted future directions of research can have a significant impact on prevention and intervention strategies for older adults. The interdependent and synergistic processes of hearing and cognition require careful approach for research and clinical care. The current limitations in dementia treatment necessitate innovative approaches for dementia intervention. Identification of additional early markers of dementia, a potential role of central auditory function with continued research may aid in this process, as well as inform optimal strategies for hearing management itself. Considering the presence of other conditions, like hearing loss, and optimizing our strategies to evaluate and treat hearing loss could diminish the risk of adverse outcomes and enhance health and quality of life for older adults.
DP was responsible for the initial drafting, editing, and formatting. EO, NR, FL, and JD contributed to content and editing. All authors contributed to the article and approved the submitted version.
DP was supported by NIH/NIA T32AG066576. JD was supported by NIH/NIA grant K01AG054693. EO was supported by NIH grant R01AG057725. NR was supported by NIH/NIA grant K23AG065443.
NR reports being a scientific advisory board member of Shoebox Inc and Neosensory. FL reports being a consultant to Frequency Therapeutics, speaker honoraria from Caption Call, and being the director of a public health research center funded in part by a philanthropic gift from Cochlear Ltd to the Johns Hopkins Bloomberg School of Public Health.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Parts of this manuscript were adapted from that printed in the Journal of the Association for Research in Otolaryngology. 2021 July; 22(4): 387–403. doi: 10.1007/s10162-021-00799-y. While common ideas are represented across manuscripts for consistency across disciplines related to current knowledge and key gaps in future research, differences in scientific writing and discussions of emphasis are uniquely tailored to the respective journal of publication.
Alattar, A., Bergstrom, J., Laughlin, G., Kritz-Silberstein, D., Richard, E., Reas, E., et al. (2020). Hearing impairment and cognitive decline in older, community dwelling adults. J. Gerontol. A Biol. Sci. Med. Sci. 75, 567–573.
Albers, M. W., Gilmore, G. C., Kaye, J., Murphy, C., Wingfield, A., Bennett, D., et al. (2015). At the interface of sensory and motor dysfunctions and Alzheimer’s disease. Alzheimer’s Dementia 11, 70–98. doi: 10.1016/j.jalz.2014.04.514
Alfandari, D., Criend, C., Heslenfeld, D. J., Versfeld, N. J., Kramer, S. E., and Zekveld, A. D. (2018). Brain volume differences associated with hearing impairment in adults. Trends Hear. 22, 1–8.
Amieva, H., and Ouvrard, C. (2020). Does treating hearing loss in older adults improve cognitive outcomes? a review. J. Clin. Med. 9:805. doi: 10.3390/jcm9030805
Amieva, H., Ouvrard, C., Giulioli, C., Meillon, C., Rullier, L., and Dartigues, J.-F. (2015). Self-reported hearing loss, hearing aids, and cognitive decline in elderly adults: a 25-year study. J. Am. Geriatr. Soc. 63, 2099–2104. doi: 10.1111/jgs.13649
Armstrong, N. M., An, Y., Doshi, J., Erus, G., Ferrucci, L., Davatzikos, C., et al. (2019). Association of midlife hearing impairment with late-life temporal lobe volume loss. JAMA Otolaryngology-Head Neck Surg. 145, 794–802. doi: 10.1001/jamaoto.2019.1610
Bainbridge, K. K., and Wallhagen, M. I. (2014). Hearing loss in an aging american population: extent, impact, and management. Ann. Rev. Public Health 35, 139–152. doi: 10.1146/annurev-publhealth-032013-182510
Baltes, P. B., and Lindenberger, U. (1997). Emergence of a powerful connection between sensory and cognitive function across the adult lifespan: a new window to the study of cognitive aging? Psychol. Aging 12, 12–21. doi: 10.1037//0882-7974.12.1.12
Bigelow, R., Reed, N., Brewster, N., Huang, A., Rebok, G., Rutherford, B. R., et al. (2020). Association of hearing loss with psychological distress and utilization of mental health services among adults in the United States. JAMA Network Open 3:e2010986. doi: 10.1001/jamanetworkopen.2020.10986
Bott, A., Hickson, L., Meyer, C., Bardy, F., Van dun, B., Pachana, N., et al. (2020). Is cortical automatic threshold estimation a feasible alternative for hearing threshold estimation with adults with dementia living in aged care? Int. J. Audiol. 59, 745–752. doi: 10.1080/14992027.2020.1746976
Bott, A., Meyer, C., Hickson, L., and Pachana, N. A. (2019). Can adults living with dementia complete pure-tone audiometry. Int. J. Audiol. 58, 185–192.
Braak, H., and Braak, E. (1991). Neuropathological stageing of Alzheimer-related changes. Acta Neuropathol. 82, 239–259.
Braak, H., and Braak, E. (1997). Frequency of stages of Alzheimer-related lesions in different age categories. Neurobiol. Aging 18, 551–357.
