
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Immunol. , 21 June 2019
Sec. Autoimmune and Autoinflammatory Disorders
Volume 10 - 2019 | https://doi.org/10.3389/fimmu.2019.01303
This article is part of the Research Topic Skin Autoimmunity View all 69 articles
 Claudia Zeidler1
Claudia Zeidler1 Manuel Pedro Pereira1
Manuel Pedro Pereira1 Flavien Huet2,3
Flavien Huet2,3 Laurent Misery2,3
Laurent Misery2,3 Kerstin Steinbrink1
Kerstin Steinbrink1 Sonja Ständer1*
Sonja Ständer1*Pruritus in autoimmune and inflammatory dermatoses is a common symptom that can be severe and affect the quality of life of patients. In some diseases, pruritus is related to disorders activity and severity or may occur independent of the disease. Despite the high prevalence, the symptom is still underrated and there are only a few trials investigating the efficacy of drugs for disease-specific pruritus. In this review, the characteristics and possible pathomechanisms of pruritus in various dermatoses like autoimmune bullous diseases, connective tissue diseases as well as autoimmune-associated dermatoses (atopic dermatitis, psoriasis vulgaris) is illustrated. Additionally, studies analyzing the antipruritic treatment are discussed. Summarizing, the prevalence of pruritus in these diseases demonstrates the importance for symptom recognition and the need for an efficient antipruritic therapy.
Autoimmune diseases occur due to a deregulated immune response directed to the body own tissues. Cutaneous manifestations may occur secondarily to systemic autoimmune conditions such as lupus erythematosus (LE) or systemic sclerosis (SSc) or result from primary dermatoses as e.g., in autoimmune bullous diseases (AIBD) or in vitiligo (1). A feature of autoimmune disorders is the occurrence of an exacerbated inflammation owing to an enhanced release of pro-inflammatory mediators. One common symptom is pruritus which is listed by the Global Burden of Disease project as one of the 50 most common interdisciplinary symptoms leading to high burden levels (2). Chronic pruritus (CP) is often accompanied by paresthetic sensations like warmth, burning and stinging (3). Physicians should be alert to this debilitating symptom and offer patients with adequate antipruritic care. In this review we provide an overview of the most relevant autoimmune dermatoses focusing on pruritus, including, pathophysiological mechanisms, clinical features and when available anti-pruritic treatment options (Table 1). Atopic dermatitis (AD) and psoriasis vulgaris are included since autoimmunity phenomena have been observed in these (4–7).
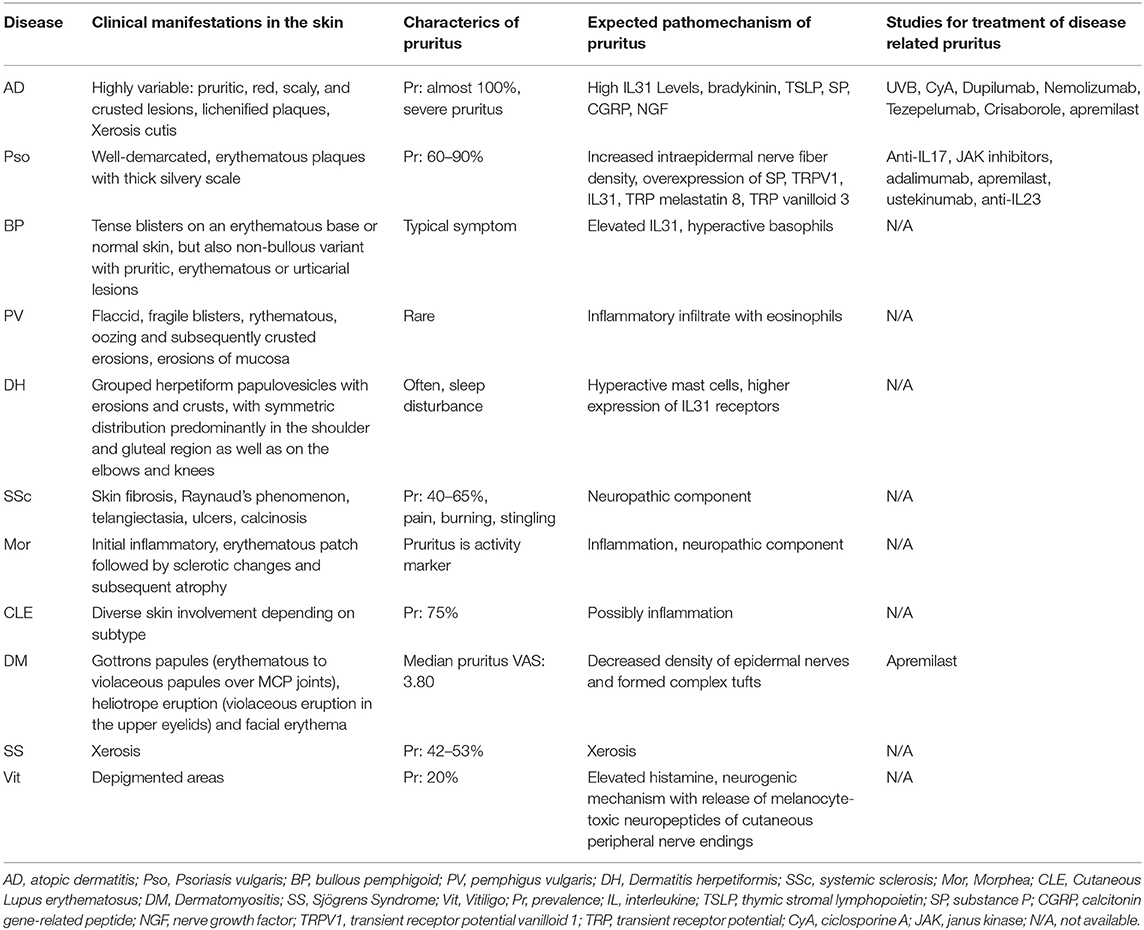
Table 1. Overview of diseases and pruritus-specific data.
