 Giorgia Sebastiani1*†
Giorgia Sebastiani1*† Vicente Andreu-Fernández2,3†
Vicente Andreu-Fernández2,3† Ana Herranz Barbero1
Ana Herranz Barbero1 Victoria Aldecoa-Bilbao1Xavier Miracle1Eva Meler Barrabes4Arantxa Balada Ibañez1Marta Astals-Vizcaino1Silvia Ferrero-Martínez5
Victoria Aldecoa-Bilbao1Xavier Miracle1Eva Meler Barrabes4Arantxa Balada Ibañez1Marta Astals-Vizcaino1Silvia Ferrero-Martínez5 María Dolores Gómez-Roig5
María Dolores Gómez-Roig5 Oscar García-Algar1,2
Oscar García-Algar1,2- 1Neonatal Unit, Hospital Clinic-Maternitat, Institut Clinic de Ginecologia, Obstetricia i Neonatologia (ICGON), Barcelona Center for Maternal Fetal and Neonatal Medicine (BCNatal), Barcelona, Spain
- 2Grup de Recerca Infancia i Entorn (GRIE), Institut d'investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Barcelona, Spain
- 3Valencian International University (VIU), Valencia, Spain
- 4Fetal i+D Fetal Medicine Research Center, BCNatal-Barcelona Center for Maternal-Fetal and Neonatal Medicine (Hospital Clínic and Hospital Sant Joan de Déu), IDIBAPS, University of Barcelona, Barcelona, Spain
- 5Hospital Sant Joan de Déu, Barcelona Center for Maternal Fetal and Neonatal Medicine (BCNatal), Barcelona, Spain
Introduction: Eating disorders (EDs) have increased globally in women of childbearing age, related to the concern for body shape promoted in industrialized countries. Pregnancy may exacerbate a previous ED or conversely may be a chance for improving eating patterns due to the mother's concern for the unborn baby. EDs may impact pregnancy evolution and increase the risk of adverse outcomes such as miscarriage, preterm delivery, poor fetal growth, or malformations, but the knowledge on this topic is limited.
Methods: We performed a systematic review of studies on humans in order to clarify the mechanisms underpinning the adverse pregnancy outcomes in patients with EDs.
Results: Although unfavorable fetal development could be multifactorial, maternal malnutrition, altered hormonal pathways, low pre-pregnancy body mass index, and poor gestational weight gain, combined with maternal psychopathology and stress, may impair the evolution of pregnancy. Environmental factors such as malnutrition or substance of abuse may also induce epigenetic changes in the fetal epigenome, which mark lifelong health concerns in offspring.
Conclusions: The precocious detection of dysfunctional eating behaviors in the pre-pregnancy period and an early multidisciplinary approach comprised of nutritional support, psychotherapeutic techniques, and the use of psychotropics if necessary, would prevent lifelong morbidity for both mother and fetus. Further prospective studies with large sample sizes are needed in order to design a structured intervention during every stage of pregnancy and in the postpartum period.
Introduction
Pregnancy is an exceptional condition that implicates intense psychological and biological transformations, which may change the perception of body shape, as well as influence modifications in eating patterns. Pregnancy therefore represents a period of increased weakness that triggers or aggravates symptoms of problematic eating behaviors (1).
According to the Diagnostic and Statistical Manual of Mental Disorders Fifth edition (DSM-V), Eating Disorders (EDs) are “disturbances in eating behavior that result in altered consumption of food and that significantly impair physical health and psychosocial functioning” (2). Anorexia Nervosa (AN) is characterized by a restriction of energy intake, leading to significant weight loss, intense anxiety around gaining weight, and a distorted perception of body weight and shape, associated with perfectionism and overcontrol. Bulimia Nervosa (BN) is associated with recurrent episodes of binge eating (eating a great amount of food in a discrete period of time with a sense of lack of control over eating and impulsivity), accompanied by inappropriate compensatory habits such as self-induced vomiting, abuse of laxatives or diuretics, and/or excessive exercise. Binge-eating disorder (BED) is defined by recurrent episodes of binge eating more rapidly than normal, which are followed by feeling uncomfortable, disgusted, depressed, or guilty as a result, however it is not associated with compensatory behaviors to prevent weight gain. Other Specified Feeding of Eating Disorders (OSFED) or Eating Disorders Not Otherwise Specified (EDNOS) refer to heterogeneous symptoms of feeding or ED resulting in a clinically significant problem that does not meet the full criteria of others disorders (2). Patients with chronic EDs often change between types of EDs (most commonly between AN and BN).
EDs are common in women of reproductive age. The prevalence of AN is an estimated 7 per 1,000 in the UK, with more incidence in adolescent girls and young women. BN is more frequent and affects older age groups, with a prevalence of 0.5–1% in women of reproductive age (3). Atypical EDs are probably more common but the literature about their prevalence is scarce. According to the American Association of EDs, at least 0.9% of American women suffer from AN, 1.5% from BN, and 2.8% from BED in their lifetime (4). In Europe, AN is reported at 1–4%, BN at 1–2%, BED at 1–4%, and subthreshold eating disorders at 2–3% of women (5). Some recent epidemiological studies estimate that the percentage of EDs has increased over the last years to ~5–10% of women of childbearing age (6).
The prevalence of EDs has been estimated at up to 7.5% in pregnant women (7). The incidence of EDs in the Norwegian Mother and Child Cohort was about 5%, where they found high incidence of BED in particular (8). In Italy the prevalence of AN, BN, and purging disorders during gestation was valued at up to 5.5% (9). A study conducted on pregnant Brazil population showed a prevalence of 17.3% of binge eating patterns associated with anxiety and mood liability (10).
Pregnancy and the postpartum period are related to variations in eating patterns such as overeating, strong rejection of specific foods or drinks, changes in taste perception, and women experience major body changes unseen since adolescence, which may trigger an ED in otherwise healthy pregnant patients (11, 12). Our culture which promotes slimness, weight concern and dissatisfaction with gaining weight, might lead to more dysfunctional eating attitudes (13, 14), because pregnant women may feel stressed and anxious over their changing body shape (15–17). In addition, the adaptive neuroendocrine modifications during gestation may alter brain function, impairing metabolism, appetite regulation, and mood (18).
Nevertheless, for most women ED symptoms tend to reduce during pregnancy because of the concern for the fetus, however this transient improvement of symptoms may revert in the postpartum period (19). A retrospective study reported that the prevalence of EDs was 11.5% from 3 to 7 months post-partum, with the most incidence in younger women (20), and a longitudinal study found that 12.8% of postpartum mothers suffered from a clinical eating disorder (21). This underlines that the postnatal period represents a vulnerable time for the exacerbation of disordered eating, probably due to anxiety about the postpartum body shape and to the frustration and stress of taking care of demanding infants, especially if there is not enough marital support (22). Furthermore, a longitudinal case-control study underlined that women with a recent ED had a higher rate of concern about weight gain and more loss of control over eating during pregnancy, and women with a past ED presented more compensatory behaviors than controls (23). In cross-sectional data in a Norwegian pregnant population, the incidence of BED during gestation was linked to social problems, symptoms of anxiety and depression, low life satisfaction, history of sexual and physical abuse, and smoking. Apprehension about pregnancy-related weight gain was the variable most strongly related to the onset of BED (24). Dysfunctional eating patterns may also reflect stress-response mechanisms related to the activation of Hypothalamic-pituitary-adrenal (HPA) axis and the corticotropin-releasing hormone (CRH) secretion which modulate food intake. Stress both stimulates the proopiomelanocortin (POMC) neurons eliciting anorexic signals and induces suppression of NPY secretion, declining its central orexigenic and anxiolytic actions (25).
Additionally, there are cultural influences that may trigger an ED during pregnancy. For example, food restriction during pregnancy is common in Chinese women, owing to the belief that this may protect the child and avoid complications such as miscarriage, stillbirth, death of the mother, and imperfections in newborns. For this reason, traditional women avoid cold foods or wet-hot foods, which are considered bad for the baby. These restrictions are often associated with symptoms of depression (26). Recent evidence showed that maternal disordered eating behaviors impact the course of pregnancy and fetal development. Updated reviews of the literature highlighted that the major obstetric and gynecologic complications were infertility, high rate of miscarriage, poor nutrition during pregnancy, hyperemesis gravidarum, cesarean section, preterm delivery, and postpartum depression (27–30). The most described detrimental effects on fetal development were fetal growth delay, small for gestational age babies and small head circumference, low Apgar score and an increased risk of perinatal mortality (27–30).
Despite the risk of EDs for both mother and fetus, the recognition of EDs during pregnancy is considered a challenge. ED is a multifactorial pathology, and it may be linked to predisposing factors including genetics, familiar and social dysfunction, mental illness such as Obsessive-Compulsive Personality Disorder (in AN) and Borderline Personality Disorder (in BN), or psychiatric disorders such as anxiety, depression, and substance abuse (31). There are not specific biochemical markers or precise instruments for the diagnosis of EDs in pregnant population, but standardized screening method, and questionnaires are available, which may differentiate normative dieting and eating concern from more dysfunctional behaviors (32, 33) (see Supplementary Material). Moreover, it is difficult to recognize the onset of an ED, because women often keep their condition secret (34). Stigmatizing attitudes may contribute to feelings of shame and guilt that lead them to hide their disorder and avoid help (35). On the other hand, clinical symptoms during pregnancy may be masked due to a reduction in clinical features or the presence of pregnancy sickness and hyperemesis gravidarum (36). Nonetheless, it is imperative to reach an early diagnosis in order to prevent long-lasting effects on women of reproductive age and impaired fetal outcomes (37). Clinicians should pay attention to warning signs such as lack of weight gain in consecutive visits during the second trimester, hyperemesis gravidarum that persists more than 20 weeks, or previous history of ED, depression, or dieting (38).
The purpose of this systematic review was to provide an update on the existing studies in humans focused on the effects of EDs during pregnancy on maternal and fetal outcomes. Specifically, our aim was to increase our knowledge on the topic of EDs during pregnancy, in order to highlight the importance of early prevention of these disturbances. We also focused on the effect of these dietary patterns have on fetal development and maternal psychopathology, to find a target therapy that could avoid fetal complications.
Methods
The manuscripts included in this systematic review mainly concern EDs such as AN, BN, BED, and ENDOS. We did not assess studies about other types of EDs. Studies were screened based on PRISMA methodology, by searching titles and abstracts in the following electronic databases: SCOPUS, MEDLINE//PubMed, and Cochrane. The research was based on the combination of the following descriptors: eating disorders, anorexia nervosa, bulimia nervosa, binge eating disorders, pregnancy outcomes, fetal development, small for gestational age, epigenetics, preterm delivery, malformations, food intake, eating patterns, fertility, gestational weight gain, postpartum depression, maternal psychopathology, and breastfeeding/human milk. Boolean terms AND/OR/XOR were combined in the search.
Inclusion criteria were: the period covered from January 1 of 2000 to May 31, 2020, the presence of selected descriptors in the title of the papers or as keywords, only articles written in English language and only studies performed in humans, excluding books and documents as well as all references which results were based on animal models. Original manuscripts were selected by screening titles and abstracts, creating a reference list of relevant papers for the topics explored in this review. Of note, pre-conception period was also included. Two investigators (A.-F.V. and S.G.) conducted each stage of the studies selection, deleted duplicate inputs and evaluated the quality of the studies. All data were extracted by one investigator (S.G.) and cross-checked by a second investigator (A.-F.V.). In case of discrepancies in the selected studies, we opted for reconciliation through team discussion. The following variables were also explored: study characteristics including study design (case–control, review, longitudinal cohort, and cross-sectional), sample size, country, characteristics of participant population (number of cases, diagnostic criteria for EDs, hospitalized patients, type of EDs) and results (including strengths, limitations, conclusions, and possible biases). The quality of controlled studies (randomized, non-randomized, before-after) was critically appraised using the Cochrane Collaboration's Risk of Bias Tool (39).
The initial search identified a total of 249 papers once the inclusion and exclusion criteria were applied. After reviewing the abstract 126 studies were not selected because they were out of the scope of this review (eating disorders, pregnancy and fetal outcomes) and we also discarded 11 duplicate studies. Thirty records were selected through other sources by their relevance in the field. This resulted in 142 published studies. Additionally, for epigenetics section, the search was “(eating disorders or anorexia nervosa or bulimia nervosa or binge eating disorders) and (pregnancy or fetal outcome or preterm) and epigenetics” obtaining 25 results. Twenty articles were selected and 5 additional papers were included from other sources by their relevance in this issue. In the case of breastfeeding section, the terms used were “(eating disorders or anorexia nervosa or bulimia nervosa or binge eating disorders) and (pregnancy or fetal outcome or preterm) and breastfeeding” showing 42 results. Thirty studies were finally selected. Both sections were performed following the same inclusion and exclusion criteria. Finally, 197 studies were selected to perform this review.
We expected an important bias due to the heterogeneous results observed in the literature selected by the different populations compared, the distinct health condition of them, the lack of randomized trials in pregnant women with EDs the use of questionnaires to detect nutritional deficits and psychological alterations as well as the small sample size observed in some studies. Otherwise Table S1 included the American Dietetic Association Guidelines for pregnancy and the International Guidelines for the management of EDs during pregnancy to contextualize the nutritional requirements during this period. Moreover, scientific papers related to the nutritional and hormonal status of pregnant women were also included to evaluate possible detrimental effects on fetal development.
Review
Periconceptional Period in Women With EDs
Women with EDs are reported to have menstrual irregularity, problems with sexuality linked to a conflicted relationship with their body, decreased libido, and high sexual anxiety (40, 41). This can lead to insufficient use of contraception methods with a consequent unplanned pregnancy. In a prospective pregnancy cohort study, 50% of women with AN reported unplanned pregnancy when compared to a control group without EDs (42). An unplanned pregnancy may add risk to fetal development due to poor prenatal care, such as drinking alcohol, failing in balanced nutrition, or delaying the intake of prenatal vitamins. Moreover, unintentional pregnancy may exacerbate contrasting feelings in women, such as excitement yet depression and anxiety, when discovering their pregnant status.
There is a critical level of accumulated energy or fat mass that is essential for maintaining regular menstruation. EDs may affect fertility and menstruation because malnutrition and weight loss may alter hormonal status. Reduced levels of luteinizing hormone (LH) and follicle-stimulating hormone (FSH) suggest hypothalamic and pituitary dysfunction, which often lead to anovulation and amenorrhea. Sex hormones interact with neurotransmitters to achieve central control of appetite and energy balance, so in EDs there is a deregulation of appetite mechanisms (43). Women with AN may experience a drop in levels of leptin, a hormone that inhibits appetite and it is linked to energy homeostasis. This fall in leptin is associated with low caloric intake and with low fat mass, resulting in the reduction of the pulsatile release of gonadotropin-releasing-hormone (GnRH). All these hormonal pathways provoke dysfunction in ovulation, menstruation, and bone growth (44). Moreover, it has been reported that women with BN may be affected by hyperandrogenism and polycystic ovary syndrome (PCOS), a common cause of infertility, characterized by higher levels of circulating androgens. Testosterone is known to stimulate appetite and has been linked to altered impulse control and depression, so patients with PCOS exhibit a deregulation of appetite that may exacerbate bulimic symptoms (45). In addition, elevated ghrelin levels observed in patients with EDs may produce continuing inhibition of the hypothalamic-pituitary-ovarian axis and amenorrhea in spite of normal body fat and leptin levels. Low insulin status is also linked to amenorrhea, related to hypothalamic sensors of insulin levels. In patients with EDs, the activation of the HPA axis starts as a result of a stress reaction, leading to increased levels of CRH and cortisol, and failure of the circadian rhythm of cortisol. Through metabolic pathways, these hormones interact with the GnRH directly or through neuropeptide mediators (neuropeptide Y or kisspeptin). The final result of these metabolic signals in patients with EDs, is the inhibition of the normal pulsatile GnRH, low levels of LH, FSH, estradiol and small ovaries, the main causes of infertility (46).
There is little data about the prevalence of EDs in women affected by fertility problems. The prevalence of ovulatory disturbances is considerably higher in females with severe EDs (47). A recent longitudinal study conducted on women who started infertility treatment, found that the prevalence of EDs was 20.7% and the most prevalent EDs were AN and BED (48). In the longitudinal Avon study cohort of Parents and Children (ALSPAC) (49), the EDs groups with AN or AN+BN participants, took no longer than 12 months to conceive, but they delayed more than the general population (>6 months), and were more likely to conceive the current pregnancy with fertility treatment. This study underlines that women with AN, or AN+BN experienced conception problems without meeting the criteria for infertility (defined as inability to conceive for more than 12 months). This group included women with the lowest preconception BMI, which may explain the difficulty in conceiving. The authors concluded that fertility was affected in the EDs group but not considerably impaired. The limitation of this study is that the classification of EDs was made on the basis of self-reporting. A recent longitudinal population-based cohort study performed in the Netherlands showed that EDs were associated with increased odds of receiving fertility treatment and twin births, regardless of pre-pregnancy BMI (50). Another study showed that female patients with EDs recruited at Helsinki University Central Hospital had impaired reproductive health with the lowest pregnancy rate in patients with AN and a high rate of miscarriage in patients affected by BED (51).