Bregman, A. S. (1993). “Auditory scene analysis: hearing in complex environments,” in Thinking in Sound: the Cognitive Psychology of Human Audition, eds S. McAdams and E. Bigand (Oxford: Oxford University Press).
Brenowitz, W., Kaup, A., and Yaffe, K. (2019). Multiple sensory impairment is associated with increased risk of dementia among black and white older adults. J. Gerontol. Med. Sci. 74, 890–896. doi: 10.1093/gerona/gly264
Brenowitz, W. D., Filshtein, T. J., Yaffe, K., Walter, S., Ackley, S. F., Hoffman, T. J., et al. (2020). Association of genetic risk score for Alzheimer disease and hearing impairment. Neurology 95, e2225–e2234.
Brewster, K. K., Ciarleglio, A., Brown, P. J., Chen, C., and Kim, H. (2018). Age-Related hearing loss and its association with depression in later life. Am. J. Geriatric Psychiatry 26, 788–796. doi: 10.1016/j.jagp.2018.04.003
Brewster, K. K., Hu, M., Wall, M., Brown, P., Zilcha-Mano, S., Roose, S. P., et al. (2021). Age-related hearing loss, neuropsychological performance, and incident dementia in older adults. J. Alzheimer’s Dis. 80, 855–864. doi: 10.3233/jad-200908
Brewster, K. K., Pavlicova, M., Stein, A., Chen, M., Chen, C., Brown, P. J., et al. (2020). A pilot randomized controlled trial of hearing aids to improve mood and cognition in older adults. Int. J. Geriatr. Psychiatry 35, 842–850. doi: 10.1002/gps.5311
Campbell, J., and Sharma, A. (2014). Cross-modal re-organization in adults with early stage hearing loss. PLoS One 9:e90594. doi: 10.1371/journal.pone.0090594
CHABA (1988). Speech understanding and aging. working group on speech understanding and aging. committee on hearing, bioacoustics, and biomechanics, commission on behavioral and social sciences and Education, National Research Council. J. Acoustical Soc. Am. 83, 859–895. doi: 10.1121/1.395965
Chang, H., Ho, C., and Chou, P. (2009). The factors associated with a self-perceived hearing handicap in elderly people with hearing impairment- results from a community-based study. Ear. Hear. 30, 576–583. doi: 10.1097/AUD.0b013e3181ac127a
Chen, D. S., Betz, J., Yaffe, K., Ayonayon, H. N., Kritchevsky, S., Martin, K. R., et al. (2015). Association of hearing impairment with declines in physical functioning and the risk of disability in older adults. J. Gerontol. Series A Biol. Sci. Med. Sci. 70, 654–661. doi: 10.1093/gerona/glu207
Choi, J. S., Betz, J., Deal, J., Contrera, K. J., and Genther, D. J. (2016). A comparison of self-report and audiometric measures of hearing and their associations with functional outcomes in older adults. J. Aging Health 28, 890–910. doi: 10.1177/0898264315614006
Croll, P. H., Vernooij, M. W., Reid, R. I., Goedegebure, A., Power, M. C., Rigters, S. C., et al. (2020). Hearing loss and microstructural integrity of the brain in a dementia-free older population. Alzheimer’s Dementia 16, 1515–1523. doi: 10.1002/alz.12151
Curhan, S. G., Eliassen, A. H., Eavey, R. D., Wang, M., Lin, B. M., and Curhan, G. C. (2017). Menopause and postmenopausal hormone therapy and risk of hearing loss. Menopause 24, 1049–1056. doi: 10.1097/gme.0000000000000878
Dawes, P., Emsley, R., Cruickshanks, K. J., Moore, D. R., Fortnum, H., Edmondson-Jones, M., et al. (2015). Hearing loss and cognition: the role of hearing aids, social isolation and depression. PLoS One 10:e0119616. doi: 10.1371/journal.pone.0119616
Dawes, P., Wolski, L., Himmelsbach, I., Regan, J., and Leroi, I. (2019). Interventions for hearing and vision impairment to improve outcomes for people with dementia: a scoping review. Int. Psychogeriatr. 31, 203–221.
Deal, J. A., Albert, M. S., Arnold, M., Bangdiwala, S. I., Chisolm, T., Davis, S., et al. (2017). A randomized feasibility pilot trial of hearing treatment for reducing cognitive decline: results from the aging and cognitive health evaluation in Elders Pilot Study. Alzheimer’s Dementia: Transl. Res. Clin. Interventions 3, 410–415. doi: 10.1016/j.trci.2017.06.003
Deal, J. A., Beta, J., Yaffe, K., Harris, T., Purchase-Helzner, E., Satterfield, S., et al. (2016). Hearing impairment and incident dementia and cognitive decline in older adults: the health ABC Study. J. Gerontol. Ser. A: Biol. Sci. Med. Sci. 72, 703–709.
