An Insight Into COVID-19: A 21st Century Disaster and Its Relation to Immunocompetence and Food Antioxidants
 Faisal Siddique1*
Faisal Siddique1*  Rao Zahid Abbas2
Rao Zahid Abbas2  Muhammad Khalid Mansoor3
Muhammad Khalid Mansoor3  Etab Saleh Alghamdi4 Muhammad Saeed5 Muhammad Mazhar Ayaz6 Moazur Rahman7 Muhammad Shahid Mahmood8 Asif Iqbal9 Maida Manzoor8 Asghar Abbas10 Asif Javaid11 Irshad Hussain12
Etab Saleh Alghamdi4 Muhammad Saeed5 Muhammad Mazhar Ayaz6 Moazur Rahman7 Muhammad Shahid Mahmood8 Asif Iqbal9 Maida Manzoor8 Asghar Abbas10 Asif Javaid11 Irshad Hussain12- 1Department of Microbiology, Cholistan University of Veterinary and Animal Sciences, Bahawalpur, Pakistan
- 2Department of Parasitology, University of Agriculture, Faisalabad, Pakistan
- 3Department of Microbiology, The Islamia University of Bahawalpur, Bahawalpur, Pakistan
- 4Department of Food and Nutrition, Faculty of Human Sciences and Design, King Abdul-Aziz University, Jeddah, Saudi Arabia
- 5Department of Poultry Sciences, Cholistan University of Veterinary and Animal Sciences, Bahawalpur, Pakistan
- 6Department of Parasitology, Cholistan University of Veterinary and Animal Sciences, Bahawalpur, Pakistan
- 7School of Biological Sciences, University of the Punjab, Lahore, Pakistan
- 8Institute of Microbiology, University of Agriculture, Faisalabad, Pakistan
- 9Department of Parasitology, Riphah International University, Lahore, Pakistan
- 10Department of Veterinary and Animal Sciences, Muhammad Nawaz Shareef University of Agriculture, Multan, Pakistan
- 11Department of Animal Nutrition, Cholistan University of Veterinary and Animal Sciences, Bahawalpur, Pakistan
- 12Department of Microbiology, University of Veterinary and Animal Sciences, Lahore, Pakistan
Coronavirus Disease 2019 (COVID-19) ranks third in terms of fatal coronavirus diseases threatening public health, coming after SARS-CoV (severe acute respiratory syndrome coronavirus), and MERS-CoV (Middle East respiratory syndrome coronavirus). SARS-CoV-2 (severe acute respiratory syndrome coronavirus type 2) causes COVID-19. On January 30, 2020, the World Health Organization (WHO) announced that the current outbreak of COVID-19 is the sixth global health emergency. As of December 3, 2020, 64 million people worldwide have been affected by this malaise, and the global economy has experienced a loss of more than $1 trillion. SARS-CoV-2 is a positive-sense single-stranded RNA virus belonging to the Betacoronavirus genus. The high nucleotide sequence identity of SARS-CoV-2 with the BatCoV RaTG13 genome has indicated that bats could be the possible host of SARS-CoV-2. SARS-CoV-2 penetrates the host cell via binding its spike protein to the angiotensin-converting enzyme 2 (ACE2) receptor, which is similar to the mechanisms of SARS-CoV and MERS-CoV. COVID-19 can spread from person to person via respiratory droplets and airborne and contaminated fomites. Moreover, it poses a significant risk to smokers, the elderly, immunocompromised people, and those with preexisting comorbidities. Two main approaches are used to control viral infections, namely, vaccination, and biosecurity. Studies to analyze the antigenicity and immunogenicity of SARS-CoV-2 vaccine candidates are underway, and few vaccines may be available in the near future. In the current situation, the Human Biosecurity Emergency (HBE) may be the only way to cope effectively with the novel SARS-CoV-2 strain. Here, we summarize current knowledge on the origin of COVID-19 as well as its epidemiological relationship with humans and animals, genomic resemblance, immunopathogenesis, clinical-laboratory signs, diagnosis, control and prevention, and treatment. Moreover, we discuss the interventional effects of various nutrients on COVID-19 in detail. However, multiple possibilities are explored to fight COVID-19, and the greatest efforts targeted toward finding an effective vaccine in the near future. Furthermore, antioxidants, polyphenols, and flavonoids, both synthetic and natural, could play a crucial role in the fight against COVID-19.
Introduction
Coronaviruses are emerging as a threat to people in the 21st century. They are responsible for high morbidity and mortality rates, especially in the elderly and immunocompromised people. In the last two decades, two human coronaviruses (HCoVs) have been reported to cause mild disease (1). In 2003, SARS-CoV (severe acute respiratory syndrome coronavirus) triggered the first human outbreak in Guangdong Province, China. It affected more than 20 countries worldwide due to international travel (2). A total of 8,098 cases were registered, of which ~916 died during the 2002–2003 SARS-CoV wave (3). At this time, SARS-CoV was the emerging public health infectious outbreak of this century. However, the pandemic ended in 2004, but the estimated global economic loss exceeded $90 billion (4).
After a decade of SARS-CoV infection, the emergence of a new type of coronavirus called MERS-CoV (Middle East respiratory syndrome coronavirus) has challenged the world. Since November 2019, MERS-CoV has affected 2,494 people worldwide, with ~858 deaths (5). Based on molecular and phylogenetic studies, the bats were identified as a natural host of SARS-CoV and MERS-CoV (6).
On 31 December 2019, the third pandemic of a new variant of Betacoronavirus occurred in a seafood market in Wuhan, Hubei, China (7). The three new coronavirus epidemics first emerged among the Chinese population, and this is probably due to their traditional eating habits of wild animals such as bats, snakes, foxes, and dogs (8). At the end of February 2020, this novel viral strain was named 2019-nCoV and its disease COVID-19 by the World Health Organization (WHO). The International Committee on Taxonomy of Viruses (ICTV) has declared that the virus has been classified as SARS-CoV-2 (9, 10).
This catastrophe was linked to vast markets of animals and seafood, and research continues to establish the origins of this infectious disease. The primary investigation found that SARS-CoV-2 has a close homology to the amino acid sequence of SARS-CoV and binds to the same receptor (ACE2) as SARS-CoV and MERS-CoV. To date, more than 200 countries/regions have been affected by the COVID-19 pandemic. As of December 3, 2020, ~64 million confirmed cases had been reported, including 1.5 million worldwide deaths due to the COVID-19 pandemic.
On January 30, 2020, the WHO declared that the COVID-19 pandemic was the sixth global public health emergency, preceded by influenza (H1N1) in 2009; Ebola hemorrhagic fever in West Africa in 2014 and 2016; poliomyelitis in 2014; Zika virus outbreak in 2016; and Ebola epidemics in the Democratic Republic of the Congo in 2019 (11, 12). The disease is spread to healthy individuals via respiratory droplets, contaminated mites, and airborne methods. Furthermore, cooperation among people employed in the health sector, physicians, medical personnel, and private and government institutions is required to stop its spread around the world (13).
Epidemiology OF SARS-CoV-2
At the end of December 2019, the first case of COVID-19 was reported in Wuhan, China. The COVID-19 pandemic has changed people's habits and lives worldwide, and this includes restrictions on travel and tourism. Many countries have implemented a policy of lockdown to limit movements of citizens from one region to another within the country (4).
Preliminary analyses have shown that the origin of the new virus strain is linked to the Chinese market for seafood. SARS-CoV-2 crossed the species boundary and was transmitted from animals to humans during November or December 2019, and clinical cases were observed almost at the end of December (14). Chinese researchers have rapidly isolated SARS-CoV-2 from a patient with pneumonia. This new virus's genome sequence is close to that of SARS-CoV (80%) and bats (96%). Subsequently, several studies have shown that the bat could be the potential host reservoir of SARS-CoV-2, although bats are not sold in this seafood market (15, 16). To date, there is no definitive phylogenetic proof that SARS-CoV-2 has appeared in the Chinese seafood market (17).
Based on the phylogenetic and proteomic analysis, potential intermediate hosts of SARS-CoV-2 include snakes, turtles, and pangolins (18). SARS-CoV-2 is primarily transmitted to humans through respiratory droplets of people infected with SARS-CoV-2 while coughing, sneezing, and talking. These heavy water droplets are suspended in the atmosphere and rapidly fall to the ground or onto solid objects. If people touch the hands, mouths, or tainted clothes or shoes of an infected person, they are more likely to catch COVID-19 (12).
Moreover, the transmission of SARS-CoV-2 occurs through airborne droplets in an indoor environment, extended access to respiratory debris, and improper ventilation. Airborne spread is distinguished from droplet spread based on the size of expired droplets of the infected person: if the particle size is >5 μm, it is a droplet; if the particle size is <5 μm, it is an aerosol. The SARS-CoV-2 reside within droplet nuclei. SARS-CoV-2 is stable and viable in aerosols for several hours compared to SARS-CoV and can be spread over distances >1 m to healthy individuals. Few research reports have documented the airborne transmission of COVID-19, which might cause a possible aerosolized spread of the disease (19–21). Airborne spread of SARS-CoV-2 has been observed in cats and ferrets. Moreover, a close relationship between air pollutants, for example, PM2.5, PM10, NO2, and O, and COVID-19 has been observed. SARS-CoV-2 can bind to atmospheric contaminants and can spread through the air. Several studies have shown promising results in isolating the SARS-CoV-2 genome in airborne samples using a polymerase chain reaction assay (22, 23). The epidemiological comparison of different biological features among various important coronaviruses (SARS-CoV, MERS-CoV, and SARS-CoV-2) is demonstrated in Table 1.