AD is a common disease which affects about 20% of children and 5% of adults (8). The pathophysiological mechanisms are an immune deviation toward T helper cells 2 cells secreting predominantly IL4, IL5, and IL13 in in the initiation phase with consequent increased IgE production, a deficient skin barrier function, an abnormal microbial colonization and a neurogenic inflammation (9). Severe pruritus appears in almost all patients (10), correlating with severity of AD (11). Ninety-three percent of patients reported to scratch often or very often, and perceive scratching as pleasurable which lead to itch-scratch cycle (12). Further, stinging and burning were described, suggesting a neuropathic component. Pruritus impacts strongly the sleep and the quality of live (QoL), which leads to a higher rate of anxiety, depression and suicidal ideation (13). Among pruritus mediators, the role of histamine is restrained, as indicated by the inefficacy of anti-histamine treatment (14). Proteinase activated receptor-2 expressed by keratinocytes and cutaneous free nerve endings is involved in the pruritus pathway of AD (15). Recently, ORAI1, a channel mediating store-operated Ca2+ influx which is required for NFAT-dependent cytokines expression, was shown to be an regulator of AD cytokine and itch-causing compound (16). Activated nerves fibers release neuropeptides like CGRP and substance P (SP). IL31 produced by Th2 cells is overexpressed in lesional skin and in serum (17) and correlates with the disease severity (18). Thus, IL31 induces directly itching via its receptor which is expressed on keratinocytes and nerve fibers (NF) (19). Also, environment plays a role. Various organic components of pollutant activate the aryl hydrocarbon receptor in keratinocytes and stimulate artemin, a neurotrophic factor which is responsible for epidermal hyperinnervation (20). This may be partly responsible for itch sensitization, although a new study questions this affirmation (21, 22).
A few studies have investigated the treatment of AD-associated pruritus. In addition to known therapies like narrow band UVB, which lead to a decreased pruritus intensity in 90% of patients with AD (23), or cyclosporine which has shown a significant reduction of pruritus intensity and decreased IL31 serum levels (24) also new treatment regimens have been investigated for their antipruritic effect in AD. Dupilumab, a monoclonal antibody (mAb) binds to the alpha subunit of the IL4 receptor, thereby inhibiting the binding of IL4 and IL13. In placebo controlled studies, dupilumab significantly reduced pruritus (44–51% reduction) (25). Tralokinumab and lebrikizumab target anti-IL13 leading to AD improvement and decrease of pruritus. Nemolizumab, a IL-31 receptor mAb, inhibits the IL31 signaling and reduced the intensity of pruritus in a phase II study [up to 90% in a 52 week (26)]. Tezepelumab is a mA targeting TSLP. In light of the role of TSLP in atopic pruritus, tezepelumab seems very interesting. Nevertheless, in a phase II study, tezepelumab showed limited efficacy on pruritus and inflammatory signs (27).
Phosphodiesterase 4 (PDE4) is an enzyme that regulates cAMP levels and thereby pro-inflammatory cytokines involved in AD. Crisaborole, a new topical PDE4 inhibitorapproved in AD, showed improvement in pruritus (28). In a phase II study, apremilast, an oral PDE4 inhibitor, showed modest efficacy in AD and a decrease in pruritus but no significant compared to placebo (25).
JAK/STAT pathways are activated by typical AD cytokines such as IL,4, IL13, or IL31. Inhibitors are being evaluated for oral treatment of AD. First results seem promising (29).
The level of SP is involved in neurogenic inflammation and increased pruritus. Though effective in prurigo nodularis, in phase II study with oral NK1-receptor antagonist, serlopitant did not show improvement in pruritus of patients with AD.
Psoriasis was considered as a non-pruritic dermatosis. Nowadays, numerous studies have clearly documented that pruritus is a very frequent symptom of psoriasis (30) with a prevalence of 60–90% in patients suffering from psoriasis and a mean severity around 6/10 points on visual analog scale (VAS) (30). Pruritus is higher in patients with dry skin, stress (31) or the presence of depression and anxiety disorders (32). CPcorrelates also with the use of antacids, angiotensin receptor blockers, angiotensin enzyme converting inhibitors and beta-blockers (33).
A large majority of patients with psoriasis consider pruritus as the most bothersome symptom of their disease (34). Patients with pruritus report a greater reduction in their health-related QoL, including the ability to sleep, compared to those without pruritus. The severity of pruritus correlates with the degree of QoL impairment. The pathogenesis of pruritus in psoriasis is poorly known since the main cytokines involved in psoriasis are not known to be pruritogenic. The major concept of pruritus origin is focused on neurogenic inflammation, through the release of neuropeptides from nerve endings, in association with a modified innervation density in psoriasis as well as an abnormal functioning of the peripheral opioid system (22). Overexpression of genes, such as phospholipase A2 IVD, SP, voltage-gated sodium channel 1.7, transient receptor potential (TRP) vanilloid 1, IL17A, IL23A, IL31, TRP melastatin 8, TRP vanilloid 3, phospholipase C, and IL36α/γ, has been shown in pruritic psoriatic skin (35). The efficacy of treatments of psoriasis is commonly judged on their effects on visible skin lesions but it might be more important to consider the resolution of pruritus, since it is the first preoccupation of the patients (34) and because there is no specific antipruritic therapy to treat pruritus in psoriasis. A systematic meta-analysis has evaluated the effect of systemic psoriasis treatments on psoriatic pruritus (36). Anti-IL17 showed the greatest antipruritic effect. JAK inhibitors were more effective than adalimumab, which was more effective than apremilast. Other studies could not be included in the meta-analysis for methodological reasons. Nevertheless, UVB phototherapy and cyclosporine were also noted to be effective. Some studies showed the favorable effects of ustekinumab (anti-IL12) (37) and anti-IL23 (38) on pruritus. A topical inhibitor of nerve growth factor (NGF) receptor has also been shown to be effective for the treatment of pruritus due to psoriasis (39).