Deal, J. A., Goman, A. M., Albert, M. S., Arnold, M. L., Burgard, S., Chisolm, T., et al. (2018). Hearing treatment for reducing cognitive decline: design and methods of the aging and cognitive health evaluation in Elders randomized controlled trial. Alzheimer’s Dementia: Transl. Res. Clin. Interventions 4, 499–507. doi: 10.1016/j.trci.2018.08.007
Dryden, A., Allen, H. A., Henshaw, H., and Heinrich, A. (2017). The association between cognitive performance and speech-in-noise perception for adult listeners: a systematic literature review and meta-analysis. Trends Hear. 21:2331216517744675. doi: 10.1177/2331216517744675
Eckert, M. A., Kuchinsky, S. E., Vaden, K. I., Cute, S. L., Spampinato, M. V., and Dubno, J. (2013). White matter hyperintensities predict low frequency hearing in older adults. J. Assoc. Res. Otolaryngol. 14, 425–433. doi: 10.1007/s10162-013-0381-4
Eckert, M. A., Vaden, K. I. Jr., and Dubno, J. R. (2019). Age-related hearing loss associations with changes in brain morphology. Trends in Hearing 23:2331216519857267.
Fausto, B., Badana, A., Arnold, M., Lister, J., and Edwards, J. (2018). Comparison of subjective and objective measures of hearing, auditory processing, and cognition among older adults with and without mild cognitive impairment. J. Speech Lang. Hear Res. 61, 945–956. doi: 10.1044/2017_JSLHR-H-17-0263
Fifer, R., Berger, J., Berlin, C., Tobey, E. A., and Campbell, J. C. (1983). Development of a dichotic sentence identification test for hearing-impaired adults. Ear Hear. 4, 300–305. doi: 10.1097/00003446-198311000-00007
Fortunato, S., Forli, F., Guglielmi, V., De Corso, E., Paludetti, G., Berrettini, S., et al. (2016). A review of new insights on the association between hearing loss and cognitive decline in ageing. Acta Otorhinolaryngol. Ital. 36, 155–166.
Füllgrabe, C. (2020). On the possible overestimation of cognitive decline: the impact of age-related hearing loss on cognitive-test performance. Front. Neurosci. 14:454. doi: 10.3389/fnins.2020.00454
Gallacher, J., Ilubaera, V., Ben-Shlomo, Y., Bayer, A., Fish, M., Babisch, W., et al. (2012). Auditory threshold, phonologic demand, and incident dementia. Neurology 79, 1583–1590. doi: 10.1212/WNL.0b013e31826e263d
Gao, J., Armstrong, N., Deal, J., Lin, F., and He, P. (2020). Hearing loss and cognitive function among Chinese older adults: the role of participation in leisure activities. BMC Geriatrics 20:215. doi: 10.1186/s12877-020-01615-7
Gates, G. A. (2012). Central presbycusis: an emerging view. Otolaryngology-Head Neck Surg. 141, 1–2. doi: 10.1177/0194599812446282
Gates, G. A., Anderson, M. L., McCurry, S. M., Feeney, M. P., and Larson, E. B. (2008). Central auditory dysfunction in older people with memory impairment or Alzheimer’s dementia. Arch. Otolaryngol. Head Neck Surg. 134, 771–777. doi: 10.1001/archotol.134.7.771
Gates, G. A., Anderson, M. L., McCurry, S. M., Feeney, M. P., and Larson, E. B. (2011). Central auditory dysfunction as a harbinger of Alzheimer’s dementia. Arch. Otolaryngol. Head Neck Surg. 137, 390–395. doi: 10.1001/archoto.2011.28
Gates, G. A., Cogg, J. L., Linn, R. T., Rees, T., Wolf, P. A., and D’Agostino, R. B. (1996). Central auditory dysfunction, cognitive dysfunction, and dementia in older people. Arch. Otolaryngol. Head Neck Surg. 122, 161–167. doi: 10.1001/archotol.1996.01890140047010
George, E., Zekveld, A., Kramer, S., Goverts, T., Festen, J., and Houtgast, T. (2007). Auditory and nonauditory factors affecting speech reception in noise by older listeners. J. Acoust. Soc. Am. 121:2362. doi: 10.1121/1.2642072
Goll, J. C., Crutch, S. J., Loo, J. H. Y., Rohrer, J. D., Frost, C., Bamiou, D. E., et al. (2010). Non-verbal sound processing in the primary progressive aphasia. Brain 133, 272–285. doi: 10.1093/brain/awp235
Goll, J. C., Kim, L. G., Hailstone, J. C., Lehman, M., Buckley, A., Crutch, S. J., et al. (2011). Auditory object cognition in dementia. Neuropsychologia 49, 2755–2765. doi: 10.1016/j.neuropsychologia.2011.06.004
Goll, J. C., Kim, L. G., Ridgway, G. R., Hailston, J. C., Lehman, M., and Buckley, A. H. (2012). Impairments of auditory scene analysis in Alzheimer’s disease. Brain 135, 190–200.