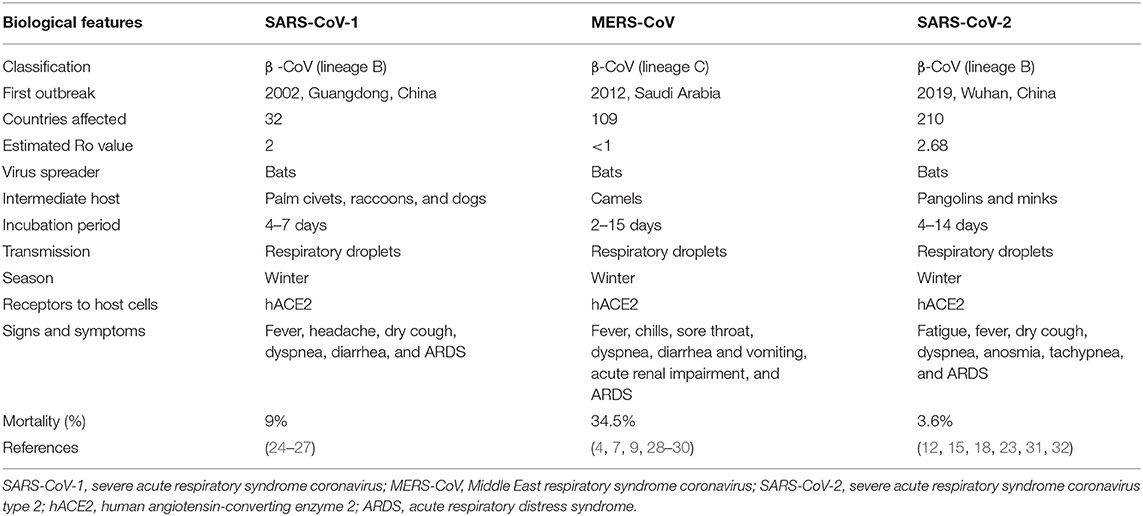
Table 1. Epidemiological comparison of human coronaviruses.
Smokers, people aged >60 years, doctors, paramedical staff, immunocompromised patients, children (<5 years old), patients with chronic lung and heart diseases, and family members (i.e., relatives, mother, father, wife, and children) and friends of infected patients are at significant risk of COVID-19 (33).
Evidence from the global epidemic suggests that comorbidities, such as hypertension, diabetes, and obesity, are the leading causes of death in patients with COVID-19 (34, 35). Hypertension is the highest preexisting comorbidity among patients with COVID-19 and is the leading cause of death (36). Patients with hypertension are usually treated with renin-angiotensin system inhibitors (ACEIs) and angiotensin receptor blockers (ARBs). Since ACEIs and ARBs can significantly increase ACE2 expression, several researchers speculate that they are correlated with an increased risk of COVID-19. Moreover, renin-angiotensin inhibitors are commonly used to treat patients with cardiovascular diseases who have an increased mortality risk during COVID-19 epidemics (31). Diabetes is the third most common potential comorbidity among patients with COVID-19. Individuals with diabetes are more vulnerable to diseases and are at high risk of developing multiple comorbidities, such as cardiovascular diseases and hypertension (37). In addition, the critical risk factors for COVID-19 infection are preexisting respiratory conditions, such as asthma and chronic obstructive pulmonary disease, and chronic liver disease (35). The average incubation period of SARS-CoV-2 is 4–14 days (38).
Epidemiological Relationship Between COVID-19 and Animals
The Coronaviridae family affects various types of animals, such as poultry, goats, dogs, cats, horses, and fish, and human beings (39). In most cases, their infections are subclinical or asymptomatic (40). However, enteritis has been observed in cattle and horses; respiratory illness has been seen in dogs, cats, and poultry; and asymptomatic to symptomatic respiratory infections have been detected in humans (32, 41). Coronaviruses induce clinical illness in laboratory animals such as mice, rabbits, rats, and guinea pigs. Among the coronaviruses, bovine coronaviruses, SARS-CoV, MERS-CoV, HCoV-NL63, and SARS-CoV-2 have zoonotic origins (42). Zoonotic coronaviruses, especially SARS-CoV, MERS-CoV, and SARS-CoV-2, can cross the species barrier due to genetic recombination in the receptor-binding domain (43). COVID-19 has spread worldwide due to the instability of the RNA replicase enzyme, which is incapable of proofreading activity, and an increased mutation rate in the receptor-binding domain of the spike protein gene (35). The genetic reshuffling of the spike protein gene can increase the spread, virulence, and host species from animals to humans (44).
Preliminary research has shown that the origin of the first case of COVID-19 was observed in the seafood market in Wuhan, Hubei, China. Restaurants in this market offer all sorts of wild animal meat, such as broilers, snakes, tortoises, bats, pangolins, marmots, and hedgehogs (24). The initial thought was that the SARS-CoV-2 virus had been transmitted from animals to humans through the seafood industry. This hypothesis was reinforced by the previous zoonotic coronaviruses such as SARS-CoV and MERS-CoV (45). MERS-CoV was transmitted through nasal secretions, feces, and milk (46). The literature has shown that certain bat-origin coronaviruses, such as SARS-CoV and MERS-CoV, have infected humans. As a result, scientists predicted the role of bats in the emergence and circulation of the recent COVID-19 epidemic (47, 48). Recently, a Chinese researcher reported that the genomic structure of SARS-CoV-2 was identical to that of SARS-CoV (80%) and horseshoe bat (96%) and indicated that the bat may be the potential host reservoir of SARS-CoV-2. Hence, bats are responsible for transmitting zoonotic diseases to humans (49). The spike protein of SARS-CoV-2 is similar to that of the pangolin coronavirus. Therefore, bats and pangolins are considered to be sources of SARS-CoV-2 in humans (25).
To date, two cases of COVID-19 have been reported in two separate breeds of dogs, that is, Pomeranian, and German Shepherd (50). A Pomeranian dog was regarded to be a possible intermediate host due to multiple swaps in the dog's ACE2 receptor after its owner was found to be COVID-19 positive, indicating that SARS-CoV-2 had crossed the species barrier (17). In Hong Kong, two German shepherd dogs were also found to be positive for COVID-19 out of 15 dogs tested. The genomic sequences of SARS-CoV-2 isolated from both dogs were similar to those found in human cases, suggesting human-to-dog transmission (28).
The first case of cat infection with COVID-19 was registered at the end of March 2019. The history of these infections in dogs and cats has indicated that their owners have been infected with COVID-19. They both developed immunoglobulins that fight infection. These findings may suggest human-to-animal transmission of COVID-19 (29). Other countries such as Belgium, France, Germany, Russia, and the United States have also documented cases of COVID-19 in cats. Based on these observations and other laboratory research, it can be concluded that these two companion animals are prone to SARS-CoV-2 (30). Cats are sensitive and can spread the disease to other naive cats, whereas dogs are less resistant to infection (23). Laboratory animals, particularly golden Syrian hamsters, have been infected with SARS-CoV-2. High viral loads in the upper and lower respiratory tracts were observed within the first week of infection (51). Moreover, ferrets are highly susceptible to SARS-CoV-2 and effectively transmit SARS-CoV-2 to other naive ferrets via direct, indirect, and airborne transmission. SARS-CoV-2 replicates in the upper respiratory tract of ferrets, making them an acceptable candidate animal model for the evaluation of antiviral drugs or vaccine candidates for COVID-19 (52).
The SARS-CoV-2 outbreak has been reported in four mink farms in the Netherlands. Histopathological results showed that minks died of pneumonia caused by SARS-CoV-2, verified by reverse transcription-polymerase chain reaction (RT-PCR) examination. However, animal transmission and minimal accidental spillover from humans have been observed. The genomic sequence cluster of SARS-CoV-2 was similar to that of minks with seven nucleotide variations. The molecular findings have confirmed its zoonotic importance (53).
Domestic animals like pigs, camels, goats, donkeys, horses, sheep, and poultry are not found to be receptive to SARS-CoV-2 (22, 23). Wild animals like tigers, lions, Egyptian fruit bats, African green monkeys, and rhesus monkeys have been reported to be susceptible to COVID-19 (42). A recent study has shown that Nadia, a 4-year-old tiger, exhibited respiratory symptoms such as coughing and sneezing on March 27, 2020, in the Bronx Zoo in New York City. Samples were obtained and a COVID-19 positive test was found (54). Later on, no confirmatory evidence was obtained suggesting that canines can acquire COVID-19 disease or transfer the virus to humans (55).
Genomic Categorization of Coronaviruses (COVs)
Coronaviruses are a set of viruses that cause infections in humans and feathered animals. According to ICTV, coronaviruses belong to the Riboviria realm, Nidovirales order, Coronaviridae family, Orthocoronavirinae subfamily, and Betacoronavirus genus (56). They are comprised of an encapsulated lipid bilayer and a non-segmented RNA genome. They are the largest viruses among RNA viruses, ~34 kb in size (57). The electron micrograph of the coronavirus has a spike-like or stick-like surface protein close to the crown. The word “corona” is derived from the Latin word “corona,” meaning crown (58).
Coronaviruses are classified into four genera, alpha, beta, gamma, and delta coronaviruses, based on their protein sequences. Most human coronaviruses belong to the Betacoronavirus genus that is further subcategorized into lineages A, B, C, and D (59). Bats and rodents serve as intermediate hosts for alpha- and betacoronaviruses, whereas birds act as intermediate hosts for gamma- and deltacoronaviruses. Coronaviruses have crossed their biological limits and have emerged as new human pathogens, such as SARS-CoV-2. To date, six Betacoronaviruses have been isolated and identified globally as follows: HCoV-HKU1, HCoV-OC43, SARS-CoV, MERS-CoV, HCoV-229E, and SARS-CoV-2 (60).
High mortality rates have been seen in zoonotic SARS-CoV and MERS epidemics over the last two decades, whereas other coronavirus classifications are typically associated with negligible upper respiratory tract disease. However, they can lead to complex diseases, if they affected an immunocompromised person (26).
The genetic sequence of SARS-CoV-2 belongs to the lineage B betacoronaviruses that is similar to more than 90% of the bat and pangolin coronavirus genomes. Bats are suspected to be the natural carriers of the novel coronavirus COVID-19 based on complete virus genome sequences and phylogenetic analysis. SARS-CoV-2 is known to use the same receptors as SARS-CoV, such as angiotensin-converting enzyme 2, to infect humans (61). The SARS-CoV-2 genetic material serves as an infectious agent containing a 5′-methylated cap and a 3′-polyadenylated tail. The complete genome sequence of SARS-CoV-2 contains 29,811 nucleotides consisting of 8,903, 5,482, 5,852, and 9,574 adenosines, cytosines, guanines, and thymines, respectively (27).
SARS-CoV-2 consists of different structural proteins, including spike (S), membrane (M), envelope (E), and nucleoproteins (N). Petal or club-shaped S proteins are tightly packed membrane glycoproteins that help bind viruses to host cells (62, 63). The pentameric small-integer E protein is involved in the assembly and pathogenesis of viruses (64). The integral M protein of type III is connected to the matrix formation. The N protein leads to the encapsidation of the genome, protein, and RNA synthesis. All these structural proteins (S, M, E, and N) of SARS-CoV-2 can act as antigens to human cells, stimulate the development of antibodies, and increase the immune response of T cells (16).