AIBD are a heterogeneous group of severe dermatoses characterized by the presence of autoantibodies against cutaneous adhesion molecules (40).
Pruritus in the elderly patients is a frequent complaint and bullous pemphigoid (BP) is a rare but an important differential diagnosis. Recent data suggest that pruritus of BP might be linked to elevated levels of cutaneous IL31 (41). Histologically, BP is characterized by a dense infiltrate of eosinophils which produce and release IL31 (42). IL31 is well-known for the induction of pruritus via inflammatory and neuronal mechanisms (43). In addition, histamine released from basophils seems to play a role. Basophils might be present in BP lesions, too (44). Compared to healthy control basophils, circulating peripheral basophils from BP patients degranulate and release histamine when incubated with BP180 (45).
In BP, all clinical phenotypes are associated with severe pruritus (46). Pruritus can precede the development of the lesions (47). In a preclinical stage, pruritus without visible skin lesions can be the only manifestation of BP (48, 49). Interestingly, there are also many reports of atypical, mainly non-bullous, clinical variants of BP associated with IgG autoantibodies against BP180 and BP230 associated with pruritus as the common leading clinical symptom (50). These subtypes are heterogeneous and include eczematous, erythematous plaques, urticarial, papular and/or nodular skin lesions (50). However, a small study including patients with chronic pruritic skin disorders (n = 78) and patients with non-inflammatory skin disease (n = 93) failed to detect specific autoantibodies (40). Elderly patients with pruritus may present with a broad range of underlying diseases including metabolic diseases, drug intake and neuropathic conditions (51). To address the specific question on the prevalence of atypical BP as an origin of CP in the elderly, a large population of patients' needs to be investigated.
Scratching typically accompanies pruritus in BP. Subsequently, patients develop excoriations, bleeding and crusts (Figure 1). Some can even develop chronic prurigo lesions due to prolonged scratching behavior (52). Patients experience pruritus to all day and night times without a preference and aggravation after emotional stress (46).

Figure 1. Seventy-eight-year old female patient with BP. Excoriations, bleeding and crusts caused by scratching can be observed.
The current therapy recommendations do not outline specific antipruritic therapies besides the immunosuppressive therapies (52). Pruritus parallels the disease course in BP. Accordingly, cessation of pruritus is one criterion of disease control in BP (49) and monitoring of pruritus is an important step which can be done using the Subjective Bullous Pemphigoid Disease Area Index pruritus score (49). For patients with impaired mental functioning, indirect assessment of pruritus via presence of signs of scratching and sleep disturbance is suggested (49).
Pemphigus is a potentially life-threatening AIBD and characterized by flaccid fragile blisters and erosions of the skin and/or mucous membranes. In contrast to BP, pruritus is less frequently present and with lower intensity in the pemphigus group (46). The most common subjective symptoms reported by patients with pemphigus vulgaris are burning (83.1%), pain (68.4%), and pruritus (47.5%) (53). Histopathologically, a suprabasal, akantholytic separation and blistering with a retention of basal keratinocytes along the basement membrane zone, and sparse inflammatory infiltrate in the dermis with eosinophils can be observed in pemphigus. The inflammation might be of great relevance for the induction of pruritus. Pemphigus foliaceus is another disease of this group. Here, pruritus occurs in more than half of the patients (61%) (54). The histopathological characteristic findings include intraepithelial cleavage with acantholysis beneath the stratum corneum and a dermal inflammation, predominantly with neutrophils, mast cells and plasma cells (54). Although there is little systematic data on pruritus in the pemphigus group, the parameter pruritus contributes to the assessment whether the disease is controlled or not (55).
Dermatitis herpetiformis (DH) is found more often in young adults and children and often associated with coeliac disease. It is characterized by granular deposits of IgA in dermal papillae, as well as deposits of other immunoglobulins and complement components (56). Pruritus is common and often the first symptom. The intensity of pruritus is high with a mean intensity of pruritus of 8/10 on a numerical rating scale. 2/3 of patients have sleep disorders related to pruritus (57). In the same study group the serum IL31 levels were reduced in DH compared to a healthy control group. This was surprising, because IL31 levels are increased in other pruritic dermatoses like AD (58) and psoriasis vulgaris (59). One explanation could be that mast cells are hyperactive which leading to a higher expression of IL31 receptors, which may be the reason for the low serum concentration of IL31 (57). Usually, pruritus reliefs during treatment but further studies on antipruritic effects are missing.
The manifestations of SSc are diverse. Abnormalities of the circulation (most notably Raynauds phenomenon) and involvement of multiple organ systems, including the renal, pulmonary, cardiac, and gastrointestinal systems due to fibrosis and vasculopathy development, are most prominent. Skin involvement is characterized by variable extent and severity of skin thickening and hardening with edematous swelling and erythema. With a prevalence of 40–65%, pruritus is a common symptom of SSc, which occurs not only in the affected areas but also often on the extremities or generalized (60). In addition to pruritus, patients experience stinging, burning and pain, which suggests that pruritus in SSc has a neuropathic component (61) caused by compression of small NF by thickened collagen. There are no data which investigate the antipruritic effect by an effective therapy of SSc. However, it might be assumed that modified NF necessitates a specific antipruritic therapy.
Morphea is an idiopathic, inflammatory disorder. The initial sign is often an inflammatory, erythematous patch followed by sclerotic dermal changes and subsequent atrophy. There are a lot of variants describing the clinically based division into circumscribed (65%), generalized (8%), linear (6%), and mixed forms (62). Pruritus is a distressing symptom in morphea, which causes a reduction in QoL (63). Interestingly, pruritus leads to a greater restriction than the location of lesions in cosmetically or functionally sensitive sites (63). In particular, in an active morphea, pruritus is noticeable, so that it is proposed as an activity marker. The cause of pruritus has not been elucidated. Based on the previously described observation, it can be concluded that inflammation with an infiltrate from lymphocytes, plasma cells, eosinophils, and mast cells is an important factor in the development of pruritus. However, a neuropathic component in the later stage of the morphea by compression of small NF is also conceivable. Further investigations on antipruritic therapy are not available.