Goman, A., and Lin, F. R. (2016). Prevalence of hearing loss by severity in the United States. Am. J. Public Health 106, 1820–1822. doi: 10.2105/ajph.2016.303299
Goman, A., Reed, N. S., and Lin, F. R. (2017). Addressing estimated hearing loss in adults in 2060. JAMA Otolaryngol. Head Neck Surg. 143, 732–734.
Griffiths, T. D., Lad, M., Kumar, S., Holmes, E., McMurrary, B., Maguire, E., et al. (2020). How can hearing loss cause dementia? Neuron 108, 401–412. doi: 10.1016/j.neuron.2020.08.003
Grube, M., Bruffaerts, R., Schaeverbeke, J., Neyens, V., De Weer, A. S., Seghers, A., et al. (2016). Core auditory processing deficits in primary progressive aphasia. Brain 139, 1817–1829. doi: 10.1093/brain/aww067
Guerreiro, M. J. S., and Van Gerven, P. W. M. (2017). Disregarding hearing loss leads to overestimation of age-related cognitive decline. Neurobiol. Aging 56, 180–189. doi: 10.1016/j.neurobiolaging.2017.05.001
Hickson, L., Meyer, C., Lovelock, K., Lampert, M., and Khan, A. (2014). Factors associated with success with hearing aids in older adults. Int. J. Audiol. 53, 18–27.
Hoffman, H. J., Dobie, R. A., Losonczy, K. G., Themann, C. L., and Flamme, G. A. (2017). Declining prevalence of hearing loss in US adults aged 20 to 69 Years. JAMA Otolaryngol. Head Neck Surg. 143, 274–285. doi: 10.1001/jamaoto.2016.3527
Hubbard, H. I., Mamo, S. K., and Hopper, T. (2018). Dementia and hearing loss: interrelationships and treatment considerations. Sem. Speech Lang. 39, 197–210. doi: 10.1055/s-0038-1660779
Huddle, M. G., Goman, A. M., Kernizan, F. C., Foley, D. M., Price, C., Frick, K. D., et al. (2017). The economic impact of adult hearing loss: a systematic review. JAMA Otolaryngol. Head Neck Surg. 143, 1040–1048. doi: 10.1001/jamaoto.2017.1243
Hultcrantz, M., Simonoska, R., and Stenberg, A. (2006). Estrogen and hearing: a summary of recent investigations. Acta Otolaryngol. 126, 10–14. doi: 10.1080/00016480510038617
Humes, L. E. (2013). Understanding the speech-understanding problems of older adults. Am. J. Audiol. 22, 303–305. doi: 10.1044/1059-0889(2013/12-0066)
Humes, L. E. (2021). Factors underlying individual differences in speech-recognition thresholds (SRT) in noise among older adults. Front. Aging Neurosci. 13:702739. doi: 10.3389/fnagi.2021.702739
Humes, L. E., Busey, R. A., Craig, J., and Kewley-Port, D. (2013a). Are age-related changes in cognitive function driven by age-related changes in sensory processing? Atten. Percept. Psychophys. 75, 508–524. doi: 10.3758/s13414-012-0406-9
Humes, L. E., Kidd, G. R., and Lentz, J. L. (2013b). Auditory and cognitive factors underlying individuals differences in aided-speech-understanding among older adults. Front. Systems Neurosci. 7:55. doi: 10.3389/fnsys.2013.00055
Humes, L. E., Dubno, J., Gordon-Salant, S., Lister, J. L., Cacae, A. T., Cruickshanks, K. J., et al. (2012). Central presbycusis: a review and evaluation of the evidence. J. Am. Acad. Audiol. 23, 635–666. doi: 10.3766/jaaa.23.8.5
Humes, L. E., and Young, L. A. (2016). Sensory-cognitive interactions in older adults. Ear Hear. 37, (Suppl. 1), 52S–61S.
Husain, F. T., Medina, R. E., Davis, C. W., Szymko-Bennett, Y., Simonyan, K., Pajor, N. M., et al. (2011). Neuoanatomical changes due to hearing loss and chronic tinnitus: a combined VBM and DTI study. Brain Res. 1369, 74–88. doi: 10.1016/j.brainres.2010.10.095
Idrizbegovic, E., Hederstierna, C., Dahlquist, M., Kämpfe Nordström, C., Jelic, V., and Rosenhall, U. (2011). Central auditory function in early Alzheimer’s disease and in mild cognitive impairment. Age. Ageing 40, 249–254.
Jayakody, D., Menegola, H., Yiannos, J., Goodman-Simpson, J., Fiedland, P., and Taddei, K. (2020). The peripheral hearing and central auditory processing skills of individuals with subjective memory complaints. Front. Neurosci. doi: 10.3389/fnins.2020.00888
Jerger, J. (2019). Toward differentiation between SNHL, SNHL with cognitive decline, and SNHL with APD. Hear. Rev. 26, 18–22.
Johnson, J. C. S., Marshall, C. R., Weil, R. S., Bamiou, D. E., Hardy, C. J. D., and Warren, J. D. (2021). Hearing and dementia: from ears to brain. Brain 144, 391–401.