Preconception Nutritional Profile in Adolescents and Women With EDs (See Tables 1, 2)
Healthy BMI prior to pregnancy is considered between 18.5 and 25 kg/m2 and current evidence suggests that poor or excessive gestational weight gain (GWG) are risk factors for perinatal complications. According to the Institute of Medicine(IOM) there are reference tables for correct GWG during pregnancy (see Table 1) (73–76).
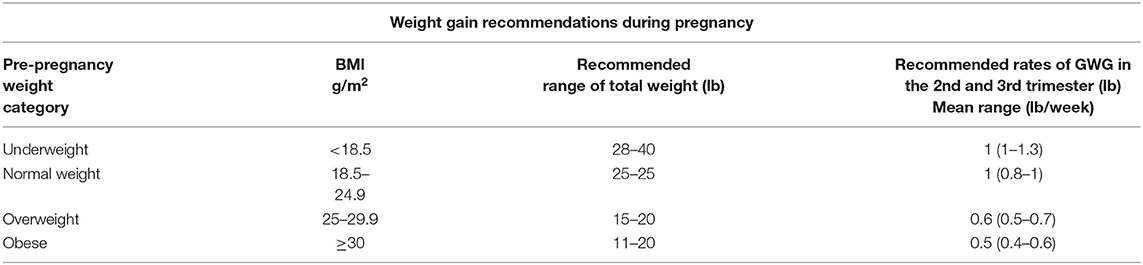
Table 1. IOM weight gain recommendations during pregnancy (52).
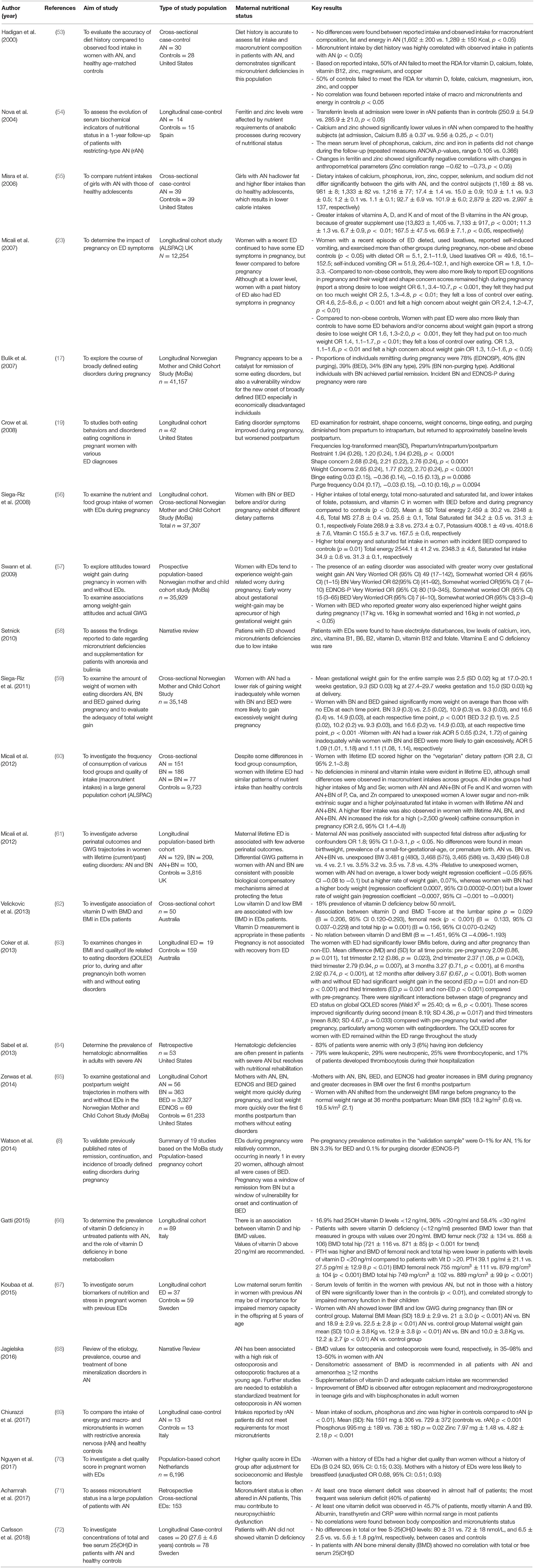
Table 2. Studies about the effects of eating disorders on maternal nutritional status: pre-conception period and pregnancy.
Few studies reported micronutrients status in patients with EDs with controversial results, because the majority evaluated dietary intake based on questionnaire reports and others assessed plasma levels. Cross-sectional and longitudinal case-control studies conducted on women of childbearing age with a history of AN determined a predominance of low intake of micronutrients like vitamin D, calcium, phosphorus, folate, sodium, magnesium, zinc, and copper. With regard to vitamin B12, results about the intake were contradictory: one study showed low intake in patients with AN characterized by high rate of vegetarians, but others did not find differences in intake when compared with the control group (53, 69). The limitations of these studies were the small sample sizes and the estimation of food portions, which were based on food questionnaire, since patients may underestimate or overestimate their nutrient intake. The high rate of vegetarianism among EDs women and consequently the lack of intake of meat and fish, is linked to a low source of iodine, iron, vitamins A, D, B12 and long chain omega-3 polyunsaturated fatty acids (77).
Another cross-sectional study did not find differences in dietary intake of minerals in adolescent girls with AN. In fact, the authors described a great intake of vitamins due to higher supplement consumption. However, these results were described in community-dwelling girls with AN, included in interventional and support strategies (55).
A review of literature conducted by Setnick (58), reported blood electrolyte disturbances in patients with EDs due to purging behaviors. Moreover, the author showed inadequate calcium intake, iron deficiency anemia, and zinc deficiency because patients restricted meat and practiced heavy exercise with consequent impaired absorption of elements. In contrast, vitamin A could be elevated in serum due to inadequate intake of other nutrients essential for vitamin A metabolism like dietary fats. Patients with EDs were found to have low ingestion of Vitamin B1, B2, and B6 because of restrictive eating patterns associated with alcohol consumption. Plasma deficiencies of Vitamin B12 and folic acid were also present in patients with EDs due to low intake, as judged by elevated plasma levels of homocysteine. Hematological deficiencies such as anemia, leucopenia, and thrombocytopenia are often present in patients with severe AN (54, 64).
Adolescence is a critical period for bone mass content, which is regulated by hormonal pathways. Estrogen and androgen release are decreased and cortisol increases in patients with EDs. Furthermore, conversion of free T3 and production of insulin-like growth factor-1 (IGF-1), are reduced. Such hormonal imbalances joined with nutritional deficiencies in vitamin D and calcium, decrease bone establishment, so 50% of adolescents with EDs displayed low mineral density (78). Young women affected by EDs were found to be vitamin D deficient (<50 nmol/L) and vitamin D levels predict low bone mineral density (BMD) in the lumbar spine, femoral neck and total hip. Weight gain was the most important factor in the improvement of BMD (62, 66). AN is associated with a high risk of osteoporosis and osteoporotic fractures at a young age (68). Conversely, Carlsson et al. (72) didn't find any differences in total and free 25 (OH) vitamin D in AN patients and healthy controls. A possible explanation could be that AN patients have a lower amount of adipose tissue, and vitamin D is a fat-soluble vitamin stored in fat tissue. If these patients present a deficit in fat mass, adipose tissue can't uptake vitamin D, resulting in increased levels. Nevertheless, this study was conducted in a specific population (Swedish), and vitamin D supplements were not registered, so it is difficult to generalize these results.
One of the most recent studies documenting nutritional status in 153 young women with AN found at least one trace element and one vitamin deficiencies in almost half of patients, the most frequent were selenium, vitamin A and B9, suggesting that micronutrient status is often disrupted in AN patients (71).
The Impact of EDs During Pregnancy on Eating Patterns and Maternal Nutritional Profile (See Table 2)
Weight management during pregnancy is imperative for the health of offspring and it is linked to a balanced diet and to a regular physical activity (see Table S1). The majority of studies that report on eating behaviors in pregnant patients with EDs have found a high rate of remission of symptoms related to image concern, and decreased restrictive and purging attitudes (8, 19). These changes might be related to a sense of responsibility for fetal development, a different perception of their body during pregnancy, and greater support from family and clinicians (79). Other studies redact that pregnancy may trigger a relapse of EDs symptoms (23). Moreover, pregnancy may promote a remission of symptoms in patients with BN but it may generate the onset or continuation in BED patients (17). A recent systematic review showed that women with lifetime AN, BN, or AN+BN had similar nutritional patterns and similar intake of supplements as healthy women suggesting a remission of ED symptoms during gestation. This data only found greater energy and fat intakes in BED population (80).
A study conducted in a large UK general population cohort (ALSPAC) (60) included 414 patients and 9,723 controls and assessed eating patterns and nutrient intake in women with lifetime EDs during the third trimester of gestation using the Food Frequency Questionnaire (FFQ). The results showed that, in general, dietary patterns during pregnancy in women with EDs were similar to women from the general population. In relation to energy, carbohydrate, fat, and protein intake, no differences were found in the EDs group when compared to the control group. Nevertheless, they highlight that women with EDs consumed more soy products and plant-based food than controls and defined themselves as vegetarians. Moreover, women with AN and AN+BN showed high folate and potassium consumption; women with AN+BN had a higher intake of calcium, phosphorus, zinc, and vitamin C, and women with BN had higher vitamin E ingestion. They did not observe differences linked to macronutrient consumption. Interestingly, women with EDs consumed higher amounts of caffeine (>2,500 mg/week) than general population during pregnancy (81), probably due to its stimulating properties and to the desire to inhibit appetite.
Siega-Riz et al. (56) conducted a cross-sectional study in a large (n = 35,148) Norwegian Mother and Child Cohort (MoBa) and investigated food group intake by FFQ in pregnant women with BN and BED in the first half of pregnancy. Women with BED showed greater intake of total energy and total mono-saturated and saturated fat. As for micronutrient consumption, a small difference was found in women with EDs compared with controls. Furthermore, women with BED showed a lower intake of folate, potassium, and vitamin C related to lower intake of fruit and juices and a greater intake of fat (butter, margarines, and oils) and milk dessert. BN patients exhibited a lower intake of fatty meat but there was higher consumption of artificially sweetened drinks among women with BN and BED. Women with active BED also consumed more coffee than the control group in order to suppress appetite and to increase energy waste. The higher socio-economic status of such population may induce bias.
Nguyen et al. (70) investigated a diet quality score in pregnant women with EDs and found a higher quality score in EDs group after adjustment for socioeconomic and lifestyle factors. This result has been observed probably because women with EDs had a preference for food with health advantages (vegetables, skim milk) so they provide themselves a healthy diet out of concern about fetal development.
The strength of the studies described were the large population-based prospective design. The main limitations were related to self-reported ED history, because this may underestimate the ED, and to the assessment of portion size by FFQ, which is not precise.
In a recent longitudinal cohort study, Koubaa et al. (67) investigated pregnant nulliparous non-smoking women with a history of AN and/or BN vs. controls, analyzing biomarkers of nutrition during early pregnancy. Women with AN showed a higher prevalence of anemia, lower BMI, low GWG during pregnancy when compared to BN and the control group. Moreover, the authors found low plasma ferritin levels suggesting depleted iron stores. During pregnancy, mild anemia is a normal consequence of hemodilution and the requirement for iron rises because of increased fetal necessity and transfer across the placenta. Preconception iron stores determine the risk of iron deficiency anemia, so patients with EDs are at a greater risk for gestational anemia.
The main limitation of aforementioned studies is the lack of distinction between recent or ancient ED which may influence the nutritional profile of pregnant women with EDs.
Therefore, evidences support that pregnant women with EDs show sufficient quality in their diet demonstrating an improvement in ED symptoms during pregnancy. However, the ED subgroups exhibit differences related to the relapse of symptoms during pregnancy, micronutrient deficiencies and iron deficiency anemia, regardless to their intake and linked to malabsorption or impaired intestinal motility which should be close monitored. The increased demand for nutrient supply to maintain fetal growth might lead to the possible risk of unbalanced nutrient transfer, if required diet has not reached.
The Impact of EDs During Pregnancy on GWG (See Table 2)
Studies carried out in longitudinal cohorts in Norway and the Netherlands exhibited higher and quicker GWG in women with EDs compared to controls. Micali et al. (60) described that women with AN had lower body weight but greater rates of GWG, whereas women with BN had higher body weight but lower rates of GWG.
Siega-Riz et al. (59) assessed GWG during pregnancy in the Norwegian Mother and Child Cohort Study in a cross-sectional approach. Authors demonstrated that women with AN had a lower risk of gaining inadequate weight during pregnancy, while women with BN and BED gained significantly more weight than those without an ED. Similar results were obtained by Zerwas et al. (65). These differences in GWG were linked to their eating pathologies, which persisted during pregnancy albeit more attenuate. Women with AN gained more weight than would be expected, probably because they exhibited the lowest pre-pregnancy weight, therefore evoking more concern for the unborn baby and undergoing partial remission of deregulated eating patterns. Gaining weight in women with ED might be protective for the increased demand of the fetus and it is the result of an improvement in ED behaviors and better control over purging patterns. The main limitations of these studies were the self-reported history of EDs and that GWG was based on maternal self-report which may underestimate it and induce bias. Moreover, large population samples included healthier patients with EDs than hospitalized women, and less severe symptoms were more likely to improve GWG.
Nonetheless, Koubaa et al. (82) found in a smaller sample, that anorexic pregnant women had considerably lower weight gain than controls (10.4 kg compared with 12.1 kg), demonstrating the persistence of restricted eating patterns and relapse of disordered eating during pregnancy. A possible explanation is that, in this study, patients with AN showed higher pre-pregnancy BMI if compared to the other studies, so the GWG was lower. On the other hand, women with BED who reported greater concern for GWG also experienced higher weight gain during pregnancy (57). Another study conducted in a small sample of ED patients found low GWG during every stage of pregnancy (63). This slow velocity of GWG may be explained by the most severe clinical manifestations in these samples of clinical patients with EDs, producing harmful effects on pregnancy and fetal outcomes.
The Impact of EDs on Pregnancy Outcomes (See Tables 3, 4)
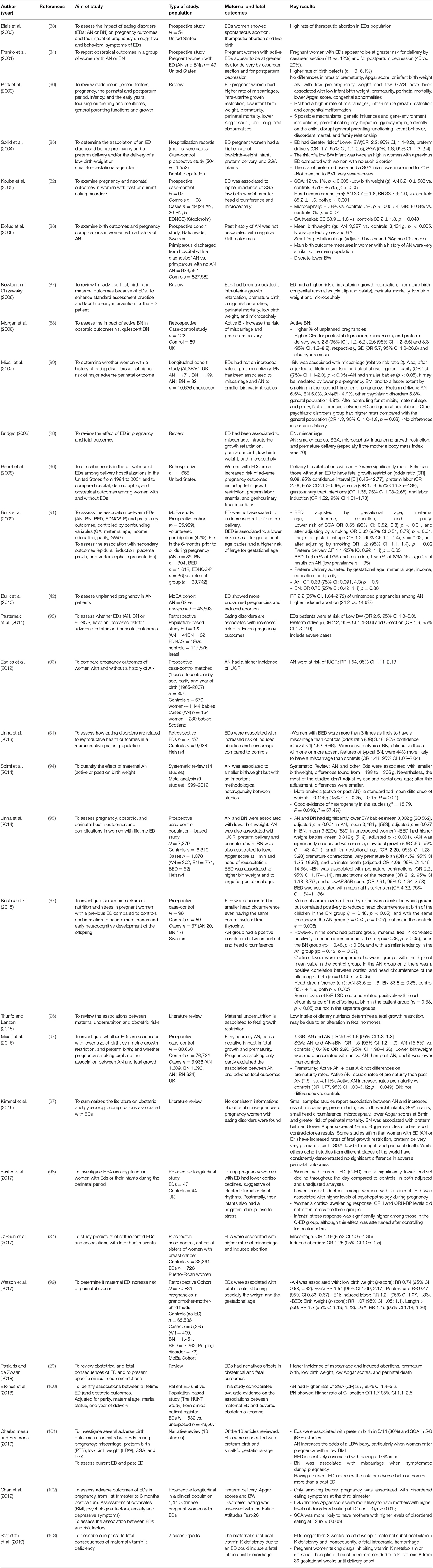
Table 3. Studies about the effects of eating disorders on pregnancy and fetal outcomes.