Cutaneous LE (CLE) shows diverse skin manifestations depending on the present subtype. The classification is based on clinical characteristics like photosensitive lesions which lead to hyperpigmentation, scarring and hair loss in discoid lupus erythematosus or purple plaques/nodules and edematous skin mainly in the acral regions in chilblain lupus {Patel 2013 #13}. The prevalence of pruritus is 75% in patients suffering from CLE (64). The severity was widely ranged from mild (62.1%), moderate (23.1%), and severe (14.8%) (64). The intensity of pruritus correlates with the activity of skin lesions suggesting that the pathomechanism of pruritus is related to inflammation. However, there are no pruritus specific studies regarding the pathophysiology. Immunosuppressive therapy like use corticosteroids and steroid-sparing agents can relieve pruritus (65, 66). However, pruritus is a common side effect antimalarial drugs which are often used in the treatment of CLE (67).
Sjögren syndrome (SS) is a rare autoimmune disease characterized by chronic dryness of the mucous membranes (sicca's syndrome) and by chronic, progressive inflammation and exocrine gland insufficiency (68). The syndrome can be divided into a primary (cause unknown) and a secondary SS (association with connective tissue disease) (68). The prevalence of pruritus is 42–53% in both types of SS together. Patients suffering from SS and pruritus have a greater impairment of QoL and a higher rate of sleep disturbance (69). An important factor in the pathophysiology of pruritus in SS is xerosis cutis which is underlined by the fact that the most pruritic locations in SS are the shins—a very common location of xerosis induced pruritus (70).
Dermatomyositis (DM) is a rare systemic autoimmune disease characterized by immunological responses to vascular and muscle-derived proteins, resulting in inflammation of the skin and muscles, and typical skin lesions such as Gottron's papules (erythematous to violaceous papules over MCP joints), heliotrope eruption (violaceous eruption in the upper eyelids) and facial erythema (71). In addition, skin lesions may be accompanied by pruritus, which is more intense when compared to pruritus in CLE (median VAS DM: 3.80/10, median VAS CLE: 2/10). Additionally pruritus affects the QoL in patients with DM (72). Pathophysiologically, a small fiber neuropathy with a decreased density of epidermal nerves and formed complex tufts is thought to contribute to pruritus in DM (73). Recently, the antipruritic effect of apremilast in dermatomyositis induced scalp pruritus was reported. However, further studies on antipruritic effects of drugs are missing (65).
Vitiligo is a rare, congenital or acquired, localized skin pigmentation disorder. The disease is due to destruction and loss of melanocytes. There are a lot of hypotheses on the etiology of vitiligo including cytotoxic immune responses and presence of antibodies against melanocytes (74). However, vitiligo is not considered as a typical autoimmune disease by itself but patients have a genetic susceptibility to other autoimmune or autoinflammatory diseases like thyroid disease (75). Other hypotheses focus on a neurogenic mechanism with release of melanocyte- toxic neuropeptides of cutaneous peripheral nerve endings (Al-Abadie) which may also explain incidental occurrence of pruritus in vitiligo. Other authors speculate on histamine exhibiting a role in vitiligo associated pruritus (76). Elevated blood histamine levels have been found in patients with vitiligo and pruritus in comparison with matched controls (76). The prevalence of pruritus in vitiligo is 20% (77). Interestingly, active vitiligo was associated in 78.1% of patients with pruritus and Koebner phenomenon. Most patients reported a moderate pruritus (average 5/10 on NRS) and several sensory qualities of pruritus as tingling (82.7%), crawling (18.5%), and burning (18.5%). Concerning the QoL, those patients with pruritus and vitiligo had significant higher DLQI scores than those without it (78). The majority of patients with pruritus had daily activity (60.5%) and several had also sleep disturbances (39.5%). Improvement was reported by topical corticosteroids (55.6%) and oral antihistamines (9.9%).
If there is no proven treatment and/or the causative therapy failed to relieve CP it is recommended to add stepwise an antipruritic treatment (Figure 2).
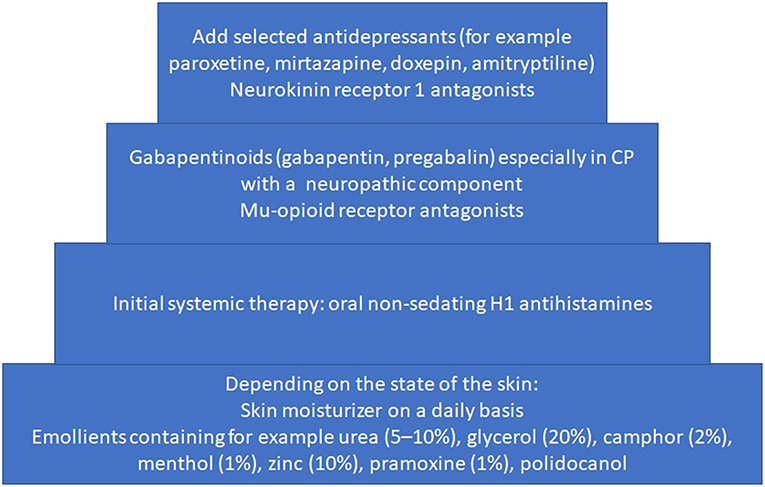
Figure 2. Stepwise therapeutic approach based on European S2k Guideline on Chronic Pruritus if causative treatment failed (79).
Pruritus is a common symptom of autoimmune conditions affecting the skin. However, it is often overlooked in clinical routine and by the scientific community. Therefore, awareness on this issue should be raised. A better understanding of the pathophysiological mechanisms leading to pruritus and of the clinical features in these diseases is needed. Additionally, clinical trials analyzing the anti-pruritic efficacy of relevant substances for this patient group would be an important step in order to achieve a better care for these patients and ultimately improve their QoL.
CZ, MP, LM, FH, KS, and SS wrote the paper. CZ and MP prepared the figure. CZ prepared the table.