Kales, H. C., Gitlin, L. N., and Lyketsos, C. G. (2014). Detroit expert panel on the assessment, and management of the neuropsychiatric symptoms of dementia. management of neuropsychiatric symptoms of dementia in clinical settings: recommendations from a multisensory expert panel. J. Am. Geriatr. Soc. 62, 762–769. doi: 10.1111/jgs.12730
Kamil, R. J., Li, L., and Lin, F. R. (2014). Association of hearing impairment and frailty in older adults. J. Am. Geriatric Soc. 62, 1186–1188. doi: 10.1111/jgs.12860
Kim, A. S., Garcia Morales, E. E., Amjad, H., Cotter, V. T., Lin, F. R., Lyketsos, C. G., et al. (2020). Association of hearing loss with neuropsychiatric symptoms in older adults with cognitive impairment. Am. J. Psychiatry 29, 544–553. doi: 10.1016/j.jagp.2020.10.002
Laughlin, G. A., McEvoy, L. K., Barrett-Connor, E., Daniels, L. B., and Ix, J. H. (2013). Fetuin-A, a new vascular biomarker of cognitive decline in older adults. Clin. Endocrinol. 81, 134–140. doi: 10.1111/cen.12382
Liljas, A., Carvalho, L., Papachristou, E., De Oliveira, C., Wannamethee, G., Ramsay, S. E., et al. (2017). Self-reported hearing impairment and incident frailty in English community-dwelling older adults: a 4-year follow-up study. J. Am. Geriatr. Soc. 65, 958–965. doi: 10.1111/jgs.14687
Lin, B., Li, W., Curhan, S., Stankovic, K., Qureshi, A. A., and Curhan, G. C. (2017). Skin pigmentation and risk of hearing loss in women. Am. J. Epidemiol. 186, 1–10.
Lin, F. L., Metter, J., O’Brien, R. J., Resnick, S. M., Zonderman, A. B., and Ferrucci, L. (2011). Hearing loss and incident dementia. Arch. Neurol. 68, 214–220.
Lin, F. R., and Albert, M. (2014). Hearing loss and dementia- who’s listening? Aging Ment. Health 18, 671–673. doi: 10.1080/13607863.2014.915924
Lin, F. R., Ferrucci, L., An, Y., Goh, J. O., Doshi, J., Metter, E. J., et al. (2014). Association of hearing impairment with brain volume changes in older adults. Neuorimage 90, 84–92.
Lin, F. R., Yaffe, K., Xia, J., Xue, Q., Harris, T., Purchase-Helzner, E., et al. (2013). Hearing loss and cognitive decline among older adults. JAMA Int. Med. 173:10.1001/jamainternmed.2013.1868
Littlejohn, J., Bowen, M., Constantinidou, F., Dawes, P., Dickinson, C., Heyn, P., et al. (2021). International practice recommendations for the recognition and management of hearing and vision impairment in people with dementia. Gerontology doi: 10.1159/000515892
Livingston, G., Huntley, J., Sommerlad, A., Ames, D., Ballad, C., Banerjee, S., et al. (2020). Dementia prevention, intervention, and care. Lancet 396, 413–446.
Livingston, G., Sommerlad, A., Orgeta, V., Costafreda, S. G., Huntley, J., Ames, D., et al. (2017). Dementia prevention, intervention, and care. Lancet 390, 2673–2734.
Lopez, D., McCaul, K., Hankey, G., Norman, P., Almeida, O., Dobson, A., et al. (2011). Falls, injuries from falls, health related quality of life and mortality in older adults with vision and hearing impairment—is there a gender difference? Maturitas 69, 359–364. doi: 10.1016/j.maturitas.2011.05.006
Loughrey, D. G., Kelly, M. E., Kelley, G. A., Brennan, S., and Lawlor, B. A. (2018). Association of age-related hearing loss with cognitive function, cognitive impairment and dementia: a systematic review and meta-analysis. JAMA Otolaryngology-Head Neck Surg. 144, 115–126. doi: 10.1001/jamaoto.2017.2513
Maharani, A., Dawes, P., Nazroo, J., Tampubolon, G., and Pendleton, N. (2018). Longitudinal relationship between hearing aid use and cognitive function in older Americans. J. Am. Geriatr. Soc. 66, 1130–1136. doi: 10.1111/jgs.15363
Maharani, A., Pendleton, N., and Leroi, I. (2019). Hearing impairment, loneliness, social isolation, and cognitive function: longitudinal analysis using English Longitudinal Study on Ageing. Am. J. Geriatric Psychiatry 27, 1348–1356. doi: 10.1016/j.jagp.2019.07.010