SARS-CoV-2 Pathogenesis
SARS-CoV-2 virulence begins after the viral entry through inhalation of respiratory and airborne droplets or contact with infected fomites. The pathogenesis of SARS-CoV-2 depends on various factors, such as age, sex, preexisting comorbidities, immune status, nutritional status, and smoking. Human respiratory epithelial cells contain receptors called hACE2 (human angiotensin-converting enzyme 2) (65). This enzyme lowers blood pressure by converting angiotensin II to angiotensin 1–7. Moreover, other human coronaviruses, e.g., SARS-CoV, MERS-CoV, and HCoV-NL63, bind to ACE2 receptors on host cells (66).
The SARS-CoV-2 S protein is bound to the hACE2 receptor of the host cells. This attachment is required for the initiation of pathogenesis (67, 68). S protein is further subdivided into two active subunits, S1 and S2. A similar pattern of S protein subdivision has been reported for MERS-CoV infection (69, 70). The replication of the SARS-CoV-2 genome occurred in the cytoplasm. The virus produces various structural and non-structural proteins using the host cell's machinery. Infectious viruses are released through host cell lysis (71).
Immune Response of Host vs. SARS-CoV-2
The SARS-CoV-2 antigen is recognized by different antigens-presenting cells, for example, alveolar macrophages and monocytes that patrol the epithelial cells of the respiratory tract. Virus-specific cytotoxic T lymphocytes recognize these antigenic peptides by means of MHC (major histocompatibility complex) molecules. Pro-inflammatory cytokines, e.g., IL-10, IL-2, TNF-α, IL-10, G-CSF, and MCP-1, were observed during infection with SARS-CoV-2 (72).
The high level of these inflammatory cytokines is known as the cytokine storm, and it has an essential role in the determination of SARS-CoV-2 virulence. Similar findings were documented during SARS-CoV and MERS-CoV infections (73).
This cytokine storm can lead to life-threatening complications, such as developing hypoxic conditions, ARDS (acute respiratory distress syndrome), breathlessness, pneumonia, heart failure, and eventually death. ARDS is a common cause of death in SARS-CoV, MERS-CoV, and SARS-CoV-2 infections. However, little information is available about cytokine storms, and the detailed immune mechanism of SARS-CoV-2 infection is still unknown (74).
Antigen-presenting cells also activate virus-specific B and T cells. The concentration of CD4+ and CD8+ T has decreased significantly in the peripheral blood of infected individuals with COVID-19. Similar findings have been documented in SARS-CoV and MERS-CoV infections (75). Typical patterns of immunoglobulin development, e.g., IgM and IgG, have been observed during acute SARS-CoV infections. Immunoglobulin production starts after 3 days of infection and reaches an optimum level on day 14 (76). These findings can provide useful evidence for vaccine preparation to cure SARS-CoV-2. Coronaviruses, particularly SARS-CoV and MERS-CoV, use a number of mechanisms to modulate host immune response, including the development of double-membrane vesicles that inhibit INF-I pathways and affect different antigen-presenting cells (77).
Clinical-Laboratory Cautions of SARS-CoV-2
Clinical signs of COVID-19 include respiratory tract, digestive tract, and generalized symptoms of the body. The clinical indication of COVID-19 disease occurs 6 days after incubation. The most common signs and symptoms of COVID-19 infection are as follows: fever, 99%; dyspnea, 80%; fatigue, 70%; dry cough and anosmia, 59.4% (67, 78). No clinical signs were seen in neonates (78); however, a newborn was tested positive for SARS-CoV-2 at Tongji Hospital, Wuhan, China. Neonates can be infected through perinatal or uterine pathways (79). Asymptomatic carriers have been found among individuals infected with SARS-CoV-2 and clinical symptoms such as cough, fever, and fatigue have not been observed. These carriers have the capacity to shed the virus for up to 21 days and are a possible source of disease transmission to healthy individuals (4). Serious signs and symptoms of COVID-19 are primarily seen in elderly people with cardiovascular disease, hypertension, asthma, and diabetes and those with compromised immune function (80). The SARS-CoV-2 RNA was isolated from stool samples in patients, suggesting that it may be transmitted via the fecal-oral pathway if the virus was intact (81).
The clinical signs and symptoms of COVID-19 contagion are classified based on the severity of infection, which would depend on various risk factors such as age, smoking habit, concurrent bacterial and viral infections, and immune status. The first category is mild illness (81%): patients experience mild symptoms, such as slight fever, nasal congestion, cough, headache, rhinorrhea, nausea, vomiting, muscle pain, diarrhea, abdominal pain, sore throat, loss of taste, and smell; however, they do not suffer from shortness of breath or trouble breathing and have a normal radiographic image (76). Mild diseases are typically managed outside the hospital (82). The second category is a moderate form of the disease in which patients show respiratory symptoms of dyspnea, dry cough, wheezing, and tachypnea (RR >30/min) (83). The third category is the severe form of the disease in which patients presented with sepsis, kidney injury, liver damage, intense pneumonia, ARDS, respiratory rate >30/min, PaO2/FiO2 < 300, and SpO2 ≤ 93%, with a moderate or absent fever (79, 82). The severe or critical form of COVID-19 causes ARDS that could be responsible for worsening respiratory failure. Two forms of ARDS are clinically identified in patients based on PaO2/FiO2 values as follows: moderate form, PaO2/FiO2 values = 100 mmHg−200 mmHg; extreme form, PaO2/FiO2 values ≤ 100 mmHg. Moreover, ARDS has been diagnosed with computed tomography (CT) scanning in which we studied crazy paving, consolidation, ground-glass opacity, and peripheral disease distribution (84).
Currently, ~15% of people require hospitalization (usually for mild to extreme pneumonia), whereas the other 5% have serious illness and need further help. Patients with COVID-19 with preexisting comorbidities have higher mortality rates. These comorbidities include cardiovascular diseases, hypertension, diabetes, and tumor problems. Lower mortality rates have been observed in patients with no comorbidities (35, 36). Laboratory observations of COVID-19 infection detected increased ALT (alanine transaminase), creatine kinase, lactate dehydrogenase, C-reactive protein, plasma interleukins (IL-7, TNFa, IL-2, IL-10, and MCPI), erythrocyte sedimentation rate, blood urea level, and decreased CD4 and CD8 cells (85, 86).
Diagnosis of SARS-CoV-2
The confirmatory diagnosis of COVID-19 is primarily dependent on history (traveling, age, concurrent infection, etc.), signs and symptoms, and laboratory diagnostic techniques (87). Two types of laboratory diagnostic techniques are used in the diagnosis of SARS-CoV-2. The first is a molecular diagnostic technique, which can recognize part of the viral genome in respiratory specimens. The second is serology or antibody testing, which can identify unique SARS-CoV-2 antibodies in serum samples. Symptomatic or asymptomatic carriers can be identified by molecular tests, as these tests are highly sensitive in order to avoid false-negative results. On the other hand, serological tests can detect the SARS-CoV-2 antigen in patients, as they are specific to the exclusion of false-positive findings (88).
According to WHO, throat swab, nasopharyngeal swab, and samples of sputum, urine, and serum should be collected from the suspected person. If a person had a positive test result, the test should be repeated one more time to double-check. A negative result with robust clinical manifestation should also be repeated (85). Samples such as nasopharyngeal swabs and sputum were collected from infected patients for virus isolation (87). Moreover, the samples have been inoculated into the kidney fibroblasts (Vero cells) of the African green monkey. The electron micrograph of the supernatant has verified the existence of SARS-CoV-2. Real-time RT-PCR is commonly used for an early diagnosis of atypical pneumonia caused by SARS-CoV-2. The commercially available RT-PCR diagnostics for COVID-19 are either one-step or two-step RT-PCR techniques. The main features of the One-Step RT-PCR assay are high detection speed, minimal cross-contamination, being reproducible, low human error rate. On the other hand, the two-step RT-PCR technique is versatile and tunable with high sensitivity and low detection (89, 90).
Many commercially available RT-PCR-based kits have been used worldwide for COVID-19 as follows: Abbott RealTime SARS-CoV-2, Roche's cobas® SARS-CoV-2 Test, Cepheid's Xpert® Xpress SARS-CoV-2, DiaSorin's Simplexa™ COVID-19 Direct RT-PCR kit, and Hologic's Panther Fusion® SARS-CoV-2 (91). Some alternative molecular diagnostic tools, such as LAMP and CRISPR, are used to diagnose COVID-19. The FDA approved the Atila BioSystems iAMP COVID-19 Detection Kit and the Sherlock™ CRISPR SARS-CoV-2 kit for the LAMP and CRISPR tests, respectively. Both kits showed a 100% sensitivity (89). In addition, the full genome sequence and phylogenetic analysis of the virus isolate showed that the isolate had more than 99.9% sequencing identification with other publicly available SARS-CoV-2 genomes (92). Lateral flow immunoassay (LFIA) and enzyme-linked immunosorbent assay (ELISA) are two serologically important tests widely used for the diagnosis of COVID-19 (90). IgM and IgG antibodies are identified by various serological tests. Serological tests can offer false-negative and false-positive results due to cross-contamination of antibodies to other human coronaviruses such as SARS-CoV, MERS-CoV, HKU1, 229E, and NL63. LFIAs are a simple, quick (5–20 min), long-use (up to 18 months), and relatively inexpensive method for detecting COVID-19 antibodies. However, some drawbacks of these tests have been found in positive COVID-19 cases, such as an increased risk of an operator getting infected and false-negative outcomes (93). In many countries/regions, including Spain, Taiwan, Switzerland, Denmark, China, France, Brazil, the United States, South Korea, Indiana, Pakistan, and Malaysia, seroprevalence rates have been reported in COVID-19 hot spots. Among them, Spain has the highest prevalence rate, followed by other countries. However, over time, the rate may increase or decrease. Periodic surveillance of seroprevalence at each site should be determined to ascertain the epidemiology of COVID-19 (94).
Control and Prevention of SARS-CoV-2
COVID-19 is an infectious disease that is spread from person to person. Two approaches are used to monitor the infection of COVID-19, namely, Human Biosecurity Emergency (HBE) and vaccination (95). HBE can be used to monitor the latest strain on a global scale. HBE is declared to lock a specific infected area by preventing the movement of any person or object. To date, the city of COVID-19 birth, Wuhan, China, successfully combated the infection after a 76-days complete lockdown. During lockdown, schools, colleges, universities, public and private transport, malls, grocery shops, and borders were closed and people were confined to their homes (96). For the general public, the risk of infection can be minimized by the use of Infection Prevention and Control (IPC) strategies, such as the use of face masks, washing hands with soap and sanitizer for 20 s, maintaining an acceptable social distance (1 m or 3 feet), and self-isolation if you feel sick (19). People with low immunity are advised to avoid group gatherings, close contact with wild and domestic birds and animals, and rubbing their noses, mouths, and eyes with dirty hands (39). Doctors and paramedical staff must wear FFP3 masks or N95 masks, eye goggles, medical gloves, and protective gowns during the care of infected persons (97, 98).