LM: principal investigator for Abvie, Biogen, Janssen, Leo, Lilly, Pfizer, Sanofi; member of scientific advisory boards/consultant for Bayer, Celgene, Expanscience, Fresenius, Janssen, La Roche-Posay, Leo, Lilly, Menlo, Nestlé Skin Health, Novartis, Pierre Fabre, Sanofi; received grants from Beiersdorf, Bioderma, Celgene, Clarins, Expanscience, Johnson&Johnson, Nestlé Skin Health. FH: received finance of research project from Beiersdorf; consultant for Celgene; received material support from Novartis. KS: received research grants from Pfizer; principal investigator for Actelion; consultant for Leo. SS: principal investigator for Menlo Therapeutics Inc, Dermasence, Trevi Therapeutics, Galderma, Kiniksa, and Novartis; member of scientific advisory boards/consultant for Beiersdorf, Celgene, Galderma, Menlo Therapeutics Inc, NeRRe Therapeutics, Sienna, and Trevi Therapeutics, Novartis.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We acknowledge support from the Open Access Publication Fund of the University of Münster.
1. Rashtak S, Pittelkow MR. Skin involvement in systemic autoimmune diseases. Curr Dir Autoimmun. (2008) 10:344–58. doi: 10.1159/000131754
2. Hay RJ, Johns NE, Williams HC, Bolliger IW, Dellavalle RP, Margolis DJ, et al. The global burden of skin disease in 2010: an analysis of the prevalence and impact of skin conditions. J Invest Dermatol. (2014) 134:1527–34. doi: 10.1038/jid.2013.446
3. Schneider G, Pogatzki-Zahn E, Marziniak M, Stumpf A, Ständer S. Cutaneous sensory function is not related to depression and anxiety in patients with chronic pruritus with dysesthetic subqualities. Acta Derm Venereol. (2015) 95:289–93. doi: 10.2340/00015555-1933
4. Holmes J, Fairclough LC, Todd I. Atopic dermatitis and autoimmunity: the occurrence of autoantibodies and their association with disease severity. Arch Dermatol Res. (2019) 311:141–62. doi: 10.1007/s00403-019-01890-4
5. Das D, Akhtar S, Kurra S, Gupta S, Sharma A. Emerging role of immune cell network in autoimmune skin disorders: an update on pemphigus, vitiligo and psoriasis. Cytokine Growth Factor Rev. (2019) 45:35–44. doi: 10.1016/j.cytogfr.2019.01.001
6. Maurer M, Altrichter S, Schmetzer O, Scheffel J, Church MK, Metz M. Immunoglobulin E-Mediated Autoimmunity. Front Immunol. (2018) 9:689. doi: 10.3389/fimmu.2018.00689
7. Mylonas A, Conrad C. Psoriasis: Classical vs. paradoxical. The yin-yang of TNF and type i interferon. Front Immunol. (2018) 9:2746. doi: 10.3389/fimmu.2018.02746
8. Roduit C, Frei R, Depner M, Karvonen AM, Renz H, Braun-Fahrländer C, et al. Phenotypes of atopic dermatitis depending on the timing of onset and progression in childhood. JAMA Pediatr. (2017) 171:655–62. doi: 10.1001/jamapediatrics.2017.0556
9. Weidinger S, Novak N. Atopic dermatitis. Lancet. (2016) 387:1109–22. doi: 10.1016/S0140-6736(15)00149-X
10. Dawn A, Papoiu AD, Chan YH, Rapp SR, Rassette N, Yosipovitch G. Itch characteristics in atopic dermatitis: results of a web-based questionnaire. Br J Dermatol. (2009) 160:642–4. doi: 10.1111/j.1365-2133.2008.08941.x
11. Huet F, Severino-Freire M, Cheret J, Gouin O, Praneuf J, Pierre O, et al. Reconstructed human epidermis for in vitro studies on atopic dermatitis: a review. J Dermatol Sci. (2018) 89:213–8. doi: 10.1016/j.jdermsci.2017.11.015
12. Huet F, Faffa M-S, Poizeau F, Merhand S, Misery L, Brenaut E. Characteristics of pruritus in relation to self-assessed severity of atopic dermatitis. Acta Derm Venereol. (2019) 99:279–83. doi: 10.2340/00015555-3053
13. Drucker AM, Wang AR, Li W-Q, Sevetson E, Block JK, Qureshi AA. The burden of atopic dermatitis: summary of a report for the national eczema association. J Invest Dermatol. (2017) 137:26–30. doi: 10.1016/j.jid.2016.07.012
14. Sher LG, Chang J, Patel IB, Balkrishnan R, Fleischer AB JR. Relieving the pruritus of atopic dermatitis: a meta-analysis. Acta Derm Venereol. (2012) 92:455–61. doi: 10.2340/00015555-1360
15. Lee SE, Jeong SK, Lee SH. Protease and protease-activated receptor-2 signaling in the pathogenesis of atopic dermatitis. Yonsei Med J. (2010) 51:808–22. doi: 10.3349/ymj.2010.51.6.808
16. Wilson SR, The L, Batia LM, Beattie K, Katibah GE, McClain SP, et al. The epithelial cell-derived atopic dermatitis cytokine TSLP activates neurons to induce itch. Cell. (2013) 155:285–95. doi: 10.1016/j.cell.2013.08.057
17. Otsuka A, Tanioka M, Nakagawa Y, Honda T, Ikoma A, Miyachi Y, et al. Effects of cyclosporine on pruritus and serum IL-31 levels in patients with atopic dermatitis. Eur J Dermatol. (2011) 21:816–7. doi: 10.1684/ejd.2011.1470
18. Lu J, Wu K, Zeng Q, Xiang Y, Gao L, Huang J. Serum interleukin-31 level and pruritus in atopic dermatitis: a meta-analysis. Zhong Nan Da Xue Xue Bao Yi Xue Ban. (2018) 43:124–30. doi: 10.11817/j.issn.1672-7347.2018.02.003