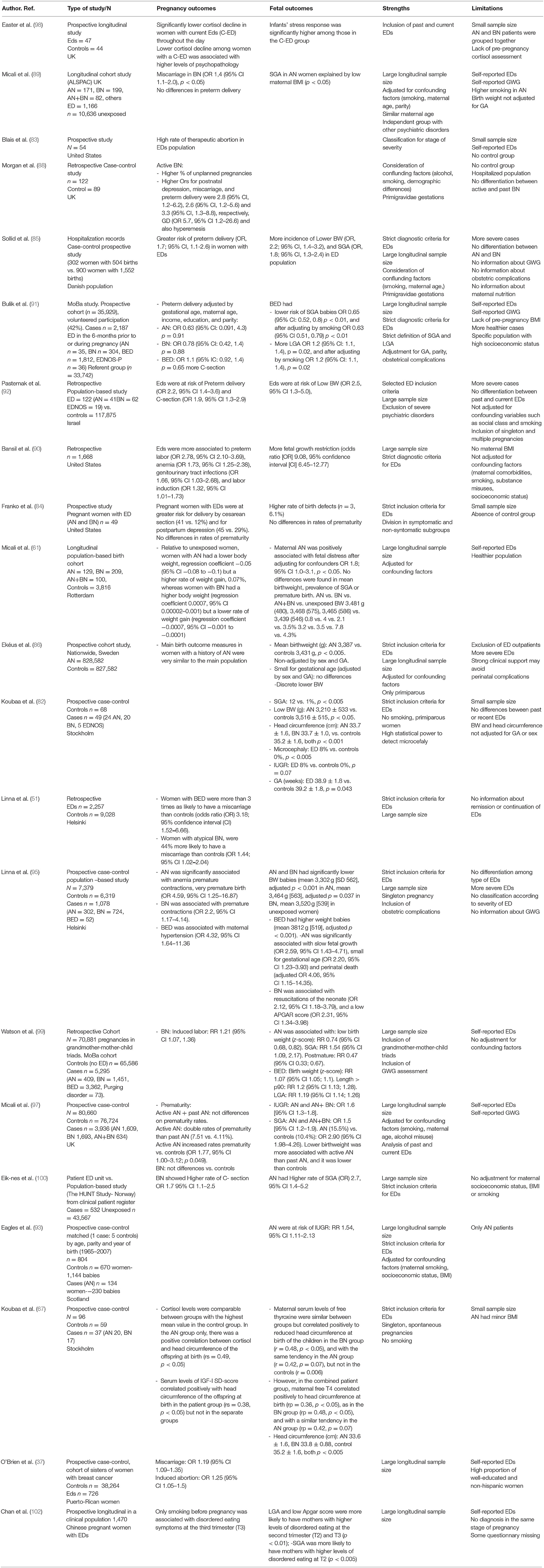
Table 4. Comparison among studies on pregnancy and fetal outcomes.
Endocrine Manifestations
EDs women display low levels of GnRH and consequently decreased levels of LH and FSH due to hypothalamic dysfunction. Moreover, even if in normal pregnancy leptin levels increase (104), low levels of leptin and peptide YY, both anorexic hormones, and high levels of ghrelin, an orexigenic peptide, have been described in women with EDs. The suppressed gonadotropin secretion in AN is associated with low T3 levels and low TSH, suggestive of a hypothalamic origin of suppressed thyroid function. Cortisol and CRH levels have been found to be elevated in women with AN and BN (105). GH levels are increased while IGF-1 levels decreased, demonstrating a GH resistant status as an adaptive mechanism to starvation. Most studies have also found increased levels of adiponectin in AN, which is inversely related to BMI and is associated with increased insulin sensitivity seen in AN women (106). Easter et al. (98) assessed HPA axis regulation in women with EDs. They observed different patterns of circadian salivary cortisol in pregnant patients, such as low morning cortisol levels, suggesting a blunted response of cortisol during the day. A possible explanation may be a decrease in HPA axis response due to a pre-gestational prolonged period of hypercortisol exposure in women with EDs. Moreover, this may be triggered by higher symptoms of anxiety and stress during pregnancy. The strength of this data was the longitudinal design and the inclusion of past and recent ED women. The limitations included that AN and BN patients were grouped together, the small sample size, and the lack of pre-pregnancy cortisol assessment. Further less, as depression or anxiety are multifactorial pathologies, it is difficult to establish a correlation with cortisol levels.
Hormonal changes might play a role in the remission patterns of EDs during gestation. It has been hypothesized that increased production of dihydroepiandrosterone (DHEA) by the placenta in patients with AN may counteract the adverse effects of cortisol, increasing the rate of remission during pregnancy (79).
Pregnancy Outcomes
Recent studies focused on pregnancy outcomes in women with EDs showed controversial findings. The main studies on ED population-based sample and clinical ED patients highlighted an increase in spontaneous abortion, particularly with BN (88), and also a high incidence of preterm delivery (42, 51, 83, 88, 89). These adverse outcomes may be promoted by multiple variables such as stress, hormonal imbalance, low leptin levels and conditions like PCOS. For example, low leptin levels have been associated with the risk of miscarriage, preterm delivery, and poor fetal growth (104).
The association between EDs and preterm delivery is controversial, and it was found more strongly related to hospitalized patients. Sollid et al. (85) designed a longitudinal case-control study, comparing pregnant women with EDs with healthy controls. They observed a higher risk of preterm delivery and small for gestational age (SGA) babies in the women with EDs but they analyzed more severe cases and they did not differentiate between AN and BN. Bulik et al. (91) found a higher rate of smoking, preterm delivery, and greater risk of delivery induction only in patients with BED. Additionally, in the BED population there was a higher risk to deliver a large for gestational age (LGA) newborn and a higher rate of cesarean section. Conversely BED women had lower rate of SGA probably because they gained more GWG. It is important to mention that the data was based on maternal self-report and this population had good socioeconomic status. Pasternak et al. (92) performed a retrospective study obtaining a higher rate of preterm delivery in more severe diagnosed ED women. This finding was associated with low pre-pregnancy BMI, low GWG, and higher rate of fertility treatment in the ED group. They also found a greater rate of cesarean section in BN and BED groups. Other retrospective study found similar results about the association between EDs and obstetric complications with no links to cesarean section (90). However, this study did not take into account confounding factors such as smoking and socioeconomic status. Conversely, Micali et al. (89) didn't find any association between EDs and preterm delivery although this study included a large longitudinal community cohort with less severe disease.
Franko et al. (84) reported greater risk for cesarean birth and postpartum depression in a group of women with AN and BN but no differences in the rate of prematurity. The limitations of these data were the absence of a control group, and the small group size. Neither significant differences in preterm delivery (61, 86), nor an increased risk of gestational diabetes (GD), hypertension, pre-eclampsia, induction of labor, instrumental delivery or postpartum bleeding were found in other prospective population-based studies in EDs women.
One potential explanation for these inconsistent results may be due to the inclusion criteria: in the population-based study, participants required only self-reported ED, whereas many clinical studies selected patients with EDs on the basis of hospitalization and with a more actively ED. Moreover, GWG improved faster in Norwegian and Dutch cohorts demonstrating the concern and support by caregivers to ED women and this may explain the lack of adverse outcomes.
Recent studies found a strong causal association between preterm delivery, fetal growth restriction, and low pre-pregnancy BMI, malnutrition and a low proportion of weight gain during pregnancy. This association remains after excluding pathologies such as diabetes and hypertension (107). A recent study conducted in a Norwegian population corroborated that higher diet scores, reflecting healthy dietary behaviors in the pre-pregnancy period and during pregnancy, prevent preterm delivery (108). Maternal stress in pregnancy and consequential high levels of CRH may also influence the timing of delivery and this could elucidate the risk of preterm labor in women with lifetime EDs (109). Furthermore, altered maternal mood and anxiety may damage the intrauterine environment, enhancing the risk of obstetric adverse outcomes (110, 111).
Although the association between EDs and poor obstetric outcomes is multifactorial, the severe of disease, the persistence of symptoms, low pre-pregnancy BMI and poor GWG, joined with environmental factors such as social dysfunction, potential stressors, smoking, drugs consumption and concomitant psychiatric disorders may worsen pregnancy evolution. However, a strong caregivers' and psychological support may avoid obstetric complication displaying normal pregnancy evolution.
Of note, a current ED increases the risk of adverse outcomes during pregnancy more than a past ED (101).
The Impact of EDs on Fetal Outcomes (See Tables 3, 4)
Available studies postulate the potential association between maternal EDs symptoms during pregnancy and adverse fetal outcomes. Fetal development is intrinsically linked to balanced maternal nutrition, correct placental supply, and fetal growth factors. Maternal malnutrition may affect fetal development through the absence of nutrients, which are essential for fetal growth, modifications of placental function, and epigenetic changes in the fetal genome. Furthermore, maternal stressors may alter the imprinting of fetal regulatory elements (112). According to the theory of “early life programming,” an altered intrauterine environment may predispose the offspring to the risks of developing chronic diseases later in life (113).
Not all EDs types (AN, BN, BED, and ENDOS) have been associated with the same fetal risks and not all studies evaluated independently each type of ED. Therefore, the conclusions obtained from the different studies and reviews are not consistent.
Small for Gestational Age (SGA) and Intrauterine Growth Restriction (IUGR)
Population-based studies have shown that neonates of pregnant women with EDs are at higher risk of lower birth weight (BW) than those of healthy pregnant women. Although they included large sample size, one important limitation of these types of studies was the classification of EDs based on self-reported questionnaires. Furthermore, it is important to highlight that a large number of studies did not use the proper definition of SGA (weight percentile <10 adjusted for gender and gestational age) to evaluate neonates. For example, the study of Micali et al. (89) showed an association between AN and lower BW. This large sample size included more than 1,600 pregnant women who were classified as EDs with psychiatric disorders (n = 1,166), BN (n = 199) AN (n = 171), and AN+BN (n = 82). The data was adjusted by parity, maternal age, and smoker habits but the proper definition of SGA was not applied. The study of Watson et al. (99) also found a strict association between EDs and low BW and concluded that maternal EDs increase the risks of pregnant and neonatal complications, even when there is a correction for perinatal outcomes in the previous generation. In a similar line, Micali et al. (97) observed a higher odds of SGA (defined as birthweight <10th percentile) in both AN and BN (OR 1.6, 95% CI 1.3–1.8; OR 1.5, 95% CI 1.2–1.9, respectively) being more associated with active AN than with past AN.
Furthermore, longitudinal prospective studies conducted in Danish, Swedish, and Norwegian populations among hospitalized pregnant women diagnosed with ED according to strict criteria reported a higher incidence of low BW and SGA (82, 85, 95, 100). However, the women included in these studies were hospitalized, so they represented the most severe cases. The main limitation of Kouba's study (82) was the reduced sample size and the lack of differentiation between past or current ED. The main limitation of the study of Eik-nes et al. (100) was that, although they registered smoking and socioeconomic status, they did not consider these data to adjust the results. Recent systematic reviews (27, 28, 87, 94) supported these findings indicating that EDs are associated with low BW.
Conversely, other studies conducted in pregnant women with a clinical diagnosis of EDs, did not find differences in the association among EDs and low birth weight or the incidence of SGA (84, 86). Nevertheless, these studies included women who required hospitalization, and pregnant patients were strictly monitored and consequently this may reduce the number and severity of perinatal complications. Moreover, the study of Franko et al. (84) did not include a control group and Ekeus et al. did not report GWG, which could be a protective factor for impaired fetal growth.
With regard to IUGR, several studies corroborated the higher incidence in pregnant women with EDs, if compared to general population. Bansil et al. (90) analyzed a retrospective cohort of pregnant women with 1,668 cases of strictly classified EDs, observing an increased risk of IUGR (OR 9.08 95% CI 6.45–12.77). However, in this study the outcomes were not adjusted for maternal BMI, neither for confounding factors such as maternal comorbidities, tobacco habit, substance misuses and socioeconomic status. Eagles et al. (93) found similar conclusions in a case-control study with a larger sample size evaluating pregnant women with a clinical diagnosis of AN (134 cases), adjusting the results for confounding factors such as maternal BMI, smoking, and social class. Indeed, Kouba et al. (82) did not find those differences, but the study was conducted in a small sample size.
Therefore, we can state that generalization of these results is limited because of the diversity of study designs, the inclusion of different populations with wider range of severity, or small sample sizes. Nonetheless, updated literature endorses the notion that EDs during pregnancy may increase the risk of having a baby with low BW or SGA. The severity of EDs and an active ED have been associated with more risk of IUGR. Moreover, the strongest relationship between EDs and low BW was found in patients with low pre-pregnancy BMI and/or low GWG. In the aforementioned studies, the mean maternal body mass index was lower in the exposed than in the unexposed group. Smoking, also may interact in the delivery of low BW babies. Nevertheless, the majority of such studies didn't stratified their results for BMI categories and few studies reported GWG or nutritional status of the mother (89, 95, 99).
Large for Gestational Age (LGA)
Two case-control studies, both with more than 1,500 cases of EDs, concluded that pregnant women with an ED (BED subtype) had a higher risk of having LGA neonates (91, 99). Even more, they showed a strong association between BN or BED and gestational diabetes, which may clarify the greater incidence of LGA. Watson et al. (99) also found in BED patients a high incidence of neonates with length over the 90th percentile. The main weakness of these studies were that ED diagnosis was self-reported and in the study of Watson et al. statistical analysis was not adjusted for possible confounder factors (99).
The studies by Linna et al. (95) and Watson et al. (99) also showed that pregnancies in women with BED were more likely to be prolonged. However, they did not obtain the same magnitude of estimated risk (95, 99).
Additionally, a recent research found that women with BED had higher intake of saturated fat during pregnancy, which may explain the relationship between BED and larger size of newborns (56). Women with BED were also found to gain more gestational weight during pregnancy, affecting the fetal size (61).
Perinatal Mortality and Lower Apgar Score
Few data evaluated Apgar score and perinatal mortality in women with EDs reporting contrasting results so there is a lack of evidence to state that EDs is a risk factor for perinatal morbidity and mortality. In the case-control study of Linna et al. (95) neonates of pregnant women with BN exhibited lower Apgar at minute one and they needed more resuscitation in delivery room, but the most severe cases with binge and purge episodes were included in this study, increasing the risk of bias. Conversely, in the cohort of patients with EDs studied by Franko et al. (84), no differences were found in the Apgar score according to the diagnosis of AN or BN in pregnant women. However, this study was performed in a small sample size (only 49 EDs patients) and the results must be interpreted carefully because ED groups were not compared to a control group.
Regarding perinatal mortality, the case-control study of Eagles et al. (93) did not report increased risk in neonates of pregnant women with AN, but the study was conducted in a specific population with higher GWG which may mitigate the poor outcomes associated to EDs. Nevertheless, in the literature, the relationship between perinatal mortality and EDs has been widely reviewed (30, 87). Therefore, newborns of pregnant women with EDs are at risk of perinatal mortality if compared to general population. The relapse and exacerbation of ED symptoms during pregnancy is the most evident mechanism linked to perinatal mortality.
Lower Head Circumference(Microcephaly), Malformations, Intraventricular Hemorrhage
Two case-control studies showed lower head circumference and a higher incidence of microcephaly in neonates of pregnant women with EDs. Kouba et al. (82) were the first to describe this notion, considering that it could be due to high levels of maternal cortisol produced by stress, especially in pregnant women with AN who had a BMI <20. Another subsequent study by Koubaa et al. (67) concluded that neonates of primiparous and no smoking pregnant women with EDs, showed better head circumferences, even with the same serum levels of thyroxin, a hormone which correlated positively to head circumference. The authors concluded that, in pregnant women with AN, there was a correlation between maternal cortisol levels and neonatal cephalic perimeter. In three previous reviews on the fetal repercussions of maternal EDs, a correlation with lower head circumference was found; however, these results were observed in small sample sizes, and in the most severe ED patients but not in larger studies (27, 28, 87).
With regard to congenital malformations the reviews of Park et al. (30) and Newton et al. (87) stated that children of pregnant women with EDs showed increased incidence, but these reviews included previous studies dating back in 80's and 90's. Only Newton et al. detailed that these malformations were cleft lip and cleft palate (87).
Eight cases of prenatal intraventricular hemorrhage have been described, attributable to maternal vitamin K deficiency secondary to poor intake, or intestinal malabsorption. Placental transfer of vitamin K is scarce, and it is estimated that its concentration in cord blood is 1/30 with respect to maternal plasma levels, so a severe deficiency has been found in malnourished mothers (103).
Therefore, actually the link among EDs during pregnancy and microcephaly or malformations need more controlled studies to corroborate it, including the correction for several confounding factors such as maternal drugs, alcohol misuse, smoking, or severe maternal malnutrition.
Possible Causes for Poor Fetal Outcomes
Some studies tried to find a positive association between mothers with EDs and adverse pregnancy outcomes, impaired fetal growth, malformations, and poor prognosis in their offspring. In accordance with the theory of “fetal programming,” the nexus between nutrition and stress in pregnant women with EDs triggers the activation of maternal and fetal HPA axis, increasing levels of maternal CRH (96). As consequence, higher levels of glucocorticoids in fetal circulation have an impact on fetal programming and neural development, and are associated with low birth weight (114, 115). Smoking is frequent in AN patients, linked to the desire to control weight and appetite. Nicotine release appetite suppressors in the brain (serotonin, dopamine, and norepinephrine), which are also associated with impaired fetal growth (102, 115). In addition, the use of laxatives, diuretics, and appetite suppressants have been described to cause possible teratogenic complications (85). If nutritional deficiencies such as low iron or folate levels, low fish intake which is a source of iodine, L-PUFA and vitamins are mixed with maternal stressors, the risk of neural tube defects (67, 115), small head circumference and impaired cognitive development increases (116, 117). Furthermore, thyroid function and IGF-1 axis, essential for fetal growth, may be compromised in pregnant women with EDs (67).