Till now, no specific antiviral drug or vaccine is available to treat COVID-19 (99). Strict quarantine and various therapeutic interventions help control COVID-19 globally, such as the use of convalescent plasma, antiviral drugs, monoclonal antibodies, herbal medicine (mAbs), neutralizing antibodies, antibiotics, nutritional supplements, fluid management, oxygen therapy, and intravenous immunoglobulins (100–103).
Convalescent plasma obtained from patients recovering from COVID-19 provides rapid immunity to infected individuals. This technique offers optimal healing outcomes and can be used as a prophylaxis in high-risk immunocompromised patients and healthcare staff such as nurses, physicians, and lab technicians. Previously, this approach was used worldwide for the SARS-CoV and MERS-CoV epidemics (104). Convalescent plasma with monoclonal antibodies is now commercially available. However, passive immunity via convalescent plasma has resulted in rapid, short-term immunity in infected patients. Therefore, vaccine production is a prerequisite for long-term and stable immunity for infected individuals. Maximum protective results were achieved on day 5 of COVID-19 infection following the use of convalescent plasma. The literature revealed that patients weighing 50–80 kg were given two plasma units (200–250 mL each). However, in extreme cases, a dose of 500 ml was injected intravenously after 12 h (105, 106). Monoclonal antibodies, given intravenously, may have a crucial role in the prevention and control of COVID-19. Furthermore, monoclonal antibodies reduced inflammation by inhibiting FcR stimulation. Nevertheless, these therapies have some vulnerabilities such as abnormal reactions, short-term safety, toxins, and dissemination of causative agents (107, 108).
Traditional Chinese Medicine (TCM) plays an integral role in reducing COVID-19 symptoms through various mechanisms, such as lowering hormone doses, decreasing fever symptoms, mitigating complications, reducing glucocorticoid and antiviral doses, stabilizing oxygen, repairing T lymphocytes and antibodies, maintaining normal liver function, and reducing inflammation (102). Two natural products, such as baicalin and baicalein, have been extracted from TCM, which inhibit the growth of SARS-CoV-2 in vitro (109, 110). Cinchona is a medicinal plant that produces quinine. Studies have reported that choloquinine has DNA-interlacing properties and will become an ideal candidate for developing an effective drug for treating of SARS-CoV-2 in the future. In addition, two other important alkaloids, such as palmatine and chelidonine, inhibit the replication of RNA viruses, which are considered to be an attractive antiviral drug against COVID-19 (111). Therapeutic studies on various antiviral drugs, such as oseltamivir, remdesivir, hydroxychloroquine, and azithromycin, have been conducted based on previous investigations on SARS-CoV-2. However, there is no clear evidence that antivirals can automatically minimize SARS-CoV-2 clinical reactions (81). Immunomodulatory and therapeutic effects of hydroxychloroquine against COVID-19 infection have been documented, indicating that it stimulates the growth of macrophages and reduces the risk of cytokine storms, IL-1, IL-6, and prostaglandins. In vitro experiments have demonstrated synergistic effects of hydroxychloroquine and azithromycin on COVID-19 (112, 113).
Remdesivir is a nucleoside analog that has been successfully used in patients with COVID-19 in China. The outcomes revealed a decrease in mortality, suggesting that it is an important potential therapeutic alternative against COVID-19. The use of recombinant human ACE2 and recombinant interferon would be a therapeutic choice for the potential treatment of COVID-19 (114).
The combination of Lopinavir, Arbidol, and Shufeng Jiedu Capsule has strengthened therapeutic barriers in patients with COVID-19 (115). The current control of COVID-19 is mainly supportive treatment (116). ARDS and cytokine storm are the leading causes of death in patients with COVID-19. However, high dose corticosteroids, especially dexamethasone and cyclosporine A, reduced or cured ARDS that severely affects lung tissues. Therefore, low-/medium-dose corticosteroids are suggested to be used in patients with COVID-19 (27). Cytokine storm accompanied by hyper-inflammation during COVID-19 is a more focused strategy and an efficient treatment pathway. Tocilizumab (Rochi®) and Anakinra have been used in managing patients with COVID-19 in China for treating cytokine waves (102). Recently, a new hypothesis for treating cytokine storms by inhibiting Janus kinases (JAK) has been suggested. These small molecules can activate the IL-6 receptor to induce inflammation. Research is underway to assess the efficacy and immunity of JAK inhibitors in severe cases of COVID-19 infection (114).
Probiotics are living microorganisms that are especially used to improve the immunity of humans. Moreover, probiotics are believed to be a possible treatment for COVID-19 by increasing immunity. However, no current clinical evidence exists for the use of probiotics during COVID-19 infection. The National Health Commission of China and the National Administration of Traditional Chinese Medicine have agreed to use probiotics in treating COVID-19 (117). Probiotic supplements help combat COVID-19 by reducing cytokine storm activation and modulating intestinal microbiota damage. It is possible that the basic principle of preventive use of probiotics in SARS-CoV2 infection is related to their ability to maintain and repair health status in the gut-associated lymphoid tissue, which prevents the entrance of the virus into intestinal cells. Large clinical trials are warranted to address these burning issues and identify the most useful and safe environment for the administration of probiotics. In fact, three registered trials have evaluated the use of probiotics, such as Lactobacillus coryniformis, in patients with COVID-19 (118).
Safe and efficient vaccines are required to create a protective immune response during the COVID-19 pandemic. Numerous methods have been introduced for the preparation of COVID-19 vaccines, including inactive, live attenuated, viral vector, replicated and non-replicated, Spike protein and peptide-based, and nucleic acid techniques (119). Research on the ideal candidate for SARS-CoV-2 is important for the preparation of vaccines and is underway. The ideal characteristics for COVID-19 vaccine include the following: excellent protection for healthy adults, pregnant women, babies, the elderly, and immunocompromised individuals; minimal adverse reactions, contraindications, and post-immunization non-provoking immunopathology; prompt long-lasting protective humoral and cell-mediated responses within 2 weeks using a single dose; being easily mass-produced; and being stable at 2 weeks. A total of 167 vaccine candidates are being tested worldwide. Among these, 29 are under clinical observation and 138 are under preclinical trials until 13 August 2020 (120). The first vaccine against COVID-19 was developed and approved for use only by the Chinese army (27).
COVID-19 mRNA-based vaccines are being developed, such as Moderna (NASDAQ: MRNA), chimpanzee adenovirus vector vaccine, and INO-4800, and clinical trials will soon be conducted (119). ChAdOx1 nCoV-19 vaccine has been used in treating COVID-19 positive patients and inducing protection against the disease; its efficacy and immunogenicity will be investigated in human controls. Data showed that the ChAdOx1 nCoV-19 vaccine exhibited an appropriate safety profile and improved antibody and cellular immune responses. These findings endorse a large-scale assessment of this candidate vaccine in the ongoing phase 3 trial program (120).
S protein-based vaccines are more potent than any other type. They regulate the COVID-19 pandemic in several ways, such as preventing the viral entry and attachment to ACE2 receptors and activating both humoral and cellular immune cells. They are delivered through aerosol or oral routes in individuals. INOVIO Pharmaceuticals has prepared a plasmid-based DNA vaccine targeting the SARS-CoV-2 S protein (INO-4800). This vaccine was administered intradermally. INO-4800 developed neutralizing antibodies in mice and guinea pigs with stimulating cell-mediated and humoral immune responses. Protection (94%) and tolerability were observed in phase 1 volunteers (27). Interestingly, the BCG vaccine has been shown to be safe and effective against COVID-19 in countries with a uniform BCG policy. In addition, the formalin-inactivated Pasteurella multocida vaccine is believed to be effective against COVID-19 during early infection. Recently, Novavax® has produced a virus-like particle (VLP) vaccine against COVID-19. The VLP vaccine can be obtained from plants and contains Matrix-M adjuvants targeting the SARS-CoV-2 S protein (121). Potential pitfalls when developing COVID-19 vaccines arise, such as structural homology between the receptor-binding domain of SARS-CoV-2 and SARS-CoV and cross-reactivity of antibodies of various coronaviruses due to antibody-dependent enhancement mechanism (122). Therefore, extra caution should be taken before making a final decision on any vaccine in the market. Additionally, the comprehensive infrastructure and financial resources needed for this project are key issues and requirements that need to be legitimately addressed. However, COVID-19 vaccines will be available in early 2021 due to emergent conditions worldwide and commercial vaccines may take 10 years until reaching final production (121).
Interventional Effects of Various Nutrients on COVID-19
Presently, treatments or vaccines against COVID-19 are available. Nonetheless, many scientific studies have been published that highlight the general treatments for viral infections (as detailed above). Among various strategies to fight COVID-19, the use of micronutrients has shown promising results by improving immunity, particularly vitamins A, C, D, E, and B complex (especially B2, B3, B6, and B12) (123, 124).
Vitamin C has antioxidant potential, and its deficiency is traditionally linked with pneumonia. Moreover, vitamin C has been shown to have a therapeutic role during COVID-19 infection by reducing inflammatory responses, optimizing the opsonization process and the immune system, and maintaining vascular consistency (125). On March 23, 2020, Dr. Tom Frieden, former director of the Center for Disease Control and Prevention (CDC), suggested the use of vitamin D to control the outbreak of COVID-19. Several researchers identified the therapeutic effects of vitamin D on viral infections through several mechanisms, such as producing cathelicidins that have a direct antiviral effect on enveloped and naked viruses, reducing the development of pro-inflammatory Th1 cytokines, namely, TNF alpha, interferon Y, and IL-2, and increasing development of glutathione to regulate COVID-19 infection (126).