19. Sonkoly E, Muller A, Lauerma AI, Pivarcsi A, Soto H, Kemeny L, et al. IL-31: A new link between T cells and pruritus in atopic skin inflammation. J Allergy Clin Immunol. (2006) 117:411–7. doi: 10.1016/j.jaci.2005.10.033
20. Hidaka T, Ogawa E, Kobayashi EH, Suzuki T, Funayama R, Nagashima T, et al. The aryl hydrocarbon receptor AhR links atopic dermatitis and air pollution via induction of the neurotrophic factor artemin. Nat Immunol. (2017) 18:64–73. doi: 10.1038/ni.3614
21. Tominaga M, Takamori K. Itch and nerve fibers with special reference to atopic dermatitis: therapeutic implications. J Dermatol. (2014) 41:205–12. doi: 10.1111/1346-8138.12317
22. Tan Y, Ng WJ, Lee SZ, Lee BT, Nattkemper LA, Yosipovitch G, et al. 3-dimensional optical clearing and imaging of pruritic atopic dermatitis and psoriasis skin reveals downregulation of epidermal innervation. J Invest Dermatol. (2019) 139:1201–4. doi: 10.1016/j.jid.2018.11.006
23. Reynolds NJ, Franklin V, Gray JC, Diffey BL, Farr PM. Narrow-band ultraviolet B and broad-band ultraviolet A phototherapy in adult atopic eczema: a randomised controlled trial. Lancet. (2001) 357:2012–6. doi: 10.1016/S0140-6736(00)05114-X
24. Pacor ML, Di Lorenzo G, Martinelli N, Mansueto P, Rini GB, Corrocher R. Comparing tacrolimus ointment and oral cyclosporine in adult patients affected by atopic dermatitis: a randomized study. Clin Exp Allergy. (2004) 34:639–45. doi: 10.1111/j.1365-2222.2004.1907.x
25. Simpson EL, Imafuku S, Poulin Y, Ungar B, Zhou L, Malik K, et al. A phase 2 randomized trial of apremilast in patients with atopic dermatitis. J Invest Dermatol. (2018) 139:1063–72. doi: 10.1016/j.jid.2018.10.043
26. Kabashima K, Furue M, Hanifin JM, Pulka G, Wollenberg A, Galus R, et al. Nemolizumab in patients with moderate-to-severe atopic dermatitis: randomized, phase II, long-term extension study. J Allergy Clin Immunol. (2018) 142:1121–30.e7. doi: 10.1016/j.jaci.2018.03.018
27. Simpson EL, Parnes JR, She D, Crouch S, Rees W, Mo M, et al. Tezepelumab, an anti-thymic stromal lymphopoietin monoclonal antibody, in the treatment of moderate to severe atopic dermatitis: a randomized phase 2a clinical trial. J Am Acad Dermatol. (2018) 80:1013–21. doi: 10.1016/j.jaad.2018.11.059
28. Paller AS, Tom WL, Lebwohl MG, Blumenthal RL, Boguniewicz M, Call RS, et al. Efficacy and safety of crisaborole ointment, a novel, nonsteroidal phosphodiesterase 4 (PDE4) inhibitor for the topical treatment of atopic dermatitis (AD) in children and adults. J Am Acad Dermatol. (2016) 75:494–503.e6.
29. Misery L, Huet F, Gouin O, Ständer S, Deleuran M. Current pharmaceutical developments in atopic dermatitis. Curr Opin Pharmacol. (2019) 46:7–13. doi: 10.1016/j.coph.2018.12.003
30. Yosipovitch G, Goon A, Wee J, Chan YH, Goh CL. The prevalence and clinical characteristics of pruritus among patients with extensive psoriasis. Br J Dermatol. (2000) 143:969–73. doi: 10.1046/j.1365-2133.2000.03829.x
31. Brenaut E, Garlantezec R, Talour K, Misery L. Itch characteristics in five dermatoses: non-atopic eczema, atopic dermatitis, urticaria, psoriasis and scabies. Acta Derm Venereol. (2013) 93:573–4. doi: 10.2340/00015555-1599
32. Remrod C, Sjostrom K, Svensson A. Pruritus in psoriasis: a study of personality traits, depression and anxiety. Acta Derm Venereol. (2015) 95:439–43. doi: 10.2340/00015555-1975
33. Reszke R, Bialynicki-Birula R, Szepietowski JC. Itch in Psoriasis: a new look at well-known subject. Acta Derm Venereol. (2019) 99:429–34. doi: 10.2340/00015555-3147
34. Lebwohl MG, Bachelez H, Barker J, Girolomoni G, Kavanaugh A, Langley RG, et al. Patient perspectives in the management of psoriasis: results from the population-based Multinational Assessment of Psoriasis and Psoriatic Arthritis Survey. J Am Acad Dermatol. (2014) 70:871–81.e1–30. doi: 10.1016/j.jaad.2013.12.018
35. Nattkemper LA, Tey HL, Valdes-Rodriguez R, Lee H, Mollanazar NK, Albornoz C, et al. The Genetics of chronic itch: gene expression in the skin of patients with atopic dermatitis and psoriasis with severe itch. J Invest Dermatol. (2018) 138:1311–7. doi: 10.1016/j.jid.2017.12.029
36. Therene C, Brenaut E, Barnetche T, Misery L. Efficacy of systemic treatments of psoriasis on pruritus: a systemic literature review and meta-analysis. J Invest Dermatol. (2018) 138:38–45. doi: 10.1016/j.jid.2017.05.039
37. Reich K, Pinter A, Lacour JP, Ferrandiz C, Micali G, French LE, et al. Comparison of ixekizumab with ustekinumab in moderate-to-severe psoriasis: 24-week results from IXORA-S, a phase III study. Br J Dermatol. (2017) 177:1014–23. doi: 10.1111/bjd.15666