The inconsistent of several studies is probably due to the difference in the severity of illness between the clinical vs. the population-based sample, finding a stronger association of poor perinatal outcomes among the most severe cases of EDs. Moreover, the presence of confounding factors were not taken into account in some studies, such as maternal age, severe psychiatric pathology, maternal BMI, or toxic habits like tobacco, drugs, or alcohol. Furthermore, the majority of the studies didn't differentiate between past or active EDs.
Epigenetic Modifications: Association With EDs and Nutritional Deficits During Pregnancy (See Table 5)
Barker's hypothesis defines fetal programming as the process of fetal adaptation to the environmental conditions during development (113). Therefore, EDs or a specific nutritional deficiency during pregnancy produce severe alterations in maternal and fetal epigenetic profiles (124). Epigenetic mechanisms as the DNA methylation of CpG islands, the Histone tail modifications by enzymes as well as the expression control by microRNAs regulate the genomic imprinting, modulating cellular differentiation and organogenesis during fetal development (125).
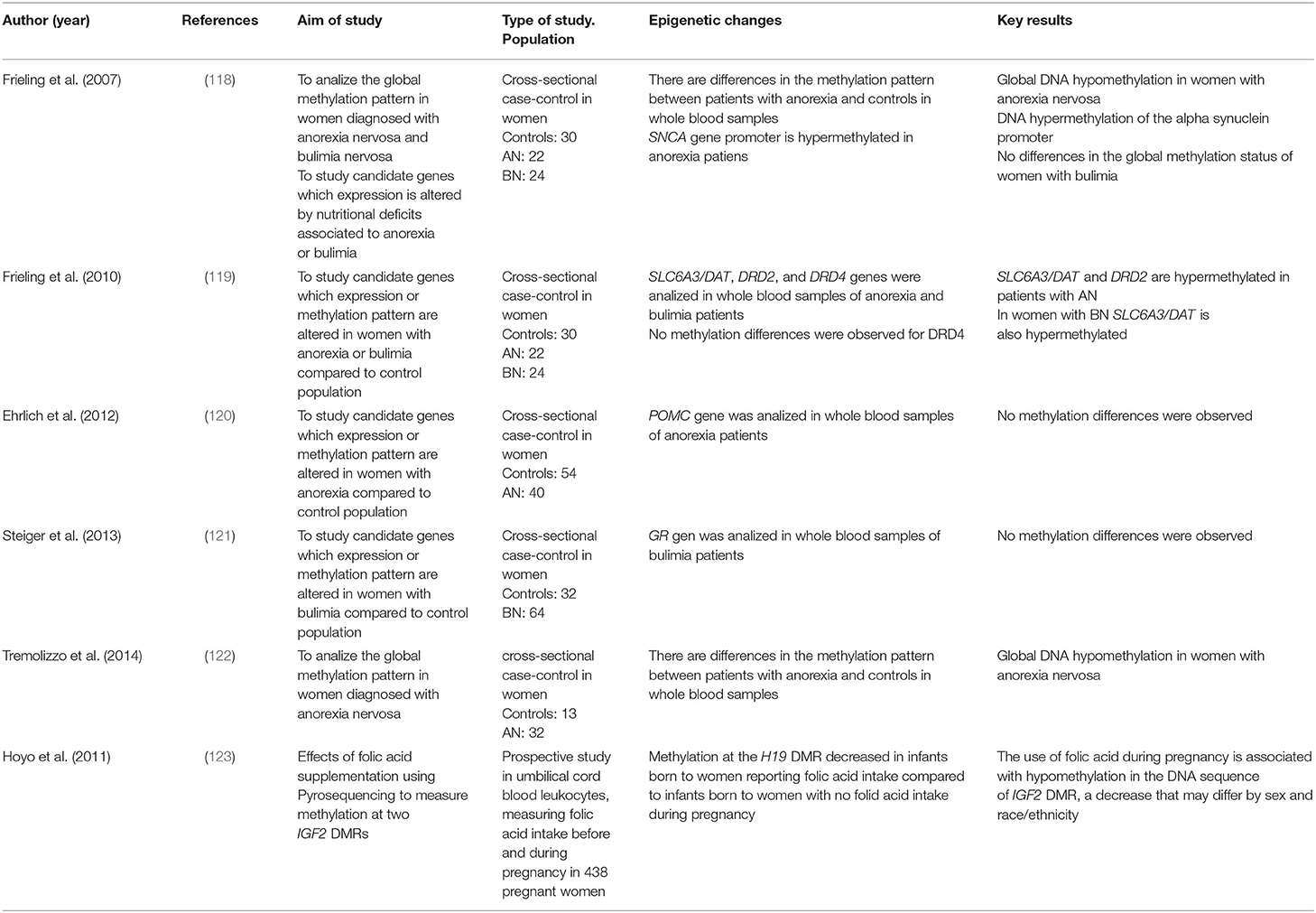
Table 5. Studies about the effects of eating disorders on epigenome.
Different nutrients are able to influence and modify these processes and therefore the epigenetic pattern, in the mother and the fetus during pregnancy, which is the most sensitive period to epigenetic changes that will persist in adult life (126). Micronutrients such as folic acid, choline, methionine, and vitamin B12 are involved in the folate pathway. The synthesis of methionine provides the methyl groups to DNA methyltransferases DNMTs1,3a, and 3b as well as Histone methyltransferases (HMTs), necessary for the global regulation of gene expression. Therefore, a deficit of one of these bioactive compounds alters the pattern of gene expression during development (127, 128). For this reason, the diet of pregnant women is always supplemented with folic acid (129). Moreover, antioxidants such as polyphenols, present in fruits like grapes and vegetables, green tea (EGCG), genistein, and curry, act by inhibiting DNMTs. These enzymes control the levels of oxidative stress, which negatively influences the metabolic profile during fetal development, predisposing the fetus to pathogenic alterations (130, 131).
Maternal malnutrition has been linked to epigenetic alterations such as the methylation (silencing) of the IGF2 gene, a key growth factor in fetal development (123). Higher levels of methylation in genes related to hepatic and cardiac function (CACNA1C and PDE1A related to intracellular calcium balance), inflammation (IL10, IL6), lipid/carbohydrate metabolism such as ABCA1 (related to cholesterol homeostasis), LEP (which regulates the synthesis of leptin that controls body weight), and GNASAS (which regulates hormonal metabolism) also appear associated with suboptimal maternal nutrition (132, 133). In accordance with Barker's hypothesis, other studies indicate that maternal malnutrition generates precocious insulin resistance which may accelerate early postnatal growth by shifting toward body fat instead of muscle mass (134). Some studies have associated DNA methylation in obesity markers with infant adiposity. Godfrey et al. (135) found a positive association between high methylation levels of RXRα and NOS3 genes in umbilical cord cells and adiposity in infants. On the other hand, a maternal high-fat diet present in BN and BED correlates to the origin of other metabolic diseases as hypertension and diabetes through changes in the hypothalamic region. A diet rich in fats also modifies the methylation status and the expression of genes related to the mesocorticolimbic reward circuit (dopamine and opioids) (136). Hyper-methylation of Leptin receptor, melanin-concentrating hormone receptor 1 (MCHR1), and proopiomelanocortin (POMC) was also related to an increase in body mass index (BMI) and a higher risk of obesity (137), also modifying energy homeostasis in the offspring (138). The permanent deregulation of the hypothalamic circuits promotes resistance to insulin and leptin, generating an increase in overweight status and food intake.
Other genes silenced by a high-fat diet and recently related to obesity are FYN (a member of the Src family of non-receptor tyrosine kinase related to inflammation, adipocyte differentiation, and insulin signaling), TAOK3 (an activator of the protein kinase MAPK cascade which affects fundamental cellular signaling pathways), PIWIL4 (a regulator of adipocyte proliferation) (139), and SIRT1 (expression stimulates the metabolism of fats in adipocytes by suppressing the Peroxisome proliferator-activated receptor PPARγ, also participating in the regulation of glucose homeostasis, anti-inflammatory activity and oxidative stress) (140). Therefore, a maternal diet rich in fat decreases the expression of SIRT1 in the fetal liver and heart, altering the fetal metabolism and generating a tendency to increase body fat.
Nutritional deficits associated with low protein intake typical of AN patients show harmful effects on fetal growth and a higher risk of obesity, diabetes, and hypertension in the offspring. These effects are caused by a deficit of folic acid, choline, and methionine. The deficiency of gestational proteins generates: hypomethylation of the Wnt2 promoter in the placenta associated with fetal growth alterations (141); decreased expression of IGF-I and IGF-II producing hyperglycemia (142); hypermethylation of the PPARγ and Glucocorticoid receptor (GR) promoters involved in the regulation of blood pressure and in the metabolism of lipids in adults (143); increased expression of angiotensin II which generates an increase in blood pressure (142) and decreased expression of the agtr1b gene involved in hypertension.
A maternal protein-restricted diet during pregnancy is also associated with hypermethylation of key adipogenesis genes such as the peroxisomal proliferator-activated receptor-α (PPAR-α) related to cardiomyopathy in the offspring and liver X-receptor promoter (LXR)α involved in glucose homeostasis in the fetal liver (144). In addition, diets with protein deficits regulate the expression of microRNA related to chronic inflammation in offspring (145), as well as the over-expression of the transcription factor C/EBPs (CCAAT-enhancer-binding protein) which regulates the expression of genes involved in energy homeostasis (146).
In the gene-environment interactions, the extreme nutritional conditions associated with EDs such as AN, BN, and BED, have been deeply studied in the pregnancy period, because these disorders alter the epigenetic pattern of the mother and the developing fetus (147). Several studies postulated that environmental factors that favor thinness can lead to the overexpression of genes that suppress appetite and/or reduce body weight in individuals that are already genetically susceptible to low BMI and reduced percentages of body fat. When the complete genome methylation status is considered, instead of specific promoter regions of candidate genes, patients with anorexia and also patients with bulimia show a clear hypomethylation in their epigenome compared to healthy controls (118, 122). This phenomenon is produced by the deficit of folate and methionine, with a consequent decrease in the activity of DNMTs and HMTs, low protein intake, and very low levels of glucose and cholesterol in the blood (148). A recent study performed in 21 active ED, 43 past ED and 126 controls concluded that offspring of women with an active restrictive ED during pregnancy showed lower global methylation pattern in their genome compared to offspring of women with past restrictive ED. This study also demonstrated a decreased methylation at the DHCR24 locus in offspring of women with active ED during pregnancy and an increased methylation at the LGALS2 locus in offspring of women with past ED compared to controls (149).
Some differences in the expression of genes related to dopamine metabolism have been observed in patients with anorexia. An increase in the expression of the dopamine transporter SLC6A3 and a decrease by hypermethylation of the dopamine receptor D2 (DRD2) promoter have been associated with the reward effect in individual diagnosed with AN (119).
Along the same line, the hypermethylation of the POMC gene, a key regulator of appetite, and also the oxytocin receptor gene OXTR, negatively associated with BMI, has been observed in patients with AN (120). Moreover, a decrease in the mRNA levels of the glucocorticoid receptor gene NR3C1 has also been observed in the anorexic population (121). Finally, maternal psychosocial stress may alter placental imprinted gene expression, and lead to suboptimal fetal growth (150).
Other environmental factors such as smoking, alcohol, and drugs of abuse, which show higher percentages of consumption in ED patients than general population (151–153) may promote alterations in the epigenetic pattern of the mothers diagnosed with ED and their offspring (154). In a cohort of 40 patients diagnosed with EDs, Ehrlich et al. demonstrated than the methylation state of the Pro-opiomelanocortin (POMC) promoter was negatively affected by smoking but it was not influenced by the nutritional status (120). The co-occurrence of smoking and ED modify the epigenome during pregnancy affecting fetal development. A Recent study determined the effect of smoking during pregnancy in the hypomethylation of the Aryl hydrocarbon receptor repressor gene (AHRR) observed in neonates (155). Moreover, prenatal alcohol exposure produces severe impairments in fetal development which can result in fetal alcohol spectrum disorders (FASD). Alcohol can alters one carbon metabolism, critical for methylation of DNA, directly inhibiting the key enzymes methylenetetrahydrofolate reductase (MTHFR) and methionine synthase (MTR) (156, 157). Furthermore, recent studies have demonstrated in prenatal alcohol exposed children a differential methylation pattern in the genes SLC6A3 and DRD4 related to the dopaminergic system; in HLADPB1 and CD11A related to the immune response; and in H19 and SLC22A18 genes (158–160).
It is important to mention that some of the hormonal imbalances observed in EDs patients, as high cortisol and low sex hormones levels, can be promoted by environmental factors and they can influence the dynamics of the gene expression. These hormones can behave as direct ligands to promoters or key regulators which interact with transcription factors, altering the expression pattern of the epigenome (161, 162).
A large amount of epigenetic studies has focused on AN whereas the studies about BN are less abundant, and, in the case of BED, there are only few publications in human subjects. Additionally, most of these studies have small sample sizes, so it is necessary to perform studies on a larger scale to confirm these results. Finally, EDs are mainly brain disorders, so that some epigenetic alterations are specific of the nervous tissue. However, the majority of the published studies are performed using saliva or blood samples, which is a limitation to take into account for future studies.
EDs During Pregnancy and Maternal Psychopathology (See Table 6)
Comorbid emotional disorders are common in women with EDs who typically experience depression, anxiety, or obsessive compulsive disorder (168). Recent evidence shows higher rates of depression and anxiety throughout pregnancy and during the postpartum period in women with active EDs related to their shape and weight concern (88, 89). Moreover, childbirth may trigger or relapse the onset of a comorbid psychiatric illness in the mother. Altered mood may impair the normal course of pregnancy and fetal development leading to adverse perinatal outcomes such as prematurity, SGA and IUGR babies (110). Furthermore, the post-partum period is the one at highest risk for worsening a depressive disturbance, particularly in women with an ED (84, 166), because infant feeding, maternal-child bonding, and the desire of weight loss, may exacerbate ED symptoms and lead to a mood disorder. Maternal adjustment during the first 3 months after delivery was clearly impaired and related to mental disturbances in mothers with EDs before pregnancy (164). Misuse of alcohol at conception, lower BMI, higher frequency of binging after delivery, and a history of AN, increased the risk of post-partum depression symptoms (169).
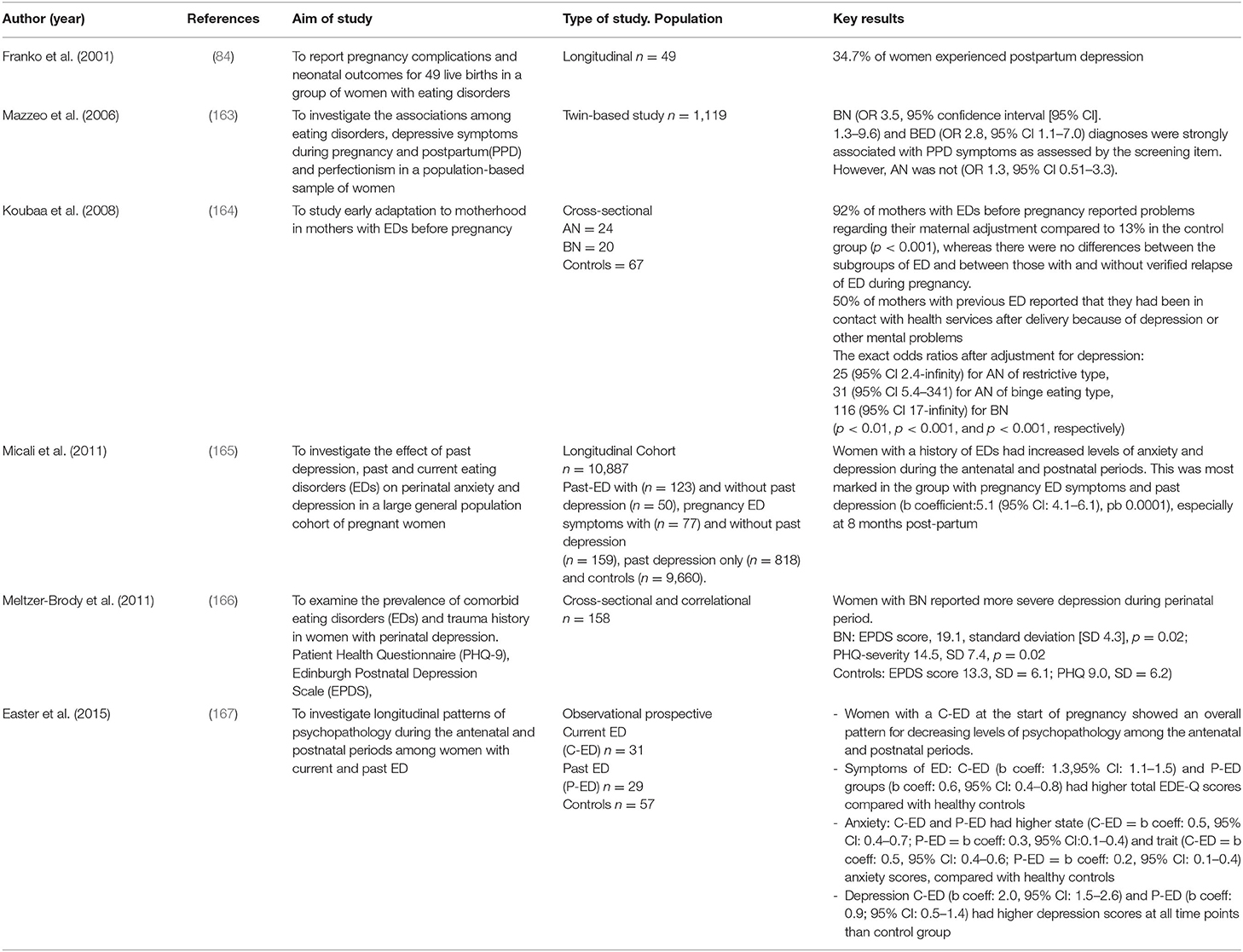
Table 6. Studies about comorbid psychopathology among pregnant women with eating disorders.