According to the literature, the use of vitamin B can be helpful in the early stages of COVID-19 management. Thiamine (vitamin B1) has the potential to enhance the immune system and minimize preexisting conditions such as diabetes, hypertension, kidney disease, cancer, and neurodegenerative disorders. Niacin (vitamin B3) and pyridoxine (vitamin B6) have immunomodulatory effects that limit the production of cytokines, such as IL-6 and TNF alpha, which help regulate cytokine storms in patients with COVID-19. Recently, folic acid (vitamin B9) was found to prevent SARS-CoV-2 S protein from binding to host cells. However, further research is warranted to determine if high doses of vitamin B will help in treating patients with COVID-19 (127). In a study investigating the mechanisms of action of minerals, Zhang and Liu (97) have reported that the suitable consumption of some minerals such as iron, selenium, and zinc can have effects not only on COVID-19 itself but also on coronaviruses-related symptoms, such as diarrhea and lower respiratory tract infection (128); the same results were observed for macronutrients, such as omega-3 fatty acids (129).
Numerous medical studies have reported the significant role of antioxidants in protecting lung cells against viruses and bacteria (130). Not only in coronavirus infections but also in many other infections, the balance between antioxidants (redox balance) and oxidants is altered with serious consequences (131). Viral infection leads to a surge in the intrapulmonary oxidative burden. The pathophysiological mechanisms by which free radicals lead to nitrative, oxidative, carbonyl, and endoplasmic reticulum stresses trigger lung inflammation and an altered lung immune response. In this scheme, dietary antioxidants can play a decisive role in fighting lung oxidative stress. Similarly, positive effects for the administration of probiotics and prebiotics have been reported since an imbalance in the intestinal microbiota was detected in patients with COVID-19 (132).
Nutritional interventions between related functions and the target of virus have been conducted worldwide. Moreover, the capacity for inflammatory cytokine release of nutrient-derived bioactive compounds has been demonstrated (133, 134). The release of inflammatory cytokines was suppressed by the administration of different plant-derived polyphenols to in vitro cultured immune cells (135). In particular, bioactive components such as flavonoids and polyphenols can act as immune modulators and inflammatory mediators and have a protective effect against lung infections. Among polyphenols, epigallocatechin 3 gallate (EGCG) is the most vigorous ingredient in green tea and exhibits antiviral, antibacterial, anticancer, antioxidative, and chemopreventive activities (136). Lately, some scientific studies have focused on the protective effects of EGCG against lung diseases such as pneumonia, chronic obstructive pulmonary disease, and asthma. Furthermore, EGCG can invade and suppress inflammation in the lungs of asthma rats. Furthermore, flavonoids may be used to lessen lung injury in mice, and they have been reported to restrain the influenza virus (129). The process to detect, prevent, and treat the disease should address the decrease in the inflammatory response and avoid the excessive postinflammatory immune cutoff, seen in such patients and defined as a compensatory response (137). Several clinical trials have shown that the curcumin spice can possibly have positive effects against COVID-19 disease via inflecting different molecular targets that play a role in the attachment and internalization of SARS-CoV-2 in many organs, including the liver, kidneys, and cardiovascular system. This spice could also modify cellular signaling pathways such as apoptosis, RNA replication, and inflammation. Moreover, it can block the combined pathways of pulmonary fibrosis and edema in COVID-19 disease. Numerous clinical trials have demonstrated that the problem regarding the curcumin bioavailability can be addressed by administering a high amount of concentration within non-toxic limits. Curcumin can be extremely efficient as an adjunct in reversing the fatal cytokine storm in dangerous cases of COVID-19. It is also interesting to report that a recent review revealed the potential impact of phytogenic plants as protective agents in both animals and humans (53, 134, 138, 139).
Conclusions
The COVID-19 pandemic, originating in Wuhan, China, and reckless behavior worldwide have posed a significant risk to the overall population, specifically the elderly, immunocompromised individuals, and healthcare staff. So far, this virus's zoonotic spread is not confirmed; however, the phylogenetic analysis showed that bats are the primary reservoir host. Human-to-human transmission should be controlled by adopting aggressive control measures such as disinfection of living places, high standards of personal hygiene, social distancing by the community, and lockdown of the virus-prevalent areas since effective preventive strategies such as antiviral drugs and vaccinations are currently unavailable. To date, the Chinese are the only nation worldwide that have successfully recovered from COVID-19 by implementing strict HBE policies in terms of lockdown. Therefore, the WHO, CDC, and international public health authorities should continue to observe the disease status globally with rapid response systems. Consequently, the longer we face this nightmare, the better we can respond.
Author Contributions
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Bonilla-Aldana DK, Dhama K, Rodriguez-Morales AJ. Revisiting the one health approach in the context of COVID-19: a look into the ecology of this emerging disease. Adv Anim Vet Sci. (2020) 8:234–7. doi: 10.17582/journal.aavs/2020/8.3.234.237
2. de Wit E, van Doremalen N, Falzarano D, Munster VJ. SARS and MERS: recent insights into emerging coronaviruses. Nat Rev Microbiol. (2016) 14:523–34. doi: 10.1038/nrmicro.2016.81
3. Cao W, Vlas SJD, Richardus JH. The severe acute respiratory syndrome epidemic in mainland China dissected. Infect Dis Rep. (2011) 3:e2–e2. doi: 10.4081/idr.2011.1794
4. Hui DS, Azhar EI, Madani TA, Ntoumi F, Kock R, Dar O, et al. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health — The latest 2019 novel coronavirus outbreak in Wuhan, China. Int J Infect Dis. (2020) 91:264–6. doi: 10.1016/j.ijid.2020.01.009
5. Menachery VD, Schäfer A, Burnum-Johnson KE, Mitchell HD, Eisfeld AJ, Walters KB, et al. MERS-CoV and H5N1 influenza virus antagonize antigen presentation by altering the epigenetic landscape. PNAS. (2018) 115:E1012–21. doi: 10.1073/pnas.1706928115
6. Cui J, Li F, Shi Z-L. Origin and evolution of pathogenic coronaviruses. Nat Rev Microb. (2019) 17:181–92. doi: 10.1038/s41579-018-0118-9
7. Ahmad T, Haroon null, Dhama K, Sharun K, Khan FM, Ahmed I, et al. Biosafety and biosecurity approaches to restrain/contain and counter SARS-CoV-2/COVID-19 pandemic: a rapid-review. Turk J Biol. (2020) 44:132–45. doi: 10.3906/biy-2005-63
8. Jalava K. First respiratory transmitted food borne outbreak? Int J Hygiene Environ Health. (2020) 226:113490. doi: 10.1016/j.ijheh.2020.113490
9. Karthik K, Aravindh Babu RP, Dhama K, Chitra MA, Kalaiselvi G, Alagesan Senthilkumar TM, et al. Biosafety concerns during the collection, transportation, and processing of COVID-19 samples for diagnosis. Arch Med Res. (2020) 51:623–30. doi: 10.1016/j.arcmed.2020.08.007
10. Malik YS, Kumar N, Sircar S, Kaushik R, Bhat S, Dhama K, et al. Coronavirus disease pandemic (COVID-19): challenges and a global perspective. Pathogens. (2020) 9:519. doi: 10.3390/pathogens9070519
11. Lai C-C, Shih T-P, Ko W-C, Tang H-J, Hsueh P-R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): the epidemic and the challenges. Int J Antimicrob Agents. (2020) 55:105924. doi: 10.1016/j.ijantimicag.2020.105924
12. Backer JA, Klinkenberg D, Wallinga J. Incubation period of 2019 novel coronavirus (2019-nCoV) infections among travellers from Wuhan, China, 20–28 January 2020. Eurosurveillance. (2020) 25:2000062. doi: 10.2807/1560-7917.ES.2020.25.5.2000062