38. Papp KA, Blauvelt A, Kimball AB, Han C, Randazzo B, Wasfi Y, et al. Patient-reported symptoms and signs of moderate-to-severe psoriasis treated with guselkumab or adalimumab: results from the randomized VOYAGE 1 trial. J Eur Acad Dermatol Venereol. (2018) 32:1515–22. doi: 10.1111/jdv.14910
39. Roblin D, Yosipovitch G, Boyce B, Robinson J, Sandy J, Mainero V, et al. Topical TrkA kinase inhibitor CT327 is an effective, novel therapy for the treatment of pruritus due to psoriasis: results from experimental studies, and efficacy and safety of CT327 in a phase 2b clinical trial in patients with psoriasis. Acta Derm Venereol. (2015) 95:542–8. doi: 10.2340/00015555-2047
40. van Beek N, Zillikens D, Schmidt E. Diagnosis of autoimmune bullous diseases. J Dtsch Dermatol Ges. (2018) 16:1077–91. doi: 10.1111/ddg.13637
41. Amber KT, Valdebran M, Kridin K, Grando SA. The role of eosinophils in bullous pemphigoid: a developing model of eosinophil pathogenicity in mucocutaneous disease. Front Med. (2018) 5:201. doi: 10.3389/fmed.2018.00201
42. Rudrich U, Gehring M, Papakonstantinou E, Illerhaus A, Engmann J, Kapp A, et al. Eosinophils are a major source of interleukin-31 in bullous pemphigoid. Acta Derm Venereol. (2018) 98:766–71. doi: 10.2340/00015555-2951
43. Feld M, Garcia R, Buddenkotte J, Katayama S, Lewis K, Muirhead G, et al. The pruritus- and TH2-associated cytokine IL-31 promotes growth of sensory nerves. J Allergy Clin Immunol. (2016) 138:500–508.e24. doi: 10.1016/j.jaci.2016.02.020
44. Hashimoto T, Rosen JD, Sanders KM, Yosipovitch G. Possible roles of basophils in chronic itch. Exp Dermatol. (2018). doi: 10.1111/exd.13705. [Epub ahead of print].
45. Dimson OG, Giudice GJ, Fu CL, van den Bergh F, Warren SJ, Janson MM, et al. Identification of a potential effector function for IgE autoantibodies in the organ-specific autoimmune disease bullous pemphigoid. J Invest Dermatol. (2003) 120:784–8. doi: 10.1046/j.1523-1747.2003.12146.x
46. Schroder L, Hertl M, Chatzigeorgakidis E, Phan NQ, Stander S. Chronic pruritus in autoimmune dermatoses: results of a comparative survey. Hautarzt. (2012) 63:558–66. doi: 10.1007/s00105-011-2319-2
47. Schmidt E, Zillikens D. Pemphigoid diseases. Lancet. (2013) 381:320–32. doi: 10.1016/S0140-6736(12)61140-4
48. Alonso-Llamazares J, Rogers RS, Oursler JR, Calobrisi SD. Bullous pemphigoid presenting as generalized pruritus: observations in six patients. Int J Dermatol. (1998) 37:508–14.
49. Bakker CV, Terra JB, Pas HH, Jonkman MF. Bullous pemphigoid as pruritus in the elderly: a common presentation. JAMA Dermatol. (2013) 149:950–3. doi: 10.1001/jamadermatol.2013.756
50. Schmidt T, Sitaru C, Amber K, Hertl M. BP180- and BP230-specific IgG autoantibodies in pruritic disorders of the elderly: a preclinical stage of bullous pemphigoid? Br J Dermatol. (2014) 171:212–9. doi: 10.1111/bjd.12936
51. Berger TG, Shive M, Harper GM. Pruritus in the older patient: a clinical review. JAMA (2013) 310:2443–50. doi: 10.1001/jama.2013.282023
52. Feliciani C, Joly P, Jonkman MF, Zambruno G, Zillikens D, Ioannides D, et al. Management of bullous pemphigoid: the european dermatology forum consensus in collaboration with the European Academy of Dermatology and Venereology. Br J Dermatol. (2015) 172:867–77. doi: 10.1111/bjd.13717
53. Ghodsi SZ, Chams-Davatchi C, Daneshpazhooh M, Valikhani M, Esmaili N. Quality of life and psychological status of patients with pemphigus vulgaris using Dermatology Life Quality Index and General Health Questionnaires. J Dermatol. (2012) 39:141–4. doi: 10.1111/j.1346-8138.2011.01382.x
54. Jordan TJ, Affolter VK, Outerbridge CA, Goodale EC, White SD. Clinicopathological findings and clinical outcomes in 49 cases of feline pemphigus foliaceus examined in Northern California, USA (1987-2017). Vet Dermatol. (2019) 30:209-e65. doi: 10.1111/vde.12731
55. Rencz F, Brodszky V, Stalmeier PF, Tamasi B, Karpati S, Pentek M, et al. Valuation of pemphigus vulgaris and pemphigus foliaceus health states: a convenience sample experiment. Br J Dermatol. (2016) 175:593–9. doi: 10.1111/bjd.14647
56. Reunala TL. Dermatitis herpetiformis. Clin Dermatol. (2001) 19:728–36. doi: 10.1016/S0738-081X(00)00184-X
57. Kulczycka-Siennicka L, Cynkier A, Waszczykowska E, Wozniacka A, Zebrowska A. The role of intereukin-31 in pathogenesis of itch and its intensity in a course of bullous pemphigoid and dermatitis herpetiformis. Biomed Res Int. (2017) 2017:5965492. doi: 10.1155/2017/5965492
58. Raap U, Wichmann K, Bruder M, Stander S, Wedi B, Kapp A, et al. Correlation of IL-31 serum levels with severity of atopic dermatitis. J Allergy Clin Immunol. (2008) 122:421–3. doi: 10.1016/j.jaci.2008.05.047
59. Narbutt J, Olejniczak I, Sobolewska-Sztychny D, Sysa-Jedrzejowska A, Slowik-Kwiatkowska I, Hawro T, et al. Narrow band ultraviolet B irradiations cause alteration in interleukin-31 serum level in psoriatic patients. Arch Dermatol Res. (2013) 305:191–5. doi: 10.1007/s00403-012-1293-6