Mamo, S., Reed, N., Sharrett, R., Albert, M., Coresh, J., Mosley, T., et al. (2019). Relationship between domain-specific cognitive function and speech-in-noise performance in older adults: the Atherosclerosis Risk in Communities Hearing Pilot Study. Am. J. Audiol. 28, 1006–1014. doi: 10.1044/2019_AJA-19-00043
Mamo, S. K., Reed, N. S., Price, C., Occhipinti, D., and Pletnikova, A. (2018). Hearing loss treatment in older adults with cognitive impairment: a systematic review. J. Speech Lang. Hear. Res. 61, 2589–2603. doi: 10.1044/2018_jslhr-h-18-0077
Martinez-Amezcua, P., Powell, D., Kuo, P. L., Reed, N. S., Sullican, K. J., Palta, P., et al. (2021). Association of age-related hearing impairment with physical functioning among community-dwelling older adults in the US. JAMA Network Open 4:e2113742. doi: 10.1001/jamanetworkopen.2021.13742
McClannahan, K., Chiu, Y. F., Somers, M., and Peelle, J. (2021). Test-Retest reliability of audiometric assessment in individuals with mild dementia. JAMA Otolaryngol. Head Neck Surg. 147, 442–449. doi: 10.1001/jamaoto.2021.0012
Mener, D. J., Betz, J., Yaffe, K., Harris, T. B., Helzner, E. P., Satterfeld, S., et al. (2016). Apolipoprotein E allele and hearing thresholds in older adults. Am. J. Alzheimer’s Dis. Other Dementias 31, 34–39. doi: 10.1177/1533317514537549
Mitchell, B. L., Thorp, J. G., Evans, D. M., Nyholt, D. R., and Martin, N. G. (2020). Exploring the genetic relationship between hearing impairment and Alzheimer’s disease. Alzheimer’s Dementia 12:e12108.
Morita, Y., Sasaki, T., Takahashi, K., Kitazawa, M., Nonomura, Y., Yagi, C., et al. (2019). Age-related hearing loss is strongly associated with cognitive decline regardless of APOE4 polymorphism. Otol. Neurotol. 40, 1263–1267. doi: 10.1097/mao.0000000000002415
Musiek, F., and Baran, J. (2018). The Auditory System: Anatomy, Physiology, and Clinical Correlates, 2nd Edn. San Diego, CA: Plural Publishing.
National Academies of Sciences, Engineering, and Medicine (2016). Hearing Health Care for Adults: Priorities for Improving Access and Affordability. Washington, DC: The National Academies Press, doi: 10.17226/23446
Nichols, E., Deal, J. A., Swenor, B. K., Abraham, A. G., Armstrong, N. M., Carlson, M. C., et al. (2021). Assessing bias in cognitive testing for older adults with sensory impairment: an analysis of differential item functioning in the baltimore longitudinal study on aging (BLSA) and the atherosclerosis risk in communities neurocognitive study (ARIC-NCS). J. Int. Neuropsychol. Soc. Online ahead of print. doi: 10.1017/S1355617721000400
Nieman, C. L., Marrone, N., Mamo, S. K., Betz, J., Choi, J. S., Contrera, K. J., et al. (2017). The Baltimore HEARS pilot study: an affordable, accessible community-delivered hearing care model. Gerontologist 57, 1173–1186. doi: 10.1093/geront/gnw153
Panza, F., Solfrizzi, V., Seripa, D., Imbimbo, B., Capozzo, R., et al. (2015). Age-related hearing impairment and frailty in Alzheimer’s disease: interconnected associations and mechanisms. Front. Aging Neurosci. 7:113. doi: 10.3389/fnagi.2015.00113
Parker, T., Cash, D. M., Lane, C., Lu, K., Malone, I. B., Nicholas, J. M., et al. (2020). Pure tone audiometry and cerebral pathology in healthy older adults. J. Neurol. Neurosurg. Psychiatry 91, 172–176. doi: 10.1136/jnnp-2019-321897
Peelle, J. (2018). Listening effort: how the cognitive consequences of acoustic challenge are reflected in brain and behavior. Ear Hear. 39, 204–214. doi: 10.1097/AUD.0000000000000494
Pichora-Fuller, M. K., Kramer, S. E., Eckert, M. A., Edwards, B., Hornsby, B. W. Y., Humes, L. E., et al. (2016). Hearing impairment and cognitive energy: the Framework for Understanding Effortful Listening (FUEL). Ear Hear. 37, 5S–27S.