13. Zhang M, Zhou M, Tang F, Wang Y, Nie H, Zhang L, et al. Knowledge, attitude, and practice regarding COVID-19 among healthcare workers in Henan, China. J Hospital Infect. (2020) 105:183–7. doi: 10.1016/j.jhin.2020.04.012
14. Dhama K, Khan S, Tiwari R, Sircar S, Bhat S, Malik YS, et al. Coronavirus Disease 2019–COVID-19. Clin Microb Rev. (2020) 33:1–75. doi: 10.1128/CMR.00028-20
15. Paraskevis D, Kostaki EG, Magiorkinis G, Panayiotakopoulos G, Sourvinos G, Tsiodras S. Full-genome evolutionary analysis of the novel corona virus (2019-nCoV) rejects the hypothesis of emergence as a result of a recent recombination event. Infect Genet Evol. (2020) 79:104212. doi: 10.1016/j.meegid.2020.104212
16. Wu F, Zhao S, Yu B, Chen Y-M, Wang W, Song Z-G, et al. A new coronavirus associated with human respiratory disease in China. Nature. (2020) 579:265–9. doi: 10.1038/s41586-020-2008-3
17. Liu Z, Xiao X, Wei X, Li J, Yang J, Tan H, et al. Composition and divergence of coronavirus spike proteins and host ACE2 receptors predict potential intermediate hosts of SARS-CoV-2. J Med Virol. (2020) 92:595–601. doi: 10.1002/jmv.25726
18. Zhou P, Yang X-L, Wang X-G, Hu B, Zhang L, Zhang W, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. (2020) 579:270–3. doi: 10.1038/s41586-020-2012-7
19. Chu DK, Akl EA, Duda S, Solo K, Yaacoub S, Schünemann HJ, et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis. Lancet. (2020) 395:1973–87. doi: 10.1016/S0140-6736(20)31142-9
20. Setti L, Passarini F, De Gennaro G, Barbieri P, Perrone MG, Borelli M, et al. Airborne transmission route of COVID-19: why 2 meters/6 feet of inter-personal distance could not be enough. Int J Environ Res Public Health. (2020) 17:2932. doi: 10.3390/ijerph17082932
21. Correia G, Rodrigues L, Gameiro da Silva M, Gonçalves T. Airborne route and bad use of ventilation systems as non-negligible factors in SARS-CoV-2 transmission. Med Hypotheses. (2020) 141:109781. doi: 10.1016/j.mehy.2020.109781
22. Morawska L, Cao J. Airborne transmission of SARS-CoV-2: the world should face the reality. Environ Int. (2020) 139:105730. doi: 10.1016/j.envint.2020.105730
23. Shi J, Wen Z, Zhong G, Yang H, Wang C, Huang B, et al. Susceptibility of ferrets, cats, dogs, and other domesticated animals to SARS–coronavirus 2. Science. (2020) 368:1016–20. doi: 10.1126/science.abb7015
24. Hui DSC, Zumla A. Severe acute respiratory syndrome: historical, epidemiologic, and clinical features. Infect Dis Clinics North Am. (2019) 33:869–89. doi: 10.1016/j.idc.2019.07.001
25. Xiao K, Zhai J, Feng Y, Zhou N, Zhang X, Zou J-J, et al. Isolation and characterization of 2019-nCoV-like coronavirus from malayan pangolins. bioRxiv. (2020) 2.17.951335. doi: 10.1101/2020.02.17.951335
26. Chan JF-W, Kok K-H, Zhu Z, Chu H, To KK-W, Yuan S, et al. Genomic characterization of the 2019 novel human-pathogenic coronavirus isolated from a patient with atypical pneumonia after visiting Wuhan. Emerg Microbes Infect. (2020) 9:221–36. doi: 10.1080/22221751.2020.1719902
27. Shang W, Yang Y, Rao Y, Rao X. The outbreak of SARS-CoV-2 pneumonia calls for viral vaccines. npj Vaccines. (2020) 5:1–3. doi: 10.1038/s41541-020-0170-0
28. Sit THC, Brackman CJ, Ip SM, Tam KWS, Law PYT, To EMW, et al. Infection of dogs with SARS-CoV-2. Nature. (2020) 586:776–8. doi: 10.1038/s41586-020-2334-5
29. Segalés J, Puig M, Rodon J, Avila-Nieto C, Carrillo J, Cantero G, et al. Detection of SARS-CoV-2 in a cat owned by a COVID-19–affected patient in Spain. PNAS. (2020) 117:24790–93. doi: 10.1073/pnas.2010817117
30. Sailleau C, Dumarest M, Vanhomwegen J, Delaplace M, Caro V, Kwasiborski A, et al. First detection and genome sequencing of SARS-CoV-2 in an infected cat in France. Transb Emerg Dis. 67:2324–28. doi: 10.1111/tbed.13659
31. Shibata S, Arima H, Asayama K, Hoshide S, Ichihara A, Ishimitsu T, et al. Hypertension and related diseases in the era of COVID-19: a report from the Japanese Society of Hypertension Task Force on COVID-19. Hypert Res. (2020) 43:1028–46. doi: 10.1038/s41440-020-0515-0
32. Salata C, Calistri A, Parolin C, Palù G. Coronaviruses: a paradigm of new emerging zoonotic diseases. Pathog Dis. (2019) 77: doi: 10.1093/femspd/ftaa006
33. Yoo J-H. The Fight against the 2019-nCoV outbreak: an arduous march has just begun. J Kor Med Sci. (2020) 35:e56. doi: 10.3346/jkms.2020.35.e56
34. Baradaran A, Ebrahimzadeh MH, Baradaran A, Kachooei AR. Prevalence of comorbidities in covid-19 patients: a systematic review and meta-analysis. Arch Bone Joint Surg. (2020) 8:247–55. doi: 10.22038/abjs.2020.47754.2346
35. Callender LA, Curran M, Bates SM, Mairesse M, Weigandt J, Betts CJ. The Impact of Pre-existing Comorbidities and Therapeutic Interventions on COVID-19. Front Immunol. (2020) 11:1991. doi: 10.3389/fimmu.2020.01991
36. Ssentongo P, Ssentongo AE, Heilbrunn ES, Ba DM, Chinchilli VM. Association of cardiovascular disease and 10 other pre-existing comorbidities with COVID-19 mortality: a systematic review and meta-analysis. PLoS ONE. (2020) 15:e0238215. doi: 10.1371/journal.pone.0238215
37. Targher G, Mantovani A, Wang X-B, Yan H-D, Sun Q-F, Pan K-H, et al. Patients with diabetes are at higher risk for severe illness from COVID-19. Diab Metab. (2020) 46:335–7. doi: 10.1016/j.diabet.2020.05.001
38. Dhama K, Patel SK, Pathak M, Yatoo MI, Tiwari R, Malik YS, et al. An update on SARS-CoV-2/COVID-19 with particular reference to its clinical pathology, pathogenesis, immunopathology and mitigation strategies. Travel Med Infect Dis. (2020) 37:101755. doi: 10.1016/j.tmaid.2020.101755
39. Andersen KG, Rambaut A, Lipkin WI, Holmes EC, Garry RF. The proximal origin of SARS-CoV-2. Nat Med. (2020) 26:450–2. doi: 10.1038/s41591-020-0820-9
40. Ji W, Wang W, Zhao X, Zai J, Li X. Cross-species transmission of the newly identified coronavirus 2019-nCoV. J Med Virol. (2020) 92:433–40. doi: 10.1002/jmv.25682
41. Dhama K, Patel SK, Sharun K, Pathak M, Tiwari R, Yatoo MI, et al. SARS-CoV-2: jumping the species barrier, lessons from SARS and MERS, its zoonotic spillover, transmission to humans, preventive and control measures and recent developments to counter this pandemic virus. Preprints. (2020) 37:101830. doi: 10.20944/preprints202004.0011.v1
42. Tiwari R, Dhama K, Sharun K, Yatoo MI, Malik YS, Singh R, et al. COVID-19: animals, veterinary and zoonotic links. Vet Q. (2020) 40:169–82. doi: 10.1080/01652176.2020.1766725
43. Rothan HA, Byrareddy SN. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J Autoimmunity. (2020) 109:102433. doi: 10.1016/j.jaut.2020.102433
44. Chen J. Pathogenicity and transmissibility of 2019-nCoV—A quick overview and comparison with other emerging viruses. Microbes Infect. (2020) 22:69–71. doi: 10.1016/j.micinf.2020.01.004
45. Nishiura H, Linton NM, Akhmetzhanov AR. Initial cluster of novel coronavirus (2019-nCoV) Infections in Wuhan, China is consistent with substantial human-to-human transmission. J Clin Med. (2020) 9:488. doi: 10.3390/jcm9020488
46. Reusken CB, Farag EA, Jonges M, Godeke GJ, El-Sayed AM, Pas SD, et al. Middle East respiratory syndrome coronavirus (MERS-CoV) RNA and neutralising antibodies in milk collected according to local customs from dromedary camels, Qatar, April 2014. Eurosurveillance. (2014) 19:20829. doi: 10.2807/1560-7917.ES2014.19.23.20829
47. Fan Y, Zhao K, Shi Z-L, Zhou P. Bat Coronaviruses in China. Viruses. (2019) 11:210–20. doi: 10.3390/v11030210
48. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. (2020) 395:1054–62. doi: 10.1016/S0140-6736(20)30566-3
49. Dr M, Np F. COVID-19: another infectious disease emerging at the animal-human interface. N Z Med J. (2020) 133:12–15.
50. Almendros A. Can companion animals become infected with Covid-19? Vet Rec. (2020) 186:388–9. doi: 10.1136/vr.m1194
51. Mohandas S, Jain R, Yadav PD, Shete-Aich A, Sarkale P, Kadam M, et al. Evaluation of the susceptibility of mice & hamsters to SARS-CoV-2 infection. Indian J Med Res. (2020) 151:479–82. doi: 10.4103/ijmr.IJMR_2235_20
52. Kim Y-I, Kim S-G, Kim S-M, Kim E-H, Park S-J, Yu K-M, et al. Infection and rapid transmission of SARS-CoV-2 in ferrets. Cell Host Microbe. (2020) 27:704–9.e2. doi: 10.1016/j.chom.2020.03.023
53. Short Report – Medical nutrition therapy for critically ill patients with COVID-19. European Review. (2020) Available online at: https://www.europeanreview.org/article/20874 (Accessed November 30, 2020).