60. Gourier G, Therene C, Mazeas M, Abasq-Thomas C, Brenaut E, Huet F, et al. Clinical characteristics of pruritus in systemic sclerosis vary according to the autoimmune subtype. Acta Derm Venereol. (2018) 98:735–41. doi: 10.2340/00015555-2980
61. Therene C, Brenaut E, Sonbol H, Pasquier E, Saraux A, Devauchelle V, et al. Itch and systemic sclerosis: frequency, clinical characteristics and consequences. Br J Dermatol. (2017) 176:1392–3. doi: 10.1111/bjd.14998
62. Tratenberg M, Gutwein F, Rao V, Sperber K, Wasserrman A, Ash J. Localized scleroderma: a clinical review. Curr Rheumatol Rev. (2017) 13:86–92. doi: 10.2174/1573397112666160907105434
63. Klimas NK, Shedd AD, Bernstein IH, Jacobe H. Health-related quality of life in morphoea. Br J Dermatol. (2015) 172:1329–37. doi: 10.1111/bjd.13572
64. Samotij D, Szczech J, Kushner CJ, Mowla MR, Danczak-Pazdrowska A, Antiga E, et al. Prevalence of pruritus in cutaneous lupus erythematosus: brief report of a multicenter, multinational cross-sectional study. Biomed Res Int. (2018) 2018:3491798. doi: 10.1155/2018/3491798
65. Charlton D, Moghadam-Kia S, Smith K, Aggarwal R, English JC, Oddis CV. Refractory cutaneous dermatomyositis with severe scalp pruritus responsive to apremilast. J Clin Rheumatol. (2019). doi: 10.1097/00124743-900000000-99059. [Epub ahead of print].
66. Smith GP, Argobi Y. Pruritus in autoimmune connective tissue diseases. Dermatol Clin. (2018) 36:267–75. doi: 10.1016/j.det.2018.02.013
67. Ajayi AA. Itching, chloroquine, and malaria: a review of recent molecular and neuroscience advances and their contribution to mechanistic understanding and therapeutics of chronic non-histaminergic pruritus. Int J Dermatol. (2018). doi: 10.1111/ijd.14252. [Epub ahead of print].
68. Ferro F, Marcucci E, Orlandi M, Baldini C, Bartoloni-Bocci E. One year in review 2017: primary Sjogren's syndrome. Clin Exp Rheumatol. (2017) 35:179–91.
69. Valdes-Rodriguez R, Rowe B, Lee HG, Moldovan T, Chan Y-H, Blum M, et al. Chronic pruritus in primary sjogren's syndrome: characteristics and effect on quality of life. Acta Derm Venereol. (2017) 97:385–6. doi: 10.2340/00015555-2524
70. Engelke M, Jensen JM, Ekanayake-Mudiyanselage S, Proksch E. Effects of xerosis and ageing on epidermal proliferation and differentiation. Br J Dermatol. (1997) 137:219–25. doi: 10.1046/j.1365-2133.1997.18091892.x
71. Mainetti C, Terziroli Beretta-Piccoli B, Selmi C. Cutaneous manifestations of dermatomyositis: a comprehensive review. Clin Rev Allergy Immunol. (2017) 53:337–56. doi: 10.1007/s12016-017-8652-1
72. Goreshi R, Chock M, Foering K, Feng R, Okawa J, Rose M, et al. Quality of life in dermatomyositis. J Am Acad Dermatol. (2011) 65:1107–16. doi: 10.1016/j.jaad.2010.10.016
73. Hurliman E, Groth D, Wendelschafer-Crabb G, Kennedy W, Kavand S, Ericson M, et al. Small-fibre neuropathy in a patient with dermatomyositis and severe scalp pruritus. Br J Dermatol. (2017) 176:209–11. doi: 10.1111/bjd.14678
74. Vachiramon V, Onprasert W, Harnchoowong S, Chanprapaph K. Prevalence and clinical characteristics of itch in vitiligo and its clinical significance. Biomed Res Int. (2017) 2017:5617838. doi: 10.1155/2017/5617838
75. Spritz RA. The genetics of generalized vitiligo: autoimmune pathways and an inverse relationship with malignant melanoma. Genome Med. (2010) 2:78. doi: 10.1186/gm199
76. Panja SK, Bhattacharya B, Lahiri SC. Role of histamine as a toxic mediator in the pathogenesis of vitiligo. Ind J Dermatol. (2013) 58:421–8. doi: 10.4103/0019-5154.119947
77. Linthorst Homan MW, Spuls PI, Korte J de, Bos JD, Sprangers MA, van der Veen JP. The burden of vitiligo: patient characteristics associated with quality of life. J Am Acad Dermatol. (2009) 61:411–20. doi: 10.1016/j.jaad.2009.03.022
78. Sangma LN, Nath J, Bhagabati D. Quality of life and psychological morbidity in vitiligo patients: a study in a teaching hospital from north-East India. Ind J Dermatol. (2015) 60:142–6. doi: 10.4103/0019-5154.152508
Keywords: itch, pruritus, psoriasis, atopic dermatitis, IL31, substance P, bullous pemphigoid
Citation: Zeidler C, Pereira MP, Huet F, Misery L, Steinbrink K and Ständer S (2019) Pruritus in Autoimmune and Inflammatory Dermatoses. Front. Immunol. 10:1303. doi: 10.3389/fimmu.2019.01303
Received: 29 March 2019; Accepted: 22 May 2019;
Published: 21 June 2019.
Edited by:
Ralf J. Ludwig, Universität zu Lübeck, GermanyReviewed by:
Christian Vestergaard, Aarhus University, DenmarkCopyright © 2019 Zeidler, Pereira, Huet, Misery, Steinbrink and Ständer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sonja Ständer, c29uamEuc3RhZW5kZXJAdW5pLW11ZW5zdGVyLmRl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.