Powell, D., Oh, E., Lin, F., and Deal, J. (2021). Hearing impairment and cognition in an aging world. J. Assoc. Res. Otolaryngol. 22, 387–403. doi: 10.1007/s10162-021-00799-7
Pye, A., Charalambous, A. P., Leroi, I., Thodi, C., and Dawes, P. (2017). Screening tools for the identification of dementia for adults with age-related acquired hearing or vision impairment: a scoping review. Int. Psychogeriatr. 29, 1771–1784. doi: 10.1017/s104161021700120x
Rabbitt, P. M. (1968). Channel-capacity, intelligibility and immediate memory. Quar. J. Exp. Psychol. 20, 241–248. doi: 10.1080/14640746808400158
Rafnsson, S. B., Orrell, M., d’Orsi, E., Hogervorst, E., and Steptoe, A. (2020). Loneliness, social integration, and incident dementia over 6 years: prospective findings from the English Longitudinal Study of Ageing. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 75, 114–124. doi: 10.1093/geronb/gbx087
Ray, J., Popli, G., and Gell, G. (2018). Association of cognition and age-related hearing impairment in the English Longitudinal Study of Ageing. JAMA Otolaryngol. Head Neck Surg. 144, 876–882. doi: 10.1001/jamaoto.2018.1656
Reed, N., Altan, A., Deal, J., Yeh, C., Kravetz, A., Wallhagen, M., et al. (2019). Trends in health care costs and utilization associated with untreated hearing loss over 10 years. JAMA Otolaryngol. Head Neck Surg. 145, 27–34. doi: 10.1001/jamaoto.2018.2875
Reed, N. S., Garcia-Morales, E., and Willink, A. (2021). Trends in hearing aid ownership among older adults in the United States from 2011 to 2018. JAMA Int. Med. 181, 383–385. doi: 10.1001/jamainternmed.2020.5682
Rigters, S. C., Bos, D., Metselaar, M., Roshchupkin, G. V., Baatengurg, de Jong, R. J., et al. (2017). Hearing impairment is associated with smaller brain volume in aging. Front. Aging Neurosci. 9:2. doi: 10.3389/fnagi.2017.00002
Rudner, M., Seeto, M., Keidser, G., Johnson, B., and Rönnberg, J. (2019). Poorer speech reception threshold in noise is associated with lower brain volume in auditory and cognitive processing regions. J. Speech Lang. Hear. Res. 62, 117–1130. doi: 10.1044/2018_JSLHR-H-ASCC7-18-0142
Rutherford, B. R., Brewster, K., Golub, J. S., Kim, A. H., and Roose, S. P. (2018). Sensation and Psychiatry: linking age-related hearing loss to late-life depression and cognitive decline. Am. J. Psychiatry 175, 215–224. doi: 10.1176/appi.ajp.2017.17040423
Salthouse, T. (1996). The processing-speed theory of adult age differences in cognition. Psychol. Rev. 103, 403–428. doi: 10.1037/0033-295x.103.3.403
Sardone, R., Battista, P., Donghia, R., Lozupone, M., Tortelli, R., Guerra, V., et al. (2020). Age-related central auditory processing disorder, MCI, and dementia in an older population in southern Italy. Otolaryngol. Head Neck Surg. 163, 348–355. doi: 10.1177/0194599820913635
Sardone, R., Battista, P., Panza, F., Lozupone, M., Griseta, C., Castellana, F., et al. (2019). The age-related central auditory processing disorder: silent impairment of the cognitive ear. Front. Neurosci. 13:619. doi: 10.3389/fnins.2019.00619
Schneider, B. A., Daneman, M., and Pichora-Fuller, M. K. (2002). Listening in aging adults: from discourse comprehension to psychoacoustics. Can. J. Exp. Pscyhol. 56, 139–152. doi: 10.1037/h0087392
Sharma, A., and Glick, H. (2017). Cross-modal plasticity in developmental and age-related hearing loss: clinical implications. Hear. Res. 343, 191–201. doi: 10.1016/j.heares.2016.08.012
Sharma, R. K., Chern, A., and Golub, J. S. (2021). Age-related hearing loss and the development of cognitive impairment and late-life depression: a scoping overview. Sem. Hear. 41, 10–25. doi: 10.1055/s-0041-1725997
Shukla, A., Harper, M., Pedersen, E., Goman, A., Suen, J. J., Price, C., et al. (2020). Hearing loss, loneliness, and social isolation: a systematic review. Otolaryngol. Head Neck Surg. 5, 622–633. doi: 10.1177/0194599820910377
Shuster, B., Depireux, D., Mong, J., and Hertzano, R. (2019). Sex differences in hearing: probing the role of estrogen signaling. J. Acoust. Soc. Am. 145, 3656–3663. doi: 10.1121/1.5111870
Sinha, U. K., Hollen, K. M., Rodriguez, R., and Miller, C. A. (1993). Auditory system degeneration in Alzheimer’s disease. Neurology 43, 779–785. doi: 10.1212/wnl.43.4.779
Snyder, P. J., Hohnson, L. N., Lim, Y. Y., Santos, C. Y., Alber, J., and Maruff, P. (2016). Nonvascular retinal imaging markers of preclinical Alzheimer’s disease. Alzheimer’s Dementia: Diag. Assess. Dis. Monitor. 4, 169–178. doi: 10.1016/j.dadm.2016.09.001
Sperling, R. A., Aisen, P. S., Beckett, L. A., Bennett, D. A., Craft, S., Fagan, A. M., et al. (2011). Toward defining the preclinical stages of Alzheimer’s disease: recommendations from the National Institute on Aging and the Alzheimer’s association workgroup. Alzheimer’s Dementia 7, 280–292. doi: 10.1016/j.jalz.2011.03.003
Surprenant, A. M., and Neath, I. (2006). “Cognitive aging,” in Gerontology: Perspectives and Issues, eds J. A. Wilmoth and K. Ferraro (New York NY: Springer).