54. Leroy EM, Ar Gouilh M, Brugère-Picoux J. The risk of SARS-CoV-2 transmission to pets and other wild and domestic animals strongly mandates a one-health strategy to control the COVID-19 pandemic. One Health. (2020) 10:100133. doi: 10.1016/j.onehlt.2020.100133
55. Sexton NR, Smith EC, Blanc H, Vignuzzi M, Peersen OB, Denison MR. Homology-based identification of a mutation in the coronavirus RNA-Dependent RNA polymerase that confers resistance to multiple mutagens. J Virol. (2016) 90:7415–28. doi: 10.1128/JVI.00080-16
56. Ye Z-W, Yuan S, Yuen K-S, Fung S-Y, Chan C-P, Jin D-Y. Zoonotic origins of human coronaviruses. Int J Biol Sci. (2020) 16:1686–97. doi: 10.7150/ijbs.45472
57. Sah R, Rodriguez-Morales AJ, Jha R, Chu DKW, Gu H, Peiris M, et al. Complete genome sequence of a 2019 novel coronavirus (SARS-CoV-2) strain isolated in nepal. Microbiol Resour Announc. (2020) 9:e00169–2. doi: 10.1128/MRA.00169-20
58. Su S, Wong G, Shi W, Liu J, Lai ACK, Zhou J, et al. Epidemiology, genetic recombination, and pathogenesis of coronaviruses. Trends Microbiol. (2016) 24:490–502. doi: 10.1016/j.tim.2016.03.003
59. Wrapp D, Wang N, Corbett KS, Goldsmith JA, Hsieh C-L, Abiona O, et al. Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. Science. (2020) 367:1260–3. doi: 10.1126/science.abb2507
60. Wei X, Li X, Cui J. Evolutionary perspectives on novel coronaviruses identified in pneumonia cases in China. Natl Sci Rev. (2020) 7:239–42. doi: 10.1093/nsr/nwaa009
61. Golonka RM, Saha P, Yeoh BS, Chattopadhyay S, Gewirtz AT, Joe B, et al. Harnessing innate immunity to eliminate SARS-CoV-2 and ameliorate COVID-19 disease. Physiol Genomics. (2020) 52:217–21. doi: 10.1152/physiolgenomics.00033.2020
62. Reed SE. The behaviour of recent isolates of human respiratory coronavirus in vitro and in volunteers: evidence of heterogeneity among 229E-related strains. J Med Virol. (1984) 13:179–92. doi: 10.1002/jmv.1890130208
63. Vellingiri B, Jayaramayya K, Iyer M, Narayanasamy A, Govindasamy V, Giridharan B, et al. COVID-19: a promising cure for the global panic. Sci Total Environ. (2020) 725:138277. doi: 10.1016/j.scitotenv.2020.138277
64. Schoeman D, Fielding BC. Coronavirus envelope protein: current knowledge. Virol J. (2019) 16:69. doi: 10.1186/s12985-019-1182-0
65. Fehr AR, Perlman S. Coronaviruses: an overview of their replication pathogenesis. In: Maier HJ, Bickerton E, Britton P, editors. Coronaviruses: Methods Protocols Methods in Molecular Biology. (New York, NY: Springer), 1–23. doi: 10.1007/978-1-4939-2438-7_1
66. Dhama K, Patel SK, Sharun K, Pathak M, Tiwari R, Yatoo MI, et al. SARS-CoV-2 jumping the species barrier: zoonotic lessons from SARS, MERS and recent advances to combat this pandemic virus. Travel Med Infect Dis. (2020) 37:101830. doi: 10.1016/j.tmaid.2020.101830
67. Belouzard S, Chu VC, Whittaker GR. Activation of the SARS coronavirus spike protein via sequential proteolytic cleavage at two distinct sites. PNAS. (2009) 106:5871–6. doi: 10.1073/pnas.0809524106
68. Millet JK, Whittaker GR. Host cell entry of Middle East respiratory syndrome coronavirus after two-step, furin-mediated activation of the spike protein. Proc Natl Acad Sci USA. (2014) 111:15214–9. doi: 10.1073/pnas.1407087111
69. Kuba K, Imai Y, Ohto-Nakanishi T, Penninger JM. Trilogy of ACE2: A peptidase in the renin–angiotensin system, a SARS receptor, and a partner for amino acid transporters. Pharmacol Therap. (2010) 128:119–28. doi: 10.1016/j.pharmthera.2010.06.003
70. Xu Z, Shi L, Wang Y, Zhang J, Huang L, Zhang C, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Resp Med. (2020) 8:420–2. doi: 10.1016/S2213-2600(20)30076-X
71. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. (2020) 395:497–506. doi: 10.1016/S0140-6736(20)30183-5
72. Fan Y-Y, Huang Z-T, Li L, Wu M-H, Yu T, Koup RA, et al. Characterization of SARS-CoV-specific memory T cells from recovered individuals 4 years after infection. Arch Virol. (2009) 154:1093–9. doi: 10.1007/s00705-009-0409-6
73. Channappanavar R, Fehr AR, Zheng J, Wohlford-Lenane C, Abrahante JE, Mack M, et al. IFN-I response timing relative to virus replication determines MERS coronavirus infection outcomes. J Clin Invest. (2019) 129:3625–39. doi: 10.1172/JCI126363
74. Li G, Chen X, Xu A. Profile of specific antibodies to the SARS-associated coronavirus. N Engl J Med. (2003) 349:508–9. doi: 10.1056/NEJM200307313490520
75. Snijder EJ, van der Meer Y, Zevenhoven-Dobbe J, Onderwater JJM, van der Meulen J, Koerten HK, et al. Ultrastructure and origin of membrane vesicles associated with the severe acute respiratory syndrome coronavirus replication complex. J Virol. (2006) 80:5927–40. doi: 10.1128/JVI.02501-05
76. Wang Y, Wang Y, Chen Y, Qin Q. Unique epidemiological and clinical features of the emerging 2019 novel coronavirus pneumonia (COVID-19) implicate special control measures. J Med Virol. (2020) 92:568–77. doi: 10.1002/jmv.25748
77. Chen H, Guo J, Wang C, Luo F, Yu X, Zhang W, et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospective review of medical records. Lancet. (2020) 395:809–15. doi: 10.1016/S0140-6736(20)30360-3
78. Rasmussen SA, Smulian JC, Lednicky JA, Wen TS, Jamieson DJ. Coronavirus Disease 2019 (COVID-19) and pregnancy: what obstetricians need to know. Am J Obstet Gynecol. (2020) 222:415–26. doi: 10.1016/j.ajog.2020.02.017
79. Cascella M, Rajnik M, Cuomo A, Dulebohn SC, Di Napoli R. Features, evaluation, and treatment of coronavirus. StatPearls (Treasure Island (FL): StatPearls Publishing). Available online at: http://www.ncbi.nlm.nih.gov/books/NBK554776/ (Accessed November 30, 2020).
80. Wang W, Tang J, Wei F. Updated understanding of the outbreak of 2019 novel coronavirus (2019-nCoV) in Wuhan, China. J Med Virol. (2020) 92:441–7. doi: 10.1002/jmv.25689
81. Holshue ML, DeBolt C, Lindquist S, Lofy KH, Wiesman J, Bruce H, et al. First Case of 2019 Novel Coronavirus in the United States. N Engl J Med. (2020) 382:929–36. doi: 10.1056/NEJMoa2001191
82. Menni C, Valdes AM, Freidin MB, Ganesh S, Moustafa JSE-S, Visconti A, et al. Loss of smell and taste in combination with other symptoms is a strong predictor of COVID-19 infection. medRxiv. (2020) 26:1037–40. doi: 10.1101/2020.04.05.20048421
83. Li T, Wei C, Li W, Hongwei F, Shi J. Beijing Union Medical College Hospital on “pneumonia of novel coronavirus infection” diagnosis and treatment proposal (V2. 0). Med J Peking Union Med Coll Hosp. (2020). Available online at: http://kns.cnki.net/kcms/detail/11.5882.r.20200130.1430.002.html
84. Hassan SA, Sheikh FN, Jamal S, Ezeh JK, Akhtar A. Coronavirus (COVID-19): a review of clinical features, diagnosis, and treatment. Cureus. (2020) 12:e7355. doi: 10.7759/cureus.7355
85. Giovanetti M, Benvenuto D, Angeletti S, Ciccozzi M. The first two cases of 2019-nCoV in Italy: Where they come from? J Med Virol. (2020) 92:518–21. doi: 10.1002/jmv.25699
86. Pan A, Liu L, Wang C, Guo H, Hao X, Wang Q, et al. Association of public health interventions with the epidemiology of the COVID-19 outbreak in Wuhan, China. JAMA. (2020) 323:1915–23. doi: 10.1001/jama.2020.6130
87. Cheng MP, Papenburg J, Desjardins M, Kanjilal S, Quach C, Libman M, et al. Diagnostic testing for severe acute respiratory syndrome–related coronavirus 2. Ann Intern Med. (2020) 172:726–34. doi: 10.7326/M20-1301
88. Afzal A. Molecular diagnostic technologies for COVID-19: Limitations and challenges. J Adv Res. (2020) 26:149–59. doi: 10.1016/j.jare.2020.08.002
89. Ai J-W, Zhang Y, Zhang H-C, Xu T, Zhang W-H. Era of molecular diagnosis for pathogen identification of unexplained pneumonia, lessons to be learned. Emerg Microb Infect. (2020) 9:597–600. doi: 10.1080/22221751.2020.1738905
90. Kubina R, Dziedzic A. Molecular and Serological Tests for COVID-19. A Comparative Review of SARS-CoV-2 coronavirus laboratory and point-of-care diagnostics. Diagnostics. (2020) 10:434. doi: 10.3390/diagnostics10060434
91. Lieberman JA, Pepper G, Naccache SN, Huang M-L, Jerome KR, Greninger AL. Comparison of commercially available and laboratory-developed assays for in vitro detection of SARS-CoV-2 in clinical laboratories. J Clin Microb. (2020) 58:1–6. doi: 10.1128/JCM.00821-20
92. Sapkal G, Shete-Aich A, Jain R, Yadav PD, Sarkale P, Lakra R, et al. Development of indigenous IgG ELISA for the detection of anti-SARS-CoV-2 IgG. Ind J Med Res. (2020) 151:444. doi: 10.4103/ijmr.IJMR_2232_20
93. Li Z, Yi Y, Luo X, Xiong N, Liu Y, Li S, et al. Development and clinical application of a rapid IgM-IgG combined antibody test for SARS-CoV-2 infection diagnosis. J Med Virol. (2020) 92:1518–24. doi: 10.1002/jmv.25727
94. Lai C-C, Wang J-H, Hsueh P-R. Population-based seroprevalence surveys of anti-SARS-CoV-2 antibody: an up-to-date review. Int J Infect Dis. (2020) 101:314–22. doi: 10.1016/j.ijid.2020.10.011
95. Ruckert A, Zinszer K, Zarowsky C, Labonté R, Carabin H. What role for One Health in the COVID-19 pandemic? Can J Public Health. (2020) 111:641–4. doi: 10.17269/s41997-020-00409-z
96. Alzyood M, Jackson D, Aveyard H, Brooke J. COVID-19 reinforces the importance of handwashing. J Clin Nurs. (2020) 29:2760–1. doi: 10.1111/jocn.15313
97. Zhang L, Liu Y. Potential interventions for novel coronavirus in China: a systematic review. J Med Virol. (2020) 92:479–90. doi: 10.1002/jmv.25707
98. Tang JW, Tambyah PA, Hui DSC. Emergence of a novel coronavirus causing respiratory illness from Wuhan, China. J Infect. (2020) 80:350–71. doi: 10.1016/j.jinf.2020.01.014
99. Sharun K, Dhama K, Patel SK, Pathak M, Tiwari R, Singh BR, et al. Ivermectin, a new candidate therapeutic against SARS-CoV-2/COVID-19. Ann Clin Microb Antimicrob. (2020) 19:23. doi: 10.1186/s12941-020-00368-w