Easter et al. (167) investigated longitudinal patterns of psychopathology during the antenatal and postnatal periods among women with current and past EDs. They found decreasing levels of psychopathology at the start of pregnancy in women with current ED. However, symptoms of anxiety, and depression remained high at all pregnancy stages. In contrast women with a past ED were at risk of increasing psychopathology throughout pregnancy and during the postnatal period. The strengths of this data were the longitudinal design and the strict inclusion criteria of EDs, but the main limitation was the small sample with insufficient power to detect potential differences. Mazzeo et al. (163) assessed the association among EDs, depressive symptoms, and perfectionism during pregnancy or post-partum in a population-based sample of pregnant women. This data showed a higher rate of depressive symptoms during pregnancy and post-partum in women with a history of EDs, in particular in women with BN and BED, and the authors found a relationship between symptoms of depression and aspects of perfectionism. One limitation of this study was the lack of information regarding the timing of the beginning of the depressive symptoms and the diagnostic criteria of post-partum depression. Along the same line, Micali et al. (165) investigated the effect of past depression, and past or current ED, on perinatal anxiety and depression in a large general population cohort of pregnant women. They found that women with a history of an ED had increased levels of anxiety and depression during the antenatal and postnatal periods. ED symptoms and past depressive episodes were related to the highest risk for a depressive and anxiety disorder during pregnancy. Data was limited to a self-reported assessment of psychiatric history. One possible explanation of these results is that women with EDs are predisposed to develop an affective disorder and this condition together with the stressful stage of pregnancy, aggravated by body image concern, weight gain, and loss of control, may trigger a psychiatric illness (28). Another possible reason may be associated with nutritional deficiencies, for example zinc deficiency has been linked to depression symptoms (58). Low levels of micronutrients like folate, vitamin D, vitamin B12, iron, selenium, and fatty acids, which are essential for the biosynthesis of several neurotransmitters (serotonin, dopamine, and norepinephrine) have been linked to perinatal depression (170). Furthermore, elevated levels of cortisol described in patients with EDs have been associated with most forms of depression (171).
The Effects of EDs on Postpartum Course, Breastfeeding, and the Composition of Human Milk
Kouba et al. (164) described that women with EDs had more problems regarding their adjustment to the new maternal situation at 3 months post-partum. Although the prevalence of postpartum remission was high, EDs continued in a large proportion of women and, in the postpartum period, women with EDs experienced a decrease in BMI during the first 6 months after delivery (65).
If the onset of EDs was before pregnancy the proportion remitting was significantly low. The presence of binge symptoms or compensatory behaviors during pregnancy, expressed a more severe form of BN, which persisted in the postpartum period. Higher BMI and psychological dysfunction were associated with continuation of BED during postpartum (172). Furthermore, a retrospective case-control study demonstrated that a third of women with EDs developed postnatal depression increasing the risk for relapse of EDs (88).
Some studies showed an increased rate of breastfeeding among women with current or prior EDs related to the motivation and the desire for weight loss, while other studies found low incidence (20, 165). Nevertheless, mothers with active or paste EDs reported problems when giving human milk, such as scarce lactation and precocious finalization of breastfeeding (46). Torgersen et al. (173) conducted a large population-based study and reported that women with EDs started breastfeeding in the same proportion as women without EDs. However, women with EDs were more likely to stop breastfeeding earlier than the control group. Women with BED had a lower rate of lactation. A possible explanation was that women with EDs felt embarrassment when breastfeeding and they showed high shape dissatisfaction and lower self-esteem. Moreover, they had low social support and felt depressed when breastfeeding. Stress has also been related to the short duration of lactating period (174). Low leptin levels in ED patients could influence the capacity to regulate the mechanisms of satiety in breastfed infants, leading to lactation failure (175). Squires et al. (176) showed that ED women were likely to have less mother-infant interaction during feeding. They described that such mothers were less sensitive when feeding their babies, more stressed, and with dysregulated interaction patterns.
To our knowledge there is a lack of studies regarding the composition of human milk in ED patients. A recent study described that the variance in milk fat content has been associated with BMI, and maternal body composition may be related to the nutritional value of human milk (177). We may speculate that mothers with an ED have low pre-pregnancy nutritional status that can lead to low maternal fat stores for lactation, and low nutritional amounts for the baby. For example, lower iron and vitamin B12 intake in mothers with an ED may cause deficiency of these elements in breastfed infants with consequent neurological disabilities (178). Moreover, low maternal vitamin D status described in AN patients may affect vitamin D quantities received by the breastfed neonate (179).
EDs During Pregnancy: Risk Factors and Psychological Intervention
The most important risk factors linked to the onset of EDs during pregnancy are: (24, 102) personality characterized by low self-esteem and perfectionism; mood disorders such as depression, anxiety and obsessive-compulsive disorder; a history of social dysfunction, maltreatment or sexual abuse; toxic consumption like smoking, drugs of abuse and alcohol; inadequate or excessive stres; greater BMI changes from pre-pregnancy period; unplanned pregnancy and lower marital and social support. The major risk factor is a past history of EDs or family history of EDs (180).
Psychological intervention focused on symptoms of dietary restriction and overevaluation of shape and weight, helps the patients to establish a pattern of regular eating, avoid compensatory behaviors and reducing dieting in order to address motivation (181).
Nevertheless, there is a lack of clinical trials about psychological intervention in pregnant women with EDs. The treatment includes Cognitive Behavioral Therapy (CBT) and Interpersonal Psychotherapy (IPT) which have been used as treatments for prenatal and postnatal depression demonstrating potential benefits but it is difficult to know which is the most effective (14, 182). The goal is to maintain regular eating patterns and optimize nutritional intake for the mother and fetus (183) The body of evidence supporting IPT use is far more modest than it is for CBT (184). CBT reached higher rates of remission in patients with BN and BED (185).
EDs During Pregnancy: Target Therapy
Based on current evidence pregnancy is a critical period for an intervention in EDs women which should be strictly monitored prior, during, and after pregnancy. Nonetheless, there are several challenges for clinicians. The best approach for pregnant women with EDs implies a multidisciplinary management comprised of gynecologists, midwives, nutritionists, and mental health professionals working as a team. However, there is an insufficient medical training to openly discuss eating behaviors with the patient (29). Women with EDs do not often disclose this information to clinicians due to fear of stigmatization or misunderstanding. Some questionnaires are applied to ED identification, but none of them are specific to pregnant population. UK guidelines (NICE) suggest asking one or two specific questions. The SCOFF questionnaire has been also proposed (6). Recently, Emery et al. reported a structured clinical interview to assess disordered eating patterns among overweight and obese pregnant women [The Eating Disorder Examination Pregnancy Version (EDE-PV)] (186). Identifying women with EDs but with normal weight is still more difficult.
Otherwise pregnant women with EDs show a specific nutritional patterns: many of them are vegetarian (or with a lower intake of meat), they smoke and consume high amounts of coffee and do not show significant deficiencies in mineral and vitamins (60). Moreover, dietary supplements are similar between pregnant women with and without EDs (187). Therefore, pregnant women with EDs should receive accurate information from a dietitian about a balanced diet involving food from each nutritional group correctly represented and also about daily energy requirements, not only during pregnancy, but also during post-partum and breastfeeding (80).
It is also important to mention that the use of psychotropic, analgesic, and gastrointestinal medication should be assessed (188). AN or recurrent self-induced purging in the absence of binge eating (EDNOS-P) was directly associated with the use of anxiolytics and sedatives post-partum (adjusted RR: 5.11, 99% CI: 1.53–17.01 and adjusted RR: 6.77, 99% CI: 1.41–32.53, respectively). The use of analgesics was higher in pregnant women with BED, and laxatives were also used by all women with EDs, before, during, and after pregnancy. In severe cases of BN, antidepressant medication could be needed. The most common are selective serotonin reuptake inhibitors (SSRIs) (14). Clinicians should be encouraged to query about patients' medication and provide evidence-based counseling about the risks of treatment exposure vs. the risks of untreated psychiatric diseases.
Discussion (Table 7)
The incidence of EDs has increased globally in the last years, particularly in developed countries. These disturbances start at an early age in adolescent girls due to the social pressure about body shape stereotypes and the impact of beauty canons showed in social programs or mass media. Slimness reflects healthy nutritional habits if it is not associated with self-destructive behaviors, emotional dysregulation, excessive pursuit of thinness, and restrictive and bulimic eating patterns, typical of EDs. The combination of body changes during puberty, anxiety, and psychological disorders may trigger the first episodes of vomiting and purging, becoming into pathologically dysfunctional eating behaviors (55).
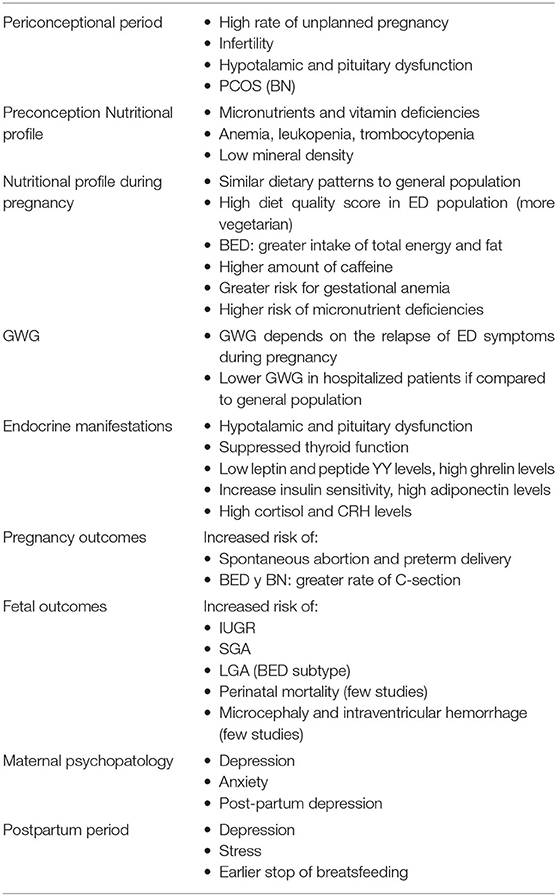
Table 7. EDs during pregnancy: bullets points.
Stress and anxiety may play a critical role in the onset of EDs. Binges and purging episodes are described more likely to happen in response to environmental stressors. Stress promotes long-term maladaptive modifications in neural circuits that regulate food intake, included neuroendocrine and sympathetic pathways (189).
Patients present a deficit in emotion regulation abilities in response to an acute psychosocial stressor (190). Stress itself may complicate the course of pregnancy and can cause preterm deliveries or intrauterine growth restriction, regardless the diagnosis of ED (191).
Women with EDs may display severe malnutrition, leading to hypothalamic dysfunction, low bone mass and precocious osteopenia (44, 62). Moreover, patients with AN have been found to have at least one vitamin and trace element deficiencies suggesting an alteration of micronutrient status (71).
In this line diet is one of the most important factors during pregnancy, which may program the health of the offspring. Therefore, unbalanced diet may predispose the developing fetus to several diseases in adulthood as the demand of macro and micronutrients increases during pregnancy (192–195). Furthermore, a malnutrition status as well as alterations in hormonal pathways may reduce but no abolish fertility in ED women, leading to an insufficient use of contraception and therefore producing a high incidence of unplanned pregnancy. This condition promotes an additional risk of impaired fetal development due to the lack of concern about prenatal care (abstinence from alcohol, no smoking, multivitamin supplements, and balanced nutrition) (42).
Pregnancy represents a period of increased vulnerability, which may trigger dysfunctions on the eating patterns or may be a chance to improve and treat EDs due to the concern for the unborn baby and a different perception of body image during gestation.
Our systematic review displays a global overview about the impact of EDs during pregnancy explaining its multifactorial mechanisms.
Patients with EDs show adverse pregnancy outcomes such as miscarriage, preterm delivery, or fetal disabilities as poor fetal growth or malformations. However, the multifactorial origin of EDs as well as the limited experimental studies performed in humans make difficult to establish a clear relationship between EDs during pregnancy and birth impairments. Maternal malnutrition and poor GWG suggesting a relapse of EDs symptoms alter the fetal supply of nutrients and trigger the deregulation of several hormonal pathways, increasing the risk of damage to intrauterine environment. An altered nutritional pattern in mothers, also induce epigenetic changes in the global expression pattern of the fetus, which will trigger biological and psychological alterations in offspring lifelong outcomes. Additionally, substances of abuse such as alcohol, narcotics, or tobacco, more frequent in EDs patients, may have a comorbid impact on fetal development. These environmental factors also produce changes in the global pattern of gene expression as well as hormonal imbalances. So that, they represent some of the multifactorial variables that strongly influence the epigenetic profile of the mothers with EDs and their offspring.
Considering the evidence that previous and most severe EDs are at the highest risk of fetal impairment, it is imperative to detect altered eating patterns in childbearing age women during the pre-conception period. Once diagnosed, a multidisciplinary team have to start the treatment for the specific ED detected, which includes nutritional support, a screening related to alcohol and drugs of abuse, psychotherapeutic techniques, and the use of psychotropics if necessary. Early detection is essential to prevent malnutrition, mental and somatic comorbidities, and the relapse of symptoms during gestation with consequent poor obstetric and fetal outcomes. An early intervention will empower the woman to her own care and would avoid lifelong morbidity for both mother and fetus.
The present study has been performed following the PRISMA methodology for systematic reviews and the authors' clinical experience.
However, some of the studies explored in this review show opposite results probably because they investigated different populations with different health conditions: for example, hospitalized patients with severe EDs vs. a sample of general populations with self-reported EDs.
An important bias in the majority of the papers evaluated was the diagnosis of maternal EDs by self-reported screening and the dietary intake through a food frequency questionnaire. The main limitations of these questionnaires were the different food lists and the possible mistakes in self-reporting. Moreover, the self-reporting method for determining the inclusion criteria of EDs usually underestimate their prevalence as well as some important features such as mental mood, GWG, and nutritional status of the mother. Otherwise the fetal adverse outcomes have multifactorial causes, so a combination of several comorbid disorders may impair fetal development such as undernutrition, psychiatric pathologies, or substance abuse besides EDs. Moreover, a large number of studies did not distinguish between past or active EDs and several studies did not adjust for confounding factors such as smoking, drugs, pre-conception maternal BMI or the severity of the illness, generating biases.
Pregnant ED patients may display a good gestational evolution if they reach a healthier BMI preceding pregnancy, a correct GWG, a balanced nutrition, and a healthy mental state of the mother.
Nevertheless, the recognition of dysregulated eating patterns is a challenge for clinicians due to the lack of a standardized screening method during pregnancy. EDs impair gastrointestinal function leading to esophageal acidic damage for self- inducing vomiting, gastric distension, dysphagia, increased intestinal motility and chronic diarrhea. Clinician should detect such symptoms and practice the differential diagnosis with intestinal disease like celiac disease, gastroesophageal reflux, and inflammatory bowel diseases (196).
Clinicians have to be alert to recognize the psychological features associated with the onset of EDs during gestation, reinforcing the positive changes of body image in pregnant women and focusing on self-nurturing interventions to reduce stress and anxiety (15). Clinicians have also to motivate pregnant women to supplement essential nutrients such as iron, folate, and iodine for an adequate fetal development.
This target intervention must be continued in the postpartum period, which is the most vulnerable stage for the relapse of EDs symptoms and for the overlap with psychiatric disorders. Mothers with EDs also experience stress during the breastfeeding period, therefore a strict postpartum follow-up is necessary.
Finally, it is also necessary to clarify the biological mechanisms that promote harmful effects on the fetus of mothers diagnosed of EDs. Further prospective studies with large sample sizes are needed, discriminating the consequences of the different subtypes of EDs. Human trials would also determine appropriate approaches to treat these disorders in order to design structured interventions during gestation.
Author Contributions
GS conceptualized, designed, and drafted the initial manuscript and tables supported by the rest of the authors. VA-F supervised the methodology. GS and VA-F reviewed the manuscript. VA-F, VA-B, AH, XM, EM, MA-V, AB, and SF-M contributed to bibliographic sources as well as the elaboration of the initial manuscript and tables, performing the different topics explored in this review. GS, MG-R, OG-A, and VA-F conceptualized and coordinated the review. MG-R and OG-A performed the final check of the manuscript, respectively, from gynecologist's and neonatologist's point of view. All authors critically reviewed the manuscript and approved the final manuscript as submitted.