Taubman, L. B., Palmer, C. V., Durrant, J. D., and Pratt, S. (1999). Accuracy of hearing aid use time as reported by experienced hearing aid wearers. Ear Hear. 20, 299–305. doi: 10.1097/00003446-199908000-00003
Thomson, R. S., Auduong, P., Miller, A. T., and Gurgel, R. K. (2017). Hearing loss as a risk factor for dementia: a systematic review. Laryngoscope Investigat. Otolaryngol. 2, 69–79. doi: 10.1002/lio2.65
Tun, P. A., McCoy, A., and Wingfield, A. (2009). Aging, hearing acuity, and the attentional costs of effortful listening. Psychol. Aging 24, 761–766. doi: 10.1037/a0014802
Tun, P. A., Willaims, V. A., Small, B. J., and Hafter, E. R. (2012). The effects of aging on auditory processing and cognition. Am. J. Audiol. 21, 344–350. doi: 10.1044/1059-0889(2012/12-0030)
Tuwaig, M., Savard, M., Jutras, B., Poirier, J., Louis Collins, D., Rosa-Neto, P., et al. (2017). Deficit in central auditory processing as a biomarker of pre-clinical Alzheimer’s disease. J. Alzheimer’s Dis. 60, 1589–1600. doi: 10.3233/JAD-170545
Uhlmann, R. F., Larson, E. B., Rees, R. S., Koepsell, T. D., and Duckert, L. G. (1989). Relationship of hearing impairment to dementia and cognitive dysfunction in older adults. J. Am. Med. Assoc. 261, 1916–1919. doi: 10.1001/jama.261.13.1916
Villeneuve, A., Hommet, C., Aussedat, C., Lescanne, E., Reffet, K., and Bakhos, D. (2017). Audiometric evaluation in patients with Alzheimer’s diseae. Eur. Arch. Otorhinolaryngol. 274, 151–157. doi: 10.1007/s00405-016-4257-1
Wayne, R. V., and Johnsrude, I. S. (2015). A review of causal mechanisms underlying the link between age-related hearing loss and cognitive decline. Ageing Res. Rev. 23, 154–166. doi: 10.1016/j.arr.2015.06.002
Wells, H., Freidin, M., Zainul Abidin, F., Payton, A., Dawes, P., Munro, K. J., et al. (2019). GWAS identifies 44 independent associated genomic loci for self-reported adult hearing difficulty in UK biobank. Am. J. Hum. Genet. 105, 788–802. doi: 10.1016/j.ajhg.2019.09.008
Whalley, L. J., Deary, I. J., Appleton, C. L., and Starr, J. M. (2004). Cognitive reserve and the neurobiology of cognitive aging. Ageing Res. Rev. 3, 369–382.
Whitson, H. E., Cronin-Golomb, A., Cruickshanks, K. J., Gilmore, G. C., and Owsley, C. (2018). American geriatrics society and national institute on aging bench-to-bedside conference: sensory impairment and cognitive decline in older adults. J. Am. Geriatr. Soc. 66, 2052–2058. doi: 10.1111/jgs.15506
Wingfield, A., and Peelle, J. E. (2015). The effects of hearing loss on neural plasticity and processing. Front. Systems Neurosci. 9:35. doi: 10.3389/fnsys.2015.00035
Wingfield, A., Tun, P. A., and McCoy, S. L. (2005). Hearing loss in older adulthood-what it is and how it interacts with cognitive performance. Curr. Direct. Psychol. Sci. 14, 144–148.
Yuan, J., Sun, Y., Sang, S., Huynh Pham, J., and Kon, W. (2018). The risk of cognitive impairment associated with hearing function in older adults: a pooled analysis of data from eleven studies. Sci. Rep. 8:2137. doi: 10.1038/s41598-018-20496-w
Zhang, Y., Wang, Y., Shi, C., Shen, M., and Lu, F. (2021). Advances in retina imaging as potential biomarkers for early diagnosis of Alzheimer’s disease. Transl. Neurodegenerat. 10:6.
Keywords: hearing loss, cognitive decline, dementia, prevention, dementia management, sensory loss, risk factor
Citation: Powell DS, Oh ES, Reed NS, Lin FR and Deal JA (2022) Hearing Loss and Cognition: What We Know and Where We Need to Go. Front. Aging Neurosci. 13:769405. doi: 10.3389/fnagi.2021.769405
Received: 02 September 2021; Accepted: 29 October 2021;
Published: 28 February 2022.
Edited by:
Weidong Le, Dalian Medical University, ChinaReviewed by:
Jason Warren, Dementia Research Centre, United KingdomCopyright © 2022 Powell, Oh, Reed, Lin and Deal. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Danielle S. Powell, ZHBvd2VsMzNAamh1LmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.