100. Becker RC. Covid-19 treatment update: follow the scientific evidence. J Thromb Thrombolysis. (2020) 50:43–53. doi: 10.1007/s11239-020-02120-9
101. Panyod S, Ho C-T, Sheen L-Y. Dietary therapy and herbal medicine for COVID-19 prevention: a review and perspective. J Tradit Compl Med. (2020) 10:420–7. doi: 10.1016/j.jtcme.2020.05.004
102. Zhang L, Yu J, Zhou Y, Shen M, Sun L. Becoming a faithful defender: traditional chinese medicine against coronavirus disease 2019 (COVID-19). Am J Chin Med. (2020) 48:763–77. doi: 10.1142/S0192415X2050038X
103. Alghamdi AN, Abdel-Moneim AS. Convalescent plasma: a potential life-saving therapy for coronavirus disease 2019 (COVID-19). Front Public Health. (2020) 8:437. doi: 10.3389/fpubh.2020.00437
104. Sharun K, Tiwari R, Yatoo MI, Patel SK, Natesan S, Dhama J, et al. Antibody-based immunotherapeutics and use of convalescent plasma to counter COVID-19: advances and prospects. Expert Opinion Biol Ther. (2020) 20:1033–46. doi: 10.1080/14712598.2020.1796963
105. Sharun K, Tiwari R, Patel SK, Karthik K, Yatoo MI, Malik YS, et al. Coronavirus disease 2019 (COVID-19) in domestic animals and wildlife: advances and prospects in the development of animal models for vaccine and therapeutic research. Hum Vacc Immunother. (2020) 4:1–12. doi: 10.1080/21645515.2020.1807802
106. Tiberghien P, de Lamballerie X, Morel P, Gallian P, Lacombe K, Yazdanpanah Y. Collecting and evaluating convalescent plasma for COVID-19 treatment: why and how? Vox Sanguinis. (2020) 115:488–94. doi: 10.1111/vox.12926
107. Schijns V, Lavelle EC. Prevention and treatment of COVID-19 disease by controlled modulation of innate immunity. Europ J Immunol. (2020) 50:932–8. doi: 10.1002/eji.202048693
108. Kaddoura M, AlIbrahim M, Hijazi G, Soudani N, Audi A, Alkalamouni H, et al. COVID-19 therapeutic options under investigation. Front Pharmacol. (2020) 11:1196. doi: 10.3389/fphar.2020.01196
109. Su H, Yao S, Zhao W, Li M, Liu J, Shang W, et al. Discovery of baicalin and baicalein as novel, natural product inhibitors of SARS-CoV-2 3CL protease in vitro. (2020) 04.13.038687. doi: 10.1101/2020.04.13.038687
110. Patel SK, Saikumar G, Rana J, Dhama J, Yatoo MI, Tiwari R, et al. Dexamethasone: a boon for critically ill COVID-19 patients? Travel Med Infect Dis. (2020) 37:101844. doi: 10.1016/j.tmaid.2020.101844
111. Jahan I, Onay A. Potentials of plant-based substance to inhabit and probable cure for the COVID-19. Turk J Biol. (2020) 44:228–41. doi: 10.3906/biy-2005-114
112. Tang N, Bai H, Chen X, Gong J, Li D, Sun Z. Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J Thromb Haemost. (2020) 18:1094–99. doi: 10.1111/jth.14817
113. Burrage DR, Koushesh S, Sofat N. Immunomodulatory drugs in the management of SARS-CoV-2. Front Immunol. (2020) 11:1844. doi: 10.3389/fimmu.2020.01844
114. Felsenstein S, Herbert JA, McNamara PS, Hedrich CM. COVID-19: immunology and treatment options. Clin Immunol. (2020) 215:108448. doi: 10.1016/j.clim.2020.108448
115. Villamor E, Mbise R, Spiegelman D, Hertzmark E, Fataki M, Peterson KE, et al. Vitamin A supplements ameliorate the adverse effect of HIV-1, Malaria, and diarrheal infections on child growth. Pediatrics. (2002) 109:e6. doi: 10.1542/peds.109.1.e6
116. Omolo CA, Soni N, Fasiku VO, Mackraj I, Govender T. Update on therapeutic approaches and emerging therapies for SARS-CoV-2 virus. Europ J Pharmacol. (2020) 883:173348. doi: 10.1016/j.ejphar.2020.173348
117. Gao QY, Chen YX, Fang JY. 2019 Novel coronavirus infection and gastrointestinal tract. J Digest Dis (2020) 21:125–6. doi: 10.1111/1751-2980.12851
118. Infusino F, Marazzato M, Mancone M, Fedele F, Mastroianni CM, Severino P, et al. Diet supplementation, probiotics, and nutraceuticals in SARS-CoV-2 infection: a scoping review. Nutrients. (2020) 12:1718. doi: 10.3390/nu12061718
119. Dhama K, Sharun K, Tiwari R, Dadar M, Malik YS, Singh KP, et al. COVID-19, an emerging coronavirus infection: advances and prospects in designing and developing vaccines, immunotherapeutics, and therapeutics. Hum Vaccin Immunother. (2020) 1232–8. doi: 10.1080/21645515.2020.1735227
120. Rabaan AA, Al-Ahmed SH, Sah R, Tiwari R, Yatoo MohdI, Patel SK, et al. SARS-CoV-2/COVID-19 and advances in developing potential therapeutics and vaccines to counter this emerging pandemic. Ann Clin Microbiol Antimicrob. (2020) 19:40. doi: 10.1186/s12941-020-00384-w
121. Yatoo MI, Hamid Z, Parray OR, Wani AH, Haq AU, Saxena A. COVID-19 - Recent advancements in identifying novel vaccine candidates and current status of upcoming SARS-CoV-2 vaccines. Hum Vaccines Immunoth. (2020) 25:1–14. doi: 10.1080/21645515.2020.1788310
122. Alagawany M, Attia Y, Farag M, Elnesr S, Nagadi S, Shafi M, et al. The strategy of boosting the immune system of food-producing under CoViD-19 pandemic. Front Vet Sci. (2020) 7:398. doi: 10.3389/fvets.2020.570748
123. Jayawardena R, Sooriyaarachchi P, Chourdakis M, Jeewandara C, Ranasinghe P. Enhancing immunity in viral infections, with special emphasis on COVID-19: a review. Diab Metab Syndrome. (2020) 14:367–82. doi: 10.1016/j.dsx.2020.04.015
124. Jaggers GK, Watkins BA, Rodriguez RL. COVID-19: repositioning nutrition research for the next pandemic. Nutr Res. (2020) 81:1–6. doi: 10.1016/j.nutres.2020.07.005
125. Messina G, Polito R, Monda V, Cipolloni L, Di Nunno N, Di Mizio G, et al. Functional role of dietary intervention to improve the outcome of COVID-19: a hypothesis of work. Int J Mol Sci. (2020) 21:3104. doi: 10.3390/ijms21093104
126. Grant WB, Lahore H, McDonnell SL, Baggerly CA, French CB, Aliano JL, et al. Evidence that vitamin D supplementation could reduce risk of influenza and COVID-19 infections and deaths. Nutrients. (2020) 12:988. doi: 10.3390/nu12040988
127. Shakoor H, Feehan J, Mikkelsen K, Dhaheri ASA, Ali HI, Platat C, et al. Be well: a potential role for vitamin B in COVID-19. Maturitas. (2020) 144:P108–111 doi: 10.1016/j.maturitas.2020.08.007
128. Jayaweera JAAS, Reyes M, Joseph A. Childhood iron deficiency anemia leads to recurrent respiratory tract infections and gastroenteritis. Scient Rep. (2019) 9:12637. doi: 10.1038/s41598-019-49122-z
129. Cianciosi D, Forbes-Hernández TY, Afrin S, Gasparrini M, Reboredo-Rodriguez P, Manna PP, et al. Phenolic compounds in honey and their associated health benefits: a review. Molecules. (2018) 23:2322. doi: 10.3390/molecules23092322
130. Attia YA, Al-Harthi MA, Abo El-Maaty HM. The effects of different oil sources on performance, digestive enzymes, carcass traits, biochemical, immunological, antioxidant, and morphometric responses of broiler chicks. Front Vet Sci. (2020) 7:181. doi: 10.3389/fvets.2020.00181
131. Galvão AM, de Andrade AD, de Maia MBS, da Silva KER, de Bezerra AA, de Melo JF, et al. Antioxidant supplementation for the treatment of acute lung injury: a meta-analysis. Rev Bras Ter Intensiva. (2011) 23:41–48.
132. Anand P, Kunnumakkara AB, Newman RA, Aggarwal BB. Bioavailability of curcumin: problems and promises. Mol Pharm. (2007) 4:807–18. doi: 10.1021/mp700113r
133. Attia YA, Alagawany MM, Farag MR, Alkhatib FM, Khafaga AF, Abdel-Moneim A-ME, et al. Phytogenic products and phytochemicals as a candidate strategy to improve tolerance to coronavirus. Front Vet Sci. (2020) 7:573151. doi: 10.3389/fvets.2020.573159
134. Kiros M, Andualem H, Kiros T, Hailemichael W, Getu S, Geteneh A, et al. COVID-19 pandemic: current knowledge about the role of pets and other animals in disease transmission. Virol J. (2020) 17:143. doi: 10.1186/s12985-020-01416-9
135. Mani JS, Johnson JB, Steel JC, Broszczak DA, Neilsen PM, Walsh KB, et al. Natural product-derived phytochemicals as potential agents against coronaviruses: a review. Virus Res. (2020) 284:197989. doi: 10.1016/j.virusres.2020.197989
136. Gentile LF, Cuenca AG, Efron PA, Ang D, Bihorac A, McKinley BA, et al. Persistent inflammation and immunosuppression: a common syndrome and new horizon for surgical intensive care. J Trauma Acute Care Surg. (2012) 72:1491–501. doi: 10.1097/TA.0b013e318256e000
137. Moballegh Nasery M, Abadi B, Poormoghadam D, Zarrabi A, Keyhanvar P, Khanbabaei H, et al. Curcumin delivery mediated by bio-based nanoparticles: a review. Molecules. (2020) 25:689. doi: 10.3390/molecules25030689
138. Hafez HM, Attia YA. Challenges to the poultry industry: current perspectives and strategic future after the COVID-19 outbreak. Front Vet Sci. (2020) 7:516. doi: 10.3389/fvets.2020.00516
139. Molenaar RJ, Vreman S, Hakze-van der Honing RW, Zwart R, de Rond J, Weesendorp E, et al. Clinical and pathological findings in SARS-CoV-2 Disease Outbreaks in Farmed Mink (Neovison vison), clinical and pathological findings in SARS-CoV-2 disease outbreaks in farmed mink (Neovison vison). Vet Pathol. (2020) 57:653–7. doi: 10.1177/0300985820943535
Keywords: COVID-19, genome, viral pneumonia, health emergency, ACE2, immune-competence, antioxidants
Citation: Siddique F, Abbas RZ, Mansoor MK, Alghamdi ES, Saeed M, Ayaz MM, Rahman M, Mahmood MS, Iqbal A, Manzoor M, Abbas A, Javaid A and Hussain I (2021) An Insight Into COVID-19: A 21st Century Disaster and Its Relation to Immunocompetence and Food Antioxidants. Front. Vet. Sci. 7:586637. doi: 10.3389/fvets.2020.586637
Received: 23 July 2020; Accepted: 10 December 2020;
Published: 13 January 2021.
Edited by:
Hafez Mohamed Hafez, Freie Universität Berlin, GermanyReviewed by:
Kuldeep Dhama, Indian Veterinary Research Institute (IVRI), IndiaFrancois Frederick Maree, Agricultural Research Council of South Africa (ARC-SA), South Africa
Copyright © 2021 Siddique, Abbas, Mansoor, Alghamdi, Saeed, Ayaz, Rahman, Mahmood, Iqbal, Manzoor, Abbas, Javaid and Hussain. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Faisal Siddique, faisalsiddique@cuvas.edu.pk