Funding
This work was supported by Red de Salud Materno-Infantil y del Desarrollo (SAMID) (RD12/0026/0003, RD16/0022/0002) from Instituto de Salud Carlos III and PI15/01179 grant from Instituto de Salud Carlos III.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2020.00587/full#supplementary-material
Table S1. Dietary Reference Intakes (DRIs) during pregnancy recommended by the Institute of Medicine (IOM).
References
1. ACOG. Gynecologic care for adolescents and young women with eating disorders. Obs Gynecol. (2018) 131:205–13. doi: 10.1097/AOG.0000000000002652
2. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. Chapter 18. 5th Edition. In: APA, editor. Diagnostic and Statistical Manual of Mental Disorders. Washington, DC (2013).
3. National Collaborating Centre for Mental Health (UK). Eating Disorders: Core Interventions in the Treatment and Management of Anorexia Nervosa, Bulimia Nervosa and Related Eating Disorders. Leicester: British Psychological Society (2004).
4. Hudson JI, Hiripi E, Pope HG, Kessler RC. The prevalence and correlates of eating disorders in the national comorbidity survey replication. Biol Psychiatry. (2007) 61:348–58. doi: 10.1016/j.biopsych.2006.03.040
5. Keski-Rahkonen A, Mustelin L. Epidemiology of eating disorders in Europe: prevalence, incidence, comorbidity, course, consequences, and risk factor. Curr Opin Psychiatry. (2016) 29:372–7. doi: 10.1097/YCO.0000000000000278
6. Micali N. Management of eating disorders during pregnancy. Prog Neurol Psychiatry. (2010) 14:24–6. doi: 10.1002/pnp.158
7. Easter A, Bye A, Taborelli E, Corfield F, Schmidt U, Treasure J, et al. Recognising the symptoms: how common are eating disorders in pregnancy? Eur Eat Disord Rev. (2013) 21:340–4. doi: 10.1002/erv.2229
8. Watson HJ, Holle A Von, Hamer RM, Berg CK, Magnus P, Stoltenberg C, et al. Remission, continuation, and incidence of eating disorders during early pregnancy: a validation study on a population-based birth cohort. Psychol Med. (2014) 43:1723–34. doi: 10.1017/S0033291712002516
9. Popovic M, Pizzi C, Rusconi F, Gagliardi L, Galassi C, Trevisan M, et al. The role of maternal anorexia nervosa and bulimia nervosa before and during pregnancy in early childhood wheezing: findings from the NINFEA birth cohort study. Int J Eat Disord. (2018) 51:842–51. doi: 10.1002/eat.22870
10. Soares RM, Antunes Nunes MA, Schmidt MI, Giacomello A, Manzolli P, Camey S, et al. Inappropriate eating behaviors during pregnancy: prevalence and associated factors among pregnant women attending primary care in Southern Brazil. Int J Eat Disord. (2009) 42:387–93. doi: 10.1002/eat.20643
11. Cardoso Pinto J, Pazo Pires A. Eating behavior disorders in pregnancy: a review. Psicol Reflex Crit. (2012) 25:139–46. doi: 10.1590/S0102-79722012000100017
12. Orloff NC, Hormes JM. Pickles and ice cream! food cravings in pregnancy: hypotheses, preliminary evidence, and directions for future research. Front Psychol. (2014) 5:1076. doi: 10.3389/fpsyg.2014.01076
13. Franko DL, Spurrell EB. Detection and management of eating disorders during pregnancy. Obs Gynecol. (2000) 95:942–6. doi: 10.1016/S0029-7844(00)00792-4
14. Cardwell MS. CME review article. Eating disorders during pregnancy. Obstet Gynecol Surv. (2013) 68:312–23. doi: 10.1097/OGX.0b013e31828736b9
15. Fogarty S, Elmir R, Hay P, Schmied V. The experience of women with an eating disorder in the perinatal period: a meta-ethnographic study. BMC Pregnancy Childbirth. (2018) 18:121. doi: 10.1186/s12884-018-1762-9
16. Conrad R, Schablewski J, Schilling G, Liedtke R. Worsening of symptoms of bulimia nervosa during pregnancy. Psychosomatics. (2003) 44:76–8. doi: 10.1176/appi.psy.44.1.76
17. Bulik CM, Holle A Von, Hamer R, Berg CK, Torgersen L, Magnus P, et al. Patterns of remission, continuation, and incidence of broadly defined eating disorders during early pregnancy in the norwegian mother and child cohort study (MoBa). Psychol Med. (2007) 37:1109–18. doi: 10.1017/S0033291707000724
18. Russell J, Douglas A, Ingram C. Brain preparations for maternity–adaptive changes in behavioral and neuroendocrine systems during pregnancy and lactation. An overview. Prog Brain Res. (2001) 133:1–38. doi: 10.1016/S0079-6123(01)33002-9
19. Crow SJ, Agras WS, Crosby R, Halmi K, Mitchell JE. Eating disorder symptoms in pregnancy: a prospective study. Int J Eat Disord. (2008) 41:277–9. doi: 10.1002/eat.20496
20. Larsson G, Andersson-Ellström A. Experiences of pregnancy related body shape changes and of breastfeeding in women with a history of eating disorders. Eur Eat Disord Rev. (2003) 11:116–24. doi: 10.1002/erv.497
21. Pettersson CB, Zandian M, Clinton D. Eating disorder symptoms pre- and postpartum. Arch Womens Ment Health. (2016) 19:675–80. doi: 10.1007/s00737-016-0619-3
22. Lai BP, Tang CS, Winni Kwok TSE. A longitudinal study investigating disordered eating during the transition to motherhood among Chinese women in hong kong. Int J Eat Disord. (2006) 39:303–11. doi: 10.1002/eat.20266
23. Micali N, Treasure J, Simonoff E. Eating disorders symptoms in pregnancy: a longitudinal study of women with recent and past eating disorders and obesity. J Psychosom Res. (2007) 63:297–303. doi: 10.1016/j.jpsychores.2007.05.003
24. Knoph Berg C, Torgersen L, Von Holle A, Hamer RM, Bulik CM, Reichborn-Kjennerud T. Factors associated with binge eating disorder in pregnancy. Int J Eat Disord. (2011) 44:124–33. doi: 10.1002/eat.20797
25. Lo Sauro C, Ravaldi C, Cabras PL, Faravelli C, Ricca V. Stress, hypothalamic-pituitary-adrenal axis and eating disorders. Neuropsychobiology. (2008) 57:95–115. doi: 10.1159/000138912
26. Lau Y. Traditional Chinese pregnancy restrictions, health-related quality of life and perceived stress among pregnant women in Macao, China. Asian Nurs Res. (2012) 6:27–34. doi: 10.1016/j.anr.2012.02.005
27. Kimmel MC, Ferguson EH, Zerwas S, Bulik CM, Meltzer-Brody S. Obstetric and gynecologic problems associated with eating disorders HHS public access. Int J Eat Disord. (2016) 49:260–75. doi: 10.1002/eat.22483
29. Paslakis G, de Zwaan M. Clinical management of females seeking fertility treatment and of pregnant females with eating disorders. Eur Eat Disord Rev. (2019) 27:215–23. doi: 10.1002/erv.2667
30. Park RJ, Senior R, Stein A. The offspring of mothers with eating disorders. Eur Child Adolesc Psychiatry. (2003) 12:1. doi: 10.1007/s00787-003-1114-8
31. Capasso A, Petrella C, Milano W. Recent clinical aspects of eating disorders. Rev Recent Clin Trials. (2009) 4:63–9. doi: 10.2174/157488709787047594
32. Luck AJ, Morgan JF, Reid F, Brien AO, Brunton J, Price C, et al. The SCOFF questionnaire and clinical interview for eatingdisorders in general practice: comparative study. BMJ. (2012) 325:755–6. doi: 10.1136/bmj.325.7367.755
33. Richter F, Strauss B, Braehler E, Altmann U, Berger U. Psychometric properties of a short version of the eating attitudes test (EAT-8) in a German representative sample. Eat Behav. (2016) 21:198–204. doi: 10.1016/j.eatbeh.2016.03.006
34. Little L, Lowkes E. Critical issues in the care of pregnant women with eating disorders and the impact on their children. J Midwifery Women's Heal. (2000) 45:301–7. doi: 10.1016/S1526-9523(00)00031-3
35. Bye A, Shawe J, Bick D, Easter A, Kash-Macdonald M, Micali N. Barriers to identifying eating disorders in pregnancy and in the postnatal period: a qualitative approach. BMC Pregnancy Childbirth. (2018) 18:114. doi: 10.1186/s12884-018-1745-x
36. Austin K, Wilson K, Saha S. Hyperemesis gravidarum. Nutr Clin Pract. (2019) 34:226–41. doi: 10.1002/ncp.10205
37. O'Brien KM, Whelan DR, Sandler DP, Hall JE, Weinberg CR. Predictors and long-term health outcomes of eating disorders. PLoS ONE. (2017) 12:e0181104. doi: 10.1371/journal.pone.0181104
38. Martos-Ordonez C. Pregnancy in women with eating disorders: a review. Br J Midwifery. (2014) 13:446–8. doi: 10.12968/bjom.2005.13.7.18372
39. Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The cochrane collaboration's tool for assessing risk of bias in randomised trials. BMJ. (2011) 343:d5928. doi: 10.1136/bmj.d5928
40. Taborelli E, Easter A, Keefe R, Schmidt U, Treasure J, Micali N. Transition to motherhood in women with eating disorders: a qualitative study. Psychol Psychother Theory, Res Pract. (2016) 89:308–23. doi: 10.1111/papt.12076
41. Pinheiro AP, Raney TJ, Thornton LM, Fichter MM, Berrettini WH, Goldman D, et al. Sexual functioning in womem with eating disorders. Int J Eat Disord. (2010) 43:123–9. doi: 10.1002/eat.20671
42. Bulik CM, Hoffman ER, Von Holle A, Torgersen L, Stoltenberg C, Reichborn-Kjennerud T. Unplanned pregnancy in anorexia nervosa. Obs Gynecol. (2010) 116:1136–40. doi: 10.1097/AOG.0b013e3181f7efdc
43. Geary N, Asarian L. Modulation of appetite by gonadal steroid hormones. Philos Trans R Soc B Biol Sci. (2006) 361:1251–63. doi: 10.1098/rstb.2006.1860
44. Chan JL, Mantzoros CS. Role of leptin in energy-deprivation states: normal human physiology and clinical implications for hypothalamic amenorrhoea and anorexia nervosa. Lancet. (2005) 366:74–85. doi: 10.1016/S0140-6736(05)66830-4
45. Hirschberg AL. Sex hormones, appetite and eating behaviour in women. Maturitas. (2012) 71:248–56. doi: 10.1016/j.maturitas.2011.12.016
46. Andersen Arnold E, Ryan GL. Eating disorders in the obstetric and gynecologic patient population. Obstet Gynecol. (2009) 114:1353–67. doi: 10.1097/AOG.0b013e3181c070f9
47. Assens M, Ebdrup NH, Pinborg A, Schmidt L, Hougaard CO, Hageman I. Assisted reproductive technology treatment in women with severe eating disorders: a national cohort study. Acta Obstet Gynecol Scand. (2015) 94:1254–61. doi: 10.1111/aogs.12727
48. Freizinger M, Franko DL, Dacey M, Okun B, Domar AD. The prevalence of eating disorders in infertile women. Fertil Steril. (2010) 93:72–8. doi: 10.1016/j.fertnstert.2008.09.055
49. Easter A, Treasure J, Micali N. Fertility and prenatal attitudes towards pregnancy in women with eating disorders: results from the avon longitudinal study of parents and children. BJOG An Int J Obstet Gynaecol. (2011) 118:1491–8. doi: 10.1111/j.1471-0528.2011.03077.x
50. Micali N, Dos-Santos-Silva I, De Stavola B, Steenweg-De Graaf J, Jaddoe V, Hofman A, et al. Fertility treatment, twin births, and unplanned pregnancies in women with eating disorders: findings from a population-based birth cohort. BJOG An Int J Obstet Gynaecol. (2014) 121:408–15. doi: 10.1111/1471-0528.12503
51. Linna MS, Raevuori A, Haukka J, Suvisaari JM, Suokas JT, Gissler M. Reproductive health outcomes in eating disorders. Int J Eat Disord. (2013) 46:826–33. doi: 10.1002/eat.22179
52. National Institute for Health and Care Excellence. Eating Disorders: Recognition and Treatment NICE guideline. (2017). Available online at: nice.org.uk/guidance/ng69
53. Hadigan CM, Anderson EJ, Miller KK, Hubbard JL, Herzog DB, Klibanski A, et al. Assessment of macronutrient and micronutrient intake in women with anorexia nervosa. Int J Eat Disord. (2000) 28:284–92. doi: 10.1002/1098-108X(200011)28:3<284::AID-EAT5>3.0.CO;2-G
54. Nova E, Lopez-Vidriero I, Varela P, Toro O, Casas J, Marcos A. Indicators of nutritional status in restricting-type anorexia nervosa patients: a 1-year follow-up study. Clin Nutr. (2004) 23:1353–9. doi: 10.1016/j.clnu.2004.05.004
55. Misra M, Tsai P, Anderson EJ, Hubbard JL, Gallagher K, Soyka LA, et al. Nutrient intake in community-dwelling adolescent girls with anorexia nervosa and in healthy adolescents. Am J Clin Nutr. (2006) 84:698–706. doi: 10.1093/ajcn/84.4.698
56. Siega-Riz AM, Haugen M, Meltzer HM, Von Holle A, Hamer R, Torgersen L, et al. Nutrient and food group intakes of women with and without bulimia nervosa and binge eating disorder during pregnancy. Am J Clin Nutr. (2008) 87:1346–55. doi: 10.1093/ajcn/87.5.1346
57. Swann RA, Von Holle A, Torgersen L, Gendall K, Reichborn-Kjennerud T, Bulik CM. Attitudes toward weight gain during pregnancy: results from the norwegian mother and child cohort study (MoBa). Int J Eat Disord. (2009) 42:394–401. doi: 10.1002/eat.20632
58. Setnick J. Micronutrient deficiencies and supplementation in anorexia and bulimia nervosa: a review of literature. Nutr Clin Pract. (2010) 25:137–42. doi: 10.1177/0884533610361478
59. Siega-Riz AM, Von Holle A, Haugen M, Meltzer HM, Hamer R, Torgersen L, et al. Gestational weight gain of women with eating disorders in the norwegian pregnancy cohort. Int J Eat Disord. (2011) 44:428–34. doi: 10.1002/eat.20835
60. Micali N, Northstone K, Emmett P, Naumann U, Treasure JL. Nutritional intake and dietary patterns in pregnancy: a longitudinal study of women with lifetime eating disorders. Br J Nutr. (2012) 108:2093–9. doi: 10.1017/S0007114512000256
61. Micali N, De Stavola B, Dos-Santos-Silva I, Steenweg-De Graaff J, Jansen PW, Jaddoe VWV, et al. Perinatal outcomes and gestational weight gain in women with eating disorders: a population-based cohort study. BJOG An Int J Obstet Gynaecol. (2012) 119:1493–502. doi: 10.1111/j.1471-0528.2012.03467.x
62. Velickovic KMC, Makovey J, Abraham SF. Vitamin D, bone mineral density and body mass index in eating disorder patients. Eat Behav. (2013) 14:124–7. doi: 10.1016/j.eatbeh.2013.01.010
63. Coker EL, Mitchell-Wong LA, Abraham SF. Is pregnancy a trigger for recovery from an eating disorder? Acta Obstet Gynecol Scand. (2013) 92:1407–13. doi: 10.1111/aogs.12256
64. Sabel AL, Gaudiani JL, Statland B, Mehler PS. Hematological abnormalities in severe anorexia nervosa. Ann Hematol. (2013) 92:605–13. doi: 10.1007/s00277-013-1672-x
65. Zerwas SC, Von holle A, Perrin EM, Skinner AC, Reba-Harrelson L, Hamer RM, et al. Gestational and postpartum weight change patterns in mothers with eating disorders. Eur Eat Disord Rev. (2014) 22:397–404. doi: 10.1002/erv.2314
66. Gatti D, El Ghoch M, Viapiana O, Ruocco A, Chignola E, Rossini M, et al. Strong relationship between vitamin D status and bone mineral density in anorexia nervosa. Bone. (2015) 78:212–5. doi: 10.1016/j.bone.2015.05.014
67. Koubaa S, Hällström T, Brismar K, Hellström PM, Hirschberg AL. Biomarkers of nutrition and stress in pregnant women with a history of eating disorders in relation to head circumference and neurocognitive function of the offspring. BMC Pregnancy Childbirth. (2015) 15:1–8. doi: 10.1186/s12884-015-0741-7
68. Jagielska G. Bone mineralization disorders as a complication of anorexia nervosa - etiology, prevalence, course and treatment. Psychiatr Pol. (2016) 50:509–20. doi: 10.12740/PP/59289
69. Chiurazzi C, Cioffi I, De Caprio C, De Filippo E, Marra M, Sammarco R, et al. Adequacy of nutrient intake in women with restrictive anorexia nervosa. Nutrition. (2017) 38:80–4. doi: 10.1016/j.nut.2017.02.004
70. Nguyen AN, de Barse LM, Tiemeier H, Jaddoe VWV, Franco OH, Jansen PW, et al. Maternal history of eating disorders: diet quality during pregnancy and infant feeding. Appetite. (2017) 109:108–14. doi: 10.1016/j.appet.2016.11.030
71. Achamrah N, Coëffier M, Rimbert A, Charles J, Folope V, Petit A, et al. Micronutrient status in 153 patients with anorexia nervosa. Nutrients. (2017) 9:1–10. doi: 10.3390/nu9030225
72. Carlsson M, Brudin L, Wanby P. Directly measured free 25-hydroxy vitamin D levels show no evidence of vitamin D deficiency in young Swedish women with anorexia nervosa. Eat Weight Disord. (2018) 23:247–54. doi: 10.1007/s40519-017-0392-y
73. Ehrenberg HM, Dierker L, Milluzzi C, Mercer BM. Low maternal weight, failure to thrive in pregnancy, and adverse pregnancy outcomes. Am J Obstet Gynecol. (2003) 189:1726–30. doi: 10.1016/S0002-9378(03)00860-3
74. Rasmussen KM, Yaktine AL, Institute of Medicine (US) and National Research Council (US) Committee to Reexamine IOM Pregnancy Weight Guidelines, (editors). Weight Gain During Pregnancy: Reexamining the Guidelines. Washington, DC: National Academies Press (2009).
75. National Institute for Health and Clinical Excellence (NICE). Weight Management Before, During and After Pregnancy. Public Health Guideline (2010). Available online at: www.nice.org.uk/guidance/ph27
76. ACOG. Committee opinion: weight gain during pregnancy. Obstet Gynecol. (2013) 121:210–2. doi: 10.1097/01.AOG.0000425668.87506.4c
77. Bardone-Cone AM, Fitzsimmons-Craft EE, Harney MB, Maldonado CR, Lawson MA, Smith R, et al. The inter-relationships between vegetarianism and eating disorders among females. J Acad Nutr Diet. (2012) 112:1247–52. doi: 10.1016/j.jand.2012.05.007
78. Hall CH, Hewitt G, Stevens SL. Assessment and management of bone health in adolescents with anorexia nervosa. Part two: bone health in adolescents with anorexia nervosa. J Pediatr Adolesc Gynecol. (2008) 21:221–4. doi: 10.1016/j.jpag.2008.02.006
79. Madsen IR, Hrder K, Stving RK. Remission of eating disorder during pregnancy: five cases and brief clinical review. J Psychosom Obstet Gynecol. (2009) 30:122–6. doi: 10.1080/01674820902789217
80. Dörsam AF, Preißl H, Micali N, Lörcher SB, Zipfel S, Giel KE. The impact of maternal eating disorders on dietary intake and eating patterns during pregnancy: a systematic review. Nutrients. (2019) 11:840. doi: 10.3390/nu11040840
81. Procter SB, Campbell CG. Position of the academy of nutrition and dietetics: nutrition and lifestyle for a healthy pregnancy outcome. J Acad Nutr Diet. (2014) 114:1099–103. doi: 10.1016/j.jand.2014.05.005
82. Kouba S, Hällström T, Lindholm C, Hirschberg AL. Pregnancy and neonatal outcomes in women with eating disorders. Obstet Gynecol. (2005) 105:255–60. doi: 10.1097/01.AOG.0000148265.90984.c3
83. Blais MA, Becker AE, Burwell RA, Flores AT, Nussbaum KM, Greenwood DN, et al. Pregnancy: outcome and impact on symptomatology in a cohort of eating-disordered women. Int J Eat Disord. (2000) 27:140–9. doi: 10.1002/(SICI)1098-108X(200003)27:2<140::AID-EAT2>3.0.CO;2-E
84. Franko DL, Blais MA, Becker AE, Delinsky SS, Greenwood DN, Flores AT, et al. Pregnancy complications and neonatal outcomes in women with eating disorders. Am J Psychiatry. (2001) 158:1461–6. doi: 10.1176/appi.ajp.158.9.1461
85. Sollid CP, Wisborg K, Hjort J, Secher NJ. Eating disorder that was diagnosed before pregnancy and pregnancy outcome. Am J Obstet Gynecol. (2004) 190:206–10. doi: 10.1016/S0002-9378(03)00900-1
86. Ekéus C, Lindberg L, Lindblad F, Hjern A. Birth outcomes and pregnancy complications in women with a history of anorexia nervosa. BJOG An Int J Obstet Gynaecol. (2006) 113:925–9. doi: 10.1111/j.1471-0528.2006.01012.x
87. Newton MS, Chizawsky LLK. Treating vulnerable populations: the case of eating disorders during pregnancy. J Psychosom Obstet Gynecol. (2006) 27:5–7. doi: 10.1080/01674820500451517
88. Morgan JF, Lacey JH, Chung E. Risk of postnatal depression, miscarriage, and preterm birth in bulimia nervosa: retrospective controlled study. Psychosom Med. (2006) 68:487–92. doi: 10.1097/01.psy.0000221265.43407.89
89. Micali N, Simonoff E, Treasure J. Risk of major adverse perinatal outcomes in women with eating disorders. Br J Psychiatry. (2007) 190:255–9. doi: 10.1192/bjp.bp.106.020768
90. Bansil P, Kuklina EV, Whiteman MK, Kourtis AP, Posner SF, Johnson CH, et al. Eating disorders among delivery hospitalizations: prevalence and outcomes. J Women's Heal. (2008) 17:1523–8. doi: 10.1089/jwh.2007.0779
91. Bulik CM, Von Holle A, Siega-Riz AM, Torgersen L, Kveim Lie K, Hamer RM, et al. Birth outcomes in women with eating disorders in the norwegian mother and child cohort study (MoBa). Int J Eat Disord. (2009) 42:9–18. doi: 10.1002/eat.20578
92. Pasternak Y, Weintraub AY, Shoham-Vardi I, Sergienko R, Guez J, Wiznitzer A, et al. Obstetric and perinatal outcomes in women with eating disorders. J Women's Heal. (2011) 21:61–5. doi: 10.1089/jwh.2011.2907
93. Eagles JM, Lee AJ, Raja EA, Millar HR, Bhattacharya S. Pregnancy outcomes of women with and without a history of anorexia nervosa. Psychol Med. (2012) 42:2651–60. doi: 10.1017/S0033291712000414
94. Solmi F, Sallis H, Stahl D, Treasure J, Micali N. Low birth weight in the offspring of women with anorexia nervosa. Epidemiol Rev. (2014) 36:49–56. doi: 10.1093/epirev/mxt004
95. Linna MS, Raevuori A, Haukka J, Suvisaari JM, Suokas JT, Gissler M. Pregnancy, obstetric, and perinatal health outcomes in eating disorders. Am J Obstet Gynecol. (2014) 211:392.e1–8. doi: 10.1016/j.ajog.2014.03.067
96. Triunfo S, Lanzon A. Impact of maternal under nutrition on obstetric outcomes. J Endocrinol Invest. (2015) 38:31–8. doi: 10.1007/s40618-014-0168-4
97. Micali N, Stemann Larsen P, Strandberg-Larsen K, Nybo Andersen AM. Size at birth and preterm birth in women with lifetime eating disorders: a prospective population-based study. BJOG An Int J Obstet Gynaecol. (2016) 123:1301–10. doi: 10.1111/1471-0528.13825
98. Easter A, Taborelli E, Bye A, Zunszain PA, Pariante CM, Treasure J, et al. Perinatal hypothalamic-pituitary-adrenal axis regulation among women with eating disorders and their infants. Psychoneuroendocrinology. (2017) 76:127–34. doi: 10.1016/j.psyneuen.2016.11.004
99. Watson HJ, Zerwas S, Torgersen L, Gustavson K, Diemer EW, Knudsen GP, et al. Maternal eating disorders and perinatal outcomes: a three-generation study in the norwegian mother and child cohort study. J Abnorm Psychol. (2017) 126:552–64. doi: 10.1037/abn0000241
100. Eik-Nes TT, Horn J, Strohmaier S, Holmen TL, Micali N, Bjørnelv S. Impact of eating disorders on obstetric outcomes in a large clinical sample: a comparison with the HUNT study. Int J Eat Disord. (2018) 51:1134–43. doi: 10.1002/eat.22916
101. Charbonneau KD, Seabrook JA. Adverse birth outcomes associated with types of eating disorders: a review. Can J Diet Pract Res. (2019) 80:131–6. doi: 10.3148/cjdpr-2018-044
102. Chan CY, Lee AM, Koh YW, Lam SK, Lee CP, Leung KY, et al. Course, risk factors, and adverse outcomes of disordered eating in pregnancy. Int J Eat Disord. (2019) 52:652–8. doi: 10.1002/eat.23065
103. Sotodate G, Matsumoto A, Konishi Y, Toya Y, Endo M, Oyama K. Fetal intracranial hemorrhage due to maternal subclinical vitamin K deficiency associated with long-term eating disorder. J Obstet Gynaecol Res. (2019) 45:461–5. doi: 10.1111/jog.13825
104. Henson MC, Castracane VD. Leptin in pregnancy: an update1. Biol Reprod. (2006) 74:218–29. doi: 10.1095/biolreprod.105.045120
105. Monteleone P, Luisi M, Colurcio B, Casarosa E, Monteleone P, Ioime R, et al. Plasma levels of neuroactive steroids are increased in untreated women with anorexia nervosa or bulimia nervosa. Psychosom Med. (2001) 63:62–8. doi: 10.1097/00006842-200101000-00008
106. Warren MP. Endocrine manifestations of eating disorders. J Clin Endocrinol Metab. (2011) 96:333–43. doi: 10.1210/jc.2009-2304
107. Schieve LA, Cogswell ME, Scanlon KS, Perry G, Ferre C, Blackmore-Prince C, et al. Prepregnancy body mass index and pregnancy weight gain. Obstet Gynecol. (2000) 96:194–200. doi: 10.1097/00006250-200008000-00008
108. Hillesund ER, Bere E, Sagedal LR, Vistad I, Seiler HL, Torstveit MK, et al. Pre-pregnancy and early pregnancy dietary behavior in relation to maternal and newborn health in the norwegian fit for delivery study – a post hoc observational analysis. Food Nutr Res. (2018) 62:1–14. doi: 10.29219/fnr.v62.1273
109. Wadhwa PD. Psychoneuroendocrine processes in human pregnancy influence fetal development and health. Psychoneuroendocrinology. (2005) 30:724–43. doi: 10.1016/j.psyneuen.2005.02.004
110. Stein A, Pearson RM, Goodman SH, Rapa E, Rahman A, McCallum M, et al. Effects of perinatal mental disorders on the fetus and child. Lancet. (2014) 384:1800–19. doi: 10.1016/S0140-6736(14)61277-0
111. Shapiro GD. Psychosocial stress in pregnancy and preterm birth: associations and mechanisms. J Perinat Med. (2013) 41:631–45. doi: 10.1515/jpm-2012-0295
112. Liu Y, Murphy SK, Murtha AP, Fuemmeler BF, Schildkraut J, Huang Z, et al. Depression in pregnancy, infant birth weight and DNA methylation of imprint regulatory elements. Epigenetics. (2012) 7:735–46. doi: 10.4161/epi.20734
113. Barker DJP, Eriksson JG, Forsén T, Osmond C. Fetal origins of adult disease: strength of effects and biological basis. Int J Epidemiol. (2002) 31:1235–9. doi: 10.1093/ije/31.6.1235
114. Meaney MJ, Szyf M, Seckl JR. Epigenetic mechanisms of perinatal programming of hypothalamic-pituitary-adrenal function and health. Trends Mol Med. (2007) 13:269–77. doi: 10.1016/j.molmed.2007.05.003
115. Micali N, Treasure J. Biological effects of a maternal ED on pregnancy and foetal development: a review. Eur Eat Disord Rev. (2009) 17:448–54. doi: 10.1002/erv.963
116. Sandman CA, Davis EP, Buss C, Glynn LM. Exposure to prenatal psychobiological stress exerts programming influences on the mother and her fetus. Neuroendocrinology. (2012) 95:8–21. doi: 10.1159/000327017
117. Starling P, Charlton K, McMahon AT, Lucas C. Fish intake during pregnancy and foetal neurodevelopment-A systematic review of the evidence. Nutrients. (2015) 7:2001–14. doi: 10.3390/nu7032001
118. Frieling H, Gozner A, Römer KD, Lenz B, Bönsch D, Wilhelm J, et al. Global DNA hypomethylation and DNA hypermethylation of the alpha synuclein promoter in females with anorexia nervosa. Mol Psychiatry. (2007) 12:229–30. doi: 10.1038/sj.mp.4001931
119. Frieling H, Rómer KD, Scholz S, Mittelbach F, Wilhelm J, De Zwaan M, et al. Epigenetic dysregulation of dopaminergic genes in eating disorders. Int J Eat Disord. (2010) 43:577–83. doi: 10.1002/eat.20745
120. Ehrlich S, Walton E, Roffman JL, Weiss D, Puls I, Doehler N, et al. Smoking, but not malnutrition, influences promoter-specific DNA methylation of the proopiomelanocortin gene in patients with and without anorexia nervosa. Can J Psychiatry. (2012) 57:168–76. doi: 10.1177/070674371205700306
121. Steiger H, Labonté B, Groleau P, Turecki G, Israel M. Methylation of the glucocorticoid receptor gene promoter in bulimic women: associations with borderline personality disorder, suicidality, and exposure to childhood abuse. Int J Eat Disord. (2013) 46:246–55. doi: 10.1002/eat.22113
122. Tremolizzo L, Conti E, Bomba M, Uccellini O, Rossi MS, Marfone M, et al. Decreased whole-blood global DNA methylation is related to serum hormones in anorexia nervosa adolescents. World J Biol Psychiatry. (2014) 15:327–33. doi: 10.3109/15622975.2013.860467
123. Hoyo C, Murtha AP, Schildkraut JM, Jirtle R, Demark-Wahnefried W, Forman MR, et al. Methylation variation at IGF2 differentially methylated regions and maternal folic acid use before and during pregnancy. Epigenetics. (2011) 6:928–36. doi: 10.4161/epi.6.7.16263
124. Vanhees K, Vonhögen IGC, Van Schooten FJ, Godschalk RWL. You are what you eat, and so are your children: the impact of micronutrients on the epigenetic programming of offspring. Cell Mol Life Sci. (2014) 71:271–85. doi: 10.1007/s00018-013-1427-9
125. McGowan PO, Meaney MJ, Szyf M. Diet and epigenetic reprogramming of phenotypic differences in behavior. Brain Res. (2008) 1237:12–24. doi: 10.1016/j.brainres.2008.07.074
126. Joy Dauncey M. Genomic and epigenomic insights into nutrition and brain disorders. Nutrients. (2013) 5:887–914. doi: 10.3390/nu5030887
127. Frieling H, Römer K, Röschke B, Bönsch D, Wilhelm J, Fiszer R, et al. Homocysteine plasma levels are elevated in females with anorexia nervosa. J Neural Transm. (2005) 112:979–85. doi: 10.1007/s00702-005-0315-3
128. Frieling H, Röschke B, Kornhuber J, Wilhelm J, Römer KD, Gruß B, et al. Cognitive impairment and its association with homocysteine plasma levels in females with eating disorders - findings from the HEaD-study. J Neural Transm. (2005) 112:1591–8. doi: 10.1007/s00702-005-0392-3
129. McGarel C, Pentieva K, Strain JJ, McNulty H. Emerging roles for folate and related B-vitamins in brain health across the lifecycle. Proc Nutr Soc. (2015) 74:46–55. doi: 10.1017/S0029665114001554
130. Berletch JB, Liu C, Love WK, Andrews LG, Katiyar SK, Tollefsbo TO. Epigenetic and genetic mechanisms contribute to telomerase inhibition by EGCG. J Cell Biochem. (2008) 103:509–19. doi: 10.1002/jcb.21417
131. Vanhees K, Coort S, Ruijters EJB, Godschalk RWL, van Schooten FJ, van Waalwijk SB, et al. Epigenetics: prenatal exposure to genistein leaves a permanent signature on the hematopoietic lineage. FASEB J. (2011) 25:797–807. doi: 10.1096/fj.10-172155
132. Sayols-Baixeras S, Subirana I, Fernández-Sanlés A, Sentí M, Lluís-Ganella C, Marrugat J, et al. DNA methylation and obesity traits: an epigenome-wide association study. The REGICOR study. Epigenetics. (2017) 12:909–16. doi: 10.1080/15592294.2017.1363951
133. Tobi EW, Heijmans BT, Kremer D, Putter H, Delemarre-van de Waal HA, Finken MJJ, et al. DNA methylation of IGF2, GNASAS, INSIGF and LEP and being born small for gestational age. Epigenetics. (2011) 6:171–6. doi: 10.4161/epi.6.2.13516
134. Zheng S, Rollet M, Pan YX. Maternal protein restriction during pregnancy induces CCAAT/enhancer-binding protein (C/EBPβ) expression through the regulation of histone modification at its promoter region in female offspring rat skeletal muscle. Epigenetics. (2011) 6:161–70. doi: 10.4161/epi.6.2.13472
135. Godfrey KM, Sheppard A, Gluckman PD, Lillycrop KA, Burdge GC, McLean C, et al. Epigenetic gene promoter methylation at birth is associated with child's later adiposity. Diabetes. (2011) 60:1528–34. doi: 10.2337/db10-0979
136. Vucetic Z, Kimmel J, Totoki K, Hollenbeck E, Reyes TM. Maternal high-fat diet alters methylation and gene expression of dopamine and opioid-related genes. Endocrinology. (2010) 151:4756–64. doi: 10.1210/en.2010-0505
137. Movérare-Skrtic S, Mellström D, Vandenput L, Ehrich M, Ohlsson C. Peripheral blood leukocyte distribution and body mass index are associated with the methylation pattern of the androgen receptor promoter. Endocrine. (2009) 35:204–10. doi: 10.1007/s12020-009-9153-7
138. Chen H, Simar D, Lambert K, Mercier J, Morris MJ. Maternal and postnatal overnutrition differentially impact appetite regulators and fuel metabolism. Endocrinology. (2008) 149:5348–56. doi: 10.1210/en.2008-0582
139. Huang RC, Garratt ES, Pan H, Wu Y, Davis EA, Barton SJ, et al. Genome-wide methylation analysis identifies differentially methylated CpG loci associated with severe obesity in childhood. Epigenetics. (2015) 10:995–1005. doi: 10.1080/15592294.2015.1080411
140. Nogueiras R, Habegger KM, Chaudhary N, Finan B, Banks AS, Dietrich MO, et al. Sirtuin 1 and sirtuin 3: physiological modulators of metabolism. Physiol Rev. (2012) 92:1479–514. doi: 10.1152/physrev.00022.2011
141. Reamon-Buettner SM, Buschmann J, Lewin G. Identifying placental epigenetic alterations in an intrauterine growth restriction (IUGR) rat model induced by gestational protein deficiency. Reprod Toxicol. (2014) 45:117–24. doi: 10.1016/j.reprotox.2014.02.009
142. Gong L, Pan YX, Chen H. Gestational low protein diet in the rat mediates Igf2 gene expression in male offspring via altered hepatic DNA methylation. Epigenetics. (2010) 5:619–26. doi: 10.4161/epi.5.7.12882
143. Rszer T, Ricote M. PPARs in the renal regulation of systemic blood pressure. PPAR Res. (2010) 2010:698730. doi: 10.1155/2010/698730
144. Slater-Jefferies JL, Lillycrop KA, Townsend PA, Torrens C, Hoile SP, Hanson MA, et al. Feeding a protein-restricted diet during pregnancy induces altered epigenetic regulation of peroxisomal proliferator-activated receptor- in the heart of the offspring. J Dev Orig Health Dis. (2011) 2:250–5. doi: 10.1017/S2040174410000425
145. Zheng J, Xiao X, Zhang Q, Wang T, Yu M, Xu J. Maternal low-protein diet modulates glucose metabolism and hepatic microRNAs expression in the early life of offspring. Nutrients. (2017) 9:E205. doi: 10.3390/nu9030205
146. Sinclair KD, Allegrucci C, Singh R, Gardner DS, Sebastian S, Bispham J, et al. DNA methylation, insulin resistance, and blood pressure in offspring determined by maternal periconceptional B vitamin and methionine status. Proc Natl Acad Sci USA. (2007) 104:19351–6. doi: 10.1073/pnas.0707258104
147. Crider KS, Yang TP, Berry RJ, Bailey LB. Folate and DNA methylation: a review of molecular mechanisms and the evidence for folate's role. Adv Nutr. (2012) 3:21–38. doi: 10.3945/an.111.000992
148. Pogribny IP, Karpf AR, James SR, Melnyk S, Han T, Tryndyak VP. Epigenetic alterations in the brains of fisher 344 rats induced by long-term administration of folate/methyl-deficient diet. Brain Res. (2008) 1237:25–34. doi: 10.1016/j.brainres.2008.07.077
149. Kazmi N, Gaunt TR, Relton C, Micali N. Maternal eating disorders affect offspring cord blood DNA methylation: a prospective study. Clin Epigenetics. (2017) 9:120. doi: 10.1186/s13148-017-0418-3
150. Lambertini L, Li Q, Ma Y, Zhang W, Hao K, Marsit C, et al. Placental imprinted gene expression mediates the effects of maternal psychosocial stress during pregnancy on fetal growth. J Dev Orig Health Dis. (2019) 10:196–205. doi: 10.1017/S2040174418000545
151. Solmi M, Veronese N, Sergi G, Luchini C, Favaro A, Santonastaso P, et al. The association between smoking prevalence and eating disorders: a systematic review and meta-analysis. Addiction. (2016) 111:1914–22. doi: 10.1111/add.13457
152. Root T, Pinheiro AP, Thornton L, Strober M, Fernandez-aranda F, Brandt H, et al. Substance use disorders in women with anorexia nervosa. Int J Eat Disord. (2011) 43:14–21. doi: 10.1002/eat.20670
153. Fouladi F, Mitchell JE, Crosby RD, Engel SG, Crow S, Hill L, et al. Prevalence of alcohol and other substance use in patients with eating disorders. Eur Eat Disord Rev. (2015) 23:531–6. doi: 10.1002/erv.2410
154. Steiger H, Thaler L. Eating disorders, gene-environment interactions and the epigenome: roles of stress exposures and nutritional status. Physiol Behav. (2016) 162:181–5. doi: 10.1016/j.physbeh.2016.01.041
155. Novakovic B, Ryan J, Pereira N, Boughton B, Craig JM, Saffery R. Postnatal stability and tissue- and time-specific effects of AHRR methylation change in response to maternal smoking in pregnancy. Epigenetics. (2013) 9:377–86. doi: 10.4161/epi.27248
156. Barak AJ, Beckenhauer HC, Tuma DJ, Badakhsh S. Effects of prolonged ethanol feeding on methionine metabolism in rat liver. Biochem Cell Biol. (1987) 65:230–3. doi: 10.1139/o87-029
157. Ngai YF, Sulistyoningrum DC, O'Neill R, Innis SM, Weinberg J, Devlin AM. Prenatal alcohol exposure alters methyl metabolism and programs serotonin transporter and glucocorticoid receptor expression in brain. Am J Physiol Regul Integr Comp Physiol. (2015) 309:R613–22. doi: 10.1152/ajpregu.00075.2015
158. Portales-Casamar E, Lussier AA, Jones MJ, MacIsaac JL, Edgar RD, Mah SM, et al. DNA methylation signature of human fetal alcohol spectrum disorder. Epigenetics Chromatin. (2016) 9:25. doi: 10.1186/s13072-016-0074-4
159. Laufer BI, Kapalanga J, Castellani CA, Diehl EJ, Yan L, Singh SM. Associative DNA methylation changes in children with prenatal alcohol exposure. Epigenomics. (2015) 7:1259–74. doi: 10.2217/epi.15.60
160. Knight AK, Smith AK. Epigenetic biomarkers of preterm birth and its risk factors. Genes. (2016) 7:15. doi: 10.3390/genes7040015
161. Schorr M, Miller KK. The endocrine manifestations of anorexia nervosa: mechanisms and management. Nat Rev Endocrinol. (2017) 13:174–86. doi: 10.1038/nrendo.2016.175
162. Klump KL, Culbert KM, Sisk CL. Sex differences in binge eating: gonadal hormone effects across development. Annu Rev Clin Psychol. (2017) 13:183–207. doi: 10.1146/annurev-clinpsy-032816-045309
163. Mazzeo SE, Slof-Op't MCT, Landt I, Jones I, Mitchell K, Kendler KS, et al. Associations among postpartum depression, eating disorders, and perfectionism in a population-based sample of adult women. Int J Eat Disord. (2006) 39:202–11. doi: 10.1002/eat.20243
164. Koubaa S, Hällström T, Hirschberg AL. Early maternal adjustment in women with eating disorders. Int J Eat Disord. (2008) 41:405–10. doi: 10.1002/eat.20521
165. Micali N, Simonoff E, Treasure J. Pregnancy and post-partum depression and anxiety in a longitudinal general population cohort: the effect of eating disorders and past depression. J Affect Disord. (2011) 131:150–7. doi: 10.1016/j.jad.2010.09.034
166. Meltzer-Brody S, Zerwas S, Leserman J, von Holle A, Regis T, Bulik C. Eating disorders and trauma history in women with perinatal depression. J Women's Heal. (2011) 20:863–70. doi: 10.1089/jwh.2010.2360
167. Easter A, Solmi F, Bye A, Taborelli E, Corfield F, Schmidt U, et al. Antenatal and postnatal psychopathology among women with current and past eating disorders: longitudinal patterns. Eur Eat Disord Rev. (2015) 23:19–27. doi: 10.1002/erv.2328
168. Swinbourne J, Hunt C, Abbott M, Russell J St. Clare T, Touyz S. The comorbidity between eating disorders and anxiety disorders: prevalence in an eating disorder sample and anxiety disorder sample. Aust N Z J Psychiatry. (2012) 46:118–31. doi: 10.1177/0004867411432071
169. Astrachan-Fletcher E, Veldhuis C, Lively N, Fowler C, Marcks B. The reciprocal effects of eating disorders and the postpartum period: a review of the literature and recommendations for clinical care. J Women Heal. (2008) 17:227–39. doi: 10.1089/jwh.2007.0550
170. Sparling TM, Nesbitt RC, Henschke N, Gabrysch S. Nutrients and perinatal depression: a systematic review. J Nutr Sci. (2017) 6:e61. doi: 10.1017/jns.2017.58
171. Stetler C, Miller GE. Depression and hypothalamic-pituitary-adrenal activation: a quantitative summary of four decades of research. Psychosom Med. (2011) 73:114–26. doi: 10.1097/PSY.0b013e31820ad12b
172. Knoph C, Von Holle A, Zerwas S, Torgersen L, Tambs K, Stoltenberg C, et al. Course and predictors of maternal eating disorders in the postpartum period. Int J Eat Disord. (2013) 46:355–68. doi: 10.1002/eat.22088
173. Torgersen L, Ystrom E, Haugen M, Meltzer HM, Von Holle A, Berg CK, et al. Breastfeeding practice in mothers with eating disorders. Matern Child Nutr. (2010) 6:243–52. doi: 10.1111/j.1740-8709.2009.00208.x
174. Dozier AM, Nelson A, Brownell E. The relationship between life stress and breastfeeding outcomes among low-income mothers. Adv Prev Med. (2012) 2012:902487. doi: 10.1155/2012/902487
175. Cannon AM, Kakulas F, Hepworth AR, Lai CT, Hartmann PE, Geddes DT. The effects of leptin on breastfeeding behaviour. Int J Environ Res Public Health. (2015) 12:12340–55. doi: 10.3390/ijerph121012340
176. Squires C, Lalanne C, Murday N, Simoglou V, Vaivre-Douret L. The influence of eating disorders on mothers' sensitivity and adaptation during feeding: a longitudinal observational study. BMC Pregnancy Childbirth. (2014) 14:274. doi: 10.1186/1471-2393-14-274
177. Bzikowska-Jura A, Czerwonogrodzka-Senczyna A, Oledzka G, Szostak-Wegierek D, Weker H, Wesołowska A. Maternal nutrition and body composition during breastfeeding: association with human milk composition. Nutrients. (2018) 10:E1379. doi: 10.3390/nu10101379
178. Honzik T, Adamovicova M, Smolka V, Magner M, Hruba E, Zeman J. Clinical presentation and metabolic consequences in 40 breastfed infants with nutritional vitamin B12 deficiency - what have we learned? Eur J Paediatr Neurol. (2010) 14:488–95. doi: 10.1016/j.ejpn.2009.12.003
179. Dawodu A, Tsang RC. Maternal vitamin D status : effect on milk vitamin D content and vitamin D status. Adv Nutr An Int Rev J. (2012) 3:353–61. doi: 10.3945/an.111.000950
180. National ED Collaboration. Pregnancy and eating disorders : a professional's guide to assessment and referral. In: The National Eating Disorders Collaboration. p. 1–24. Available online at: nedc.com.au
181. Murphy R, Straebler S, Cooper Z, Fairburn CG. Cognitive behavioral therapy for eating disorders. Psychiatr Clin North Am. (2010) 33:611–27. doi: 10.1016/j.psc.2010.04.004
182. van Ravesteyn LM, Lambregtse-van den Berg MP, Hoogendijk WJG, Kamperman AM. Interventions to treat mental disorders during pregnancy: a systematic review and multiple treatment meta-analysis. PLoS ONE. (2017) 12:e0173397. doi: 10.1371/journal.pone.0173397
183. Meltzer-Brody S, Howard LM, Bergink V, Vigod S, Jones I, Munk-Olsen T, et al. Postpartum psychiatric disorders. Nat Rev Dis Primers. (2018) 4:18022. doi: 10.1038/nrdp.2018.22
184. Murphy R, Straebler S, Basden S, Cooper Z, Fairburn CG. Interpersonal psychotherapy for eating disorders. Clin Psychol Psychother. (2012) 19:150–8. doi: 10.1002/cpp.1780
185. Hay PPJ, Bacaltchuk J, Stefano S, Kashyap P. Psychological treatments for bulimia nervosa and binging. Cochrane Database Syst Rev. (2009) 4:CD000562. doi: 10.1002/14651858.CD000562.pub3
186. Emery RL, Grace JL, Kolko RP, Levine MD. Adapting the eating disorder examination for use during pregnancy: Preliminary results from a community sample of women with overweight and obesity. Int J Eat Disord. (2017) 50:597–601. doi: 10.1002/eat.22646
187. Dellava JE, Von Holle A, Torgersen L, Reichborn-Kjennerud T, Haugen M, Meltzer HM, et al. Dietary supplement use immediately before and during pregnancy in norwegian women with eating disorders. Int J Eat Disord. (2011) 44:325–32. doi: 10.1002/eat.20831
188. Lupattelli A, Spigset O, Torgersen L, Zerwas S, Hatle M, Reichborn-Kjennerud T, et al. Medication use before, during, and after pregnancy among women with eating disorders: a study from the Norwegian mother and child cohort study. PLoS ONE. (2015) 10:e0133045. doi: 10.1371/journal.pone.0133045
189. Hardaway JA, Crowley NA, Bulik CM, Kash TL. Integrated circuits and molecular components for stress and feeding: implications for eating disorders. Genes Brain Behav. (2015) 14:85–97. doi: 10.1111/gbb.12185
190. Monteleone AM, Ruzzi V, Patriciello G, Cascino G, Pellegrino F, Vece A, et al. Emotional reactivity and eating disorder related attitudes in response to the trier social stress test: an experimental study in people with anorexia nervosa and with bulimia nervosa. J Affect Disord. (2020) 274:23–30. doi: 10.1016/j.jad.2020.05.051
191. Levine TA, Grunau RE, Segurado R, Daly S, Geary MP, Kennelly MM, et al. Pregnancy-specific stress, fetoplacental haemodynamics, and neonatal outcomes in women with small for gestational age pregnancies: a secondary analysis of the multicentre prospective observational trial to optimise paediatric health in intrauterine growth. BMJ Open. (2017) 7:1–11. doi: 10.1136/bmjopen-2016-015326
192. Fall CH. Fetal programming and the risk of non-communicable disease. Indian J Pediatr. (2013) 80:S13–20. doi: 10.1007/s12098-012-0834-5
193. Dietary reference values for nutrients summary report. EFSA J. (2017) 14:e15121. doi: 10.2903/sp.efsa.2017.e15121
194. Hanson MA, Bardsley A, De-Regil LM, Moore SE, Oken E, Poston L, et al. The international federation of gynecology a nd obstetrics (FIGO) recommendations on adolescent, preconception, and maternal nutrition: “Think Nutrition First”. Int J Gynaecol Obs. (2015) 131:S213–53. doi: 10.1016/S0020-7292(15)30034-5
195. Kominiarek MA. Nutrition recommendations in pregnancy and lactation. Med Clin North Am. (2016) 100:1199–215. doi: 10.1016/j.mcna.2016.06.004
Keywords: eating disorders, anorexia nervosa, bulimia nervosa, binge eating disorders, pregnancy, fetal outcomes, epigenetics, maternal psychopathology
Citation: Sebastiani G, Andreu-Fernández V, Herranz Barbero A, Aldecoa-Bilbao V, Miracle X, Meler Barrabes E, Balada Ibañez A, Astals-Vizcaino M, Ferrero-Martínez S, Gómez-Roig MD and García-Algar O (2020) Eating Disorders During Gestation: Implications for Mother's Health, Fetal Outcomes, and Epigenetic Changes. Front. Pediatr. 8:587. doi: 10.3389/fped.2020.00587
Received: 17 May 2020; Accepted: 10 August 2020;
Published: 17 September 2020.
Edited by:
Yogen Singh, Cambridge University Hospitals NHS Foundation Trust, United KingdomReviewed by:
Surendra Sharma, Women & Infants Hospital of Rhode Island, United StatesSilvia Salvatore, University of Insubria, Italy
Copyright © 2020 Sebastiani, Andreu-Fernández, Herranz Barbero, Aldecoa-Bilbao, Miracle, Meler Barrabes, Balada Ibañez, Astals-Vizcaino, Ferrero-Martínez, Gómez-Roig and García-Algar. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Giorgia Sebastiani, Z3NlYmFzdGlAY2xpbmljLmNhdA==
†These authors share first authorship